Back to Journals » Journal of Blood Medicine » Volume 13
Hematological Profile Changes Among Oral Contraceptive Users: A Narrative Review
Authors Tekle E ![]() , Gelaw Y
, Gelaw Y ![]() , Asrie F
, Asrie F
Received 4 July 2022
Accepted for publication 22 September 2022
Published 29 September 2022 Volume 2022:13 Pages 525—536
DOI https://doi.org/10.2147/JBM.S379841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Esayas Tekle,1 Yemataw Gelaw,2 Fikir Asrie2
1Department of Medical Laboratory Sciences, Institute of Health Sciences, Wallaga University, Nekemte, Ethiopia; 2Department of Hematology and Immunohematology, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Esayas Tekle, Email [email protected]
Abstract: Hematological profiles are measurable indices of blood that can be used to identify and monitor some pathological and physiological abnormalities. Oral contraceptives are one of the factors which may exert an influence on hematological laboratory test results and have a critical importance. Therefore, the main goal of this review was to evaluate the hematologic profile alterations brought on by the use of oral contraceptives. Accordingly, even though there were studies that showed no significant difference, most of the oral contraceptive users had higher hemoglobin, platelet, and erythrocyte counts than non-users. Other erythrocyte metrics, such as mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration and red cell dispersion width, did not significantly change. Moreover, leukocyte count and leukocyte differential count had no significant change among the oral contraceptive users in comparison to non-users. Oral contraceptive users typically have shorter prothrombin times, activated partial thromboplastin times, thrombin times, and greater levels of fibrinogen and D-dimer compared to non-users. However, this review is a narrative review and did not show the pooled effect of oral contraceptives on these hematological parameters. Therefore, it is recommended to do systematic and meta-analysis to determine the pooled effect of oral contraceptives.
Keywords: contraceptives, hematological parameters, hematopoiesis, hemostasis, oral contraceptives, thromboembolism
Introduction
Background
Hematological profiles are measurable indices of blood that can be used to identify and monitor some pathological and physiological abnormalities. Different illness situations that influence hematopoietic physiology and immunological responses can have an impact on these profiles,1,2 and they are frequently utilized in clinical settings in the medical field.3,4 These include parameters routinely given by complete blood count that gives a clue about erythrocyte count (EC), Mean corpuscular volume (MCV), Mean corpuscular hemoglobin concentration (MCHC), Mean corpuscular hemoglobin (MCH), Erythrocyte volume fraction (EVF), Hemoglobin (Hb) concentration and Red cell dispersion width (RDW).5
Hematological markers that have levels outside of normal ranges can be used to diagnose disorders like cancer, immunological diseases, and cardiovascular disease.6 For example, RDW, RBC parameter that measures the variability in the size of erythrocytes circulating in the blood circulation, is usually used for the differential diagnosis of hematological disorders7 including iron deficiency anemia (anemia that results when there is deficiency of iron for the production of erythrocytes), megaloblastic anemia, and thalassemia8,9 and a variety of other diseases, such as heart failure,5 atrial fibrillation,10 lung cancer11 or disorders characterized by inflammation.12 Hematocrit, more commonly known as the EVF, is a determinant of whole blood viscosity, the viscosity of which will affect peripheral resistance to blood flow, which will affect blood pressure.13 Red cell destruction due to RBCs’ reduction in deformability and an increase in cell size, high and low Hb levels are associated with cardiovascular risk.14
The second most frequent cell type, platelets are small anucleated cell fragments that are essential for maintaining vascular integrity and controlling hemostasis. In addition to their primary role in hemostasis, platelets are crucial in the defense against viral infections.15 The most important parameters related to platelet count include plateletcrit, Mean platelet volume (MPV) which is the measure of average size of platelets, and Platelet distribution width (PDW).4 The morphology of platelets changes as a result of their activation, and an increase in platelet swelling results in a rise in MPV and PDW.16 A more precise index of activation platelet is the distribution width of platelets, which represents the reactivity of the thrombocytes.17 In circumstances like hypertension, activation of thrombocytes is a risk factor for thrombotic disorders.18
White blood cells (WBC) are immune system cells that protect the body against external substances and infectious diseases. Similar to how RBCs and thrombocytes are created, they are all created in the bone marrow microenvironment from hematopoietic stem cells (HSC). These cells, called WBCs, can be seen all over the body, especially in the lymphatic and blood systems.18 Changes in WBC may indicate different disorders, including infection, inflammation, and hematological cancer.6
Coagulation tests encompassing Prothrombin time, Activated partial thromboplastin time (APTT), and fibrinogen are frequently used to evaluate coagulopathy and to guide hemostatic interventions.19,20 Additional tests can be performed to quantify the levels of particular coagulation factors, screen for inhibitors of particular coagulation factors, and evaluate the thrombin clotting time.20 Thrombin, activated factor XIII and plasmin work in sequence to create a D-dimer antigen, which is another coagulation parameter and a distinctive hallmark of fibrin breakdown. Its testing has primarily been used in clinical settings to rule out venous thromboembolism (VTE).21
The rise in fibrinolytic activity balances out the heightened coagulation activity, maintaining hemostatic equilibrium. However, thrombus formation can happen when there is local vascular endothelium damage or when other thromboembolism risk factors, such smoking and advanced age, combine. The little variations in coagulation factor levels among women using different oral contraceptive (OC) formulations may be significant in these circumstances.22
The laboratory results of hematological tests may be impacted by various conditions. Age, activity, bed rest, food ingestion, alcohol ingestion, menstrual cycle, obesity, posture, pregnancy, race, gender, smoking, and OC utilization are among factors that may influence laboratory results.23 The present review was designed to give a brief account of the studies carried out to elucidate the changes in hematological profiles linked to the usage of OCs.
Mechanism of Action of Oral Contraceptives on Hematopoiesis
Estrogen administration significantly increases the division and proliferation of HSCs and thus explains the higher blood counts in women during the reproductive years.24,25 High amounts of the estrogen receptor (ER) are expressed by HSCs, and estrogen/ERα signaling promotes self-renewal of HSC, HSC expansion and erythropoiesis.25
The use of hormonal contraceptives, which is generally associated with lighter menstrual periods, is associated with better indicators of iron status indicators.26–29 Poorer iron status indicators (low levels of serum ferritin and Hb) have been linked to menstrual blood loss.27,30,31 Serum iron levels have been shown to be higher among OC users.29,32 The endometrium shrinks as a result of progestogenic tablets’ endometrial atrophy, and their usage results in scanty withdrawal bleeding that is less than in a typical cycle. This is the first factor that is assumed to be the cause of elevated blood iron content.33
Additionally, OCs improve gut absorption of iron34 and were known to increase biomarkers of tissue iron stores (serum ferritin) thus lowering the risk of developing anemia.26,35,36 The OC pill increases serum ferritin, therefore improves the body’s iron status.37,38 Oral contraceptives enhanced inflammatory-driven increases in ferritin while decreasing the frequency and volume of menstrual bleeding.39 As a result, the usage of OCs may be linked to an improvement in Hb status, enhancing the health of low-socioeconomic-class women.40
Oral contraceptive decreases intestinal re-absorption of folate and vitamin B-12 which resulted in significantly decreased serum levels of these vitamins in women taking OC pills, even when controlling for intake through diet, and may end up in megaloblastic anemia.41–44
Mechanism of Action of Oral Contraceptives on Hemostasis System
With enhanced procoagulant effects, decreased anticoagulant effects, and equivocal effects on fibrinolysis, oral contraceptives have a net prothrombotic impact (with increases in the activity of the antifibrinolytic system).45 The biologic, unifying mechanism underlying the thrombotic effects of OC pills is still unclear, despite the fact that individual alterations in procoagulants and anticoagulants with OC pill usage are widely characterized.46
Procoagulant Effects
Oral contraceptives increase adenosine diphosphate, which causes fibrinogen binding and platelet aggregation.47 They also cause a noticeable and long-lasting increase in the synthesis of cell membrane lipids.48 An increased synthesis can have a significant influence on hemostatic physiology since platelet membrane lipids are crucial pro-coagulant factors in hemostasis.49 There have also been reports of increased endothelial replication of endothelial cells and increased endothelial synthesis of the Von Willebrand factor (VWF).50 This may also explain why platelets stick to vascular endothelium more readily and why thrombosis is more likely to occur.
