Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Healthcare Workers’ Knowledge, Attitude, and Practice Regarding Personal Protective Equipment for the Prevention of COVID-19
Authors Hossain MA ![]() , Rashid MUB, Khan MAS
, Rashid MUB, Khan MAS ![]() , Sayeed S
, Sayeed S ![]() , Kader MA, Hawlader MDH
, Kader MA, Hawlader MDH ![]()
Received 27 November 2020
Accepted for publication 30 December 2020
Published 2 February 2021 Volume 2021:14 Pages 229—238
DOI https://doi.org/10.2147/JMDH.S293717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohammad Ali Hossain,1 Md Utba Bin Rashid,2 Md Abdullah Saeed Khan,3 Sabrina Sayeed,4 Md Abdul Kader,5 Mohammad Delwer Hossain Hawlader6
1Ibn Sina Medical College Hospital, Dhaka, 1216, Bangladesh; 2Nutrition and Clinical Services Division (NCSD), International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), Mohakhali, Dhaka, 1212, Bangladesh; 3Infectious Disease Hospital, Dhaka, 1212, Bangladesh; 4Eminence Associates for Social Development, Dhaka, 1207, Bangladesh; 5International Organization for Migration, Cox’s Bazar, 4700, Bangladesh; 6Department of Public Health, North South University, Dhaka, 1229, Bangladesh
Correspondence: Md Utba Bin Rashid
Nutrition and Clinical Service Division (NCSD), International Centre for Diarrhoeal Disease Research, Bangladesh, Mohakhali, Dhaka, 1212, Bangladesh
Tel +8801673306380
Email [email protected]
Purpose: Adequate knowledge, positive attitude, and proper practice of personal protective equipment by healthcare workers are necessary to get protection from COVID-19 infection. But this area is yet to be explored. Hence, we aimed to assess the knowledge, attitude, and practice (KAP) regarding personal protective equipment (PPE) among healthcare workers, along with a survey of the possible determinants.
Subjects and Methods: For this cross-sectional study, online and offline surveys were conducted among a sample of 393 healthcare workers from five different districts of Bangladesh. A validated self-administered questionnaire comprising five sections (socio-demography, work-related information, knowledge, attitude, and practice) was used for data collection. Multivariate stepwise forward logistic regression was applied to find significant factors associated with good attitude, and practice using SPSS version 25.
Results: The average age of the 393 participants was 28.9± 5.2 years with a male-female ratio of one. Of them, 99.5% (n=391) had good knowledge, 88.8% (n=349) had positive attitude and 51.7% (n=203) had good practice regarding PPE. Results revealed that being a physician and living at home were significantly associated with a positive attitude. While being a non-physician, having lower education, working in private hospitals, and using office transport were associated with good practice regarding PPE.
Conclusion: The findings demonstrated that the healthcare workers had an overall good knowledge and a positive attitude but a poor practice regarding PPE. This study also highlighted the factors influencing KAP towards PPE that must be addressed in future education, awareness, and counseling programs.
Keywords: knowledge, attitude, practice, personal protective equipment, health personnel
Introduction
Coronavirus Disease 2019 (COVID-19), a deadly respiratory disease caused by SARS CoronaVirus-2 (SARS CoV-2), was declared a global pandemic on 11th March 2020 by World Health Organization (WHO).1,2 As of 21st October 2020, over 40 million cases and over 1 million deaths due to COVID-19 were reported around the world.3 Bangladesh is in the phase of community transmission and has so far confirmed 390,206 cases and 5681 deaths.4 Due to transmission from asymptomatic individuals, the disease is expected not to go away any sooner. As a result, there is a continuous need for frontline healthcare workers (HCW) for the management of COVID-19 patients, making them the most vulnerable group to contract the disease.5 According to WHO estimates, around 14% of those affected are HCWs.6 A study conducted among the HCWs working in a COVID-19 dedicated hospital in Bangladesh found than 10.79% of them contracted the disease.7
Coming into close contact with COVID-19 patients during the symptomatic period is associated with a high transmission risk.8 HCWs involved in the management of patients and the collection, extraction, and preparation of samples for rt-PCR testing are frequently exposed to symptomatic cases, increasing their risk of getting the virus. However, the transmission risk can be reduced with the proper use of Personal Protective Equipment (PPE).9 During the onset of the pandemic, the main concern was an inadequate supply of personal protective equipment for healthcare workers and a lack of training regarding its use. Bangladesh was not well-prepared with sufficient healthcare facilities, personal protective equipment, and testing kits to fight the COVID-19 at the incipient phase of the outbreak.10,11 Consequently, HCWs might have been deprived of systematic training and practice regarding PPE.
WHO recommends regular hand washing, physical and social distancing, keeping rooms well-ventilated, and respiratory hygiene to prevent COVID-19 transmission.12 Although these measures may reduce the risk in the wider community, HCWs are likely to encounter repeated close exposures due to their nature of work. Guidelines and online refresher courses were developed by WHO, CDC (Center for Disease Control and Prevention), and various governmental and private organizations in different countries to boost infection prevention and control (IPC) strategies in healthcare facilities. Despite the availability of guidelines, attitude and practice towards infection control and prevention measures might vary because of the socioeconomic contexts, preparation of the healthcare system, and the beliefs and motivation of the HCWs of a country. It can be reasonably assumed that good knowledge and a positive attitude regarding the use of personal protective measures should lead to the proper practice of IPC. However, no study has assessed the KAP of PPE among health personnel so far. Therefore, the purpose of the study was to assess the KAP regarding PPE among HCWs who are at increased risk of exposure to SARS-CoV2 due to involvement in the management of COVID-19 patients.
