Back to Journals » International Journal of Women's Health » Volume 17
Hepatic Angiosarcoma with eosinophilia: A Case Report and Literature Review
Authors Chen M, Chen X, Wang S, Lei D, Peng C
Received 6 November 2024
Accepted for publication 8 March 2025
Published 14 March 2025 Volume 2025:17 Pages 785—791
DOI https://doi.org/10.2147/IJWH.S505065
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Meiqin Chen,1 Xiguo Chen,2 Shun Wang,1 Dan Lei,1 Chunxian Peng1
1Department of Infectious Diseases, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou, People’s Hospital, Quzhou, People’s Republic of China; 2Department of Electromechanical Engineering, Quzhou College of Technology, Quzhou, People’s Republic of China
Correspondence: Chunxian Peng, Email [email protected]
Background: Hepatic angiosarcoma is an extremely rare, uncontrollable tumor with strong invasion, high mortality rate, and extremely poor prognosis. There is first report on hepatic angiosarcoma accompanied by eosinophilia.
Case Presentation: A woman with a chief complaint of poor appetite for about 3 months presented to a local hospital with a liver mass. Laboratory examination revealed a significant increase in eosinophils count was 9.58% in the serum. Abdominal MRI revealed multiple focal high-density lesions in the liver and spleen, and cranial MRI revealed multiple high-density shadows in the skull. Laparoscopic biopsy revealed a hepatic angiosarcoma and targeted treatment with Anlotinib was performed. Two months later, the patient died of splenic rupture and bleeding.
Conclusion: Hepatic angiosarcoma often has no specific clinical manifestations, and we found that this case can lead to an increase in eosinophils, which is worth the attention of clinical physicians.
Keywords: hepatic angiosarcoma, eosinophilia, prognosis, diagnosis, case report
Introduction
Primary eosinophilia is relatively rare, whereas autoimmune, infectious, and inflammatory diseases, malignant tumors, and allergies can cause secondary eosinophilia. Treatment may be more effective for infectious diseases, inflammatory diseases, autoimmune diseases, and malignancies accompanied by eosinophilia.1
Primary hepatic angiosarcoma (PHA) is a rare mesenchymal derived liver tumor, accounting for only 0.1% −2% of all primary liver malignancies.2,3 Diagnosis of PHA is challenging due to its atypical symptoms and difficulties in distinguishing it from other malignancies through imaging. Surgical resection is the most effective treatment option, but most cases are already metastatic at diagnosis. Systemic or local chemotherapy can be used for palliative treatment. Anti-angiogenic therapy shows promise but lacks comparative efficacy data. In 1974, PHA was first reported by Block,4 since then, there have been relatively few data and reports on the diagnosis, treatment, and prognosis of this tumor owing to its rarity.5 This report is the first case of PHA with increased eosinophils, with missed surgical opportunity, unsuccessful targeted treatment, and fatal outcome, emphasizing the need for early detection and intervention in PHA cases.
