Back to Journals » Infection and Drug Resistance » Volume 12
Helicobacter pylori, Endoscopic, And Histologic Features Among Kidney Transplant Candidates In Southern Iran
Authors Niknam R ![]() , Barfei M
, Barfei M ![]() , Mahmoudi L
, Mahmoudi L ![]()
Received 20 August 2019
Accepted for publication 6 November 2019
Published 29 November 2019 Volume 2019:12 Pages 3687—3693
DOI https://doi.org/10.2147/IDR.S228026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Ramin Niknam,1 Maryam Barfei,2 Laleh Mahmoudi3
1Gastroenterohepatology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran; 2Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran; 3Department of Clinical Pharmacy, School of Pharmacy, Shiraz University of Medical Sciences, Shiraz, Iran
Correspondence: Laleh Mahmoudi
Department of Clinical Pharmacy, School of Pharmacy, Shiraz University of Medical Sciences, PO Box 7146864685, Shiraz, Iran
Tel +98 713 242 4128
Fax +98 713 242 4126
Email [email protected]
Background: The risks of gastrointestinal disorders and cancer are higher in chronic kidney disease (CKD) patients than the general population. There are only a few published reports on the association of helicobacter pylori (H. pylori) infection, endoscopic findings, and histology in these patients. This study was designed to address these controversial topics among kidney transplant candidates as the first study in southern Iran.
Patients and methods: In this cross-sectional study, patients undergoing renal transplantation in the largest center of southern Iran during 2016–2017 were evaluated for the frequency of H. pylori infection, endoscopic findings, and histology. Gastric endoscopic findings (normal, abnormal non-ulcerative, ulcerative) and histological findings of gastric biopsy (normal/non-significant, inflammation, premalignant lesions (PMLs), malignant lesions) were studied.
Results: In total, 293 patients underwent endoscopy for transplant work up. The mean age (SD) was 47.37 (13.14) years. The most common endoscopic finding was abnormal gastric lesions. Overall, 78.8% patients had abnormal gastric histologic findings, of which 6.1% had PMLs. There was no significant association between laboratory data of patients with H. pylori infection. Of these, 147 (50.2%) patients were positive and the others were H. Pylori negative. Positive H. pylori infection was significantly associated with gastric ulcerative lesions. Positive H. pylori infection was also strongly associated with inflammation (P<0.01), but not significantly associated with PMLs (P=0.99) in gastric histology.
Conclusion: The present study showed that abnormal endoscopic and histologic findings as well as positive H. pylori infection were observed in a large number of kidney transplant candidates, so upper endoscopy with biopsy is an acceptable procedure for these patients. However, further studies are recommended to determine the relationship of H. pylori with abnormal endoscopic and histologic findings considering other confounding factors in kidney transplant candidates as well as the efficacy of H. pylori eradication therapy to improve these abnormal findings.
Keywords: chronic kidney disease, transplantation, endoscopic findings, premalignant lesion, Helicobacter pylori
Introduction
Chronic kidney disease (CKD) can be interpreted as an irreversible reduction in kidney function that could be as severe as being fatal in the case of no dialysis or transplantation. This condition is associated with several various pathological conditions of the gastrointestinal, cardiac, vascular, pulmonary and immunological systems.1
The risk of gastrointestinal complications and cancer are higher in CKD patients than the general population.2,3 Recent studies demonstrated the relationship between helicobacter pylori (H. pylori) infection and CKD,4–8 but there is no evidence to approve direct association of H. pylori infection with renal disease.9,10 H. pylori is the most common chronic bacterial infection of the gastrointestinal tract of humans.11,12 The prevalence of H. pylori infection in the United States is estimated to be ~30–50%.11,13 H. pylori infection is strongly associated with chronic active gastritis, peptic ulcer diseases, and malignancies.11,14
Gastric cancer, as the third highest cause of mortality, is a major public health problem.15–17 Histologic pre-malignant lesions (PMLs) are precursors of cascade for the development of gastric cancer.15,16 PMLs are classified as atrophic gastritis, complete or incomplete intestinal metaplasia, and gastric dysplasia.15–17 Infection by H. pylori has been described in more than 90% of the cases of gastric mucosa associated lymphoid tissue.18 Moreover, the role of upper GI endoscopy and the detection and/or treatment of H. pylori infection in non-dyspeptic renal transplant candidates are unclear, although some published studies have described the association or correlation between endoscopic findings and histologic changes.19
Like normal populations, PMLs are particularly important in patients with CKD and require careful endoscopic and histological follow-up to prevent further malignancy. It is reasonable to assume that eliminating malignancies or premalignant lesions prior to transplantation may help to reduce the incidence of post-transplant malignancy. Our center, like many other centers, routinely performs upper gastrointestinal endoscopy on all CKD patients that are candidates for kidney transplantation, but the usual role of endoscopy in these patients is unclear. On the other hand, there are only a few published reports on the association of H. pylori infection, endoscopic findings, and histology in these patients. Therefore, we designed this study to address these controversial topics among kidney transplant candidates as the first study in southern Iran.
