Back to Journals » Infection and Drug Resistance » Volume 19
Hidden Toll of CRE Colonization: Tripled Three-Year Mortality Risk and Increased Bloodstream Infection Burden After Allo-HSCT—A Propensity-Adjusted Study
Authors Zhang Y, Wang R, Lyu G, Wang L, Liu X, Tian L, Huang Y, Kou J, Wu S, Cao W
Received 26 November 2025
Accepted for publication 30 January 2026
Published 10 February 2026 Volume 2026:19 579493
DOI https://doi.org/10.2147/IDR.S579493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Yuan Zhang,1 Rong Wang,1 Guoqing Lyu,1– 3 Lihua Wang,1 Xiankai Liu,1 Linlin Tian,1 Yan Huang,1– 3 Jiesen Kou,1 Sun Wu,1– 3 Weijie Cao4
1Department of Hematology, the First Affiliated Hospital of Xinxiang Medical University, Weihui, Henan Province, 453100, People’s Republic of China; 2Key Laboratory for Leukemia Molecular Diagnosis and Treatment in Xinxiang City, Weihui, Henan Province, 453100, People’s Republic of China; 3Key Laboratory for Lymphoma Molecular Diagnosis and Treatment in Xinxiang City, Weihui, Henan Province, 453100, People’s Republic of China; 4Department of Hematology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China
Correspondence: Sun Wu, Department of Hematology, the First Affiliated Hospital of Xinxiang Medical University, Weihui, Henan Province, 453100, People’s Republic of China, Email [email protected] Weijie Cao, Department of Hematology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China, Email [email protected]
Purpose: Carbapenem-resistant Enterobacteriaceae (CRE) colonization poses a major threat to the success of allogeneic hematopoietic stem cell transplantation (allo-HSCT). However, evidence on its long-term impact and the role of decolonization strategies remains limited.
Methods: This study included 240 allo-HSCT recipients prospectively screened for pre-transplant rectal CRE colonization (colonized n=80; non-colonized n=160; 1:2 matching). Inverse probability of treatment weighting (IPTW) was applied to achieve covariate balance (standardized mean difference < 0.10). Key outcomes included CRE bloodstream infection (BSI) incidence, hematopoietic engraftment time, graft-versus-host disease (GVHD) onset, and 3-year overall survival (OS), analyzed using Kaplan-Meier curves and Cox proportional hazards models. Strain and carbapenemase enzyme concordance between colonizing and infecting isolates were evaluated in BSI cases.
Results: CRE BSI occurred almost exclusively in colonized patients (26.6%, 21/79), with 81.0% strain concordance (predominantly Escherichia coli and Klebsiella pneumoniae) and 77.8% enzyme profile concordance (mainly metallo-β-lactamase/NDM) between pre-transplant colonizing and post-transplant infecting isolates. An 81.0% concordance rate was observed between CRE strain types isolated from perianal colonization samples and those from bloodstream infections. BSI-attributable 100-day mortality was 34.8% (8/23). Colonized patients exhibited delayed engraftment (neutrophils: 14 vs 13 days, P=0.044; platelets: 15 vs 14 days, P=0.014) and earlier chronic GVHD onset (150 vs 235 days, P=0.004), with comparable GVHD incidence. Both unweighted and IPTW-adjusted 3-year OS were markedly lower in colonized patients (62.5%/58% vs 85.0%/83%; HR 3.49, 95% CI 1.91– 6.38, P< 0.001).
Conclusion: Pre-transplant CRE colonization is strongly associated with poorer allo-HSCT outcomes, including increased CRE BSI incidence and 100-day mortality, delayed engraftment, accelerated cGVHD onset, and approximately threefold higher 3-year mortality risk. These findings position CRE colonization as a potentially modifiable driver of both early and long-term morbidity, highlighting the critical need for routine screening and targeted decolonization strategies to improve survival in this high-risk population.
Keywords: carbapenem-resistant Enterobacteriaceae, allogeneic hematopoietic stem cell transplantation, graft-versus-host-disease, overall survival: non-relapse mortality
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT serves as a curative therapy for a wide range of congenital and acquired hematopoietic disorders, as well as other life-threatening conditions.1 In China, allo-HSCT has been performed for nearly three decades, with remarkable advancements, particularly in the past ten years, leading significantly improved survival rates for patients with hematologic malignancies.2 However,patients undergoing allo-HSCT require pre-conditioning regimens and immunosuppressive agents to prevent graft-versus-host disease, rendering them more susceptible to infections. Within 100 days post-transplant, infection ranks as the third leading cause of death, with an associated mortality rate of 20%, indicating that early infections pose a significant threat to patient survival. After 100 days, infection becomes to the second leading cause of death, with an 11% mortality rate, emerging as a critical factor influencing long-term survival.3–5
Bloodstream infections (BSIs) represent the most common bacterial infection type in allo-HSCT patients, imposing a substantial clinical and economic burden. The reported the incidence of BSI after allo-HSCT ranges from 20% to 50%. Moreover, the occurrence of BSI is significantly correlated with increased post-transplant mortality.6 Antimicrobial resistance (AMR) has become a critical global public health challenge, particularly in emergency and hospital settings, where the widespread dissemination of multidrug-resistant strains has markedly increased both patient mortality and the complexity of clinical management. According to predictive statistical models, in 2019, 4.95 million deaths were associated with bacterial resistance, including 1.27 million deaths directly attributable to bacterial antimicrobial resistance. Hospital-acquired infections caused by multidrug-resistant strains have risen significantly, especially among Gram-negative bacteria resistant to carbapenems and third-generation cephalosporins. Among these, carbapenem-resistant Enterobacterales (CRE) infections, due to limited therapeutic options, have become a major concern in the global field of anti-infective therapy.7,8
The myelosuppressive effect of chemotherapy in patients with hematologic malignancies, combined with the use of myeloablative conditioning regimens and immunosuppressive agents prior to transplantation, significantly increases the risk of infection by antibiotic-resistant bacteria. These infections not only impose a serious burden on the quality of life of hematopoietic stem cell transplant recipients but also exert a direct negative impact on long-term prognosis. Currently, research on the influence of pre-transplant intestinal CRE colonization on post-transplant BSI incidence and survival outcomes after allo-HSCT remains limited. Therefore, this study aimed to evaluated the effect of pre-transplant intestinal CRE colonization on the development of post-transplant CRE BSI and long-term survival in patients undergoing allo-HSCT.
Materials and Methods
Patients
This study enrolled patients who underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT) in the Hematology Department of the First Affiliated Hospital of Xinxiang Medical University and the First Affiliated Hospital of Zhengzhou University between January 1, 2019, and December 31, 2024, and who consented to CRE screening.All participants underwent routine anal swab testing upon admission prior to transplantation. Patients with perianal colonization of carbapenem-resistant Enterobacteriaceae (CRE) were assigned to the CRE-positive group (n=80), while CRE colonization-negative patients were matched in a 1:2 ratio to serve as the control group (n=160), resulting in a total of 240 study subjects. The study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital of Xinxiang Medical University (EC-2018-694), and All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all patients for the use of their personal information in research. Follow-up was conducted through outpatient and inpatient medical record reviews, as well as telephone interviews, with the last follow-up date on July 2, 2025.
Intestinal CRE Colonization Screening
All enrolled patients underwent systematic weekly rectal swab screening for CRE colonization from admission until hematopoietic reconstitution. Rectal swabs were collected by trained clinical staff using a standardized technique: patients were positioned laterally, and a saline-moistened cotton swab was inserted >5 cm into the anus, rotated three times, and placed in a transport tube for prompt submission to the laboratory. Drug susceptibility testing was performed on detected CRE isolates.9–11
Blood Culture Collection
Blood cultures were obtained from patients presenting with chills or fever (oral temperature ≥38.3°C once or ≥38.0°C sustained for >1 hour; axillary ≥38.0°C once or ≥37.7°C sustained for >1 hour) during the peri-transplant period. Two sets of 10 mL peripheral blood samples were drawn consecutively for aerobic and anaerobic culture. CRE bloodstream infection (BSI) was diagnosed when blood cultures grew a CRE strain.9–11
Strain Isolation, Antimicrobial Susceptibility Testing, and Carbapenemase Detection
CRE strains were isolated from rectal swabs, with only one positive sample per patient counted. Bacterial identification and antimicrobial susceptibility testing were performed using the VITEK MS IVD 3.0 mass spectrometer and VITEK 2 Compact system, following the National Clinical Laboratory Operation Procedures. Targeted isolates included Enterobacteriaceae (eg, Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae, Enterobacter huaxiensis). CRE was defined as resistance to at least one carbapenem by broth microdilution (MIC ≥2 mg/L for ertapenem; ≥4 mg/L for imipenem or meropenem).