Case Presentation
A 60-year-old female who had previously been in good health was admitted to our department on April 3, 2023, with the main complaint of loss of appetite for 3 months. One day prior, the patient visited a local hospital and underwent a full abdominal CT, which revealed a liver mass. Therefore, the patient was admitted to our hospital. The patient had no significant history of past illnesses. No notable personal or family medical history was reported. On admission, the physical examination was unremarkable, with a BMI of 23. Cardiac and pulmonary auscultation were normal, and there were no abnormalities detected in the liver, spleen, or subcostal regions upon palpation. No tenderness or pain was observed. Abnormal laboratory results, other liver function tests and tumor markers levels can be seen in Table 1. Further Improvement of Upper Abdominal MRI Enhancement revealed the following findings (Figure 1A and B): Diffuse multiple nodular and patchy abnormal enhancement lesions in the liver and spleen. The larger liver lesion measured approximately 2.2×2.1cm, while the larger spleen lesion measured about 6.5×5.5 cm. Considering the possibility of a parasitic infection, the patient exhibited an increase in eosinophils and multiple nodules in the liver and spleen. The patient denied any exposure to unclean drinking water or consumption of raw shrimp and crabs. To further investigate, a lung CT scan and an enhanced MRI of the head were performed (Figure 1C and D). No evident abnormalities were detected in the chest or intracranial region. However, multiple abnormal signal shadows with enhancement or metastatic tumors were observed in the skull. This raised questions about the presence of parasites or tumors in the brain and whether the changes in the liver, spleen, and skull could be attributed to the same underlying condition. The patient’s parasite antibody test came back negative (Table 1). As a result, we conducted multidisciplinary team (MDT) discussions on the matter. The patient underwent laparoscopic resection of the liver mass, and the subsequent postoperative pathology analysis (Figure 2A and B) confirmed the presence of hepatic angiosarcoma. Microscopic