Patients And Methods
Population And Study Design
After obtaining the approval of the University Ethics Committee of Shiraz University of Medical Sciences and the Institutional Review Board (reference code: 96-01-01-14984), we conducted a retrospective cross-sectional study of patients with CKD on the transplant waiting list performed at two major referral centers in southern Iran—during 2016 and 2017. This study was conducted following the declaration of Helsinki regarding ethical principles for medical research. Written informed consent was obtained from all patients to review their medical records. The frequency of H. pylori infection, endoscopic findings, and histology in consecutive renal transplant candidates were evaluated.
We included all adult patients with a definitive CKD diagnosis who were on the transplant waiting list and we excluded patients with incomplete medical reports. Data for each patient were recorded in a checklist. We collected and evaluated various variables, including age, sex, pre-transplant screening data, endoscopy, and histology reports. For endoscopic evaluation, endoscopic findings of different parts of the upper gastrointestinal tract, including the esophagus, stomach, and duodenum, were examined. Our patients were then categorized, based on gastric endoscopic findings, into three groups of normal, abnormal non-ulcerative (any evidence of mucosal lesion without ulcer, eg, erosion, erythema, nodularity, atrophy, white plaque, and petechiae), and ulcerative.
Given the retrospective nature of our study, endoscopic biopsies of abnormal gastric mucosa as well as random gastric biopsies in all patients with normal mucosa were examined by a pathologist. The histologic findings were categorized into four groups of normal/non-significant, inflammation, PMLs, and malignant lesions. H. pylori infection was established by Giemsa stain and hematoxylin and eosin staining by the same pathologist. The frequency of H. pylori infection was studied in different types of gastric endoscopic findings as well as other parts of the upper gastrointestinal tract. Finally, three groups of gastric endoscopic findings were compared for the existence of different groups of histological findings.
Statistical Analysis
