Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Healthcare Workers’ Knowledge, Attitude, Practice and Perceived Health Facility Preparedness Regarding COVID-19 in Sierra Leone
Authors Kanu S, James PB ![]() , Bah AJ, Kabba JA, Kamara MS, Williams CEE
, Bah AJ, Kabba JA, Kamara MS, Williams CEE ![]() , Kanu JS
, Kanu JS ![]()
Received 16 October 2020
Accepted for publication 8 December 2020
Published 11 January 2021 Volume 2021:14 Pages 67—80
DOI https://doi.org/10.2147/JMDH.S287156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sulaiman Kanu,1,* Peter Bai James,2,3,* Abdulai Jawo Bah,2,4,5 John Alimamy Kabba,6 Musa Salieu Kamara,1 Christine Ellen Elleanor Williams,7 Joseph Sam Kanu8
1University of Sierra Leone Teaching Hospital Complex, Connaught Hospital, Freetown, Sierra Leone; 2Faculty of Pharmaceutical Sciences, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 3Australian Research Centre in Complementary and Integrative Medicine, School of Public Health, Faculty of Health, University of Technology Sydney, Ultimo, Sydney, NSW 2007, Australia; 4Faculty of Basic Medical Sciences, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 5Institute for Global Health and Development, Queen Margaret University Edinburg, Musselburgh, Scotland, UK; 6Department of Pharmacy Administration and Clinical Pharmacy, Center for Drug Safety and Policy Research, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 7Sierra Leone–China Friendship Hospital, Ministry of Health and Sanitation, Freetown, Sierra Leone; 8Directorate of Disease Prevention and Control, Ministry of Health and Sanitation, Freetown, Sierra Leone
*These authors contributed equally to this work
Correspondence: Peter Bai James
Faculty of Pharmaceutical Sciences, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone
Email [email protected]
Background: Healthcare workers (HCWs) are known to spearhead the fight against the COVID-19 pandemic. As such, their knowledge, attitude, and practice (KAP) toward coronavirus disease 2019 (COVID-19) are considered critical to the success of the current COVID-19 response efforts. This study aims to determine HCWs’ KAP toward COVID-19 and assesses their perception of their healthcare facilities preparedness to respond appropriately to the ongoing COVID-19 pandemic in Sierra Leone.
Methods: We conducted an online cross-sectional study among HCWs (n=516) between 1st May 2020 and 30th June 2020. We collected our data using a self-administered structured questionnaire via email and online social media platforms. We analyzed our data using descriptive statistics and regression analysis (p< 0.05).
Results: Close to three-fourth of HCWs (n=375, 72.7%) were knowledgeable regarding COVID-19. Doctors were more knowledgeable than community health workers and laboratory technicians (AOR= 2.48, 95% CI: 1.16– 5.31, p=0.019) regarding COVID-19. Close to two-thirds of HCWs (n=301, 58.3%) HCWs show positive attitudes toward COVID-19. Being male (AOR=2.08, 95% CI: 1.36– 3.20, p=0.001) and directly involved in COVID-19 patient care (AOR=3.21, 95% CI: 1.88– 5.48, p< 0.001) were identified as predictors of positive attitude towards COVID-19. HCWs are generally adhering to COVID-19 safe practices with majority indicating that they regularly wash or sanitize their hands (n=510, 98.8%) and used facemask at point of care (n=499, 96.7%). Majority of HCWs are of the view that their healthcare facilities are ill-prepared to adequately respond to COVID-19 with majority (n= 400, 77.5%) of them stating that their facilities lack enough personal protective equipment.
Conclusion: HCWs in Sierra Leone showed good knowledge, positive attitude and practice regarding COVID-19. However, HCWs are of the view that their healthcare facilities are ill-prepared to respond adequately to the COVID-19 outbreak. Health authorities and policymakers need to provide the necessary resources to allow HCWs to work in a safe environment.
Keywords: COVID-19, knowledge, attitude, practice, healthcare workers, Sierra Leone
Introduction
Pneumonia of unknown etiology was identified among patients in Wuhan, China in December 2019. The virus isolated from samples was named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and the disease caused by it was named Coronavirus disease 2019 (COVID-19).1 COVID-19 is a respiratory tract infection caused by a novel coronavirus. Genetic sequencing of the virus suggests that it is a beta coronavirus closely linked to the SARS virus.1 Mild or uncomplicated illness with COVID-19 has been seen among most people. At the same time, patients with under-lying comorbidity exhibited the worst clinical outcomes.2 Fever, dry cough, myalgia and fatigue symptoms were reported in most patients in a cohort study of 41 hospitalized Chinese patients, and less often, symptoms of expectoration, headache, hemoptysis and diarrhea were also observed.3
The World Health Organization (WHO) declared Coronavirus Disease 2019 (COVID-19) a pandemic on March 11, 2020.4 As of the 3rd December 2020, WHO has reported 63,965,092 confirmed cases and 1,488,120 deaths worldwide.5 The African region is least affected compared to other regions of the world. As of the 3rd December 2020, 1,520,631 confirmed cases and 24,464 deaths had been reported in Africa.6 As of the 3rd December 2020, in Sierra Leone, 2,416 and 74 cumulative confirmed cases and deaths have been reported, respectively,6 Experts suggest that the current figures in Africa are likely an underestimation of the real epidemiological picture of COVID-19 in the region.7 The least number of cases in Africa, including Sierra Leone, has been attributed to the fewer number of COVID-19 tests with respect to population size.7,8
Healthcare workers (HCWs) are always at the forefront in the response to emerging infectious diseases outbreaks, and as such, they are highly exposed to threats such as psychological distress, stigma, burnout that increased their risk of being infected.9 Sierra Leone healthcare workforce was unprepared when the Ebola epidemic struck in 2014. Close to 21% of the health workforce lost their lives. Despite the implementation of post-Ebola recovery strategies, the Sierra Leonean healthcare system remains fragile. Like most countries within the West African sub-region, the Sierra Leonean healthcare system was ill-equipped to respond to the Ebola outbreak. Lack of personal protective equipment, inadequate training and poor remunerations were some of the challenges faced by healthcare workers during the Ebola outbreak. Given that the current healthcare system is still considered weak, similar challenges faced by healthcare workers during the Ebola outbreak may resurface during the current COVID-19 outbreak. Some of these challenges are related to infrastructure, working environment as well as staff protection and welfare.
