Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Hepatocellular Carcinoma Precursor Lesions: From Pathological Basis to Risk Stratification and Precision Intervention
Authors Yan R, Zhang H, Jiao J, Huang Q, Wang N, Bao J, Li X ![]() , Yan S, Li J
, Yan S, Li J ![]()
Received 30 March 2026
Accepted for publication 6 June 2026
Published 18 June 2026 Volume 2026:13 613101
DOI https://doi.org/10.2147/JHC.S613101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Imam Waked
Ruijuan Yan,1,2,* Haibo Zhang,1,3,* Junzhe Jiao,1,2,* Qian Huang,1,3 Ning Wang,2 Jianfeng Bao,4 Xiaojiaoyang Li,5 Shuguang Yan,1 Jingtao Li2
1Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, People’s Republic of China; 2Liver Disease Center, Affiliated Hospital of Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, People’s Republic of China; 3College of Basic Medicine, Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, People’s Republic of China; 4Research and Teaching Department, The Hangzhou Xixi Hospital Affiliated to the Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 5Beijing University of Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this study
Correspondence: Jingtao Li; Shuguang Yan, Liver Disease Center, The Affiliated Hospital of Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, People’s Republic of China, Email [email protected]; [email protected]
Abstract: Hepatocellular carcinoma (HCC) predominantly arises against a background of chronic liver disease and cirrhosis, with its development typically following the three-step pattern of “hepatitis–cirrhosis–liver cancer.” Hepatocellular carcinoma precursor lesions represent a critical stage in this process and constitute a vital window for early diagnosis and targeted intervention. This review aims to systematically summarize the pathological basis, malignant potential, diagnostic approaches, risk stratification strategies, and precision intervention perspectives of HCC precursor lesions. Specifically, we review the pathological characteristics and malignant potential of HCC precursor lesions such as hepatocellular large/small cell transformation, dysplastic foci (DF), low/high-grade dysplastic nodules (LGDN/HGDN), and β-catenin-activated hepatocellular adenoma. We further summarize the application value and limitations of ultrasound/contrast-enhanced ultrasound (US), computed tomography (CT), and Gd-EOB-DTPA-enhanced magnetic resonance imaging (MRI) in screening and differential diagnosis. In addition, we discuss the progress in serum markers such as AFP, AFP-L3, DCP, and GP73, as well as liquid biopsy markers including CTC, ctDNA methylation, cfRNA, and tumor metabolites. We also outline the application of multivariable risk models like age-Male-ALBI-Platelet (aMAP), Gender-Age-AFP-L3-AFP-DCP (GALAD), and THRI in risk stratification and dynamic monitoring of high-risk populations. Finally, we review current treatment and follow-up strategies for HCC precursor lesions and explore the potential of radiomics, artificial intelligence, and multi-omics integration to improve risk assessment and diagnostic support, while also discussing their current limitations and the gap between research findings and routine clinical implementation. Overall, HCC precursor lesions represent an important target for early surveillance and precise intervention, and the integrated application of pathology, imaging, biomarkers, risk models, and emerging technologies may improve early identification, individualized management, and future translational research in HCC.
Keywords: dysplastic nodules, hepatocellular carcinoma, liquid biopsy, precursor lesions, risk prediction models
Introduction
Primary liver cancer remains a major global health burden, and hepatocellular carcinoma (HCC) accounts for more than 75% of cases.1 Although preventive measures such as hepatitis B vaccination have reduced some traditional risk factors, the increasing prevalence of metabolic risk factors, including obesity, diabetes, and metabolic dysfunction-associated steatotic liver disease (MASLD), continues to sustain the overall burden of HCC and has also contributed to changes in its etiological profile.1,2 Against this background, improving early detection and timely intervention has become a central challenge in HCC management.3 Hepatocarcinogenesis is typically a multistep process that develops in the setting of chronic liver disease and cirrhosis. Because early-stage HCC is often clinically silent, many patients are diagnosed only after the disease has progressed, which contributes to poor long-term outcomes.1 Importantly, hepatocarcinogenesis is usually preceded by a prolonged precursor stage in which regenerative and dysplastic nodules may undergo stepwise malignant transformation4 (Figure 1). Therefore, accurate recognition of HCC precursor lesions is of substantial clinical significance for early diagnosis, risk stratification, and precision intervention.5
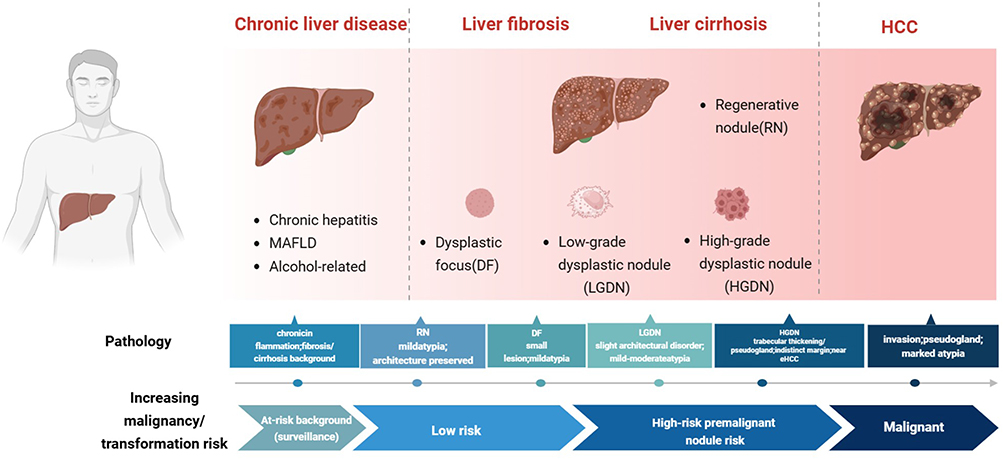 |
Figure 1 Multistep Hepatocarcinogenesis-Pathology and Clinical Risk Stratification. The sequential spectrum includes normal hepatocytes, LCC, SCC, DF, LGDN, and HGDN.The progression is characterized by increasing architectural disarray and cellular atypia (pathological features), and escalating clinical risk of malignancy. Created with BioRender.com. |
Definition and Pathological Classification
In this review, the term “HCC precursor lesions” is used as the overarching designation, whereas “preneoplastic lesions” is used specifically in sections addressing pathological classification and molecular evolution. Most of these lesions arise in the setting of chronic liver disease or cirrhosis,4,6,7 although certain entities, such as β-catenin-activated hepatocellular adenoma, may occur in non-cirrhotic liver. Pathologically, these lesions represent a spectrum of non-invasive hepatocellular proliferations with varying degrees of atypia and malignant potential. In these lesions, hepatocytes exhibit remodeling of the hepatic plate (trabecular) architecture, increasingly complex cellular arrangement, clonal expansion, and nodular proliferation, accompanied by a markedly elevated risk of malignant transformation, yet without meeting diagnostic criteria for invasive HCC.8 Morphologically, these lesions encompass a range from cytological abnormalities (such as large-cell change and small-cell change) to microscopic dysplastic foci (DF) and ultimately to grossly discernible dysplastic nodules (DN).9
The development of these lesions is generally considered a continuous multistep biological process. Under the continuous drive of inflammation and a fibrotic microenvironment, lesions typically follow the sequential evolution of DF-low-grade dysplastic nodules (LGDN)-high-grade dysplastic nodules (HGDN)-early hepatocellular carcinoma (eHCC)-typical advanced HCC (Figure 2). The discussion of the relevant content in this article is based on this continuous change.
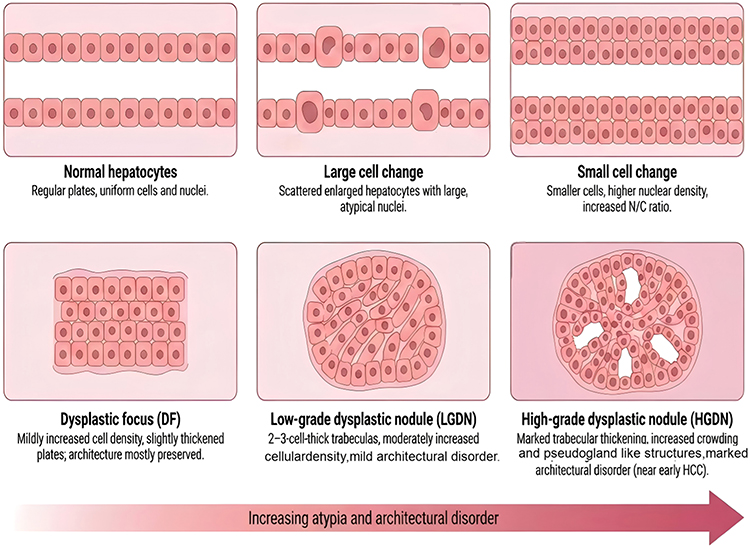 |
Figure 2 Pathological morphology of precursor lesions of HCC. Schematic illustration of the morphological spectrum from normal hepatocytes to LCC, SCC, DF, LGDN, and HGDN. The lesions show progressively increased cellular atypia, cell density, trabecular thickness, and architectural distortion. |
Hepatocellular Cytological Changes
Large-cell change (LCC) and small-cell change (SCC) are two important forms of hepatocellular morphological abnormalities in chronic liver disease, with distinct pathological features and different associations with HCC risk.