Carbapenemase production was confirmed using the modified carbapenem inactivation method (mCIM). Positive mCIM results were further differentiated by the modified EDTA-carbapenem inactivation method (eCIM): eCIM positivity indicated metallo-β-lactamase (MBL) production, while eCIM negativity suggested serine carbapenemase (with possible co-production of both enzyme types).
These procedures followed the protocols detailed in our previous publication.9
Data Collection and Variables
All clinical and epidemiological data were retrospectively extracted from the patients’ electronic medical record system and the clinical microbiology laboratory database. Collected variables encompassed demographics, pre-transplant disease characteristics, transplant-related details, antithymocyte globulin [ATG] use, CD34+ cell dose infused, hematopoietic cell transplantation-comorbidity index [HCT-CI], and Karnofsky Performance Status [KPS] score), CRE screening results (isolated CRE species and enzyme typing), and post-transplant outcomes (neutrophil and platelet engraftment status and days to engraftment, infection types and timing including perianal infection and CRE bloodstream infection [BSI], acute and chronic graft-versus-host disease [aGVHD/cGVHD] incidence, timing and severity, relapse, non-relapse mortality [NRM], overall survival [OS]).
Statistical Analysis
Baseline characteristics were summarized as medians (interquartile range, IQR) for continuous variables and counts with percentages for categorical variables. Between-group comparisons were performed using the Wilcoxon rank-sum test and χ2-test or Fisher’s exact test for categorical data, as appropriate. The exposure variable was pre-transplant anal swab status (positive=1, negative=0). The primary time-to-event outcome was overall survival (OS), defined as the time from the transplantation to death from any cause (in days). To addresspotential selection bias, an inverse probability of treatment weighting (IPTW) method based on propensity scores (PS) was applied. The PS model included baseline covariates: sex, age, ATG use, HCT-CI score, KPS score, transplant type, pretreatment intensity, and number of prior_recurrences. Logistic regression was used to estimate the probability of each patient receiving positive exposure (group=1), denoted as e(X) = P(A=1∣X). To reduce model misspecification and accountfor nonlinearity, age was modeled using natural cubic splines (df=3). Variables with few unique values (eg, number_of_forward_recurrence with only levels 0–2, and KPS) were treated as categorical factors and other covariates were entered as categorical variables. Stabilized IPTWs were calculated as follows: for the treatment group, p(A)/PS; for the control group, (1−p(A))/(1−PS). To limit influence of extreme weights, values were truncated at the 5th–95th percentiles. Covariate balance was assessed using standardized mean differences (SMDs), with |SMD| < 0.10 considered acceptable, and visualized using a Love plot. Outcome analyses were conducted on the weighted cohort. OS was evaluated with a weighted Cox proportional hazards model, reporting hazard ratios (HR) and 95% confidence intervals (CIs). The proportional hazards assumption was verified using Schoenfeld residuals. All statistical tests were two-sided with a significance level of α=0.05, and all analyses were performed in R software (version 4.5.1).
Results
Comparison of Baseline Characteristics
This study enrolled 240 patients undergoing allogeneic hematopoietic stem cell transplantation (allo-HSCT), including 80 patients with carbapenem-resistant Enterobacteriaceae (CRE) colonization detected by -positive anal swab screening, and 160 matched control without CRE colonization. The groups were matched in a 1:2 ratio to minimize potential confounding effects. This matching design improved group comparability, reduced selection bias and enabled a more reliable evaluation of the impact of CRE colonization’s on post-transplant outcomes.
Baseline characteristics were generally comparable between the two groups (Table 1). No significant difference was observed in sex distribution (56.3% male in the CRE-positive group vs 56.9% in the CRE-negative group; Z = 0.008, P = 0.927). The median age (Q1, Q3) was 33 (18, 43) years in the CRE-positive group and 28 (14, 39) years in the negative group, showing a statistically significant difference (Z = −2.144, P = 0.032).
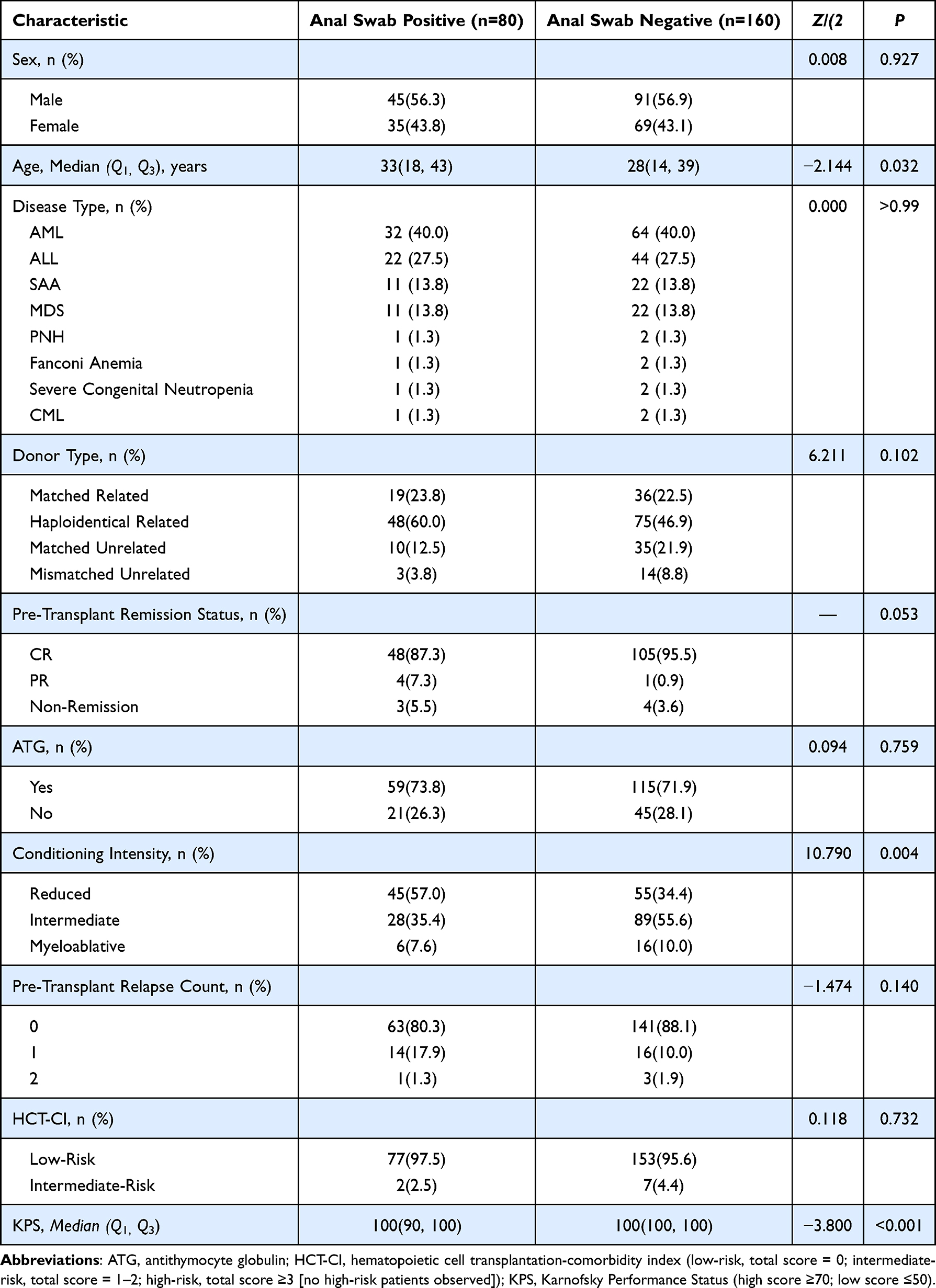 |
Table 1 Baseline Characteristics Comparison |
Regarding disease spectrum, the distributions were nearly identical between the two groups (χ2 = 0.000, P > 0.99). The majority of patients were diagnosed with acute myeloid leukemia (AML; 40.0% in both groups) and acute lymphoblastic leukemia (ALL; 27.5% in both groups), followed by severe aplastic anemia (SAA; 13.8%) and myelodysplastic syndrome (MDS; 13.8%). Less common diagnoses included paroxysmal nocturnal hemoglobinuria (PNH; 1.3%), Fanconi anemia (1.3%), severe congenital neutropenia (1.3%) and chronic myeloid leukemia (CML; 1.3%).