HCWs' knowledge, attitude and practice (KAP) regarding COVID-19 are critical to stopping the spread of the SARS-CoV-2 virus and the success of the overall COVID-19 response. Current report estimates that 175 HCWs in Sierra Leone have been infected with COVID-19.10 Such high morbidity figures have the potential to create fear among HCWs to continue providing care to COVID-19 patients, which will invariably undermine COVID-19 response efforts. The current literature indicates a conflicting picture regarding HCWs' KAP regarding COVID19. Some studies11–14 have indicated that HCWs have good knowledge of and positive attitude toward COVID-19 as well as practice safer infection, prevention and control practices put forward by international and local health authorities. On the other hand, an Ethiopian study reported poor prevention practices toward COVID-19 among HCWs15 while close to half of HCWs in Nepal were reported to have negative attitudes toward COVID-19.16 Currently, it is not known how prepared frontline HCWs are regarding the COVID-19 outbreak response in Sierra Leone. Anecdotal evidence suggests that there might be a gap in the preparedness towards COVID-19 with regards to their knowledge, attitude and practice. In order to expedite outbreak containment and management, it is essential to know frontline healthcare workers adherence to infection prevention control (IPC) measures, which mostly is affected by their knowledge, attitude and practice, and availability of IPC materials. An informed policy on the training needs of frontline health workforce on COVID-19 and quantifying the needed resources is imperative. Therefore, this study aimed to identify the gaps in preparedness and serve to provide an evidence-based knowledge in order to inform and guide policymakers for successful containment of the spread of COVID-19 and the adequate management of active cases of the disease. In order to identify the gaps in HCWs preparedness, the study assessed HCWs’ KAP towards COVID-19. It also assessed the HCWs’ perceived preparedness of their healthcare facilities to appropriately respond to the ongoing COVID-19 response.
Method
Study Design and Setting
We conducted a descriptive cross-sectional online survey among HCWs between 1st May 2020 and 30th June 2020. This study design is appropriate for a survey of this nature without disrupting service delivery, considering the present state of the pandemic, thus avoiding physical contact and breaking the chain of transmission. The study was carried out in all public healthcare facilities across Sierra Leone.
Study Participants and Sampling
All healthcare workers (Doctors, Nurses/midwives, Pharmacist, Community Health Officers, Laboratory technicians) directly or indirectly involved in COVID-19 patient care in the various study sites were targeted. A convenience sampling of 600 healthcare workers that are directly or indirectly involved in COVID-19 patient care in these study sites were reached through Email, websites and/or official WhatsApp group.
Data Collection Technique
Data collection was conducted online through the Survey monkey program. Links to the study were sent on social media platforms, especially WhatsApp, individual Emails and the registered emails of the various healthcare professional associations. We obtained the emails of the various healthcare professional associations from their websites or one of their executive members. An email was sent to these emails, asking them to share the link to the questionnaire to their members. Also, we requested the email IDs of HCWs on their various professional WhatsApp groups. A one –page recruitment notification that has a brief introduction of the study, research objectives, elements of ethical consideration and directives on how to fill the questionnaire, as well as the link and quick response (QR) code of the online questionnaire was sent via social media platforms. For those that were not reached via these above-mentioned channels, telephone interviews were conducted. HCWs’ telephone contacts were accessed through respective professional WhatsApp platforms or professional associations. We sent continuous weekly reminders via emails and WhatsApp messages to achieve optimal participation. We controlled duplication of responses by restricting each HCW to one response.
Data Collection Instruments
A structured questionnaire was used to obtain responses from respondents. The instrument was divided into three sections (A, B and C). Section A solicited respondents’ socio-demographic information. Section B assessed respondents’ KAP regarding COVID 19. Section C assessed HCWs’ perceived preparedness of their healthcare facilities to appropriately respond to the ongoing COVID-19 response. The design of the questionnaire was informed by the WHO interim guidance on the clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected17 and similar KAP studies among HCWs regarding COVID-19.11,13,18–23 These questions were answered on a true/false basis with an additional “I don’t know” option for knowledge. In contrast, questions on attitude, practice and health facility preparedness have Yes/No options. The “Yes” was given the score of 1 while the “No” and “I don’t know” options were given a score of 0. Responses to reversed questions were reversed when assigning the points (Yes=0, No=1). The total knowledge score ranged from 0 to 19, with a higher score (16–19) indicating a good knowledge of COVID-19. Similarly, the total attitude score ranged from 0 to 7. An attitude score of 5–7 was considered a positive attitude toward COVID-19. Similar cut-off points have been used in previous studies.11,24 The questionnaire was piloted among five HCWs, and their feedback informed the final version of the questionnaire. Please see supplementary material for details.
Data Analysis
Data were analyzed using Statistical Package for Social Sciences version 24. Descriptive statistics, chi-square and Fischer –exact two-tail tests were used to analyze our data. Binary logistics regression analysis was used to determine the independent association between the independent variables (respondents’ socio-demographic) and outcome variables (knowledge and attitude). In order to conduct binary logistics regression analysis knowledge scores were dichotomized into good knowledge (knowledge score 16–19) and poor knowledge (score < 16). Similarly, attitude scores were dichotomized into positive attitude (score 5–7) and negative attitude (score <5). We considered p<0.05 as statistically significant for all inferential analyses.