Means±standard deviations were reported for quantitative variables, and frequencies were reported for qualitative variables. Univariate analysis was done by chi-square test, and two independent sample t-tests. A P-value less than 0.050 was considered as significant. All data analysis was performed under IBM SPSS statistics for Windows, version 25.0 (Chicago, IL).
Results
In total, 293 patients were included. The mean (SD) age was 47.37 (14.15) years, ranging from 18–81 years. Of these, 183 (62.5%) and 110 (37.5%) patients were male and female, respectively. Mean ages in females and males were 45.66±13.84 and 41±14.27 years, respectively. The most common causes of CKD were hypertension and diabetes mellitus. The clinical and demographic characteristics of the participants are shown in Table 1.
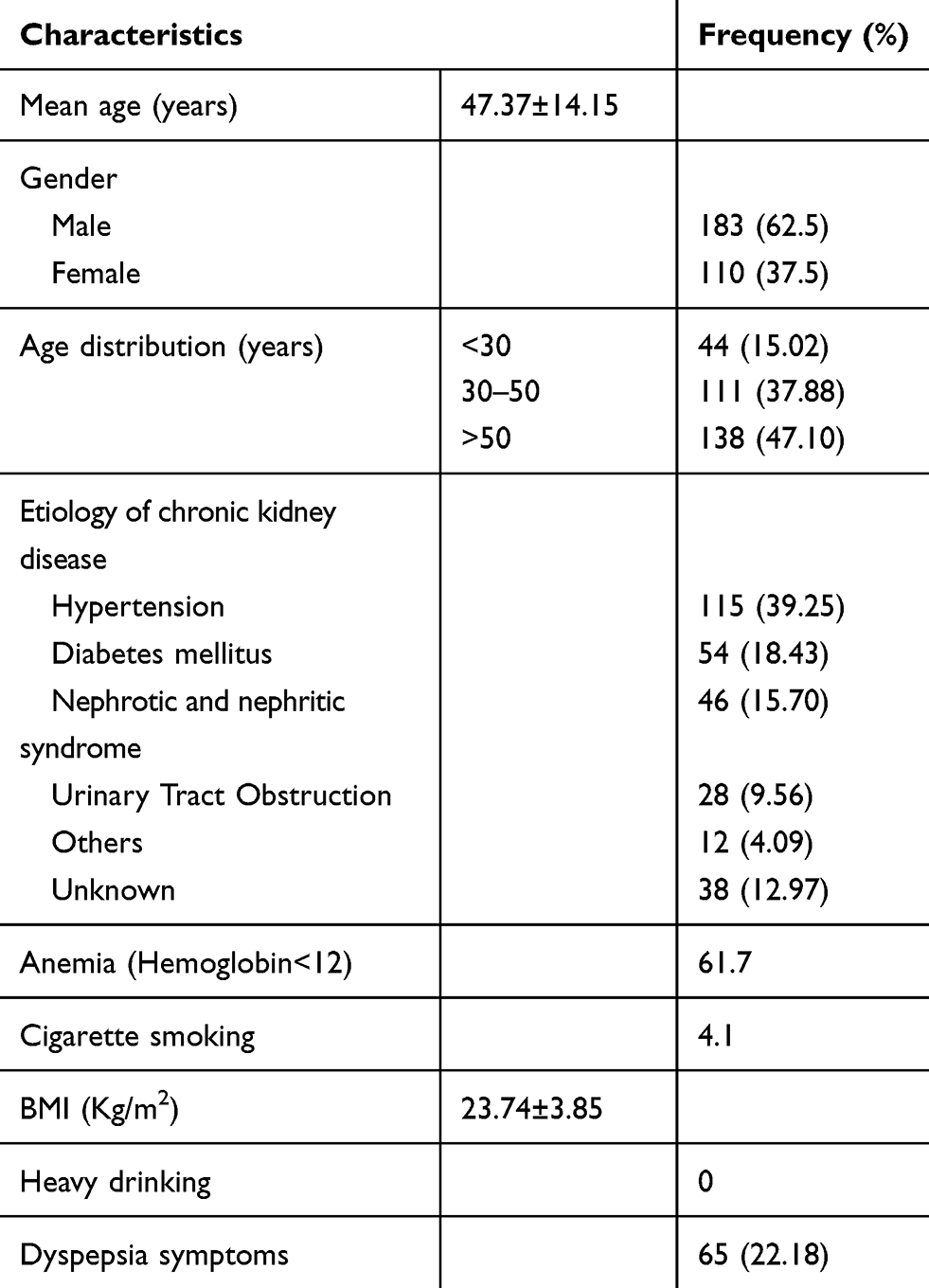 |
Table 1 Clinical And Demographic Characteristics Of The Participants Among Kidney Transplant Candidates (n=293) |
Overall, 249 (84.98%) and 44 (15.02%) patients had abnormal and normal upper gastrointestinal endoscopic findings, respectively; 94, 203, and 34 of the abnormal upper gastrointestinal endoscopic findings were gastroesophageal reflux disease, abnormal gastric lesions, and duodenal ulcer, respectively. Some patients had more than one endoscopic finding.
One hundred and forty-seven (50.2%) patients were positive and the others were H. pylori negative. There was no significant association between laboratory data of patients with H. pylori infection (Table 2). Overall, 94 patients had GERD, of whom 50 (53.19%) were positive for H. pylori infection. In the stomach, 90 (30.7%) of the patients with H. pylori infection had abnormal non-ulcerative lesions, while only 17 (5.5%) of them had gastric ulcer and 40 (13.6%) were normal. With the ratio the same as the stomach, duodenal abnormal non-ulcerative findings (12.6%) were greater than duodenal ulcers (7.1%) in patients with H. pylori infection. Table 3 shows the association between H. pylori infection and endoscopic findings. Positive H. pylori infection was significantly associated with gastric ulcerative lesions. Our data showed no significant association between other endoscopic findings with H. pylori infection.