Transplantation-related characteristics showed no significant differences on donor type between the two groups (χ2 = 6.211, P = 0.102), with haploidentical related transplantation being the most common (60.0% in the CRE-positive group vs 46.9% in the CRE-negative group). Among leukemia patients only (n = 110), the pre-transplant complete remission (CR) rate was slightly lower in the CREpositive group (87.3% vs 95.5%) (Fisher’s exact test, P = 0.053). The use of antithymocyte globulin (ATG) was comparable between groups (73.8% vs 71.9%; χ2 = 0.094, P = 0.759), as was the hematopoietic cell transplantation-comorbidity index (HCT-CI) risk category (low-risk >95% in both; corrected χ2 = 0.118, P = 0.732). In contrast, conditioning regimen intensity differed significantly (χ2 = 10.790, P = 0.004), with the CREpositive group showing a higher proportion of reduced-intensity regimens (57.0% vs 34.4%) and a lower proportion of intermediate-intensity regimens (35.4% vs 55.6%). This novel observation represents the first to quantification of the relationship between CRE colonization and conditioning regimen selection, suggesting possible clinical adjustments to reduce infection risk and supporting personalized conditioning strategies for colonized patients. Pre-transplant relapse frequency (Mann–Whitney U-test, Z = −1.474, P = 0.140) and Karnofsky Performance Status (KPS) scores [median 100 (IQR 90, 100) vs 100 (IQR 100, 100); Z = −3.800, P < 0.001] showed no clinical meaningful differences in functional status, although the latter indicated slightly higher performance in the CRE-negative group.
Baseline Characteristics Before and After Inverse Probability of Treatment Weighting (IPTW) Adjustment
To further mitigate residual confounding arising from baseline imbalances—particularly in age, conditioning regimen intensity, and pre-transplant remission status identified i initial matching—a propensity score-based inverse probability of treatment weighting (IPTW) approach was employed for key covariates. This method assigns each patient a weight inversely related to the probability of their observed CRE colonization status, thereby effectively achieving balanced distributions of key covariates between groups (Table 2).
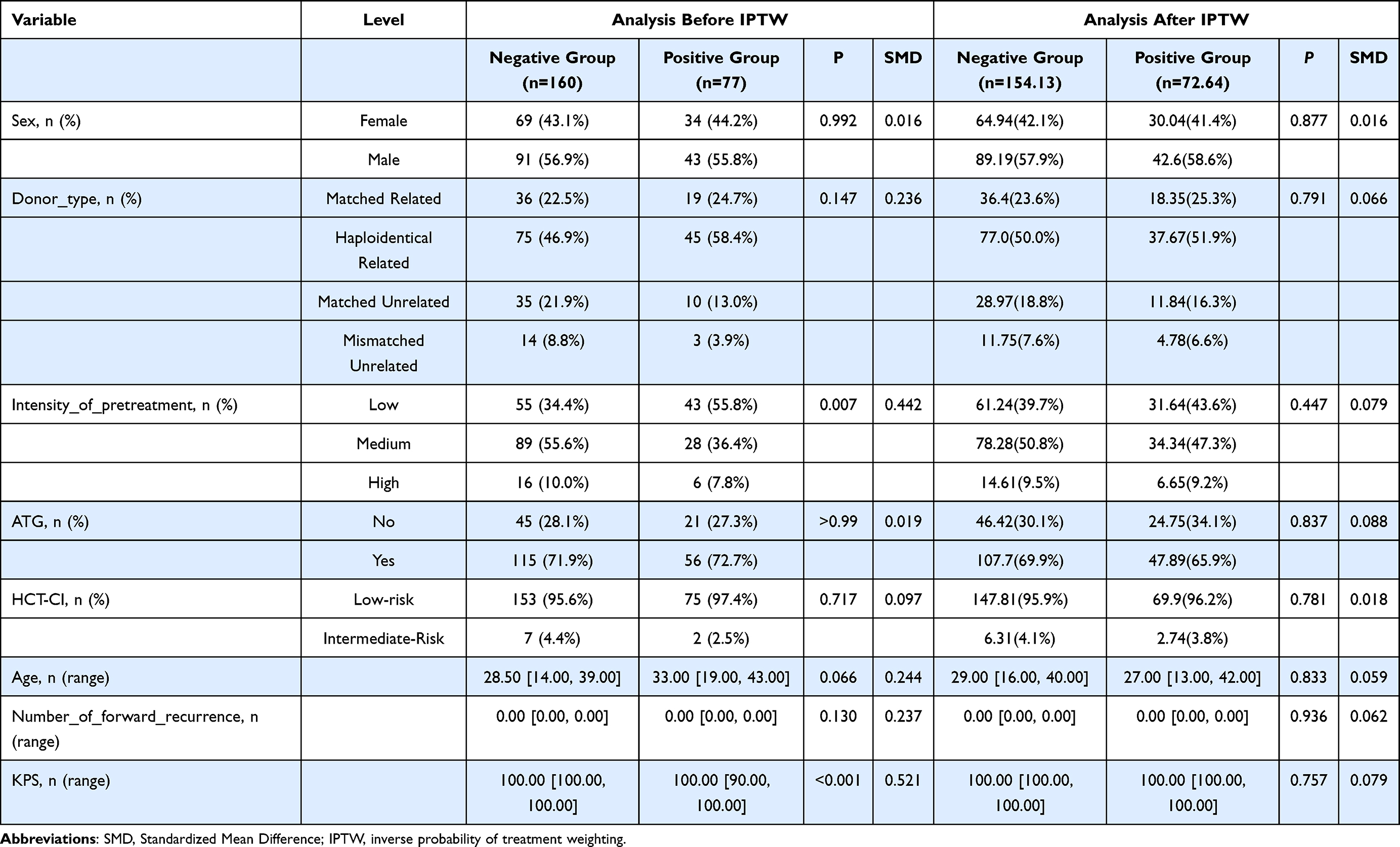 |
Table 2 Comparison of Baseline Characteristics Before and After IPTW Adjustment |
IPTW successfully equilibrated all baseline variables. Categorical factors, including sex (female: 42.1% vs 41.4%, P=0.877, SMD=0.016), donor type (eg, haploidentical related: 50.0% vs 51.9%, P=0.791, SMD=0.066), conditioning intensity (low: 39.7% vs 43.6%, P=0.447, SMD=0.079), ATG use (yes: 69.9% vs 65.9%, P=0.837, SMD=0.088), and HCT-CI risk (low-risk: 95.9% vs 96.2%, P=0.781, SMD=0.018), showed no significant differences and minimal SMDs. Continuous variables similarly achieved balance: median age shifted to 29 (16, 40) years in the negative group and 27 (13, 42) years in the positive group (P=0.833, SMD=0.059); relapse count remained at 0 (0, 0) in both (P=0.936, SMD=0.062); and KPS score equilibrated at 100 (100, 100) (P=0.757, SMD=0.079). These adjustments eliminated pre-IPTW disparities (eg, conditioning intensity P=0.007, age P=0.066, KPS P<0.001), confirming the method’s efficacy in reducing bias and supporting unbiased estimation of CRE colonization effects on transplant outcomes (Table 2).