Subjects and Methods
Study Design
This cross-sectional study was carried out from June to July 2020. The study population was Bangladeshi frontline healthcare providers who were combating the COVID-19 disease by treating the affected individuals admitted into government and private healthcare facilities. Since the country maintained a lockdown and movement restriction to reduce the spread of COVID-19, participants were conveniently selected using both offline and online methods to ensure optimum coverage in this pandemic situation. In face-to-face interviews, data were collected from HCWs of the five districts – Dhaka, Kishoreganj, Chuadanga, Mymensingh, and Cox’s Bazar, where a significant proportion of the COVID-19 patients of Bangladesh were reported. On the other hand, a self-reported structured questionnaire was prepared and incorporated in Google forms in the web-based approach. The link was shared through email, different social platforms (Facebook, WhatsApp, Viber, Twitter), and other authors’ networks. Since no previous study was conducted among the HCWs regarding their KAP towards PPE, the target sample size was estimated based on WHO recommendations for the minimal sample size needed for a prevalence study.13 Anticipating a population proportion of 50%, confidence interval 95%, and relative precision 10% (of 50%), the required sample size was calculated 384. HCWs, including doctors, nurses, pharmacists, and lab technicians, were eligible for this study. Bangladeshi nationals of age 18 or more who worked in an active healthcare facility were involved in the management of COVID-19 patients and consented to fill the form were invited to take part. The original questionnaire was prepared using the English language, further transcribed into Bangla to adopt generalizability among the study participants. All eligible respondents volunteered to participate in the survey. Eventually, 405 valid responses were collected during the survey period, and a total of 393 responses were kept after the exclusion of incomplete data.
Measures
The survey tool was developed based on a considerable literature review, PPE wearing guidelines for the healthcare providers by WHO,9,14 guidelines issued by CDC,15 and the national guidance for the COVID-19 response, Bangladesh.16 After preparing the initial draft of the questionnaire, we validated it in two steps. Firstly, we shared the tool with the study supervisor and the other researchers to give their expert opinion concerning its clarity, relativity, and significance. Secondly, a pilot study was performed by selecting a limited number of healthcare workers (n = 40) who shared their views on simplifying and shortening the questionnaire. Members from all healthcare settings were chosen for the pilot study. Participant amendments were considered and mended into the survey, thus maintaining continuity with the contemporary literature. After a thorough discussion, the authors finalized the questionnaire and dispensed it to the HCWs.
This survey comprised questions evaluating socioeconomics, job type, and knowledge, attitude, and practice of HCWs regarding PPE (Supporting information: Supplement 1). Demographic characteristics included gender, age, marital status, household members, occupation, job experience, and one item on PPE wearing. Work-related factors encompassed the type of establishment where a healthcare provider was currently rendering his/her services, his/her placement in the workplace, duty hour, place of living during that time, and lastly, transportation facilities towards the workplace.
The knowledge section incorporated ten items, and the answer to each question was either ‘Yes’ or ‘No’. The accurate answer was recorded as one, while the incorrect response was noted as zero. A cut-off level of ≤6 for poor understanding and ≥7 for useful knowledge was determined. The total score extends from 0 to10. The attitude section consisted of 8 items, and responses of each piece were documented on a 5-point Likert scale as follows: strongly agree (5-point), agree (4-point), neutral (3-point), disagree (2-point), and strongly disagree (1-point). The total score ranged from 8 to 40, with a mean score of ≥24 indicating a positive attitude toward using PPE. The practice section included 15 items, and each item comprised two responses: Yes (1-point) and No (0-point). Practice items total score ranged from 0 to15. A score of 9–15 indicated good practice and of 1–8 demonstrated poor practice toward wearing PPE during service hour. Finally, a question assessed the perception of HCWs regarding barriers in infection control practice. Content validity and reliability tests for the question construct on KAP assessment were within an acceptable range (Tables S1 and S2; Supporting information: Supplement 2). Almost all of the knowledge, attitude, and practice related questions in the relevant subsections of the questionnaire had significant content validity. Reliability scores (i.e., Cronbach’s Alpha values) for knowledge, attitude, and practice related questions were, respectively, 0.181, 0.643, and 0.735. The knowledge section’s low scores were due to dichotomous response categories and a highly skewed response proportion.
Statistical Analysis
Continuous variables were described as mean ± standard deviation (SD), while categorical variables were expressed as frequencies and percentages. The association between different responses and respondent’s characteristics was analyzed using the Chi-square test of independence. Univariate logistic regression was used to calculate the odds ratios (ORs) and the corresponding 95% confidence intervals (95% CIs) to analyze the associations between individual determinants and the respondent’s good attitude and practice. Multivariate logistic regression was conducted using the stepwise forward LR method. SPSS Inc. v25 was used for statistical analysis. Content validity and reliability were tested using Pearson’s correlation and Cronbach’s Alpha statistic, respectively. All analyses were two-sided, and P < 0.05 was regarded as statistically significant.
Ethics
All the procedures were conducted following the ethical guidelines of the institution’s review board (IRB)/ethical review committee (ERC) of North South University, Bangladesh (Memo no. 2020/OR-NSU/IRB-No.0803). The ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards were followed wherever applicable. During the face-to-face interview, informed written consent was obtained from all the participants involved in the study. However, electronic consent was attached to the web-based questionnaire where the nature, purpose, and objective of the study were clearly stated along with the declaration of confidentiality and anonymity.