Ethical Consideration
Ethical clearance was obtained from the Sierra Leone ethics and scientific review committee at the Ministry of Health and Sanitation. All respondents provided informed consents before participating in the study, and the information obtained in this study were kept confidential and used only for this research.
Results
Out of the 573 healthcare workers that agreed to participate in the study, only 516 completely filled the questionnaire and were included in the final analysis. Table 1 indicates a summary of socio-demographic characteristics of healthcare workers. The average age of healthcare workers was 33.3±6.6. Slightly more than half were females (n=273, 52.9%) and close to half were nurses (n=232, 45.0%). More than a third had a bachelor degree and less than a quarter (n=101, 19.6%) of them were directly involved in COVID-19 patient care.
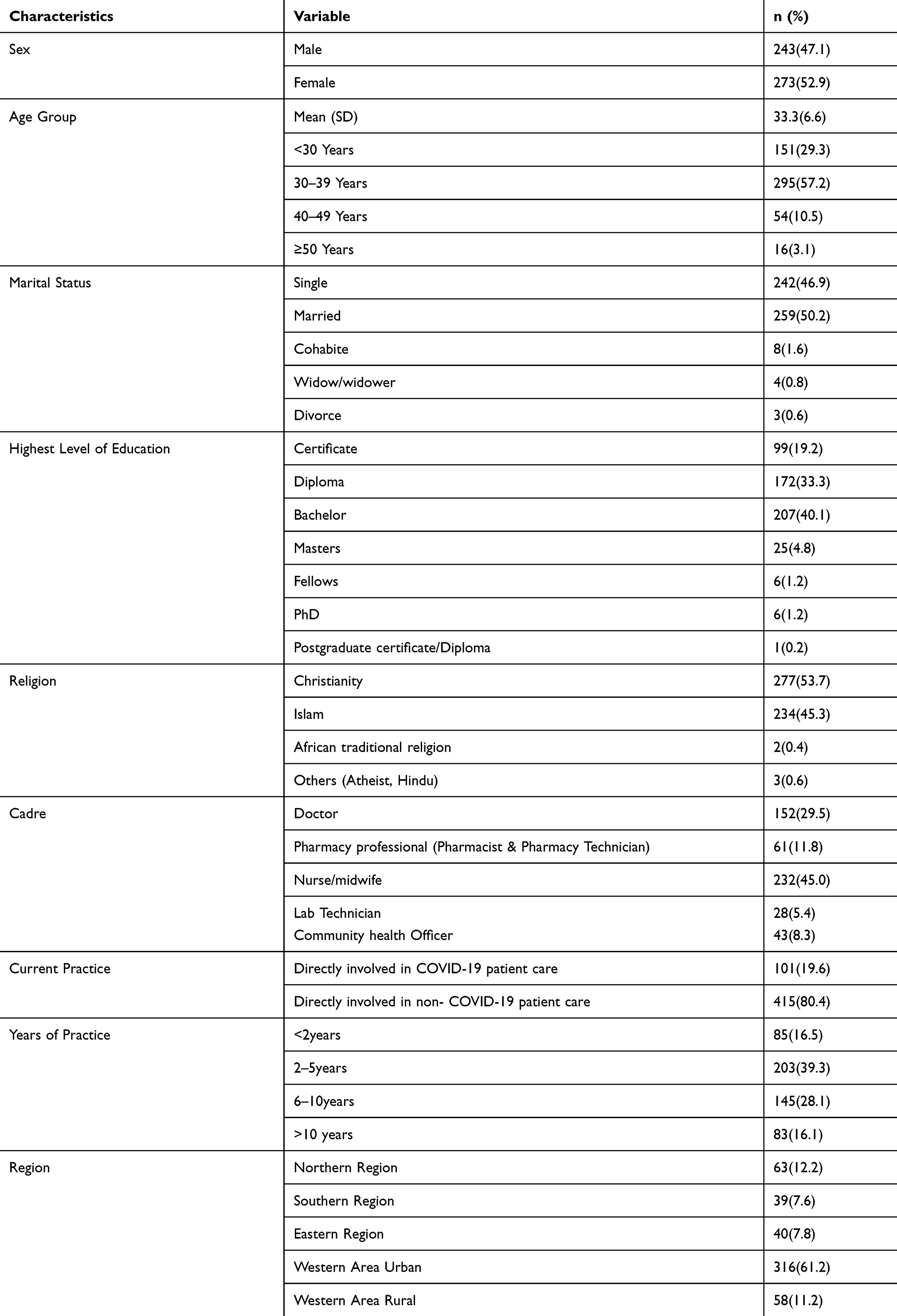 |
Table 1 Characteristics of the Respondents (N = 516) |
Knowledge Among Healthcare Workers Regarding COVID-19
Based on the mean score majority of healthcare workers in this survey reported to be very knowledgeable (16.24 ±1.86; range 5–19) about the cause, transmission, prevention and treatment regarding COVID-19. Close to three-fourth of healthcare workers (n=375, 72.7%) had a knowledge score of at least 16, which indicates good knowledge regarding COVID-19. Specifically, majority