SMDs for all covariates post-weighting were <0.10 (maximum 0.088), indicating robust balance. To minimize bias from patient baseline differences, select variables underwent propensity score-based IPTW re-evaluation, achieving comprehensive equilibrium in all baseline characteristics (Figure 1).
 |
Figure 1 Evaluation of Matching Quality Based on the Inverse Probability Weighting Model. SMDs for all covariates post-weighting were <0.10 (maximum 0.088), indicating robust balance. To minimize bias from patient baseline differences, select variables underwent propensity score-based IPTW re-evaluation, achieving comprehensive equilibrium in all baseline characteristics. |
Post-Transplant Engraftment, Acute and Chronic Graft-Versus-Host Disease (GVHD), and Viral Infections
Regarding engraftment outcomes, the CRE-colonized positive group experienced 12 cases of engraftment failure, including 10 with failure of both neutrophil and platelet engraftment and 2 with platelet-only failure; in contrast, the negative group had 4 failures, comprising 3 with dual failure and 1 with platelet-only failure. Statistical analyses indicated significant differences between groups in engraftment status (neutrophil engraftment: P = 0.002; platelet engraftment: P < 0.001). Furthermore, engraftment times were significantly delayed in the positive group compared to the negative group (neutrophils: 14 days vs 13 days, P = 0.044; platelets: 15 days vs 14 days, P = 0.014), suggesting that CRE colonization may impair hematopoietic reconstitution, potentially through microbiome disruption or subclinical inflammation.
For graft-versus-host disease (GVHD), incidence rates of acute (aGVHD: 37 cases in the positive group vs 59 in the negative group, P = 0.160) and chronic GVHD (cGVHD: 24 vs 44 cases, P = 0.663) did not differ significantly between groups. However, temporal patterns revealed notable disparities: median time to cGVHD onset was substantially shorter in the positive group (150 days vs 235 days, P = 0.004), whereas time to aGVHD was longer (34 days vs 23 days, P = 0.008). These findings imply a possible acceleration of chronic immune dysregulation in CRE-colonized patients, contrasting with delayed acute responses, which may reflect altered gut-derived alloreactivity.
Additionally, post-transplant infection rates for Epstein-Barr virus (EBV: 3 cases vs 5 cases, P = 0.768) and cytomegalovirus (CMV: 10 vs 21 cases, P = 0.920) showed no significant differences between groups, indicating that CRE colonization does not independently exacerbate these opportunistic viral threats in the allo-HSCT setting.
Incidence of CRE Bloodstream Infection After Allogeneic Hematopoietic Stem Cell Transplantation (Allo-HSCT)
Statistical analysis revealed that a total of 23 patients developed carbapenem-resistant Enterobacteriaceae (CRE) bloodstream infections post-transplant, with the majority occurring in the pre-transplant perianal CRE colonization-positive group (26.6%, 21/79), while only 2 cases were observed in the negative group (1.3%, 2/160). The incidence of CRE bloodstream infections differed significantly between the two groups (P < 0.001, Table 3), indicating that pre-transplant perianal CRE colonization is significantly associated with an increased risk of post-transplant CRE bloodstream infection (Table 3).
 |
Table 3 Post-Allo-HSCT CRE Bloodstream Infection Status |
Concordance Rate of Strain Types and Enzyme Types Between Pre-Transplant Perianal CRE Colonization and Post-Transplant CRE Bloodstream Infection Isolates
Among the 21 patients who developed carbapenem-resistant Enterobacteriaceae (CRE) bloodstream infections (BSIs) post-transplant, 17 (81.0%) exhibited identical infecting strains to those identified in pre-transplant perianal colonization. The predominant species included Escherichia coli (8 cases) and Klebsiella pneumoniae (8 cases), with one case of Klebsiella oxytoca (Figure 2A). In the 9 patients for whom enzyme typing was available, 7 (77.8%) showed concordance between the infecting strain’s enzyme profile and the pre-transplant colonizing strain, comprising 6 cases of metallo-β-lactamase (MBL) production and 1 case of NDM-type carbapenemase (Figure 2B). These findings substantiate the direct progression from gastrointestinal colonization to systemic CRE dissemination in allo-HSCT recipients, highlighting the critical role of pre-transplant screening in identifying at-risk patients.
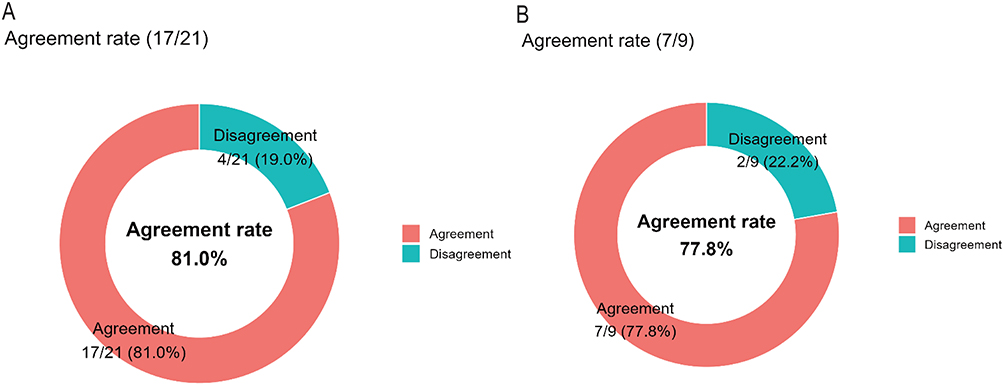 |
Figure 2 Concordance rate of strain types and enzyme types between pre-transplant perianal CRE colonization and post-transplant CRE bloodstream infection isolates. (A) Concordance rate of strain types between pre-transplant perianal CRE colonization and post-transplant CRE bloodstream infection isolates: 81.0% (17/21). (B) Concordance rate of carbapenemase enzyme types between pre-transplant perianal CRE colonization and post-transplant CRE bloodstream infection isolates: 77.8% (7/9). |
Mortality Within 100 Days Following CRE Bloodstream Infection
Among the 23 patients who developed CRE bloodstream infection after allo-HSCT, 8 deaths occurred within 100 days, yielding a mortality rate of 34.8% (8/23). Further analysis of survival times in the fatal cases revealed: the longest survival time was 59 days, the shortest was only 1 day, and the mean survival time was 22.5 days (95% CI: 8.9–36.1 days). These results indicate that patients with CRE bloodstream infection after allo-HSCT have an extremely poor prognosis, with a 100-day mortality rate as high as 34.8%, and significantly shortened survival times in fatal cases.
1-Year Overall Survival
Survival analyses revealed profound disparities between CRE-colonized (anal swab-positive) and non-colonized (anal swab-negative) patients, underscoring the prognostic burden of pre-transplant CRE colonization in allo-HSCT recipients. At 1 year post-transplant, survival rates were markedly lower in the positive group [62.0% (49/80)] compared to the negative group [86.9% (139/160)], with a highly significant difference (χ2 = 19.456, P < 0.001). Similarly, 1-year non-relapse mortality (NRM)—a critical endpoint isolating infection- and regimen-related deaths from relapse—occurred in 34.2% (27/80) of positive-group patients versus 11.8% (19/160) in the negative group (χ2 = 17.126, P < 0.001). These findings highlight CRE colonization as a potent driver of early post-transplant mortality, likely mediated by heightened susceptibility to invasive infections during profound neutropenia and immunosuppression. Median time to death post-transplant did not differ significantly between groups [86 (25, 187) days in the positive group vs 153 (84, 197) days in the negative group; Z = −1.426, P = 0.154], suggesting that while CRE accelerates mortality risk, the temporal pattern of death may be influenced by shared transplant-related toxicities rather than colonization-specific delays (Table 4).
