Back to Journals » International Medical Case Reports Journal » Volume 16
Heterotopic Pregnancy with Ipsilateral Adnexal Cyst Causing a Diagnostic Dilemma: A Case Report
Authors Teka H ![]() , Yemane A
, Yemane A ![]() , Gebremeskel M, Kinfe BA, Kiros S, Kidanu M
, Gebremeskel M, Kinfe BA, Kiros S, Kidanu M
Received 21 November 2022
Accepted for publication 24 December 2022
Published 9 January 2023 Volume 2023:16 Pages 27—34
DOI https://doi.org/10.2147/IMCRJ.S398563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ronald Prineas
Hale Teka,1 Awol Yemane,1 Mebrihit Gebremeskel,2 Birhanu A Kinfe,3 Sara Kiros,3 Mizan Kidanu4
1Department of Obstetrics and Gynecology, College of Health Sciences, Mekelle University, Mekelle, Tigray, Ethiopia; 2Department of Radiology, College of Health Sciences, Mekelle University, Mekelle, Tigray, Ethiopia; 3Department of Pathology, College of Health Sciences, Mekelle University, Mekelle, Tigray, Ethiopia; 4Department of Surgery, College of Health Sciences, Mekelle University, Mekelle, Tigray, Ethiopia
Correspondence: Hale Teka, Department of Obstetrics and Gynecology, College of Health Sciences, Mekelle University, P.O. Box: 1871, Mekelle, Tigray, Ethiopia, Email [email protected]
Background: Heterotopic pregnancy is the coexistence of intrauterine and extrauterine (ectopic) pregnancies. This is a relatively rare phenomenon with an incidence of 1 in 30,000 in spontaneously conceived pregnancies and 1 in 100 pregnancies achieved through assisted reproduction. Due to its relative rarity, diagnosis can be challenging. The presence of adnexal cystic masses complicating pregnancies can obscure the examination of the pelvis to rule in/out heterotopic pregnancy further adding to the complexity of the diagnosis.
Case Presentation: In this study, we present a 26-year-old primigravid, ethnic Tigrayan lady from the Tigray region of Ethiopia. She presented to our hospital with the complaint of progressively worsening abdominal pain of three days duration. She also had a subjective period of amenorrhea of 2 months duration. Pregnancy test was positive a few days prior to her current presentation. She reported that she had a history of treatment for pelvic inflammatory disease three months prior to her current conception. At presentation to our hospital, she was acutely ill-looking in pain, tachycardic, and hypotensive. Pelvic ultrasound showed an adnexal mass, hemoperitoneum, and an intrauterine pregnancy at 7 weeks + 5 days gestation. With the impression of ruptured ovarian cyst to rule out heterotopic pregnancy emergency, an explorative laparotomy was done which was pertinent for significant hemoperitoneum, ruptured left tubal ectopic pregnancy, and intact left ovarian cyst.
Conclusion: Physicians should consider a broad range of differential diagnosis in pregnant mothers who present with acute abdominal pain. Moreover, in the presence of an adnexal mass and hemoperitoneum, there is a need to maintain a low threshold for rare but life-threatening complications such as heterotopic pregnancy. The presence of an intrauterine gestation does not rule out extrauterine gestation. Thus, the presence of a viable intrauterine gestation should not stop physicians from carefully examining patients for the coexistence of an ectopic pregnancy.
Keywords: heterotopic pregnancy, ectopic pregnancy, adnexal cyst, diagnostic dilemma, case report
Introduction
Heterotopic pregnancy (HP) is the simultaneous occurrence of an intrauterine pregnancy (IUP) and extrauterine (ectopic) pregnancies.1 Heterotopic pregnancy is generally rare and its prevalence ranges from 1 in 30,000 in spontaneously achieved pregnancies to 1 in 100 pregnancies achieved through assisted reproduction.2 Heterotopic pregnancies share the same risk factor and clinical presentation to that of ectopic pregnancy alone. However, detection of the extrauterine component of a HP is not as straight forward as an ectopic pregnancy. The presence of an IUP is misleading because once a viable intrauterine pregnancy is observed during a scan, HP rarely comes to the physician’s attention.3 The growing uterus can also obscure the detection of the extrauterine component of HP. Moreover, the early symptoms of HP simulate the physiological changes of pregnancy, posing a delay in diagnosis.4 Thus, considerable time will be spent to confirm the diagnosis. Delays in diagnosis and failure to institute prompt intervention might lead to significant morbidity and potential mortality.5 Reporting the clinical profile, diagnostic challenge, and management of such a relatively rare phenomenon is of paramount importance. Thus, in this study, we aim to present a case of HP with a large adnexal cystic mass posing a diagnostic challenge.