Results
A total of 393 participants were included in the study. The average age of the participants was 28.9±5.2 years, most of them were aged between 21 and 30 years (76.8%), and the male-female ratio was approximately one. Nearly one-quarter of the participants completed a diploma, and 64.9% completed graduation (bachelor). Maximum participants were physicians (70.7%), and among the rest non-physicians, respectively, 27, 1.3, and 1% were nurses, pharmacists, and laboratory technicians. Among all, 45.5% were staying at home, followed in decreasing order by hostel (24.4%), dormitory (14.8%), hospital (8.9%), and hotel (6.4%). Participants had a median work experience of 4 years. Most of them were doing government jobs (53.4%), working indoors (68.4%), and were going to duty stations mostly by walk (43.0%) (Table 1). Only 25.2% of participants read one of the guidelines on PPE (Figure S1; Supporting information: Supplement 3).
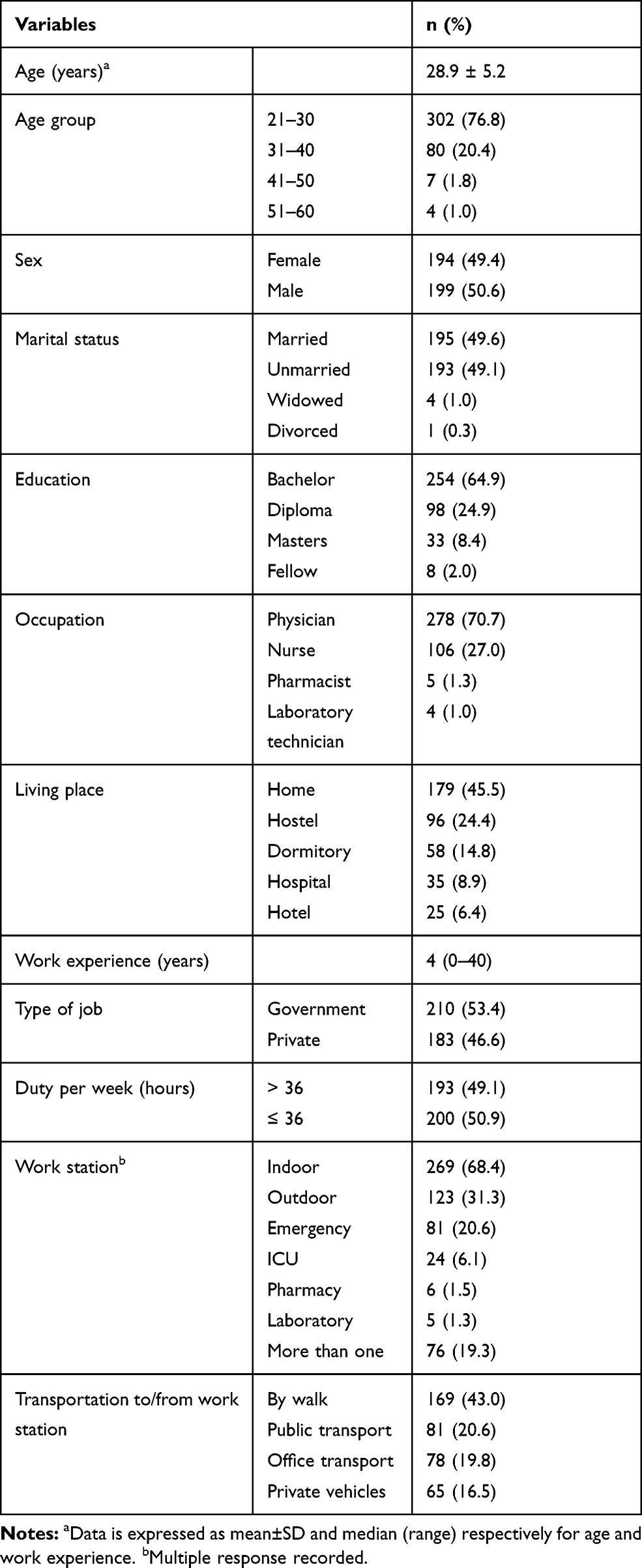 |
Table 1 Socio-Demographic Profile and Work-Related Characteristics of Participants (n=393) |
Among all, 99.5% had good knowledge, 88.8% had positive attitudes, and 51.7% had good practice regarding PPE (Table 2). There was no difference in knowledge of PPE between physicians and non-physicians. Significantly more physicians had a positive attitude than non-physicians toward PPE. But the practice regarding PPE was significantly better among non-physicians than physicians.