Estrogen is linked to a variety of prothrombotic pathways that modify coagulation proteins and tip the hemostatic scales in favor of a prothrombotic state. Increased levels of factors II, VII, VIII, X, and fibrinogen, reduced levels of protein S and Antithrombin (AT), and activated protein C resistance are some of these changes. The PT and APTT may become shorter as a result of these modifications.51
Prothrombin, factor VII, factor VIII, factor X, fibrinogen, and prothrombin fragment 1+2 levels rise while factor V levels fall during the use of OCs, according to a recent randomized, crossover research. It is now understood that prothrombin52 and factor VIII53 concentrations which are somewhat elevated are linked to a more risk of venous thrombosis. Since factor V may exhibit anticoagulant activity because of its ability to act as a cofactor in the inactivation of activated factor VIII that is mediated by activated protein C; a reduction in the level of factor V may contribute to the thrombotic side effects of OCs.54
Fibrinolytic Effects
The usage of OCs is indicated to increase fibrinolytic activity through changes in fibrinolytic variables such as plasminogen, tissue plasminogen activator (T-PA), Plasminogen activator inhibitor type 1 (PAI-1), and plasmin-antiplasmin complexes.55,56 Tissue plasminogen activator levels are raised and PAI-1 levels are decreased by COCs, which has an impact on fibrinolysis. Higher levels of Thrombin activatable fibrinolysis inhibitor (TAFI) in women taking COCs appear to counterbalance these effects, though.56
Because of the lack of evidence linking alterations in the fibrinolytic system to an elevated risk of venous thrombosis, it is unknown if alterations in fibrinolytic activity during OC usage has therapeutic consequences. The TAFI, which when activated prevents fibrinolysis by removing from fibrin the lysine residues necessary for the binding and activation of plasminogen, is one antifibrinolytic mechanism.57 Venous thrombosis is at increased risk due to elevated TAFI levels.58
The total clot-lysis time was shown to be unaffected by OC usage in an assay for clot lyses that measured the activity of both the fibrinolytic system and the TAFI dependent antifibrinolytic pathway. This data implies that the increased fibrinolytic potential caused by the use of OCs is offset by the TAFI system’s enhanced down-regulation of fibrinolysis. Increased TAFI levels and improved thrombin (the activator of TAFI) synthesis are most likely responsible for the increased TAFI-dependent inhibition of fibrinolysis.39
Change in Blood Cells and Blood Cell Parameters Among Oral Contraceptive Users
Red Blood Cell Parameters
To make sure the tissues receive a proper amount of oxygen, the red cell volume must be maintained. Erythropoietin primarily regulates the process that links red cell synthesis with tissue oxygen supply. The creation of Hb, a specialized protein necessary for delivering oxygen within the red cell, is a prerequisite for the formation of functioning RBCs. As the erythroid precursor cells develop, this protein is produced more and more. Iron atoms from heme molecules are introduced into globin to form it.59 Recycled iron from the Hb of dying erythrocytes is used to maintain the Hb level, and when necessary, iron from the reticuloendothelial storage is also used. The main protein that stores iron is called ferritin, and the concentration of ferritin in the blood is a reliable predictor of the quantity of stored iron. In plasma, the carrier molecule transferrin is linked to iron.59
RBC count60 and Hb concentration rise as a result of OCs.30,61 The decrease in menstrual blood loss, which is known to be frequent among OC users, may be to blame for the rise in RBC count.26,30,34,36,62–64 Menstrual blood loss has been linked to worse iron status markers.27,30,31 Likewise, the use of hormonal contraceptives is linked to better markers of iron status and is frequently related with lighter menstrual cycles.26–29 According to reports, OC users had higher serum iron levels.29,32 Progestogenic medications promote endometrial shrinkage and generate scanty withdrawal bleeding that is less than in a typical cycle, which is the first reason hypothesized to be the cause of elevated serum iron content.33
Additionally, OCs have a tendency to boost gastrointestinal absorption of iron34 and they are known to raise tissue iron reserves’ biomarkers, which decreases the likelihood of developing anemia.26,35,36 Higher ferritin levels in OC users are a positive biomarker impact. Reduced menstrual bleeding frequency and volume, as well as increases in ferritin brought on by inflammation, are two reasons why there may be increased levels of ferritin.39
However, several investigations revealed no discernible alteration in RBC count, EVF,60,65,66 and Hb values.46,60,66 Ended, there was also a contradictive study that showed a decrement in RBC count among OC users compared to non-users.63 However, the change in other RBC characteristics such MCV, MCH, MCHC, and RDW was not significantly impacted by the change in RBC count.60 Also a study by66 showed no difference in MCV, MCH, and MCHC between the groups who were using OCs and those who were not using (Table 1).