 |
Table 2 The Comparison Of Laboratory Data Between Positive And Negative helicobacter pylori (H. pylori) Among Kidney Transplant Candidates |
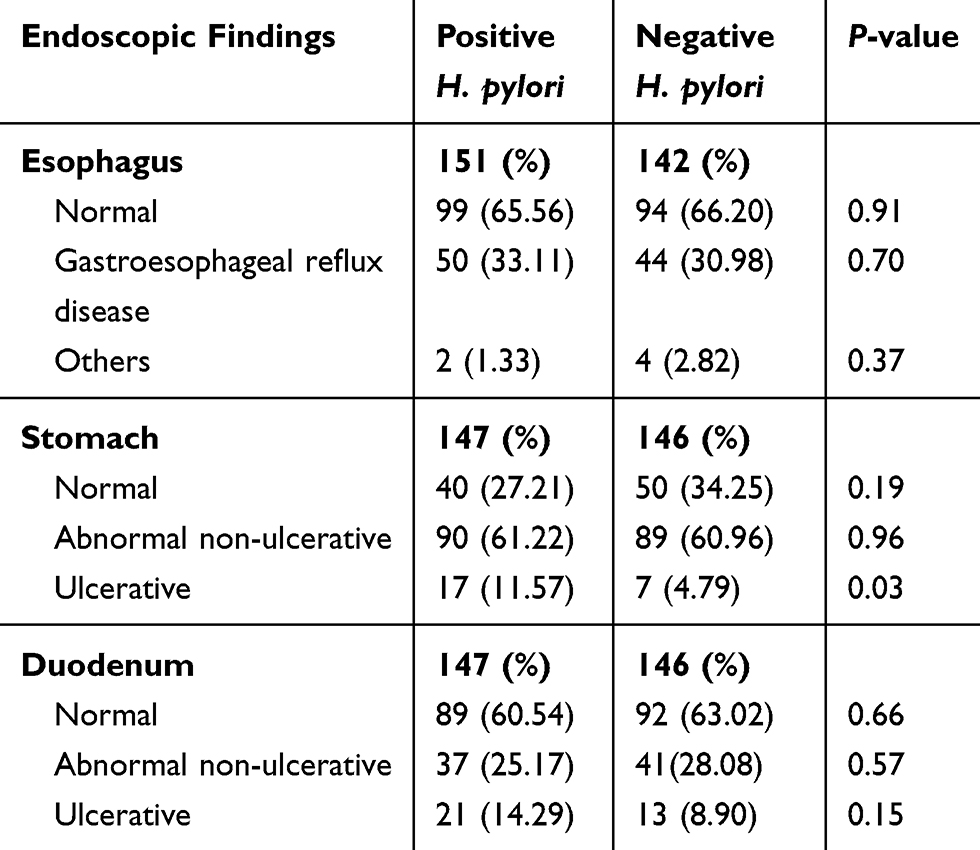 |
Table 3 The Association Between Helicobacter pylori (H. pylori) Infection And Endoscopic Findings Among Kidney Transplant Candidates (n=293) |
Overall, 231 (78.8%) had abnormal gastric histologic findings, of which 213 (72.6%) and 18 (6.1%) had inflammatory changes and PMLs, respectively. Sixty-two patients had normal/non-significant histology. The evidence of PMLs was seen in 16 and two patients with abnormal non-ulcerative and ulcerative gastric endoscopic findings, respectively. On the other hand, no normal endoscopy was associated with PMLs. Table 4 shows the association between gastric endoscopic findings and histology. Positive H. pylori infection was strongly associated with inflammation (P<0.01), but not significantly associated with PMLs (P=0.99) in gastric histology (Table 5).
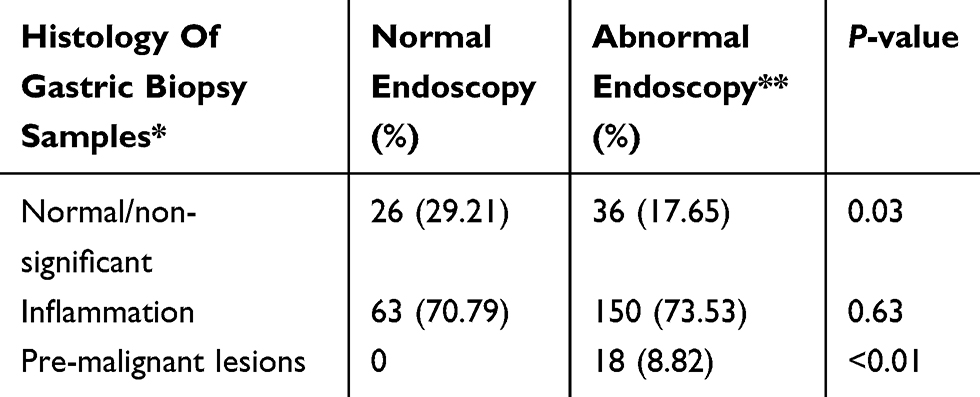 |
Table 4 The Association Between Gastric Endoscopic Findings And Histology Of Gastric Biopsy Samples Among Kidney Transplant Candidates (n=293) |
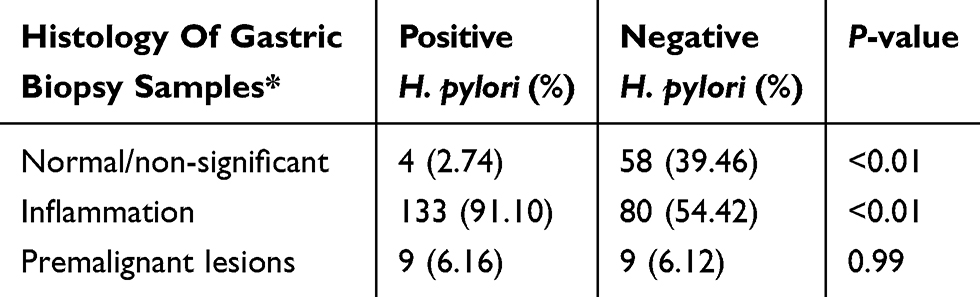 |
Table 5 The Association Between Helicobacter pylori (H. pylori) Infection And Histology Of Gastric Biopsy Samples Among Kidney Transplant Candidates (n=293) |
Discussion
H. pylori infection has been reported to be strongly associated with various gastroduodenal diseases.11,15 The prevalence of H. pylori infection in the study differs from country to country, ethnicity to ethnicity, even in the same country.12,20–22 Our study revealed that 50.2% of our population were H. pylori positive, which was lower and at the same time higher compared to local and international studies. H. pylori infection causes a spectrum of both gastric and extra gastrointestinal diseases with acute and chronic gastritis, peptic ulcer disease, gastric atrophy, intestinal metaplasia, MALT lymphoma, and gastric adenocarcinoma.21
In previous reports ~85% of the adults were IgG carriers of the H. pylori11 and histological evidence of H. pylori was noted in 89.2% of biopsies in the north of Iran.24 Both of these studies indicate the lower rate of H. pylori prevalence in our study compared to normal population compared to in previous studies. In a cross-sectional study, Asl et al25 determined the H. pylori frequency in patients with stable chronic hemodialysis with non-ulcer