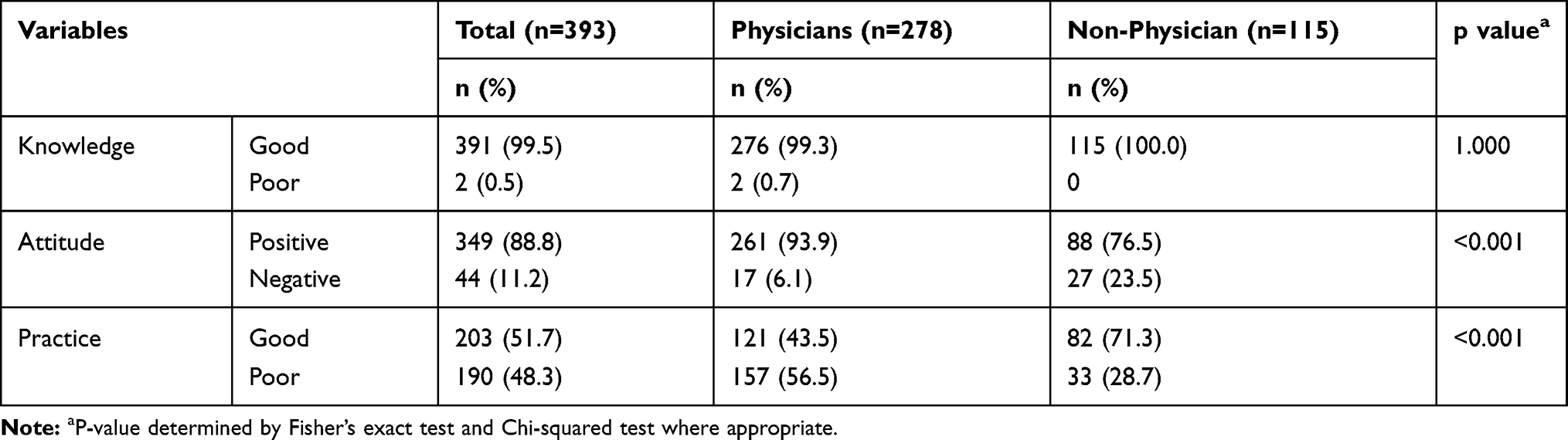 |
Table 2 Knowledge, Attitude, and Practice Regarding PPE Among Participants |
Although participants, in general, had good knowledge regarding PPE, 34.6% thought all components of PPE (except N95 mask) are not required at the hospital outdoor during treating patients with respiratory symptoms. However, 22.1% thought that family members providing care to COVID-19 patients would not get enough protection wearing a surgical mask and maintaining hygiene only. Among all, 14.5% of participants did not know about donning and doffing process. Among the eight items in the attitude questionnaire, variability in response occurred in four. Nearly one-tenth of the participants thought that using PPE is not going to keep HCWs safe from COVID-19. One-tenth found wearing PPE is inconvenient. One-fifth did not feel protected wearing PPE, and nearly one-third were dissatisfied with the PPE they were using.
Regarding the practice of PPE, 75.8% were not using PPE regularly during patient care, 62.6% did not do any fit test after wearing a mask, 58.3% did not get any training on the use of PPE, and 41.7% were not using any disposable PPE. Among the participants, 40.2% did not follow proper donning/doffing methods, and 62.6% did not use any biohazard bag during the disposal of the PPE. Surgical masks and N95 or equivalent masks were used by, respectively, 87.8 and 71% of participants. Close to 79% used gown/cover-all, 94.1% used gloves during patient care, 84% regularly disinfected or disposed of their gloves, and 85.8% used goggles and/or face-shield during duty. See Tables S1–S3 (Supporting information; Supplement 3) for the detailed item list with the frequency of responses.
