Back to Journals » Infection and Drug Resistance » Volume 13
Healthcare Workers’ Preparedness: An Exploratory Study for Measles Control in a Middle-Income Country
Authors El-Sokkary RH ![]() , Tash RME
, Tash RME ![]() , Zalat MM
, Zalat MM ![]() , Arafa M, Malek MM
, Arafa M, Malek MM ![]()
Received 11 October 2019
Accepted for publication 6 January 2020
Published 10 February 2020 Volume 2020:13 Pages 395—402
DOI https://doi.org/10.2147/IDR.S234378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Rehab H El-Sokkary, 1 Rehab M ElSaid Tash, 1 Marwa M Zalat, 2 Mohamed Arafa, 3 Mai M Malek 1
1Medical Microbiology & Immunology Department, Faculty of Medicine, Zagazig University, Zagazig, Egypt; 2Department of Community, Occupational and Environmental Medicine, Zagazig University, Zagazig, Egypt; 3Pediatrics Department, Faculty of Medicine, Zagazig University, Zagazig, Egypt
Correspondence: Rehab H El-Sokkary Email [email protected]
Background: Healthcare workers (HCWs) should have an active role in measles control.
Objective: This study aimed to assess the HCWs’ measles immune status and its influencing factors; to measure their knowledge, attitude, and practice toward measles infection/vaccination; and to identify factors predicting their vaccination status.
Methods: Data were collected using a semi-tailored questionnaire. Immunoglobulin G against measles was measured. Regression analysis for measles vaccination was performed.
Results: Approximately 97 HCWs (93.3%) were seropositive, 79 (76.0%) were vaccinated, 18 (17.3%) were previously infected, and 9 (8.7%) were both vaccinated and previously infected. One previously vaccinated participant was seronegative. The immune status was associated with marital status, residence, work duration, infection control training, and wearing personal protective equipment. Positive attitudes and practices were reported. Marital status and infection control training were predictors for measles vaccination.
Conclusion: HCWs showed readiness to control the spread of measles. National policies for compulsory HCWs’ vaccination and immune status check before training and employment are required.
Keywords: measles, healthcare workers, vaccination, middle-income countries, infection control
Introduction
Healthcare workers (HCWs), by occupational exposure, have a higher risk of both acquiring and spreading serious vaccine-preventable diseases to vulnerable patients and colleagues. The World Health Organization (WHO) estimates that approximately 59 million HCWs worldwide are potentially exposed to hazardous biological agents every day.1 When a disease can be transmitted through humans, as in the case of measles, vaccination is considered as the most important primary prevention strategy, with extended effect to HCWs’ colleagues and patients.1 Measles is a highly infectious disease that can transmit measles virus to 75–90% of susceptible contacts2 with a reported higher risk among nonimmune HCWs compared to that of the general population.3 Recently, outbreak events were reported, in Egypt and worldwide, characterized by the nosocomial transmission of measles with subsequent infection of HCWs.4,5
World Health Organization (WHO) defined measles elimination as the absence of endemic measles transmission in a defined geographical area for at least 12 months. Meanwhile, eradication is defined as the worldwide interruption of measles virus transmission in the presence of a surveillance system that has been verified to be performing well.6 In 2015, Egypt endorsed the 2016–2020 Eastern Mediterranean Vaccine Action Plan as a framework for the implementation of the Global Vaccine Action Plan in countries of the region. It included immediate measles elimination and interruption of endemic measles virus transmission, latest by 2020.6 Measures for measles containment action plan in hospital settings include early and accurate case diagnosis, prevention of infection transmission, and protection of HCWs and other hospital staff.7
Being the only reliable protection against the nosocomial spread of measles, especially for susceptible HCW, vaccination against measles is strongly recommended by international and national health authorities.4 Live attenuated measles vaccines, either monovalent vaccine or measles-containing vaccine in combination such as combined measles–rubella vaccine, measles–mumps–rubella (MMR) vaccine, or measles–mumps–rubella–varicella vaccine, induce lifelong immunity.8 At least 98% of those receiving two doses of MMR vaccine are protected against the disease.9 Vaccine-induced antibody concentrations decrease over time and may become undetectable. However, immunological memory persists and, following exposure to measles virus, most vaccinated people produce a protective immune response.8