LCC is mainly characterized by an increase in both the volume of hepatocytes and their nuclei, nuclear pleomorphism, the presence of binucleated cells, prominent nucleoli, but a generally normal nuclear-cytoplasmic ratio. Its essence is usually considered a manifestation of polyploidy caused by chronic liver injury, resulting from hepatocyte senescence and degeneration. Traditionally, LCC (especially in cholestatic liver injury) has been regarded as a warning indicator of increased HCC risk, rather than a direct precursor lesion.9 However, recent studies suggest that it may also have precancerous significance in certain cases.10
SCC is characterized by a reduction in hepatocyte size, small and irregularly shaped nuclei, a significantly increased nuclear-cytoplasmic ratio, and an increased nuclear density per unit area. SCC has a higher proliferation activity, its cell morphology is similar to that of early well-differentiated HCC,11,12 the immunophenotype is close to that of liver stem cells, and there are similar chromosomal aberrations with adjacent HCC. Compared to LCC, SCC is often associated with a significant reduction in the expression of tumor suppressor genes such as p16 and p21, as well as cumulative DNA damage.13,14 Therefore, the current academic consensus generally holds that small cell dysplasia is a lesion with greater potential for progression compared to large cell dysplasia, and is more widely regarded as a bona fide preneoplastic lesion.
In summary, LCC and SCC represent two distinct forms of hepatocellular atypia, with SCC showing a closer biological and pathological relationship to hepatocarcinogenesis. However, the prognostic significance of these cytological alterations, especially LCC, remains incompletely understood, and further longitudinal and mechanistic studies are needed to clarify their roles in HCC risk prediction.
Dysplastic Foci
Dysplastic foci (DF) are microscopic hepatocellular lesions that arise in chronic liver disease, particularly in cirrhotic livers, and are generally not visible on gross examination.6 According to the terminology proposed by the International Working Party in 1995, DF consist of small clusters of hepatocytes showing cytological atypia, including LCC and SCC.15 Among these alterations, SCC is generally considered to be more closely associated with hepatocarcinogenesis, whereas the premalignant significance of LCC remains controversial.16 In routine pathological practice, DF are most often identified incidentally in biopsy, resection, or explant specimens rather than by imaging.16 They are regarded as early microscopic precursor lesions in the multistep process of hepatocarcinogenesis and may precede the development of DN and eHCC.6,16,17
In summary, DF are considered early microscopic precursor lesions in chronic liver disease and may represent an initial step in the multistage process of hepatocarcinogenesis. However, because they are usually detected only incidentally on pathological examination and cannot be reliably identified by current imaging methods, their clinical significance and value in routine surveillance remain insufficiently defined.
Dysplastic Nodules (DN)
Dysplastic nodules are macroscopically distinct nodular lesions that differ from the surrounding liver parenchyma in color, texture, size, and overall gross appearance.17 They are generally larger than 1 mm and usually measure up to approximately 2 cm in diameter.4 DN usually occurs within liver tissue with a background of cirrhosis. The terminology and diagnostic framework for DN were standardized by the International Working Party.17 Based on structural and cellular atypia, liver DN are classified into LGDN and HGDN,18 with HGDN being more closely associated with hepatocarcinogenesis.4,7 Histologically, both LGDN and HGDN represent hepatocellular proliferative lesions, whereas HGDN usually show increased cell density and greater atypia than the surrounding liver tissue.19
LGDN often have clear boundaries, which is due to the presence of dense fibrous scarring around them. Structural atypia is lacking, and mild cellular atypia can be observed, such as LCC, with a lack of nuclear division. Commonly, within the nodules, there may be a few small malformed arteries without bile ducts or paired veins.
HGDN often have indistinct boundaries and exhibit significant structural and/or cellular atypia. Atypical structural features include intranodular nodules (subnodules), pseudoglandular formation, and hepatocyte plate thickness exceeding three cell layers. Cellular atypia includes focal or widespread SCC, iron-resistant nodules, focal steatosis with Mallory-Denk bodies or intracellular hyaline bodies, and clear cell changes. HGDN has a high risk of carcinogenesis, with studies showing that the hazard ratios for malignant transformation of LGDN and HGDN are 2.96 and 16.8, respectively.20–22
In summary, DN, particularly HGDN, are key precursor lesions linking cirrhosis-associated nodules to eHCC and therefore play an important role in pathological evaluation and risk assessment. However, substantial overlap still exists between HGDN and eHCC in morphology and imaging findings, and current evidence regarding progression risk is still based on relatively limited longitudinal studies.
Recent studies have increasingly recognized hepatocellular adenoma (HCA),23 particularly the β-catenin-activated subtype, as a precursor lesion of HCC. HCA is a heterogeneous entity that comprises several molecular subtypes, including hepatocyte nuclear factor 1-alpha (HNF1A)-inactivated HCA, inflammatory HCA, β-catenin-activated HCA, sonic hedgehog HCA, and unclassified HCA. Among these, β-catenin-activated HCA is most clearly associated with an increased risk of malignant transformation to HCC, whereas the malignant potential of the other subtypes is generally lower, although inflammatory HCA may also carry increased risk in selected settings, particularly when β-catenin activation coexists.24,25 HCA is a rare benign hepatocellular neoplasm that usually arises in non-cirrhotic liver and occurs predominantly in women. Major risk factors include oral contraceptive use, anabolic steroids, and obesity.8 Unlike the DF-DN-HCC sequence that develops in the setting of cirrhosis, β-catenin-activated HCA typically occurs in non-cirrhotic livers but carries a higher risk of malignant transformation, thereby posing distinct clinical challenges.
Currently, LGDN, HGDN, and β-catenin-activated HCA are generally regarded as precursor lesions of hepatocellular carcinoma.8,18,26 However, from a clinical management perspective, cirrhosis-associated DN and β-catenin-activated HCA represent two distinct precursor settings and should not be interpreted within the same surveillance framework. DN usually arise in patients with chronic liver disease or cirrhosis who are already enrolled in HCC surveillance programs, and the major clinical challenge lies in how to stratify and monitor indeterminate nodules over time. In contrast, β-catenin-activated HCA typically develops in non-cirrhotic livers, where the key issue is not population-based surveillance, but lesion-directed decision-making regarding biopsy, resection, and follow-up according to molecular subtype, sex, lesion size, and interval growth.27 Therefore, although both entities belong to the spectrum of HCC precursor lesions, they imply different surveillance strategies and different thresholds for intervention.
Molecular Basis of Preneoplastic Lesions in HCC
Hepatocarcinogenesis is a multistep biological process that develops on a background of chronic liver injury, inflammation, and fibrosis. During the progression from regenerative nodules (RN) and DF to LGDN, HGDN, and eHCC, cumulative genomic, epigenomic, transcriptomic, and microenvironmental alterations provide the molecular basis for the accompanying morphological changes.28
Among the earliest key events are telomere shortening and activation of telomerase reverse transcriptase (TERT).29 Marked telomere dysfunction can already be observed in cirrhotic nodules, whereas TERT promoter mutations or hepatitis B virus (HBV) integration–related TERT overexpression become more frequent in HGDN and eHCC,30 thereby promoting progression toward neoplasia.
Aberrations in the Wnt/β-catenin pathway represent another major oncogenic axis.31,32 Activating mutations in catenin beta-1 (CTNNB1)33 are frequent in subsets of HCC and are closely related to tumor differentiation status, metabolic reprogramming, and immune evasion. Such alterations are relatively uncommon in DF/DN arising in cirrhosis and are often considered later events in hepatocarcinogenesis; in contrast, β-catenin–activated HCA exhibits these alterations as molecular drivers of malignant transformation,34 which may explain why this HCA subtype carries a substantially higher risk of malignant progression than other HCA variants.In addition, alterations in TP53 and chromatin remodeling genes (such as ARID1A, ARID2, etc.) are commonly observed in HGDN, eHCC, and advanced HCC and are associated with genomic instability, defective DNA damage repair, and epigenetic reprogramming.35 In chronic inflammatory states such as chronic hepatitis and metabolic dysfunction–associated steatotic liver disease, sustained activation of pathways including interleukin-6 (IL-6)/JAK–STAT3, NF-κB, and TGF-β,36 together with oxidative stress and lipotoxic injury, provides pro-carcinogenic signals facilitating these driver events. Recent studies further indicate that hepatic fibrosis and immune microenvironment remodeling are critical in precursor lesion progression: hepatic stellate cells may remain chronically activated and transition toward tumor-associated fibroblast-like phenotypes, promoting tumorigenesis through extensive matrix deposition and secretion of immunosuppressive and pro-angiogenic factors.37
In summary, HCC preneoplastic lesions are not driven by a single genetic alteration but rather arise from coordinated effects of multiple pathways—telomere–TERT, Wnt/β-catenin, TP53/chromatin remodeling, and the fibrosis–immune microenvironment axis—thereby providing a molecular rationale for early identification of high-risk lesions and preventive intervention strategies.8 The molecular evolution of HCC precursor lesions reflects the coordinated accumulation of genomic, epigenomic, and microenvironmental alterations. However, most currently available evidence remains descriptive, and the lack of standardized molecular markers with robust prospective validation limits the immediate clinical translation of these findings.
Overall, the pathological spectrum of HCC precursor lesions supports a continuous multistep model from cytological atypia to overt malignancy. Nevertheless, diagnostic boundaries between adjacent stages remain partly overlapping, and further integration of pathology with molecular and clinical risk features is still needed to improve classification and management.