Logistic regression analysis of factors associated with attitude towards PPE showed that being a physician was associated with 4.548 times higher odds of having a positive attitude than non-physicians after adjusting for age, sex, marital status, education, job type (government vs. private), work hours, and workstation. Participants living in the hospital and hotel rather than at home were 81.8 and 78.8% less likely to have a positive attitude towards PPE (Table 3).
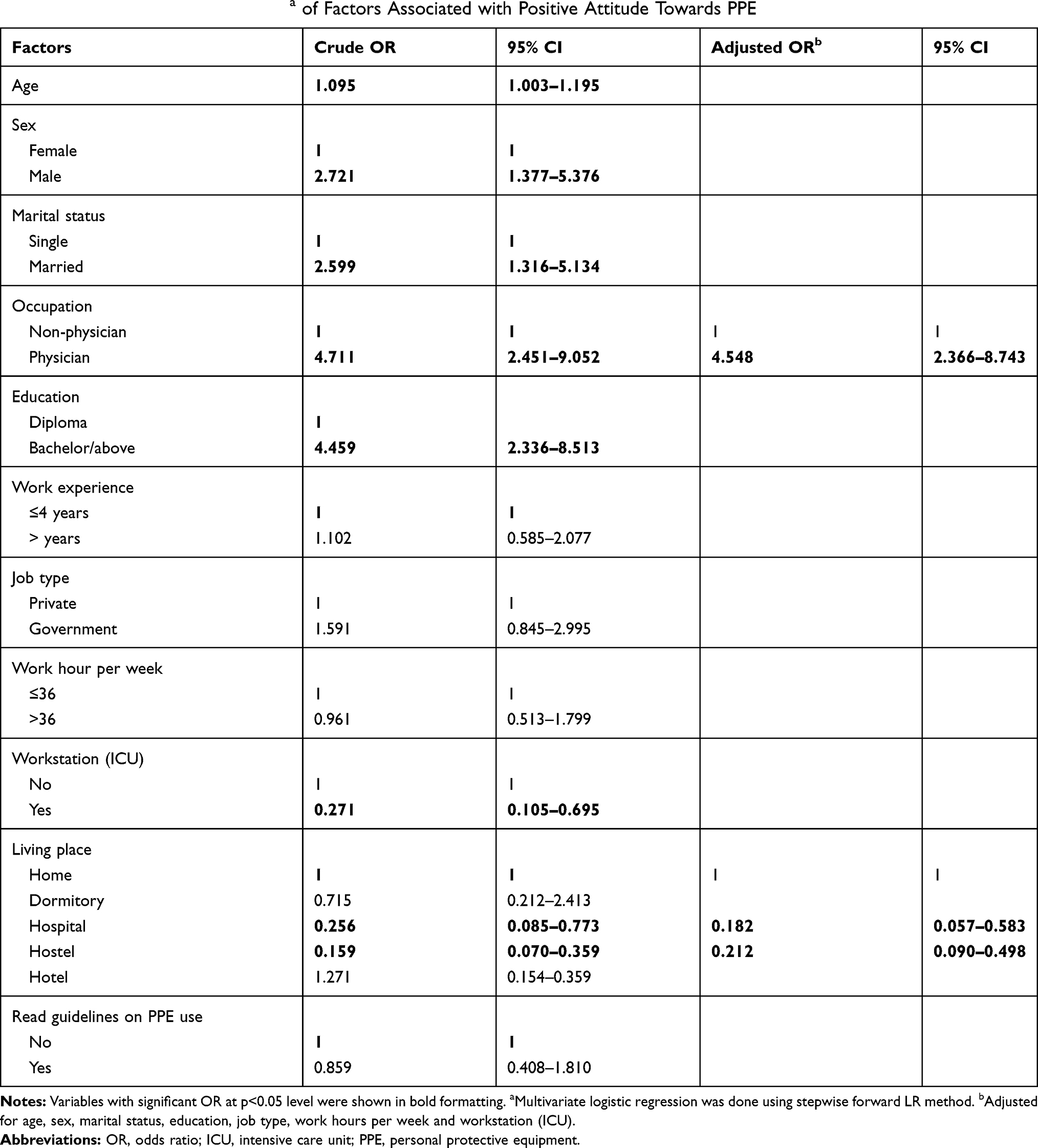 |
Table 3 Logistic Regression Analysisa of Factors Associated with Positive Attitude Towards PPE |
When adjusted for age, sex, marital status, occupation, work experience, work hours per week, work station (ICU), and living place, those who used office transport were 3.491 times, and those who read the guidelines of PPE use were 1.962 times more likely have good practice in comparison to those who walked to their office and who did not read guidelines, respectively (Table 4). Participants who completed a bachelor’s degree were 71.5% less likely to have good practice in comparison to those who completed a diploma, and government-employed healthcare workers were 80.9% less likely to have good practice in comparison to those who were doing private jobs.
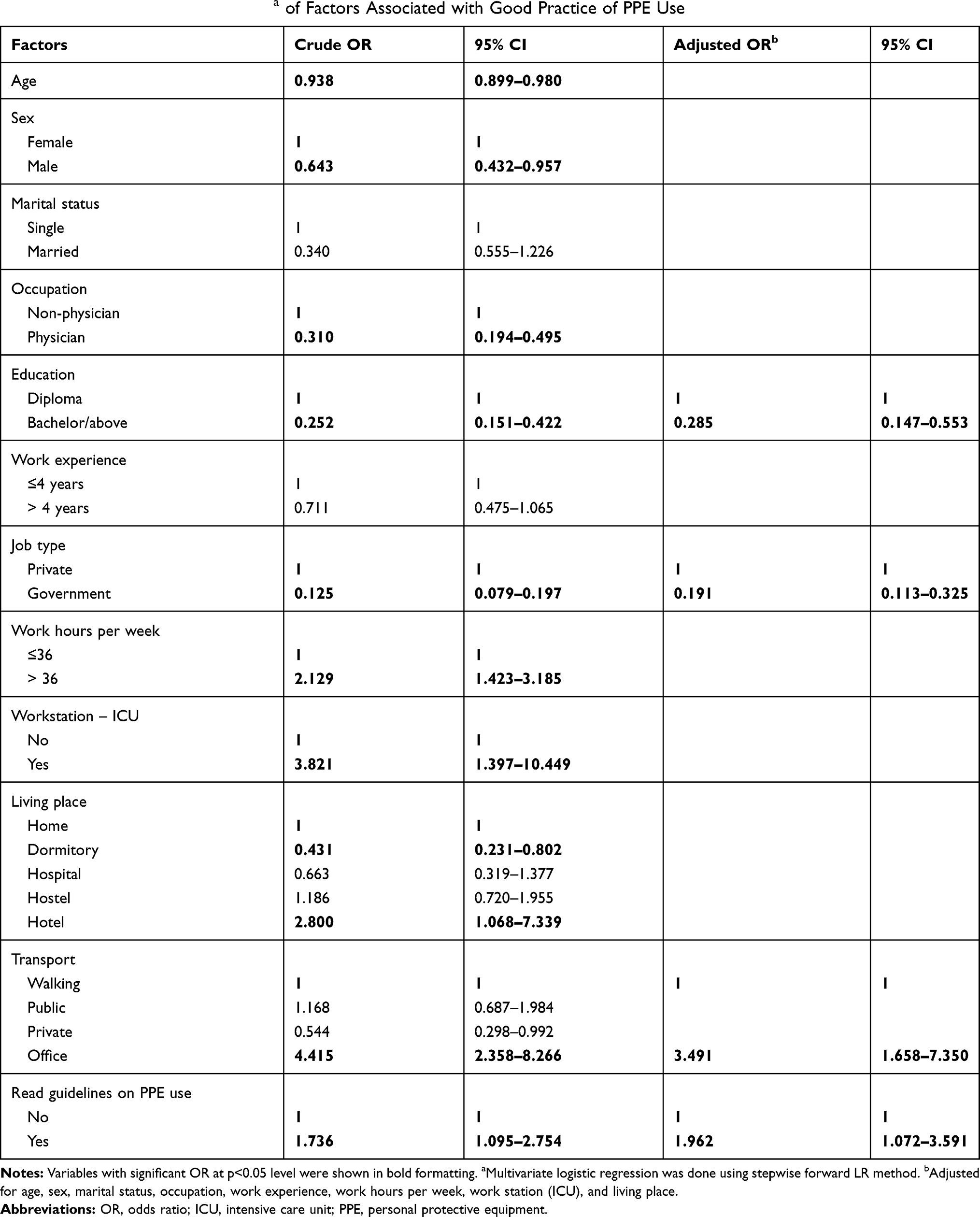 |
Table 4 Logistic Regression Analysisa of Factors Associated with Good Practice of PPE Use |
Knowledge and attitude were weakly positively correlated with practice (r=0.142 and 0.242, respectively, p<0.05 for both) among the participants (Table 5).