Globally, measles immunization coverage has improved steadily since 1990, to reach 83% in 2008. The lowest rates were in the WHO South-East Asia (75%) and African (73%) regions10 Low measles vaccination coverage was reported in several studies.8,9 The World Health Organization (WHO) recommends a threshold of 95% immunization coverage to achieve so-called “herd immunity.” However, by the end of 2018, the global coverage of the first dose of the measles vaccine was reported at 86%, the second dose is much lower, at 67%. In the past 8 years, over 20 million children worldwide missed out on measles vaccine annually, creating a pathway to current global outbreaks especially in n low- and middle-income countries.11
Healthcare workers are often referred to be the most confided source of immunization-related data for their patients and associates. They are considered in the best position to understand hesitant patients and to find ways of explaining the benefits of vaccination. However, in some instances, healthcare workers themselves can be vaccine-hesitant, they even do not recommend the vaccine for their patients. Hence, HCWs should not only be vaccinated with a documented evidence of measles immunity, but they should also be encouraged to have an active role in measles control.12
Although the Expanded Program of Immunization (EPI) in Egypt has achieved several successes in controlling vaccine-preventable diseases with coverage of over 90%, challenges still exist with measles outbreaks occurring in 2013 and 2014, and the increasing need for continuous surveillance.13 This study aimed to assess the HCWs’ measles immune status and its influencing factors; to measure their knowledge, attitude, and practice toward measles infection, potential exposure, and vaccination; and to identify factors predicting the vaccination status of the HCWs.
Materials and Methods
Study Design and Settings
A cross-sectional study was conducted from October 10, 2018, to March 10, 2019, at the Pediatric Department of Zagazig University Hospital, Zagazig City, Egypt. Participants’ workup was performed at Medical Microbiology and Immunology Laboratories, Faculty of Medicine, Zagazig University.
Study Population and Sampling Technique
The HCWs of the Pediatric Department of Zagazig University Hospital were invited to participate in this study. The sample size was calculated to be 137 HCWs. Calculations have been performed using the sample size software online (available at http://sampsize.sourceforge.net/iface/#prev) for prevalence studies.14 The total number of HCWs at the Pediatric Department was 260, assuming a seroprevalence of immunoglobulin G (IgG) against measles of 75%15 at a confidence interval of 95% and power of test of 80%. Sample selection was performed using a simple random sampling technique.
Announcement and invitation for participation in the study were sent via email and delivered at the workplace for all HCWs working at the Pediatric Department of Zagazig University Hospital. This was followed by another two reminders to increase the participants’ response rate.
Data Collection Tools
The data were collected by the researchers using a semi-tailored questionnaire adapted from previous similar studies.1,16,17
The questionnaire was translated into Arabic by a bilingual coinvestigator and back-translated by another bilingual expert to ensure validity. Before the start of the study, the questionnaire has been tested on 10 HCWs to determine if there were any ambiguity or items leading to misunderstanding in the questionnaire to reach its final form. The necessary corrections, modifications, and rewording after considering any minor differences and discrepancies have been performed to ensure clarity of all questions and ease of understanding. The reliability coefficient test (Cronbach’s alpha) was >0.72 for all questions.
The questionnaire consisted of three parts:
First Part
Questions on sociodemographic and occupational information of the participants such as age, gender, marital status, having children, residence (eg, urban or rural), occupation (medical and paramedical personnel), and current job duration.
Second Part
Questions on the history of measles exposure, past infection, and vaccination.
Third Part
Questions on knowledge, attitude, and practice of participants toward measles infection and immunization.
Procedures
Immunological Investigations
To assess the immune status of the study participants against measles, IgG against measles was measured using Enzygnost® Anti-Measles Virus/IgG (Siemens Healthcare Diagnostics Products, Germany). A 2-mL blood was collected under complete aseptic conditions. All steps were performed according to the enzyme-linked immunosorbent assay kit protocol. Photometric evaluation of the samples was performed using a measuring wavelength of 450 nm with Enzygnost® Anti-Measles Virus/IgG. Samples containing approximately 150 mIU/mL were found to be within the range of 0.100 to 0.200 ΔA. Anti–Measles Virus/IgG negative ΔA < 0:100 (cutoff value). Anti–MeaslesVirus/IgGpositive ΔA > 0:200. HCWs with negative measles IgG were informed about the results and were offered immunization with either a measles vaccine or MMR vaccine according to the availability of the vaccine and the HCWs’ sex (MMR vaccines were used for women).