of HCWs (n=475, 92.1%) were aware that SARS-COV-2 virus spreads via respiratory droplets of an infected individual. Also, majority knew that a suspected case is any patient with a history of contact with a confirmed or probable COVID 19 case in the last 14 days prior to symptom onset (n=467, 90.5%), and that asymptomatic COVID-19 cases can transmit the SARS-COV-2 virus to other (n=454,88.0%). Please see Table 2 for details. Multivariate backward stepwise binary logistics regression analysis in Table 6 indicates that doctors were more knowledgeable than community health workers and laboratory technicians (AOR= 2.48, 95% CI: 1.16–5.31, p=0.019) regarding COVID-19. However, nurses were less knowledgeable than community health workers and laboratory technicians (AOR= 0.45, 95% CI: 0.24–0.84, p=0.012)
 |
Table 2 Knowledge Among Healthcare Workers Regarding COVID-19 (N = 516) |
 |
Table 3 Healthcare Workers’ Attitude Towards COVID-19 Disease (N = 516) |
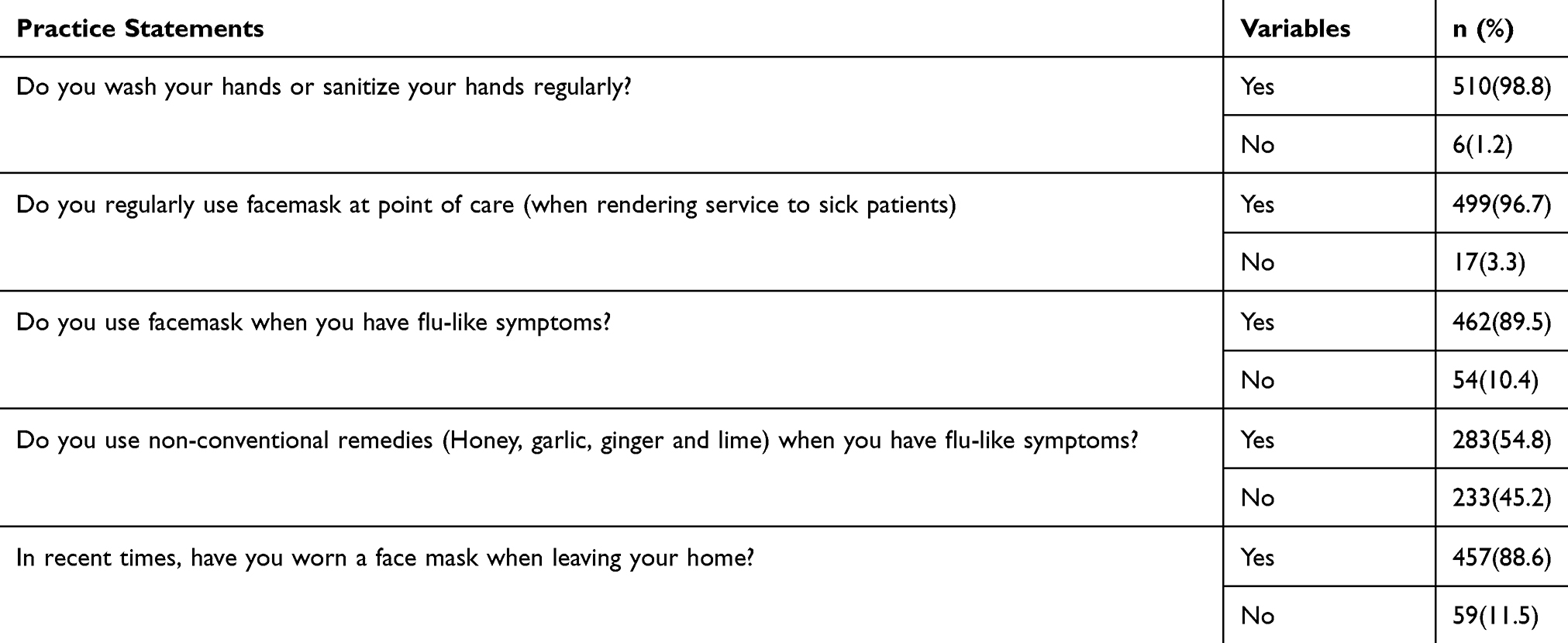 |
Table 4 COVID-19 Prevention Practices Among Healthcare Workers (N = 516) |
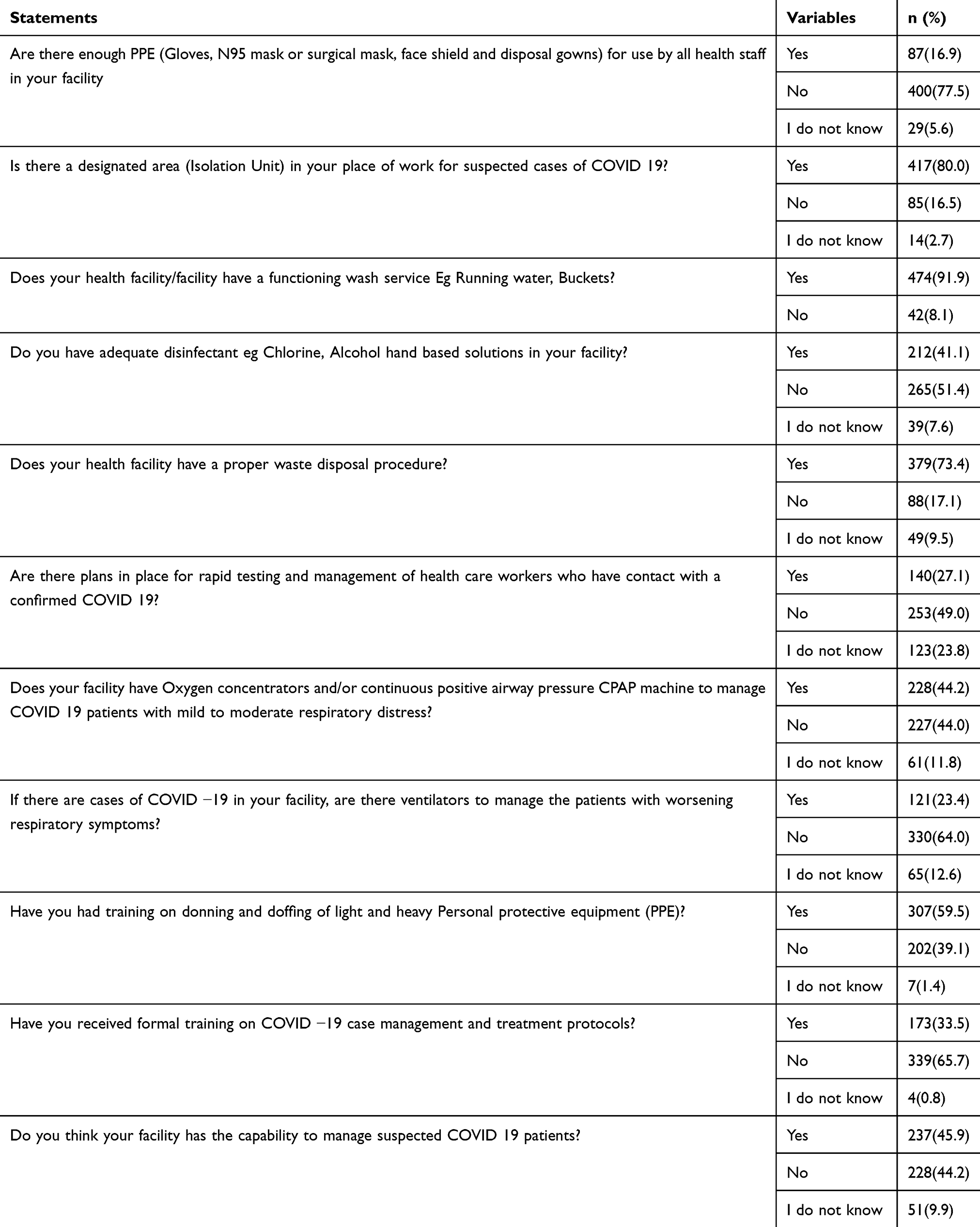 |
Table 5 Healthcare Facility Preparedness (N = 516) |
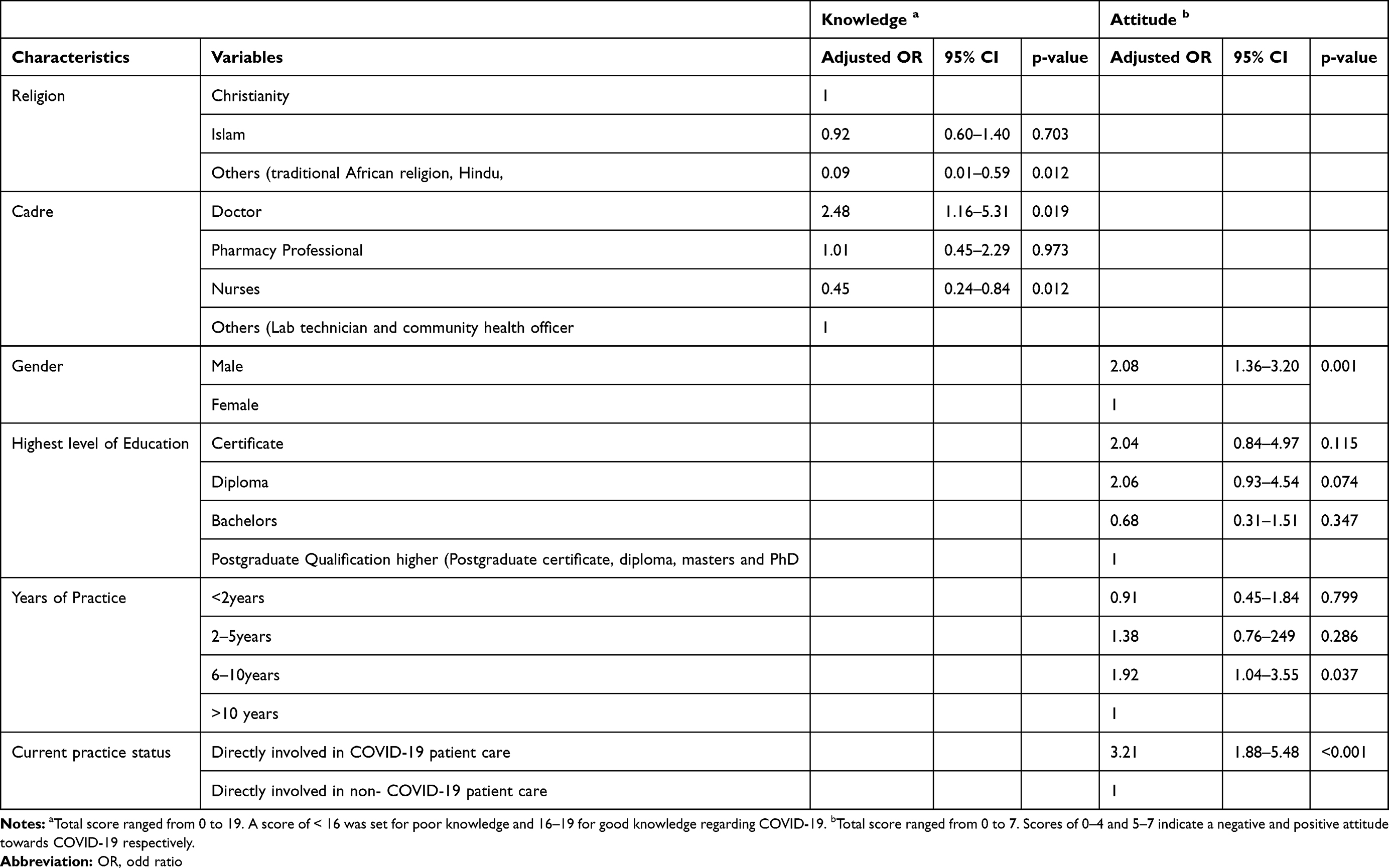 |
Table 6 Backward Stepwise Binary Logistic Regression Analysis for Factors Associated with Good Knowledge and Positive Attitude Towards COVID-19 Among Healthcare Workers in Sierra Leone |