 |
Table 5 Pearson Correlation Among Knowledge, Attitude, and Practice Scores |
Discussion
Healthcare workers play a pivotal role in COVID-19 management as front-liners. They are the first point of contact with COVID-19 patients in hospitals and laboratories. Hence, they are at high risk for severe acute respiratory syndrome from SARS-COV-2 infection.17,18 The best way for HCWs to prevent this infection is through practice and demonstrated competency in donning, doffing, and proper use of personal protective equipment (PPE).19 Hence, an assessment of the current status of knowledge, attitude, and practice towards PPE among HCWs were duly needed. According to the best of our knowledge, this is the first-ever study that entirely assessed the knowledge, attitude, and practice regarding PPE among HCWs towards COVID-19 in Bangladesh.
Participants of our study were predominantly young adults with an average age of 28.9 ± 5.2 years, and a male-female ratio of approximately one. As evidence started to accumulate that older people are particularly vulnerable to COVID-19-related mortality,20 young HCWs came to the forefront of the front-liners. As this study was conducted among the front-liners, older personnel might have sieved out of from the respondents.
All of our participants were educated, with the lowest education status being diploma (24.9%). The rest of the participants pursued qualifications ranging from undergraduate to post-doctoral. This ensured a high standard of responses to the technical questions that were posed during the data collection.
We found that 99.5% of the participants had good knowledge regarding PPE, where physicians and non-physicians both had an almost equal level of knowledge. Recent studies conducted in China,21 Iran,22 Pakistan,23 and Turkey24 found a good knowledge about COVID-19 (and the ways of protection from it) among, respectively, 88.4%, 56.5%, 93.2%, and 90% of their participants comprised various categories of HCWs. Our study results provide confidence in terms of the healthcare workers’ knowledge regarding the transmission, protection, and preventive measures of COVID-19, which is a good sign in the present situation because no vaccine is available yet. As the fight against COVID continues, HCWs must remain familiar with all the precautionary steps regarding PPE to save them from this pandemic.24–26 Despite a good average score in the knowledge questionnaire, we found a remarkable absence of knowledge regarding the proper donning and doffing method indicating an absence of training regarding PPE among the HCWs. As such a widespread outbreak had not happened in recent history, it is expected that not every HCW would have adequate knowledge regarding donning and doffing. But the current situation necessitated training of all HCWs on the PPE. Hence, a lack of knowledge is reminiscent of inadequate preparedness of the health system to handle such an infectious emergency.
This study demonstrated that 88.8% of the participants had a positive attitude towards PPE in COVID-19 management. But the proportion of HCWs having a positive attitude differed significantly between non-physician (76.5%) and physician (93.9%). Educational differences between these groups might explain this finding because a higher educational attainment was found to be associated with a positive attitude in our study as well as in studies investigating KAP about COVID-19.25
Univariate regression showed that higher age, male gender, being married, being a physician, living at home, and higher education was significantly associated with a positive attitude. Although after adjustments, being a physician and living at home were found to be the independent influencing factors. Lombardi et al27 noted that attitude towards the use of PPE among industrial workers could be influenced by “perceptions of hazards and risk”, “barriers to PPE use” and “enforcement and reinforcement”. These findings correlate with the findings of our study as we noted a tuned down perception towards the protective function of PPE because of the dissatisfaction with the supplied PPEs and discomfort of wearing those. HCWs who were attending their duty from home were most likely to be reinforced by a protective responsibility to family members. This assumption is also endorsed by the fact that we found married HCWs having a significantly higher odds of having a positive attitude (OR 2.599, 95% CI 1.316–5.134). In addition, good knowledge might have shifted the attitude towards the favorable side among the HCWs, as is evident in other studies.23
Contrary to what would be expected from people with a positive attitude, we found that nearly half (48.3%) of the respondents showed poor practice regarding PPE in our study. Moreover, a significantly higher proportion of non-physician (71.3%) showed good practice compared to physicians (43.5%). When considered individually, a younger age, female sex, being non-physician, a lower education (having diploma instead of graduation and above), being in the private job, working more than 36 hours, working in ICU, living in the hotel, provision of office transport, and reading the guideline on PPE use was associated with good practice. However, on multivariate regression, lower education, being in a private job, provision of office transport, and reading the guidelines were found to be independently associated with good practice regarding PPE use.
