Back to Journals » Psychology Research and Behavior Management » Volume 14
Healthy Behavior as a Mediator in the Relationship Between Optimism and Life Satisfaction in Health Sciences Students: A Cross-Sectional Study
Authors Rogowska AM ![]() , Nowak PF
, Nowak PF ![]() , Kwaśnicka A
, Kwaśnicka A ![]()
Received 20 August 2021
Accepted for publication 19 October 2021
Published 24 November 2021 Volume 2021:14 Pages 1877—1888
DOI https://doi.org/10.2147/PRBM.S335187
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Aleksandra M Rogowska,1 Paweł F Nowak,2 Aleksandra Kwaśnicka1
1Institute of Psychology, University of Opole, Opole, Poland; 2Faculty of Physical Education and Physiotherapy, Opole University of Technology, Opole, Poland
Correspondence: Aleksandra M Rogowska
Institute of Psychology, University of Opole, ul. Staszica 1, Room 312, Opole, 45-052, Poland
Tel +48 604732259
Email [email protected]
Purpose: This study examines the indirect relationship between optimism and life satisfaction via healthy behavior among health sciences students.
Participants and Methods: The cross-sectional study involved 349 health sciences students, including 58% of women, ranging in age between 19 and 30 years (M = 22.15, SD = 1.83). Self-report questionnaires were used to measure dispositional optimism (the Life Orientation Test-Revised, LOT-R), life satisfaction (Satisfaction with Life Scale, SWLS), and health behaviors (Health Behavior Inventory, HBI), with four subscales: healthy diet (HD), preventive behavior (PB), positive mental attitudes (PMA), and healthy practices (HP). In addition, a single mediation model (with the total HBI as mediator) was compared with a parallel mediation model (with four subscales of the HBI). Gender was controlled as a confounding variable.
Results: Women scored higher in the total HBI (p < 0.01), HD (p < 0.001) and PB (p < 0.01) than men, while men scored slightly higher in dispositional optimism (p < 0.01). General health behavior (total HBI) completely mediates the relationship between dispositional optimism and life satisfaction, R2 = 0.32. In the parallel model, only PMA was determined as a mediator of the association between dispositional optimism and satisfaction with life, R2 = 0.36. The single mediation model showed perfect fit (X2/df = 0.00, RMSEA = 0.00, SRMR = 0.00, CFI = 1.00, IFI = 1.00, NFI = 1.00), better than the parallel mediation model (X2/df = 2.353, p = 0.095, RMSEA = 0.062, SRMR = 0.020, CFI = 0.995, IFI = 995, NFI = 991).
Conclusion: The interplay mechanism between personal resources and behavioral health-related habits may explain 32% of life satisfaction variance. The intervention focused on increasing optimistic expectancies and health behaviors should be implemented in universities to increase students’ well-being and prevent depression.
Keywords: college and university students, dispositional optimism, life satisfaction, optimistic expectancies, subjective well-being, SWB, mediation analysis
Introduction
Subjective well-being determines longevity as well as physical and mental health. One of the subjective well-being (SWB) dimensions is satisfaction with life, considered as explicit and conscious evaluations of peoples’ lives, often based on factors that the individual deems relevant. Diener et al claim that satisfaction with life is an overall assessment of satisfaction with one’s achievements and living conditions. Subjective assessment of life satisfaction results from the complex interplay of culture, personality, cognitions, goals and resources, and the objective environment.2 The concept of SWB also involves experiencing high levels of pleasant emotions and moods and low levels of negative emotions and moods.3
People who are satisfied with their lives are usually optimistic about the future. Dispositional optimism is a cognitive-affective construct understood as a dimension of individual differences that describes the extent to which people hold generalized favorable expectancies for their future.4 Optimistic life orientation plays a vital role in motivation-relevant outcomes in various life situations. In an academic context, greater optimism predicts a greater likelihood of high grades, completing college, and high salaries years later. In general, greater optimism predicts greater career success, better social relations, and better health.5 An explanation of this phenomenon is that optimists seem more persistent in their academic and professional efforts over time. Optimistic people expect success and good things to happen, while pessimists expect defeat and bad outcomes.4 Dispositional optimism seems relatively independent of gender and age.6–8 Numerous studies showed beneficial effects of optimism on well-being and a positive association between dispositional optimism and life satisfaction.9–15
Another determinant of good health and well-being is leading a healthy lifestyle. Health behavior is any activity undertaken to prevent or detect disease or to improve health and well-being.16 Studies suggest that university students are at high risk of an unhealthy lifestyle, including high psychological stress, low physical activity (PA), poor diet, poor sleep, inappropriate body mass index, excessive and binge drinking, smoking cigarettes, and illicit substances use and abuse.17–20 At the same time, particular health-related behaviors (such as dieting, exercising, lack of smoking, and sleeping enough) correlate.21,22 Therefore, it is worth researching health behavior to find a comprehensive model of behaviors that determine good health. Research suggests that health conditions can have a significant impact on well-being outcomes.23 In particular, the well-being of students is related to their physical activity (PA).22 Numerous studies showed a positive relationship between life satisfaction and various health-related behaviors.24–27 Healthy behaviors, considered protective factors for various diseases, are positively related to dispositional optimism.4,5,28–30
There is a relationship between life satisfaction, dispositional optimism, and health behavior. Previous studies have indicated that both optimism and healthy behavior increase life satisfaction. According to the expectancy theory,31 positive expectancies regarding future outcomes increase motivation to exert effort, goal engagement, overcome obstacles and increase commitment. Thus, optimism is somewhat similar to hope, attribution style, and self-efficacy.5 Positive expectations may be explained in light of the following three theories: 1) selective information processing (focusing on the positive aspects of behavior); 2) the internal locus of control as a factor responsible for success; and 3) an attribution style based on a stable and internal cause of achievement.32 Das et al33 classified four SWB theories: fulfillment and engagement theories, personal orientation theories, evaluative theories, and emotional theories. Oishi et al3 suggest that genetic, situational, goal, and coping approaches are complementary rather than incompatible, and they need to be integrated. In particular, research is needed to examine the interaction of personality and environmental factors on life satisfaction.
Among the determinants of SWB, personality and health play a crucial role. Commitment to achieving important goals is a central aspect of SWB in fulfillment and engagement theories.34 Diener et al35 considered a possible mediation role of health behaviors in SWB and healthy relationships. Scheier and Carver36 also suggested health habits as a potential behavioral mechanism that explains optimistic people’s better health outcomes. However, to the best of our knowledge, the link between optimism and SWB through healthy behavior was never explored. According to the self-regulation model of goal-directed activity,37 an optimistic general outcome expectancy sustains effort toward achieving goals. Optimists may develop more adaptive health habits in disease (eg, by following a prescribed medical regimen, altering the behaviors producing the illness) and believe that they benefit from this behavior, which may increase well-being.36 Due to the general expectancy theory,36 the positive expectancy process affects physical well-being and health in various ways, like engaging in PA, coping with pain, or involving self-efficacy expectancy. Assuming that health is one of an individual’s vital goals, it seems to justify, in the view of engagement and personality theory, that dispositional optimism may increase motivation to engage in health-related behaviors, which can facilitate the achievements of good health status and longevity outcomes, which in result increases life satisfaction.
The biopsychosocial model explains the dynamic and complex interaction between physiological, psychological, and social factors that cause and effect on health.38 Recent research39 confirmed that SWB is well adjusted to the biopsychosocial model of well-being. Therefore, SWB was examined as a complex of four lower-level factors (negative and positive emotional reactions as a biological factor, life satisfaction as a psychological factor, and harmony in life as a social factor) that contribute to the general factor of SWB on a higher level in the bi-factor structure.