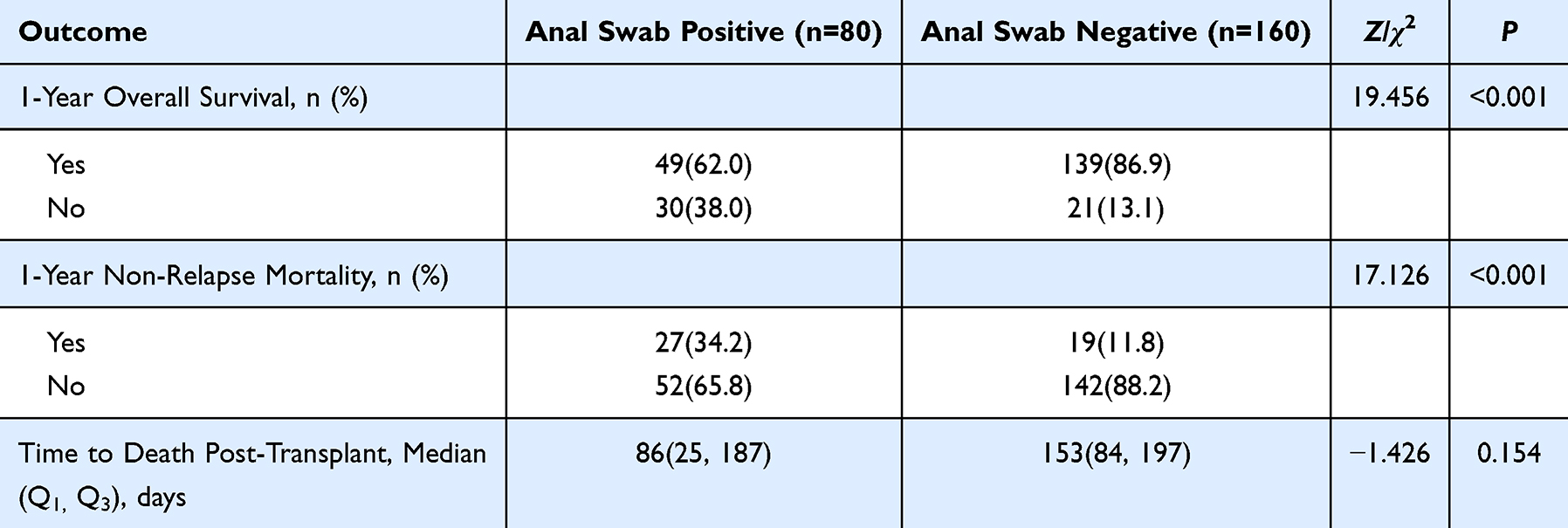 |
Table 4 Survival Outcomes |
Overall Survival (Unweighted and IPTW-Adjusted)
Kaplan-Meier survival analyses for overall survival (OS) illustrated marked disparities between carbapenem-resistant Enterobacteriaceae (CRE)-colonized (positive; cyan lines) and non-colonized (negative; pink lines) groups, presented both unweighted (left panel) and after inverse probability of treatment weighting (IPTW) with 5% trimming for the average treatment effect (right panel). In the unweighted analysis, curves diverged sharply within the first 100 days, with the positive group demonstrating accelerated decline and a 3-year OS of 62.5%, compared to 85.0% in the negative group (log-rank P < 0.0001). Post-IPTW adjustment preserved this separation, yielding 3-year OS rates of 58% for the positive group and 83% for the negative group (log-rank P < 0.0001), thereby affirming the persistence of CRE colonization’s adverse prognostic impact even after rigorous covariate balancing (Figure 3).
 |
Figure 3 Kaplan-Meier Estimates of Overall Survival (Unweighted and IPTW Log Rank Test). |
Cox Proportional Hazards Models
Cox proportional hazards models were constructed to quantify the independent impact of pre-transplant CRE colonization on overall survival (OS), with univariate (UV) and multivariate (MV) analyses performed both unweighted and after inverse probability of treatment weighting (IPTW) to address residual confounding. The primary exposure—CRE colonization status (positive vs negative)—emerged as the dominant predictor across all models, with hazard ratios (HRs) consistently exceeding 3.0 and robust statistical significance (unweighted UV: HR 3.14, 95% CI 1.81–5.43, P < 0.001; unweighted MV: HR 3.20, 95% CI 1.76–5.81, P < 0.001; IPTW UV: HR 3.28, 95% CI 1.84–5.86, P < 0.001; IPTW MV: HR 3.49, 95% CI 1.91–6.38, P < 0.001). This tripling of mortality risk persisted after adjustment for key covariates, including age, transplant type, conditioning intensity, ATG use, HCT-CI, relapse count, and KPS score, affirming CRE colonization as an unmitigated adverse factor in allo-HSCT (Table 5).
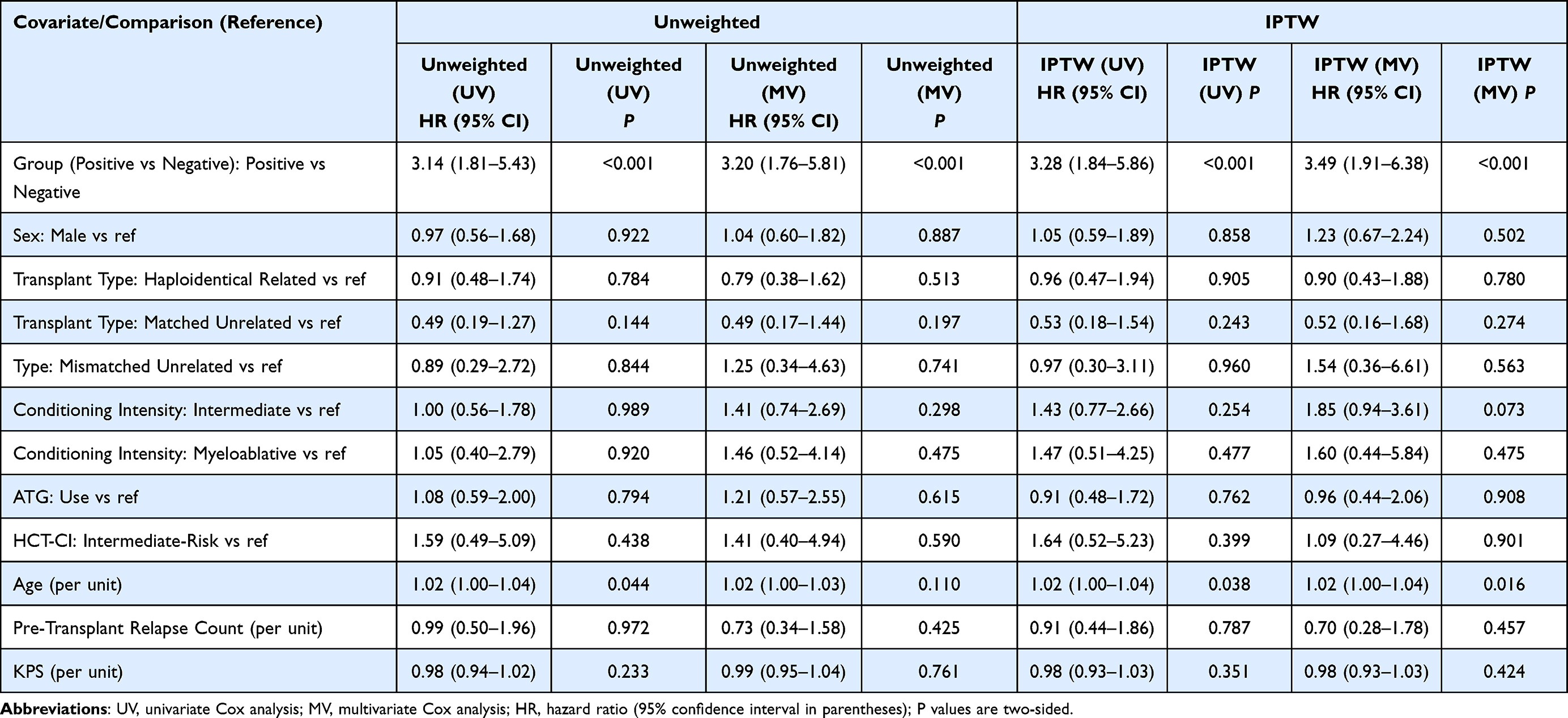 |
Table 5 Cox Regression Results for Overall Survival (Unweighted and IPTW-Adjusted) |
Secondary covariates exhibited minimal associations with OS. Sex showed no effect (eg, male vs female: unweighted MV HR 1.04, 95% CI 0.60–1.82, P = 0.887). Transplant donor types—relative to matched related—yielded HRs near unity (eg, haploidentical related: IPTW MV HR 0.90, 95% CI 0.43–1.88, P = 0.780), as did mismatched unrelated (IPTW MV HR 1.54, 95% CI 0.36–6.61, P = 0.563). Conditioning intensity (relative to reduced) trended toward higher risk with intermediate (IPTW MV HR 1.85, 95% CI 0.94–3.61, P = 0.073) or myeloablative regimens (IPTW MV HR 1.60, 95% CI 0.44–5.84, P = 0.475), though non-significant. ATG use (HR 0.96, 95% CI 0.44–2.06, P = 0.908) and HCT-CI intermediate risk (HR 1.09, 95% CI 0.27–4.46, P = 0.901) were neutral. Age per year increment conferred a modest risk elevation (IPTW MV HR 1.02, 95% CI 1.00–1.04, P = 0.016), while pre-transplant relapse count (HR 0.70, 95% CI 0.28–1.78, P = 0.457) and KPS per unit (HR 0.98, 95% CI 0.93–1.03, P = 0.424) showed no influence (Table 5).