examination revealed the presence of spindle-shaped cells with frequent mitotic activity. Immunohistochemistry demonstrated positive expression of endothelial cell markers, including CD31, CD34, and CD99, as well as ERG. Additionally, the Ki-67 proliferative index was determined to be 50%. Ultimately, the diagnosis of hepatic angiosarcoma was definitively confirmed. Chemotherapy is recommended, but the patient refused. The latest report shows6 that patients have achieved effective treatment through TACE (Transcatheter arterial chemoembolization) and treatment with Anlotinib plus Camrelizumab. So targeted treatment with anlotinib was given, but after 2 months, the patient died of splenic rupture and bleeding. The patient’s clinical course timeline is shown in Figure 3.
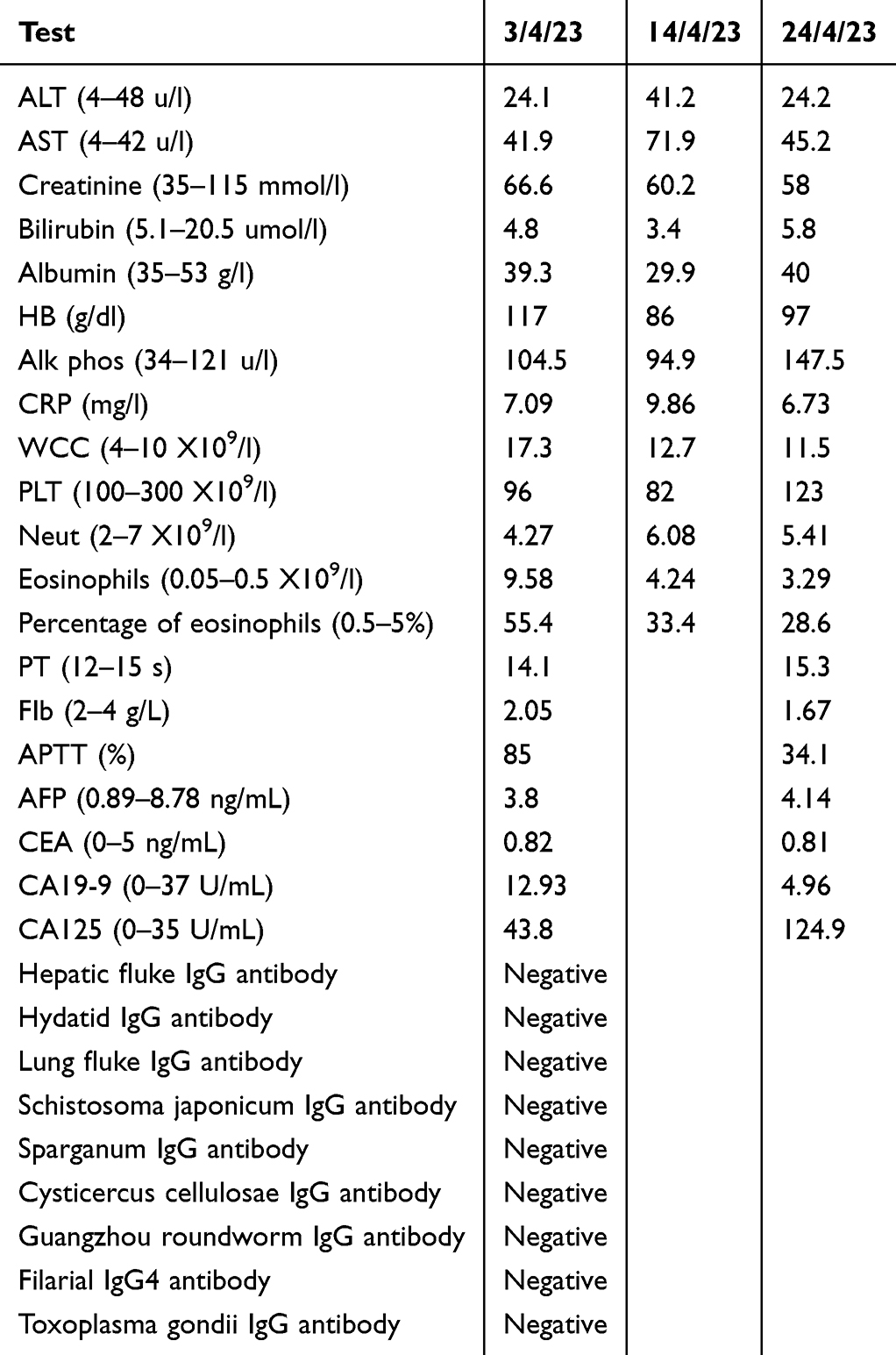 |
Table 1 Laboratory Results |
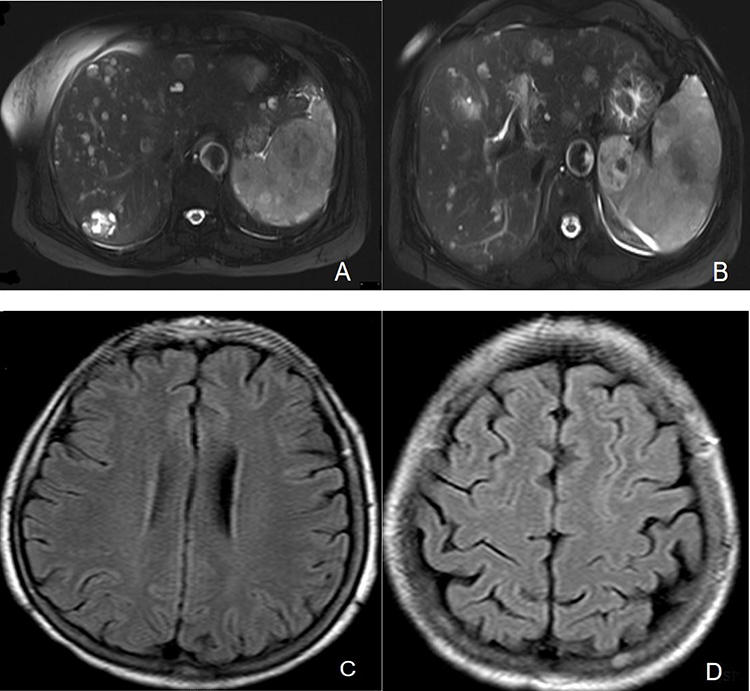 |
Figure 1 (A and B) Upper abdominal MRI enhancement: April 3, 2023: Diffuse multiple nodular and patchy T1WI low signal and T2WI mixed high signal shadows can be seen in the liver and spleen parenchyma, with unclear boundaries. The enhanced scan shows centripetal filling enhancement, some show mild enhancement, and some do not. (C and D) Enhanced cranial magnetic resonance imaging, April 7, 2023. Multiple strip shaped abnormal signal shadows in the skull are seen, showing low signal on T1WI, high signal on T2WI and FLAIR, high signal on DWI, equal or low signal on ADC, and boundary Insufficient clarity, significantly enhanced after enhancement. |
 |
Figure 2 (A and B) Liver pathology, April 24, 2023: Spindle cell tumor (liver mass), with frequent mitosis and tendency towards malignancy. |
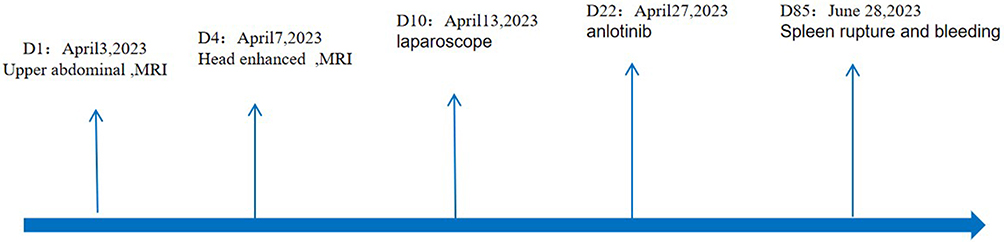 |
Figure 3 Timeline of patient’s clinical course. |
Discussion
Hemangiosarcoma belongs to a group of adult soft-tissue sarcomas, and among them primary hepatic angiosarcoma (PHA) is a rare mesenchymal tumor with a worse prognosis compared to other angiosarcomas. Although exposure to vinyl chloride, has been associated with PHA in some cases, the exact causes are still unclear for most patients. However, there is no evidence that these factors were involved in this patient.