Healthcare Workers’ Attitude Towards COVID-19 Disease
Table 3 shows that healthcare workers generally show a positive attitude toward COVID-19 disease (mean attitude score =4.69 ±1.08). Close to two-thirds of them reported scores of at least 5, which indicates a positive attitude (n=301, 58.3%) toward COVID-19. Majority (n= 508, 98.4%) believed that social distancing and handwashing could prevent against COVID 19, and only a few (n=23, 4.5%) reported that they have gone to any social event recently. On the other hand, approximately half of healthcare workers had the confidence to provide care to a suspected case of COVID 19 (n=274, 53.1%), and are willing to be vaccinated if a COVID-19 vaccine was available (n=280, 54.3%). Results from the multivariate backward stepwise binary logistics regression analysis in Table 6 revealed that males were more likely than females to show a positive attitude towards COVID-19 (AOR=2.08, 95% CI: 1.36–3.20, p=0.001). Also, healthcare workers that have practiced between 6 and 10 years were more likely to have a positive attitude towards COVID-19 than their counterparts who have practiced for more than a decade (AOR=1.92, 95% CI: 1.04–3.55, p=0.037). In addition, healthcare workers who were directly involved in COVID-19 patient care were more likely to have a positive attitude towards COVID-19 (AOR=3.21, 95% CI: 1.88–5.48, p<0.001).