Data Management
Data were coded, entered, and analyzed using the Statistical Package for the Social Sciences (SPSS) version 21.0 (SPSS, Chicago, IL, USA). Quantitative data were represented as a mean and standard deviation (SD), and qualitative data were represented as frequencies and percentages. The independent Student’s t-test was used to determine the significance of differences between the two continuous variables, and the chi-squared test was used to assess for differences in the categorical variables. Logistic regression analysis was performed to determine the factors predicting the measles vaccination of the participants. The test results were considered significant when p-value <0.05.
Ethical Considerations
This study was approved by the Zagazig University’s Institutional Review Board No: 5518-9-9-2019. Participation was voluntary, and written informed consent was obtained from all the participants after describing the aim of the study. Privacy and confidentiality were assured.
Results
Out of the 137 selected HCWs, 104 participated in the study with a response rate of 75.9%. The age of the participants ranged from 19 to 52 years old with a mean ± SD of 33.8±10.79. More than three-quarters of HCWs were female (82.7%), married (76.9%), had children (73.1%), and lived in urban areas (76.9%). Regarding the occupational data, more than half of HCWs (56.7%) were nurses, 35.6% were physicians, and the rest of them (7.7%) were paramedical personnel (technician/nonmedical staff). Most of the HCWs were working for more than 10 years (79.8%) and only 20.2% for less than 10 years.