PHA lacks specific symptoms, but presents with non-specific complaints such as stomach discomfort, fatigue, poor appetite, weakness, and a feeling of heaviness.7 The most common fatal and poorest prognosis are splenic rupture8 and bleeding, as in our case the patient died of spontaneous splenic rupture and ultimately hemorrhagic shock.
Diagnosis mainly relies on pathological examination since distinguishing PHA from other malignant tumors using ultrasound, CT, or MRI is challenging. Early detection is crucial as PHA can be misdiagnosed as a hemangioma in the early stages, and surgical resection is necessary to prevent malignant progression.6 Only a small percentage of patients eligible for surgical resection, which has shown effectiveness and long-term survival in some cases. However, most cases of liver angiosarcoma are already metastatic at the time of diagnosis and cannot be treated surgically.9 Tumors smaller than 10 cm are the only favorable factor for partial hepatectomy.10 For patients who are not candidates for surgery, systemic or local chemotherapy can be used as palliative treatment. Anti- angiogenic therapy shows promise but comparing the efficacy of different treatment strategies is challenging due to the limited number of patients and the use of diverse drugs. Neeraj11 reviewed 23 patients with hepatic vascular sarcoma revealed a median overall survival (OS) was 6 months, with 71% of patients receiving systemic chemotherapy and 29% receiving immunotherapy. 14% of patients underwent surgery or local treatment with radiation embolization. Wilson12 retrospective showed Forty-four patients with hepatic angiosarcoma, only 10 patients underwent surgical resection. Median overall survival was 5.8 months and 1-, 3-, and 5-year actual survival was 30.0%, 8.1%, and 5.6%, respectively. A prospective study conducted by Tripke et al13 reported Nine patients who underwent surgical resection with median follow-up was 15.5 months. Mangla14 analyzed 346 patients with PHA, with one- third (35.7%) received chemotherapy, and 14.6% underwent a surgical resection. The median survival was 1.9 months, with a higher median survival rate of 7.7 months for surgical resection. The median survival rate for patients receiving chemotherapy is higher than that for those not receiving chemotherapy. An overall summary of cases and characteristics of primary hepatic angiosarcoma from previous retrospective and prospective studies is presented in Table 2.
