Back to Journals » Risk Management and Healthcare Policy » Volume 12
Hearing threshold levels among steel industry workers in Samut Prakan, Thailand
Authors Kerdonfag P ![]() , Wadwongtham W, Taneepanichskul S
, Wadwongtham W, Taneepanichskul S
Received 20 February 2018
Accepted for publication 11 January 2019
Published 8 March 2019 Volume 2019:12 Pages 57—66
DOI https://doi.org/10.2147/RMHP.S166042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Kent Rondeau
Petcharat Kerdonfag,1,2 Winai Wadwongtham,3 Surasak Taneepanichskul2
1Ramathidodi School of Nursing, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2College of Public Health Sciences, Chulalongkorn University, Bangkok, Thailand; 3Department of Otolaryngology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Background: Industrial noise is generally considered from the perspective of environmental health and safety, with requirements for reduced occupational noise exposure, strict standards for hearing protection, and public health awareness campaigns.
Materials and methods: This cross-sectional study aimed to identify the hearing threshold levels (HTLs) among steel industry workers exposed to hazardous noises in Samut Prakan Province, Thailand, and investigate the associations between hearing loss and age and length of employment in the industry. Audiometric data for 93 participants were collected at the Samut Prakan Provincial Hospital. Qualified technicians performed audiometric screening using an audiometer in a quiet environment. Tests were conducted after participants had completely rested for ≥14 hours after the last exposure to workplace noise.
Results: The results showed that all participants had been employed in a work zone with a noise hazard for >1 year. Participants’ age ranged from 19 to 59 years and their work experience from 1 to 39 years. Average mean hearing thresholds in the right ear at 4, 6, and 8 kHz were 31.34, 29.62, and 25.64 dB, respectively. Mean hearing thresholds in the left ear at 4, 6, and 8 kHz were 40.15, 32.20, and 25.48 dB, respectively. Hearing loss related to work experience was greater than that attributable to age and work station. Duration of noise exposure ranged from 1 to 39 years, and more than half of the participants (60.2%) were exposed to hazardous noises from 6 to 25 years.
Conclusion: These findings show that participants’ age and experience were significantly associated with hearing loss at all levels. HTLs among industrial workers should be regularly assessed. At the health policy level, these workers need to start being protected when they begin working.
Keywords: hazardous noises, hearing threshold level, noise-induced hearing loss
Background
Sustained noise exposure can cause permanent hearing damage. Workplace noise is primarily considered from an environmental health and safety perspective rather than as a nuisance. Traditionally, workplace noise is regarded as a hazard linked to heavy industries such as the steel industry and associated with noise-induced hearing loss (NIHL). Currently, in terms of occupational health and safety, it is accepted that noise is hazardous to workers’ health in many areas of employment and by different means.1,2 Occupational NIHL is irreversible, and prevention, even in the early stages, is of the utmost importance.3
The NIHL caused by prolonged occupational noise exposure is characterized as sensorineural hearing loss, in which long periods of continuous noise exposure induce progressive and irreversible hearing loss in both ears. The pathophysiological basis of NIHL starts with acoustic signals entering the auditory system through the outer ear, pinna, and external ear canal. This funnel causes resonance that boosts the energy at high frequencies of ~2,000 Hz (heard as high pitches). The energy then reaches the eardrum and is transmitted through the middle ear by vibrating three tiny bones, called the ossicles. The eardrum and ossicles amplify the vibrations and carry them to the inner ear, called the cochlea, which contains a fluid-filled chamber inside the skull. These vibrations through the middle ear can be dampened when loud sounds cause contractions.4
The hair cells inside the cochlea are specialized sensory cells that can detect very soft sounds and tolerate loud sounds. Each person has only 16,000 or 17,000 of these cells, and damage to them is irreversible. Vibration from the middle to inner ear causes motion that stimulates the top portions of the hair cells, resulting in chemical changes that produce nerve impulses. These nerve impulses are carried along the auditory nerve to the brain, where they are interpreted as sound. The hearing sensitivity of young children with no hearing damage allows them to detect very soft sounds across a range of ~8–9 octaves.4
Loud noise is particularly harmful to the inner ear (cochlea). A one-time exposure to extremely loud sound or exposure to loud sounds for an extended period can cause hearing loss. Exposure to loud noise for an extended period can damage both cells and membranes in the cochlea and may destroy hair cells. Harmful effects of hearing loss can continue after noise exposure has stopped. Up to 30%–50% of hair cells can be damaged or destroyed before hearing loss occurs. This can be detected with an audiogram. When abnormal hearing loss is recognized, it is likely to be permanent.4As the threshold for NIHL is first reached at high frequencies (4–6 kHz) and expands to speech frequencies (0.5–3 kHz) in later phases, leading to verbal communication disorders and eventually functional loss of the middle ear.2 The Occupational Safety and Health Administration (OSHA) has established the presence of occupational noise exposure at/above 85 dB(A) as the threshold that requires the implementation of a hearing conservation program for workers.6,7 The components of hearing conservation programs include noise monitoring, noise control by engineering, administrative controls, worker education, provision of hearing protection equipment for workers, and periodic audiometric assessments. Evaluation of program efficacy is an essential component. Comparison of hearing threshold changes during exposure using periodic audiometric evaluation is an important program evaluation method.2
In 2006, the Thai government enacted a regulation that workers must not be exposed to noise over 90 dB(A) when working for 8 hours in a day. If exposure reaches 85 dB(A) throughout 8 hours of work, the employer needs to implement a workplace hearing conservation program.8,9 However, serious enforcement of workplace hearing conservation programs started in 2010. The effects of noise on Thai factory workers’ hearing were confirmed, and the standard for hearing loss prevention was subsequently enacted after many factories in Samut Prakan Province had been established. Most of these factories were established in the first era of factory-based industry in Thailand. This means that many workers in Samut Prakan continue to work in old-fashioned, less technologically advanced, noisier environments, in which it is difficult to engineer control of noise levels.
Hearing loss is associated with various factors,10–12 such as age,13,14 exposure to different sources of noise,15,16 and duration of exposure to noise.17 The hearing ability of male steel workers exposed to noise levels of 90–99 dB(A) has been shown to be significantly affected,18 with a mean shift of 6.8–7.8 dB after 6–8 years of exposure. Their levels of NIHL are significant at 4 kHz, which is a well-established clinical sign. This frequency is also speculated to be the typical notch frequency at which the largest magnitude of hearing loss is observed compared with that at other high frequencies.
An extensive literature review revealed that only a limited number of research studies on occupational NIHL were available in Thailand. The hearing threshold level (HTL) among steel industry workers needs to be clarified, and the factors related to this HTL need to be understood. The present study aimed to identify the HTL among steel industry workers in Samut Prakan Province, Thailand, and clarify the associations between hearing loss and age and length of employment among steel factory workers.
