Back to Journals » Clinical Ophthalmology » Volume 17
Heart-Rate Variability Correlates to Choroidal Thickness in Central Serous Chorioretinopathy
Authors Nordsten CB ![]() , Molbech CR, Mehlsen J
, Molbech CR, Mehlsen J ![]() , Sørensen TL
, Sørensen TL
Received 20 January 2023
Accepted for publication 3 May 2023
Published 17 August 2023 Volume 2023:17 Pages 2443—2447
DOI https://doi.org/10.2147/OPTH.S405529
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Cecilie Bagi Nordsten,1,* Christopher Rue Molbech,1,2,* Jesper Mehlsen,3 Torben Lykke Sørensen1,2
1Department of Ophthalmology, Zealand University Hospital, Roskilde, Denmark; 2Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 3Unit of Surgical Pathophysiology, University of Copenhagen, Rigshospitalet, Denmark
*These authors contributed equally to this work
Correspondence: Torben Lykke Sørensen, Department of Ophthalmology, Zealand University Hospital, Vestermarksvej 23, Roskilde, 4000, Denmark, Email [email protected]
Purpose: Patients with central serous chorioretinopathy (CSC) have previously been shown to have a lower heart rate variability (HRV), implying a lower vagal tone. Vagal tone alters mineralocorticoids, which in turn affect the thickness of the choroid. Since increased choroidal thickness is characteristic of CSC, we wanted to investigate its correlation with HRV.
Patients and Methods: In this case–control study, 21 acute CSC patients and 31 healthy controls were included. Diagnosis was confirmed by optical coherence tomography (OCT) and retinal examination. HRV was evaluated following accepted standards. Outcome measures were chosen beforehand as follows: Standard deviation of N–N intervals (SDNN), root mean square of successive differences (RMSDD), low frequency/high frequency ratio (LF/HF ratio), and standard deviation ratio from commonly used Poincare plot (SD2/SD1 ratio). Choroidal thickness was measured using OCT directly under the foveola.
Results: Patients and healthy controls did not differ in health and medical characteristics in addition to CSC disease. Choroidal thickness was greatest in patients with CSC (mean±SD: 342± 80 μm) compared to controls (235± 60 μm, p< 0.0001). A correlation was observed between LF/HF ratio and choroidal thickness in patients with CSC (Pearson correlation 0.63, p=0.02), where the CSC group had a lower LF/HF ratio (Median 2.39 ms2, IQR: 1.2– 4.34 ms2) compared to controls (Median 1.2 ms2, IQR: 0.9– 2.4 ms2, p=0.06) and SD2/SD1 ratio (CSC 0.59± 0.2 vs controls 0.74± 0.3, p=0.06).
Conclusion: We found a correlation between the thickness of the choroid and the HRV-measured LF/HF ratio in patients with CSC and showed a borderline significant reduction in HRV measurements in patients with CSC. The data imply that vagal alterations exist in patients with CSC. Due to the low n, this should be considered as a pilot study. Further studies are warranted to elucidate mechanisms and validate findings.
Keywords: vagus, vagal tone, heart rate variability
Introduction
Central serous chorioretinopathy (CSC) is a common retinopathy affecting middle-aged individuals, especially men.1 The early stage of CSC is marked by thickened choroid, serous retinal detachment, and absence of drusen.1 Patients commonly experience metamorphopsia and blurred vision. Without treatment, 90% of patients undergo spontaneous remission within 1.5 months.1 If serous detachment prevails, intervention is needed to prevent subsequent neovascularization.1 The cause of CSC is unknown, but risk factors for CSC are genetic disposition, use of corticosteroids, elevated cortisol, type A personality, emotional distress, sleep disorders, and medications, including MEK-inhibitors, phosphodiesterase-5-inhibitors, and adrenergic receptor agonists.1 The most accepted pathogenesis is alterations in the mineralocorticoid pathway and receptors1 leading to dilation of the choroidal vessels, causing mechanical flux gradients over the Bruch’s membrane, further leading to serous detachment. Heart failure patients are known to have an affected mineralocorticoid pathway2 via an abnormal sympatric-parasympathetic-ratio.3 This abnormal ratio causes a decrease in the parasympathetic inhibition of cortisol and aldosterone.4 Furthermore, patients with heart failure have an increased risk of CSC.5 Therefore, it seems likely that the abnormal mineralocorticoid pathway plays a role in the development of CSC. However, abnormal parasympathetic activity is not easily measured.6 One way to indirectly determine parasympathetic activity is to evaluate vagal activity. The vagal nerve is part of the parasympathetic system and can be measured indirectly using heart rate variability (HRV). HRV has previously been shown to be lower in CSC patients.4,7 Vagal involvement, as part of impaired parasympathetic activity, in CSC appears mechanistically likely, but its correlation with choroidal thickness is unknown. Based on previous findings4,7 we hypothesized that a lower vagal tone, determined by HRV, would correlate with increased choroidal thickness in patients with CSC compared to healthy controls.