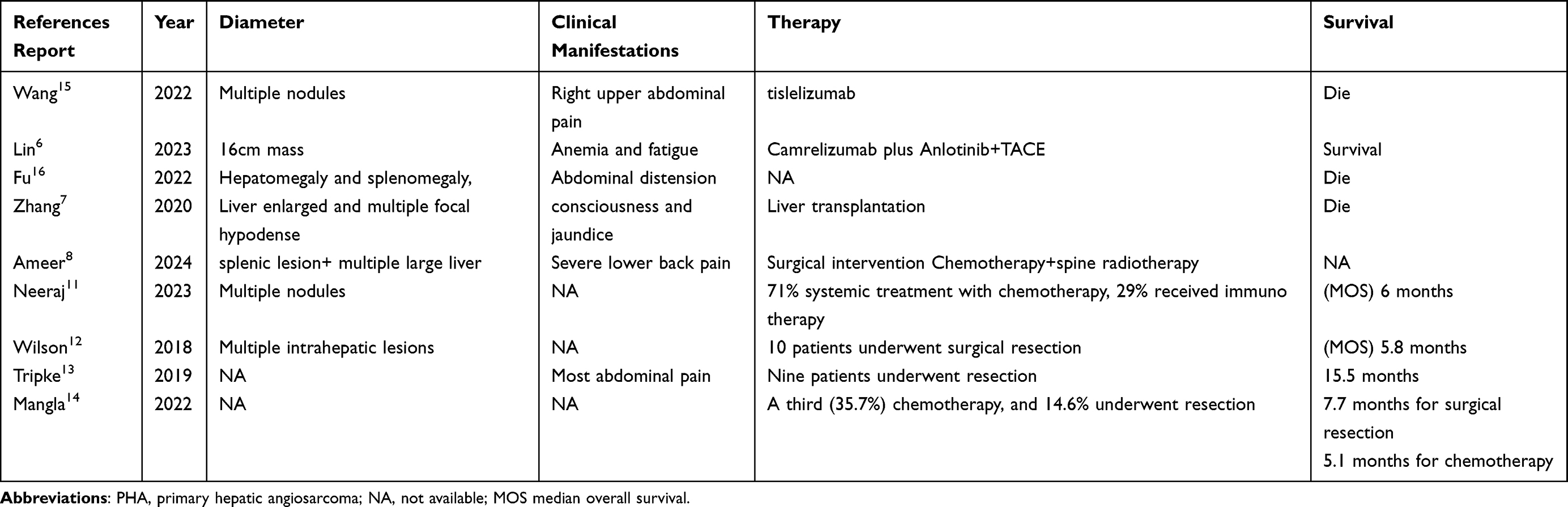 |
Table 2 An Overall Summary of Cases and Characteristics of Primary Hepatic Angiosarcoma |
The case presented involves a patient who sought medical attention due to decreased appetite and was found to have an elevated eosinophils count. Abdominal CT revealed multiple liver nodules, and surprisingly, high-density metastatic lesions were also found in the skull. Tumor markers only show CA125 Slight elevation. A laparoscopic biopsy confirmed the diagnosis of hepatic angiosarcoma, but the opportunity for surgical intervention had been missed. Although less invasive biopsies or even cytological examination have a good diagnostic yield in the diagnosis of sarcoma,17 especially in patients not eligible for excisional surgical therapy. Koyama et al18 reported a 78% success rate for biopsy, to ensure a positive detection, the MDT recommended laparoscopic extraction of the liver nodules for further examination instead of ultrasound-guided liver puncture biopsy. Consequently, the patient underwent laparoscopic resection of the liver mass. The present study showed that PHA expresses at least one among CD31, CD34, and that the Ki-67 increase, which is a common diagnostic feature of angiosarcoma.19 In this study, CD34 (+), CD31 (+), and Ki67 (about 50%) expression was consistent with that reported in the literature.15 we find CD99+, as it was reported to have an adverse prognostic role and to correlate with the development of distant metastases in angiosarcomas in other settings.20 Targeted treatment with Anlotinib was administered for two months, but the patient’s condition did not significantly improve. Eventually, the tumor ruptured, leading to bleeding and the patient’s death.
Conclusion
In clinical practice, PHA awareness should be raised, and early biopsy of lesions should be performed based on symptoms. The provides a pathological basis for subsequent treatment selection and further assist in clinical diagnosis and treatment.
Ethical Approval Statement
Informed written consent to participate in this study was provided by the participants’ legal guardians/next of kin, who and agreed for the publication of all images, clinical data and other data included in the manuscript.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received funding support by Quzhou 2022 “Guiding Project of Quzhou Science and Technology Bureau (2022007).
Disclosure
The authors declare that they have no conflicts of interest to disclose.