Materials and methods
Setting
The steel industry site is located in Samut Prakan Province in the central region of Thailand. Samut Prakan is situated at the estuary of the Chao Phraya River on the Gulf of Thailand. The west side of the river mostly consists of rice paddies, shrimp farms, and mangrove forests, while the eastern part is the urban center, including industrial factories. This area is considered part of the metropolis of Bangkok, Thailand’s capital city, and is an important source of raw materials from international and domestic warehouses. Many factories have been established in Samut Prakan Province over several decades since the first era of industry in Thailand.
Study design
The present study used a cross-sectional research design. Audiometric data from 93 participants who worked in zones with noise >85 dB(A) (designated as high noise zones) in two factories were collected from Samut Prakan Hospital records. Participants with audiometric data for 0.5, 1, 2, 3, 4, 6, and 8 kHz frequencies collected during October–December, 2016 were included in this sample. Audiometric data from this period were used in the statistical analysis.
Data collection
Data were collected from October to December 2016. Participants’ demographic data were obtained via a questionnaire. Data regarding the use of hearing protection devices (HPDs) were gathered by a self-report form, which was previously examined and confirmed by the present research team. Data on the participants’ HTLs were collected from the hospital’s audiometry records.
The audiometric data for 93 participants were collected at Samut Prakan Hospital, a provincial hospital. Audiometric testing was performed using an audiometer in an audiometric booth in a quiet environment. The HTLs were examined by a qualified occupational nurse. All participants were examined by the same examiners to ensure consistency. The tests were conducted after participants had fully rested for ≥14 hours after the last exposure to workplace noise. Audiometric air conduction tests were performed using a pure tone to the ear through earphones. The HTL (dB) was recorded at the frequency at which a specific tone was perceived 50% of the time. The better ear was first tested at 1 kHz and then at 2, 4, 6, 8, and 0.5 kHz, in that order. Audiometry tests were performed in the opposite ear in the same pattern, except for retesting at 1 kHz. The duration of the demonstrated tone was 1–3 seconds. The same interval was maintained across all tones. The total duration of the audiometry test was 3–5 minutes.
Noise exposure level
A Spark noise dosimeter (Model 706), with performance based on the ANSI S1.4-1983, ANSI S1.25-1991, IEC 60651-1993, IEC 60804-1993, and IEC 61252-1993 standards, was used. It was calibrated annually by the National Institute of Metrology (Thailand). Field calibration was done by the researchers before and after sampling. The noise dosimeter was set up with 90 dB(A) as the standard level, 5 dB as the exchange rate, and 80 dB(A) as the threshold level (reference). Individual noise levels were measured by the researchers once during working time for 8 hours because the production process was consistent. The microphone of the noise dosimeter was tapped in the hearing zone to measure each subject’s noise exposure level. The time–weight average throughout 8 hours was recorded in units of dB(A) by the dosimeter.
Ethical considerations
This study was reviewed and approved by the Institutional Review Board for Research Involving Human Research Subjects, Health Sciences Group, Chulalongkorn University. Participants were informed about the details of the study. In addition to confidentiality being assured, participants were informed that they can withdraw from the study at any time without having to give a reason. Informed consent for the study was obtained from all participants, who provided signed informed consent forms before participating in the study.
Data analysis
Data were analyzed with SPSS version 16.0 and reported using mean, SDs, ranges, frequencies, and percentages (as applicable). Line plots were used to show hearing thresholds at different frequencies. The associations of participants’ age and length of employment with hearing loss were assessed using chi-squared and t-tests, as applicable. Results were considered significant if the P-values were <0.05 (two-tailed).
Results
Participants’ characteristics
Participants’ demographic characteristics and selected variables are summarized in Table 1. All participants were men, and they were predominantly in middle age (mean age =41.67 years; SD =9.69 years, range 19–59 years). Their length of employment varied from 1 to 39 years (mean =13.99 years; SD =9.88 years). In addition, about one-third (31.0%) of participants had been exposed to a noise hazard in the workplace from 20 to 29.9 years, followed by 24.7% who had been exposed to a noise hazard for <5 years, and 20.4% with 10–19.9 years of exposure. Noise exposure levels ranged from 91.79 to 96.07 dB(A). Workers were asked how many hours per day and how many days per week they were exposed to high levels of noise. High level of noise was defined as a noise level causing them to shout to be heard by someone who was nearby but not immediately next to them. Participants reported mean noise exposure of at least 8 hours per day for 6 days per week in normal work conditions. The mean working hours was 59.09 hours per week (SD =6.42 hours), and the mean percentage of the time HPDs were used was 60.5% (SD =25.34%).
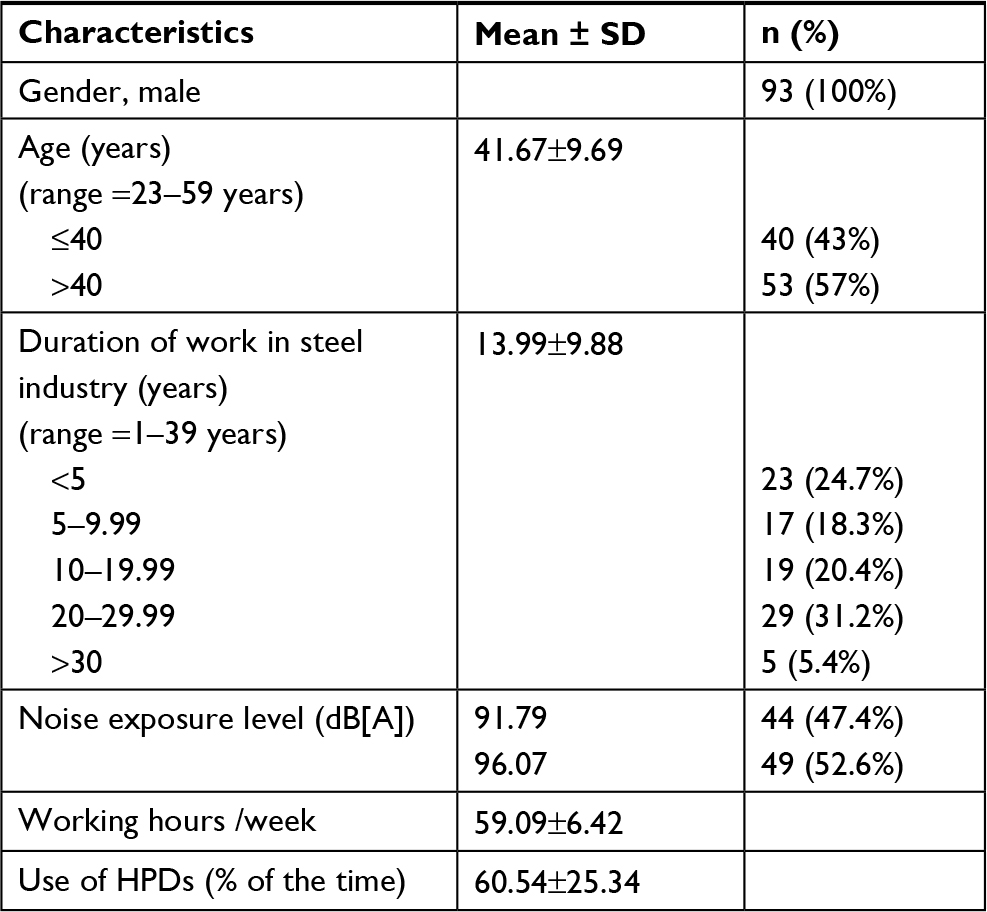 | Table 1 General characteristics of the study subjects (N=93) Abbreviation: HPDs, hearing protection devices. |
Participants’ HTLs
As regards hearing loss at single frequencies, participants’ HTLs were assessed based on audiometric data with possible dips or notches at 0.5, 1, 2, 3, 4, 6, and 8 kHz frequencies due to exposure to various noise levels. Table 2 shows the mean and SDs of HTLs for both ears and the worst ear at all test frequencies. Table 2 also shows abnormal hearing when using a HTL cutoff point of >25 dB. The number and percentage of those with abnormal hearing at single frequencies showed more variations at frequencies of 4, 6, and 8 kHz.