Diagnosis and Risk Stratification
The diameter of HCC preneoplastic lesions is mostly less than 2 cm,23 making early diagnosis challenging. Reliable preoperative detection tools are limited in routine practice, and the real-world detection rate remains low. Currently, diagnosis of HCC precursor lesions relies primarily on a combination of imaging, pathology, and molecular biological techniques.
Imaging Diagnosis
Imaging is the preferred non-invasive method for screening and characterizing HCC precursor lesions, mainly including ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI).
In the evolution of RN, LGDN, HGDN, and HCC in cirrhosis, the nodules’ blood supply, fat content, cell density, iron, and the expression of organic anion transport peptides on the cell membrane surface undergo gradual changes. Imaging can comprehensively reflect the progression of these major pathological processes. Because most HCC precursor lesions are identified in patients with chronic liver disease or cirrhosis, the Liver Imaging Reporting and Data System (LI-RADS) provides an important standardized framework for interpreting liver observations in at-risk populations.38–40 Although LI-RADS was primarily developed for standardized surveillance/diagnostic assessment of HCC rather than the definitive histologic classification of precursor lesions, it is highly relevant to the evaluation of indeterminate nodules during hepatocarcinogenesis. In particular, major and ancillary imaging features, including threshold growth, hepatobiliary phase (HBP) hypointensity, mild-to-moderate T2 hyperintensity, and diffusion restriction, may help identify nodules at increased risk of malignant transformation.41,42 However, LI-RADS alone cannot reliably distinguish all precursor lesions from eHCC, and histopathology or imaging follow-up remains necessary in many cases.43
Ultrasound Imaging (US)
Ultrasound imaging is used as a screening tool due to its convenience, real-time capability, and lack of radiation. For surveillance of HCC in at-risk populations, US has been reported to show a sensitivity of approximately 78% and a specificity of 89%;44 however, its performance for detecting precursor lesions or very early malignant transformation is substantially more limited. Contrast-enhanced ultrasound (CEUS) can further aid in differentiating LGDN, HGDN, and HCC by evaluating enhancement pattern changes after contrast administration. CEUS offers the advantages of no nephrotoxicity and can be used in patients with contraindications to iodinated or gadolinium-based contrast agents, serving as a valuable complementary imaging modality for focal liver lesions in cirrhosis. However, the performance of US is strongly affected by operator experience, patient body habitus, liver echotexture, and lesion conspicuity, which limits its sensitivity for small precursor lesions and very eHCC. In addition, CEUS is usually limited to targeted evaluation of one lesion at a time and does not provide whole-liver staging information.45
Computed Tomography (CT)
Multiphasic contrast-enhanced CT remains an important imaging modality for the noninvasive evaluation of liver nodules in at-risk patients because it is widely available and is integrated into current diagnostic frameworks for HCC. Within LI-RADS-based assessment, CT can identify major imaging features such as non-rim arterial phase hyperenhancement, washout appearance, enhancing capsule, and threshold growth, thereby contributing to lesion categorization and clinical decision-making. However, its diagnostic performance for precursor lesions remains limited. Many LGDN and a substantial proportion of HGDN do not yet show the typical vascular profile of progressed HCC on multiphasic CT, resulting in substantial overlap with RN, indeterminate nodules, and eHCC. In addition, CT generally shows lower sensitivity than MRI for small or early hepatocellular lesions. The 2025 guideline cites prospective data for 10–20 mm nodules showing a sensitivity/specificity of 67.9%/76.8% for CT, compared with 70.6%/83.2% for MRI.39 Therefore, although CT is useful for lesion detection, characterization, and staging, its role in the evaluation of HCC precursor lesions should be interpreted cautiously, and indeterminate nodules often require MRI, interval follow-up, or histopathological correlation.40
Magnetic Resonance Imaging (MRI)
MRI, due to its lack of radiation, high soft tissue resolution, and multiparametric imaging capabilities, is generally regarded as the most sensitive imaging modality for the diagnosis and monitoring of HCC precursor lesions. MRI has higher sensitivity than CT for detecting early hepatocellular lesions and precursors of hepatocellular carcinoma.46 Various MRI sequences, such as pre-contrast T1-weighted and T2-weighted imaging, diffusion-weighted imaging (DWI), in-phase and out-of-phase imaging, and HBP imaging, enable radiologists to evaluate ancillary imaging features that may help differentiate benign, premalignant, and malignant lesions. However, MRI is associated with higher cost, longer acquisition time, and greater susceptibility to motion-related artifacts, and image quality may be reduced in patients with poor cooperation or severe ascites.45 On DWI, DN may appear isointense to mildly hyperintense because of increased cellular density and architectural atypia, whereas the corresponding apparent diffusion coefficient (ADC) maps usually show isointense to mildly hypointense signal. On Gd-EOB-DTPA-enhanced MRI, HBP hypointensity is an important finding in high-risk nodules because it usually reflects reduced uptake of hepatobiliary contrast, which is mainly related to decreased expression or dysfunction of organic anion transporting polypeptides rather than blood supply alone. When an HBP-hypointense nodule additionally shows non-rim arterial phase hyperenhancement, washout appearance on portal venous or transitional phases, mild-to-moderate T2 hyperintensity, or diffusion restriction, the possibility of HGDN, eHCC, or progressed HCC should be carefully considered.47,48 By contrast, HBP-hypointense nodules without arterial phase hyperenhancement may still represent high-risk lesions and therefore warrant close imaging follow-up, as a proportion of them can undergo hypervascular transformation over time.
Overall, different imaging techniques have varying roles in the HCC precursor lesions and early-stage HCC: US/CEUS is suitable as an initial screening and follow-up tool for high-risk populations such as those with cirrhosis,49 offering advantages such as convenience, real-time imaging, and no radiation. However, it highly depends on the operator’s experience for detecting small nodules. CT, especially dynamic contrast-enhanced CT, has higher spatial resolution and is less affected by respiration and ascites, making it useful for preliminary qualitative and staging assessments of lesions. However, it carries risks related to radiation and contrast agents, and its detection rate for LGDN and HGDN is limited. Gd-EOB-DTPA-enhanced MRI, combined with T1/T2-weighted imaging, DWI, and HBP imaging, has important advantages in detecting high-risk nodules smaller than 2 cm and in helping differentiate HGDN from eHCC.40,50 Nevertheless, the diagnostic performance of current imaging modalities is still constrained by the small size of precursor lesions, overlapping radiological features between HGDN and eHCC, and the lack of universally accepted imaging criteria for progression risk assessment.Future studies integrating radiomics and deep learning, standardizing quantitative MRI metrics based on liver-specific contrast agents such as Gd-EOB-DTPA, and establishing longitudinal imaging databases may further improve reproducibility, individualized risk stratification, and long-term monitoring of HCC precursor lesions.
Blood Biomarkers and Liquid Biopsy
Blood Biomarkers
Serum Alpha-fetoprotein (AFP) levels are associated with tumor burden, poorer differentiation, and microvascular invasion in HCC, and it is the most widely used serological marker for the diagnosis of HCC. Under normal circumstances, AFP concentrations in adult serum are extremely low (<10 ng/mL), but serum AFP levels may significantly increase when hepatocytes undergo malignant transformation. However, AFP levels can also be elevated in chronic hepatitis, cirrhosis, and other conditions, reducing its diagnostic specificity, with a detection rate of 63% for eHCC.38 For high-risk groups, based on semi-annual liver US examinations, the American Association for the Study of Liver Diseases (AASLD) and the Asian Pacific Association for the Study of the Liver (APASL) recommend routine use of AFP for screening, whereas European Association for the Study of the Liver (EASL) adopts a more cautious position regarding routine AFP use and does not support relying on AFP alone for surveillance.51 The differential expression of UDP-α(1,6)-fucosyltransferase in HCC cells attaches fucose residues to AFP, increasing its affinity for lectins, which can convert it into Alpha-fetoprotein Lens culinaris agglutinin-reactive fraction 3 (AFP-L3).52 AFP-L3 is specific to HCC cells and its levels increase correspondingly with the degree of carcinogenesis. When the AFP-L3 ratio is ≥10%, it can serve as a critical value for diagnosing HCC. Therefore, the combined use of serum AFP and its isoform AFP-L3 can improve the detection rate of HCC.53
Des-gamma carboxyprothrombin (DCP), a protein induced by vitamin K deficiency or antagonists, is elevated in the serum of HCC patients due to abnormal vitamin K metabolism caused by malignant transformation of liver cells, which affects the carboxylation of prothrombin precursors, resulting in the production of a large amount of DCP, a non-biologically active protein. AFP, AFP-L3, and DCP can predict the mutations in the TP53 gene profile of HCC, thus enabling early identification of HCC.54,55
Golgi transmembrane glycoprotein 73 (GP73): It is a type II Golgi transmembrane protein, primarily expressed by epithelial cells. Its expression level is low in normal liver cells but significantly increases in liver inflammation and tumor cells. GP73 can enhance the secretion of key pro-cancer signaling proteins, such as α-fetoprotein, immune checkpoint protein B7-H3, and vascular endothelial growth factor (VEGF), leading to cancer cell proliferation, metastasis, angiogenesis, oxidative stress, and other mechanisms involved in the development of HCC.56–58 The detection of GP73 is more sensitive and specific than that of AFP, and as the malignant potential of liver diseases such as hepatitis, cirrhosis, and hepatocellular carcinoma increases, the serum levels of GP73 also rise,57 indicating its potential clinical value.
