Back to Journals » Risk Management and Healthcare Policy » Volume 13
Hepatitis B Vaccination Uptake Rate and Predictors in Healthcare Professionals of Ethiopia
Authors Getnet MA ![]() , Bayu NH, Abtew MD, W/Mariam TGM
, Bayu NH, Abtew MD, W/Mariam TGM ![]()
Received 14 October 2020
Accepted for publication 17 November 2020
Published 8 December 2020 Volume 2020:13 Pages 2875—2885
DOI https://doi.org/10.2147/RMHP.S286488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Mehammed Adem Getnet,1 Netsanet Habtie Bayu,2 Mekdes Dessie Abtew,2 Tesfamichael G/Mariam W/Mariam3
1Department of Medical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Comprehensive Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Surgical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Mehammed Adem Getnet
University of Gondar, Gondar 196, Ethiopia
Tel +251 984245934
Email [email protected]
Introduction: Healthcare professionals continue to be at risk of acquiring occupation-related hepatitis B virus infection because of noncompliance for the 3-dose primary series of hepatitis B vaccine recommended. The objective of the study was to determine the rate of and to identify the predictors of hepatitis B vaccination uptake in healthcare professionals in Ethiopia.
Methods: A multicenter cross-sectional survey was conducted between May 19 2018 and June 15 2018. A stratified with systematic random sampling technique was used to select 260 healthcare professionals. A structured questionnaire was used to collect all the necessary primary data from samples. This survey analyzed hepatitis B vaccination uptake as the binary outcome variable (“noncomplete” vs “complete”) with regard to the 30 potential predictor variables. Both descriptive and inferential statistical analysis techniques have been used to address the study objective.
Results: The rate of complete vs noncomplete hepatitis B vaccination uptake was 37.7% vs 62.3%. The significantly independent predictors of hepatitis B vaccination uptake were professional qualification (P=0.004), professional experience (P=0.013), household income (P=0.006), workload status (P=0.015), routine infant immunization program existence at the workplace (P=0.014), perceived susceptibility to infection (P=0.005), perceived safety of vaccine (P=0.001), prior occupational exposure to blood (P=0.006), training on universal precautions (P=0.015), and colleagues’ suggestion (P=0.002).
Conclusion: The rate of hepatitis B vaccination uptake found was currently low. The significantly independent predictors of hepatitis B vaccination uptake included perceived safety, colleagues’ suggestion, professional qualification, perceived susceptibility, household income, prior occupational exposure to blood, professional experience, existence of routine infant immunization program at the workplace facility, workload status, and universal precautions training.
Keywords: hepatitis B, virus, occupational risk, vaccine, healthcare professionals
Introduction
Hepatitis B (HB) is a dynamic multimodal highly contagious and pathogenic infection caused by HB virus that mainly affects the human liver. It remains a disease of major global public health burden causing substantial morbidity and mortality, with the highest prevalence in Asia and Africa.1 One of the most important risk factors in acquiring HB infection is being a healthcare professional (HCP). The HCPs are recognized as significantly 2 to 10 times more likely to acquire HB virus infection than the general adult population.2 This risk appears to be related to repetitive percutaneous and permucosal occupational exposures (OEs) to the patients’ blood in the occupation. The costs of occupational injuries and diseases are serious and real,3 often much greater than immediately understood.4 The HB virus is also one of the most serious blood-borne pathogens which are the major risks that HCPs encounter in the occupation both at the hospital and nonhospital setting worldwide.5
Fortunately, a vaccine is available as the best prevention strategy against HB virus transmission and the subsequent multifaceted negative repercussions. The HB vaccine has been proven to provide long-lasting effective protection after the completion of all 3-dose primary series amongst persons vaccinated with the recommended schedule.6 The HB immunization program is initially publicized for infants and later for children and adolescents. Nowadays, vaccination of all high-risk adults against HB virus infection is also found to be very crucial. It is expected that vaccinating healthcare providers as adults against HB virus is not only important to maintain their occupational safety and health, but also a key component of chronic HB virus infection prevention and eventual eradication. However, it is not widely implemented and not sufficiently utilized even among HCPs. The HB vaccination coverage rate with the ≥3 doses completion among HCPs differs roughly from 12.0%7 to 72.0%8 in Africa, from 38.8%9 to 85.2%10 in Asia, and from 40.0%11 to 95.0%12 in the leftover continents. The HCPs continue to be at serious risk of acquiring occupational HB infection due to vaccination noncompliance;13 only those with ≥3 doses of HB vaccine uptake are considered protected.
There are several studies indicating that the HB vaccination uptake rate and its factors associated vary between different HCP populations and settings. The rate of HB vaccination uptake could be influenced by many factors/predictors within demographic, psychosocial, behavioral, and other domains. There are very limited data from Ethiopia on this aspect.14 Therefore, the aim of the present study was to assess the HB vaccination uptake rate and predictors in HCPs in Ethiopia.
Methods
Design and Period
A questionnaire-based quantitative cross-sectional survey was conducted to assess the HB vaccination uptake rate and predictors in HCPs of Ethiopia, from May 19 2018 to June 15 2018.
Settings and Participants
This study specifically took place in Gondar, Ethiopia. Gondar, or Gonder, former capital of Ethiopia, is now the capital city of the Central Gondar Zone of the Amhara National Regional State of Ethiopia. The survey was addressing multiple health institutions from the described study area. There are 44 (eight public primary health centers, three private primary clinics, nine private medium clinics, 23 private specialist clinics, and one private primary hospital) healthcare facilities functional in Gondar city serving the general community under the zone’s health administration. All these 44 health facilities with their employees were therefore used as the study setting.
This study targeted multiple groups of HCPs in professions including physicians, dentists, nurses, midwives, laboratory technicians/technologists, physiotherapists, anesthetists, pharmacists/pharmacy technicians, and health officer clinicians. It intended to indicate those HCPs who had routine patient-care activities. Aside this, the HB vaccination program for HCPs in Ethiopia was initiated around 2004 upon the FMOH-Ethiopia infection prevention guidelines endorsement like the WHO or the CDC recommendation: all HCPs should be fully vaccinated before engaging occupational risk as well. Since there is no mandatory HB vaccination policy or mass campaign headed to HCPs documented in Ethiopia, the way of receiving HB vaccine by them appears to be through self-paid voluntary vaccination policy.
The required total sample size was determined as follows. Step I. Conveying the estimator values (z=1.96, p=0.5, e=0.05, N=597 HCPs). Step II. Computing with the standard formula (n=[z2×p×(1–p)/e2]/[1+(z2×p×(1–p)/e2×N)]). Step III. Adjusting for possible nonresponse extent (about 10%), it finally becomes certain (n=260 HCPs).
Here, n is the sample size, z is the z-score related with a 95% level of confidence, p is the hypothesized proportion of HB vaccine uptake, e is the margin of error, and N is the population size.