dyspepsia. Based on microscopic evaluation, the prevalence of H. pylori in dyspeptic patients on dialysis was 70% and 57.5% in dyspeptic patients with normal renal function. Both results are higher than our report. Gu et al26 conducted a meta-analysis on chronic renal failure patients who received hemodialysis and found that the H. pylori infection rate was about 50.8%, which is almost the same as our report.
The vast majority of our patients had abnormality in their upper endoscopy, including GERD, gastric lesions, and duodenal lesions. Ponticelli et al27 found that the most common gastrointestinal complications in transplant recipients are oral, esophageal, and gastric lesions. In a study by Ihamaki et al28 upper gastrointestinal lesions were evaluated in the general population. According to their study, the prevalence of peptic ulcer, duodenal ulcer, and gastric ulcer were 1.68%, 1.4% and 0.28%, respectively. Our study showed a higher incidence of ulcer in both positive and negative groups of H. pylori.
Gu et al26 showed that the incidence of ulcerative diseases in dialysis patients was 13.7% and in the control group was 24.9%. According to our study compared with their study, the frequency of ulcerative lesions in our population was lower.
The prevalence of erosive gastritis, erosive duodenitis, gastric ulcer, and duodenal ulcer was 12%, 10%, 2%, and 2%, respectively; according to the Akdamar et al29 study. In our study, the prevalence of gastric non-ulcerative abnormalities, duodenal non-ulcerative abnormalities, gastric ulcer, and duodenal ulcer was higher than that reported.
In a report15 the association of gastric endoscopic findings and histologic pre-malignant lesions was evaluated; this showed that abnormal gastric endoscopic findings can be considered as a risk factor for PMLs. Endoscopy and histological changes in the upper gastrointestinal tract of patients with chronic renal failure were studied by Mirsa et al30 who showed that the most frequent histological changes in gastric histology were mucosal edema (82.35%) and gastritis (23.5%). Homse Netto et al22 conducted a study of 96 patients to evaluate gastrointestinal alterations in renal transplant candidates, and found that intestinal metaplasia was present in 8.33% of their population, which was most consistent with our study. But in this study, H. pylori was significantly associated with non-ulcerative gastric findings, which was not consistent with our study.