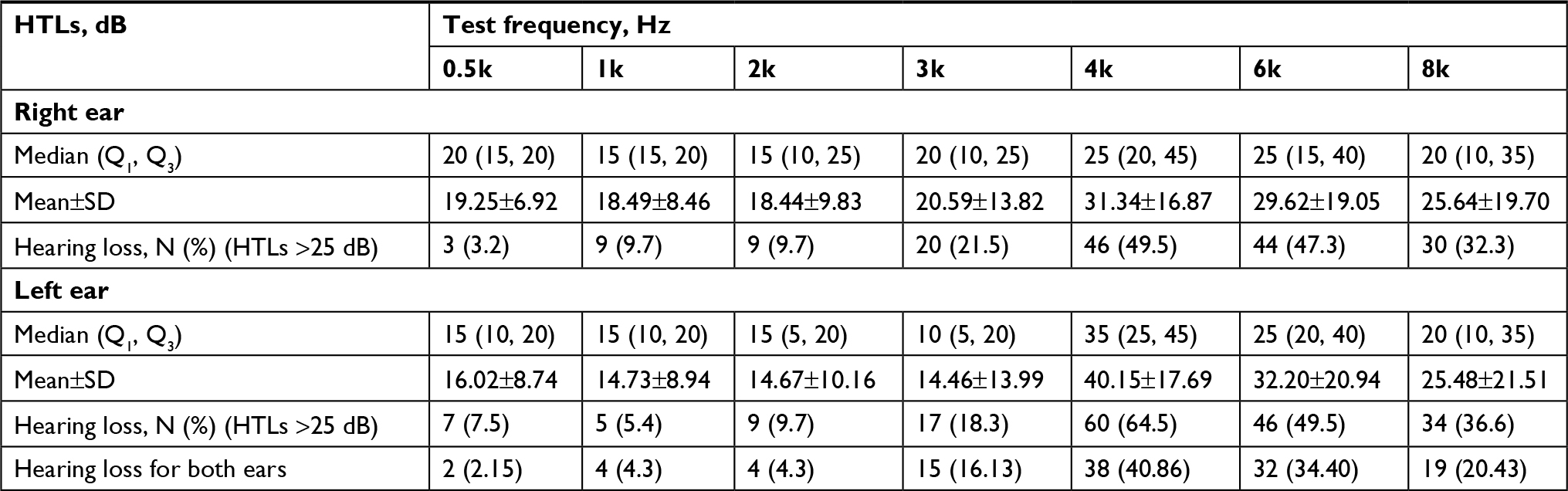 | Table 2 Hearing threshold level of subjects Abbreviation: HTLs, hearing threshold levels. |
As shown in Table 2, the prevalence of hearing loss increased at higher frequencies. More than 40% of the participants experienced hearing loss at 4 and 6 kHz. The mean HTLs for both ears at all frequencies are presented in Figure 1 to aid visualization of the trend across frequencies. Figure 1 shows that the mean HTLs were significantly increased at 4 kHz and deflated at 6 and 8 kHz. The mean HTLs in the higher frequency range (4–8 kHz) increased up to 25.48–40.15 dB.
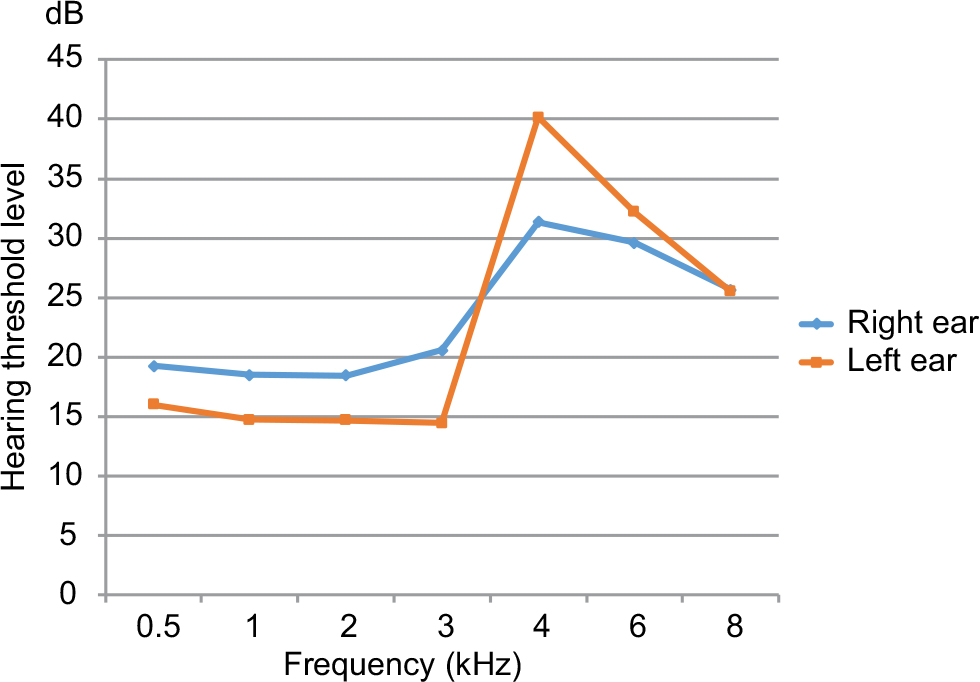 | Figure 1 Mean of hearing threshold level among steel industry workers at different frequencies. |
Figures 2 and 3 illustrate variation in hearing loss for all participants at all test frequencies by age and length of employment. The audiograms show bilateral hearing loss, with no hearing loss below fence frequencies (0.5, 1, 2, and 3 kHz), a perpendicular slope of hearing loss from 3 to 4 kHz, a notch at 4 kHz, and retrieval at 8 kHz for almost all subgroups. There was a clear notch at 4 kHz. Therefore, a Pearson’s chi-squared test was used to forecast the associations between hearing loss and different participant groups. When abnormal hearing occurred at high fence frequencies (ie, 4 and 6 kHz) as shown in Table 2, testing of the associations of participants’ age and work experience with their HTL used only high fence frequencies (ie, 4 and 6 kHz), as shown in Tables 3 and 4.