In addition, some serum biomarkers with potential value have been studied for the early diagnosis of HCC, including α-L-fucosidase, osteopontin, and glypican-3 (GPC3). The expression or activity of these biomarkers changes during the occurrence and development of HCC, which may provide additional information for the diagnosis of precancerous lesions of the liver. However, most of these biomarkers are still in the research stage and have not yet been widely adopted in routine clinical applications.
Liquid Biopsy
Liquid biopsy is an emerging technology that enables early screening for liver cancer by analyzing tumor-derived biomarkers in bodily fluids such as blood, urine, and ascites. It offers significant advantages such as being minimally invasive, efficient, and capable of repeated dynamic monitoring. The combined detection of multiple biomarkers can further enhance the sensitivity of early diagnosis. Its main detection targets include circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), various forms of RNA (ctRNA, mRNA, miRNA, ncRNA), extracellular vesicles (exosomes, microvesicles, platelets, and apoptotic bodies), proteins (tumor-associated markers and autoantigens), and tumor metabolites.
CTCs are tumor cells that detach from the primary or metastatic tumor sites and enter the bloodstream. They are characterized by the expression of epithelial cell adhesion molecules (EpCAM), cytokeratin 8 (CK8), CK18, or CK19, and the absence of leukocyte common antigen (CD45). CTCs exhibit high heterogeneity, with the vast majority being eliminated during circulation, while a small portion evades immune surveillance and treatment, leading to distant metastasis or tumor recurrence. CTCs are intact tumor cells that retain all the genetic information and molecular characteristics of the tumor. The counting and characterization of CTCs can provide clinical information regarding prognosis, cancer staging, drug selection, and treatment efficacy.
Circulating tumor DNA (ctDNA) is tumor-derived free DNA that continuously releases DNA fragments into body fluids through processes such as apoptosis and necrosis.59 Cell-free DNA (cfDNA) refers to extracellular free DNA present in various body fluids. ctDNA is a portion of cfDNA released by tumor cells. ctDNA is continuously released from tumor cells, carrying genomic information, epigenetic information, and fragmentomic information from the tumor cells. It can be sampled multiple times and can monitor treatment responses and tissue conditions in real-time under various pathophysiological conditions. The multicenter prospective early warning screening project for liver cancer uses cfDNA whole genome sequencing and 5-hydroxymethylcytosine detection technology60 to construct a multi-omics, multidimensional (high-fidelity, HIFI) scoring system, which can achieve a sensitivity of 95.42% and a specificity of 97.91% in distinguishing liver cancer from non-liver cancer,61 outperforming AFP/DCP in screening and diagnosing eHCC. In addition, the methylation markers of ctDNA can be detected early, have good biological stability, and are one of the ideal tumor markers.62 The methylation of genes such as SEPT9, RASSF1A, and APC is significantly altered in liver cancer and can be used to improve the accuracy of liver cancer diagnosis.63
Circulating free RNA (cfRNA) includes circulating tumor RNA (ctRNA), mRNA, microRNA (miRNA), and non-coding RNA. Among them, circulating miRNA is an important regulatory factor in gene expression, functioning by translational repression or degradation of mRNA targets. Circulating miRNAs have higher concentrations in blood and other bodily fluids than mRNAs, are more stable in cancer patients, and are used as biomarkers for early detection and diagnosis of diseases, or as indicators of recurrence patterns, survival prediction, and follow-up metrics.64
Tumor metabolites are a class of small molecules produced, consumed, or significantly altered during abnormal metabolic processes in cancer cells or the tumor microenvironment. For example, 2-hydroxyglutarate is significantly elevated in gliomas and can promote tumorigenesis by altering histone methylation patterns;65 identified oncometabolites include glucose, lactate, serine, glutamine, and polyamines.66 Metabolite screening, as a rapid and effective method for early tumor detection, is being increasingly adopted by more and more studies.
Based on the existing evidence, the liquid biopsy strategies closest to clinical promotion currently include: on one hand, the combined application of traditional serological markers such as AFP, AFP-L3, and DCP; on the other hand, multi-gene methylation panels or multi-omics comprehensive scoring systems based on cfDNA/ctDNA, which have shown superior eHCC detection capabilities compared to single AFP/DCP in prospective cohort studies. In contrast, tumor metabolites, certain miRNAs/ncRNAs, and extracellular vesicles are still primarily in the exploratory stage and require larger-scale clinical studies to verify their stability and clinical feasibility. It is important to note that during the precancerous stage, the tumor clone burden is low, and the tumor components released into the peripheral blood are minimal, which is a core challenge faced by liquid biopsy. Additionally, background inflammation and fibrosis associated with metabolic-related fatty liver disease can also affect the specificity of certain biomarkers. In the future, incorporating host microenvironment signals such as the degree of liver fibrosis and changes in immune cell lineages into liquid biopsy and multi-omics analysis is expected to overcome the limitations of relying solely on tumor cell-derived signals, thereby enabling earlier and more accurate identification of precancerous lesions with a high risk of malignant transformation.
Despite the growing interest in liquid biopsy for HCC precursor lesions, its application at the precancerous stage remains challenging. Because these lesions are usually very small and clonal evolution is still unstable, lesion-derived signals released into the peripheral blood are often extremely scarce and may be obscured by background biological noise. In addition, in patients with metabolic and steatohepatitis-associated liver disease (MASLD), hepatic inflammation and fibrosis may further complicate biomarker interpretation. These challenges suggest that future studies should move beyond conventional tumor-derived analytes and further explore abnormal biological signals associated with the precancerous microenvironment, including dynamic immune alterations and fibrosis-related molecular changes, to improve early warning of malignant transformation.
In summary, serological markers and liquid biopsy approaches provide important complementary information for the detection and risk assessment of HCC precursor lesions. However, the sensitivity, specificity, and standardization of these biomarkers remain insufficient for independent clinical decision-making, and their future value will likely depend on integration with imaging, pathology, and longitudinal monitoring models.
Surveillance and Management: Cirrhosis-Associated DN versus β-Catenin-Activated HCA
In cirrhosis-associated DN, surveillance is primarily determined by the underlying high-risk liver background rather than by the nodule alone.38,39 Accordingly, when LGDN, HGDN, or an indeterminate nodule is detected, the practical challenge for hepatologists is how to appropriately intensify follow-up, including short-interval repeat cross-sectional imaging, the use of alternative contrast-enhanced modalities, and selective biopsy when imaging findings remain inconclusive. In this context, management is essentially surveillance-driven and aims to identify interval evolution toward HCC, such as arterial phase hyperenhancement, washout, enhancing capsule, or threshold growth.39
By contrast, β-catenin-activated HCA usually arises outside the conventional cirrhosis surveillance setting and is better approached as a lesion-directed management problem.38,67 The major challenge is not whether the patient belongs to a surveillance population, but whether the lesion itself warrants conservative follow-up or active intervention. This issue is particularly important because β-catenin-mutated HCAs carry a higher risk of malignant transformation, whereas MRI is not specific for subtyping β-catenin-mutated adenomas and imaging cannot reliably distinguish β-catenin-activated HCA from unclassified HCA or HCC.27 Therefore, clinical decision-making often requires integrated consideration of imaging findings, biopsy when indicated, patient sex, lesion size, clinical or molecular subtype, and interval growth pattern.
Combined Detection and Integrated Analysis of Multiple Biomarkers
The performance of single variables (such as clinical indicators, biochemical indicators, imaging, etc.) in the diagnosis of precancerous lesions and eHCC is often limited. Therefore, risk assessment models68 that combine multiple variables to predict disease occurrence are particularly important. For example, the aMAP score, a risk model for HCC in the Chinese population,69,70 includes variables such as age, sex, serum protein levels, bilirubin, and platelet count.71 However, it performs moderately in the cirrhosis subgroup, while the predictive efficacy of the aMAP-2 plus score, which includes the newly added parameters of AFP and circulating free DNA, is better. The HCC risk model GALAD score69 for chronic liver disease patients includes gender, age, AFP, AFP-L3, and DCP.72,73 The Toronto HCC risk index (THRI) includes four parameters: age, sex, etiology, and platelet levels.74 There are also some HCC risk models incorporating machine learning, artificial intelligence, and traditional Chinese medicine elements that are being further explored.75–77 These models are mostly used for medium- to long-term HCC risk assessment in high-risk populations with chronic liver disease or cirrhosis, providing quantitative basis for the stratified management of follow-up strategies. The gradual refinement of HCC risk assessment models provides a more reliable basis for the precise screening of precancerous liver lesions and early-stage liver cancer.
From a clinical pathway perspective, risk prediction models can complement existing screening strategies: during the initial screening phase, regular liver US combined with AFP remains the foundation; when scores such as aMAP, GALAD, and THRI indicate high risk, patients can enter an intensified monitoring phase, with shortened follow-up intervals and a preference for high-sensitivity imaging methods like Gd-EOB-DTPA-enhanced MRI; for patients with newly developed or progressive small nodules during follow-up, the decision to perform a biopsy is made based on the model’s risk stratification, imaging characteristics, and liquid biopsy results. Through routine screening, with risk stratification and intensified monitoring gradually deepening, the ultimate goal is to achieve a graded management model for precise diagnosis, which is expected to enable more accurate identification and intervention in precancerous lesions.