COVID-19 Prevention Practices Among Healthcare Workers
Table 4 shows that healthcare workers are generally adhering to COVID-19 safe practices. For instance, almost all of them reported to wash, or sanitize their hands regularly (n=510, 98.8%), and that they regularly use facemask at point of care (n=499, 96.7%). On the other hand, more than half (n=283, 54.8%) of healthcare workers mentioned that they used non-conventional remedies such as honey, garlic, ginger and lime when they experienced flu-like symptoms.
Healthcare Facility Preparedness
Table 5 summarizes healthcare workers’ assessment of how prepared their healthcare facilities are in responding to the COVID-19 pandemic. In general, majority of HCWs are of the view that their healthcare facilities are ill-prepared to adequately respond to COVID-19. For instance, more than three-quarters (n= 400, 77.5%) of them mentioned that their facilities lack enough PPEs, and these include gloves, N95 mask or surgical mask, face shield and disposal gowns. Similarly, less than a quarter (n=121, 23.4%) stated that their healthcare facilities have ventilators to manage patients with worsening respiratory symptoms. Also, only a third (n=173, 33.5%) of them mentioned that they had received formal training on COVID −19 case management and treatment protocols, and close to half (n=228,44.2%) of them do not think their healthcare facilities have the capability to manage suspected COVID-19 patients.
Discussion
To our knowledge, this is the first study so far in Sierra Leone that have assessed healthcare workers’ knowledge, attitude, practice and perceived health facility preparedness towards COVID-19. This pandemic is affecting every facet of society and a threat to global health security. Given that healthcare workers are the ones leading the fight against this emerging global health threat, they are considered to be at high risk of being infected with the SARS-CoV-2 virus and also the medium of transmission of the virus within and outside the healthcare setting. Thus, an understanding of healthcare workers’ knowledge, attitude, practice and perceived health facility preparedness towards COVID-19 is crucial to preserving the healthcare workforce and protecting the health of the public.
In line with similar studies within11,12,15,18 and outside Africa,13,19–21,23 analysis of our data indicates that the majority of healthcare workers interviewed were knowledgeable regarding the cause, transmission, prevention and treatment of COVID-19. Specifically, approximately three-fourth of healthcare workers had a knowledge score of at least 16, which indicates a very good knowledge regarding the disease. However, our finding is lower than what was reported in recent studies conducted in Egypt,18 Pakistan,13,19 Iran,21 Vietnam20 and China,23 but higher than the values reported by Olum et al in Uganda.12 These differences may be due to variation in the number and content of the knowledge questions. Multivariate analysis further shows that medical doctors and nurses were more and less knowledgeable than community health workers and laboratory technicians regarding COVID-19, respectively. This variation in knowledge regarding COVID-19 among the cadres of healthcare workers is in contrast with a similar study conducted in Uganda,12 in which no differences in knowledge was observed among the various cadres of healthcare workers. This is in contrast to a finding from an Ethiopian study in which level of education was an independent predictor of knowledge11 regarding COVID-19. However, our finding is consistent with similar studies conducted elsewhere,18,21,23 in which medical doctors were more knowledgeable than other cadres of healthcare providers.