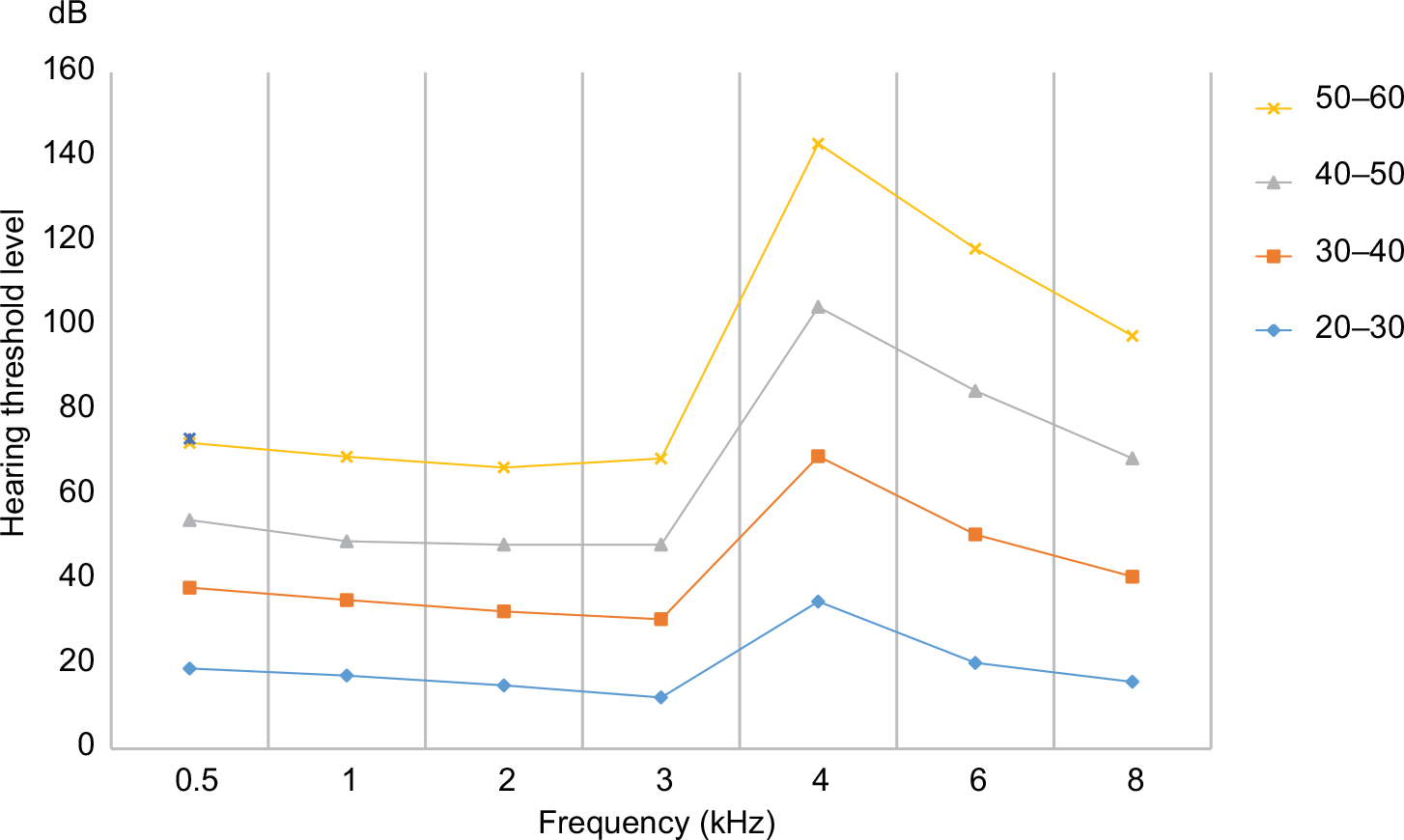 | Figure 2 Mean of hearing threshold level among steel industry workers at different ages. |
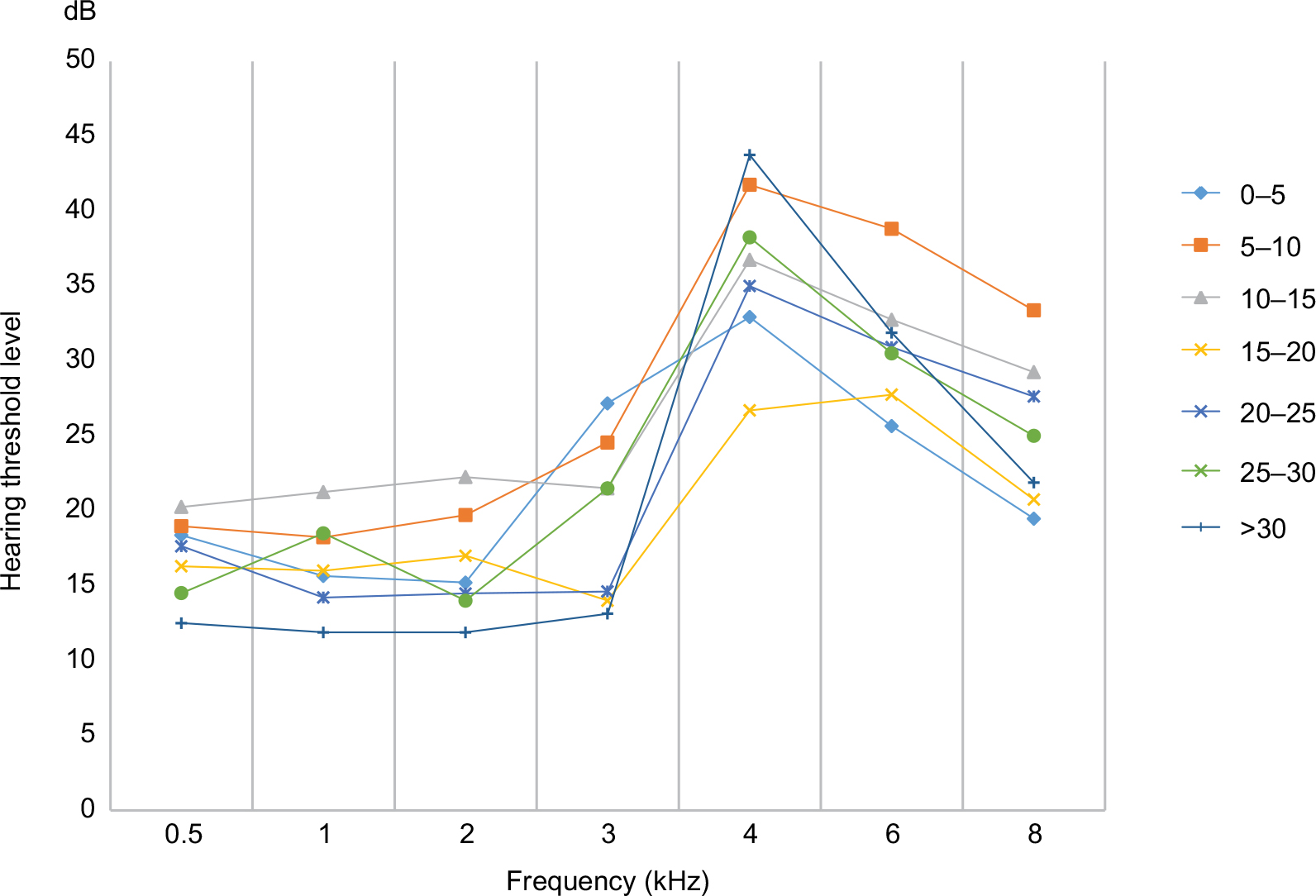 | Figure 3 Mean of hearing threshold level among steel industry workers for different lengths of employment. |
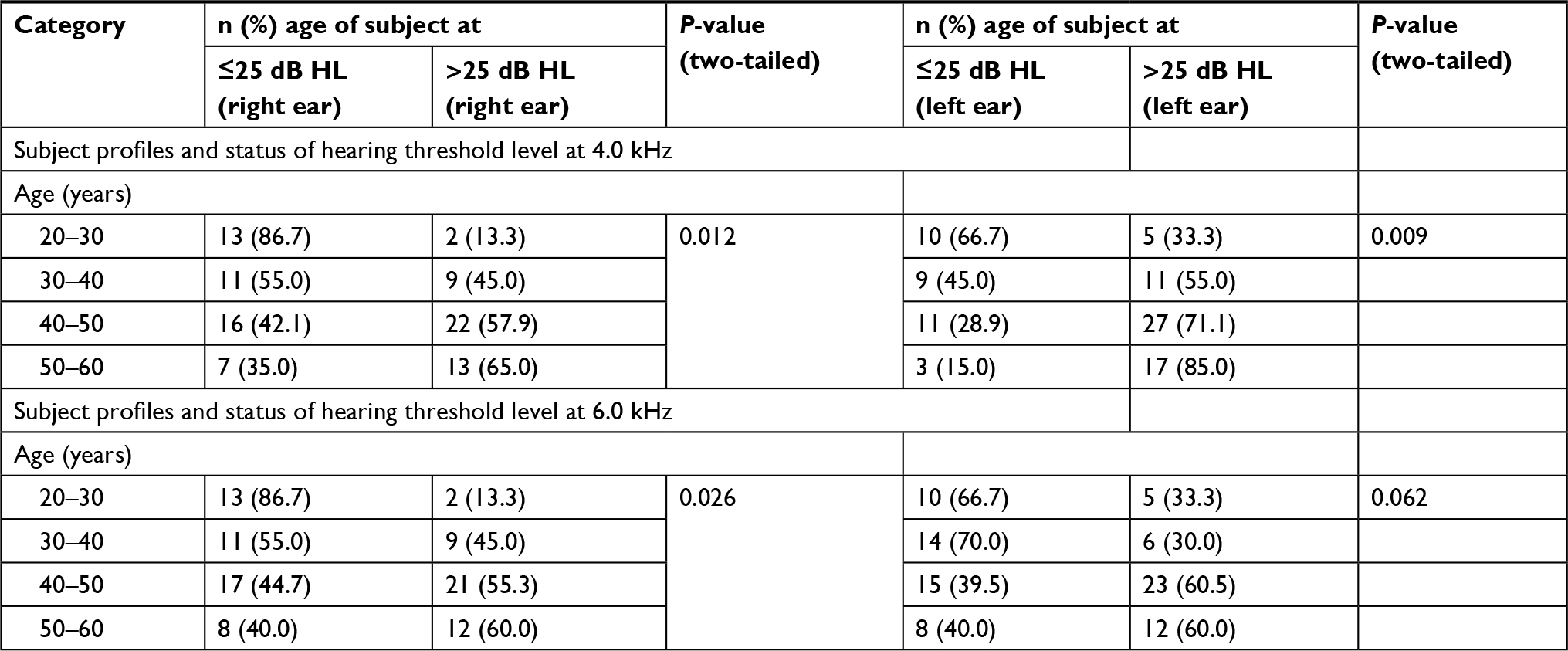 | Table 3 Pearson’s chi-squared test for age and hearing threshold level of subjects (n=93) Abbreviation: HL, hearing loss. |
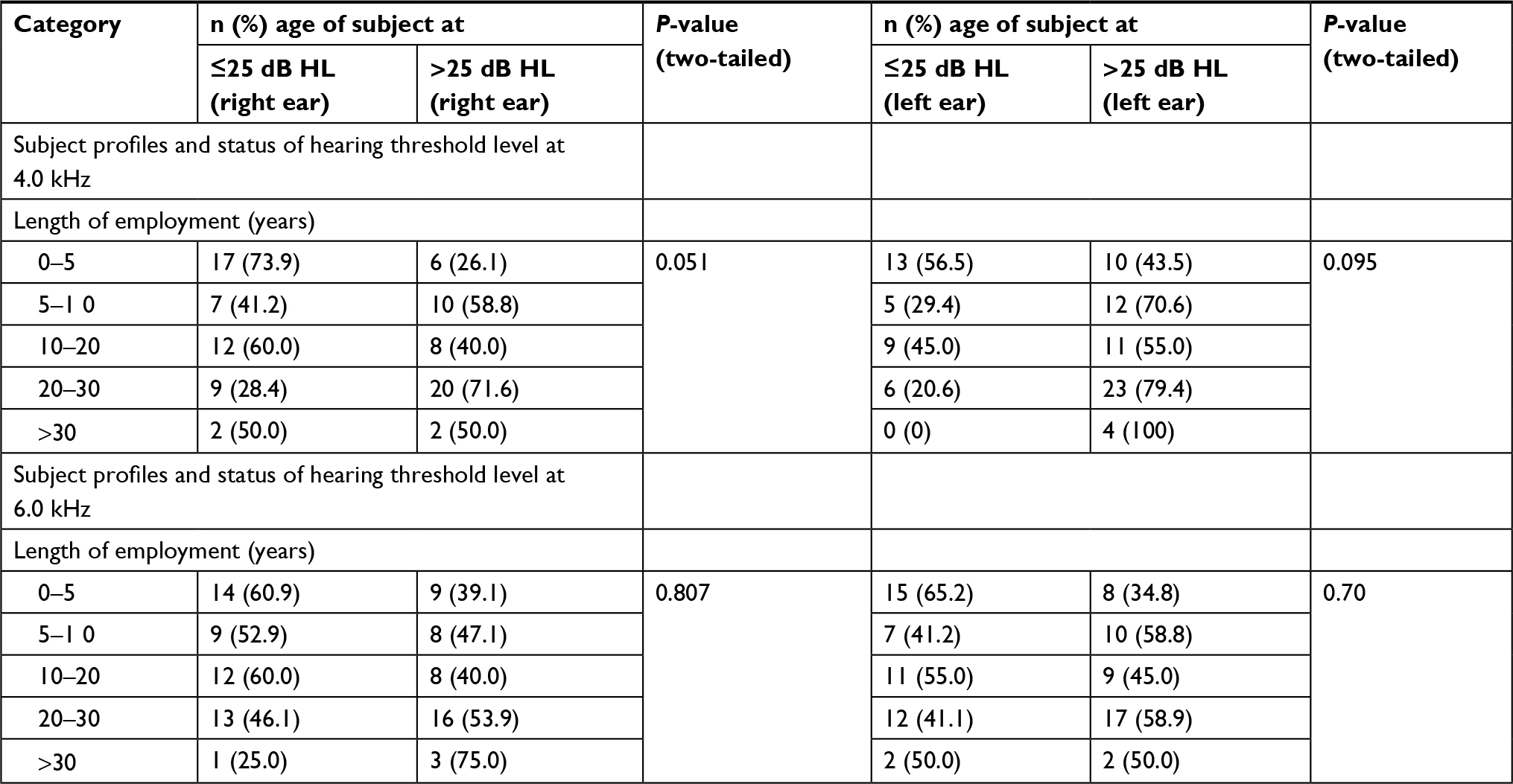 | Table 4 Pearson’s chi-squared test for the length of employment and hearing threshold level of subjects (n=93) Abbreviation: HL. |
Tables 3 and 4 show the chi-squared test results for each participant category. The HTLs of all participants were divided into two groups (≤25 dB HTL and >25 dB HTL) to identify the degree of hearing loss at 4 and 6 kHz and form an “n×k” table for the two demographic categories separately. Table 3 shows the increasing age of workers in the work zone, and a noise hazard was associated with higher HTLs at frequencies of 4 and 6 kHz (P=0.012 and P=0.026, respectively) in the right ear, but the association was significant only at 4 kHz (P=0.009) in the left ear. The chi-squared tests showed no association between HTL and length of employment at either of the test frequencies (4 and 6 kHz). Participants’ profiles with regard to length of employment and HTL are shown in Table 4.
To assess the trends of hearing loss by length of employment in the steel industry, the HTLs at a single test frequency and two indicators were divided into five length-of-employment categories (years): <5 years (n=23), 5–9.9 years (n=17), 10–19.9 years (n=20), 20–29.9 years (n=27), and ≥30 years (n=6). The hearing loss shown among steel industry workers with >9.9 years’ experience (mean age >40 years) had a characteristic sloping shape according to both noise and aging. Table 5 presents the scope of hearing loss at two groups of frequencies by length of employment in the steel industry and participants’ mean ages. The prevalence of hearing loss among those with longer length of employment in the steel industry was much higher than that among workers with fewer years of employment in the steel industry. As shown in Table 5, the majority of workers who had worked in the steel industry for longer than 19.9 years showed hearing loss at noise-sensitive frequencies (4–6 kHz). Among those with 20–29.9 years of employment, 26 of 27 steel workers (96.3%) had hearing loss at high frequencies, and 9 (33.3%) also had hearing loss at low frequencies. All six (100%) of those with over 30 years of employment in the steel industry had hearing loss at higher frequencies, and two (33.33%) also had hearing loss at low frequencies. This shows that longer duration of employment was associated with greater hearing loss at high frequencies.
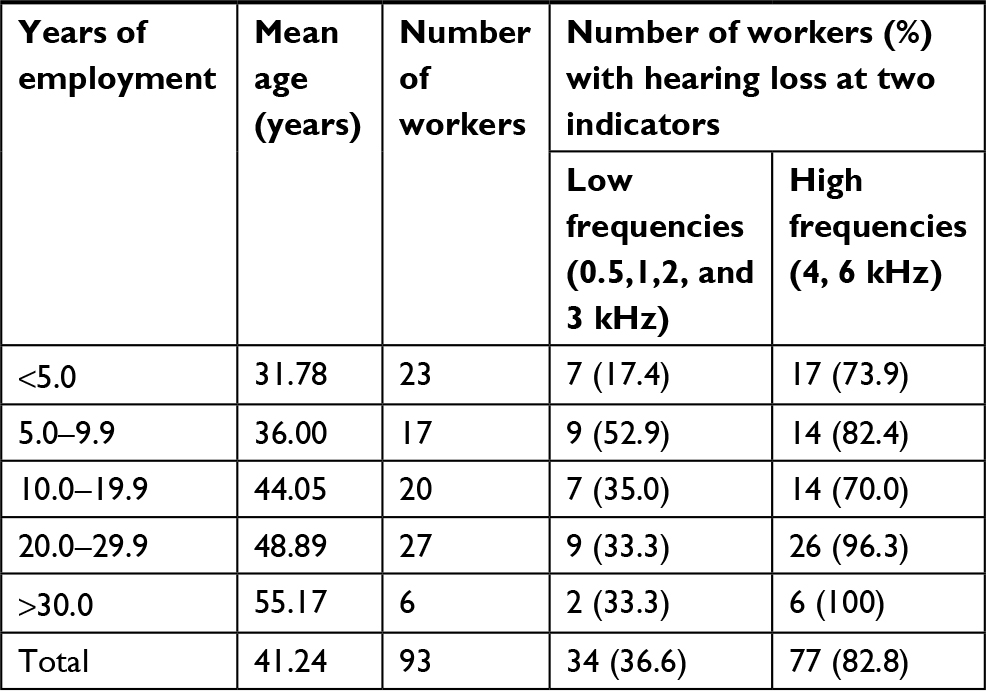 | Table 5 Prevalence of hearing loss at PTA (0.5, 1, 2, and 3 kHz) and PTA (4 and 6 kHz) by years in employment (N=93) Abbreviation: PTA, pure-tone threshold average. |
Discussion