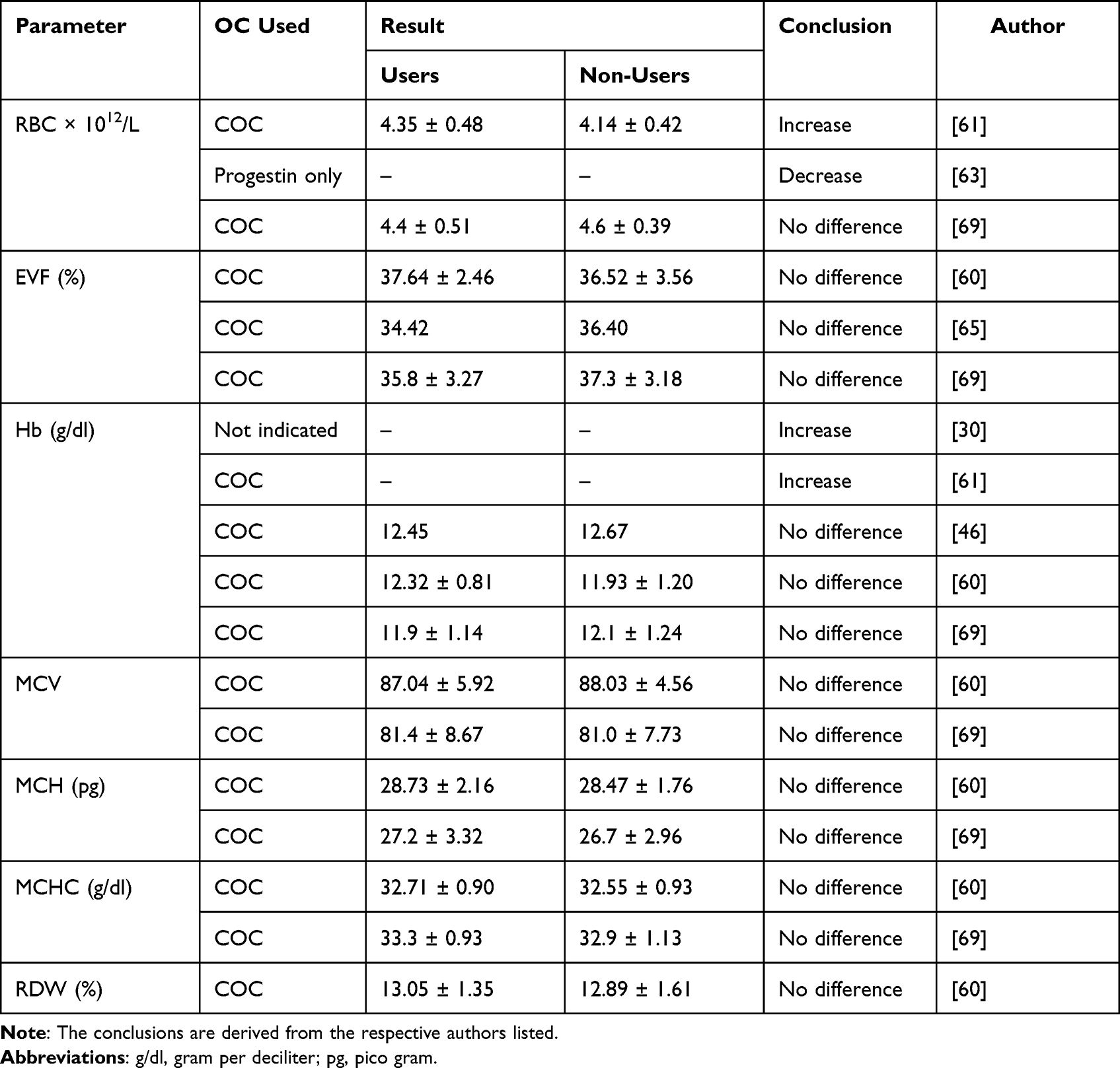 |
Table 1 Changes in Red Blood Cell Parameters Among Oral Contraceptive Users |
Platelet Parameters
Circulating platelets, coagulation factors, the endothelium of the blood vessel wall, naturally occurring anticoagulants (such protein C, protein S, and AT), and fibrinolysis (clot digestion) all interact to regulate hemostasis.59 The platelet count assesses if there are enough platelets to achieve early hemostasis. There is a typical range of 150,000 to 450,000 platelets.67
Use of OCs raises platelet count.65,67 The increase in the number of platelets may be explained by the fact that estrogen administration significantly increases the division and proliferation of HSCs in women during the reproductive years.24,25 Additionally, PLT count46,60,66,68,69 and MPV66 among OC users were observed to have remained stable. The lack of substantial alterations might be attributable to the use of smaller sample sizes or the short duration of OC usage, which might not have produced differences in these parameters (Table 2).
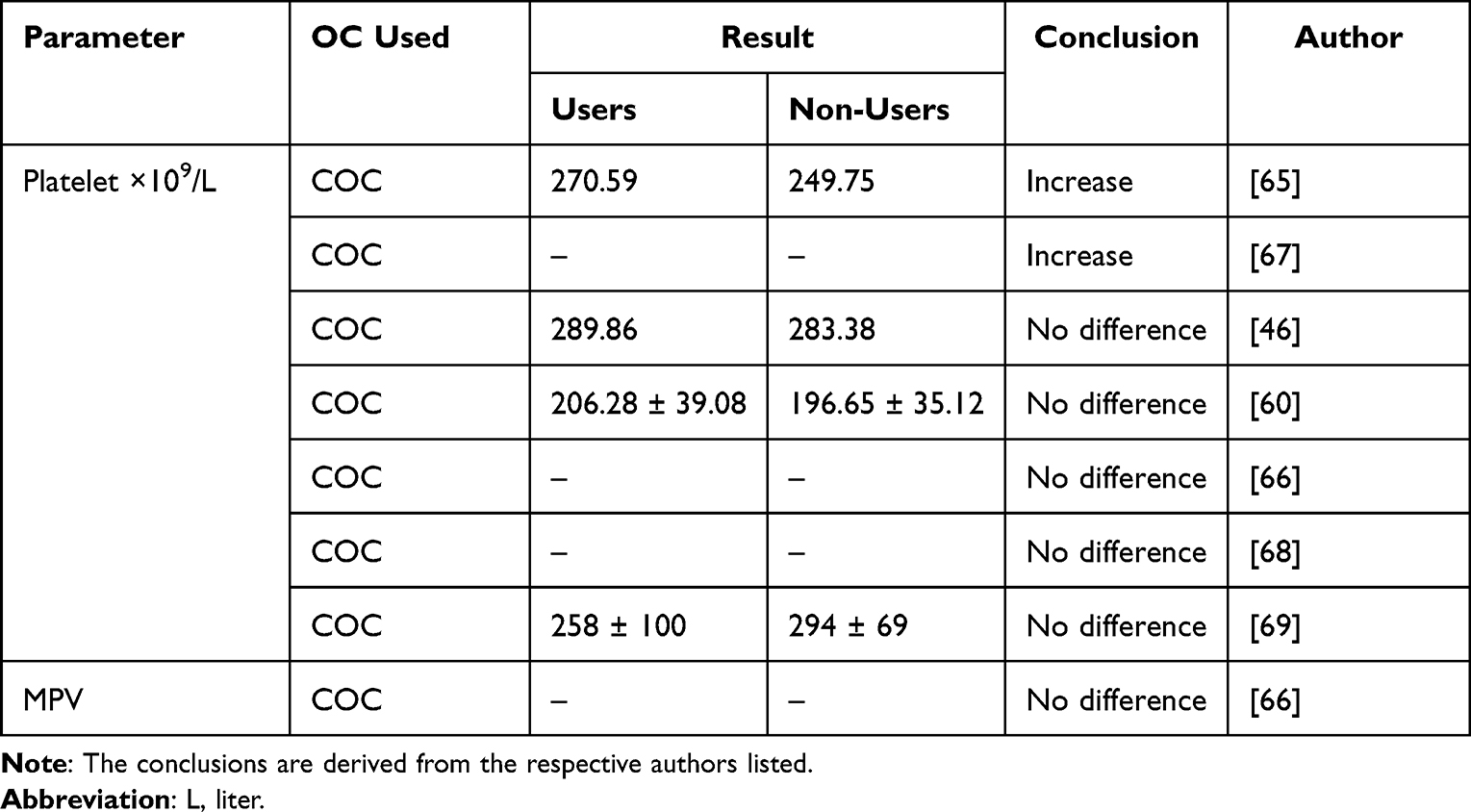 |
Table 2 Changes in Platelet Parameters Among Oral Contraceptive Users |
White Blood Cell Parameters
White blood cells, also referred as leukocytes, are the body’s defense against infection. Depending on the presence or lack of granules in the cell cytoplasm, they can be generically categorized as granulocytes or agranulocytes. Neutrophils (polymorphs), eosinophils, and basophils are examples of granulocytes. Monocytes and lymphocytes are examples of circulating agranulocytes. By phagocytosing pathogens, neutrophils and monocytes have a crucial part in the defense against acute bacterial infections. Lymphocytes help phagocytes by generating a regulated immune response.59
Regarding their count, there was no difference between OC users and non-users in WBC.46,60,65,66 Additionally, there was no discernible difference between users and non-users in the WBC differential count, which includes LYM, MON, NEU, EOS, and BAS percentages60 (Table 3).