On the other hand, Scheier and Carver40 reviewed the scientific literature to investigate how dispositional optimism predicts excellent physical well-being. The study found considerable evidence that optimists who have better diets (eg, eat more fruits and vegetables) are more physically active and are more likely to consume alcohol moderately, while pessimists are more likely to be smokers and suffer from substance abuse problems. Scheier and Carver40 proposed a biobehavioral model of health and well-being (eg, Andersen et al41) to explain the interplay mechanism between behavior and biology in promoting or inhibiting disease. According to this model, dispositional optimism can operate concurrently along two pathways: one pathway leads through health-promoting and damaging health behaviors. In contrast, the second pathway regards psychosocial factors that determine the kinds of health behaviors a person will engage in. However, the mediating effect of health behaviors on the relationship between optimism and objective physical health outcomes was never tested. For the first time, a biobehavioral health model will be adopted to explain the association between dispositional optimism (also considered as general outcome expectancies) and life satisfaction, which is thought to be mediated by health-related behaviors.
Various mediators were considered previously in the relationship between dispositional optimism and life satisfaction. Research suggests that dispositional optimism facilitates subjective well-being and good health, and coping behaviors may mediate the relationships between these variables.42 Oriol et al15 suggest that dispositional optimism may increase subjective well-being through different affective and cognitive mechanisms. The study found the mediating effect of grit, gratitude, and meaning in life on university students’ well-being. However, to the best of our knowledge, health behaviors were never considered mediators in the association between dispositional optimism and life satisfaction.
This study examines the mediator role of health behaviors in the association between dispositional optimism and life satisfaction. A review of the literature presented above suggests that this assumption is fully justified. It was previously found that optimistic expectancies and health-related behaviors can positively predict life satisfaction, and dispositional optimism is a positive predictor of healthy behavior. Therefore, we hypothesize that health behavior plays the role of a mediator in the relationship between dispositional optimism (considered a personality trait) and life satisfaction (as one of the dimensions of SWB), based on previous suggestions Deiner et al35 or Scheier and Carver36,40 as well as on the biobehavioral model of health and well-being.41 Furthermore, we assume that people vary inter- and intra-individually in health habits and practices, depending on preferences and motivation, so they engage in particular health-related behaviors with various strengths. Therefore, two mediation models will be compared: single, with a global assessment of health behaviors (the total HBI), and parallel, when health-related behavior is divided into four specific types: healthy diet, preventive behavior, positive mental attitudes, and healthy practices. Because sex was previously a significant factor in health behaviors, gender will be controlled for in this study.
Materials and Methods
Study Design and Procedure
A cross-sectional study was conducted in December 2020 at the following universities: Warsaw Medical University and University of Rzeszów. With the lecturers’ consent, the respondents completed the paper-and-pencil questionnaires at the end of their university lectures. The average time of data collection was 20 minutes. Neither form of compensation was offered as an incentive to participate. The student sample consists of representatives of both genders (male and female) and five faculties (nursing, obstetrics, medical rescue service, public health, and physical education) to minimize bias sources. Students were aware of the aim and content of the survey and that they could withdraw from the study at any time without providing a reason. All questionnaires were completed and returned. The G*Power 3.1 software was used to calculate a priori sample size for Student’s t-test (with Cohen’s d = 0.5, p < 0.05, and 95% CI) and for biserial correlations (with r = 0.3, p < 0.05, and 95% CI). The minimal sample size was 174 for the t-test and 115 for correlations.
Ethics Statement
The Research Ethics Committee approved the study protocol at the University of Opole, Poland (8/2020). The study followed the ethical requirements of anonymity and voluntariness of participation. Following the Helsinki Declaration, written informed consent was obtained from each student before inclusion. The authors of the study received no specific funding for this work.
Participants
There were no specific inclusion criteria besides being a student of the Health Sciences faculty. The total sample initially included 360 participants, but five people declined to participate in the study, and six surveys were incomplete, so excluded from the further analysis. The final study sample consisted of N = 349 health sciences students, ranging between 19 and 30 years (M = 22.15, SD = 1.83). Most students were females (n = 202, 58% of the total sample) of normal weight (n = 171, 78%). Participants studied in one of the five faculties: Nursing (n = 79, 23%), Obstetrics (n = 52, 15%), Public Health (n = 43, 12%), Medical Rescue Service (n = 77, 22%), and Physical Education (n = 98, 28%). Details are shown in Table 1.
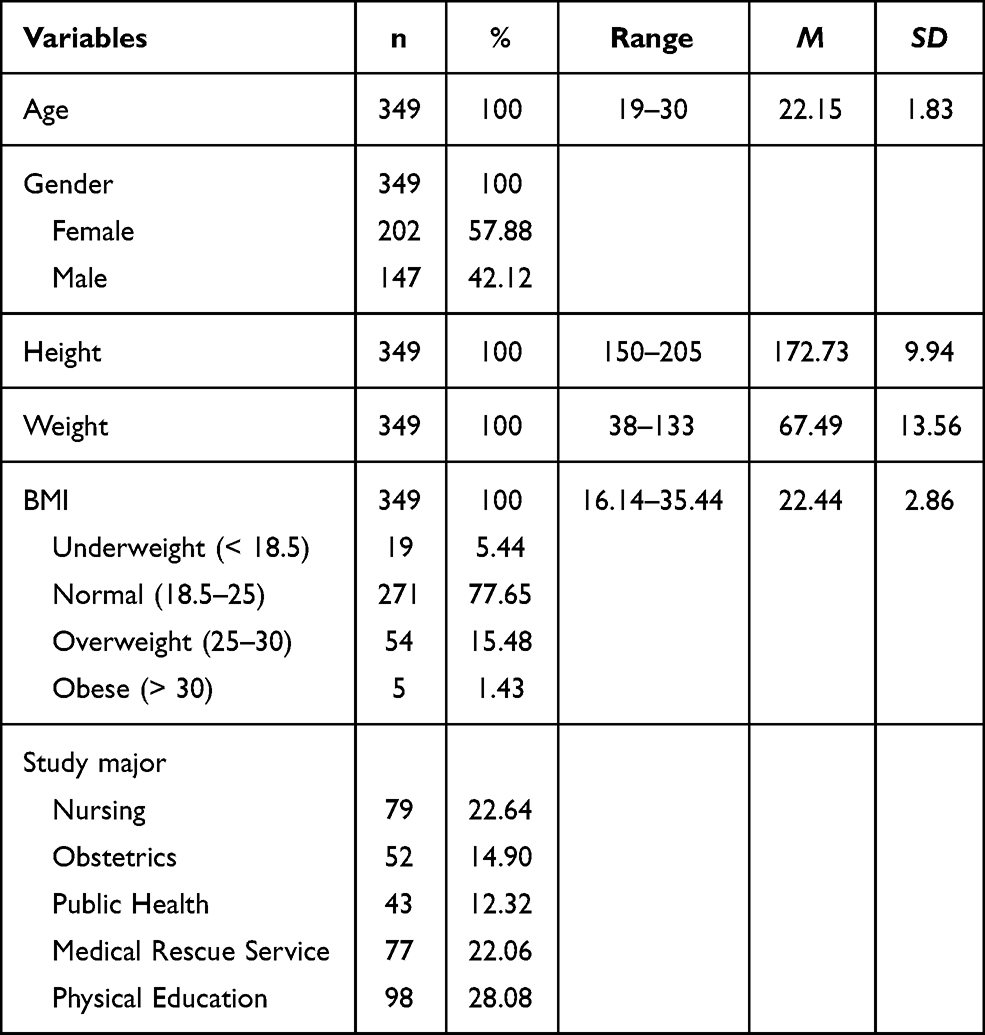 |
Table 1 Sample Characteristics |
Measures
Life Satisfaction
Satisfaction with Life Scale (SWLS) is a short 5-item scale developed as a global cognitive judgment of satisfaction with one’s life.1,31 Respondents indicate, using a 7-point Likert-type scale (ranging from 1 = Strongly disagree, to 7 = Strongly agree), how much they agreed or disagreed with each of the five items. An example of an item is: “The conditions of my life are Excellent.” Total scores (sum of all five items) ranged between 5 and 35, with higher scores suggesting greater life satisfaction. The ranges of scores may be interpreted as Extremely dissatisfied (5–9), Dissatisfied (10–14), Slightly dissatisfied (15–19), Neutral (20), Slightly satisfied (21–25), Satisfied (26–30), and Extremely satisfied (31–35). The scale shows good convergent and discriminant validity with other emotional well-being scales.43 The reliability assessed by Cronbach’s α was 0.81 in the Polish adaptation44 and 0.84 in the current study.