Regarding the history of measles exposure, infection, and vaccination of the participants, approximately 26% of HCWs had a history of measles infection, 76.9% were vaccinated, 93.8% were vaccinated for >10 years, and all of their children had received measles vaccine. Only 5.8% had clinically managed a measles patient recently, and 11.5% had increased temperature or reported skin rash over the past week.
Out of the total 104 HCWs, 97 (93.3%) were seropositive and 7 (6.7%) were seronegative for measles. The seropositive HCWs were distributed either as vaccinated only (79/76.0%), previously infected only (18/17.3%), or both vaccinated and previously infected (9/8.7%). Among the previously vaccinated (n=80) HCWs, there was one participant who showed a seronegative status for measles (Figure 1).
 |
Figure 1 Seroprevalence of IgG against measles among HCWs. |
Table 1 demonstrates a statistically significant difference between seropositive and seronegative HCWs in the following factors: marital status, residence, work duration, previous infection control training courses, and wearing personal protective equipment (PPE), specifically mask N95, while dealing with measles patients.
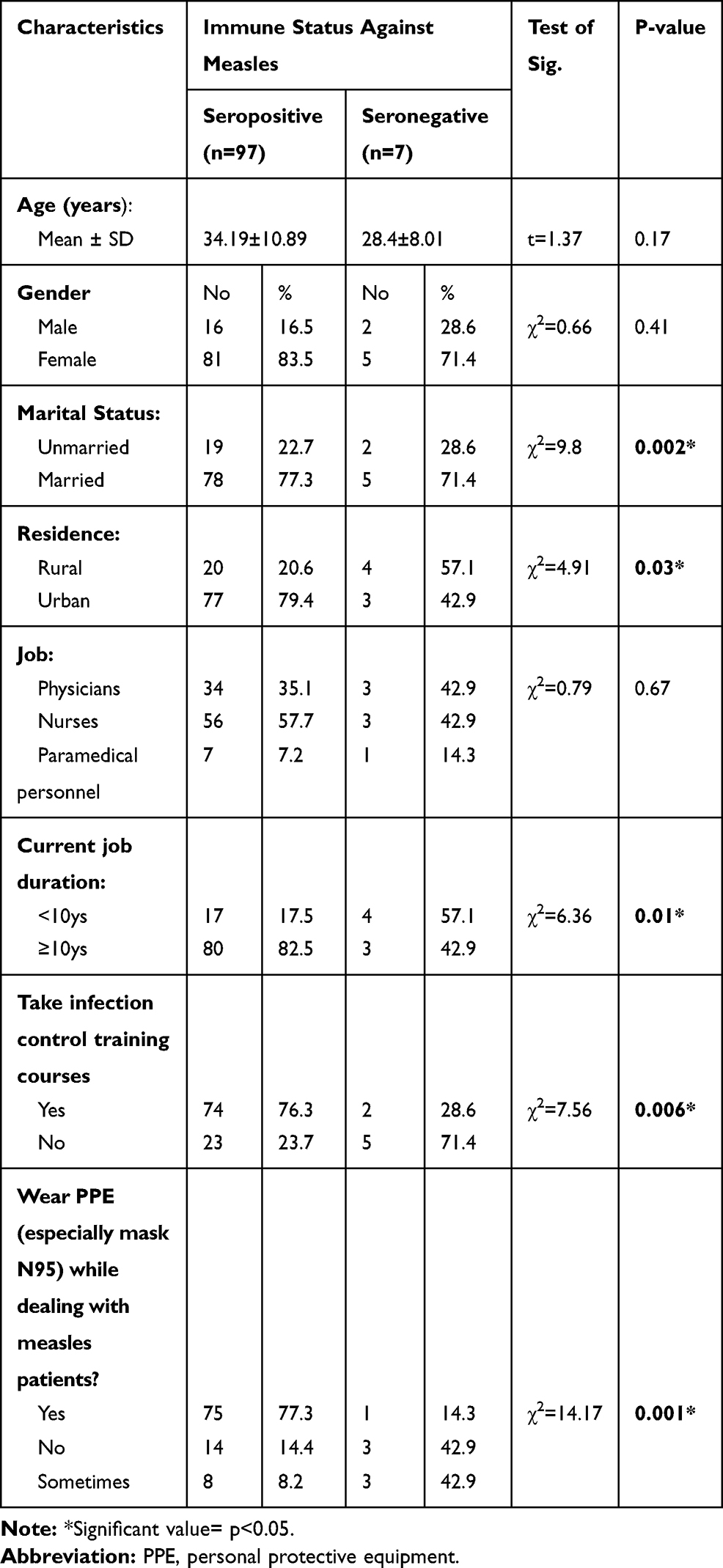 |
Table 1 Factors Affecting the Immune Status of the Study Participants Against Measles |