This study’s results indicate that steel industry workers in designated higher noise zones had a high risk for NIHL caused by exposure to noise levels in the range 91.79–96.07 dB(A). These findings align with the results of the study by Chai et al19 who measured personal noise exposure in a steel cold rolling mill. Those results showed that the noise levels in steel rolling mills varied in the range 81–100 dB(A) between sections, but the noise exposure levels of all their participant groups were >85 dB(A). Those findings may suggest that steel workers were overexposed to noise during their work shifts. In addition, the mean number of weekly work hours among the steel workers in the present study was 59.09 (SD =6.42) hours, which could be a major contributing factor to their high noise exposure, as the OSHA recommends that workers’ exposure should not exceed 90 dB(A) for 8 hours per day.20 This might be related to the result that >80% of the steel industry workers in this study had hearing loss at noise-sensitive frequencies (4–6 kHz), with a mean HTL of ~31–40 dB. These findings are consistent with previous studies’ conclusions that occupational NIHL occurs primarily at high frequencies. For example, Çelik et al5 collected data from a hydroelectric power plant, focusing on 130 industrial workers who were exposed to high noise levels. The results revealed that the sensorineural hearing loss detected in 71 workers was bilateral, symmetrical, and mainly affected 4–6 kHz frequencies. The results of a study by Pourabdiyan et al,12 which investigated the hearing standard threshold shifts (STS) of Isfahan metal industry workers, showed that 29.9% of the workers had an STS. There were significant relationships between age, exposure time, noise level, and wearing time of HPDs. The strongest risk factors predicting hearing loss were noise exposure level and duration. Participants with noise exposure levels of at least 86 dB(A) had a statistically significantly higher chance of hearing loss. National Institute for Occupational Safety and Health limits occupational exposure to 85 dB(A) to protect against hearing loss.7 The American Conference of Governmental Industrial Hygienists proposed the same standard of a noise exposure level of 85 dB(A) for 8 working hours as the threshold value to protect workers from hearing loss.20 The OSHA recommends that noise exposure should not exceed 90 dB(A) throughout 8 hours of work and that the action level should be 85 dB(A) for 8 hours, which is the same as the Thai regulation.6,22 Furthermore, we found higher mean HTLs in the left ear than the in the right ear, which was consistent with the results of other studies; this might be attributable to greater sensitivity of the left ear or workers’ exposure to noise sources from the left side.2,23–26
There are no effective treatments for NIHL.3 However, it is preventable by promotion of the use of HPDs among workers who are exposed to long-term excessive noise to help decrease their intensity of noise exposure. The use of HPDs, recommended by National Institute for Occupational Safety and Health, has proven to be effective at NIHL prevention, but previous research has shown that workers did not consistently wear or use such helpful devices. For example, Brink et al27 revealed in cross-sectional multivariate