The total sample size calculated above was also proportionally redistributed into the five strata (nj=[Nj/N]×n) and then a systematic random sampling technique (k=N/n) was applied to select each sample of each stratum (the strata is “type of health facility as a current workplace for the HCP”):
- HCPs employed in the public primary health centers (Nj=331, k≈2, nj=144)
- HCPs employed in the private primary clinics (Nj=33, k≈2, nj=14)]
- HCPs employed in the private medium clinics (Nj=96, k≈2, nj=42)
- HCPs employed in the private specialist clinics (Nj=117, k≈2, nj=51)
- HCPs employed in a private primary hospital (Nj=20, k≈2, nj=9)
Here, nj is the sample size in the stratum, Nj is the population size in the stratum, and k is the sampling interval.
We accomplished regular contacts throughout the study period in order to invite all sampled HCPs for participation after written informed consent, and to avoid re-participation.
Variables
We interviewed the participants in order to comply with the structured survey questionnaire. The questionnaire covered all the necessary data regarding the study variables.
HB vaccination uptake was used as the dependent (outcome) variable. Demographic characteristics including sex, age, marital status, number of persons in the household, income of the respondent, income of the household, professional qualification, professional role type, professional experience, sector of workplace, department of workplace, workload status, and routine infant immunization program (RIIP) presence in the workplace were used as potential independent (predictor) variables. Psychosocial characteristics including perceived susceptibility to infection, perceived severity of infection, perceived efficacy of the vaccine, perceived safety of the vaccine, perceived affordability of the vaccine, perceived accessibility of the vaccine, perceived efficacy of personal protective equipment (PPE), and perceived efficacy of post-exposure prophylaxis (PEP) were also used as potential predictor variables. Behavioral characteristics including ever tested for human immunodeficiency virus (HIV), alcohol use, tobacco use, prior OE to blood, and adherence in practicing universal precautions (UP) were also used as potential predictor variables. Miscellaneous characteristics including history of jaundice, taken training on UP, know HB infected persons, and ever gets colleagues’ suggestion were additionally used as potential predictor variables. For the definition of these variables, see Supplementary Table S1.
Statistical Analysis
The data were processed and analyzed via IBM SPSS version 25.0.0. Frequency analysis (percentage and a 95% confidence interval [CI] for percentage) was used to determine the rate of HB vaccination uptake as the outcome variable. Bivariate (crude) analysis was done using the Pearson chi-square test to explore every single potential predictor variable by the outcome variable. The potential predictors that have shown P≤0.25 in this bivariate crosstab analysis were accordingly chosen for further analysis, although only those with P<0.05 were considered significant. Multivariate (adjusted) analysis was done using the binary logistic regression model to identify the independent predictors of the outcome. All those selected potential predictors from the bivariate crosstab analysis were entered into the multivariable binary logistic regression model simultaneously. After series of logistic regression models through backward stepwise elimination approach, predictors that have shown P<0.05 were declared as independently significantly associated with the outcome. For this purpose, we computed adjusted odds ratios (AORs) and their CIs as a measure of the strength of association. The Hosmer–Lemeshow goodness of fit test was used to comment on model fitness.
Results
A total of 260 eligible participants were sampled, invited, interviewed, and ultimately analyzed in the study with 100% responses.
The frequency analysis determined that the overall complete vs noncomplete HB vaccination uptake rate was 37.7% vs 62.3% among 260 participants (Table 1).
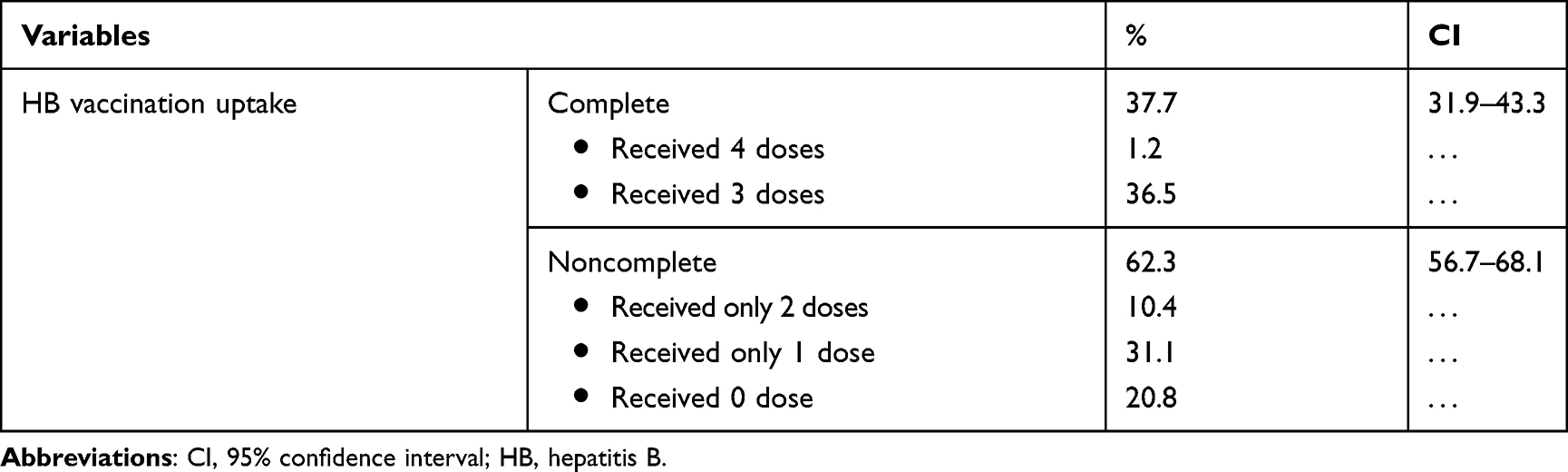 |
Table 1 Hepatitis B Vaccination Uptake Rate Among Participants (n=260) |
Tables 2–5 show the demographic, psychosocial, behavioral, and miscellaneous characteristics of participants according to HB vaccination uptake. The rate of HB vaccination uptake was significantly different for the following demographic factors at P<0.05 in the bivariate analysis: number of persons in the household, income of the respondent, and income of the household (Table 2). The rate of HB vaccination uptake was significantly different for the following psychosocial factors at P<0.05 in the bivariate analysis: perceived susceptibility to infection, perceived severity of infection, perceived efficacy of the vaccine, perceived safety of the vaccine, perceived affordability of the vaccine, perceived accessibility of the vaccine, and perceived efficacy of PPE (Table 3). The rate of HB vaccination uptake was not significantly different for any behavioral factors at P<0.05 in the bivariate analysis (Table 4). The rate of HB vaccination uptake was significantly different for the following two miscellaneous factors at P<0.05 in the bivariate analysis: taken training on UP and ever gets colleagues’ suggestion (Table 5).