Dispositional Optimism
The Life Orientation Test – Revised (LOT-R) was developed to assess individual differences in generalized optimistic expectancy.45 The LOT-R is a brief 10-item measure, with a three-item optimism subscale, three-item pessimism subscale, and four items serving as fillers (Items 2, 5, 6, and 8). Respondents rate each item on a 4-point Likert scale (0 = Strongly disagree, 1 = Disagree, 2 = Neutral, 3 = Agree, and 4 = Strongly agree). An example of an item is: “In uncertain times, I usually expect the best.” The pessimism’s items (eg, “If something can go wrong for me, it will”) are reverse scored, and then all six items are summarized, ranging from 0 to 24, with higher scores indicating higher optimism. This tool was translated and adapted in several languages and cultures. In this study, dispositional optimism will be considered as a single bipolar trait, which the authors of the LOT-R5 recommended, and was confirmed as a validating approach in the view of the confirmatory factor analysis (CFA).46,47 Cronbach’s α for the entire six scale items was 0.78 in the original study45 and 0.76 in Polish adaptation. In the present study, Cronbach’s α was 0.77.
Health Behaviors
Juczyński44 developed the Health Behavior Inventory (HBI) by elaborating on two previous tools: the General Preventative Health Behaviors Checklist48 and the Reported Health Behaviors Checklist.49 The HBI is a self-reported questionnaire consisting of 25 statements describing various health-related behaviors. Participants rate on a 5-degree Likert scale (1 = Almost never, 2 = Rarely, 3 = From time to time, 4 = Often, and 5 = Nearly always), how frequent given behavior is performed. The total score of the HBI is a sum of all answers, ranging from 24 to 120 points, and a higher total HBI score means a healthier behavior. The HBI consists of four subscales (including six items in each): Healthy Diet (HD; type of foods, well-balanced diet; eg, “I limit the consumption of products such as animal fats, sugar”), Preventive Behavior (PB; health recommendations, health, and disease information; eg, “I regularly attend medical examinations”), Positive Mental Attitudes (PMA; psychological factors, such as avoiding too strong emotions, stress, anxiety, and depressive situations; eg, “I avoid situations that depress me”), and Healthy Practices (HP; sleep habits, recreation, and physical activity; eg, “I have enough rest”). The questionnaire’s reliability in the original version was satisfactory for the total HBI (Cronbach’s α = 0.85) and acceptable for subscales, with Cronbach’s α ranging between 0.60 and.65.44 In the present study, the internal consistency was also satisfactory, with Cronbach’s α = 0.87 for the total HBI, but lower for the HD, PB, PMA, and the HP subscales (with Cronbach’s α of 0.82, 0.64, 0.74, and 0.60, respectively).
Statistical Analysis
Six questionnaires were excluded from statistical analysis because of incomplete data. Among the remaining 349 questionnaires, less than 5% of missing data were replaced by means. The reliability of the SWLS, LOT-R, and HBI scales was analyzed using Cronbach’s α coefficient. Descriptive statistical analysis included a range of scores, mean (M), median (Mdn), standard deviation (SD), skewness, and kurtosis. The Student’s t-test was used to examine differences between gender (Women, Men). Pearson’s r was calculated to assess the association between variables. The mediation role of health behaviors in the relationship between dispositional optimism and life satisfaction was tested using Model 4 of PROCESS v3.5. Macro for SPSS, designed by Hayes.50,51 Two alternative regression analysis models were conducted: 1) simple mediation for the total HBI as a mediator; and 2) parallel mediation for the complex of four subscales of the HBI (HD, PB, PMA, and the HP) included simultaneously in the analysis. Gender served as a covariate in all mediation analyses. The conditional effect was examined based on a bias-corrected bootstrapping procedure with 10,000 samples. A bootstrap confidence interval (95% CI) not including “0” signals a significant effect.
Sensitivity analysis was performed using the Structural Equation Modeling in the AMOS software of the SPSS Statistic. The bias-corrected percentile method of bootstrapping procedure was included with 2000 samples. Following fit indices were examined52 minimum discrepancy per degree of freedom (ratio χ2/df ≤ 2 or 3 is useful), root-mean-square error of approximation (acceptable if RMSEA < 0.06 to 0.08 with confidence interval), standardized root-mean-square residual (SRMR smaller is better, 0 indicates perfect fit, while <0.08 adequate fit), comparative fit index (CFI ≥ 0.95 for acceptance), incremental fit index (IFI ≥ 0.95 for acceptance), normed fit index (NFI ≥ 0.95 for acceptance), Akaike information criterion (AIC smaller the better), and Browne-Cudeck criterion (BCC smaller the better). All analyses were performed using Statistical Package for the Social Sciences (IBM SPSS Statistics, ver. 25, 2019, Predictive Solutions Sp. z o.o., Kraków, Poland).
Results
Descriptive Statistics
In the first step of statistical analyses, descriptive statistics were computed, and distributions of variables were examined. Unfortunately, skewness and kurtosis values did not reach the absolute value of 1, as shown in Table 2. Therefore, parametric tests were allowed for further statistical analyses following guidelines.53
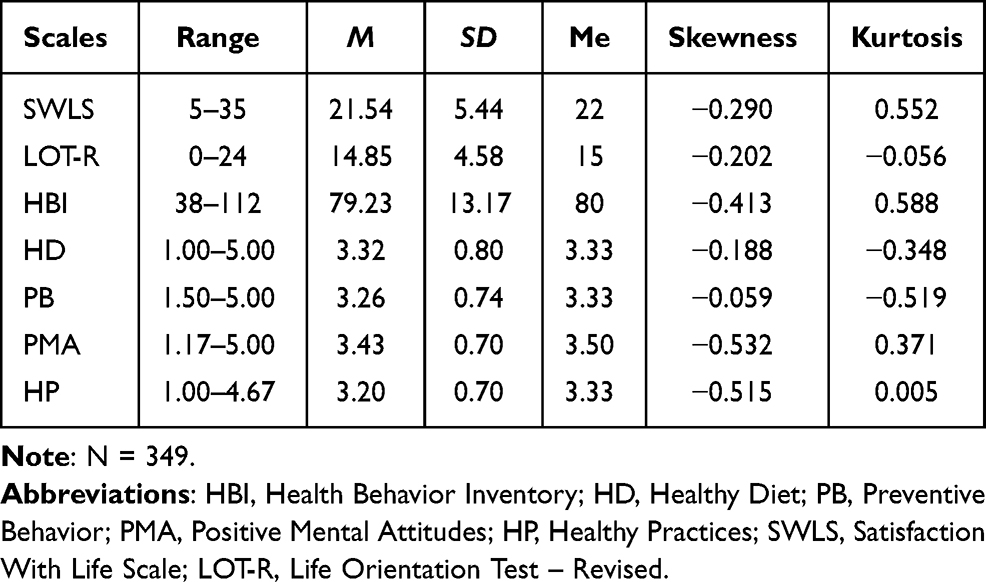 |
Table 2 Descriptive Statistics for Continuously Measured Variables |
Scores were converted to sten scores for easier interpretation of results regarding other people in the population. Sten scores ranging between 1 and 4 are interpreted as low, between 5 and 6 as the average most typical outcome, and between 7 and 10 as high. Mean sten scores in the present sample suggest that health sciences students demonstrate average scores in life satisfaction (M = 5.87, SD = 1.93), dispositional optimism (M = 5.68, SD = 2.23), and health behaviors (M = 5.10 SD = 1.77).