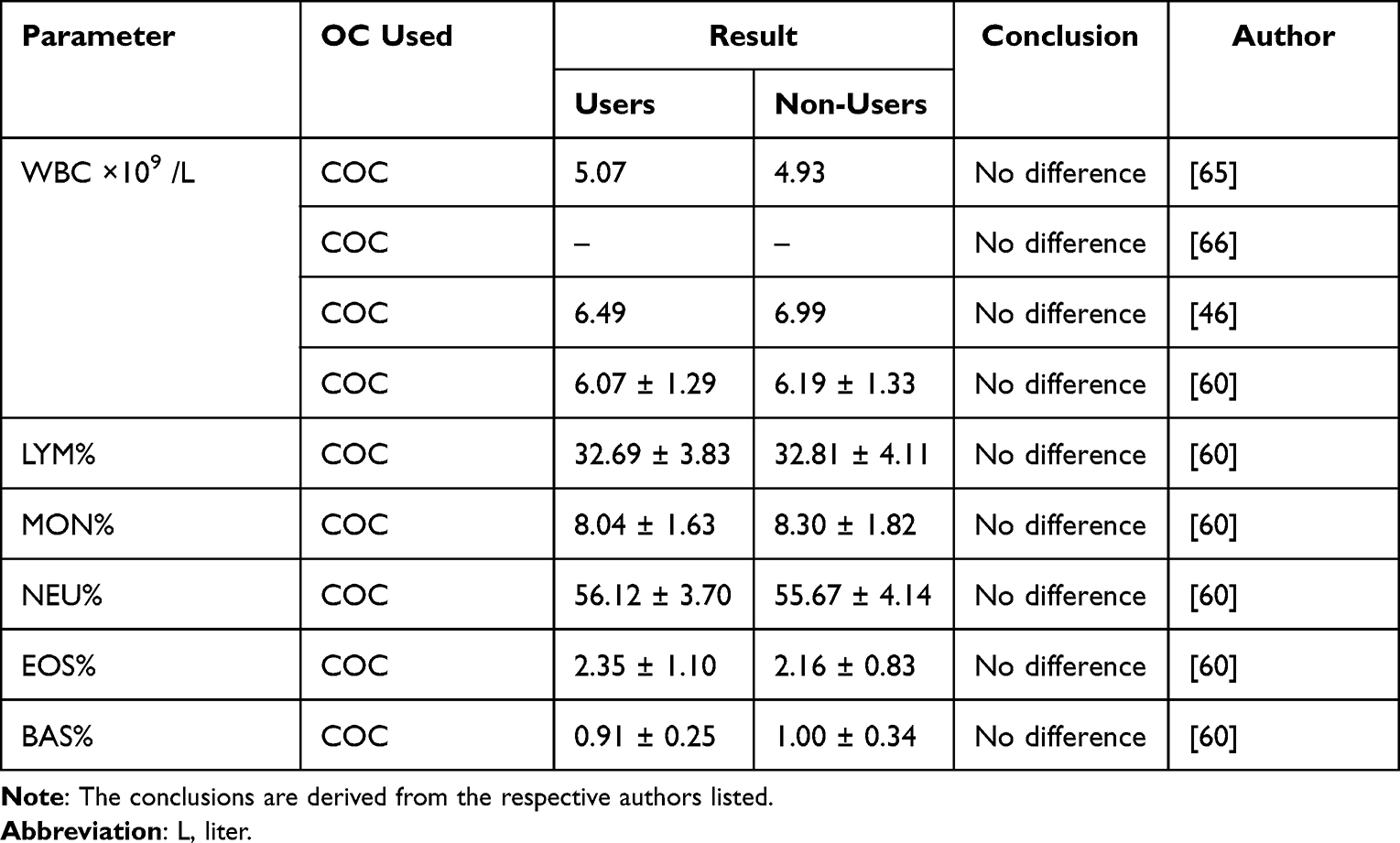 |
Table 3 Changes in White Blood Cell Parameters Among Oral Contraceptive Users |
Changes in Coagulation Profiles Among Oral Contraceptive Users
Platelets collect on the blood vessel endothelium as a result of vascular injury, and a group of coagulation factors designated by their roman numbers are activated. Von Willebrand factor serves as a carrier of factor VIII and promotes platelet interaction with the exposed endothelium. The final step in the coagulation pathway’s activation is thrombin’s conversion of fibrinogen into a fibrin gel. A sophisticated network of activating and feedback processes makes sure that proteases are formed to both activate and degrade the coagulation factors, avoiding the development of large-scale clots.59
The fibrinolytic system, which is made up of the proenzyme plasminogen and its related activators and inhibitors, regulates the removal of fibrin. The tissue protease, T-PA, which is triggered concurrently with the initiation of the coagulation process, is the primary activator of plasminogen. The fibrinolytic system’s final step is plasmin, which breaks down fibrin and fibrinogen into degradation products (FDPs) such fibrinopeptide A and D-dimer. Plasminogen activator inhibitor-1 is a potent inhibitor of T-PA and is mostly generated by endothelial cells.59
The liver produces proteins C and S, which are physiological anticoagulants that depend on vitamin K. Through the neutralization of active coagulation factors V and VIII, they work as one of the primary regulators of hemostasis. Congenital or acquired protein C or S deficiency are both possible.70 A glycoprotein called antithrombin predominantly inhibits thrombin while also inhibiting a number of activated coagulation proteins.71
Several investigations were made to clarify the effects of OCs on blood coagulation72,73 and it is important to emphasize here the changes to the coagulation profile brought on by using these drugs.