Healthcare workers in our study generally show a positive attitude toward COVID-19. Majority believed that social distancing and handwashing could prevent against COVID 19, and have not recently attended any social event. Our finding is consistent with what was reported in similar studies conducted elsewhere,11,13,19,24 but was not in line with a similar hospital-based Cameroonian study.22 Our study also indicates that healthcare workers who were directly involved in COVID-19 patient care were more likely to exhibit a positive attitude towards COVID-19 compared to those that were not directly involved in COVID-19 patient care. Similar findings were observed in studies among healthcare workers in Henan, China.23,25 Healthcare workers directly involved in COVID-19 patient care have increased exposure to the SARS-CoV-2 virus compared to those not directly involved in their care, and therefore, may explain the positive attitude observed among healthcare workers directly involved in COVID-19 patient care. Our study also revealed that close to half of the healthcare workers interviewed indicated that they do not feel confident to provide care to a suspected case of COVID-19. The fear of providing care to COVID-19 patients have been reported in a similar study in Uganda, where 60% of HCWs disclosed that they had avoided suspected COVID-19 patients.12 HCWs’ reluctance or lack of confidence to provide care to suspected COVID-19 patients may likely be due to lack of personal protective equipment and adequate disinfectants in their healthcare facilities. Our speculation is supported by the fact that less than a quarter of HCWs in our study reported that there are not enough PPEs for use in their healthcare facilities. The shortage of PPEs was identified as a key factor that promoted the spread of the Ebola virus disease among HCWs during the West African Ebola outbreak,9 and the shortage of PPEs continues to be a global challenge in the current fight against COVID-19.26,27 Consistent with a study on the acceptance of a potential COVID-19 vaccine among healthcare workers28 and the general population,29,30 our study reports that approximately half of HCWs affirmed that they are willing to take a potential COVID-9 vaccine if and when it is available. Potential COVID-19 vaccine hesitancy among HCWs in our study may be explained by personal risk-benefit perception, which may be informed by false information regarding the safety and effectiveness of the vaccine. Such misinformation can be widespread, given how fast research into developing a COVID-19 vaccine is being conducted. Educational strategies to change perception among HCWs should focus on building and maintaining trust rather than assuming potential COVID-19 vaccine acquiescence by HCWs, including the public, which is based on misinterpretation of science.31
We observed in our study that the majority of HCWs adhere to COVID-19 prevention practices, which is concordant with similar studies conducted in Uganda,12 Pakistan13 and China.23 The routine washing or sanitizing of hands and use of face mask is crucial to preventing transmission of SARS-CoV-2 virus and protecting HCWs and their families. In as much as personal COIVID-19, safe practices by HCWs are critical, health facility preparedness is equally essential in mitigating the transmission of the SARS-CoV-2 virus among HCWs. HCWs in our study are of the view that their healthcare facilities are not well prepared to adequately respond to COVID-19 outbreak. Majority stated that their healthcare facilities lack adequate PPE such as gloves, N95 mask or surgical mask, face shield and disposal gowns. Close to two-thirds of HCWs also mentioned that their healthcare facilities lack ventilators to manage patients with severe respiratory symptoms. HCWs’ perception regarding their healthcare facilities ill-preparedness to appropriately respond to COVID-19 outbreak in our study resonates with findings of a similar study conducted in Jordan.32 In the Jordanian study, only less than a quarter of doctors interviewed reported that all protective measures are available in their healthcare facilities. In addition, an Indian study reported that infection prevention and control measures were suboptimal among the primary healthcare facilities surveyed.33 Healthcare facility preparedness is achieved by making the working environment of HCWs safer through appropriate infection, prevention and control measures.34 Healthcare facility preparedness has been identified in previous infectious disease outbreaks as crucial in curtailing the spread of the disease, and policymakers have been urged to develop structures and provide the required resources that ensure HCWs’ working environment safer during an emerging infectious disease such as COVID-19.35,36 Our findings further reiterate that call for the provision of the required resources, especially training on COVID −19 case management and treatment protocols and PPEs.
Study Limitations
Our study has several limitations that need to be considered when interpreting our findings. First, our study is cross-sectional and therefore, cannot conclude any direct causality between independent and dependent variables. Secondly, we were unable to use a standardized instrument to measure KAP regarding COVID-19 among HCWs, given that the KAP tool was not validated. Thirdly, we used an online survey to capture the views of HCWs, and a convenient sample was employed to target HCWs. With that in mind, our findings may not be representative of all of HCWs in Sierra Leone. However, we were able to capture the views of HCWs across all regions of the country.
Conclusion
Our findings suggest that HCWs in Sierra Leone have good knowledge, positive attitude and good practice regarding COVID-19. However, HCWs are not convinced that their healthcare facilities are well prepared to respond adequately to the COVID-19 outbreak. Health authorities and policymakers need to provide all the required resources to allow HCWs to work in a safer environment.
Abbreviations
AOR, adjusted odd ratio; HCWs, healthcare workers; COVID-19, coronavirus disease; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; KAP, knowledge attitude and practice; PPE, personal protective equipment; WHO, World Health Organisation.
Data Sharing Statement
The datasets used for the current study are available from the corresponding author on reasonable request [email protected].
Ethics
Ethical clearance was obtained from the Sierra Leone ethics and scientific review committee at the Ministry of Health and Sanitation. All respondents provided informed consents before participating in the study, and the information obtained in this study were kept confidential and used only for this research.
Acknowledgments
We would like to extend our thanks and appreciation to all healthcare workers who participated in this study.
Funding
This work was self-funded by the authors.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. New England J Med. 2020;382:727–733. doi:10.1056/NEJMoa2001017
2. Ejaz H, Alsrhani A, Zafar A, et al. COVID-19 and comorbidities: deleterious impact on infected patients. J Infect Public Health. 2020;13:1833–1839. doi:10.1016/j.jiph.2020.07.014
3. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
4. WHO. Rolling updates on coronavirus disease (COVID-19); 2020. Available from: https://wwwwhoint/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen.
5. WHO. WHO Coronavirus Disease (COVID-19) dashboard; 2020. Available from: https://covid19whoint/Accessed.
6. WHO-AFRO. COVID-19 in the WHO African Region; 2020. Available from: https://whomapsarcgiscom/apps/opsdashboard/indexhtml#/0c9b3a8b68d0437a8cf28581e9c063a9.
7. Makoni M. COVID-19 in Africa: half a year later. Lancet Infect Dis. 2020;20(10):1127. doi:10.1016/S1473-3099(20)30708-8
8. Ihekweazu C, Agogo E. ‘ ‘Africa’s response to COVID-19. BMC Med. 2020;18(1):151. doi:10.1186/s12916-020-01622-w
9. Selvaraj SA, Lee KE, Harrell M, Ivanov I, Allegranzi B. Infection rates and risk factors for infection among health workers during Ebola and Marburg virus outbreaks: a systematic review. J Infect Dis. 2018;218(suppl_5):S679–S689. doi:10.1093/infdis/jiy435
10. WHO-AFRO. Situation Update for the African region- external situation report 28. https://wwwafrowhoint/health-topics/coronavirus-covid-19.