analyses that years of employment, male gender, and proportion of time wearing HPDs were the factors that had the strongest associations with hearing loss (P<0.0001), controlling for age, transfer status (as a surrogate for previous noise exposure), race, and lifetime average noise exposure. The most consistent predictor of hearing loss in both univariate and multivariate analyses was the percentage of time having used HPDs during the workers’ tenure. Further, a study by Hong28 revealed that over 60% of workers showed hearing loss at the noise-sensitive higher frequencies of 4 and 6 kHz. In that study, HPDs were reported to be used for an average of 48% of the time during which they were required to be used. A significant inverse relationship was found between HPD use and hearing loss at higher frequency (4–6 kHz). Participants in the present study wore HPDs for only 60% of their working time. This finding indicates that the hearing conservation program for steel industry workers is ineffective. Moreover, data collected concerning the hearing conservation program’s training methods showed that there was no clearly defined format, and the program was only available to workers who had days off. Steel workers generally work overtime year-round, meaning that managers are the only workers who have time to participate in this training. This may be a reason why the hearing conservation program is not yet fully effective for this group. Although the Thai government enacted a regulation in 2006 stating that workers must not be exposed to noise over 90 dB(A) when working 8 hours in a day, serious implementation of workplace hearing conservation programs only started in 2010. In other words, action relating to this recommendation started in Thailand ~6 years before the present study’s data collection, whereas the participants’ mean length of employment was ~14 years, and the duration of employment ranged from 1 to 39 years. Therefore, the participants’ hearing loss likely started before workplace hearing conservation programs were first implemented. A cohort study is necessary to confirm this.
All workers who participated in this study were men. They worked long hours (mean: 59 hours per week). This suggests that these steel industry workers were overexposed to noise during their work shift, according to National Institute for Occupational Safety and Health, during which regular and continuous use of HPDs is required. Factors related to hearing loss include age, exposure time, and noise level. As indicated in Table 3, the chi-squared tests of independence demonstrated that hearing loss was dependent on age. According to this study’s findings, age over 40 years was a risk factor that may affect hearing loss. Johansson and Arlinger14 also reported a strong association between HTLs and age. They also showed that HTLs increased more rapidly in those aged over 50 years at frequencies over 3 kHz. Similarly, Edwards29 showed a strong association between hearing loss and age in a study conducted among gold miners. This study also indicated that hearing loss progressed in increasing 10-year age bins up to age 50–60 years.