Gender differences were examined in regard to all measured dimensions (Table 3). Women showed significantly higher levels of health behavior (in general and for HD and PB scales) than men HD. However, men scored higher than women in dispositional optimism. No differences were found in SWLS and the two remaining subscales of HBI.
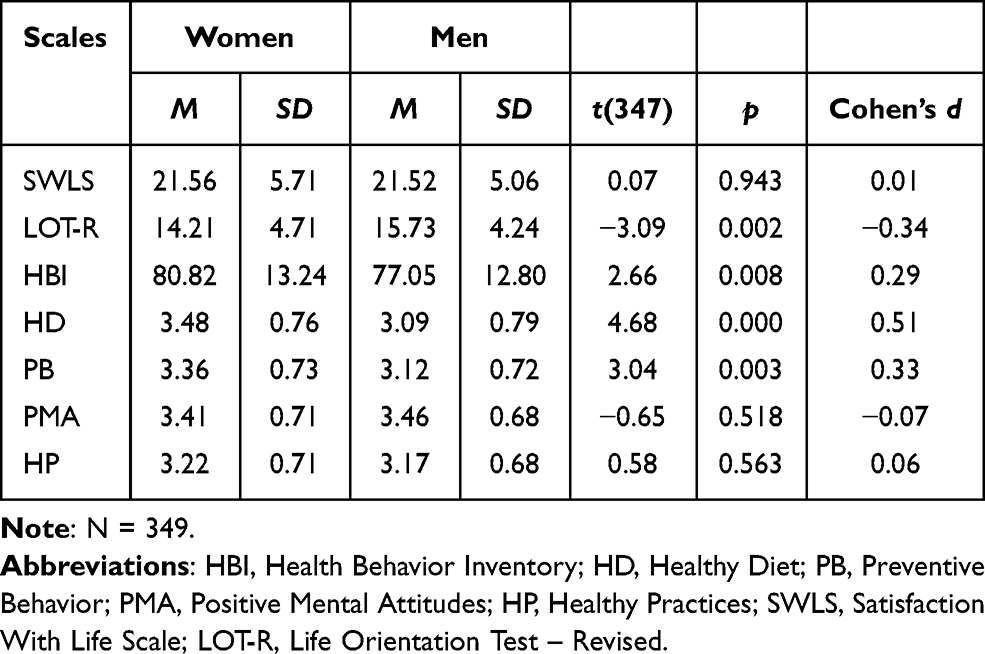 |
Table 3 Gender Differences in Life Satisfaction (SWLS), Dispositional Optimism (LOT-R), and Health Behaviors (HBI) |
Relationships Between Life Satisfaction, Dispositional Optimism, and Health Behaviors
As shown in Table 3, life satisfaction is significantly correlated with dispositional optimism and health behaviors (as a general score and distinct behaviors). All correlations are positive, suggesting that higher dispositional optimism and more frequent practicing health behaviors are connected with higher life satisfaction. Moderate strength of association was found between the SWLS and LOT-R, total HBI and PMA, while weak correlations between SWLS and HNN, PB, and HP scales of health behavior. A moderate correlation of dispositional optimism with PMA was shown, and a weak association with total HBI, HP, and PB. All subscales of the HBI are positively and strongly related to the total HBI, whereas particular subscales correlate with each other moderately or weakly (Table 4).
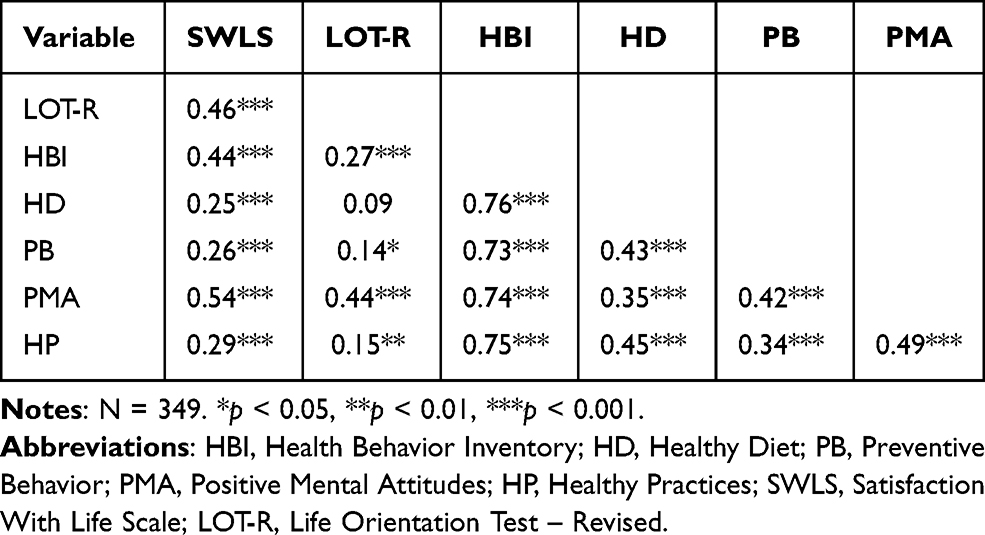 |
Table 4 Pearson’s r Correlations Between Life Satisfaction, Dispositional Optimism and Health Behaviors |
Single Mediation Model for the Life Satisfaction
The hypothesis of the mediating role of general health behaviors on the relationship between dispositional optimism and life satisfaction was examined using a single mediation model (model 4 of the PROCESS). In addition, gender was included in the mediation model as a covariate. The results indicated that HBI partially mediated the relationship between dispositional optimism and life satisfaction (Figure 1).
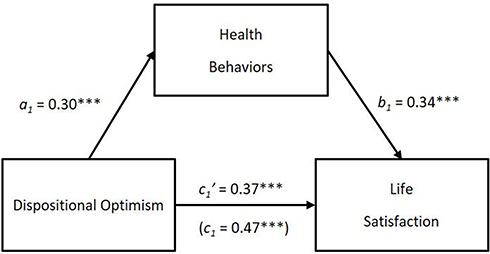 |
Figure 1 Standardized path coefficients for the relationship between life orientation and life satisfaction as mediated by general health behaviors. Notes: The a1-path represents the impact of the independent variable (IV = dispositional optimism) on the mediator variable (M = health behaviors). The b1-path represents the impact of the mediator on the dependent variable (DV = life satisfaction). The c1-path represents the total effect of IV on the DV and c’ represents the direct effect of IV on DV accounting for the indirect effect of a mediator. ***p < 0.001. |
Positive association suggests that health sciences students with greater dispositional optimism are more engaged in health behaviors and these habits increase life satisfaction. Optimistic life orientation is a significant predictor of satisfaction with life (b = 0.56, SE b = 0.06, 95% CI = 0.45; 0.67, β = 0.47, t = 9.80, p < 0.001), but gender cannot serve as a predictor (b = −0.89, SE b = 0.53, 95% CI = −1.94; 0.15, β = −0.02, t = −0.08, p = 0.09), R2 = 0.22, F(2, 346) = 48.02, p < 0.001. Dispositional optimism is also significant predictor of health behaviors (b = 0.86, SE b = 0.15, 95% CI = 0.57; 1.15, β = 0.30, t = 5.81, p < 0.001), whereas gender is negative predictor of health behaviors (b = −5.07, SE b = 1.37, 95% CI = −7.77; −2.38, β = −0.19, t = −3.70, p < 0.001), R2 = 0.11, F(2, 346) = 20.77, p < 0.001. This result suggests that optimistic people and women are significantly more likely to engage in health behaviors than pessimistic people and men. However, when optimism and health behaviors were included in the model of mediation, together with gender as a covariate, gender was not a significant predictor of life satisfaction (b = −0.18, SE b = 0.50, 95% CI = −1.17; 0.81, β = −0.02, t = −0.35, p = 0.73). Health behavior was found to be a mediator in the relationship between dispositional optimism and life satisfaction. The bootstrapped standardized indirect effect of optimism on life satisfaction via health behaviors was statistically significant and equaled 0.10, Boot SE = 0.03, and Boot 95% CI = (0.05, 0.16). The total variance of life satisfaction accounted for by simple mediation model was 32%, R2 = 0.32, F(3, 345) = 54.48, p < 0.001.