H. pylori infection has been reported to be strongly associated with various gastroduodenal diseases.11,14 The important question is how useful the eradication therapy of H. pylori can be in patients with CKD. In a recent study by Sugimoto et al23 they concluded that, since patients with CKD have a higher risk of gastroduodenal diseases, all hemodialysis patients are advised to use endoscopic examinations and H. pylori eradication therapies. In a study by Hsu et al31 on pre-ESRD patients and matched patients on ESRD, they concluded that early H. pylori eradication has a lower risk of peptic ulcer bleeding in positive H. pylori infection.
The role of H. pylori eradication therapies in improving the nutritional status of patients with CKD has also been studied. Some studies have shown that infection with H. pylori in CKD patients is associated with malnutrition, and it is recommended that eradication of H. pylori may improve nutritional status.23,32 In a pilot study,32 the effect of H. pylori eradication therapy on nutritional status in H. pylori positive hemodialysis patients was investigated. They concluded that eradication of H. pylori may improve nutritional status by increasing serum cholinesterase and cholesterol levels in hemodialysis patients, especially in patients with mild-to-moderate gastric mucosal atrophy.
There was no consensus on the type of H. pylori eradication regimen for patients with CKD,23,33–36 but a study by Alimadadi et al37 to investigate the effect of creatinine clearance on H. pylori eradication showed no association between the success rate of H. pylori eradication and renal function. In a study by Seyyed Majidi et al34 CKD patients with positive H. pylori were divided into four groups treated for 2 weeks to evaluate different treatment regimens. There was no significant difference between the success rates of H. pylori eradication regimens in the different groups. They conclude that, with fewer drugs and less risk of side-effects and drug interactions, a sequential regimen is the best. In another study by Itatsu et al,35 hemodialysis patients with positive H. pylori were divided into two groups treated for 1 week to evaluate different treatment regimens. They concluded that a low-dose lansoprazole, amoxicillin, and clarithromycin regimen is safe, effective, and recommended in these patients. The long-term effect of H. pylori eradication in patients with peptic ulcer with and without CKD was evaluated by Tseng et al.36 They concluded that the recurrence of peptic ulcer after H. pylori eradication was higher in patients with CKD than in patients without renal disease. Although there are several studies on the eradication of H. pylori treatment in CKD, the clinical protocol and appropriate eradication regimens are controversial and further studies are needed to better elucidate this issue.
As far as we know, this is the first study to investigate the association between H. pylori infection, gastric endoscopy, and histological changes in kidney transplant candidates in Iran. Our research had some important limitations. This study was a retrospective study that was conducted in only two centers. H. pylori infection was diagnosed with only one method. Except for the results presented, we did not have further documentation to evaluate other potential risk factors and confounding factors that make patients susceptible to abnormal endoscopy or histology. Given these limitations and to determine the significance of our results, multi-center research can be used. Compared to other studies,22 one of the strengths of our study was the significant size of the sample with important variables available including pre-transplant laboratory data, endoscopy, and histological reports. Another strength of our study was that endoscopic and histologic findings were classified into different groups and the frequency of H. pylori infection was evaluated in different types of endoscopic and histological findings. The findings of this study showed a lower prevalence of H. pylori infection compared to many studies. The majority of our patients had abnormal endoscopic findings. Abnormal non-ulcerative and ulcerative changes constituted the dominant endoscopic findings in H. pylori-positive patients. Abnormal histology findings were especially significant in abnormal endoscopic findings. Until further studies are revealed, this study could send a message to nephrologists and gastroenterologists that upper gastrointestinal endoscopy is an acceptable procedure for all kidney transplant candidates with or without gastrointestinal symptoms, and in all patients, even with normal endoscopic findings, random biopsy for evaluation of H. pylori and abnormal histology can be helpful.
Conclusions
The present study showed that abnormal endoscopic and histologic findings as well as positive H. pylori infection were observed in a large number of kidney transplant candidates, so upper endoscopy with biopsy is an acceptable procedure for these patients. However, further studies are recommended to determine the relationship of H. pylori with abnormal endoscopic and histologic findings considering other confounding factors in kidney transplant candidates as well as the efficacy of H. pylori eradication therapy to improve these abnormal findings.
Acknowledgment
This study was a part of a MD thesis written by Maryam Barfei and was supported by the research Council of Shiraz University of Medical Sciences, Shiraz, Iran (96-01-01-14984).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Laeeq SM, Tasneem AA, Hanif FM, et al. Upper gastrointestinal bleeding in patients with end stage renal disease: causes, characteristics and factors associated with need for endoscopic therapeutic intervention. J Transl Int Med. 2017;5(2):106–111. doi:10.1515/jtim-2017-0019
2. Cabello Benavente R, Quicios Dorado C, Lopez Martin L, et al. The candidate for renal transplantation work up: medical, urological and oncological evaluation. Arch Esp Urol. 2011;64(5):441–460.