Fibrinogen
Fibrinogen level increases among users of OCs.46,65,67,74,75 The increase may be because of the effect of the estrogen hormone. The hormone has been reported to increase the level of various coagulation proteins including fibrinogen.51 On the contrary, fibrinogen level in OC pill users was found to be similar to non-users among Chinese women.76,77
Activated Partial Thromboplastin Time
A test called activated partial thromboplastin time is used to check for anomalies in the intrinsic and general clotting systems as well as to track how well circulating heparin is preventing clotting. It assesses the activity of factors from the intrinsic and common pathways, including factors I, II, V, VIII, IX, X, and XI.78
Shorter APTT has been demonstrated among users of OC.65,69,73,75,79 Shorter APTTs may occur with the administration of OCs if one or more of the clotting factors, including as prothrombin, factor VIII, factor X, fibrinogen, and prothrombin fragment 1+2, as well as due to decreases in the levels of protein S, AT, and activated protein C resistance.22,50,80 Few studies, meanwhile, claimed that there was no discernible difference in APTT levels between people who used and did not use OC.46,67,76
Prothrombin Time
The extrinsic and common coagulation pathways are tested in the laboratory using the prothrombin time. It is the amount of time needed for platelet-poor plasma to clot after calcium, phospholipid, and tissue factor have been added. The component that is “extrinsic” to the plasma-based coagulation mechanism is the tissue factor. Patients on warfarin for anticoagulation may experience isolated prolongations of the PT due to factor VII insufficiency, fibrinogen abnormalities, or both. It is also regarded as the most accurate screening method for coagulopathies caused by malfunction of the liver.81
Shortening of the PT46,65,67,73,75 has been demonstrated in OC users. Increases in the levels of activity of one of the clotting factors including prothrombin, factor VII, factor X, fibrinogen, and prothrombin fragment 1+2 and decreases in the levels of factor V, AT, protein S, and activated protein C resistance during the use of OCs might cause shorter PT.22,51 However, the PT of OC users resulted in no difference from the non-users according to other studies.69,76,77,79
Thrombin Time
The term “thrombin time” (TT) refers to the amount of time needed for fibrin to polymerize into a solid clot when thrombin is present.6 It mostly reflects the fibrinogen concentration. However, it also reflects the fibrinopeptides’ cleavability and fibrinogen’s polymerization.82 When fibrinogen levels are low, fibrinogen is dysfunctional, or thrombin inhibitors such heparin or fibrin-split products are present, the TT is extended but remains normal in individuals with abnormalities in the intrinsic or extrinsic route.20
Shortening of the TT has been reported among women that were using OCs.65,67,75,77 The shortening of TT maybe because of the increase in the concentration of fibrinogen among OC users.51,80,82
D-Dimer
The D-dimer antigen, a characteristic biological indicator of fibrin breakdown, is produced by the sequential activities of the enzymes thrombin, activated factor XIII, and plasmin.21 Oral pill users were shown to have considerably higher D-dimer levels than non-users.65,79,83 The enhanced fibrinolytic activity that prevents excessive fibrin deposition inside the vascular channels and its obstructive effects is reflected in the higher plasma D-dimer level. As independently reported by Winkler and Meijers et al, the enhanced fibrinolysis thereby physiologically counteracts the hypercoagulable condition and maintains normal circulation55,56 (Table 4).
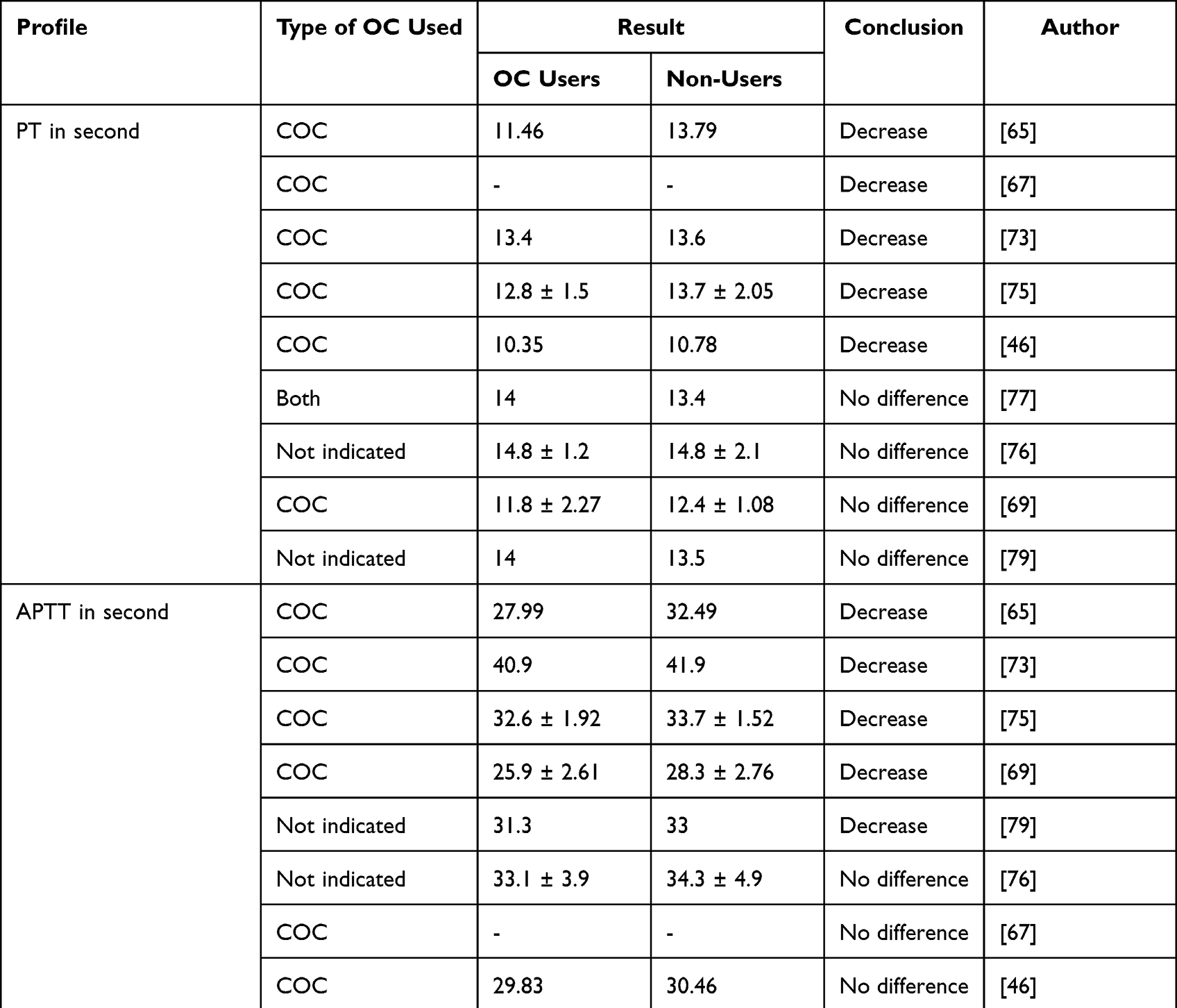 |
Table 4 Changes in Coagulation Profile Among Oral Contraceptive Users |
Oral Contraceptive Use Associated Coagulation Disorders
Women on combined OCs have consistently noted changes in blood coagulation that may be the cause of their elevated risk of thromboembolic illness.73 The balance of hemostasis is impacted by estrogen, and its usage as Combination oral contraceptives5 are linked to an increased risk of arterial thrombosis52 and a greater risk of VTE, however the exact risk is uncertain.84,85
The risk of VTE may vary across different OCs due to the progestin component.84 The risk of thrombosis was increased more among users of OCs containing third-generation progestin, drospirenone, and cyproterone acetate than in users of second-generation tablets.85 It is essential to comprehend that women utilizing COCs run the chance of developing VTE if there is a family history of the condition.86 The risk of venous thrombosis decreases in COC users with sustained use and reduced estrogen dose. Progestogen-only drugs were not associated with an increased risk of venous thrombosis.81,87
Conclusion
Despite studies that found no difference to be statistically significant, most OC users had higher Hb, PLT, and RBC counts than non-users did. However, other RBC characteristics as MCV, MCH, MCHC, and RDW showed no obvious difference. Moreover, WBC and its differential count had no significant change among the OC users in comparison to non-users.