Materials and Methods
21 patients with acute CSC and 31 healthy participants were included in this case–control study. Subjects were recruited from the outpatient ophthalmic clinic of Zealand University Hospital (Roskilde, Denmark), which is a tertiary academic referral center. The project was approved by the Regional Ethics Committee in Research of the Region of Zealand (jr. no. SJ-510) and the Danish Data Protection Agency (jr. no. REG-17-2016). Participants were informed about the purpose of the study, in accordance with the Declaration of Helsinki, and gave oral and written consent before enrollment. Power calculations were based on Tewari et al4 and predicted group sizes of 20 to achieve power with an alpha of 0.05 and a beta of 0.2 with mean and SD estimates.
Enrolled patients had had a minimum of 3 months from initial symptoms due to referral only after expected treatment. All included were subjected to a structured interview on lifestyle factors and medical history. Patients with active infection, diseases affecting the immune system or active use of steroidal medication were excluded (active infection determined by plasma C-reactive protein greater than 15 mg/L). An ophthalmological examination using a slit-lamp, swept source optical coherence tomography (OCT) (Heidelberg Engineering, Lübeck, Germany), spectral domain OCT (Topcon Medical Systems, Oakland, NJ, USA) and fundus photography was performed upon inclusion. The diagnosis was made by an experienced specialist and, in case of doubt, fluorescence angiography was performed using fluorescein and indocyanine green. Choroidal thickness was measured in the center of the macula with enhanced depth imaging-OCT or line-OCT with the building tool in Heidelberg (Heidelberg Engineering, Lübeck, Germany) and in IMAGEnet i-base (Topcon Medical Systems, Oakland, NJ, USA). In case of disagreement, the image with the best depth resolution was used. HRV was measured using faros 360 (Mega Electronics Ltd, Kuopio, Finland) with 5 leads, 1000 Hz recording sensitivity, and in the supine position for 20 minutes. HRV was calculated using Kubios software (Kubios HRV, v. 2.2 from the University of Eastern Finland). A 5-minute artefact-free ECG was chosen from the last 15 minutes of the measurement.
Heart rate variability was analyzed using the interbeat intervals in the electrocardiogram denoted normal to normal beats (NN). The standard deviation of normal-to-normal beats (SDNN) describes the total variation in the timescale, whereas the numerical difference between successive beats represented by the root mean squared successive difference (RMSSD) is the short-term variation in the timescale primarily reflecting respiration and vagal activity. In the frequency domain achieved by Fast Fourier Transformation, the low-frequency component (LF) primarily represents the baroreceptor regulation and the sympathetic activity, and the high-frequency component (HF) represents respiration and vagal activity. To eliminate noise, it is common to use the LF/HF ratio as a surrogate for the balance between the sympathetic and parasympathetic divisions.8 In a simple deterministic analysis, the single beat (NN) is plotted against the following (NN+1; Poincaré plot) and the result is an ellipse with its long axis following the line of identity and representing slow variations (SD2) and the short axis representing the beat-to-beat variations (SD1). The SD2/SD1 reflects the same information as LF/HF. For all indices except the LF/HF and SD2/SD1 ratios the larger the value, the more parasympathetic/vagal input is seen.8
Data were analysed in bulk and blinded to category. All normally distributed data were analysed using parametric tests and shown with mean ± standard deviation (SD). Non-normally distributed data are shown with median and interquartile ranges (IQR) and analysed using nonparametric tests. Statistics were performed using SPSSTM (version 23, IBM Corporation, Armonk, New York, USA).