3. Hardinger KL, Brennan DC, Lowell J, Schnitzler MA. Long-term outcome of gastrointestinal complications in renal transplant patients treated with mycophenolate mofetil. Transpl Int. 2004;17(10):609–616. doi:10.1111/tri.2004.17.issue-10
4. Khedmat H, Ahmadzad-Asl M, Amini M, et al. Gastro-duodenal lesions and Helicobacter pylori infection in uremic patients and renal transplant recipients. Transplant Proc. 2007;39(4):1003–1007. doi:10.1016/j.transproceed.2007.03.034
5. Lin SY, Lin CL, Liu JH, et al. Association between Helicobacter pylori infection and the subsequent risk of end-stage renal disease: a nationwide population-based cohort study. Int J Clin Pract. 2015;69(5):604–610. doi:10.1111/ijcp.12602
6. Afsar B, Ozdemir FN, Elsurer R, Sezer S. Helicobacter pylori infection may increase renal resistive index. Med Hypotheses. 2007;69(4):956–957. doi:10.1016/j.mehy.2007.01.061
7. Hsu WY, Lin CH, Lin CC, Sung FC, Hsu CP, Kao CH. The relationship between Helicobacter pylori and cancer risk. Eur J Intern Med. 2014;25(3):235–240. doi:10.1016/j.ejim.2014.01.009
8. Lai CY, Yang TY, Lin CL, Kao CH. Helicobacter pylori infection and the risk of acute coronary syndrome: a nationwide retrospective cohort study. Eur J Clin Microbiol Infect Dis. 2015;34(1):69–74. doi:10.1007/s10096-014-2207-7
9. Sotoudehmanesh R, Ali Asgari A, Ansari R, Nouraie M. Endoscopic findings in end-stage renal disease. Endoscopy. 2003;35(6):502–505.
10. Ala-Kaila K. Upper gastrointestinal findings in chronic renal failure. Scand J Gastroenterol. 1987;22(3):372–376. doi:10.3109/00365528709078607
11. Wijarnpreecha K, Thongprayoon C, Nissaisorakarn P, et al. Association between Helicobacter pylori and end-stage renal disease: a meta-analysis. World J Gastroenterol. 2017;23(8):1497–1506. doi:10.3748/wjg.v23.i8.1497
12. Salih BA. Helicobacter pylori infection in developing countries: the burden for how long? Saudi J Gastroenterol. 2009;15(3):201–207. doi:10.4103/1319-3767.54743
13. Pounder RE, Ng D. The prevalence of Helicobacter pylori infection in different countries. Aliment Pharmacol Ther. 1995;9 Suppl 2:33–39.
14. Burkitt MD, Duckworth CA, Williams JM, Pritchard DM. Helicobacter pylori-induced gastric pathology: insights from in vivo and ex vivo models. Dis Model Mech. 2017;10(2):89–104. doi:10.1242/dmm.027649
15. Niknam R, Manafi A, Fattahi MR, Mahmoudi L. The association between gastric endoscopic findings and histologic premalignant lesions in the Iranian rural population. Medicine (Baltimore). 2015;94(17):e715. doi:10.1097/MD.0000000000000715
16. Niknam R, Manafi A, Maghbool M, Kouhpayeh A, Mahmoudi L. Is endoscopic nodular gastritis associated with premalignant lesions? Neth J Med. 2015;73(5):236–241.