Case Presentation
A 26-year-old primigravid lady presents to our hospital with the complaint of progressively worsening abdominal pain of 3 days duration. After arrival to our hospital, she fainted but maintained consciousness. She reported a recent urine pregnancy test positive result in another clinic but did not have a pelvic ultrasound. The pregnancy was wanted, planned, and supported. On physical examination, she was acutely sick looking in severe pain, hypotensive (60/40 mmHg), and tachycardic (120 beats/minute). She had tender abdomen with guarding and rigidity on palpation. Blood exams showed a hemoglobin of 12.5 g/dL. Transabdominal ultrasound scanning was pertinent for significant hemoperitoneum to the level of Morrison’s pouch, left adnexal cystic mass, and IUP with crown-to-rump length based gestational age of 7 weeks + 5 days (Figure 1). Visualization of the ectopic pregnancy was limited by the presence of the adnexal cyst. However, due to cultural sensitivity, our patient declined transvaginal sonography.
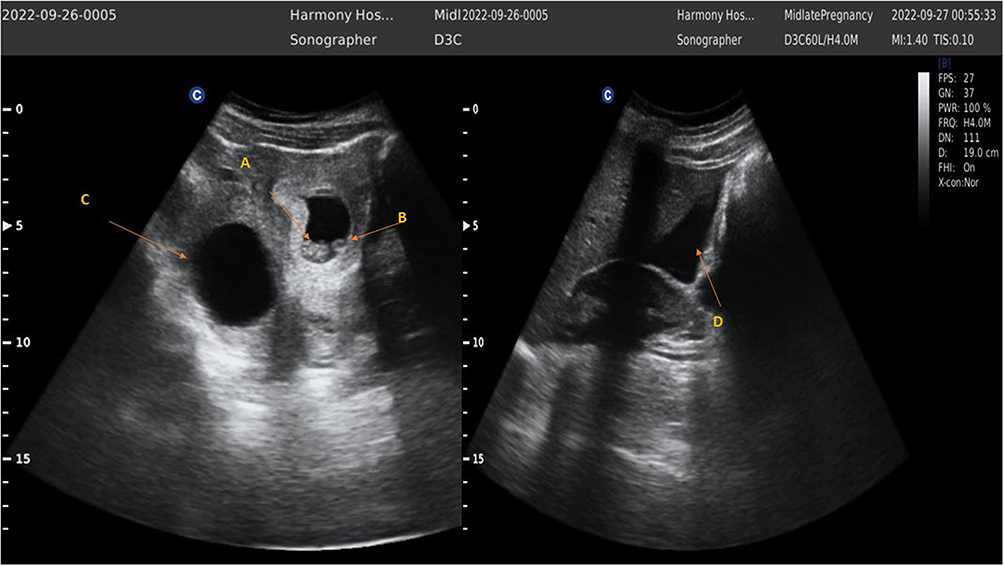 |
Figure 1 Visible intrauterine pregnancy with fetal pole (A), yolk sac (B), left adnexal cyst (C), and significant hemoperitoneum extending to the Morrison’s pouch (D). |
With the impression of a ruptured ovarian cyst to rule out HP, she was rushed to an emergency laparotomy. The intra-operative findings were pertinent for approximately 1000 mL of hemoperitoneum, ruptured left tubal ectopic pregnancy, and intact left ovarian cystic lesion. As the ovarian tissue was thinly spread over the cyst sparing the ipsilateral ovary was technically difficult. With this impression, a left total salpingio-oophorectomy was done. To preserve the IUP, care was taken to avoid excessive uterine manipulation.