Participants were asked about measles infection, transmission, and vaccination (Table 2). A significant variation was observed among HCWs about the mode of transmission. Although all of them were aware that measles is a contagious disease, the virus can spread from children to HCWs, can cause complications, and can be prevented by administering the vaccine, only 7.7% of HCWs were aware that measles virus could not be transmitted by food. Regarding the infectivity period, 69.2% of them thought the measles patient to be a source of infection of the offenders before the onset of rash, and 15.4% of HCWs considered the measles patient as not a source of infection for the offenders only after the emergence of skin rash.
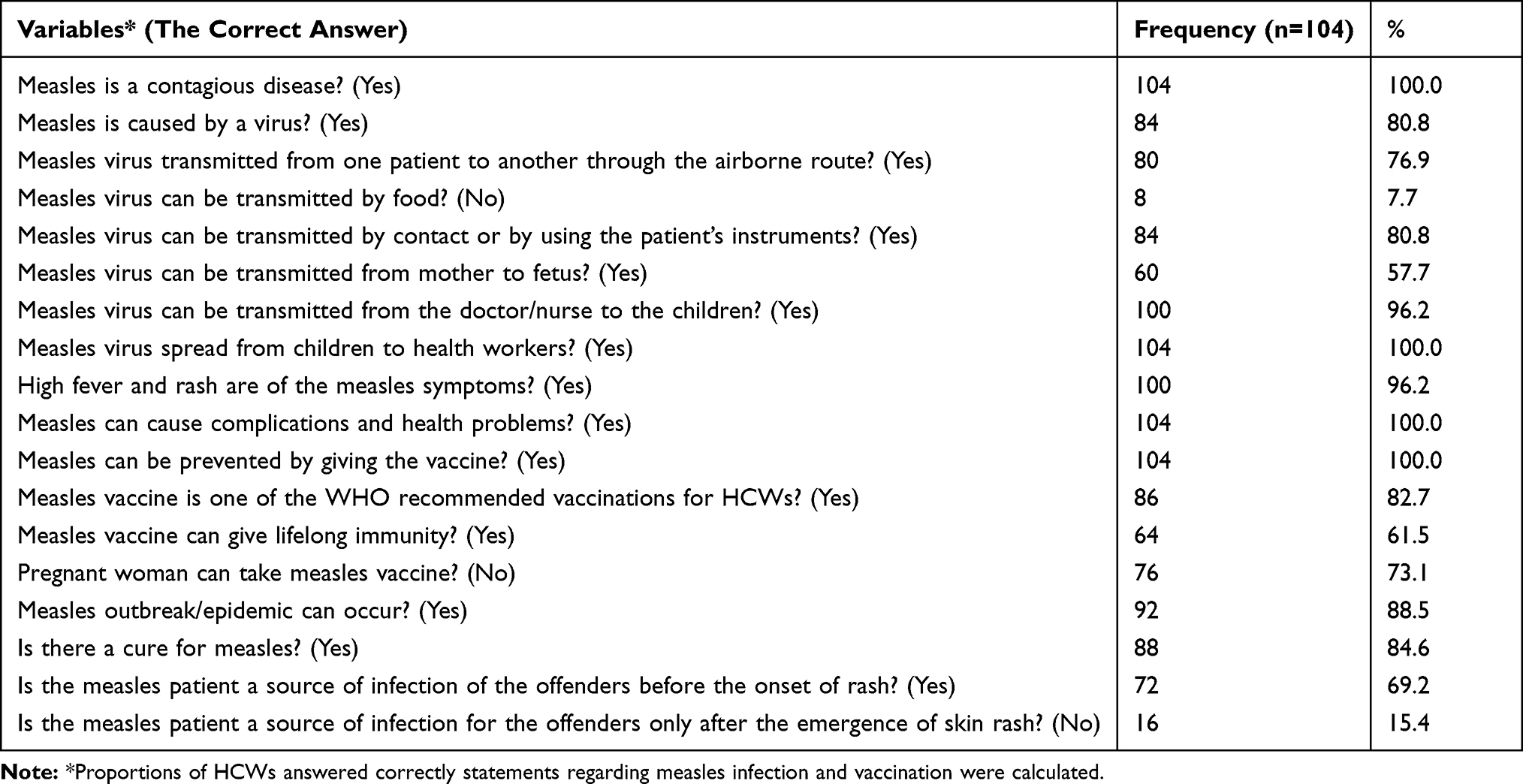 |
Table 2 Knowledge of HCWs Regarding Measles Infection and Vaccination |
Table 3 describes the participants’ attitude and practice toward measles infection and vaccination. A high percentage of positive attitudes and practices was reported such as the following: advising the mothers of children to take the measles vaccine and take a complementary dose; believing that measles vaccine should be compulsory for the HCWs; believing that measles vaccine has to be taken even if infection control measures are followed; wearing PPE, specifically mask N95, while dealing with patients; taking infection control training course in hospitals for measles prevention; and readiness in taking training course for those who were not trained (92.3%, 86.5%, 81.7%, 73.1%, 73.1%, and 71.4%, respectively). More than two-thirds of the participants (67.3%) agreed that it is important to check their immune status against measles and (60.6%) to isolate measles patient in a single room in the hospital.