Results
There were no differences between CSC patients and healthy participants in terms of lifestyle factors and medical history (data not shown). Patients with CSC had a thicker choroid, as expected, as this is one of the most important findings in CSC.9 No significant differences were observed between healthy participants and patients with CSC in HRV (Table 1), however, with both the LF/HF and the SD2/SD1 ratio being nearly significantly different (both p = 0.06). A significant correlation was observed between the LF/HF ratio and the thickness of the choroid (Pearson correlation 0.63, p-value of 0.02) was observed. The remaining HRV parameters did not correlate with the thickness of the choroid. In healthy participants, age was inversely correlated with choroidal thickness (Pearson correlation −0.548, p = 0.0003, Table 2). To evaluate the effect size and the power estimation, Cohen’s d was calculated (Table 1). The SD2/SD1 ratio is worth highlighting since it showed a medium effect size despite a “nonsignificant” result when regarding p > 0.05 as insignificant.
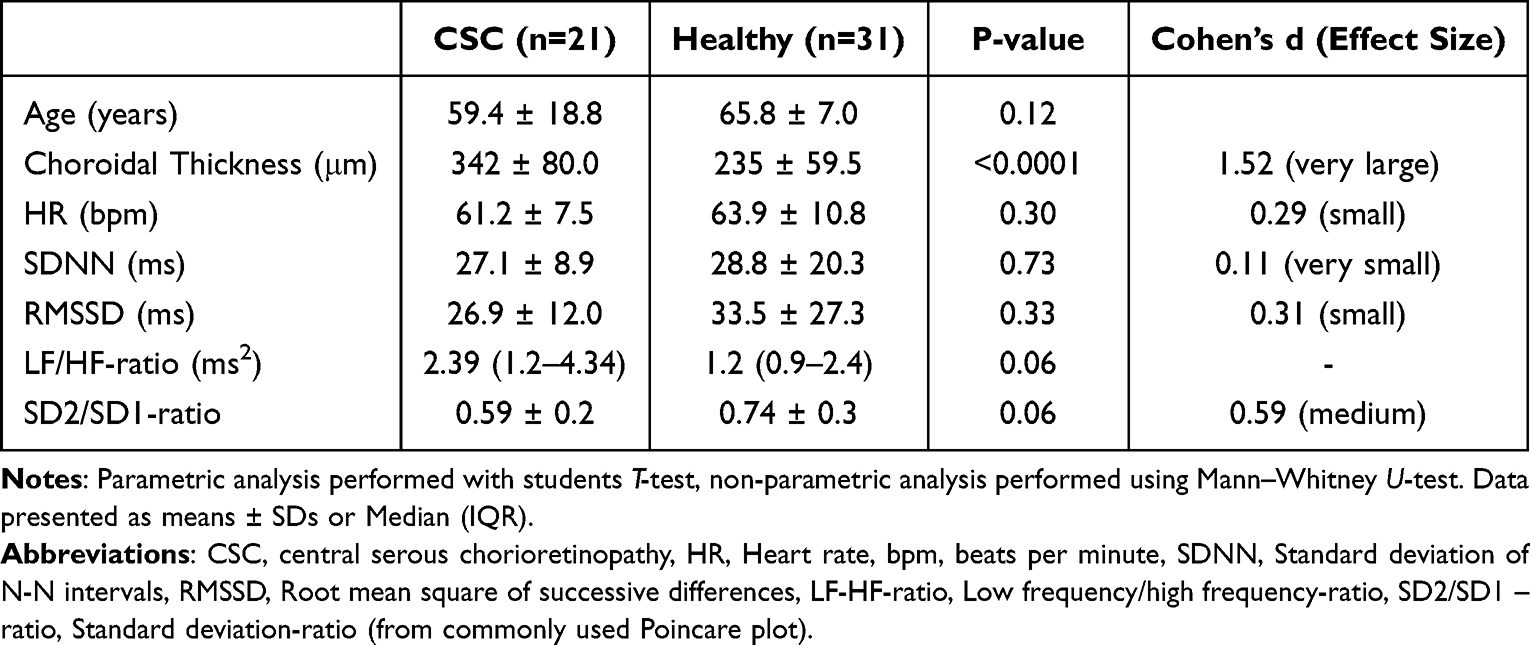 |
Table 1 Characteristics and Comparisons for Patients with CSC and Healthy Participants |
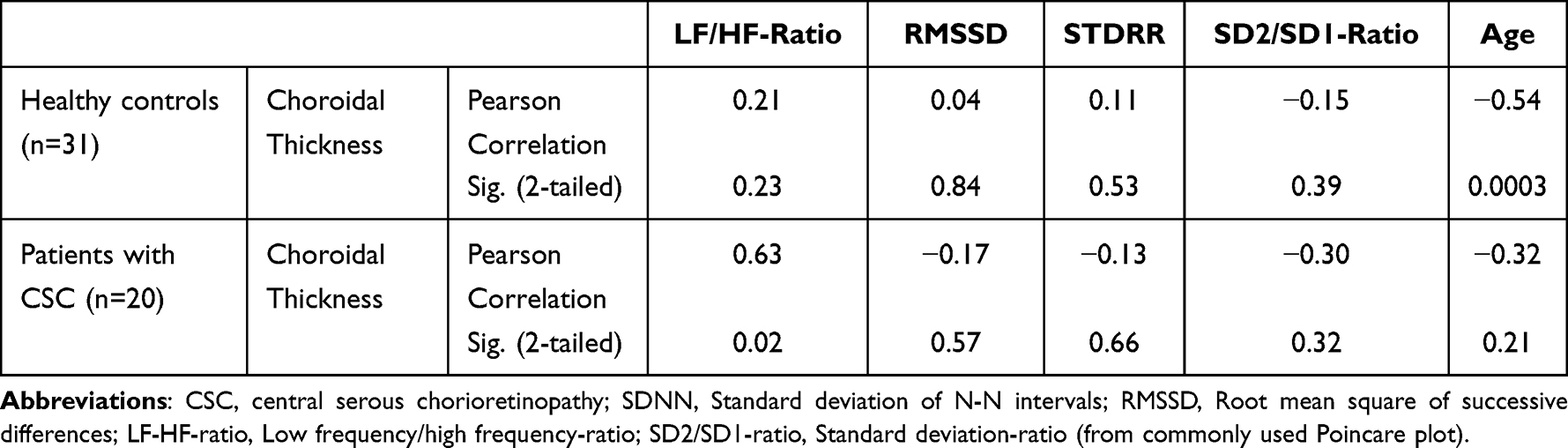 |
Table 2 Correlations Between Outcome Measured Within CSC and Controls |
Discussion
Despite not being a new technique, HRV is a relatively unknown entity. Variations in heart rhythm from beat to beat are a result of nervous activity of both vagal fibers and sympathetic fibers. In the supine position, there is relatively little sympathetic nervous activity, making it possible to assess the degree of vagal modulation in the heart. Patients with CSC had lower vagal activity. The results are congruent with those of Tewari et al, being nearly statistically significant.4 A correlation between choroidal thickness and the LF/HF ratio seems to exist. It should be noted that measurements, although performed on the same ECG sample, are computed differently. The LF/HF ratio is derived from a fast Fourier transformation, which is a mathematical method used to determine the degree of vagal activity applied to the heart.