“Artificial Intelligence + Large Sample Clinical Data + Novel Biomarkers” Model
Given this multistep biological background,4,78 the major clinical challenge is to identify which precursor lesions are most likely to progress and therefore require closer surveillance or intervention. With the accumulation of large-scale follow-up cohorts and electronic medical record data, the “artificial intelligence (AI) + large clinical samples + novel biomarkers” model, centered around machine learning/deep learning, is gradually becoming an important direction for identifying high-risk populations and high-risk lesions for liver cancer. In populations with chronic hepatitis B and hepatitis B-related cirrhosis, multiple studies have integrated conventional clinical data such as age, liver function, virological indicators, and serum tumor markers from thousands of patients to develop risk-prediction algorithms using artificial neural networks and other machine-learning approaches, including ensemble methods. These models provide individualized predictions of HCC occurrence risk within 5–10 years, demonstrating significantly superior discriminative ability compared to traditional scoring systems like PAGE-B, thereby achieving fine stratification and optimization of screening strategies for pre-cancerous populations.79–81 In non-alcoholic fatty liver disease cohorts, deep learning models developed based on over 200,000 electronic health records can handle time-dependent covariates and highly imbalanced outcomes, offering early warnings for the very few individuals who will progress to HCC in the future.82 At the imaging level, radiomics- and deep learning-based approaches are being investigated as adjunctive tools for short-term HCC risk stratification in patients with cirrhosis. Recent multicenter studies using baseline three-phase CT, including models integrating liver-spleen image signatures with clinical scores such as aMAP, have shown improved predictive performance for short-term HCC development in research settings.83,84 However, these approaches are not yet part of routine clinical practice, as further prospective validation, standardization of imaging and analytic pipelines, and integration into clinical workflows are still needed. At the nodule level, AI-assisted digital pathology and radiomics remain investigational but have shown potential for improving the differentiation of hepatocellular nodular lesions in cirrhosis. A large whole-slide pathology study reported strong external-validation performance for multiclass classification of hepatocellular nodular lesions, particularly for challenging distinctions such as HGDN versus well-differentiated HCC.85 In parallel, an MRI-based radiomics study has shown potential for differentiating RN, DN, and HCC.86 Nevertheless, routine diagnosis of liver nodules in cirrhosis still relies on established contrast-enhanced imaging criteria and, when non-invasive criteria are not met, histopathological confirmation. These advances provide an important foundation for the development of AI-based molecular markers integrated with large-sample clinical data (Figure 3).
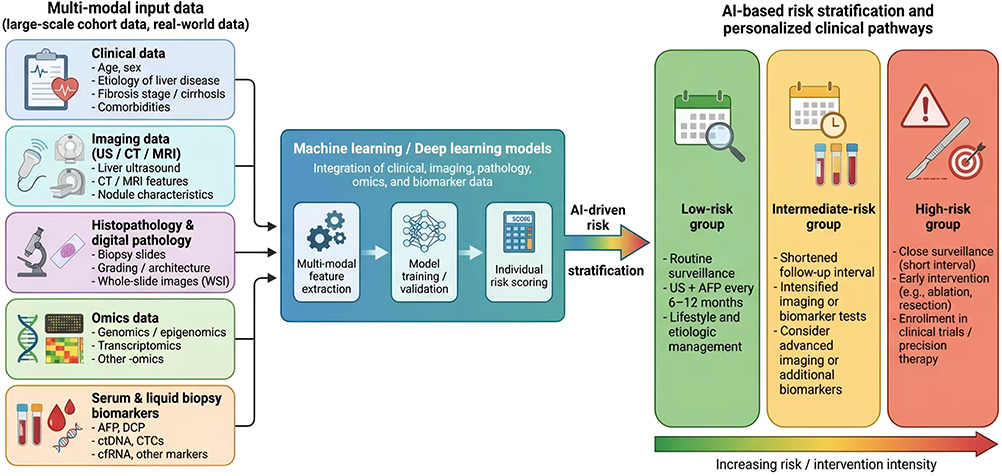 |
Figure 3 Al-driven multi-modal risk stratification and precision intervention in HCC. Multimodal inputs, including clinical variables, imaging, histopathology, omics profiling, and serum or liquid biopsy biomarkers, are integrated into machine learning or deep learning models for feature extraction, model training, and risk scoring. The output supports stratification into low-, intermediate-, and high-risk groups, with corresponding surveillance and intervention strategies. |
However, despite these advances, the clinical implementation of AI- and multi-omics-based risk prediction remains constrained by several important limitations. Many published models have been developed in retrospective, single-center, or geographically restricted cohorts and still lack rigorous prospective and external validation.87–89 Model transportability may be particularly challenging across populations with different etiological backgrounds, including HBV-, hepatitis C virus (HCV)-and alcohol-related liver disease, as well as across healthcare systems with different imaging quality, pathology workflows, access to sequencing platforms, and longitudinal follow-up capacity.39,90 Most existing risk prediction models have been derived predominantly from cohorts with hepatitis B virus- or hepatitis C virus-related cirrhosis, which may further limit their applicability in populations with different genetic backgrounds, lifestyles, and etiological compositions. In addition, some models rely on relatively complex predictive variables, which may reduce their feasibility in routine clinical practice. Moreover, variability in data acquisition, annotation standards, omics preprocessing, and data harmonization may further reduce reproducibility and broader clinical applicability.87,91 Future studies should therefore prioritize prospective multicenter and multinational validation, transparent subgroup-specific performance reporting, standardized data acquisition and annotation, and model calibration across diverse etiological and clinical settings.91,92
Treatment and Follow-Up
Although DF-DN-eHCC is generally considered to represent a continuous evolutionary process, current international guidelines have not yet reached a consensus on the optimal timing and specific strategies for intervention in such lesions. On the one hand, some studies advocate for intervention in the early stages of the disease in order to prevent its progression toward malignancy;93 on the other hand, others argue that premature or excessive intervention may increase potential iatrogenic risks and impose an unnecessary clinical burden.94
Management of HCC precursor lesions is not yet standardized; in patients with indeterminate or high-risk nodules in cirrhosis, current practice mainly varies in the use of short-interval imaging surveillance, selective biopsy, and the threshold for curative-intent intervention, while the supporting evidence remains limited because few prospective comparative studies have specifically focused on true precursor lesions such as HGDN.38 With advances in imaging technology, the multistep progression of DF, DN, and eHCC can now be distinguished through imaging. By integrating imaging, molecular biology, and histopathological examinations to enable timely intervention, curative treatments such as local ablation and surgical resection remain the most effective therapeutic approaches. However, it is essential to carefully balance the trade-offs between the extent and method of surgery and the resulting prognostic benefits to effectively improve long-term outcomes.
Currently, international organizations such as AASLD and EASL do not recommend routine treatment for precancerous liver lesions,38,39 However, for patients with DN who exhibit abnormal AFP-related serum markers or have concomitant cirrhosis, dynamic monitoring of imaging changes every 3–6 months is recommended. If the size of the nodules changes during follow-up, a biopsy for histopathological examination may be performed as necessary. During follow-up, nodules showing interval growth or evolving suspicious imaging features should undergo multidisciplinary reassessment, and biopsy may be considered when histological confirmation would alter management. In the absence of concerning interval change, continued imaging surveillance is recommended, with stable lesions returning to routine 6-month follow-up when appropriate.38,49
Nevertheless, the interpretation of dynamic monitoring remains inherently uncertain in clinical practice. Serial changes in lesion size, vascular profile, imaging visibility, and serum biomarkers are not always concordant, and some indeterminate nodules may remain stable for prolonged periods whereas others progress despite initially subtle findings. Therefore, decisions to continue surveillance, perform biopsy, or initiate treatment should be individualized within a multidisciplinary framework, with attention to underlying etiology, liver functional reserve, imaging quality, biomarker trends, and the feasibility of repeated surveillance.49,51,94 For patients with strong imaging and biomarker evidence of eHCC and adequate liver reserve, a multidisciplinary assessment should be conducted to individually select local ablation, surgical resection, or other curative treatments to halt disease progression (Figure 4).