The consistency of the CRE effect across unweighted and IPTW-stratified models underscores the latter’s value in bolstering causal inference, with IPTW MV estimates slightly amplifying the HR (3.49 vs 3.20), likely due to refined balancing of conditioning intensity imbalances. An innovation herein is the seamless incorporation of IPTW into Cox frameworks for CRE-specific prognostication—the first such application in a prospectively screened allo-HSCT cohort—enabling more precise risk attribution and supporting CRE decolonization as a modifiable intervention to attenuate this three-fold survival decrement.
Causes of Death After Allogeneic Hematopoietic Stem Cell Transplantation (Allo-HSCT)
Among the 53 total deaths observed in the cohort (30 in the CRE-colonized positive group and 23 in the negative group), infections emerged as the predominant cause, accounting for 47.2% (25/53) overall. This burden was disproportionately higher in the positive group [50.0% (15/30)] compared to the negative group [43.5% (10/23)], aligning with the elevated non-relapse mortality previously documented and implicating CRE colonization as a key facilitator of invasive infections in the post-transplant period. Acute graft-versus-host disease (aGVHD) ranked second at 17.0% (9/53) overall, with comparable distributions [13.4% (4/30) vs 21.7% (5/23)], suggesting that immune-mediated complications were not differentially influenced by colonization status. Cerebrovascular disease contributed 13.2% (7/53) of deaths [10.0% (3/30) vs 17.4% (4/23)], while relapse—a graft-versus-leukemia-independent endpoint—accounted for 9.4% (5/53) [10.0% (3/30) vs 8.7% (2/23)], indicating no excess disease progression attributable to CRE. Less frequent etiologies included hemorrhagic shock and transplant-related complications (each 5.7%; 3/53), heart failure (1.9%; 1/53), with minor group variations that did not reach statistical thresholds due to small event numbers (Table 6).
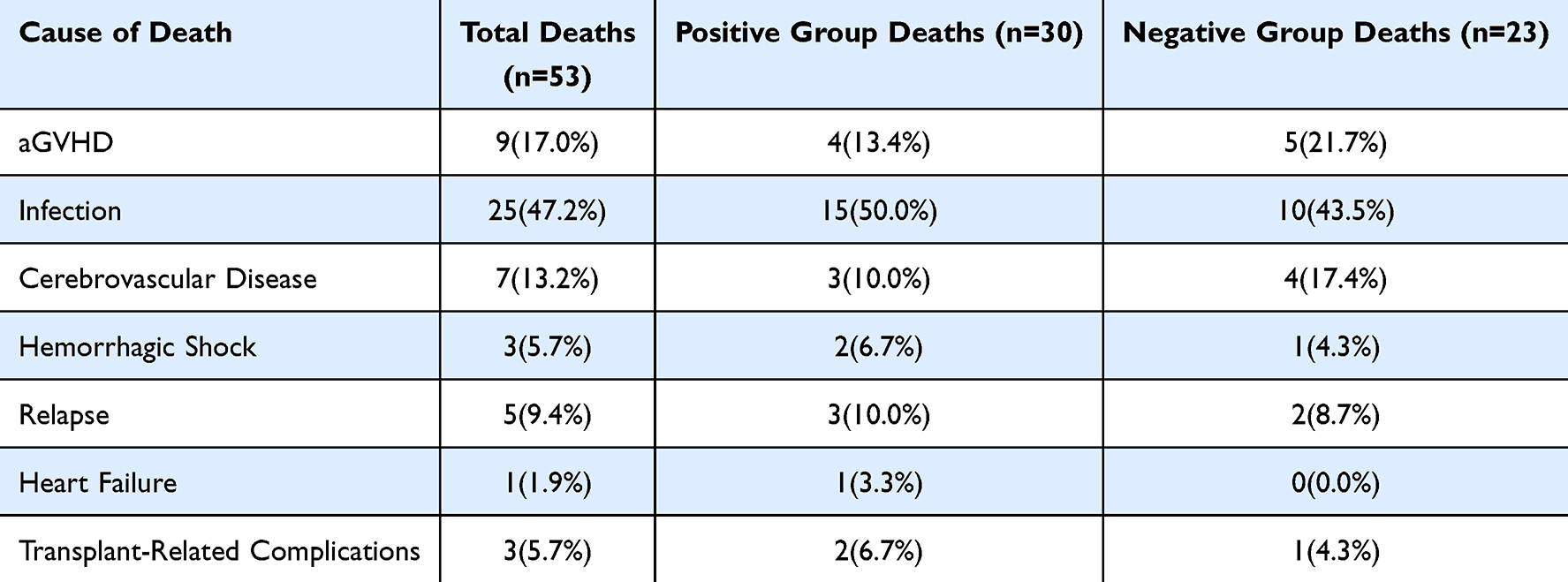 |
Table 6 Causes of Death After Allo-HSCT |
Discussion
Carbapenem antibiotics are the preferred drugs for treating multidrug-resistant bacterial infections in clinical practice and serve as the “last line of defense” against such infections. However, the emergence of carbapenem-resistant bacteria has become an undeniable global public health crisis. As early as 2013, a report released by the US Centers for Disease Control and Prevention (CDC) listed CRE as one of the three most urgent antibiotic resistance threats.12,13
This study found that the majority of the 23 patients with CRE bloodstream infections came from the pre-transplant perianal CRE colonization-positive group, with only 2 cases in the negative group, confirming that pre-transplant intestinal CRE colonization is a strong predictor of post-allo-HSCT CRE bloodstream infection. This result is highly consistent with the conclusions of Cao et al9 in a study of 185 allo-HSCT patients with hematologic diseases including AML, ALL, and MDS. Their research, using rectal swab screening, found that CRE intestinal colonization patients had a significantly increased risk of post-transplant CRE-related bloodstream infections, and carbapenem-resistant Klebsiella pneumoniae (CR-KP) colonization was an independent risk factor for bloodstream infection. Similarly, it aligns closely with the results of Zhang L et al and Bilinski J et al,14,15 confirming that pre-transplant CRE intestinal colonization significantly increases the risk of subsequent CRE bloodstream infection in patients and clearly establishing CRE bloodstream infection as a primary cause of patient mortality. The multicenter retrospective survey conducted by Girmenia C et al16 in Italy showed that 53.8% of transplant centers reported at least one CRE infection in their patients post-hematopoietic stem cell transplantation. The study also confirmed that CRE infection is an independent factor associated with death in infected patients after allo-HSCT (P=0.007), with high prevalence and lethality of CRE infection in allo-SCT patients (infection-related mortality rate 64.4%) and an upward trend in incidence. Currently, novel antibiotics such as ceftazidime/avibactam, meropenem/vaborbactam, imipenem/relebactam, tigecycline, polymyxins, and eravacycline have demonstrated excellent antibacterial activity and clear clinical efficacy in treating CRE-related infections; among them, combination therapy strategies show strong potential in enhancing therapeutic effects, delaying or reducing the risk of resistance development, providing important options for treating CRE-BSI in allo-HSCT patients.17–22
Further strain and enzyme consistency analysis revealed that 81.0% of the infecting strains matched the colonizing strains in species, and 77.8% of patients showed enzyme type consistency, suggesting that intestinal colonizing strains are the primary source of post-transplant bloodstream infections. Although 81.0% of infecting strains were concordant with pre-transplant colonizing strains, 19.0% were discordant. This discrepancy may be explained by several factors, including de novo post-transplant acquisition of CRE (such as nosocomial transmission during prolonged hospitalization or periods of neutropenia), polyclonal colonization with minor clones that were not detected at baseline, or technical limitations of strain typing methods (eg, reliance on phenotypic approaches rather than whole-genome sequencing). These considerations underscore the complexity of CRE epidemiology in the transplant setting and highlight the need for future studies using high-resolution genomic techniques. Among the nine patients with available enzyme typing data, seven (77.8%) demonstrated concordance between colonizing and infecting strains. Of these concordant cases, six involved metallo-β-lactamase (MBL) production and one involved an NDM-type carbapenemase. This is consistent with the conclusion of “genomic homology between colonizing and bloodstream infection strains” mentioned in the EHA conference report by Professor Feng Sizhou’s team, which confirmed through multilocus sequence typing that bloodstream infection strains originate from the pre-transplant colonization pool.23 Another retrospective analysis from a hematopoietic stem cell transplant center in South Africa similarly confirmed that patients with CRE colonization had a significantly increased risk of BSI, with approximately 30%–40% of CRE-colonized patients developing CRE-related BSI.24 Therefore, pre-transplant pathogen screening can significantly reduce infections and improve early prognosis in HSCT patients, serving as an important strategy for optimizing transplant infection management.25
The high rates of strain and enzyme concordance observed in this study support intestinal colonization as the predominant source of CRE bloodstream infections in allo-HSCT recipients. These findings underscore the value of routine pre-transplant CRE screening—preferably using enrichment broth methods to maximize sensitivity—as part of standard pre-conditioning assessment. Positive screening results could inform individualized prophylactic strategies, including targeted carbapenem-sparing regimens, oral colistin- or aminoglycoside-based selective gut decontamination, or early consideration of fecal microbiota transplantation in high-risk patients. Such risk-stratified approaches may help disrupt the progression from colonization to infection and ultimately reduce the substantial morbidity and mortality associated with CRE-BSI.