The main limitation of this study is that patients were included at least 3 months after the appearance of symptoms. This was due to the referral system in Denmark and, in part, deliberated to have the least “white-coat” syndrome that interfered with HRV measurements. Nervousness affects heart rate. To counteract this effect, patients were exposed to the same conditions. The delay in referral may have resulted in the inclusion of patients with CSC in a convalescence phase that may already have normalized HRV. This should have decreased the expected difference between the groups. Furthermore, our controls were slightly older, and HRV generally decreases with age. This may have reduced the difference between groups. Regarding the power calculation, Tewari et al had some extreme values of HRV in the healthy group perhaps suggesting that some results were biased by artefacts. This influenced our power estimate, which may simply have been too low. We calculate Cohen’s d to show if power was an issue. Since Cohen’s d takes into account n, the medium effect size of the SD2/SD1 ratio indicates that there is indeed an effect even if it is insignificant in terms of p-value, and therefore we are most likely to have committed a “type II error”. Moreover, Cohen’s d were not calculated for LF/HF-ratio so it is uncertain if a “type II error” had also occured here. Lastly, a difference in the thickness of the choroid was observed. This was expected and the lack of thickness would have indicated a flawed selection, as increased choroidal thickness is central to the CSC pathogenesis.10
Reservations should be made when interpreting the results with regard to causality given the cross-sectional nature of the study. Future studies are needed to elaborate on mechanistic and causal relations. The prospect of a possible link is attractive since vagal activity is modifiable, eg, electrical stimulation and physical activity, and thus may potentially offer a treatment option with less complications for CSC.11 Furthermore, patients may be able to monitor their own convalescence with smart wear, such as smartwatches and HR bands, using the link between HRV, cortisol, and CSC.12
Conclusion
Lower HRV is seen in patients with CSC. These results were borderline significant with a medium effect size. One out of four different HRV measurements was significantly correlated with choroidal thickness, which is indicative of a possible target for the treatment of CSC. There are indications that our study was underpowered. Future studies are warranted to investigate further. Given the progress of wearable technology, where patients can monitor HRV themselves, these results may be the first steps toward making self-monitoring a possibility for patients with CSC.