Regarding length of employment, previous studies suggested that exposure to 85 dB(A) for 5 or more years increased the risk of hearing loss.7,9,30,31 This study indicated that employment duration exceeding 5 years tended to accelerate the severity of NIHL among steel workers. However, the association was not statistically significant, which was inconsistent with the findings of previous studies. This discrepancy might have resulted from the implementation of the preventive measure policy for hearing loss from 2010. However, hearing loss still tended to increase with length of employment. Previous studies such as that of Toppila et al32 also noted that impulsive noise appears to be more harmful to hearing at high noise exposure levels. In the present study, workers were often not protected from exposure to continuous or impulsive noise levels above 90 dB(A), so the prevalence of hearing loss was higher. Moreover, they worked for 60–72 hours per week, which was significantly longer than the prescribed numbers of working hours of 48 per week (as per the Indian Factory Act) or 40 per week (in the US and European countries). Thus, hearing loss was associated with overall occupational noise exposure and other risk factors similar to the findings reported by Ahmed et al.33 A similar finding that NIHL could be monitored at 4 kHz with occupational exposure exceeding 17 years in two bottling plants was reported by Abbate et al.16 However, the present study revealed that participants’ hearing loss at 4 kHz increased with every 5 years of work duration.
Strengths of this study
The main strength of this study was that HTL measurement was assessed using audiometry performed on Monday morning, which is the first day of the work week. This avoided the effects of temporary threshold shifts. In addition, all participants were examined by the same examiners to ensure consistency and validity.
Limitations and uncertainties
The limitations of this study included the data collection being conducted only at two steel factories in Thailand. Therefore, the findings cannot be generalized to other industries. In addition, this was a cross-sectional study, meaning that the findings could not show cause-and-effect relationships. Finally, only male workers in this high noise setting were selected, and certain technical limitations could not be avoided.
Conclusion
The age of steel workers in zones with high noise hazards was significantly associated with hearing loss at different levels. However, length of employment was not significantly associated with hearing loss in this population. The HTLs of industrial workers should be regularly assessed, and workers need to start being protected when they begin working in the industry. Occupational noise exposure can be minimized by efficient control measures such as engineering controls, administrative controls, and the use of HPDs. Often, engineering and administrative controls are not feasible in developing countries for technical and financial reasons. A complete hearing conservation program, including training, audiometry, job rotation, and the use of HPDs, is the most feasible means of protecting industrial workers from general workplace noise in the developing countries.