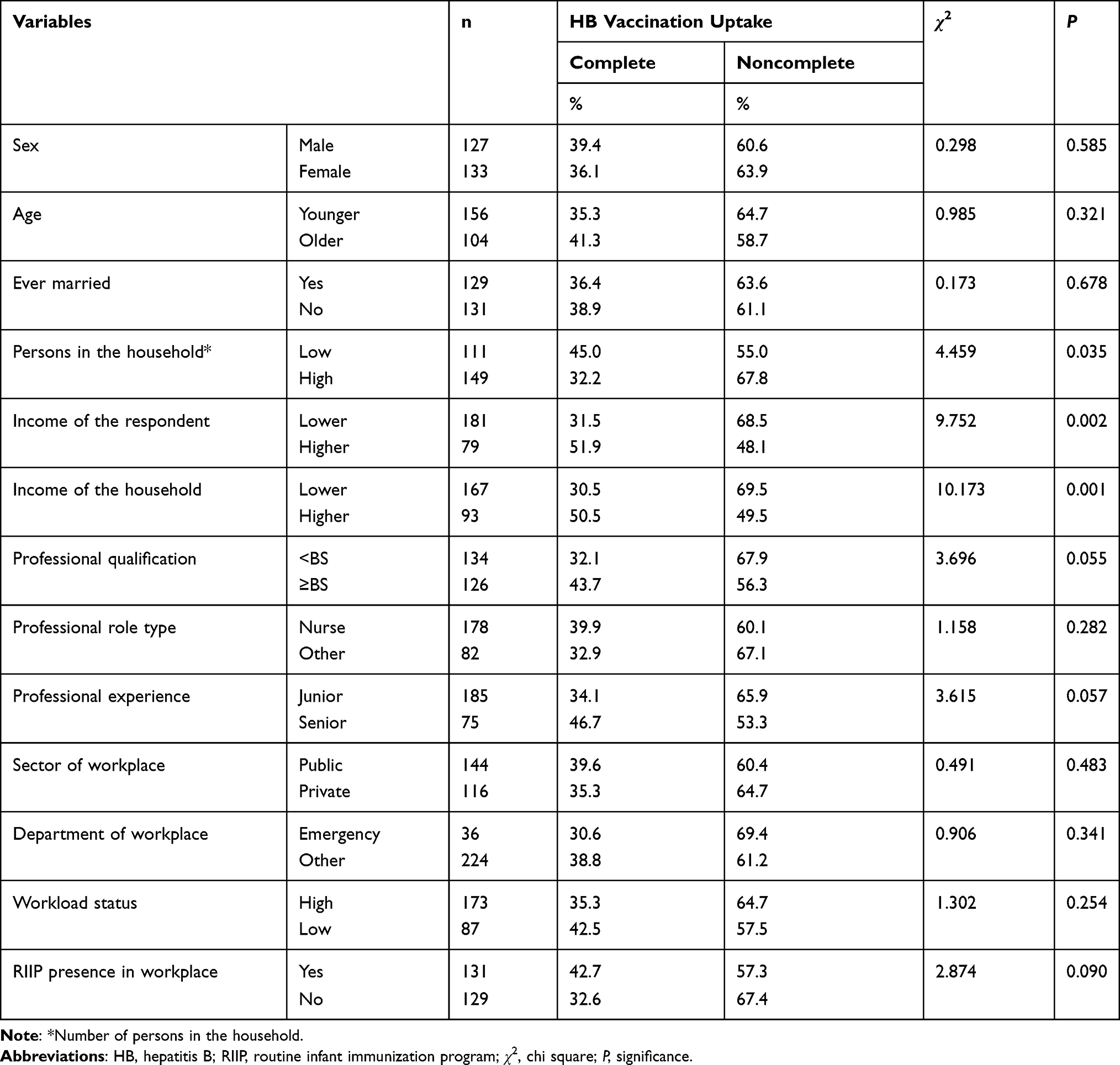 |
Table 2 Participants’ Demographic Characteristics and Hepatitis B Vaccination Uptake |
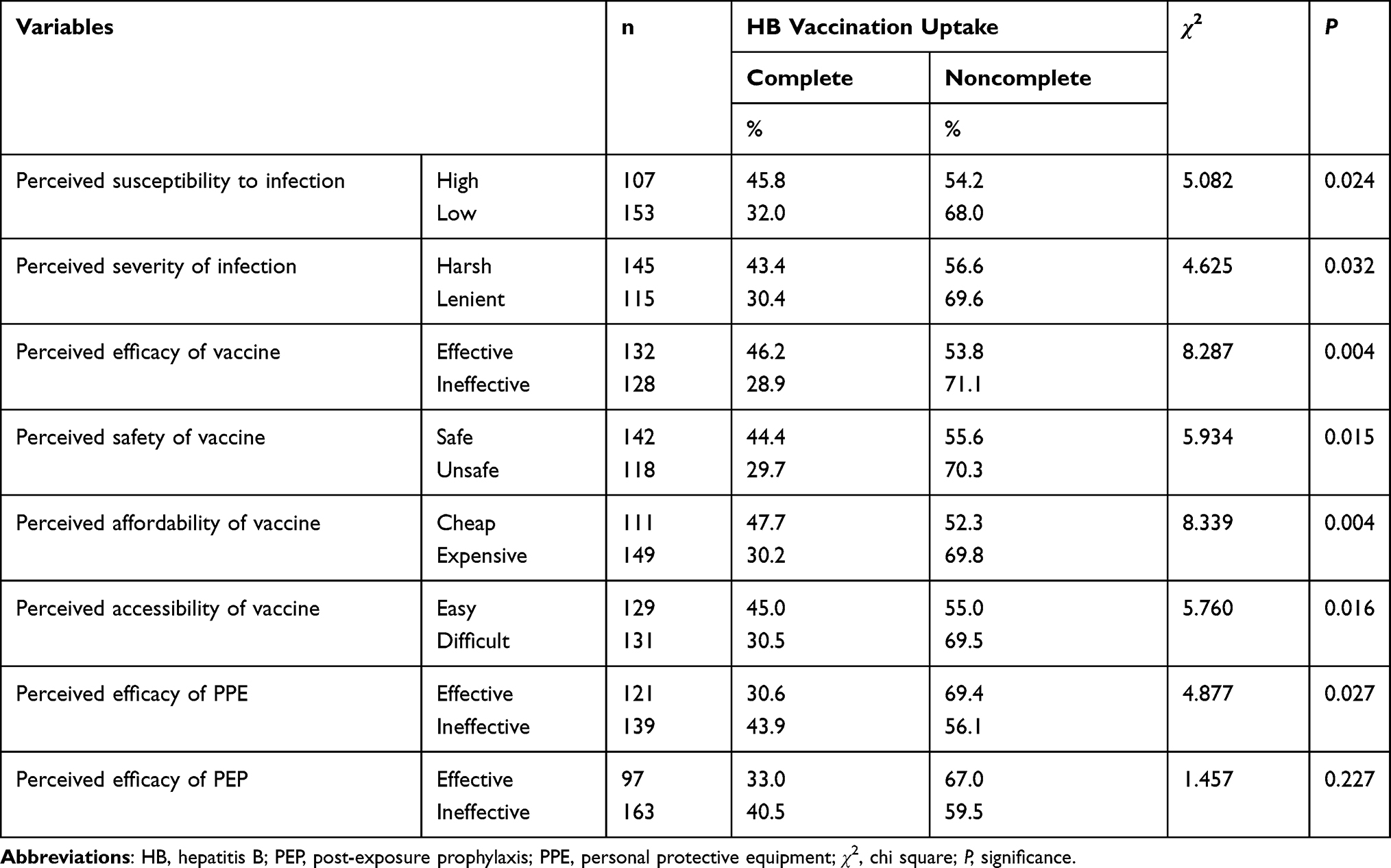 |
Table 3 Participants’ Psychosocial Characteristics and Hepatitis B Vaccination Uptake |
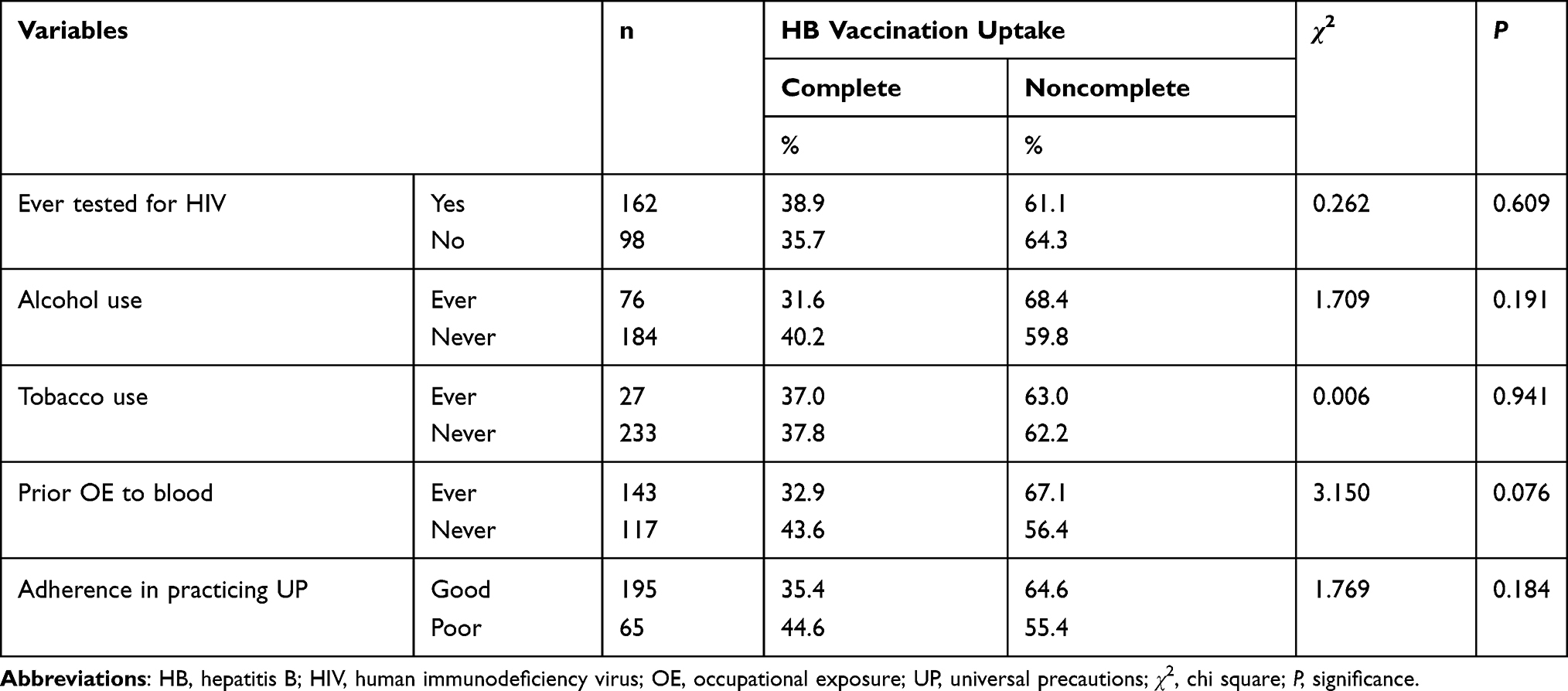 |
Table 4 Participants’ Behavioral Characteristics and Hepatitis B Vaccination Uptake |
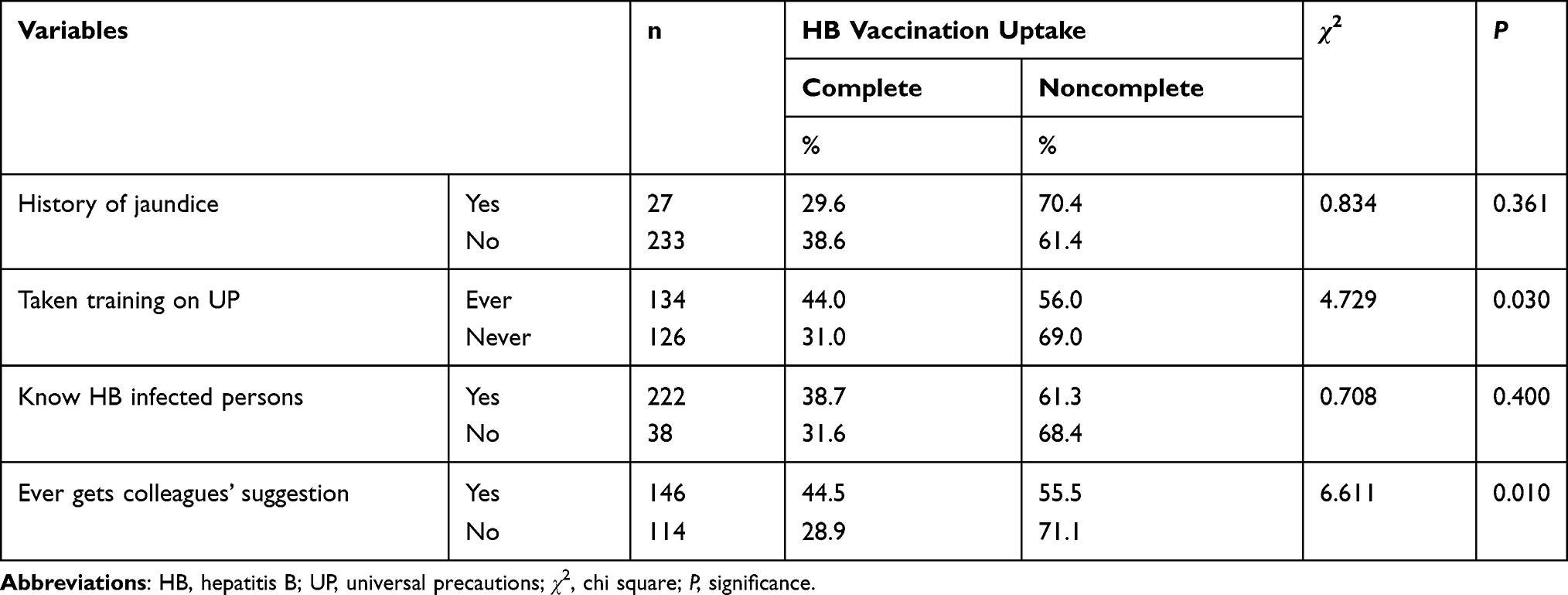 |
Table 5 Participants’ Miscellaneous Characteristics and Hepatitis B Vaccination Uptake |
Regardless of the statistical significance criterion stated, all those 20 of the 30 potential predictors that have shown P≤0.25 from the bivariate crosstab analysis were entered into the multivariable binary logistic regression analysis simultaneously. After series of logistic regression models through backward stepwise elimination approach, 10 different predictors were finally identified as independently associated with HB vaccination uptake at P<0.05 statistically significant criterion (Table 6): perceived safety, colleagues’ suggestion, professional qualification, perceived susceptibility, household income, prior OE, professional experience, RIIP existence, workload status, and UP training. The Hosmer–Lemeshow test suggests the overall predictive model is a good fit to the data (Table 6).