The entire surgical specimen was subjected for histopathology (Figure 2). She had a smooth postoperative course and was discharged on post-operative day-1. Obstetric ultrasound scan on the 30th laparotomy day showed a viable IUP heralding the continuation of the pregnancy (Figure 3). The detailed description of the histopathology is presented below (Figures 4–6). On her postoperative period, she was put on 250 mg intramuscular 17α-hydroxyprogesterone weekly for 3 doses.
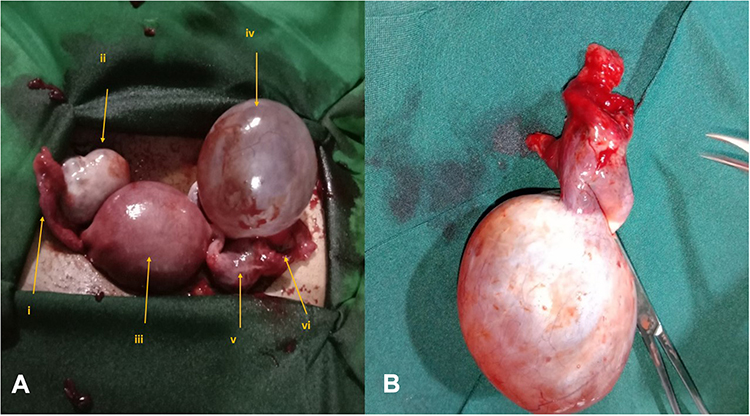 |
Figure 2 Intraoperative finding (A) showing normal right fallopian tube (i), normal right ovary (ii), gravid uterus (iii), left ovarian cyst (iv), left tubal ectopic pregnancy (v), and ruptured fimbrial end with active bleeding (vi), and surgical specimen (B). |
 |
Figure 3 Follow up scan a month later shows 11 weeks + 5 days intrauterine gestation (A) with positive fetal heart tone (B and C). |
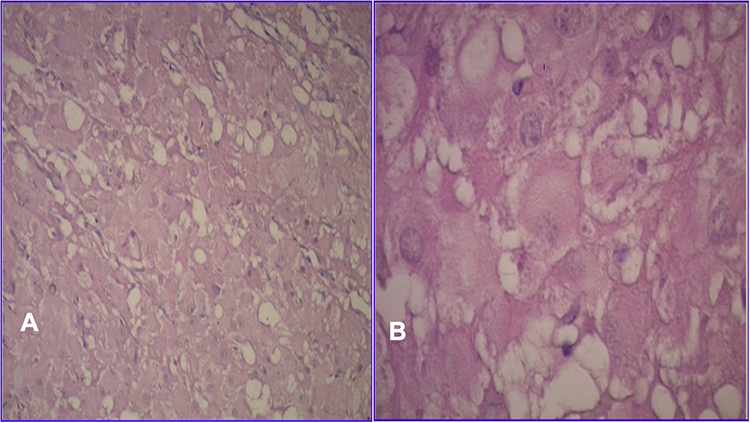 |
Figure 4 Granulosa lutein cells with abundant eosinophilic cytoplasm (A) and central vesicular nuclei (B). (H&E, AΧ10, BΧ40). |
 |
Figure 5 Prominent intramural edema involving the stroma of the plicae (A). Eosinophilic fibrin clot inside a thin-walled vein (B). (H&E, A and BΧ10). |
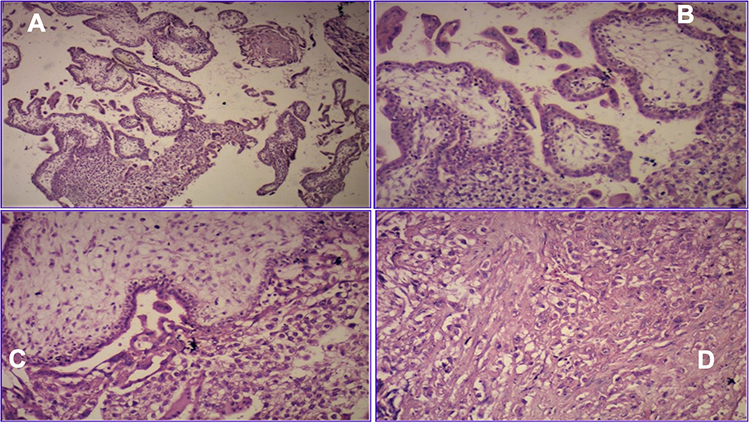 |
Figure 6 Mildly edematous chorionic villi of variable size and adjacent syncytiotrophoblastic giant cells as well as extravillous intermediate trophoblasts (A–C). Sheets of intermediate trophoblasts infiltrating the fallopian tube wall (D). (H&E, A, B, C and DΧ10). |
Gross Pathology
Macroscopically the received specimen consisted of a 7x6x6 cm cystic mass with 6 cm long opened up fimbriated fallopian tube. Cut surface through the cystic tissue showed an uninoculated cyst filled with serous fluid.