In contrast to non-users, OC users’ coagulation states, measured through tests including PT, APTT, and TT, were shortened, and their levels of fibrinogen and D-dimer tended to rise. An increase in coagulation proteins and a decrease in anticoagulant proteins may be the cause. These might increase the risk of thrombosis among OC users. When pre-exposure variables such as family history of VTE exist, the thrombotic risks might be further increased. Since VTE runs in families, caution should be used while giving these OCs to patients.
Oral contraceptives had a substantial impact on the hematological profile, particularly RBC count, platelet count, Hb, and coagulation states including APTT, PT, TT, fibrinogen, and D-dimer levels, albeit results were not consistent across studies. As a narrative review, our analysis did not demonstrate the pooled impact of OCs on these hematological parameters. Therefore, systematic and meta-analysis are advised to ascertain the combined impact of OCs.
Abbreviations
APTT, Activated Partial Thromboplastin Time; AT, Antithrombin; COC, Combined Oral Contraceptive; EC, Erythrocyte count; ERα, Estrogen Receptor-α, EVF, Erythrocyte Volume Fraction; Hb, Haemoglobin; HSC, Hematopoietic Stem Cell; MPV, Mean Platelet Volume; MCH, Mean Corpuscular Hemoglobin; MCHC, Mean Corpuscular Hemoglobin Concentration; MCV, Mean Corpuscular Volume; OC, Oral Contraceptive; PAI-1, Plasminogen Activator Inhibitor Type-1; PDW, Platelet Distribution Width; TAFI; Thrombin Activatable Fibrinolysis Inhibitor; PT, Prothrombin Time; TT, Thrombin Time; T-PA, Tissue Plasminogen Activator; RBC, Red Blood Cell; RDW, Red Cell Dispersion Width; VTE, Venous Thromboembolism; VWF, Von Willbrand Factor; WBC, White Blood Cell.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fahy JV. Eosinophilic and neutrophilic inflammation in asthma: insights from clinical studies. Proc Am Thorac Soc. 2009;6(3):256–259. doi:10.1513/pats.200808-087RM
2. Kelly FJ, Fussell JC. Air pollution and airway disease. Clin Exp Allergy. 2011;41(8):1059–1071. doi:10.1111/j.1365-2222.2011.03776.x
3. Kelada SN, Aylor DL, Peck BC, et al. Genetic analysis of hematological parameters in incipient lines of the collaborative cross. Genes Genomes Genet. 2012;2(2):157–165. doi:10.1534/g3.111.001776
4. Wiwanitkit V. Plateletcrit, mean platelet volume, platelet distribution width: its expected values and correlation with parallel red blood cell parameters. Clin Appl Thromb Hemost. 2004;10(2):175–178. doi:10.1177/107602960401000208
5. Felker GM, Allen LA, Pocock SJ, et al. Red cell distribution width as a novel prognostic marker in heart failure: data from the CHARM Program and the Duke Databank. J Am Coll Cardiol. 2007;50(1):40–47. doi:10.1016/j.jacc.2007.02.067
6. Evans DM, Frazer IH, Martin NG. Genetic and environmental causes of variation in basal levels of blood cells. Twin Res Hum Genet. 1999;2(4):250–257. doi:10.1375/twin.2.4.250
7. Karabulut A, Uzunlar B. Correlation between red cell distribution width and coronary ectasia in the acute myocardial infarction. Clin Appl Thromb Hemost. 2012;18(5):551–552. doi:10.1177/1076029611436198
8. Montagnana M, Cervellin G, Meschi T, Lippi G. The role of red blood cell distribution width in cardiovascular and thrombotic disorders. Clin Chem Lab Med. 2012;50(4):635–641. doi:10.1515/cclm.2011.831
9. Bessman JD, Gilmer PR, Gardner FH. Improved classification of anemias by MCV and RDW. Am J Clin Pathol. 1983;80(3):322–326. doi:10.1093/ajcp/80.3.322
10. Adamsson Eryd S, Borné Y, Melander O, et al. Red blood cell distribution width is associated with incidence of atrial fibrillation. J Intern Med. 2014;275(1):84–92. doi:10.1111/joim.12143
11. Koma Y, Onishi A, Matsuoka H, et al. Increased red blood cell distribution width associates with cancer stage and prognosis in patients with lung cancer. PLoS One. 2013;8(11):e80240. doi:10.1371/journal.pone.0080240
12. Song CS, Park DI, Yoon MY, et al. Association between red cell distribution width and disease activity in patients with inflammatory bowel disease. Dig Dis Sci. 2012;57(4):1033–1038. doi:10.1007/s10620-011-1978-2
13. Rampling M. Haemorheological disturbances in hypertension: the influence of diabetes and smoking. Clin Hemorheol Microcirc. 1999;21(3–4):183–187.
14. Enawgaw B, Adane N, Terefe B, Asrie F, Melku M. A comparative cross-sectional study of some hematological parameters of hypertensive and normotensive individuals at the university of Gondar hospital, Northwest Ethiopia. BMC Hematol. 2017;17(1):1–7. doi:10.1186/s12878-017-0093-9
15. Seyoum M, Enawgaw B, Melku M. Human blood platelets and viruses: defense mechanism and role in the removal of viral pathogens. Thromb J. 2018;16(1):1–6. doi:10.1186/s12959-018-0170-8
16. Boos CJ, Lip GY. Assessment of mean platelet volume in coronary artery disease—what does it mean? Thromb Res. 2007;120(1):11–13. doi:10.1016/j.thromres.2006.09.002
17. Sahan E, Polat S. Neutrophil to lymphocyte ratio is associated with more extensive, severe and complex coronary artery disease and impaired myocardial perfusion. Turk Kardiyol Dern Ars. 2014;42(4):415. doi:10.5543/tkda.2014.87036
18. Maton A. Human Biology and Health. Prentice Hall; 1997.
19. Haas T, Fries D, Tanaka K, Asmis L, Curry N, Schöchl H. Usefulness of standard plasma coagulation tests in the management of perioperative coagulopathic bleeding: is there any evidence? Br J Anaesth. 2015;114(2):217–224. doi:10.1093/bja/aeu303
20. Greaves M, Preston FE. Approach to the bleeding patient. In: Colman H, Marder C, editors. Haemostasis and Thrombosis: Basic Principles and Clinical Practice. George Lippincott Williams and Wilkins; 2001.
21. Adam SS, Key NS, Greenberg CS. D-dimer antigen: current concepts and future prospects. Blood. 2009;113(13):2878–2887.
22. David SL, George MS. Estrogen and progestins. In: Laurence LB, editor. Goodman & Gillman’s the Pharmacological Basis for Therapeutics.
23. Clinical and Laboratory Standards Institute (NCCLS). Procedures for the Collection of Diagnostic Blood Specimens by Venipuncture; Approved Standard, NCCLS Document H3-A5 (ISBN 1-56238-515-1).
24. Egbunah M, Eze E, Ebirien-Agana B, Jeremiah Z. Haematological profiles of women on some contraceptives in selected family planning clinics in Kaduna State, Nigeria. J Med Sci Clin Res. 2018;6(12):73–84.