References
1. Thomsen GN, Christoffersen MN, Lindegaard HM. The multidisciplinary approach to eosinophilia.. Front Oncol. 2023;13:1193730. doi:10.3389/fonc.2023.1193730
2. Mani H, Van Thiel DH. Mesenchymal tumors of the liver. Clin Liver Dis. 2001;5(1):219–57,viii. doi:10.1016/s1089-3261(05)70162-8
3. Molina E, Hernandez A. Clinical manifestations of primary hepatic angiosarcoma. Dig Dis Sci. 2003;48(4):677–682. doi:10.1023/a:1022868221670
4. Block JB. Angiosarcoma of the liver following vinyl chloride exposure. JAMA. 1974;229(1):53–54.
5. Zhu Y-P, Chen Y-M, Matro E. Primary hepatic angiosarcoma: a report of two cases and literature review. World J Gastroenterol. 2015;21(19):6088–6096. doi:10.3748/wjg.v21.i19.6088
6. Lin Y, Chen Z, Yang J. Advanced diffuse hepatic angiosarcoma treated successfully with TACE and targeted immunotherapy: a case report. Front Oncol. 2023;13:1071403. doi:10.3389/fonc.2023.1071403
7. Zhang X-M, Tong Y, Li Q, He Q. Diffused hepatic angiosarcoma with Kasabach-Merritt syndrome-case report and literature review. BMC Gastroenterol. 2020;20(1):80. doi:10.1186/s12876-020-01216-z
8. Awashra A, Sawaftah Z, Odah AB. Spontaneous splenic rupture as a primary manifestation of angiosarcoma: a case report. J Surg Case Rep. 2024;2024(10):rjae633. doi:10.1093/jscr/rjae633
9. Kim HR, Rha SY, Cheon SH, Roh JK, Park YN, Yoo NC. Clinical features and treatment outcomes of advanced stage primary hepatic angiosarcoma. Ann Oncol. 2009;20(4):780–787. doi:10.1093/annonc/mdn702
10. Li DB, Si XY, Wan T, Zhou YM. A pooled analysis of treatment and prognosis of hepatic angiosarcoma in adults. Hepatobiliary Pancreatic Dis Int. 2018. 3: 198–203.
11. Ramakrishnan N, Mokhtari R, Charville GW, Bui N, Ganjoo K. Management Strategies and Outcomes in Primary Liver Angiosarcoma. Am J Clin Oncol. 2023;46(10):439–444. doi:10.1097/coc.0000000000001032
12. Wilson GC, Lluis N, Nalesnik MA. Hepatic Angiosarcoma: a Multi-institutional, International Experience with 44 Cases. Ann Surg Oncol. 2018;26(2):576–582. doi:10.1245/s10434-018-7062-9
13. Tripke V, Heinrich S, Huber T, et al. Surgical therapy of primary hepatic angiosarcoma. BMC Surg. 2019;19(1). doi:10.1186/s12893-018-0465-5
14. Mangla A, Cioffi G, Barnholtz-Sloan JS, Lee RT. Treatment outcomes for primary hepatic angiosarcoma: national cancer database analysis 2004–2014. Current Oncol. 2022;29(5):3637–3646. doi:10.3390/curroncol29050292
15. Wang J, Sun L-T. Primary hepatic angiosarcoma: a case report. World J Clin Cases. 2022;10(31):11590–11596. doi:10.12998/wjcc.v10.i31.11590
16. Ha F-S, Liu H, Han T, Song D-Z. Primary hepatic angiosarcoma manifesting as hepatic sinusoidal obstruction syndrome: a case report. World J Gastroint Oncol. 2022;14(5):1050–1056. doi:10.4251/wjgo.v14.i5.1050
17. Pagliuca F, Ronchi A, Cozzolino I, Montella M, Zito Marino F, Franco R. Mesenchymal neoplasms: is it time for cytology? New perspectives for the pre-operative diagnosis of soft tissue tumors in the molecular era. Pathol Res Pract. 2020;216(6):152923. doi:10.1016/j.prp.2020.152923
18. Koyama T, Fletcher JG, Johnson CD, Kuo MS, Notohara K, Burgart LJ. Primary hepatic angiosarcoma: findings at CT and MR imaging. Radiology. 2002. 3: 667–673.
19. Zhou Y, Hou P, Wang F, Li B, Gao J. Primary hepatic malignant vascular tumors: a follow-up study of imaging characteristics and clinicopathological features. Cancer Imag. 2020;20(1). doi:10.1186/s40644-020-00336-9
20. Ronchi A, Cozzolino I, Zito Marino F. Primary and secondary cutaneous angiosarcoma: distinctive clinical, pathological and molecular features. Ann Diagn Pathol. 2020;48:151597. doi:10.1016/j.anndiagpath.2020.151597
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.