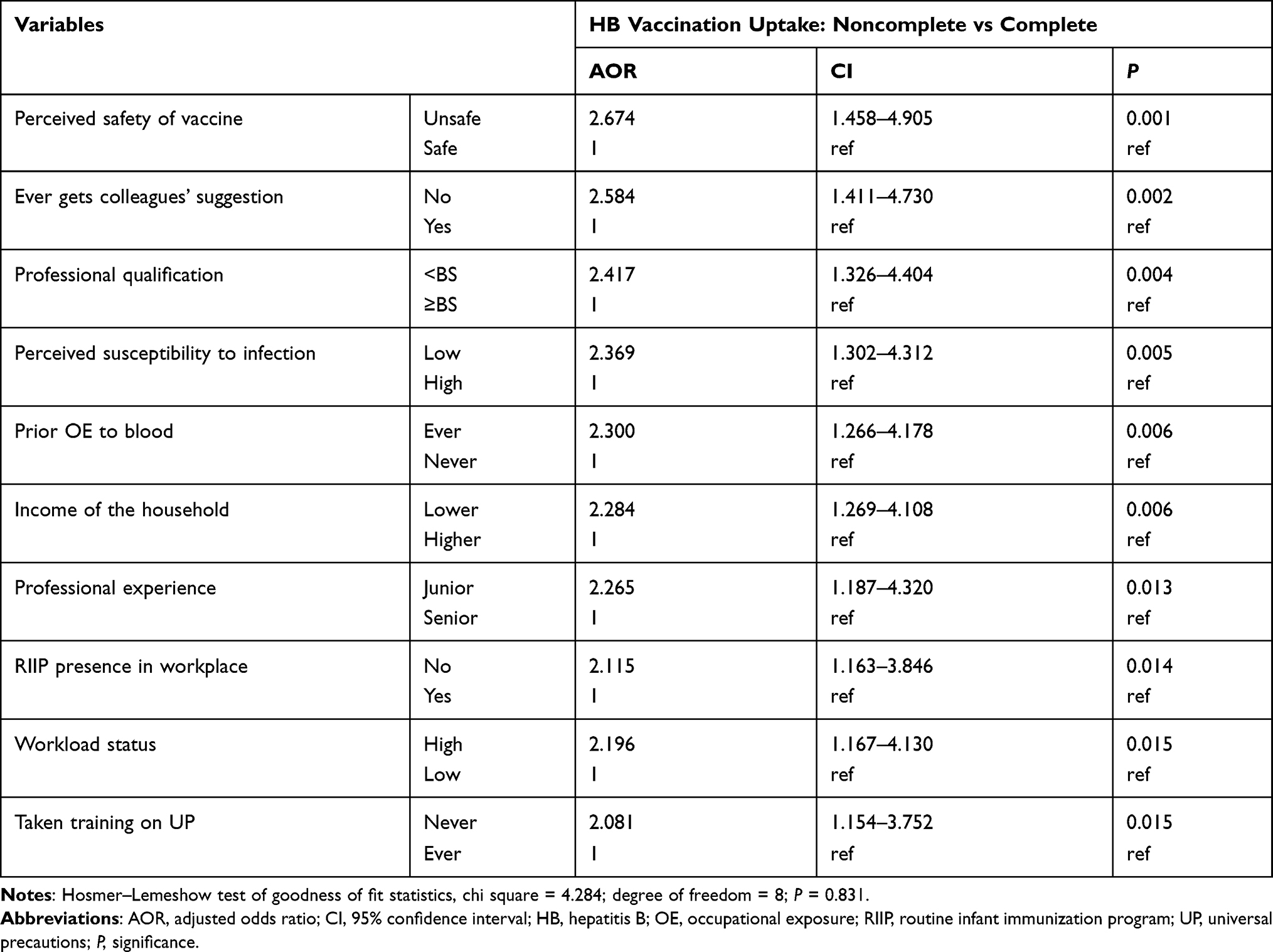 |
Table 6 Significantly Independent Predictors of Hepatitis B Vaccination Uptake in 260 Participants |
Discussion
The first specific objective of this survey was to determine the rate of HB vaccination uptake in HCPs of Ethiopia during 2018. The finding shows that the complete HB vaccination uptake rate was 37.7% (CI 31.9–43.3). The majority of the HCPs remained whether “partially vaccinated” (41.5%) or “unvaccinated” (20.8%), resulting in 62.3% (CI 56.7–68.1) for the noncomplete HB vaccination uptake rate.
Although direct comparison seems difficult, these compliance vs noncompliance rates are in line with the rates from Tanzania―during 2015,15 India―during 2011,9 Pakistan―during 2010,16 China―during 2008,17 and Sweden―during 2006.11 Our study’s key result on the HB vaccine compliance rate is also higher than the rates from some sub-Saharan African areas, such as Benin City, Nigeria―during 2011;18 Yaoundé, Cameroon―during 2014;7 and Shashemene, Ethiopia―during 2015.19 But it is lower than many others shown throughout the globe, including those in Oceania,12 Americas,20,21 Europe,22–24 Asia,10,25–27 and Africa8,28,29 with mysterious time variation between studies. The unexplained parity or disparity, in broad, maybe relies on the presence or absence of comprehensive data per exact context, as well as due to such differences or similarities as concerning the study design, period, place, and/or population attribute.