Histopathology
Sections from the cystic mass showed thick cyst wall made up of luteinized granulosa cells theca lutein cells with abundant eosinophilic cytoplasm and central vesicular nuclei.
Sections from the fallopian tube show edematous wall infiltrated by variable sized chorionic villi with hydropic changes, extra-villus intermediate trophoblasts, fibrin clots, congestion and hemorrhage.
With these macroscopic and histopathologic findings, the diagnosis was finalized as ectopic pregnancy plus theca lutein cyst.
Discussion
Heterotopic pregnancy is a relatively rare phenomenon with a commonly cited prevalence of 1 in 30,000 natural conceptions. However, it tends to be more prevalent in pregnancies achieved through assisted reproduction than in spontaneous conceptions.6 The prevalence of heterotopic pregnancy can reach as high as 5% following in vitro fertilization.7 The patient in this report conceived spontaneously.
The relative rarity and the presence of intrauterine gestations pose a diagnostic challenge. In all cases of acute abdomen in pregnancy abdominopelvic ultrasound remains the first logical diagnostic modality. Recent reports advocate that transvaginal ultrasound has superior diagnostic accuracy than a transabdominal approach.8,9 In equivocal cases, abdominopelvic MRI can be helpful. In times of diagnostic uncertainties, laparoscopy or explorative laparotomy can also be sought for both diagnosis and management purposes. The presence or absence of relevant risk factors can also guide us to where or what to look for. The most common risk factors associated with heterotopic pregnancy are tubal pathology and/or assisted reproduction.10–12 Fallopian tubes can become abnormal as a result of pelvic inflammatory disease (PID), previous tubal surgery, and previous ectopic pregnancy. Our patient conceived naturally but had a history of treatment for PID three months prior to her current conception. Knowing that a diagnosis of HP, based only on the presenting complaints, increases once suspicion based on the presence of relevant risk factors such as PID might be helpful.4 Nonetheless, it is equally important to note that many reports of heterotopic pregnancies had no apparent risk factors.7,13,14
Nearly all extrauterine components of heterotopic gestations are tubal. In our patient, consistent to most reports, the extrauterine component was located in the ampullary segment of the left fallopian tube. However, other sites such as implantation in the cervices, ovaries and abdominal cavities have been rarely reported.12,15–19
Similar to our patient’s presentation, most women carrying heterotopic gestations tend to be symptomatic in the first trimester, usually from 5–8 weeks of gestation.13 However, it can occasionally remain asymptomatic.2 Asymptomatic second and third trimester heterotopic pregnancies have also been reported.18,20,21 Unfortunately, by the time the patients become symptomatic, rupture of the ectopic pregnancy has occurred. Similar to our patient’s presentation, several studies reported that women with heterotopic pregnancies mainly present with abdominal pain.2,7 With significant intraperitoneal bleeding patients can also have chest pain, gastrointestinal disturbance such as vomiting, and syncope. In agreement with these reports, with an estimated blood loss of close to 1000 mL our patient had episodes of fainting. They can also have associated vaginal bleeding.7
In the present report, due to the disproportionate symptomatology and significant hemoperitoneum with an initial impression of a ruptured ovarian cyst, heterotopic pregnancy was considered in the list of differentials. Visualization of the ectopic pregnancy was obscured by the presence of a large adnexal cyst. However, due to the deteriorating patient condition and the significant hemoperitoneum surgical intervention was instituted. A laparoscopy is considered the gold standard surgical approach for heterotopic pregnancy.10 Because of set up limitations, an exploratory laparotomy was done in our case. It is also important to note that, as in our case, laparotomy retains its indications especially in forms with hemorrhagic shock.22 Preservation of the ovarian tissue, including in situations of extrauterine gestation implantation in the ovaries, has been reported.23 During either laparoscopy or laparotomy, if conditions allow, it is prudent that priority be given to preserve the future fertility of the women. In our case, since the ovarian pathology precluded salvage of the ovary, a salpingio-oophorectomy was performed and the pregnancy was supported with weekly intramuscular hydroxy progesterone. It is worth noting that medical management such as ultrasound-guided injection of potassium chloride into the corneal sac or fetal heart are possible options in hemodynamically stable patients with an unruptured extrauterine component of heterotopic gestation.9 However, this management is attended with higher abortion rates than surgical management.