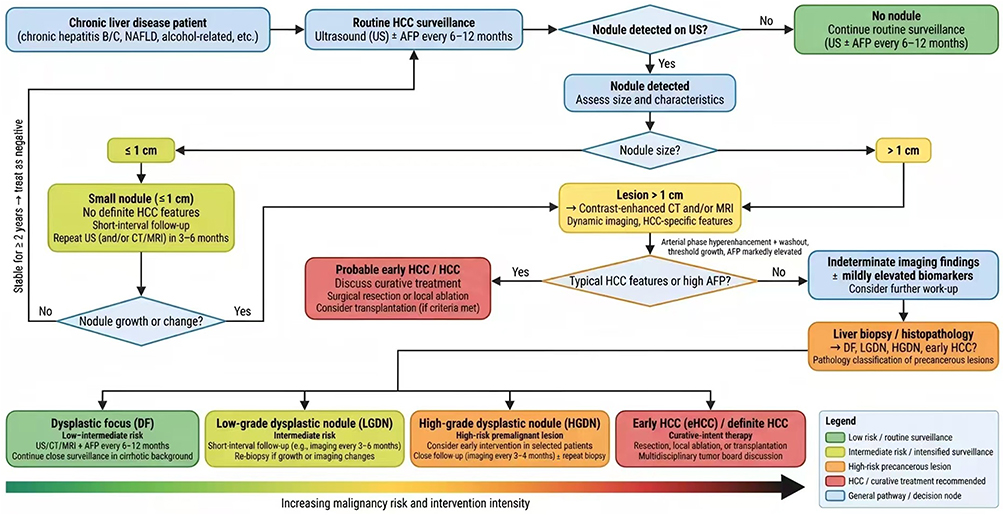 |
Figure 4 Clinical pathway for surveillance and management of nodules in chronic liver disease. The flowchart outlines the surveillance strategy for patients with chronic liver disease, beginning with routine screening and subsequent evaluation of detected nodules by lesion size, imaging, and serum biomarkers. |
Conclusion
As a critical intermediate stage in the occurrence and development of HCC, precancerous lesions of hepatocellular carcinoma serve as both a window period for early diagnosis and an important node for precise intervention. This review summarizes the pathological and molecular evolution of HCC precursor lesions, the current diagnostic approaches based on imaging and biomarkers, and the emerging role of risk prediction models in identifying lesions or populations at increased risk of malignant transformation.Existing evidence shows that precancerous lesions have clear molecular and morphological evolution patterns, progressing from cytological changes and DF to DN, and then to eHCC, forming a continuous and recognizable pathological process. However, due to multiple factors-including the complex pathological nature of nodules in the context of cirrhosis, the high degree of similarity in their imaging features, and the weak signal intensity of biomarkers derived from liquid biopsy—the clinical identification of such lesions remains significantly challenging. In current clinical practice, imaging assessment, multi-biomarker testing, and risk prediction models are gradually being integrated, driving a shift in diagnostic strategies from the traditional focus on “detecting lesions” toward “predicting progression.” Taken together, these advances provide readers with a more structured framework for understanding how HCC precursor lesions may be recognized, stratified, and monitored in different clinical settings, and why this stage is clinically important for earlier surveillance and more individualized intervention. Nevertheless, issues such as insufficient standardization, limited detection sensitivity, and a lack of consensus on clinical intervention strategies continue to constrain the effectiveness of early diagnosis and intervention for precancerous lesions to varying degrees. Therefore, future progress will depend on continuous breakthroughs in large-scale prospective cohort studies, advanced artificial intelligence algorithms, and novel biomarkers to establish more precise risk stratification and personalized monitoring systems.
In summary, research in the field of precancerous liver lesions is gradually transitioning from traditional descriptive diagnostic models to a new phase that emphasizes the elucidation of mechanisms, risk prediction, and precision management. By integrating pathology, imaging, biomarkers, and risk models into one framework, this review also highlights the practical knowledge currently available for improving early recognition and longitudinal assessment of high-risk lesions. With ongoing breakthroughs in radiomics, liquid biopsy, multimodal technology integration, and reversible intervention strategies, the feasibility of early screening, diagnosis, and intervention for precancerous lesions is increasingly improving. However, the near-term value of these approaches will depend not only on proof-of-concept performance, but also on their reproducibility, transportability, and applicability across heterogeneous patient populations and real-world care environments. Thus, the clinical relevance of this field lies not only in refining diagnostic classification, but also in supporting more timely follow-up and better-informed management decisions for patients at risk of HCC. In the future, further strengthening interdisciplinary collaboration and promoting the establishment of international consensus will lay a critical foundation for reducing the overall disease burden of hepatocellular carcinoma and improving long-term patient outcomes.
While many unresolved issues remain in the field of HCC precancerous lesions, this also points to the vast research potential in this area. In the future, if we can further strengthen the two-way translation between basic and clinical research, promote multidisciplinary collaboration, and foster international consensus, we may be better positioned to establish a more precise, accessible, and sustainable management system for precancerous lesions. This would effectively reduce the incidence and mortality rates of HCC and improve long-term patient outcomes.
Data Sharing Statement
This is a review article. No new data were generated or analyzed in this study. All information discussed in this article is derived from previously published studies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Science and Technology Major Project of the Ministry of Science and Technology of China (No. 2025ZD0551500, 2025ZD0551503, 2025ZD01906002); the National Natural Science Foundation of China (No. 82174330, 82405335); the National Traditional Chinese Medicine Advantage Specialty Construction Project (Department of Hepatology); the Shaanxi Provincial Department of Science and Technology (No. 2025JC-YBMS-887); the Shaanxi Provincial Administration of Traditional Chinese Medicine (No. SZY-KJCYC-2025-JC-019); the University-level High-level Key Discipline of Traditional Chinese Medicine of Shaanxi University of Chinese Medicine (No. 2024XKZD20); the Discipline Innovation Team of Shaanxi University of Chinese Medicine (No. 2019-YL05); and the Qinchuangyuan Traditional Chinese Medicine Industry Innovation Cluster Project (No. L2024-QCY-ZYYJJQ-Y01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–17. doi:10.3322/caac.21834
2. Liu Y, Liu L. Changes in the epidemiology of hepatocellular carcinoma in Asia. Cancers. 2022;14(18):4473. doi:10.3390/cancers14184473
3. Porukala M, Vinod PK. Gene expression signatures of stepwise progression of hepatocellular carcinoma. PLoS One. 2024;19(1):e0296454. doi:10.1371/journal.pone.0296454
4. Liao Z, Tang C, Luo R, Gu X, Zhou J, Gao J. Current concepts of precancerous lesions of hepatocellular carcinoma: recent progress in diagnosis. Diagnostics. 2023;13(7):1211. doi:10.3390/diagnostics13071211
5. Lee Y, Fujiwara N, Yang JD, Hoshida Y. Risk stratification and early detection biomarkers for precision HCC screening. Hepatology. 2023;78(1):319–362. doi:10.1002/hep.32779
6. Wen KW, Kakar S. Hepatic precancerous lesions and early hepatocellular carcinoma. Gastroenterol Clin North Am. 2024;53(1):109–132. doi:10.1016/j.gtc.2023.11.005
7. International Consensus Group for Hepatocellular Neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatology. 2009;49(2):658–664. doi:10.1002/hep.22709.
8. Desjonqueres E, Campani C, Marra F, Zucman-Rossi J, Nault JC. Preneoplastic lesions in the liver: molecular insights and relevance for clinical practice. Liver Int. 2022;42(3):492–506. doi:10.1111/liv.15152
9. Su Q, Benner A, Hofmann WJ, Otto G, Pichlmayr R, Bannasch P. Human hepatic preneoplasia: phenotypes and proliferation kinetics of foci and nodules of altered hepatocytes and their relationship to liver cell dysplasia. Virchows Arch. 1997;431(6):391–406. doi:10.1007/s004280050116
10. Lu LY, Chen CW, Fu AF, Liu SL, Gu KT. Quantitative study of ICM-DNA in normal hepatocytes, hepatocytes with large-cell change, hepatocellular carcinoma, and altered hepatocytes in paracarcinomatous tissue. Ganzang. 2000;1:7–9.
11. Wang XM, Wang BE, Wang TL, et al. Malignant transformation tendency of basophilic small-cell foci during experimental hepatocarcinogenesis [in Chinese]. Chin J Hepatol. 2006;7:495–498.
12. Ferrell LD, Crawford JM, Dhillon AP, Scheuer PJ, Nakanuma Y. Proposal for standardized criteria for the diagnosis of benign, borderline, and malignant hepatocellular lesions arising in chronic advanced liver disease. Am J Surg Pathol. 1993;17(11):1113–1123. doi:10.1097/00000478-199311000-00004
13. Libbrecht L, Desmet V, Roskams T. Preneoplastic lesions in human hepatocarcinogenesis. Liver Int. 2005;25(1):16–27. doi:10.1111/j.1478-3231.2005.01016.x
14. Bioulac-Sage P, Balabaud C. Liver nodules resembling focal nodular hyperplasia. J Hepatol. 2001;34(5):781–782. doi:10.1016/s0168-8278(01)00007-1
15. Wanless IR. Terminology of nodular hepatocellular lesions. Hepatology. 1995;22(3):983–993. doi:10.1002/hep.1840220341
16. Zhao YQ, Cong WM. Advances in the diagnostic pathological features of precancerous lesions of hepatocellular carcinoma. Zhonghua Gan Zang Bing Za Zhi. 2019;27(7):491–493. doi:10.3760/cma.j.issn.1007-3418.2019.07.004
17. International Working Party. Terminology of nodular hepatocellular lesions. Hepatology. 1995;22(3):983–993. doi:10.1016/0270-9139(95)90324-0.
18. Liver Cancer Study Group, Chinese Society of Hepatology, Chinese Medical Association, Editorial Board of Chinese Journal of Hepatology. Multidisciplinary expert consensus on diagnosis and treatment of precancerous lesions of hepatocellular carcinoma (2023 version) [in Chinese]. Zhonghua Gan Zang Bing Za Zhi. 2023;31(12):1250–1261. doi:10.3760/cma.j.cn501113-20231010-00136.
19. Field DT, Bellamy CO, Kendall TJ. Dysplastic lesions of the liver: two cases demonstrating the key pathological principles. Diagn Histopathol. 2025;31(6):401–404. doi:10.1016/j.mpdhp.2025.03.016
20. Cabibbo G, Antonucci M, Genco C. Update on new approaches in the management of hepatocellular carcinoma. Hepat Med. 2010;2:163–173. doi:10.2147/HMER.S7132
21. Di Tommaso L, Sangiovanni A, Borzio M, Park YN, Farinati F, Roncalli M. Advanced precancerous lesions in the liver. Best Pract Res Clin Gastroenterol. 2013;27(2):269–284. doi:10.1016/j.bpg.2013.03.015
22. Ojima H, Masugi Y, Tsujikawa H, et al. Early hepatocellular carcinoma with high-grade atypia in small vaguely nodular lesions. Cancer Sci. 2016;107(4):543–550. doi:10.1111/cas.12893
23. Choi JH, Thung SN. Pathology and diagnostic approaches to well-differentiated hepatocellular lesions: a narrative review. J Yeungnam Med Sci. 2024;42:5. doi:10.12701/jyms.2024.00766
24. Beaufrère A, Paradis V. Hepatocellular adenomas: review of pathological and molecular features. Hum Pathol. 2021;112:128–137. doi:10.1016/j.humpath.2020.11.016
25. Nault JC, Paradis V, Ronot M, Zucman-Rossi J. Benign liver tumours: understanding molecular physiology to adapt clinical management. Nat Rev Gastroenterol Hepatol. 2022;19(11):703–716. doi:10.1038/s41575-022-00643-5
26. Ryan BM, Faupel-Badger JM. The hallmarks of premalignant conditions: a molecular basis for cancer prevention. Semin Oncol. 2016;43(1):22–35. doi:10.1053/j.seminoncol.2015.09.007
27. European Association for the Study of the Liver. EASL clinical practice guidelines on the management of benign liver tumours. J Hepatol. 2016;65(2):386–398. doi:10.1016/j.jhep.2016.04.001.