The second specific objective of this survey was to identify the predictors of HB vaccination uptake in HCPs of Ethiopia during 2018. The finding shows that only two of several psychosocial factors assessed were found the best independent predictors of HB vaccination uptake among HCPs: “perceived susceptibility” and “perceived safety.” The HCPs who perceived themselves as low susceptible were significantly more likely to have vaccination noncompliance (AOR 2.369, CI 1.302–4.312, P 0.005) than those who perceived themselves as high susceptible. A study from Nigeria demonstrates a similar pattern.30 The HCPs who perceived the vaccine as unsafe were significantly more likely to have noncomplete vaccination uptake (AOR 2.674, CI 1.458–4.905, P 0.001) when compared with those who perceived the vaccine as safe. This finding is congruent to literatures respectively from India,9 Georgia,31 and England.32 It also agrees with a study that described “[T]he main reason for declining vaccination was the risk of vaccine side effects.”33 The aftermath of a person’s perceived susceptibility to the harsh disease threat and a person’s perceived safety of taking successful action to reduce that threat may help them for willingness to pay for the cost of the vaccine being received.
Based on the Health Belief Model, the individual’s demographic characteristics and knowledge levels are modifying factors. Hypothesize that diverse demographic and cognitive factors affect the individual’s perception and thus indirectly influence the individual’s health-related behavior. For example, educational achievement, believed to have an indirect effect on HB vaccination uptake as the recommended health action or behavior by influencing the individual’s perceived threat agent (such as susceptibility to and severity of the infection) and perceived benefits–barriers of the action agent (such as safety, efficacy, and affordability of the vaccine) being taken to reduce that threat.34 However, our study shows that some demographics including professional, socioeconomic, and organizational characteristics have independently shown a statistically significant relationship with HB vaccination uptake from the best-fit predictive model.
The HCPs who had below BS degree were significantly more likely (AOR 2.417, CI 1.326–4.404, P 0.004) to have noncomplete vaccination uptake than those who had BS degree or above. This result is supported by a study carried out in Nigeria.29 Similarly, junior HCPs were significantly more likely (AOR 2.265, CI 1.187–4.320, P 0.013) to have noncomplete vaccination uptake than senior HCPs. This is consistent with previous studies,22,29 but not with another one showing insignificant association.35
The HCPs who had low-level household income were significantly more likely (AOR 2.284, CI 1.269–4.108, P 0.006) to have noncomplete HB vaccination uptake than those who had high-level household income. This designate may be modifiable through perceived cost of the vaccine, number of persons generating income for the household, number of economically dependent persons in the household, income of the respondent themselves, and readiness to pay for the cost of the vaccine being taken. Although income of the respondent36 and perceived affordability of the vaccine37 are among important predictors of the individual’s vaccination behavior, they become insignificant after adjustment in the present study. There is no previous statistical evidence from the literature showing the effect of household income on HB vaccination uptake among HCPs. We statistically discovered that association was best explained by income of the household rather than income of the respondent and perceived affordability of the vaccine. According to previous studies, lack of money to pay for the vaccine7 or high cost of the vaccine37 is described as one of the most common self-declared reasons among unvaccinated and/or incompletely vaccinated HCPs, which may be best explained by household income. According to one previous study carried out in the USA, the highest compliance rates are associated with hospitals paying the cost of vaccinating high-risk healthcare workers.38 We also believe that household income and other factors on the path can no longer be affecting the outcome if the vaccine is available with free cost for HCPs or if the institutions can pay for the cost of vaccinating them.
The HCPs who had high workload were significantly more likely (AOR 2.196, CI 1.167–4.130, P 0.015) to have vaccination noncompliance compared to those who had low workload. Whereas high workload could lead to lack of time to spend in getting vaccination, lack of time is also described as one of the most common self-declared reasons by unvaccinated and/or partially vaccinated HCPs.7,14 Other studies have shown that the department17 and sector19 of workplace facility have independent significant association with HB vaccination uptake behavior. These organizational demographics found not to be significant in our study as well as the result about the department and/or sector agrees with results from Tanzania,15 Nigeria,39 and India.9 It suggests that slight effects might be explained in part by workload variations between workplaces through that time spent-mediated pathway. However, this possibility was not directly explored in the present study, and further investigation is required.
The HCPs who are employed in the healthcare facilities not having RIIP had been significantly more likely to have vaccination noncompliance (AOR 2.115, CI 1.163–3.846, P 0.014) than those employed in the healthcare facilities having RIIP. Here, establishing RIIP throughout healthcare facilities could also be very important to increase the vaccination uptake rate in their employees against HB virus infection, despite further exploration for the mechanism of the association appears unclear, and would require further research with a better approach to clarify this quantitative evidence discovered for the first time. Additionally probing why that program is not available between healthcare institutions will have multidimensional benefits.
Among behavioral factors, OE history becomes an independent predictor of the outcome. The adjusted odds of being unvaccinated/partially vaccinated were significantly higher (AOR 2.300, CI 1.266–4.178, P 0.006) in the HCPs ever exposed to blood compared to those never exposed to blood. This result contradicts with another study showing statistically significantly higher rates of HB vaccination in Serbian healthcare workers who had at least one episode of OE to blood over the past year;22 OE as a positive motivating factor for favorable vaccination behavior. The main explanation for this inconsistence may be due to the national prevalence level of HB virus infection. It is clear that high prevalence of HB virus in developing countries (eg, Ethiopia) increases the risk of OE for HCPs who had contact with the patients’ blood to acquire/develop acute and/or chronic HB infections. One known divergent clinical perspective in this pathogenesis-mediated pathway is PEP (post-OE prophylactic therapy with anti-HB virus immunoglobulin); its availability, effectiveness, and usage may raise another question among the exposed HCPs. Somehow, frequent OE can probably bound them from receiving vaccination by making them ignorant unless actually infected – or by making them anxious toward acceptance of a volunteer HB surface antigen test as a requirement for PEP or vaccination eligibility in Ethiopia, and therefore national struggles must be ready to improve pre-OE compliance of vaccination in HCPs when they are approaching a high-risk target group.
Of the miscellaneous factors, both colleagues’ suggestion and UP training persisted independently significant. HCPs who did not get colleagues’ suggestion were significantly more likely to have vaccination noncompliance against HB virus (AOR 2.584, CI 1.411–4.730, P 0.002) than those who get colleagues’ suggestion. This is congruent to previous results from Italy,40 Georgia,31 and Ethiopia.37 Lastly, HCPs untrained on UP were significantly more likely to have HB vaccination noncompliance (AOR 2.081, CI 1.154–3.752, P 0.015) than those who trained on UP. UP training may influence their decision to choose their own best preventive action being taken to reduce that threat through a cognitive-mediated pathway. This result is supported by a previous study carried out in the Amhara regional state hospitals of Ethiopia that mentions that UP training will increase the awareness level of infection prevention among health professionals so they will become ready to be vaccinated.37
The results from this study will be very important to develop context-based comprehensive implementation and policy-making that may be effective to improve the HB vaccine uptake by HCPs as the best primary prevention strategy of HB infection; many potential influencing factors were tested, thereby the statistically significant independent factors were identified from the specific situation. This could fundamentally contribute to maintain the occupational safety and health among HCPs. Devoting in occupational safety and health reduces both direct and indirect costs, increasing societal security and health, decreases absenteeism, increases worker and coworker morale, and then improves overall performance and productivity in the country. Nationally, reduced societal security and healthcare costs means better economic performance and enhanced societal benefits.4 Our study might further oblige as part of the “global hepatitis eradication goal by 2030“ which is planned by the WHO and is already accepted by the regime FMOH-Ethiopia.