Conclusion
Physicians should consider a broad differential diagnosis for mothers who present with acute abdominal pain, including a heightened index of suspicion to rare but life-threatening complications such as HP. The presence of a viable IUP should not stop physicians from carefully examining sites such as the adnexa for the presence of an ectopic pregnancy. More importantly, a routine early ultrasound of the adnexa during the first trimester is of paramount importance to obtain an accurate diagnosis and proper management. Moreover, prompt surgical intervention should be sought in women with an acute abdomen and hemoperitoneum even in the face of diagnostic uncertainty. To preserve the intrauterine pregnancy, manipulation of the uterus should be avoided; and provision of 17α-hydroxyprogesterone should be considered.
Abbreviations
HP, heterotopic pregnancy; IUP, intrauterine pregnancy; PID, pelvic inflammatory disease.
Data Sharing Statement
All datasets generated and/or analyzed during the current study are included in this article.
Ethics Approval and Consent to Participate
Not applicable. Our institution does not require an approval for publication of case reports.
Consent for Publication
Written informed consent for publication of her clinical details and/or clinical images was obtained from the patient. A copy of the consent form is available for review by the editor of this journal.
Acknowledgments
We sincerely thank the patient for accepting the publication of her story.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was solicited for this work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Maduako KT, Onoh V. Term delivery of a heterotopic pregnancy coexisting with ruptured tubal ectopic pregnancy: a case report duverney first described heterotopic pregnancy. Afr J Reprod Health. 2022;26:110–113.
2. Ali T, Tawab MA, Abdel M, Elhariri G, Ayad AA. Heterotopic pregnancy: a case report. Egypt J Radiol Nucl Med CAS. 2020;9:0–3.
3. Abdelmonem AH, Sayed G, Kohla S, Youssef R. Heterotopic pregnancy after a spontaneous conception a case report with a review of clinical, laboratory and imaging findings. Clin Case Rep. 2021;1–6:e04649.
4. Livani S, Fatemi A. Heterotopic pregnancy after in vitro fertilization ending with a successful term labor, a case report. Gene Cell TIssue. 2021;8(4):0–4. doi:10.5812/gct.114142
5. Nkurunziza C, Rurangwa T, Ngendahimana V. Case report second trimester heterotopic triplet pregnancy with intrauterine twin pregnancy and ruptured interstitial pregnancy: a maternal near-miss case report. Case Rep Obstet Gnecol. 2020;2020:6–8.
6. Aziz M, Arronte J. A case of spontaneous heterotopic pregnancy in natural conception complicated with hemoperitoneum. Heliyon. 2020;6(2):e03373. doi:10.1016/j.heliyon.2020.e03373
7. Aroke D, Ngek LT, Tindong M, et al. Blighted ovum and tubal pregnancy: a rare form of heterotopic pregnancy: case report. BMC Res. 2018:2–5. doi:10.1186/s13104-018-3345-2
8. Jurkovic D, Mavrelos D. Catch me if you scan: ultrasound diagnosis of ectopic pregnancy. Ultrasound Obstet Gynecol. 2007;30(1):1–7. doi:10.1002/uog.4077
9. Panelli DM, Phillips CH, Brady PC. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review. Fertil Res Pract. 2015;1(1):1–20. doi:10.1186/s40738-015-0008-z
10. Chadee A, Rezai S, Kirby C, et al. Case report spontaneous heterotopic pregnancy: dual case report and review of literature. Case Rep Obstet Gnecol. 2016;2016:1.