Data Sharing Statement
Data are available upon request.
Ethics Approval and Informed Consent
The project was approved by the Regional Committee of Ethics in Research of the Region of Zealand (jr. no. SJ-510) and the Danish Data Protection Agency (jr. no. REG-17-2016). Participants gave their oral and written informed consent prior to enrollment.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This project was funded by the Region Zealand Research Fund, Fight for Sight Denmark, and Synoptikfonden. The sponsors had no influence on the design or execution of the project or the decision to publish it.
Disclosure
CRM has previously received a travel grant from Bayer. CBM reports grants from Region of Zealand Research fund, Fight for Sight Denmark and Synoptikforeningen, during the conduct of the study; grants from Bayer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. van Rijssen TJ, van Dijk EHC, Yzer S, et al. Central serous chorioretinopathy: towards an evidence-based treatment guideline. Prog Retin Eye Res. 2019:73. doi:10.1016/j.preteyeres.2019.07.003
2. Vizzardi E, Regazzoni V, Caretta G, et al. Mineralocorticoid receptor antagonist in heart failure: past, present and future perspectives. Int J Cardiol Hear Vessel. 2014;3:6. doi:10.1016/J.IJCHV.2014.03.005
3. Zhang DY, Anderson AS. The Sympathetic Nervous System and Heart Failure. Cardiology Clinics. 2014;32(1):33–45. doi:10.1016/j.ccl.2013.09.010
4. Tewari HK, Gadia R, Kumar D, Venkatesh P, Garg SP. Sympathetic-parasympathetic activity and reactivity in central serous chorioretinopathy: a case-control study. Invest Ophthalmol Vis Sci. 2006;47(8):3474–3478. doi:10.1167/iovs.05-1246
5. Huang KH, Chen YH, Lee LC, et al. Relationship between heart failure and central serous chorioretinopathy: a cohort study in Taiwan. J Chinese Med Assoc. 2019;82(12):941–947. doi:10.1097/JCMA.0000000000000207
6. Zygmunt A, Stanczyk J. Methods of evaluation of autonomic nervous system function. Arch Med Sci. 2010;6(1):11–18. doi:10.5114/AOMS.2010.13500
7. Bernasconi P, Messmer E, Bernasconi A, Thölen A. Assessment of the sympatho-vagal interaction in central serous chorioretinopathy measured by power spectral analysis of heart rate variability. Graefes Arch Clin Exp Ophthalmol. 1998;236(8):571–576. doi:10.1007/s004170050123
8. Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Heal. 2017;5:258. doi:10.3389/fpubh.2017.00258
9. Wang M, Munch IC, Hasler PW, Prünte C, Larsen M. Central serous chorioretinopathy. Acta Ophthalmol. 2008;86(2):126–145. doi:10.1111/j.1600-0420.2007.00889.x
10. van Rijssen TJ, van Dijk EHC, Scholz P, et al. Patient characteristics of untreated chronic central serous chorioretinopathy patients with focal versus diffuse leakage. Graefe’s Arch Clin Exp Ophthalmol. 2019;257(7):1419–1425. doi:10.1007/s00417-019-04333-y
11. Yuan H, Silberstein SD. Vagus Nerve and Vagus Nerve Stimulation, a Comprehensive Review: part III. Headache. 2016;56(3):479–490. doi:10.1111/head.12649
12. Pellissier S, Dantzer C, Mondillon L, et al. Relationship between vagal tone, cortisol, TNF-alpha, epinephrine and negative affects in Crohn’s disease and irritable bowel syndrome. PLoS One. 2014;9(9):e105328. doi:10.1371/journal.pone.0105328
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.