25. Nakada D, Oguro H, Levi BP, et al. Oestrogen increases haematopoietic stem-cell self-renewal in females and during pregnancy. Nature. 2014;505(7484):555–558. doi:10.1038/nature12932
26. Milman N, Kirchhoff M, Jørgensen T. Iron status markers, serum ferritin and hemoglobin in 1359 Danish women in relation to menstruation, hormonal contraception, parity, and postmenopausal hormone treatment. Ann Hematol. 1992;65(2):96–102. doi:10.1007/BF01698138
27. Milman N, Rosdahl N, Lyhne N, Jørgensen T, Graudal N. Iron status in Danish women aged 35–65 years: relation to menstruation and method of contraception. Acta Obstet Gynecol Scand. 1993;72(8):601–605. doi:10.3109/00016349309021150
28. Prasad AS, Oberleas D, Moghissi K, Lei K, Stryker JC. Effect of oral contraceptive agents on nutrients: i. Minerals. Am J Clin Nutr. 1975;28(4):377–384. doi:10.1093/ajcn/28.4.377
29. Burton J. Effect of oral contraceptives on haemoglobin, packed-cell volume, serum-iron, and total iron-binding capacity in healthy women. Lancet. 1967;289(7497):978–980. doi:10.1016/S0140-6736(67)92359-8
30. Milman N, Clausen J, Byg K-E. Iron status in 268 Danish women aged 18–30 years: influence of menstruation, contraceptive method, and iron supplementation. Ann Hematol. 1998;77(1):13–19. doi:10.1007/s002770050405
31. Beard JL. Iron requirements in adolescent females. J Nutr. 2000;130(2):440S–442S. doi:10.1093/jn/130.2.440S
32. Briggs M, Briggs M. Contraceptives and serum proteins. Br Med J. 1970;3(5721):521. doi:10.1136/bmj.3.5721.521-a
33. Grant EC. Hormone balance of oral contraceptives. BJOG. 1967;74(6):908–918. doi:10.1111/j.1471-0528.1967.tb15578.x
34. Margen S, King JC. Effect of oral contraceptive agents on the metabolism of some trace minerals. Am J Clin Nutr. 1975;28(4):392–402. doi:10.1093/ajcn/28.4.392
35. Massé PG, Andrée G. Long-term effect of low-dose combined steroid contraceptives on body iron status. Contraception. 1992;46(3):243–252. doi:10.1016/0010-7824(92)90005-E
36. Frassinelli-Gunderson EP, Margen S, Brown JR. Iron stores in users of oral contraceptive agents. Am J Clin Nutr. 1985;41(4):703–712. doi:10.1093/ajcn/41.4.703
37. Yeasmin T, Haque MS, Yeasmin S, Amin MR. Iron status in women using oral contraceptives. Bangladesh J Physiol Pharmacol. 2010;26(1–2):25–29. doi:10.3329/bjpp.v26i1-2.19963
38. Davis A, Godwin A, Lippman J, Olson W, Kafrissen M. Triphasic norgestimate-ethinyl estradiol for treating dysfunctional uterine bleeding. Obstet Gynecol. 2000;96(6):913–920.
39. Sim M, Dawson B, Landers G, Trinder D, Peeling P. Iron regulation in athletes: exploring the menstrual cycle and effects of different exercise modalities on hepcidin production. Int J Sport Nutr Exerc Metab. 2014;24(2):177–187. doi:10.1123/ijsnem.2013-0067
40. Prema K. Haemoglobin levels in contraceptive users. Indian J Med Res. 1979;69:756–760.
41. McArthur JO, Tang H, Petocz P, Samman S. Biological variability and impact of oral contraceptives on vitamins B6, B12 and folate status in women of reproductive age. Nutrients. 2013;5(9):3634–3645. doi:10.3390/nu5093634
42. Wakeman MP. A review of the effects of oral contraceptives on nutrient status, with especial consideration to folate in UK. J Adv Med Med Res. 2019;1–17. doi:10.9734/jammr/2019/v30i230168
43. Shere M, Bapat P, Nickel C, Kapur B, Koren G. Association between use of oral contraceptives and folate status: a systematic review and meta-analysis. J Obstet Gynaecol Can. 2015;37(5):430–438. doi:10.1016/S1701-2163(15)30258-9
44. Berenson AB, Rahman M. Effect of hormonal contraceptives on vitamin B12 level and the association of the latter with bone mineral density. Contraception. 2012;86(5):481–487. doi:10.1016/j.contraception.2012.02.015
45. Kuhl H, März W, Jung-Hoffmann C, Heidt F, Gross W. Time-dependent alterations in lipid metabolism during treatment with low-dose oral contraceptives. Am J Obstet Gynecol. 1990;163(1):363–369. doi:10.1016/0002-9378(90)90583-S
46. Zia A, Callaghan MU, Callaghan JH, et al. Hypercoagulability in adolescent girls on oral contraceptives‐global coagulation profile and estrogen receptor polymorphisms. Am J Hematol. 2015;90(8):725–731. doi:10.1002/ajh.24064
47. McGregor L, Toor B, McGregor J, Renaud S, Clemetson K. Effects of oral contraceptives, or lanosterol, on ADP-induced aggregation and binding of 125I-fibrinogen to rat platelets. Thromb Res. 1984;33(5):517–522. doi:10.1016/0049-3848(84)90017-3
48. Ciavatti M, Davenas E, Blache D, Monnier MA, Renaud S. Biosynthesis of platelet lipids in relation to aggregation in women using oral contraceptives. Contraception. 1982;25(6):629–638. doi:10.1016/0010-7824(82)90064-6
49. O’Donnell CJ, Larson MG, Feng D, et al. Genetic and environmental contributions to platelet aggregation: the Framingham heart study. Circulation. 2001;103(25):3051–3056. doi:10.1161/01.CIR.103.25.3051
50. Harrison R, McKee P. Estrogen stimulates von Willebrand factor production by cultured. Blood. 1984;63(3):657–665. doi:10.1182/blood.V63.3.657.657
51. Kenneth AB, Gregory YH. Overview of the causes of VTE- oral and transdermal contraceptives. Available from: http://www.update.com/content/overviewofvenousthrombosis.
52. Poort S, Rosendaal F, Reitsma P, Bertina R. A common genetic variation in the 3’-untranslated region of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase in venous thrombosis. Blood. 1996;88(10):3698–3703. doi:10.1182/blood.V88.10.3698.bloodjournal88103698
53. Kraaijenhagen RA, Koopman MM, Reitsma PH, Prins MH, van den Ende A, Büller HR. High plasma concentration of factor VIIIc is a major risk factor for venous thromboembolism. Thromb Haemost. 2000;83(01):5–9. doi:10.1055/s-0037-1613747
54. Shen L, Dahlbäck B. Factor V and protein S as synergistic cofactors to activated protein C in degradation of factor VIIIa. J Biol Chem. 1994;269(29):18735–18738. doi:10.1016/S0021-9258(17)32228-7
55. Winkler UH. Blood coagulation and oral contraceptives: a critical review. Contraception. 1998;57(3):203–209. doi:10.1016/S0010-7824(98)00020-1
56. Meijers JC, Middeldorp S, Tekelenburg W, et al. Increased fibrinolytic activity during use of oral contraceptives is counteracted by an enhanced factor XI-independent down regulation of fibrinolysis. Thromb Haemost. 2000;84(07):9–14. doi:10.1055/s-0037-1613959
57. Bajzar L, Manuel R, Nesheim ME. Purification and characterization of TAFI, a thrombin-activable fibrinolysis inhibitor. J Biol Chem. 1995;270(24):14477–14484. doi:10.1074/jbc.270.24.14477
58. van Tilburg NH, Rosendaal FR, Bertina RM. Thrombin activatable fibrinolysis inhibitor and the risk for deep vein thrombosis. Blood. 2000;95(9):2855–2859.