This study has several limitations. First is that the vaccination behavior was investigated by interviewing the participants, for which reflected recall bias may have affected the results of this study. It is also measured only based on the number of doses received by the participant, regardless of time after the last dose and time lapses between doses. As the second limitation was while vaccination did not always render into serologic antibody response, we were unable to investigate anti-HBs serologic antibody titers. Integrating the survey results with medical records or laboratory assessment of anti-HBs serologic antibody titers would have helped to inform policy change mainly including whether post primary series completion booster doses are required. In addition, we were unable to use pre-enrollment serologic HB virus antigen screening. Serologic antigen laboratory investigation would be required to exclude the HB-infected HCPs from analysis and then would have helped to avoid underestimation of vaccination uptake rates. The third limitation was as the largest proportion of participants in our study are nursing HCPs, we were only able to analyze other groups of HCPs (eg, physicians, lab technologists, physiotherapists, anesthetists) merged due to tiny frequency distributions. Caution must be therefore used to generalize the results to other groups of HCPs separately (vs nursing HCPs) regarding professional role type. The fourth limitation was that we were restricted to the forms of indicators we could use. We were unable to examine the effect of the availability of HB vaccine particularly for HCPs between their own workplace facilities, instead, we used the availability of RIIP between their own workplace facilities and their perception toward the accessibility of HB vaccine in any nearby facility as indicators. We believe that only vaccinated participants tend to have default information on whether the HB vaccine is available at their own workplace institutions for vaccinating themselves even if that information is inadequately broadcast to the overall participants. Direct investigation of the healthcare workplace facilities for the availability of HB vaccination for vaccinating HCPs is therefore required. As professional role type was reclassified quite broadly in the present study, our categories differed from those often used in previous studies. In addition, self-declared reasons for non- or partial-vaccination status against HB virus infection were not directly described in the scope of the present study because they are not applicable to conduct such statistical comparison among all analytic participants. Separate enrollment and analysis of unvaccinated/partially vaccinated participants is therefore required to clearly determine whether there is any effect from self-declared reasons. These limitations may affect the results of this study, making them less generalizable. Future research studies should take these points into account as well.
Conclusion
The rate of HB vaccination uptake in HCPs of Ethiopia found was currently low. The significantly independent predictors of HB vaccination uptake included perceived safety, colleagues’ suggestion, professional qualification, perceived susceptibility, household income, prior OE to blood, professional experience, existence of RIIP at workplace facility, workload status, and UP training.
Abbreviations
AOR, adjusted odds ratio; CDC, Centers for Disease Control and Prevention; CI, 95% confidence interval; FMOH, Federal Ministry of Health; HB, hepatitis B; HCP, healthcare professional; HIV, human immunodeficiency virus; IBM, International Business Machines Corporation; OE, occupational exposure; PEP, post-exposure prophylaxis; PPE, personal protective equipment; RIIP, routine infant immunization program; SPSS, Statistical Product and Service Solutions; UP, universal precautions; WHO, World Health Organization.
Data Sharing Statement
All relevant data are available in this manuscript and its supplementary materials.
Ethics Approval and Consent to Participate
The University of Gondar the College of Medicine and Health Sciences ethics committee approved the study protocol. In addition, the study obtained an official permission letter from the Central Gondar Zone Health Administration. All participants gave their written informed consent to participate.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Burns GS, Thompson AJ. Viral hepatitis B: clinical and epidemiological characteristics. Cold Spring Harb Perspect Med. 2014;4(12):a024935. doi:10.1101/cshperspect.a024935
2. Poorolajal J, Majdzadeh R. Prevalence of chronic hepatitis B infection in Iran: a review article. J Res Med Sci. 2009;14(4):249–258.
3. Leigh JP. Economic burden of occupational injury and illness in the United States. Milbank Q. 2011;89(4):728–772. doi:10.1111/j.1468-0009.2011.00648.x
4. International Labour Organization. Global trends on occupational accidents and diseases. World Day Saf Heal Work. 2015:1–7.
5. Pappas SC, Fisher MM. Preventing hepatitis B in health care workers. Can Fam Physician. 1985;31:1941–1944.
6. Jin H, Tan Z, Zhang X, Wang B, Zhao Y, Liu P. Comparison of accelerated and standard hepatitis B vaccination schedules in high-risk healthy adults: a meta-analysis of randomized controlled trials. PLoS One. 2015;10(7):e0133464. doi:10.1371/journal.pone.0133464
7. Tatsilong HOP, Noubiap JJN, Nansseu JRN, et al. Hepatitis B infection awareness, vaccine perceptions and uptake, and serological profile of a group of health care workers in Yaoundé, Cameroon. BMC Public Health. 2016;16(1):706. doi:10.1186/s12889-016-3388-z
8. Ziglam H, El-Hattab M, Shingheer N, Zorgani A, Elahmer O. Hepatitis B vaccination status among healthcare workers in a tertiary care hospital in Tripoli, Libya. J Infect Public Health. 2013;6(4):246–251. doi:10.1016/j.jiph.2013.02.001
9. Pathak R, Chaudhary C, Pathania D, Ahluwalia SK, Mishra PK, Kahlon AS. Hepatitis B vaccine: coverage and factors relating to its acceptance among health care workers of a tertiary care center in North India. Int J Med Public Heal. 2013;3(1):55–59. doi:10.4103/2230-8598.109324
10. Abdifard E, Faraji A, Sepahvand E, Aghae A, Khachian A. Hepatitis B vaccination coverage and its associated factors in nurses of Imam Reza (AS) Hospital in Kermanshah. J Client-Centered Nurs Care. 2016;2(2):97–102. doi:10.32598/jccnc.2.2.97
11. Dannetun E, Tegnell A, Torner A, Giesecke J. Coverage of hepatitis B vaccination in Swedish healthcare workers. J Hosp Infect. 2006;63(2):201–204. doi:10.1016/j.jhin.2006.01.014