28. Jee BA, Choi JH, Rhee H, et al. Dynamics of genomic, epigenomic, and transcriptomic aberrations during stepwise hepatocarcinogenesis. Cancer Res. 2019;79(21):5500–5512. doi:10.1158/0008-5472.CAN-19-0991
29. Nault JC, Calderaro J, Di Tommaso L, et al. Telomerase reverse transcriptase promoter mutation is an early somatic genetic alteration in the transformation of premalignant nodules in hepatocellular carcinoma on cirrhosis. Hepatology. 2014;60(6):1983–1992. doi:10.1002/hep.27372
30. Jang JW, Kim JS, Kim HS, et al. Significance of TERT genetic alterations and telomere length in hepatocellular carcinoma. Cancers. 2021;13(9):2160. doi:10.3390/cancers13092160
31. Bioulac-Sage P, Rebouissou S, Thomas C, et al. Hepatocellular adenoma subtype classification using molecular markers and immunohistochemistry. Hepatology. 2007;46(3):740–748. doi:10.1002/hep.21743
32. Verma S, Yadav M, Verma S, Srivastava AK, Mugale MN. EZH2-mediated hypermethylation of H3K27me3 downregulates claudin-4 and upregulates the wnt/β-catenin signaling pathway in hepatocellular carcinoma metastasis. Biochim Biophys Acta Mol Cell Res. 2026;1873(1):120076. doi:10.1016/j.bbamcr.2025.120076
33. Lin B, Li M. Role of the wnt/β-catenin signaling pathway in the development of HCC. Front Immunol. 2025;16:1691297. doi:10.3389/fimmu.2025.1691297
34. Nault JC, Zucman Rossi J. Molecular classification of hepatocellular adenomas. Int J Hepatol. 2013;2013:315947. doi:10.1155/2013/315947
35. Campani C, Zucman-Rossi J, Nault JC. Genetics of hepatocellular carcinoma: from tumor to circulating DNA. Cancers. 2023;15(3):817. doi:10.3390/cancers15030817
36. Yao N, Jiang W, Wang Y, et al. An immune-related signature for optimizing prognosis prediction and treatment decision of hepatocellular carcinoma. Eur J Med Res. 2023;28(1):123. doi:10.1186/s40001-023-01091-w
37. Lin A. Decoding the hepatic fibrosis-hepatocellular carcinoma axis: from mechanisms to therapeutic opportunities. Hepatol Int. 2025;19(4):732–759. doi:10.1007/s12072-025-10838-y
38. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
39. Sangro B, Argemi J, Ronot M, et al. EASL clinical practice guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82(2):315–374. doi:10.1016/j.jhep.2024.08.028
40. Kierans AS, Fowler KJ, Chernyak V. LI-RADS in 2024: recent updates, planned refinements, and future directions. Abdom Radiol. 2024;50(7):2868–2880. doi:10.1007/s00261-024-04730-w
41. Dawit H, Lam E, McInnes MDF, et al. LI-RADS CT and MRI ancillary feature association with hepatocellular carcinoma and malignancy: an individual participant data meta-analysis. Radiology. 2024;310(2):e231501. doi:10.1148/radiol.231501
42. Singal AG, Taouli B, Gopal P, Kanwal F, Parikh ND. Evaluation of LI-RADS 3 and 4 lesions. Gastroenterology. 2025;168(4):667–674.e1. doi:10.1053/j.gastro.2024.10.028
43. Kanneganti M, Singal AG. Diagnosis and management of indeterminate liver nodules in patients with cirrhosis. Clin Liver Dis. 2023;22(5):181–183. doi:10.1097/CLD.0000000000000069
44. Chou R, Cuevas C, Fu R, et al. Imaging techniques for the diagnosis of hepatocellular carcinoma: a systematic review and meta-analysis. Ann Intern Med. 2015;162(10):697–711. doi:10.7326/M14-2509
45. Liu X, Tan SBM, Awiwi MO, et al. Imaging findings in cirrhotic liver: pearls and pitfalls for diagnosis of focal benign and malignant lesions. RadioGraphics. 2023;43(9):e230043. doi:10.1148/rg.230043
46. Liang Y, Xu F, Guo Y, et al. Diagnostic performance of LI-RADS for MRI and CT detection of HCC: a systematic review and diagnostic meta-analysis. Eur J Radiol. 2021;134:109404. doi:10.1016/j.ejrad.2020.109404
47. Inchingolo R, Faletti R, Grazioli L, et al. MR with Gd-EOB-DTPA in assessment of liver nodules in cirrhotic patients. World J Hepatol. 2018;10(7):462–473. doi:10.4254/wjh.v10.i7.462
48. Huh J, Kim KW, Kim J, Yu E. Pathology-MRI correlation of hepatocarcinogenesis: recent update. J Pathol Transl Med. 2015;49(3):218–229. doi:10.4132/jptm.2015.04.15
49. Kamaya A, Fetzer DT, Seow JH, et al. LI-RADS US surveillance version 2024 for surveillance of hepatocellular carcinoma: an update to the American College of Radiology US LI-RADS. Radiology. 2024;313(3):e240169. doi:10.1148/radiol.240169
50. Ozaki K, Tanahashi Y, Goshima S. Gadoxetic acid-enhanced MRI in hepatocellular carcinoma: a comprehensive review of diagnostic, surveillance, and treatment response prediction and assessment. Jpn J Radiol. 2026;44(1):2–23. doi:10.1007/s11604-025-01870-x
51. Singal AG, Sanduzzi-Zamparelli M, Nahon P, et al. International Liver Cancer Association (ILCA) white paper on hepatocellular carcinoma risk stratification and surveillance. J Hepatol. 2023;79(1):226–239. doi:10.1016/j.jhep.2023.02.022
52. Norman JS, Li PJ, Kotwani P, Shui AM, Yao F, Mehta N. AFP-L3 and DCP strongly predict early hepatocellular carcinoma recurrence after liver transplantation. J Hepatol. 2023;79(6):1469–1477. doi:10.1016/j.jhep.2023.08.020
53. Liou WL, Tan SY, Yamada H, et al. Performance of the GALAD model in an Asian cohort undergoing hepatocellular carcinoma surveillance: a prospective cohort study. J Gastroenterol Hepatol. 2025;40(7):1818–1824. doi:10.1111/jgh.16997
54. Ahn KS, O’Brien DR, Kim YH, et al. Associations of serum tumor biomarkers with integrated genomic and clinical characteristics of hepatocellular carcinoma. Liver Cancer. 2021;10(6):593–605. doi:10.1159/000516957
55. Xie C, Lin BL, Deng H, Zhang XH, Zhao QY, Gao ZL. Multi-omics combined test performance effectiveness on opportunistic screening of high-risk liver cancer population [in Chinese]. Zhonghua Gan Zang Bing Za Zhi. 2024;32(2):140–147. doi:10.3760/cma.j.cn501113-20231125-00235
56. Liu Y, Zhou S, Shi J, et al. MYC transactivates GP73 and promotes metastasis of hepatocellular carcinoma cells through GP73-mediated MMP-7 trafficking in a mildly hypoxic microenvironment. Oncogenesis. 2019;8(10):58. doi:10.1038/s41389-019-0166-7
57. Liu Y, Wang J, Yang R, et al. GP73-mediated secretion of AFP and GP73 promotes proliferation and metastasis of hepatocellular carcinoma cells. Oncogenesis. 2021;10(10):69. doi:10.1038/s41389-021-00358-3
58. Bayliss RJ, Parker AL. GP73: the key to unlocking immunotherapy efficacy in solid tumors? J Immunother Cancer. 2025;13(5):e011989. doi:10.1136/jitc-2025-011989
59. Qi J, Hong B, Wang S, et al. Plasma cell-free DNA methylome-based liquid biopsy for accurate gastric cancer detection. Cancer Sci. 2024;115(10):3426–3438. doi:10.1111/cas.16284
60. Cai J, Chen L, Zhang Z, et al. Genome-wide mapping of 5-hydroxymethylcytosines in circulating cell-free DNA as a non-invasive approach for early detection of hepatocellular carcinoma. Gut. 2019;68(12):2195–2205. doi:10.1136/gutjnl-2019-318882
61. Wu T, Fan R, Bai J, et al. The development of a cSMART-based integrated model for hepatocellular carcinoma diagnosis. J Hematol Oncol. 2023;16(1):1. doi:10.1186/s13045-022-01396-z
62. Yang D, Yao Y, Gui F, Mei W, Zeng C. Decoding the epigenetic landscape: ctDNA methylation as a game-changer in hepatocellular carcinoma management. Biochim Biophys Acta Rev Cancer. 2025;1880(6):189497. doi:10.1016/j.bbcan.2025.189497
63. He GX, Huang LM, Tian HW. Research progress on clinical application of artificial intelligence-assisted liquid biopsy technology in early screening and diagnosis of liver cancer [in Chinese]. Zhongguo Yiyao Shengwu Jishu. 2025;20(Suppl 2):102–107. doi:10.3969/j.issn.1673-713X.2025.suppl2.017