17. Fock KM. Review article: the epidemiology and prevention of gastric cancer. Aliment Pharmacol Ther. 2014;40(3):250–260. doi:10.1111/apt.2014.40.issue-3
18. Nakamura S, Matsumoto T. Helicobacter pylori and gastric mucosa-associated lymphoid tissue lymphoma: recent progress in pathogenesis and management. World J Gastroenterol. 2013;19(45):8181–8187. doi:10.3748/wjg.v19.i45.8181
19. Akeel M, Elmakki E, Shehata A, et al. Prevalence and factors associated with H. pylori infection in Saudi patients with dyspepsia. Electron Physician. 2018;10(9):7279–7286. doi:10.19082/7279
20. Chen J, Bu XL, Wang QY, Hu PJ, Chen MH. Decreasing seroprevalence of Helicobacter pylori infection during 1993–2003 in Guangzhou, southern China. Helicobacter. 2007;12(2):164–169. doi:10.1111/j.1523-5378.2007.00487.x
21. Mahmoudi L, Farshad S, Seddigh M, et al. High efficacy of gemifloxacin-containing therapy in Helicobacter Pylori eradication: a pilot empirical second-line rescue therapy. Medicine (Baltimore). 2016;95(42):e4410. doi:10.1097/MD.0000000000004410
22. Homse Netto JP, Pinheiro JPS, Ferrari ML, et al. Upper gastrointestinal alterations in kidney transplant candidates. J Bras Nefrol. 2018;40(3):266–272. doi:10.1590/2175-8239-jbn-3829
23. Sugimoto M, Yasuda H, Andoh A. Nutrition status and Helicobacter pylori infection in patients receiving hemodialysis. World J Gastroenterol. 2018;24(15):1591–1600. doi:10.3748/wjg.v24.i15.1591
24. Malekzadeh R, Sotoudeh M, Derakhshan MH, Mikaeli J, Yazdanbod A, Merat S, et al. Prevalence of gastric precancerous lesions in Ardabil, a high incidence province for gastric adenocarcinoma in the northwest of Iran. J Clin Pathol. 2004;57(1):37–42
25. Asl MK, Nasri H. Prevalence of Helicobacter pylori infection in maintenance hemodialysis patients with non-ulcer dyspepsia. Saudi J Kidney Dis Transpl. 2009;20(2):223–226.
26. Gu M, Xiao S, Pan X, Zhang G. Helicobacter pylori infection in dialysis patients: a meta-analysis. Gastroenterol Res Pract. 2013;2013:785892. doi:10.1155/2013/785892
27. Ponticelli C, Passerini P. Gastrointestinal complications in renal transplant recipients. Transpl Int. 2005;18(6):643–650. doi:10.1111/tri.2005.18.issue-6
28. Ihamaki T, Varis K, Siurala M. Morphological, functional and immunological state of the gastric mucosa in gastric carcinoma families. Comparison with a computer-matched family sample. Scand J Gastroenterol. 1979;14(7):801–812. doi:10.3109/00365527909181408
29. Akdamar K, Ertan A, Agrawal NM, McMahon FG, Ryan J. Upper gastrointestinal endoscopy in normal asymptomatic volunteers. Gastrointest Endosc. 1986;32(2):78–80. doi:10.1016/S0016-5107(86)71760-4
30. Misra V, Misra SP, Shukla SK, et al. Endoscopic and histological changes in upper gastrointestinal tract of patients with chronic renal failure. Indian J Pathol Microbiol. 2004;47(2):170–173.
31. Hsu CH, Hu HY, Huang N, Chang SS. Early eradication has a lower risk of peptic ulcer bleeding in Helicobacter pylori-infected chronic kidney disease patients. Eur J Intern Med. 2016;33:112–117. doi:10.1016/j.ejim.2016.06.035
32. Aguilera A, Codoceo R, Bajo MA, et al. Helicobacter pylori infection: a new cause of anorexia in peritoneal dialysis patients. Perit Dial Int. 2001;21 Suppl 3:S152–S156.
33. Ehsani Ardakani MJ, Aghajanian M, Nasiri AA, et al. Comparison of half-dose and full-dose triple therapy regimens for Helicobacter pylori eradication in patients with end-stage renal disease. Gastroenterol Hepatol Bed Bench. 2014 Summer;7(3):151–5.
34. Seyyed Majidi M, Sanjari Pirayvatlou P, Rajabikashani M, et al. Comparison of Helicobacter pylori eradication regimens in patients with end stage renal disease. Gastroenterol Hepatol Bed Bench. 2018 Winter;11(1):15–19.
35. Itatsu T, Miwa H, Nagahara A, et al. Eradication of Helicobacter pylori in hemodialysis patients. Ren Fail. 2007;29(1):97–102. doi:10.1080/08860220601039122
36. Tseng GY, Lin HJ, Fang CT, et al. Recurrence of peptic ulcer in uraemic and non-uraemic patients after Helicobacter pylori eradication: a 2-year study. Aliment Pharmacol Ther. 2007;26(6):925–933. doi:10.1111/j.1365-2036.2007.03438.x
37. Alimadadi M, Seyyedmajidi M, Amirkhanlou S, et al. Impact of creatinine clearance on Helicobacter pylori eradication rate in patients with peptic ulcer disease. Iran J Kidney Dis. 2015;9(6):427–432.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.