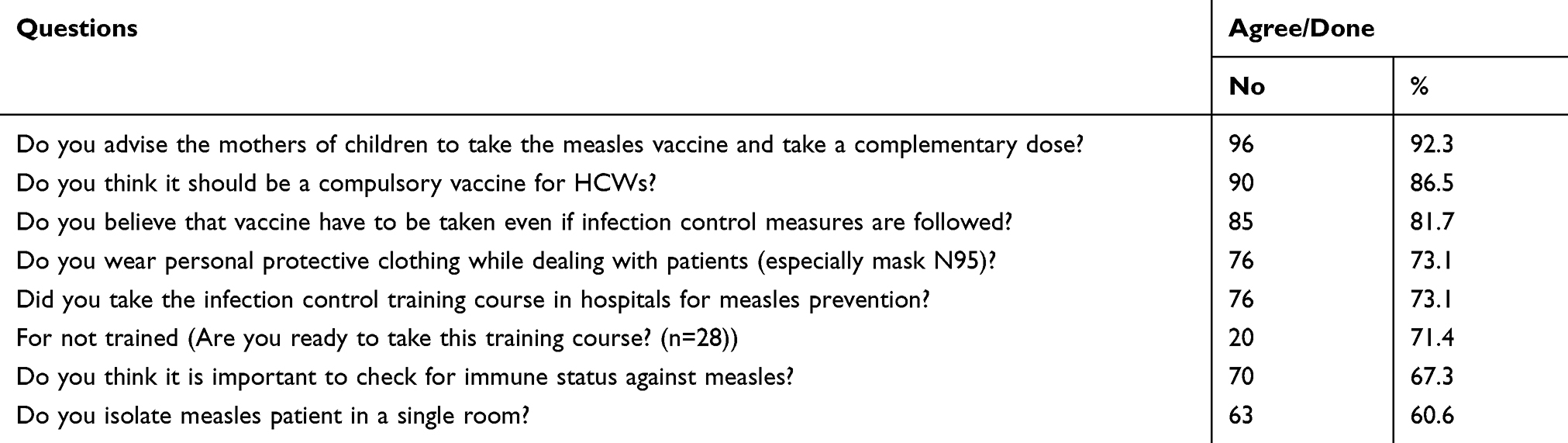 |
Table 3 Attitude and Practice of HCWs Regarding Measles Infection and Vaccination (N=104) |
Table 4 shows that marital status and taking infection control training courses are statistically significant predicting factors influencing the measles vaccination status among the investigated HCWs (p<0.05).
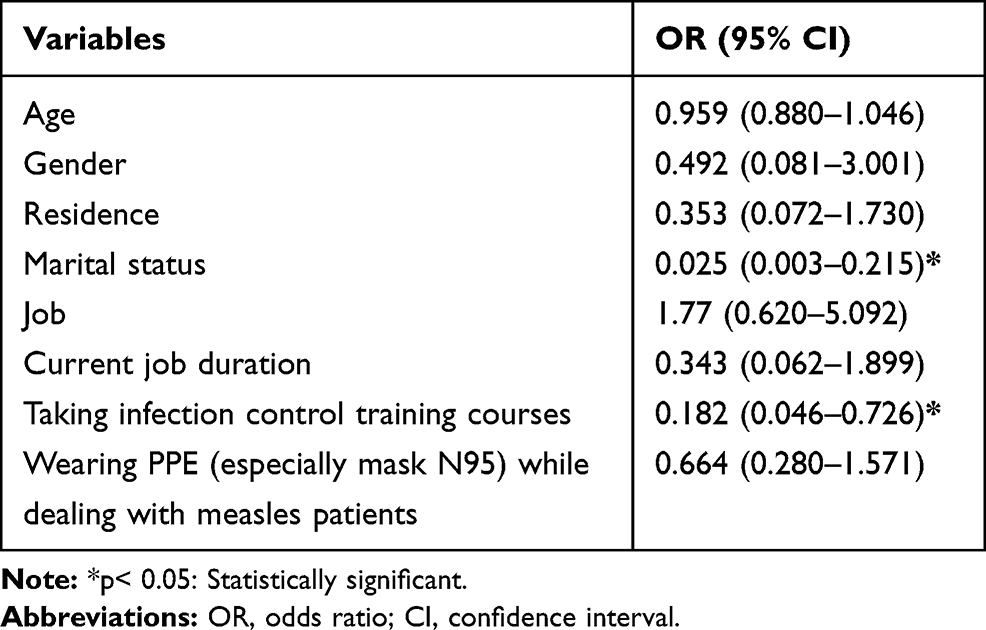 |
Table 4 Regression Analysis for Predicting Factors Affecting Measles Vaccination Among the Investigated HCWs |
Discussion
Measles vaccination of healthcare workers is an efficient mean of prevention of nosocomial measles outbreaks and could contribute to eliminate measles in the general population. Adults over 20 years old have a higher risk of severe or fatal measles than adults less than 20 years old.18 HCWs’ vaccination recommendations work better if they are focused on specific HCWs’ groups and appropriate diseases such as measles.19 As measles is a common childhood illness, the current study targeted HCWs at the pediatric hospital, the place where measles-infected children visit very frequently.