59. Evans K, Amenhotep Z, Dawson D, Waters H, Ardern J. Chapter 9.11 - Hematology. In: Wild D, editor. The Immunoassay Handbook.
60. Coffie S, Abaka-Yawson A, Quarshie SS, et al. Effects of hormonal contraceptives on haematological parameters among women in the cape coast metropolis, Ghana. Asian Hematol Res J. 2020;3(1):1–9.
61. Bathija H, Lei Z, Cheng X, et al. Effects of contraceptives on hemoglobin and ferritin. Contraception. 1998;58(5):261–273.
62. Buchan PC, MacDonald HN. Altered haemorheology in oral-contraceptive users. Br Med J. 1980;280(6219):978–979. doi:10.1136/bmj.280.6219.978
63. Afsar NA, Barakzai Q, Adil SN. Effect of A ‘Progestin Only’Contraceptive on platelet aggregation in a Pakistani set of population. J Ayub Med Coll Abbottabad. 2005;17(3):1–6.
64. Akinloye O, Adebayo T, Oguntibeju OO, Oparinde D, Ogunyemi E. Effects of contraceptives on serum trace elements, calcium and phosphorus levels. West Indian Med J. 2011;60(3):308–315.
65. Abubakar SB. Some haemostatic changes in women on hormonal contraceptives attending family planning clinic at Ahmadu Bello University Teaching Hospital Shika-Zaria, Nigeria. Faculty of Internal Medicine; 2013.
66. Bulur S, Albayrak M, Keskin F, et al. Effect of combined oral contraceptive use on platelet volume in women at reproductive age. Clin Exp Obstet Gynecol. 2012;39(3):314–316.
67. Babatunde A, Olatunji P. Short-term effect of oral contraceptive pills on some haemostatic parameters in healthy Nigerian women. Niger Postgrad Med J. 2004;11(4):246–250.
68. Joseph J, Abdulazeez A, Obisesan O. Effect of hormonal contraceptives on some haemostatics parameters in women attending family planning clinics in Jos, Nigeria. Niger J Health Biomed Sci. 2008;7(1):15–18. doi:10.4314/njhbs.v7i1.11656
69. Afsar NA, Barakzai Q, Adil SN. Effect of low dose oral pill on haemostatic parameters in a set of Pakistani population. J Pak Med Assoc. 2008;58(5):229.
70. Stegnar M. Thrombophilia screening--at the right time, for the right patient, with a good reason. Clin Chem Lab Med. 2010;48:S105–S13. doi:10.1515/CCLM.2010.367
71. Jennings I, Cooper P. Screening for thrombophilia: a laboratory perspective. Br J Biomed Sci. 2003;60(1):39–51. doi:10.1080/09674845.2003.11783675
72. Inman W, Vessey M, Westerholm B, Engelund A. Thromboembolic disease and the steroidal content of oral contraceptives. A report to the Committee on Safety of Drugs. Br Med J. 1970;2(5703):203–209. doi:10.1136/bmj.2.5703.203
73. Leck I, Thomson J, Bocaz J, et al. A multicentre study of coagulation and haemostatic variables during oral contraception: variations with geographical location and ethnicity. Int J Epidemiol. 1991;20(4):913–920. doi:10.1093/ije/20.4.913
74. Famodu A. Serial changes in plasma fibrinogen concentration and fibrinolytic activity in African women on oral contraceptive pills. Afr J Reprod Health. 1997;1(2):90–95. doi:10.2307/3583380
75. Sirhindi GA, Tayyib M, Tasneem T, Farooq M, Chaudhary NA. Fibrinogen degradation products and coagulation parameters in women taking oral contraceptives. Ann King Edw Med Univ. 2003;9(3). doi:10.21649/akemu.v9i3.1331
76. Chan P, Yeh CJ, Pan WH. Influence of contraceptive pill use, premenopause and postmenopausal state on hemostatic parameters in ethnic Chinese women. J Thromb Thrombolysis. 1996;3(1):9–12. doi:10.1007/BF00226404
77. Elsayid M, Elbasheer MAM, Elgari MM, Elfaki T. The effect of contraceptive pills on coagulation tests among Sudanese women in Khartoum State-Sudan; 2016.
78. Rodak BF, Keohane EM, Fritsma GA. Hematology-E-Book: Clinical Principles and Applications. Elsevier Health Sciences; 2013.
79. Mohammed E, Ahmed E, Eldirderi S, Gafar S. Research article effect of oral contraceptives on coagulation parameters among Sudanese women in Khartoum state. EC Gynaecol. 2020;9:1–5.
80. Middeldorp S, Meijers JC, van den Ende AE, et al. Effects on coagulation of levonorgestrel-and desogestrel-containing low dose oral contraceptives: a cross-over study. Thromb Haemost. 2000;84(07):4–8. doi:10.1055/s-0037-1613958
81. van Hylckama Vlieg A, Helmerhorst F, Vandenbroucke J, Doggen C, Rosendaal F. The venous thrombotic risk of oral contraceptives, effects of oestrogen dose and progestogen type: results of the MEGA case-control study. BMJ. 2009;339:b2921.
82. Bhagavan NV, Ha C-E. Chapter 34 - biochemistry of hemostasis. In: Bhagavan NV, Ha C-E, editors. Essentials of Medical Biochemistry.
83. Osman ZAA, Babiker SE, Babiker NE. Estimation of D-dimer level among Sudanese women under contraceptive pill. J Drug Deliv Ther. 2019;9(6–s):53–57. doi:10.22270/jddt.v9i6-s.3738
84. Sehovic N, Smith KP. Risk of venous thromboembolism with drospirenone in combined oral contraceptive products. Ann Pharmacother. 2010;44(5):898–903. doi:10.1345/aph.1M649
85. Plu-Bureau G, Maitrot-Mantelet L, Hugon-Rodin J, Canonico M. Hormonal contraceptives and venous thromboembolism: an epidemiological update. Best Pract Res Clin Endocrinol Metab. 2013;27(1):25–34. doi:10.1016/j.beem.2012.11.002
86. Zöller B, Li X, Ohlsson H, Ji J, Sundquist J, Sundquist K. Family history of venous thromboembolism as a risk factor and genetic research tool. Thromb Haemost. 2015;114(11):890–900. doi:10.1160/TH15-04-0306
87. Lidegaard Ø, Løkkegaard E, Svendsen AL, Agger C. Hormonal contraception and risk of venous thromboembolism: national follow-up study. BMJ. 2009;339:b2890–b2890. doi:10.1136/bmj.b2890
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association Between HbA1c Levels And Hematological Biomarkers in Adults with Type 2 Diabetes Mellitus: A Retrospective Study
AlJedai A, Amin HA, Alanazi F, AlSudais H, Alshalani A
International Journal of General Medicine 2025, 18:7725-7737
Published Date: 20 December 2025