11. Kassie BA, Adane A, Tilahun YT, Kassahun EA, Ayele AS, Belew AK. Knowledge and attitude towards COVID-19 and associated factors among health care providers in Northwest Ethiopia. PLoS One. 2020;15(8):e0238415. doi:10.1371/journal.pone.0238415
12. Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. Coronavirus disease-2019: knowledge, attitude, and practices of health care workers at makerere university teaching Hospitals, Uganda. Frontiers Public Health. 2020;8:
13. Saqlain M, Munir MM, Rehman SU, et al. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: a cross-sectional survey from Pakistan. J Hosp Infect. 2020;105(3):419–423. doi:10.1016/j.jhin.2020.05.007
14. Malik UR, Atif N, Hashmi FK, et al. Knowledge, attitude, and practices of healthcare professionals on covid-19 and risk assessment to prevent the epidemic spread: a multicenter cross-sectional study from Punjab, Pakistan. Int J Environ Res Public Health. 2020;17(17):6395. doi:10.3390/ijerph17176395
15. Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health. 2020;48:72. doi:10.1186/s41182-020-00254-3
16. Limbu DK, Piryani RM, Sunny AK. Healthcare ‘workers’ knowledge, attitude and practices during the COVID-19 pandemic response in a tertiary care hospital of Nepal. PLoS One. 2020;15(11):e0242126. doi:10.1371/journal.pone.0242126
17. WHO. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease is Suspected: Interim Guidance. Geneva: World Health Organization;2020; 2020 March 13.
18. Abdel Wahed WY, Hefzy EM, Ahmed MI, Hamed NS. Assessment of knowledge, attitudes, and perception of health care workers regarding covid-19, a cross-sectional study from Egypt. J Community Health. 2020;1–10.
19. Hussain I, Majeed A, Imran I, et al. Knowledge, attitude, and practices toward covid-19 in primary healthcare providers: a cross-sectional study from three tertiary care hospitals of Peshawar, Pakistan. J Community Health. 2020. doi:10.1007/s10900-020-00879-9
20. Huynh G, Nguyen T, Tran V, Vo K, Vo V, Pham L. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13(6):260–265.
21. Maleki S, Najafi F, Farhadi K, Fakhri M, Hosseini F, Naderi M. Knowledge, attitude and behavior of health care workers in the prevention of COVID-19. Research Square. Available from: https://www.researchsquare.com/article/rs-23113/v1. Accessed December 22, 2020.
22. Woromogo SH, Djeukang GG, Yagata MFE. Assessing knowledge, attitudes, and practices of healthcare workers regarding biomedical waste management at biyem-assi district hospital, yaounde: a cross-sectional analytical study. Adv Public Health. 2020;2020:2874064. doi:10.1155/2020/2874064
23. Zhang M, Zhou M, Tang F, et al. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J Hospital Infection. 2020;105(2):183–187. doi:10.1016/j.jhin.2020.04.012
24. Muhammad S, Zia M, Noman A, et al. Knowledge, attitude and preventive practices related to COVID-19 among health professionals of Punjab province of Pakistan. J Infection Developing Countries. 2020;14:07.
25. Zhou M, Tang F, Wang Y, et al. Knowledge, attitude and practice regarding COVID-19 among health care workers in Henan, China. J Hospital Infection. 2020.
26. Ranney ML, Griffeth V, Jha AK. Critical supply shortages—the need for ventilators and personal protective equipment during the Covid-19 pandemic. New England J Med. 2020;382(18):e41. doi:10.1056/NEJMp2006141
27. Bauchner H, Fontanarosa PB, Livingston EH. Conserving supply of personal protective equipment—a call for ideas. JAMA. 2020;323(19):1911. doi:10.1001/jama.2020.4770
28. Dror AA, Eisenbach N, Taiber S, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. 2020;35(8):775–779. doi:10.1007/s10654-020-00671-y
29. Barello S, Nania T, Dellafiore F, Graffigna G. Vaccine ‘hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur J Epidemiol. 2020;35(8):781–783. doi:10.1007/s10654-020-00670-z
30. Palamenghi L, Barello S, Boccia S, Graffigna G. Mistrust in biomedical research and vaccine hesitancy: the forefront challenge in the battle against COVID-19 in Italy. Eur J Epidemiol. 2020;35(8):785–788. doi:10.1007/s10654-020-00675-8
31. Goldenberg MJ. Public misunderstanding of science? Reframing the problem of vaccine hesitancy. Perspectives Sci. 2016;24(5):552–581. doi:10.1162/POSC_a_00223
32. Suleiman A, Bsisu I, Guzu H, et al. Preparedness of frontline doctors in jordan healthcare facilities to covid-19 outbreak. Int J Environ Res Public Health. 2020;17(9):3181. doi:10.3390/ijerph17093181
33. Garg S, Basu S, Rustagi R, Borle A. Primary health care facility preparedness for outpatient service provision during the covid-19 pandemic in india: cross-sectional study. JMIR Public Health Surveillance. 2020;6(2):e19927. doi:10.2196/19927
34. Lee H-Y, Oh M-N, Park Y-S, Chu C, Son T-J. Public health crisis preparedness and response in Korea. Osong Public Health Research Perspectives. 2013;4(5):278–284. doi:10.1016/j.phrp.2013.09.008
35. Jacobsen KH, Aguirre AA, Bailey CL, et al. Lessons from the Ebola outbreak: action items for emerging infectious disease preparedness and response. EcoHealth. 2016;13(1):200–212. doi:10.1007/s10393-016-1100-5
36. Rajakaruna SJ, Liu W-B, Ding Y-B, Cao G-W. Strategy and technology to prevent hospital-acquired infections: lessons from SARS, Ebola, and MERS in Asia and West Africa. Military Med Res. 2017;4(1):32. doi:10.1186/s40779-017-0142-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.