A sensitivity analysis was conducted using Structural Equation Modeling (SEM) to examine the single mediation model’s structural validity. Three observed variables were included in the mediation model: dispositional optimism (exogenous variable), health behaviors, and satisfaction with life (both endogenous variables). First, the SEM analysis was performed in the total sample (N = 349). All associations were significant and confirmed the mediation role of health behaviors in the relationship between dispositional optimism and life satisfaction (see Figure S1 in Supplementary Materials). The fit indices suggest that a single mediation model has a perfect fit.44 The discrepancy function of the model was CMIN/df = 0.000, RMSEA = 0.000, SRMR = 0.000. The comparative fit indexes: CFI = 1.000, IFI = 1.000, NFI = 1.000. Information theory goodness-of-fit measures were: AIC = 12.000, BCC = 12.140.
Next, the SEM analysis was conducted separately in both gender samples, namely for Women (n = 202) and Men (n = 147). The mediating role of health behaviors was confirmed for both sexes (see Figures S2 and S3 in Supplementary Materials). In women sample, dispositional optimism was positive predictor of life satisfaction (b = 0.40, SE b = 0.07, p < 0.001, β = 0.33, Boot β 95% CI = 0.21; 0.45) and positive predictor of health behaviors (b = 0.98, SE b = 0.19, p < 0.001, β = 0.35, Boot β 95% CI = 0.21; 0.48), and health behavior was positive predictor of life satisfaction (b = 0.16, SE b = 0.03, p < 0.001, β = 0.38, Boot β 95% CI = 0.24; 0.51). In men sample, dispositional optimism was positive predictor of life satisfaction (b = 0.49, SE b = 0.09, p < 0.001, β = 0.41, Boot β 95% CI = 0.27; 0.34) and positive predictor of health behaviors (b = 0.65, SE b = 0.24, p < 0.01, β = 0.22, Boot β 95% CI = 0.02; 0.40), and health behavior was positive predictor of life satisfaction (b = 0.11, SE b = 0.03, p < 0.001, β = 0.28, Boot β 95% CI = 0.14; 0.43). The model fit indices were CMIN/df = 0.000, RMSEA = 0.000, SRMR = 0.000, CFI = 1.000, IFI = 1.000, NFI = 1.000, AIC = 24.000, BCC = 24.585.
Parallel Mediation Model for the Life Satisfaction
Alternatively, a parallel model of mediation (model 4 of the PROCESS) was performed in the next step of analysis (Figure 2). In contrast to previous model, particular subscales of the HBI (ie, HD, PB, PMA, and HP) were considered as concurrent mediators in the association between optimistic expectancies and satisfaction with life. Gender also served here as a covariate. The results showed that dispositional optimism can predict positively all four dimensions of the HBI: HD (b = 0.02, SE b = 0.01, 95% CI = 0.01; 0.04, β = 0.13, t = 2.55, p < 0.01, R2 = 0.08, F(2, 346) = 14.36, p < 0.001), PB (b = 0.03, SE b = 0.01, 95% CI = 0.01; 0.04, β = 0.17, t = 3.14, p < 0.001, R2 = 0.05, F(2, 346) = 9.68, p < 0.001), PMA (b = 0.07, SE b = 0.01, 95% CI = 0.05; 0.08, β = 0.45, t = 9.20, p < 0.001, R2 = 0.20, F(2, 346) = 42.56, p < 0.001), and HP (b = 0.02, SE b = 0.01, 95% CI = 0.01; 0.04, β = 0.16, t = 3.00, p < 0.001, R2 = 0.03, F(2, 346) = 4.67, p < 0.001). Gender was significant predictor of HHB (b = −0.43, SE b = 0.08, 95% CI = −0.59;-0.26, β = −0.27, t = −5.07, p < 0.01), and PB (b = −0.28, SE b = 0.08, 95% CI = −0.44;-0.13, β = −0.19, t = −3.55, p < 0.01), but cannot predict PMA (b = −0.05, SE b = 0.07, 95% CI = −0.19; 0.08, β = −0.04, t = −0.80, p = 0.43), and HP (b = −0.08, SE b = 0.08, 95% CI = −1.07; 0.08, β = −0.06, t = −1.07, p = 0.29).
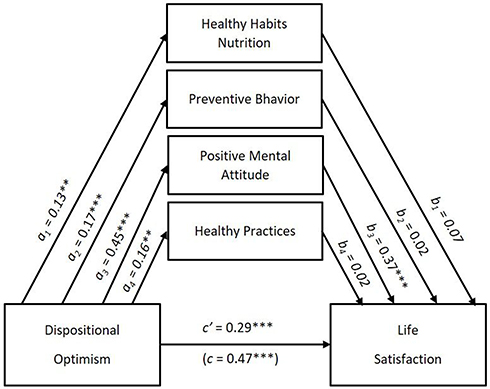 |
Figure 2 Standardized path coefficients for the relationship between life orientation and life satisfaction as mediated by four types of health behaviors. Notes: The a-path represents the impact of the independent variable (IV) on the mediator variable (M). The b-path represents the impact of the mediator on the dependent variable (DV). The c-path represents the total effect of IV on the DV and c’ represents the direct effect of IV on DV accounting for the indirect effect of a mediator. **p < 0.01. ***p < 0.001. |
Life satisfaction may be positively predicted by dispositional optimism (b = 0.34, SE b = 0.06, 95% CI = 0.23; 0.46, β = 0.29, t = 5.90, p < 0.001) and PMA (b = 2.91, SE b = 0.45, 95% CI = 2.04; 3.79, β = 0.37, t = 6.52, p < 0.001). This result suggests that PMA is a mediator in the relationship between dispositional optimism and life satisfaction. The standardized bootstrap indirect effect of optimism on life satisfaction via Positive Mental Attitudes was 0.17, Boot SE = 0.03, and Boot 95% CI = (0.11, 0.23), which confirmed that PMA partially mediates the assumed association.
Although HD was not a significant predictor of life satisfaction (b = 0.46, SE b = 0.36, 95% CI = −0.25; 1.16, β = 0.07, t = 1.28, p = 0.20), the standardized bootstrap effect was 0.01, Boot SE = 0.01, and Boot 95% CI = (0.00, 0.03), suggesting that HD mediates the association between optimistic orientation and life satisfaction. The other two subscales of the HBI, namely PB (b = 0.16, SE b = 0.37, 95% CI = −0.57; 0.90, β = 0.02, t = 0.44, p = 0.66, Boot effect = 0.00, Boot SE = 0.01, and Boot 95% CI = −0.01; 0.02) and HP (b = 15, SE b = 41, 95% CI = −0.66; 0.96, β = 0.02, t = 0.36, p = 0.72, Boot effect = 0.00, Boot SE = 0.01, and Boot 95% CI = −0.02; 0.02) are not predictors of life satisfaction, since neither significant effect was found in regression analysis, nor in bootstrap procedure. Also, gender was not significant predictor of life satisfaction (b = −0.43, SE b = 0.50, 95% CI = −1.47; 0.51, β = −0.04, t = −0.95, p = 0.34, Boot mean = −0.48, Boot SE = −0.47, and Boot 95% CI = −1.51; 0.51). Overall, the parallel model of mediation explains 36% of total variance of life satisfaction, R2 = 0.36, F(6, 342) = 32.66, p < 0.001.