The measles vaccine is fundamental for susceptible HCWs as in recent years the epidemiology of these diseases has changed, involving a significant number of adults and elderly individuals instead of children.20 Little attention is paid by HCWs to the importance of receiving vaccination against measles. This was evident in a previous Egyptian study (32.8%).17 In a previous report, about 61.6% of Italian HCWs do not believe that the measles vaccine should be mandatory to HCWs. Fortunately, this study showed a significantly higher vaccination rate (76.9%). This might be attributed to the target group in the current study who works at the pediatric hospital with more readiness to protect themself from measles infection; a prevalent disease among children.
Susceptible HCWs who work in patient care are at high risk of becoming a source for disease transmission among patients.18 In the present study, testing seroprevalence IgG against measles among HCWs revealed that 6.7% were seronegative and hence were susceptible to measles infection. Measles vaccine unresponsiveness could be explained by host or vaccine-related factors. Actually, 2–10% of individuals fail to raise antibody levels to routine vaccines. Immune and health status as well as genetic factors are important key players. Vaccine-related ones include inadequate attenuation, wrong route or interrupted schedule and interruption of cold chain.21–24 In Egypt, measles vaccine was introduced as a compulsory vaccine to children at the age of 9 months, in which the vaccine might interfere with maternal Abs. In response, this time has been changed later to be at 12 months.22–24 In the current study, only one participant showed a seronegative response, despite being vaccinated. When interviewed, he stated that he only received one dose of the vaccine and forgot the second one.
Disseminating data about the current vaccine non-responsiveness status supports the importance of complying with the recent Centers for Disease Control and Prevention recommendation; the use of N95 or equivalent respirator for suspected measles cases regardless of the immunity status. This is because, in several instances, HCWs may be unaware of their immune status. Thus, they expose themselves to significant risk, and they mostly have a false sense of security when they deal with a suspected case.25
Comparing the characteristics of nonimmune HCWs with that of immune ones, the results showed that most of them, excluding medical doctors, are nonimmune. The junior ones and those who did not take measles prevention and control course showed the highest percentages of nonimmunity. This could be significantly helpful for hospital managers to select the target groups for any proposed vaccination campaigns. It emphasizes the importance of a preemployment and training assessment of immune status against measles. In 2019, the World Health Organization (WHO) reports confirmed that proof/documentation of HCWs’ immunity or immunization to measles should be required as a pretraining and employment requirement.26
Good knowledge is associated with a positive attitude, which was evident in the present study. Participants’ knowledge about the routes of transmission is still insufficient, which was reflected in the improper practice and attitude toward patient isolation and protective clothing. All of the HCWs are well aware of the significance and effects of measles and the possible risk of acquiring the infection from their patients and vice versa. A finding was confirmed regarding their willingness to take training courses about prevention (61.0% are already trained, and the majority of the untrained HCWs are ready to take training courses). However, HCWs have insufficient knowledge regarding the infectivity period (15.4% only knows the right answer); hence, this should be taken into consideration in future training and educational session.
All participants are aware that the vaccine prevents measles; however, 82.7% know that it is recommended by the WHO for HCWs, and 61.5% only knows that it gives lifelong immunity. Approximately 86.5% have a positive attitude toward a compulsory vaccine for HCWs. Similar results were reported from other studies.1,17,27 A previous study reported low immunization coverage among HCWs and attributed this finding to personal decisions and not immunization strategies.19 Vaccine hesitancy to measles vaccine could be related to false beliefs about the vaccine; some accused it of causing autism, measles and even death. An important other factor is the lack of knowledge and awareness of vaccine role in preventing measles outbreaks. Previous vaccination side effect (bad experience) is also considered another contributor to vaccine hesitancy. Most successful interventions are based on education and improving knowledge about vaccine safety, effectiveness, or the need for vaccines.28–30 Logistic regression analysis demonstrated that marital status and taking infection control training courses are statistically significant predicting factors influencing the measles vaccination status among the investigated HCWs.