11. Bright DA, Gaupp FB. Heterotopic pregnancy: a reevaluation. J Am Board Fam Pract. 1990;3(2):125–128.
12. Tal J, Haddad S, Gordon N, Timor-Tritsch I, Timor-Tritsch I. Heterotopic pregnancy after ovulation induction and assisted reproductive technologies: a literature review from 1971 to 1993. Fertil Steril. 1996;66(1):1–12. doi:10.1016/S0015-0282(16)58378-2
13. Samborski A, Williams C, Spivack LE, Gubbels AL. Case report ruptured heterotopic pregnancy following spontaneous conception case report. J Clin Gynecol Obstet. 2020;9(3):9–12. doi:10.14740/jcgo673
14. Russman C, Gruner M, Jiang X, Schnatz PF. Gynecology & obstetrics spontaneous heterotopic pregnancy: a case report. Gynecol Obstet. 2015;5(9):10–12.
15. Kamath MS, Aleyamma TK, Muthukumar K, Sc M, Phil M. CASE REPORT A rare case report: ovarian heterotopic pregnancy after in vitro fertilization. Fertil Steril. 2010;94(5):1910.e9–1910.e11. doi:10.1016/j.fertnstert.2010.02.045
16. Viviano M, Emery SL, Del VF, Malinverno U, Abdulcadir J. Annals of case reports ovarian heterotopic pregnancy after ovulation induction: a case report. Ann Case Rep. 2022;7(02):1–7.
17. Oliveira FG, Abdelmassih V, Costa AL, Balmaceda JP, Abdelmassih S, Abdelmassih R. Rare association of ovarian implantation site for patients with heterotopic and with primary ectopic pregnancies after ICSI and blastocyst transfer. Hum Reprod. 2001;16(10):2227–2229. doi:10.1093/humrep/16.10.2227
18. Utalo T, Getu J. A unique case of coexisting intrauterine and abdominal pregnancy which progress to term with a positive birth outcome. BMC Pregnancy Childbirth. 2022;22(1):243. doi:10.1186/s12884-022-04561-x
19. Delrieu D, Antaki R, Phillips S, Kadoch I. Selective reduction of a triplet heterotopic cervical pregnancy after embryo transfer. Case Rep Clin Med. 2013;2(9):568–572. doi:10.4236/crcm.2013.29143
20. Kajdy A, Muzyka-placzy K, Filipecka-tyczka D, Modzelewski J, Sta M. A unique case of diagnosis of a heterotopic pregnancy at 26 weeks – case report and literature review. BMC Pregnancy Childbirth. 2021;21:1–6. doi:10.1186/s12884-020-03485-8
21. Ludwig M, Kaisi M, Bauer O, Diedrich K. The forgotten child — a case of heterotopic, intra- abdominal and intrauterine pregnancy carried to term. Hum Reprod. 1999;14(5):1372–1374. doi:10.1093/humrep/14.5.1372
22. Ouafidi B, Kiram H, Benaguida H, Lamrissi A, Fichtali K, Bouhya S. International journal of surgery case reports diagnosis and management of a spontaneous heterotopic pregnancy: rare case report. Int J Surg Case Rep. 2021;84:106184. doi:10.1016/j.ijscr.2021.106184
23. Maree G, Mohammad S, Moualla Z, Alshoumary L, Makhos R, Alfarra A. Case reports in women’ s health spontaneous ovarian and intrauterine non-viable heterotopic pregnancy at 12 weeks of gestation: a case report. Case Rep Womens Heal. 2022;35:e00423. doi:10.1016/j.crwh.2022.e00423
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.