The structural validity of the parallel model of mediation was also examined, using an SEM as a sensitivity analysis (see Figure S4 in Supplementary Materials). Six observed variables were included in the model of mediation; exogenous variable was dispositional optimism (the LOT-R), while endogenous variables were Healthy Diet (HD scale of the HBI), preventive behavior (PB scale of the HBI), Positive Mental Attitudes (PMA scale of the HBI), healthy practices (HP scale of the HBI), and satisfaction with life (the SWLS). Results of regression model and bootstrap analysis suggest that both PMA (b = 2.56, SE b = 0.42, p < 0.001, β = 0.33, Boot β 95% CI = 0.24; 0.42) and PB (b = 1.00, SE b = 0.00, p < 0.001, β = 0.13, Boot β 95% CI = 0.12; 0.14) are predictors of life satisfaction, and plays a mediation role in the association between dispositional optimism and life satisfaction. Goodness-of-fit indices showed that the parallel mediation model is acceptable, although the single model demonstrated better fit of the total sample (N = 349), CMIN/df = 4.553, p < 0.05, RMSEA = 0.101 (90% CI = 0.023, 0.203), SRMR = 0.016, CFI = 0.993, IFI = 993, NFI = 991, AIC = 44.553, and BCC = 45.374.
Using SEM, the multigroup parallel mediation analysis was also conducted comparatively for Women (n = 202) and Men (n = 147). In women, dispositional optimism was a significant predictor of all four subscales of the HBI (HD, PB, PMA, and HP). Also, significant predictors of life satisfaction were PMA and PB. Therefore, the indirect effect of dispositional optimism on life satisfaction via PMA and PB was confirmed (see Figure S5 in Supplementary Materials). In men, only PMA was significantly associated with dispositional optimism and satisfaction with life, so PMA was found the sole mediator of the relationship between dispositional optimism and life satisfaction (see Figure S6 in Supplementary Materials). The model fit indices suggested an acceptable model but worse than both single models and parallel model for the total sample, since CMIN/df = 2.353, p = 0.095, RMSEA = 0.062 (90% CI = 0.000, 0.138), SRMR = 0.020, CFI = 0.995, IFI = 995, NFI = 991, AIC = 84.706, and BCC = 88.176.
Discussion
The present study examined the mediating role of health behavior in the association between dispositional optimism and life satisfaction in health care students. Several analyses were performed to answer the research question, including descriptive statistics and analyses of gender difference, correlation, and mediation. Overall, health sciences students demonstrated average life satisfaction, dispositional optimism, and health behaviors, with gender differences in health-related behavior and optimistic expectancies.
The previous research54 found a high risk of health-related behaviors among nursing/midwifery and teacher education students. Undergraduates showed alcohol drinking (93.2%), an unhealthy diet (26.3%), physical inactivity (26%), tobacco smoking (17%), cannabis use (11.6%), and high levels of stress (41.9%). Physical activity (PA) was negatively associated with social support and depression among young adults from 21 European countries.22 In the cross-national sample of young adults,22 73.2% of men and 68.3% of women engaged in PA. A high risk of frequent alcohol use, binge drinking, smoking, low physical activity, low vegetable intake, low fruit intake, and poor sleep was identified among 34% of male and 22% of female college students.21 Aceijas et al18 concern that the hazardous university students’ health-related lifestyle might be unlikely to change in future generations.
Health care students appear to be a critical group because they will be responsible for patients’ health. Health care workers are especially vulnerable to mental and physical health problems and burnout because of the stressful work environment. In particular, nursing professionals face extraordinary stressors related to long work hours, coping with pain, loss, and emotional suffering, and providing support to patient’s families.55 Such a working environment could potentially lead to lateral anxiety, depression, and violence among nurses. Also, shift work can have physical, mental health, and safety consequences among nurses. Healthcare students should especially care about preventing the adverse effects of an unhealthy lifestyle by employing a variety of mental and behavioral methods.56
In accordance with previous studies,20,57 women showed higher scores than men in HD (with medium strength) and the total scores of HBI and PB (but with a small effect size). Dispositional optimism differed between genders, with higher levels in men than in women, but the effect size was small. This result is consistent with previous research that found some gender differences, but relatively marginal.6–8,47
This study found positive correlations of life satisfaction with dispositional optimism (moderately strong) and all health behaviors dimensions (weak for HD, PB, and HP, and moderate for general score and PMA). Dispositional optimism was also moderately associated with PMA and weakly with total HBI, HP, and PB. Thus, the hypothesis about the mediating role of general health behaviors on the relationship between dispositional optimism and life satisfaction (with gender as a confounding variable) was partially confirmed in this study. The simple mediation model accounted for 32% of the life satisfaction variance explained. Furthermore, SEM showed an almost perfect fit of this model performed in the total sample, and a good fit for a single multigroup model, comparing women with men.
Oishi et al3 indicated that life satisfaction depends on various factors, including dispositional dimensions of individual differences in temperament and personality, adaptation, goals, and coping strategies. Studies of heritability demonstrate that personality plays a vital role in predicting life satisfaction. Previous research suggested that core self-evaluations (ie, individual differences in personality dimensions such as self-esteem, general self-efficiency, neuroticism, and locus of control) can partially mediate the effect of dispositional optimism on life satisfaction. However, behavioral information, including sleep disturbances, alcohol consumption, PA level, and lack of appetite, offers another insight into well-being.58 The present research found the indirect effect of dispositional optimism (considered a personality dimension) on life satisfaction via a healthy lifestyle, including a healthy diet, preventive behaviors, positive mental attitudes, and healthy practices among health care students.
Optimists are usually more engaged in protective health-related behaviors.5 Dispositional optimism increases when exercising, taking vitamins, eating low-fat foods, reducing risky sexual behavior, and safeguarding self-health.4 Carver et al4 suggest optimistic people take action and effort to minimize health risks by selectively attending to the potentially serious risks and threatening them to achieve well-being. Optimistic explanatory style leads people to perceive desired goals as achievable, to actively confront adversities, resulting in increased goal attainment and perseverance.28
Pessimism reduces the possibility of improving dietary patterns. A more recent meta-analytic study confirmed that more optimistic individuals tend to engage in healthier behaviors regarding physical activity, diet, and cigarette smoking than less optimistic individuals.59 Research also found an association between high optimism and high diet quality and less snacking behavior among the general population.60
An alternative parallel model of mediation found the mediation role of PMA and, to some extent, HD (but not PB and HP) in the association between optimistic expectancies and satisfaction with life when gender was included as a covariate. However, SEM showed that PMA and PB (but not HD and HP) are mediators in the relationship between optimistic expectancies and satisfaction with life when the analysis was conducted on the total sample. Furthermore, when a multigroup mediation analysis was performed using SEM, both mediators PMA and PB were confirmed in women, while in men, only PMA was found as mediator. The gender differences may be related to the motivational aspect of healthy behavior, which seems much more substantial in women than men. The previous study evidenced that if the expectancy is consistent with the desired outcome’s specificity, the impact of optimistic expectations on outcome increases.61 Both dispositional optimism and goal adjustment are essential for general subjective well-being.62
Both parallel models showed the worst fit than both single mediation models. It suggests that a global measure of health behaviors is better than analyzing particular healthy habits regarding diet, various practices, prevention, and mental health care. Although several dimensions of healthy behavior may be more interesting for health care professionals from a practical perspective, these health-related behaviors correlate moderately (see Table 3 and Figures S4–S6, for more details), therefore more appropriate is to consider health behaviors as an umbrella covering various dimensions or types. The present result is to some extent consistent with previous research, which suggests that risky health behaviors tend to cluster.6–8,21,47
Limitation of the Study and Directions for Future Studies
Although this study’s results strongly supported the hypothesis about the mediation role of health behaviors in the association between dispositional optimism and life satisfaction, some limitations cannot allow for this research’s generalizability. First of all, this is a cross-sectional study, so causal links should be considered with caution. Future studies should be conducted longitudinally to confirm the current cross-sectional results in the causal model. Second, the present sample was conventional and does not include all major health sciences departments. Therefore, the research cannot be generalized to this population. Third, the present sample represented a healthy population of young adults. However, it would be interesting if differences in health behaviors exist regarding people with various mental and somatic diseases. Further research should be conducted on a random sample of students representing various fields of study and compared to those with various diseases. The mediation model can also be tested in the general adult population. Another limitation of the study that may be a source of measurement error is the self-report assessment and short scales, which may not cover all important items or components of life satisfaction, dispositional optimism, and health behavior. Further studies should replicate the present findings by using the other measures to assess life satisfaction, dispositional optimism, and health behavior. Also, an experimental design could help resolve the problem of measurement error. Future research should be repeated across the general population of different countries, taking into account other confusing variables other than gender, such as educational level, socioeconomic status, personality, and temperamental characteristics, and by controlling the risk of mental disorders (eg, anxiety, depression, obsessive-compulsive disorders, addiction).