64. Pinzani P, D’Argenio V, Del Re M, et al. Updates on liquid biopsy: current trends and future perspectives for clinical application in solid tumors. Clin Chem Lab Med. 2021;59(7):1181–1200. doi:10.1515/cclm-2020-1685
65. Ahmad O, Ahmad T, Pfister SM. IDH mutation, glioma immunogenicity, and therapeutic challenge of primary mismatch repair deficient IDH-mutant astrocytoma (PMMRDIA): a systematic review. Mol Oncol. 2024;18(12):2822–2841. doi:10.1002/1878-0261.13598
66. Shi D, Li T. Metabolic reprogramming in cancer: signaling pathways and therapeutic targets. Mol Cancer. 2026;25(1):e02582. doi:10.1186/s12943-026-02582-0
67. Frenette C, Mendiratta-Lala M, Salgia R, Wong RJ, Sauer BG, Pillai A. American College of Gastroenterology (ACG) clinical guideline: focal liver lesions. Am J Gastroenterol. 2024;119(7):1235–1271. doi:10.14309/ajg.0000000000002857
68. Mo HF, Chen YP, Han H, et al. Research methods and steps of clinical prediction models [in Chinese]. Chin J Evid Based Med. 2024;24(2):228–236. doi:10.7507/1672-2531.202308135
69. Villa E, Donghia R, Coletta S, et al. Insights into the GALAD score: a new optimal cut-off for hepatocellular carcinoma. World J Gastroenterol. 2025;31(40):111727. doi:10.3748/wjg.v31.i40.111727
70. Fujiwara N, Lopez C, Marsh TL, et al. Phase 3 validation of PAaM for hepatocellular carcinoma risk stratification in cirrhosis. Gastroenterology. 2025;168(3):556–567.e7. doi:10.1053/j.gastro.2024.10.035
71. Fan R, Papatheodoridis G, Sun J, et al. aMAP risk score predicts hepatocellular carcinoma development in patients with chronic hepatitis. J Hepatol. 2020;73(6):1368–1378. doi:10.1016/j.jhep.2020.07.025
72. Johnson PJ, Pirrie SJ, Cox TF, et al. The detection of hepatocellular carcinoma using a prospectively developed and validated model based on serological biomarkers. Cancer Epidemiol Biomarkers Prev. 2014;23(1):144–153. doi:10.1158/1055-9965.EPI-13-0870
73. Marsh TL, Parikh ND, Roberts LR, et al. A phase 3 biomarker validation of GALAD for the detection of hepatocellular carcinoma in cirrhosis. Gastroenterology. 2025;168(2):316–326.e6. doi:10.1053/j.gastro.2024.09.008
74. Sharma SA, Kowgier M, Hansen BE, et al. Toronto HCC risk index: a validated scoring system to predict 10-year risk of HCC in patients with cirrhosis. J Hepatol. 2018;68(1):92–99. doi:10.1016/j.jhep.2017.07.033
75. Christodoulou E, Ma J, Collins GS, Steyerberg EW, Verbakel JY, Van Calster B. A systematic review shows no performance benefit of machine learning over logistic regression for clinical prediction models. J Clin Epidemiol. 2019;110:12–22. doi:10.1016/j.jclinepi.2019.02.004
76. Lee HW, Kim H, Park T, et al. A machine learning model for predicting hepatocellular carcinoma risk in patients with chronic hepatitis B. Liver Int. 2023;43(8):1813–1821. doi:10.1111/liv.15597
77. Gao F, Cai P, Liu C, Xia F, Wang J. Research progress in imaging characteristics of precancerous nodules in hepatocellular carcinoma cells [in Chinese]. Zhonghua Gan Zang Bing Za Zhi. 2020;28(1):9–13. doi:10.3760/cma.j.issn.1007-3418.2020.01.004
78. Johnson PJ, Kalyuzhnyy A, Boswell E, Toyoda H. Progression of chronic liver disease to hepatocellular carcinoma: implications for surveillance and management. BJC Rep. 2024;2:39. doi:10.1038/s44276-024-00050-0
79. Hou Y, Yan J, Shi K, et al. Development and validation of a machine learning-based model used for predicting hepatocellular carcinoma risk in patients with hepatitis B-related cirrhosis: a retrospective study. Oncol Targets Ther. 2024;17:215–226. doi:10.2147/OTT.S444536
80. Wu T, Yan J, Xiong F, et al. Machine learning-based model used for predicting the risk of hepatocellular carcinoma in patients with chronic hepatitis B. J Hepatocell Carcinoma. 2025;12:659–670. doi:10.2147/JHC.S498463
81. Wu L, Liu Z, Huang H, et al. Development and validation of an interpretable machine learning model for predicting the risk of hepatocellular carcinoma in patients with chronic hepatitis B: a case-control study. BMC Gastroenterol. 2025;25(1):157. doi:10.1186/s12876-025-03697-2
82. Li Z, Lan L, Zhou Y, et al. Developing deep learning-based strategies to predict the risk of hepatocellular carcinoma among patients with nonalcoholic fatty liver disease from electronic health records. J Biomed Inform. 2024;152:104626. doi:10.1016/j.jbi.2024.104626
83. Fan R, Shi YR, Chen L, et al. Hepatocellular carcinoma risk stratification for cirrhosis patients: integrating radiomics and deep learning computed tomography signatures of the liver and spleen into a clinical model. J Clin Transl Hepatol. 2025;13(9):743–753. doi:10.14218/JCTH.2025.00091
84. Guo L, Hao X, Chen L, et al. Early warning of hepatocellular carcinoma in cirrhotic patients by three-phase CT-based deep learning radiomics model: a retrospective, multicentre, cohort study. eClinicalMedicine. 2024;74:102718. doi:10.1016/j.eclinm.2024.102718
85. Cheng N, Ren Y, Zhou J, et al. Deep learning-based classification of hepatocellular nodular lesions on whole-slide histopathologic images. Gastroenterology. 2022;162(7):1948–1961.e7. doi:10.1053/j.gastro.2022.02.025
86. Wen X, Pan W, Liu T, et al. MRI-based radiomics model for predicting the nature of nodules in cirrhotic liver. Asian J Surg. 2025;48(8):4757–4765. doi:10.1016/j.asjsur.2024.12.152
87. Clusmann J, Balaguer-Montero M, Bassegoda O, et al. The barriers to uptake of artificial intelligence in hepatology and how to overcome them. J Hepatol. 2025;83(6):1410–1426. doi:10.1016/j.jhep.2025.07.003
88. Collins GS, Moons KGM, Dhiman P, et al. TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ. 2024;385:e078378. doi:10.1136/bmj-2023-078378
89. Moons KGM, Damen JAA, Kaul T, et al. PROBAST+AI: an updated quality, risk of bias, and applicability assessment tool for prediction models using regression or artificial intelligence methods. BMJ. 2025;388:e082505. doi:10.1136/bmj-2024-082505
90. Chan SL, Sun HC, Xu Y, et al. The Lancet Commission on addressing the global hepatocellular carcinoma burden: comprehensive strategies from prevention to treatment. Lancet. 2025;406(10504):731–778. doi:10.1016/S0140-6736(25)01042-6
91. Lekadir K, Frangi AF, Porras AR, et al. FUTURE-AI: international consensus guideline for trustworthy and deployable artificial intelligence in healthcare. BMJ. 2025;388:e081554. doi:10.1136/bmj-2024-081554
92. Ghosh S, Zhao X, Alim M, Brudno M, Bhat M. Artificial intelligence applied to ‘omics data in liver disease: towards a personalised approach for diagnosis, prognosis and treatment. Gut. 2025;74(2):295–311. doi:10.1136/gutjnl-2023-331740
93. Brandi N, Renzulli M. Liver lesions at risk of transformation into hepatocellular carcinoma in cirrhotic patients: hepatobiliary phase hypointense nodules without arterial phase hyperenhancement. J Clin Transl Hepatol. 2024;12(1):100–112. doi:10.14218/JCTH.2023.00130
94. Koo E, Seif El Dahan K, Daher D, et al. Risk of hepatocellular carcinoma in subcentimeter liver nodules identified on surveillance ultrasound: a systematic review. Clin Gastroenterol Hepatol. 2024;23(8):1320–1327.e2. doi:10.1016/j.cgh.2024.08.051
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of Hepatocellular Carcinoma Risk Prediction Models in Patients with Hepatitis B-Related Cirrhosis
Cheng R, Xu X
Journal of Hepatocellular Carcinoma 2022, 9:987-997
Published Date: 12 September 2022
Prognostic Significance of Liquid Biopsy-Detected Genetic Alterations in Hepatocellular Carcinoma

Sarıtaş AG, Yavuz B, Aydın İ, Ağca H, Topal U, Ballı T, Bisgin A, Ülkü A, Akçam AT
Journal of Hepatocellular Carcinoma 2025, 12:2035-2043
Published Date: 5 September 2025