Acknowledgments
The authors thank the safety officer and all staff members of the participating factories for their support. The authors are also grateful to all of the workers who participated in this study. This study was supported by funds made available from the 90th Anniversary of the Chulalongkorn University Fund; Ramathibodi School of Nursing, Faculty of Medicine, Ramathibodi Hospital, Mahidol University; the National Research Council of Thailand (NRCT); and the Ratchadapisak Sompoch Fund (2015), Chulalongkorn University (CU-58-007-AS). The abstract of this paper was presented at the 19th International Conference on Occupational Health and Safety in 2017 as an oral presentation with interim findings. The oral abstract was published in the Conference Proceedings of the 19th World Academy of Science, Engineering and Technology Conference; Dec 18–19, 2017.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Agarwal G, Nagpure PS, Gadge SV. Noise induced hearing loss in steel factory workers. Int J Occup Saf Health. 2016;4(2):34–43. | ||
Attarchi M, Sadeghi Z, Dehghan F, Sohrabi M, Mohammadi S. Assessment of hearing standard threshold shift based on audiometric findings in steel company workers. Iran Red Crescent Med J. 2010;12(6):644–649. | ||
Cloeren M, Gean C, Kesler D, et al. American College of occupational and environmental medicine’s occupational and environmental medicine competencies-2014. J Occup Environ Med. 2014;56(5):e21–e40. | ||
New US Department of Health and Human Services. Loud Noise Can Cause Hearing Loss [Online]. 2017. Available from: https://www.cdc.gov/nceh/hearing_loss/how_does_loud_noise_cause_hearing_loss.html. Accessed July 28, 2018. | ||
Çelik O, Yalçin S, Oztürk A. Hearing parameters in noise exposed industrial workers. Auris Nasus Larynx. 1998;25(4):369–375. | ||
OSHA (Occupational Safety and Health Administration). Occupational noise exposure limits [Online]. 1991. Available from: https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=9735. Accessed March 6, 2012. | ||
NIOSH (National Institute for Occupational Safety and Health). Occupational noise exposure. DHHS (NIOSH) Publication No. 98-126 [Online]. 1998. Available from: http:// www.cdc.gov/niosh/docs/98-126/. Accessed March 6, 2012. | ||
Morata TC, Byrne DC, Rabinowitz PM. Noise exposure and hearing disorders. In: Levy BS, Wegman DH, Baron SL, Sokas RK, editors. Occupational and Environmental Health Recognizing and Preventing Disease and Injury. 6th ed. New York: Oxford University Press; 2011:461–475. | ||
US Department of Health and Human Services. Criteria for a recommended standard Occupational Noise Exposure Revised Criteria 1998 [Online]. 1998. Available from: www.cdc. gov/niosh/docs/98-126/pdfs/98-126.pdf. Accessed March 6, 2012. | ||
Borchgrevink HM. Does health promotion work in relation to noise? Noise Health. 2003;5(18):25–30. | ||
Joshi S, Devkota S, Chamling S, Shrestha S. Environmental noise induced hearing loss in Nepal. Noise Health. 2005;7(29):42. | ||
Pourabdiyan S, Ghotbi M, Yousefi H, Habibi E, Zare M. The epidemiologic study on hearing standard threshold shift using audiometric data and noise level among workers of Isfehan metal industry. Koomesh. 2009;10(4):253–260. | ||
Kim HN, Kim SG, Lee HK, et al. Incidence of Presbycusis of Korean populations in Seoul, Kyunggi and Kangwon provinces. J Korean Med Sci. 2000;15(5):580–584. | ||
Johansson MSK, Arlinger SD. Hearing threshold levels for an otologically unscreened, non-occupationally noise-exposed population in Sweden. Int J Audiol. 2002;41(3):180–194. | ||
Amedofu GK. Hearing-impairment among workers in a surface gold mining company in Ghana. Afr J Hlth Sci. 2002;9:91–97. | ||
Abbate C, Concetto G, Fortunato M, et al. Influence of environmental factors on the evolution of industrial noise-induced hearing loss. Environ Monit Assess. 2005;107(1–3):351–361. | ||
McBride DI, Williams S. Audiometric Notch as a sign of noise induced hearing loss. Occup Environ Med. 2001;58(1):46–51. | ||
Howell RW. A seven-year review of measured hearing levels in male manual steelworkers with high initial thresholds. Occup Environ Med. 1978;35(1):27–31. | ||
Chai DL, Lü JQ, Zeng L, Su YG, Lei Z, Zhao YM. [Measurement of personal noise exposure in a cold rolling mill]. Zhonghua Yu Fang Yi Xue Za Zhi. 2006;40(2):93–96. Chinese. | ||
Singh LP, Bhardwaj A, Deepak KK. Occupational exposure in small and medium scale industry with specific reference to heat and noise. Noise Health. 2010;12(46):37. | ||
ACGIH (American Conference of Governmental Industrial Hygiene). TLVs and BEIs. USA: Signature Publications; 2011. | ||
Department of Labour Protection and Welfare. Ministerial regulation on the prescribing of standard for administration and management of occupational safety, health and environment in relation to heat, light and noise B.E. 2549 [Online]. 2006. Available from: ble from: http://www.shawpat.or.th/index.php?option=com_phocadownload&view=category&id=12%3A ministerial-regulation&Itemid=15. Accessed March 20, 2012. | ||
Simpson TH, McDonald D, Stewart M. Factors affecting laterality of standard threshold shift in occupational hearing conservation programs. Ear Hear. 1993;14(5):322–331. | ||
Broste SK, Hansen DA, Strand RL, Stueland DT. Hearing loss among high school farm students. Am J Public Health. 1989;79(5):619–622. | ||
Marvel ME, Pratt DS, Marvel LH, Regan M, May JJ. Occupational hearing loss in New York dairy farmers. Am J Ind Med. 1991;20(4):517–531. | ||
Pirilä T, Jounio-Ervasti K, Surri M. Left-right asymmetries in hearing threshold levels in three age groups of a random population. Int J Audiol. 1992;31(3):150–161. | ||
Brink LL, Talbott EO, Burks JA, Palmer CV. Changes over time in audiometric thresholds in a group of automobile stamping and assembly workers with a hearing conservation program. AIHA J (Fairfax, Va). 2002;63(4):482–487. | ||
Hong O. Hearing loss among operating engineers in American construction industry. Int Arc OccupEnviron Health. 2005;78(7):565–574. | ||
Edwards AK. Characteristics of noise-induced hearing loss in gold miners [master’s thesis]. Pretoria: University of Pretoria; 2008. | ||
Thamasunthorn A. Audiometric test [Online]. 2012. Available from: http://i-medipro.com.www.readyplanet. net/_m/article/content/content.php?aid=70931. Accessed April 2, 2012. | ||
Sriopas A, Chapman RS, Sutammasa S, Siriwong W. Occupational noise-induced hearing loss in auto part factory workers in welding units in Thailand. J Occup Health. 2017;59(1):55–62. | ||
Toppila E, Pyykkö I, Starck J, Kaksonen R, Ishizaki H. Individual risk factors in the development of noise-induced hearing loss. Noise Health. 2000;2(8):59–70. | ||
Ahmed HO, Dennis JH, Badran O, Ahmad HO, et al. Occupational noise exposure and hearing loss of workers in two plants in eastern Saudi Arabia. Ann Occup Hyg. 2001;45(5):371–380. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.