Conclusion
The mediation analysis results supported the hypothesis that health-related behaviors mediated the relationship between optimistic expectations and life satisfaction. The partial effect of mediation explains 32% of the variance in life satisfaction in single mediation model. Although a higher variance was explained (36%) in the parallel mediation model (when four subscales of HBI were considered concurrently multiple mediators), SEM showed poorer fit indices for this model than simple mediation. Among the four subscales of HBI, PMA can play a mediator role in both men and women, while PB is a significant mediator in women (but not in men). In this study, gender's moderating role has not been fully elucidated. More research is needed to verify the presented results in the future. Partial mediation also suggests that the current HBI measurement may not cover all relevant components, or that another variable should be included in the mediation model to fully explain life satisfaction. Our empirical findings contribute to a better understanding of the interplay mechanism between personality and behavior that contributes to SWB.
This study’s result suggests optimistic expectancies and health-related behaviors should be improved concurrently to increase life satisfaction. Carver et al4,5 and Scheier & Carver40 recommend cognitive-behavioral therapies to change negative cognitive distortions into positive patterns, cancel barriers and limitations while achieving goals, reduce pessimistic thinking and negative emotions, and develop positive thinking and negative emotions expectancies towards outcomes and self-efficacy. Training skills in optimistic explanations for events, decreasing negative automatic thoughts, and increasing constructive thoughts and behaviors may prevent depression and positively affect well-being. Just two weeks of daily 5-minute sessions of imagining one’s best possible self can increase optimism. On the other hand, university-based interventions focused on increasing health behaviors in physical activity, diet, and weight loss can improve health for university and college students.63,64
Disclosure
The authors report no conflicts of interest in this work.
References
1. Diener E, Emmons RA, Larsen RJ, et al. The satisfaction with life scale. J Pers Assess. 1985;49:71–75. doi:10.1207/s15327752jpa4901_13
2. Diener E, Suh EM, Lucas RE, et al. Subjective well-being: three decades of progress. Psychol Bull. 1999;125:276–302. doi:10.1037/0033-2909.125.2.276
3. Oishi S, Diener E, Lucas RE. Subjective well-being: the science of happiness and life satisfaction. In: Snyder CR, Lopez SJ, Edwards LM, et al., editors. The Oxford Handbook of Positive Psychology.
4. Carver CS, Scheier MF, Segerstrom SC. Optimism. Clin Psychol Rev. 2010;30:879–889. doi:10.1016/j.cpr.2010.01.006
5. Carver CS, Scheier MF. Dispositional optimism. Trends Cogn Sci. 2014;18:293–299. doi:10.1016/j.tics.2014.02.003
6. Glaesmer H, Rief W, Martin A, et al. Psychometric properties and population-based norms of the Life Orientation Test Revised (LOT-R). Br J Health Psychol. 2012;17:432–445. doi:10.1111/j.2044-8287.2011.02046.x
7. Hinz A, Sander C, Glaesmer H, et al. Optimism and pessimism in the general population: psychometric properties of the Life Orientation Test (LOT-R). Int J Clin Health Psychol. 2017;17:161–170. doi:10.1016/j.ijchp.2017.02.003
8. Schou-Bredal I, Heir T, Skogstad L, et al. Population-based norms of the Life OrientationTest-Revised (LOT-R). Int J Clin Health Psychol. 2017;17:216–224. doi:10.1016/j.ijchp.2017.07.005
9. Scheier MF, Carver CS. Effects of optimism on psychological and physical well-being: theoretical overview and empirical update. Cognit Ther Res. 1992;16:201–228. doi:10.1007/BF01173489
10. Zanni GR. Optimism and health. Consult Pharm. 2008;23:112–116. doi:10.4140/TCP.n.2008.112
11. Daukantaitė D, Zukauskiene R. Optimism and subjective well-being: affectivity plays a secondary role in the relationship between optimism and global life satisfaction in the middle-aged women. Longitudinal and cross-cultural findings. J Happiness Stud. 2012;13:1–16. doi:10.1007/s10902-010-9246-2
12. Sahai A, Singh A. A correlation study: the relationship between optimism and subjective well-being of education sector employees. Indian J Posit Psychol. 2017;8:347–350.
13. Liu C, Cheng Y, Hsu ASC, et al. Optimism and self-efficacy mediate the association between shyness and subjective well-being among Chinese working adults. PLoS One. 2018;13:e0194559. doi:10.1371/journal.pone.0194559
14. Satici B. Testing a model of subjective well-being: the roles of optimism, psychological vulnerability, and shyness. Health Psychol Open. 2019;6(2):205510291988429. doi:10.1177/2055102919884290
15. Oriol X, Miranda R, Bazán C, et al. Distinct routes to understand the relationship between dispositional optimism and life satisfaction: self-control and grit, positive affect, gratitude, and meaning in life. Front Psychol. 2020;11:907. doi:10.3389/fpsyg.2020.00907
16. Conner M, Norman P. Predicting Health Behaviour. Maidenhead, Berkshire, UK: Open University Press; 1996.
17. Dinger MK, Brittain DR, Hutchinson SR. Associations between physical activity and health-related factors in a national sample of college students. J Am Coll Health. 2014;62:67–74. doi:10.1080/07448481.2013.849710
18. Aceijas C, Waldhäusl S, Lambert N, et al. Determinants of health-related lifestyles among university students. Perspect Public Health. 2017;137:227–236. doi:10.1177/1757913916666875
19. West AB, Bittel KM, Russell MA, et al. A systematic review of physical activity, sedentary behavior, and substance use in adolescents and emerging adults. Transl Behav Med. 2020;10:1155–1167. doi:10.1093/tbm/ibaa008
20. Rogowska AM, Pavlova I, Kuśnierz C. Comparison of healthy behavior in Ukrainian and Polish students of physical education. Phys Activ Rev. 2021;9:56–65. doi:10.16926/par.2021.09.21
21. Luo J, Agley J, Hendryx M, et al. Risk patterns among college youth: identification and implications for prevention and treatment. Health Promot Pract. 2014;16:132–141. doi:10.1177/1524839914520702
22. Steptoe A, Wardle J, Fuller R, et al. Leisure-time physical exercise: prevalence, attitudinal correlates, and behavioral correlates among young Europeans from 21 countries. Prev Med. 1997;26:845–854. doi:10.1006/pmed.1997.0224
23. Diener E, Oishi S, Tay L. Advances in subjective well-being research. Nat Hum Behav. 2018;2:253–260. doi:10.1038/s41562-018-0307-6
24. Pettay RS. Health Behaviors and Life Satisfaction in College Students [dissertation]. Manhattan, USA: Kansas State University; 2008. Available from: http://hdl.handle.net/2097/669.