Delayed hematopoietic reconstitution is another key issue posed by CRE colonization. This study showed that the neutrophil and platelet engraftment times were significantly prolonged in the colonization-positive group, with reduced engraftment success rates. Multiple studies have further confirmed that pre-transplant intestinal CRE colonization is not only closely associated with lower engraftment success rates in patients but also significantly increases their non-relapse mortality; in the specific population of patients with malignant hematologic diseases, the mortality rate associated with such colonization can even exceed 50%.26–29 For the non-malignant hematologic disease patients included in this study, such as those with SAA, PNH, and congenital neutropenia, the degree of pre-transplant immune dysfunction differs from that in malignant tumor patients, yet they still exhibited a significant increase in post-colonization infection risk, suggesting that the risk effect of CRE colonization is consistent across different types of hematologic disease transplant populations.
The results of this study showed no significant difference in the incidence of acute and chronic GVHD between the two groups. Previous studies have confirmed that myeloablative conditioning regimens lead to a significant decline in intestinal microbiota diversity, and this reduction in intestinal microbiota diversity is closely associated with a significant increase in GVHD risk.30,31 The above results suggest that intestinal CRE colonization may not have a substantial impact on intestinal microbiota diversity. GVHD is a major risk factor affecting the prognosis of allo-HSCT patients. For patients with established GVHD, ≥ grade 2 acute GVHD is primarily treated with methylprednisolone (2 mg/kg/day) or equivalent doses of prednisone; for newly diagnosed chronic GVHD or steroid-refractory aGVHD, ruxolitinib is the preferred option.32 Microbial diversity exerts its effects by supporting the function of immunoregulatory T cells (such as MAIT and Vδ2 cells); therefore, maintaining or restoring intestinal microbial diversity—such as through probiotics or fecal microbiota transplantation—may become a new strategy for improving allo-HSCT prognosis, and MAIT and Vδ2 cells can serve as biomarkers for predicting post-transplant immune reconstitution and GVHD risk.33
The strengths of this study lie in addressing common baseline confounding issues by using IPTW to adjust for confounding factors (such as age, sex, pre-transplant KPS score, and conditioning intensity), confirming that CRE colonization positivity remains significantly associated with mortality risk after adjustment, thereby substantially enhancing the reliability of the causal association between colonization and adverse outcomes. Additionally, precise hypothesis testing was applied to each outcome indicator (eg, engraftment success rate, GVHD incidence, BSI rate), with P values refined to levels such as 0.001 and 0.044, ensuring the statistical analysis process adheres to the standards of clinical research in the allo-HSCT field and yielding high result credibility.
This study has the following limitations: First, the sample size is relatively limited, particularly with enzyme typing for CRE bloodstream infections covering only 9 patients, and uneven distribution of sample sizes across different disease types (eg, only 6 cases of severe congenital neutropenia), which may affect result stability; second, whole-genome sequencing analysis was not performed on CRE strains, precluding clarification of the evolutionary relationships between colonizing and infecting strains and the mechanisms of resistance gene transmission. Future research can expand the sample size, conduct stratified analyses, and integrate metagenomic sequencing techniques to further validate the conclusions of this study and optimize clinical management strategies.
Conclusion
In summary, pre-transplant intestinal CRE colonization is an independent risk factor for post-allo-HSCT CRE bloodstream infection, delayed hematopoietic reconstitution, and increased mortality risk, with intestinal colonizing strains serving as the primary source of infection. Pre-transplant CRE screening should be a routine examination during the pre-conditioning phase for allo-HSCT patients with various hematologic diseases, and early interventions for colonization-positive patients may improve their clinical prognosis.
Ethical Statement
This study has been approved by the Medical Ethics Committee of the First Affiliated Hospital of Xinxiang Medical University (EC-2018-694), and All procedures were conducted in accordance with the Declaration of Helsinki.
Consent to Publish
All authors have consented to the publication of the manuscript.
Author Contributions
Yuan Zhang, Rong Wang, and Guoqing Lyu should be regarded as joint first authors. All authors contributed significantly to the reported work through conception, study design, execution, data acquisition, analysis, and interpretation; participated in drafting, revising, or critically reviewing the article; approved the final version for publication; agreed on the submission journal; and accept accountability for all aspects of the work.
Disclosure Statements
The authors declare no conflicts of interest.
Funding
This work was supported by the 2025 Provincial Hospital Fiscal Funding Audit and Allocation Mechanism Project (Project Code: 210020113); the Henan Science and Technology Department Scientific Research Fund (Grant No. 182102311141), the Joint Construction Project LHGJ20220595, LHGJ20210508 funded by the Henan Provincial Health Committee and Henan Provincial Medical Science and Technology Program.