Although government authorities have ensured an adequate supply of PPE lately, a lack of other measures as well as the questionable quality of the equipment might affect the trust and practice towards PPE among the HCWs working in these facilities.27,28 While private hospitals might have ensured the provision of an adequate supply of high-quality PPE, proper donning, doffing, and disposal arrangements, training regarding its use, and administrative supervision and monitoring regarding protection measures, ensuring the significantly better practice (80.9% better) among private HCWs. Previously Andaleeb29 has shown that private hospitals can ensure better quality service than government hospitals in Bangladesh because they generate their financial resources from clients. This might also be applicable in case of infection prevention and control measures taken by the private facilities. We found that HCWs who use office transport had a higher odds (OR: 3.491, 95% CI 1.658–7.350) of good practice regarding PPE compared to those who walk to the hospitals. A provision of office transport could have given HCWs the opportunity to put on their PPE at their home before leaving for the duty station. In addition, commuting in public and/or private transport might have been associated with a perceived fear of inadequacy of protective measures. In such a setting, dedicated office transports can increase the perceived protection among their users. Another counterintuitive finding was the association of relatively lower education (having a diploma compared to having a bachelorette or higher-level degree) with good practice. This also reflects that non-physician were more likely to do a good practice regarding PPE than physicians. But further research is required to explore this interesting association.
The transmission of COVID-19 can be prevented if the healthcare workers wash their hands, maintain hygiene, and take precautions by wearing PPE properly. The study conducted by Kara et al,26 Mohammad et al,30 Naser et al,31 and Saqlain et al23 indicated that healthcare workers with good knowledge regarding COVID-19 had a good attitude and showed good practices. But in this study, we found only a weak positive correlation between knowledge or attitude and practice scores. A considerable proportion of HCWs had good knowledge (99.5%) and a positive attitude (88.8%) regarding PPE, but the good practice was found only among 51.7% of participants. We have highlighted some of the possible reasons and factors behind such findings, but specific causes need to be explored. Good knowledge, positive attitude, and proper practices among healthcare workers regarding basic protective measures are necessary to deal with COVID-19 affected people as it decreases the chances of transmission. Moreover, the current pandemic has made it mandatory for HCWs to increase their protection. Proper practice of HCWs in complying with precautionary measures will not only save them from COVID-19 but also create awareness among the patients as well as the population in general.
We recommend the following measures in light of the findings of our study. Further large-scale explanatory research (both qualitative and quantitative) should be conducted to find out the causes behind poor practice regarding PPE among the healthcare workers of Bangladesh. Appropriate measures should be taken at the policy level to ensure adequate infection prevention and control measures. Training sessions regarding the use of PPE should be arranged on a regular basis. Strong monitoring and evaluation need to be introduced to ensure the proper practice of PPE.
The major limitation of our study was the inability to randomize the participants. In addition, as the study was conducted mainly through an online self-administered questionnaire, we could not observe the practice of PPE use rather had to rely on self-reported assessment for that. Another limitation was that we failed to collect adequate participation from the laboratory technicians and pharmaceuticals; as a result, our study findings regarding the non-physicians mainly represented nurses.
Conclusion
COVID-19 is currently the burning topic all around the world, including Bangladesh, due to its deadly nature. To mitigate its aftermath, it is now necessary for the government to adopt some immediate steps towards developing and honing positive practices to protect the communities better. To our knowledge, our current study is a unique one where we tried to describe the experience, attitude, and approach of all the frontline HCWs of our country regarding the use of PPE, which is the essential tool for them to be practiced for safekeeping. However, we identified a significant gap in practice toward using PPE among our healthcare workers. Interestingly, we found that education, reading guidelines, and lack of proper training opportunities are the steering factors leading to variation among our study participants. As the global threat of COVID-19 continues, more significant efforts through educational campaigns that target HCWs and the broader population beyond borders are urgently needed in our current context as most of us must adjust to this new normal phenomenon.
Strobe Statement
A STROBE checklist for this study is available as supplement 4 (Supporting information: Supplement 4).
Data
Available as electronic supplement (Supporting information: Supplement 5).
Ethical Approval
The study was ethically approved by institution’s review board (IRB)/ethical review committee (ERC) of North South University, Bangladesh (Memo no. 2020/OR-NSU/IRB-No.0803).
Acknowledgments
The authors acknowledge the participants for providing the information to conduct the study. The authors would like to thank Dr. Mostak Ahmed, Dr. Hadi Zia Uddin, Dr. SK Mahmud Hasan, and Dr. Tamim Al Mishu for helping in the data collection process.
Funding
No funding was recieved for this study.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Ducharme J. World Health Organization declares COVID-19 a “pandemic”: here’s what it means. Time. 2020. Available from: https://time.com/5791661/who-coronavirus-pandemic-declaration/.
2. Yin Y, Wunderink RG. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology. 2018;23(2):130–137. doi:10.1111/resp.13196
3. World Health Organization. WHO Coronavirus Disease (COVID-19) dashboard. 2020. Available from: https://covid19.who.int/.
4. World Health Organization. WHO Bangladesh COVID-19 Morbidity and Mortality Weekly Update (MMWU). 2020. Available from: https://www.who.int/docs/default-source/searo/bangladesh/covid-19-who-bangladesh-situation-reports/who-covid-19-update-34-20201019.pdf?sfvrsn=e47d5329_2.
5. Black JRM, Bailey C, Przewrocka J, Dijkstra KK, Swanton C. COVID-19: the case for healthcare worker screening to prevent hospital transmission. Lancet. 2020;395(10234):1418–1420. doi:10.1016/S0140-6736(20)30917-X
6. World Health Organization. Keep health workers safe to keep patients safe: WHO. 2020. Available from: https://www.who.int/news/item/17-09-2020-keep-health-workers-safe-to-keep-patients-safe-who.