25. Grygiel E, Cygnar E, Zwolinska-Mirek K, et al. Health behaviours and life satisfaction of health spa patients. Med Sci Pulse. 2018;12:22–28. doi:10.5604/01.3001.0012.1160
26. Shi Y, Joyce C, Wall R, et al. A life satisfaction approach to valuing the impact of health behaviours on subjective well-being. BMC Public Health. 2019;19:1547. doi:10.1186/s12889-019-7896-5
27. Beck MR, Gregorini P. How dietary diversity enhances hedonic and eudaimonic well-being in grazing ruminants. Front Vet Sci. 2020;7:191. doi:10.3389/fvets.2020.00191
28. Avvenuti G, Baiardini I, Giardini A. Optimism’s explicative role for chronic diseases. Front Psychol. 2016;7:295. doi:10.3389/fpsyg.2016.002
29. Pänkäläinen M, Fogelholm M, Valve R, et al. Pessimism, diet, and the ability to improve dietary habits: a three-year follow-up study among middle-aged and older Finnish men and women. Nutr J. 2018;17:92. doi:10.1186/s12937-018-0400-8
30. Scheier MF, Swanson JD, Barlow MA, et al. Optimism versus pessimism as predictors of physical health: a comprehensive reanalysis of dispositional optimism research. Am Psychol. 2021;76(3):529–548. doi:10.1037/amp0000666
31. Bandura A. Self-efficacy mechanism in human agency. Am Psychol. 1982;37:122–147. doi:10.1037/0003-066X.37.2.122
32. Hecht D. The neural basis of optimism and pessimism. Exp Neurobiol. 2013;22:173–199. doi:10.5607/en.2013.22.3.173
33. Das KV, Jones-Harrell C, Fan Y, et al. Understanding subjective well-being: perspectives from psychology and public health. Public Health Rev. 2020;41:25. doi:10.1186/s40985-020-00142-5
34. Diener E. Subjective well-being. Psychol Bull. 1984;95:542–575. doi:10.1037/0033-2909.95.3.542
35. Diener E, Pressman SD, Hunter J, et al. If, why, and when subjective well-being influences health, and future needed research. Appl Psychol Health Well Being. 2017;9:133–167. doi:10.1111/aphw.12090
36. Scheier MF, Carver CS. Dispositional optimism and physical well-being: the influence of generalized outcome expectancies on health. J Pers. 1987;55:169–210. doi:10.1111/j.1467-6494.1987.tb00434.x
37. Scheier MF, Carver CS. Optimism, coping, and health: assessment and implications of generalized outcome expectancies. Health Psychol. 1985;4:219–247. doi:10.1037/0278-6133.4.3.219
38. Engel GL. The clinical application of the biopsychosocial model. Am J Psychiatry. 1980;137:535–544.
39. Nima AA, Cloninger KM, Lucchese F, et al. Validation of a general subjective well-being factor using classical test theory. Peer J. 2020;8:e9193. doi:10.7717/peerj.9193
40. Scheier MF, Carver CS. Dispositional optimism and physical health: a long look back, a quick look forward. Am Psychol. 2018;73:1082–1094. doi:10.1037/amp0000384
41. Andersen BL, Kiecolt-Glaser JK, Glaser R. A biobehavioral model of cancer stress and disease course. Am Psychol. 1994;49:389–404. doi:10.1037/0003-066X.49.5.389
42. Wrosch C, Scheier MF. Personality and quality of life: the importance of optimism and goal adjustment. Qual Life Res. 2003;12:59–72. doi:10.1023/A:1023529606137
43. Pavot W, Diener E. Review of the satisfaction with life scale. Psychol Assess. 1993;5:164–172. doi:10.1037/1040-3590.5.2.164
44. Juczyński Z. Measurement Tools in Health Promotion and Psychology. Warszawa, Poland: PTP; 2009.
45. Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a re-evaluation of the Life Orientation Test. J Pers Soc Psychol. 1994;67:1063–1078. doi:10.1037/0022-3514.67.6.1063
46. Cano-García FJ, Sanduvete-Chaves S, Chacón-Moscoso S, et al. Factor structure of the Spanish version of the Life Orientation Test-Revised (LOT-R): testing several models. Int J Clin Health Psychol. 2015;15:139–148. doi:10.1016/j.ijchp.2015.01.003
47. Steca P, Monzani D, Greco A, et al. Item response theory analysis of the life orientation test-revised: age and gender differential item functioning analyses. Assessment. 2015;22:341–350. doi:10.1177/1073191114544471
48. Amir D. Preventive behaviour and health status among the elderly. Psychol Health. 1987;1:353–377. doi:10.1080/08870448708400337
49. Prohaska TR, Leventhal EA, Leventhal H, et al. Health practices and illness cognition in young, middle aged, and elderly adults. J Gerontol. 1985;40:569–578. doi:10.1093/geronj/40.5.569
50. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
51. Hayes AF. PROCESS (Version 3.3.) [Macro for Windows and SPSS]; 2019. Available from: http://www.processmacro.org/download.html.
52. Schreiber JB, Stage FK, King J, et al. Reporting structural equation modeling and confirmatory factor analysis results: a review. J Educ Res. 2006;99:323–337. doi:10.3200/JOER.99.6.323-338
53. George D, Mallery P. IBM SPSS Statistics 26 Step by Step: A Simple Guide and Reference.
54. Deasy C, Coughlan B, Pironom J, et al. Psychological distress and lifestyle of students: implications for health promotion. Health Promot Int. 2014;30:77–87. doi:10.1093/heapro/dau086
55. Botha E, Gwin T, Purpora C. The effectiveness of mindfulness based programs in reducing stress experienced by nurses in adult hospital settings: a systematic review of quantitative evidence protocol. JBI Database System Rev Implement Rep. 2015;13:21–29. doi:10.11124/jbisrir-2015-2380
56. Brown JP, Martin D, Nagaria Z, et al. Mental health consequences of shift work: an updated review. Curr Psychiatry Rep. 2020;22:7. doi:10.1007/s11920-020-1131-z
57. Rogowska AM. Healthy behavior patterns among physical education students. J Phys Educ Health. 2020;15:5–11.
58. Diener E. Assessing subjective well-being: progress and opportunities. Soc Indic Res. 1994;31:103–157. doi:10.1007/BF01207052
59. Boehm JK, Chen Y, Koga H, et al. Is optimism associated with healthier cardiovascular-related behavior? Meta-analyses of 3 health behaviors. Circ Res. 2018;122:1119–1134. doi:10.1161/CIRCRESAHA.117.310828
60. Ait-hadad W, Bénard M, Shankland R, et al. Optimism is associated with diet quality, food group consumption and snacking behavior in a general population. Nutr J. 2020;19:6. doi:10.1186/s12937-020-0522-7
61. Armor DA, Taylor SE. Situated optimism: specific outcome expectancies and self-regulation. In: Zanna M, editor. Advances in Experimental Social Psychology. Vol. 30. Cambridge, MS: Academic Press; 1998:309–379.
62. Rasmussen HN, Wrosch C, Scheier MF, et al. Self-regulation processes and health: the importance of optimism and goal adjustment. J Pers. 2006;74:1721–1747. doi:10.1111/j.1467-6494.2006.00426.x
63. Plotnikoff RC, Costigan SA, Kennedy SG, et al. Efficacy of interventions targeting alcohol, drug and smoking behaviors in university and college students: a review of randomized controlled trials. J Am Coll Health. 2019;67:68–84. doi:10.1080/07448481.2018.1462821
64. Plotnikoff RC, Costigan SA, Williams RL, et al. Effectiveness of interventions targeting physical activity, nutrition and healthy weight for university and college students: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2015;12:45. doi:10.1186/s12966-015-0203-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.