12. Murray SB, Skull SA. Poor health care worker vaccination coverage and knowledge of vaccination recommendations in a tertiary Australia hospital. Aust N Z J Public Health. 2002;26(1):65–68. doi:10.1111/j.1467-842X.2002.tb00273.x
13. Chaudhari CN, Bhagat MR, Ashturkar A, Misra RN. Hepatitis B immunisation in health care workers. Med J Armed Forces India. 2009;65(1):13–17. doi:10.1016/S0377-1237(09)80046-4
14. Malewezi B, Omer SB, Mwagomba B, Araru T. Protecting health workers from nosocomial hepatitis B infections: a review of strategies and challenges for implementation of hepatitis B vaccination among health workers in Sub-Saharan Africa. J Epidemiol Glob Health. 2016;6(4):229–241. doi:10.1016/j.jegh.2016.04.003
15. Aaron D, Nagu TJ, Rwegasha J, Komba E. Hepatitis B vaccination coverage among healthcare workers at national hospital in Tanzania: how much, who and why? BMC Infect Dis. 2017;17(1):786. doi:10.1186/s12879-017-2893-8
16. Yousafzai MT, Qasim R, Khalil R, Kakakhel MF, Rehman SU. Hepatitis B vaccination among primary health care workers in Northwest Pakistan. Int J Health Sci (Qassim). 2014;8(1):67–76. doi:10.12816/0006073
17. Zheng YB, Gu YR, Zhang M, et al. Health care workers in Pearl River Delta Area of China are not vaccinated adequately against hepatitis B: a retrospective cohort study. BMC Infect Dis. 2015;15(1):542. doi:10.1186/s12879-015-1278-0
18. Azodo C, Ehizele A, Uche I, Erhabor P. Hepatitis-B vaccination status among dental surgeons in Benin City, Nigeria. Ann Med Health Sci Res. 2012;2(1):24. doi:10.4103/2141-9248.96932
19. Abebaw T-A, Aderaw Z, Gebremichael B. Hepatitis B virus vaccination status and associated factors among health care workers in Shashemene Zonal Town, Shashemene, Ethiopia: a cross sectional study. BMC Res Notes. 2017;10(1):260. doi:10.1186/s13104-017-2582-0
20. Byrd KK, Lu PJ, Murphy TV. Hepatitis B vaccination coverage among health-care personnel in the United States. Public Health Rep. 2013;128(6):498–509. doi:10.1177/003335491312800609
21. Ciorlia LAS, Zanetta DMT. Hepatitis B in healthcare workers: prevalence, vaccination and relation to occupational factors. Braz J Infect Dis. 2005;9(5):384–389. doi:10.1590/S141386702005000500005
22. Kisic-Tepavcevic D, Kanazir M, Gazibara T, et al. Predictors of hepatitis B vaccination status in healthcare workers in Belgrade, Serbia, December 2015. Euro Surveill. 2017;22(16):
23. Nee PA, Randall PE, Heyworth J. Hepatitis B vaccination: uptake by medical staff in accident and emergency departments. J Accid Emerg Med. 1995;12(4):282–285. doi:10.1136/emj.12.4.282
24. Garruto V, Scalingi S, Siclari M, Chiarini M, La Torre G, Mannocci A. Knowledge, attitude and behaviours towards recommended vaccinations among healthcare workers. Healthcare. 2017;5(1):13. doi:10.3390/healthcare5010013
25. Momeni N, Akhoundi MSA, Alavian SM, et al. HBV vaccination status and response to hepatitis B vaccine among Iranian dentists, correlation with risk factors and preventive measures. Hepat Mon. 2015;15(1):e20014. doi:10.5812/hepatmon.20014
26. Batra V, Goswami A, Dadhich S, Kothari D, Bhargava N. Hepatitis B immunization in healthcare workers. Ann Gastroenterol. 2015;28(2):276–280.
27. Kumar HNH, Nambiar RP, Mohapatra S, Khanna A, Praveen R, Bhawana DS. A cross-sectional study on hepatitis B vaccination status and post-exposure prophylaxis practices among health care workers in teaching hospitals of Mangalore. Ann Glob Heal. 2015;81(5):664–668. doi:10.1016/j.aogh.2015.08.015
28. Abiola AHO, Agunbiade AB, Badmos KB, Lesi AO, Lawal AO, Alli QO. Prevalence of HBsAg, knowledge, and vaccination practice against viral hepatitis b infection among doctors and nurses in a secondary health care facility in Lagos state, south-western Nigeria. Pan Afr Med J. 2016;23:160. doi:10.11604/pamj.2016.23.160.8710
29. Omotowo IB, Meka IA, Ijoma UN, et al. Uptake of hepatitis B vaccination and its determinants among health care workers in a tertiary health facility in Enugu, South-East, Nigeria. BMC Infect Dis. 2018;18(1):288. doi:10.1186/s12879-018-3191-9
30. Ochu CL, Beynon CM. Hepatitis B vaccination coverage, knowledge and sociodemographic determinants of uptake in high risk public safety workers in Kaduna State, Nigeria: a cross sectional survey. BMJ Open. 2017;7(5):e015845. doi:10.1136/bmjopen-2017-015845
31. Topuridze M, Butsashvili M, Kamkamidze G, Kajaia M, Morse D, McNutt LA. Barriers to hepatitis B vaccine coverage among healthcare workers in the Republic of Georgia: an international perspective. Infect Control Hosp Epidemiol. 2009;31(02):158–164. doi:10.1086/649795
32. Heyworth J. Hepatitis B vaccination in United Kingdom accident and emergency departments. Emerg Med J. 1988;5(2):59–68. doi:10.1136/emj.5.2.59
33. Riccò M, Vezzosi L, Gualerzi G, Signorelli C. Knowledge, attitudes and practices (KAP) towards vaccinations in the school settings: an explorative survey. J Prev Med Hyg. 2017;58(4):E266–E278. doi:10.15167/2421-4248/jpmh2017.58.4.673
34. Al-Hussami M. Knowledge and acceptance of hepatitis B vaccine. Internet J Healthc Adm. 2001;2(1):1–41. doi:10.5580/a8b
35. Bekele A, Tadesse A. Status of hepatitis B vaccination among surgeons practicing in Ethiopia: a cross sectional study. Ethiop Med J. 2014;52(3):107–112.
36. Yimer YS, Mohammed MS, Muhammed KM, Tsige Y. Predictors and vaccination status of nurses against hepatitis B virus at public hospitals in Addis Ababa, Ethiopia. Int J Public Heal Saf. 2017;2(4):142.
37. Feleke BE. Low coverage of hepatitis B vaccine and determinants among health professionals working in Amhara regional state hospitals, Ethiopia. J Public Health Africa. 2016;7(2):553. doi:10.4081/jphia.2016.553
38. Alexander PG, Johnson R, Williams WW, Hadler SC, White JW, Coleman PJ. Hepatitis B vaccination programs for health care personnel in U.S. hospitals. Public Health Rep. 1990;105(6):610–616.
39. Okwara EC, Enwere OO, Diwe CK, Azike JE, Chukwulebe AE. Theatre and laboratory workers’ awareness of and safety practices against hepatitis B and C infection in a suburban university teaching hospital in Nigeria. Pan Afr Med J. 2012;13:2.
40. Fortunato F, Tafuri S, Cozza V, Martinelli D, Prato R. Low vaccination coverage among Italian healthcare workers in 2013: contributing to the voluntary vs. mandatory vaccination debate. Hum Vaccines Immunother. 2015;11(1):133–139. doi:10.4161/hv.34415
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.