7. Yasmin R, Parveen R, Azad NA, et al. Corona virus infection among healthcare workers in a COVID dedicated tertiary care hospital in Dhaka, Bangladesh. J Bangladesh Coll Phys Surg. 2020;38(July):43–49. doi:10.3329/jbcps.v38i0.47442
8. Liu T, Liang W, Zhong H, et al. Risk factors associated with COVID-19 infection: a retrospective cohort study based on contacts tracing. Emerg Microbes Infect. 2020;9(1):1546–1553. doi:10.1080/22221751.2020.1787799
9. World Health Organization. Rational use of Personal Protective Equipment (PPE) for Coronavirus Disease (COVID-19): interim guidance. 2020. Available from: https://apps.who.int/iris/handle/10665/331695.
10. Anwar S, Nasrullah M, Hosen MJ. COVID-19 and Bangladesh: challenges and how to address them. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.00154
11. Howlader T, Khan HR. Battling the COVID-19 pandemic is Bangladesh prepared. Medrxiv. 2020:1–20. Available from: http://medrxiv.org/cgi/content/short/2020.04.29.20084236. Accessed January 11, 2021.
12. World Health Organization. Coronavirus Disease (COVID-19) advice for public. 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public.
13. Lwanga SK, Lemeshow S, World Health Organization. Sample size determination in health studies: a practical manual/S. K. Lwanga and S. Lemeshow. 1991. Available from: https://apps.who.int/iris/handle/10665/40062.
14. World Health Organization. Contact droplet COVID-19 precautions. 2020. Available from: https://www.who.int/csr/resources/publications/Contact-Droplet-COVID-19-Precautions.pdf?ua=1.
15. Center for Disease Control and Prevention. Guidance for the selection and use of Personal Protective Equipment (PPE) in healthcare settings. 2020. Available from: https://www.cdc.gov/hai/pdfs/ppe/PPEslides6-29-04.pdf.
16. Directorate General of Health Service. National guidelines on clinical management of Coronavirus Disease 2019 (Covid-19). 2020. Available from: https://dghs.gov.bd/images/docs/Guideline/COVID_Guideline_v7.pdf.
17. Siddiqui MK, Parcell B, Allstaff S, Palmer C, Chalmers JD, Bell S. Characteristics and outcomes of health and social care workers testing positive for SARS-CoV-2 in the Tayside region of Scotland. Eur Respir J. 2020;56(3):2002568. doi:10.1183/13993003.02568-2020
18. Sikkema RS, Pas SD, Nieuwenhuijse DF, et al. COVID-19 in health-care workers in three hospitals in the south of the Netherlands: a cross-sectional study. Lancet Infect Dis. 2020;20(11):1273–1280. doi:10.1016/S1473-3099(20)30527-2
19. Ortega R, Gonzalez M, Nozari A, Canelli R, Ingelfinger JR. Personal protective equipment and Covid-19. Ingelfinger JR, ed. N Engl J Med. 2020;382(26):e105. doi:10.1056/NEJMvcm2014809
20. Kang SJ, Jung SI. Age related morbidity and mortality among patients with COVID-19. Infect Chemother. 2020;52(2):154–164. doi:10.3947/ic.2020.52.2.154
21. Wang J, Zhou M, Liu F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect. 2020;105(1):100–101. doi:10.1016/j.jhin.2020.03.002
22. Bhagavathula AS, Aldhaleei WA, Rahmani J, Mahabadi MA, Bandari DK. Knowledge and perceptions of COVID-19 among health care workers: Cross-Sectional Study. JMIR Public Health Surveill. 2020;6(2):e19160. doi:10.2196/19160
23. Saqlain M, Munir MM, Rehman SU, et al. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: a cross-sectional survey from Pakistan. J Hosp Infect. 2020;105(3):419–423. doi:10.1016/j.jhin.2020.05.007
24. Basheti IA, Nassar R, Barakat M, et al. Pharmacists’ readiness to deal with the coronavirus pandemic: assessing awareness and perception of roles. Res Soc Adm Pharm. 2020. doi:10.1016/j.sapharm.2020.04.020
25. Dawoud D. Emerging from the other end: key measures for a successful COVID-19 lockdown exit strategy and the potential contribution of pharmacists. Res Soc Adm Pharm. 2020. doi:10.1016/j.sapharm.2020.05.011
26. Kara E, Demirkan K, Ünal S. Knowledge and attitudes among hospital pharmacists about COVID-19. Turkish J Pharm Sci. 2020;17(3):242–248. doi:10.4274/tjps.galenos.2020.72325
27. Lombardi DA, Verma SK, Brennan MJ, Perry MJ. Factors influencing worker use of personal protective eyewear. Accid Anal Prev. 2009;41(4):755–762. doi:10.1016/j.aap.2009.03.017
28. Khan MR 20,000 fake N95 masks supplied to 10 hospitals. The daily star. 20AD. Available from: https://www.thedailystar.net/frontpage/news/20000-fake-n95-masks-supplied-10-hospitals-1969713.
29. Andaleeb SS. Public and private hospitals in Bangladesh: service quality and predictors of hospital choice. Health Policy Plan. 2000;15(1):95–102. doi:10.1093/heapol/15.1.95
30. Muhammad K, Saqlain M, Hamdard A, et al. Knowledge, attitude, and practices of community pharmacists about COVID-19: a cross-sectional survey in two provinces of Pakistan. medRxiv. 2020;May:
31. Naser AY, Dahmash EZ, Alswafi H, et al. Knowledge and practices towards COVID-19 during its outbreak: a multinational cross-sectional study. medRxiv. 2020. doi:10.1101/2020.04.13.20063560
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.