References
1. Xu L-P, Lu P-H, Wu D-P, et al. Hematopoietic stem cell transplantation activity in China 2019: a report from the Chinese blood and marrow transplantation registry group. Bone Marrow Transplant. 2021;56(12):2940–16. doi:10.1038/s41409-021-01431-6
2. Lv M, Huang X-J. Allogeneic hematopoietic stem cell transplantation in China: where we are and where to go. J Hematol Oncol. 2012;5(1):10. doi:10.1186/1756-8722-5-10
3. D’Souza A, Fretham C, Lee SJ, et al. Current use of and trends in hematopoietic cell transplantation in the United States. Biol Blood Marrow Transplant. 2020;26(8):e177–e182. doi:10.1016/j.bbmt.2020.04.013
4. Maertens JA, Girmenia C, Brüggemann RJ, et al. European guidelines for primary antifungal prophylaxis in adult haematology patients: summary of the updated recommendations from the European conference on infections in Leukaemia. J Antimicrob Chemotherapy. 2018. doi:10.1093/jac/dky286
5. Ljungman P, De La Camara R, Robin C, et al. Guidelines for the management of cytomegalovirus infection in patients with haematological malignancies and after stem cell transplantation from the 2017 European conference on infections in Leukaemia (ECIL 7). Lancet Infect Dis. 2019;19(8):e260–e272. doi:10.1016/S1473-3099(19)30107-0
6. Averbuch D, Dufour C, Mohty M, et al. The EBMT Handbook. Cham:Springer International Publishing; 2019:265–272. doi:10.1007/978-3-030-02278-5_36
7. Frieri M, Kumar K, Boutin A. Antibiotic resistance. J Infect Public Health. 2017;10(4):369–378. doi:10.1016/j.jiph.2016.08.007
8. Ma J, Song X, Li M, et al. Global spread of carbapenem-resistant Enterobacteriaceae: epidemiological features, resistance mechanisms, detection and therapy. Microbiolog Res. 2023;266:127249. doi:10.1016/j.micres.2022.127249
9. Cao W, Zhang J, Bian Z, et al. Active screening of intestinal colonization of carbapenem-resistant enterobacteriaceae for subsequent bloodstream infection in allogeneic hematopoietic stem cell transplantation. Infect Drug Resistance. 2022;15:5993–6006. doi:10.2147/IDR.S387615
10. Tansarli GS, Athanasiou S, Falagas ME. Evaluation of antimicrobial susceptibility of enterobacteriaceae causing urinary tract infections in Africa. Antimicrob Agents Chemotherapy. 2013;57(8):3628–3639. doi:10.1128/AAC.00359-13
11. Yang X, Wang D, Zhou Q, et al. Antimicrobial susceptibility testing of Enterobacteriaceae: determination of disk content and Kirby-Bauer breakpoint for ceftazidime/avibactam. BMC Microbiol. 2019;19(1):240. doi:10.1186/s12866-019-1613-5
12. Potter RF, D’Souza AW, Dantas G. The rapid spread of carbapenem-resistant Enterobacteriaceae. Drug Resistance Updates. 2016;29:30–46. doi:10.1016/j.drup.2016.09.002
13. Nicolau DP. Carbapenems: a potent class of antibiotics. Exp Opinion Pharmacotherapy. 2008;9(1):23–37. doi:10.1517/14656566.9.1.23
14. Zhang L, Zhai W, Lin Q, et al. Carbapenem-resistant Enterobacteriaceae in hematological patients: outcome of patients with Carbapenem-resistant Enterobacteriaceae infection and risk factors for progression to infection after rectal colonization. Int J Antimicrob Agents. 2019;54(4):527–529. doi:10.1016/j.ijantimicag.2019.06.023
15. Bilinski J, Robak K, Peric Z, et al. Impact of gut colonization by antibiotic-resistant bacteria on the outcomes of allogeneic hematopoietic stem cell transplantation: a retrospective, single-center study. Biol Blood Marrow Transplantat. 2016;22(6):1087–1093. doi:10.1016/j.bbmt.2016.02.009
16. Girmenia C, Rossolini GM, Piciocchi A, et al. Infections by carbapenem-resistant Klebsiella pneumoniae in SCT recipients: a nationwide retrospective survey from Italy. Bone Marrow Transplant. 2015;50(2):282–288. doi:10.1038/bmt.2014.231
17. Almangour TA, Ghonem L, Aljabri A, et al. Ceftazidime-avibactam versus colistin for the treatment of infections due to carbapenem-resistant enterobacterales: a multicenter cohort study. Infect Drug Resistance. 2022;15:211–221. doi:10.2147/IDR.S349004
18. Sader HS, Mendes RE, Duncan L, et al. Ceftazidime-avibactam, meropenem-vaborbactam, and imipenem-relebactam activities against multidrug-resistant Enterobacterales from United States medical centers (2018–2022). Diagnostic Microbiol Infect Dis. 2023;106(2):115945. doi:10.1016/j.diagmicrobio.2023.115945
19. Zheng G, Cai J, Zhang L, et al. Ceftazidime/avibactam-based versus polymyxin B-based therapeutic regimens for the treatment of carbapenem-resistant klebsiella pneumoniae infection in critically Ill patients: a retrospective cohort study. Infect Dis Therapy. 2022;11(5):1917–1934. doi:10.1007/s40121-022-00682-0
20. Tamma PD, Aitken SL, Bonomo RA, et al. Infectious diseases society of America 2023 guidance on the treatment of antimicrobial resistant gram-negative infections. Clin Infect Dis. 2024:ciae403.
21. Qu J, Xu J, Liu Y, et al. Real-world effectiveness of ceftazidime/avibactam versus polymyxin B in treating patients with carbapenem-resistant Gram-negative bacterial infections. Inte J Antimicrob Agents. 2023;62(2):106872. doi:10.1016/j.ijantimicag.2023.106872
22. Mackow NA, Van Duin D. Reviewing novel treatment options for carbapenem-resistant Enterobacterales. Exp Rev Anti-Infect Therapy. 2024;22(1–3):71–85. doi:10.1080/14787210.2024.2303028
23. Li J, Guo W, Wang J, et al. Strong homology between colonizing and bloodstream carbapenem-resistant acinetobacter Spp.: implications for empiric antibiotic therapy in hematological patients. Infect Drug Resistance. 2024;17:1827–1838. doi:10.2147/IDR.S458427
24. Van leeuwen LPM, Du Toit J, McMillan B, et al. Bloodstream infections and colonization in hematopoietic stem cell transplant recipients at a South African center: a retrospective analysis. Transplant Cellular Therapy. 2025;31(4):
25. Kamel N, Abdalla M, Al Ali A, et al. Effectiveness of pre-transplant screening for high-priority multidrug-resistant pathogens on pre-engraftment infections after hematopoietic stem cell transplantation. Infect Drug Resistance. 2024;17:2249–2260. doi:10.2147/IDR.S463868
26. Wu W-Q, Zhang Y-Q, Xu J, et al. Risk factors for carbapenem-resistant enterobacteriaceae colonization and the effect on clinical outcomes and prognosis in allogeneic hematopoietic stem cell transplanted patients. Infect Drug Resistance. 2023;16:6821–6831. doi:10.2147/IDR.S424048
27. Su F, Luo Y, Yu J, et al. Tandem fecal microbiota transplantation cycles in an allogeneic hematopoietic stem cell transplant recipient targeting carbapenem-resistant Enterobacteriaceae colonization: a case report and literature review[J/OL]. Euro J Med Res. 2021;26(1):37. doi:10.1186/s40001-021-00508-8
28. Trecarichi EM, Pagano L, Martino B, et al. Bloodstream infections caused by Klebsiella pneumoniae in onco-hematological patients: clinical impact of carbapenem resistance in a multicentre prospective survey. Ame J Hematol. 2016;91(11):1076–1081. doi:10.1002/ajh.24489
29. Pagano L, Caira M, Trecarichi EM, et al. Carbapenemase-producing Klebsiella pneumoniae and hematologic malignancies. Emerg Infect Dis. 2014;20(7):1235–1236. doi:10.3201/eid2007.130094
30. Van Lier YF, Vos J, Blom B, et al. Allogeneic hematopoietic cell transplantation, the microbiome, and graft-versus-host disease. Gut Microbes. 2023;15(1):2178805. doi:10.1080/19490976.2023.2178805
31. Shouval R, Waters NR, Gomes ALC, et al. Conditioning regimens are associated with distinct patterns of microbiota injury in allogeneic hematopoietic cell transplantation. Clin Cancer Res. 2023;29(1):165–173. doi:10.1158/1078-0432.CCR-22-1254
32. Penack O, Marchetti M, Aljurf M, et al. Prophylaxis and management of graft-versus-host disease after stem-cell transplantation for haematological malignancies: updated consensus recommendations of the European society for blood and marrow transplantation. Lancet Haematol. 2024;11(2):e147–e159. doi:10.1016/S2352-3026(23)00342-3
33. Andrlová H, Miltiadous O, Kousa AI, et al. MAIT and Vδ2 unconventional T cells are supported by a diverse intestinal microbiome and correlate with favorable patient outcome after allogeneic HCT. Sci Translat Med. 2022;14(646):eabj2829. doi:10.1126/scitranslmed.abj2829
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.