Indeed, changing the vaccine safety message directed to HCWs to highlight the benefits they will gain from being vaccinated is urgently required to ensure a better vaccination rate in the near future. Although vaccination without screening is cost-effective, the costs should not be solely calculated upon the direct costs of vaccination procedure (vaccine price and administration cost). There are other aspects regarding the indirect costs of vaccination associated with lost work time and potential side effects of the vaccine and their consequent costs (medical care costs including healthcare provider visits, investigations and treatment).31–33 This could be helpful for the healthcare authorities to promote another appropriate message for the selected target groups, so they could achieve a better coverage for vaccination campaigns.
Conclusion
Good vaccination rate, good knowledge level, and positive attitude and practice are evident among HCWs with readiness to control measles spread in their hospital. However, collaborative efforts should be exerted to fill in the insufficient knowledge reflected on negative attitudes toward vaccine and control measures. A new articulated vaccine safety message should be directed to HCWs. National policies should be formulated to support the compulsory vaccination and immune status check before HCWs’ training and employment in healthcare facilities. Different HCWs’ groups should be targeted by future studies on a wider scale.
Acknowledgment
The authors dedicate their sincere appreciation to the participating HCWs for their cooperation and help in facilitating data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. La Torre G, Scalingi S, Garruto V, Siclari M, Chiarini M, Mannocci A. Knowledge, attitude and behaviours towards recommended vaccinations among healthcare workers. Healthcare. 2017;5:3. doi:10.3390/healthcare5010013
2. Freund R, Krivine A, Pre’vost V, et al. measles immunity and measles vaccine acceptance among healthcare workers in Paris, France. J Hosp Infect. 2013;84:38–43. doi:10.1016/j.jhin.2013.01.002
3. Barbadoro P, Marigliano A, Di Tondo E, et al. Measles among healthcare workers in a teaching hospital in Central Italy. J Occup Health. 2012;54:336–339. doi:10.1539/joh.12-0016-BR
4. Jia H, Ma C, Lu M, et al. Transmission of measles among healthcare workers in Hospital W, Xinjiang autonomous region in China 2016. BMC Infect Dis. 2018;18:36–42. doi:10.1186/s12879-018-2950-y
5. Kandil A, Gewaifel G, Abdelhai R, Ramadan A, Teleb N. A national survey to evaluate Measles-Rubella National Vaccination Campaign Coverage in Egypt . J High Inst Public Health. 2019;49(1):19–29. doi:10.21608/jhiph.2019.29462
6. World Health Organization 2015. Eastern Mediterranean Vaccine Action Plan (EMVAP) 2016–2020 A framework for implementation of Global Vaccine Action Plan (GVAP). WHO; 2015. Available from: http://www.emro.who.int/vpi/vpi-infocus/eastern-mediterranean-vaccine-action-plan.html. Accessed December 17, 2019.
7. Shakoor S, Mir F, Zaidi A, Zafar A. Hospital preparedness in community measles outbreaks: challenges and recommendations for low-resource settings. Emerging Health Threats J. 2015;8:24173. doi:10.3402/ehtj.v8.24173
8. WHO 2009. Measles vaccines: WHO position paper. Weekly Epidemiol Rec. 2009;84(35):349–360.
9. Komitova R, Kunchev A, Mihneva Z, Marinova L. Nosocomial transmission of measles among healthcare workers, Bulgaria, 2010. Euro Surveill. 2011;16(15):
10. World Health Organization-United Nations International Children’s Emergency Fund (WHO/UNICEF) estimate of national immunization coverage. Global Health Observatory (GHO). Measles immunization coverage Geneva; 2009. Available from: https://www.who.int/gho/mdg/child_mortality/situation_trends_measles_immunization/en/.
11. World Health O. Measles vaccines: WHO position paper, April 2017 - recommendations. Vaccine. 2017;37:219–222.
12. Filia A, Tavilla A, Bella A, et al. Measles in Italy, July 2009 to September 2010. Euro Surveill. 2011;16:pii19925.
13. World Health Organization. Regional office for the Eastern Mediterranean. Egypt. Expanded Programme on Immunization. WHO. 2016. Available at http://www.emro.who.int/egy/programmes/expanded-programme-on-immunization.html. Accessed December 15, 2019.
14. Sampsize. Sample size for a prevalence survey, with finite population correction. Available from: http://sampsize.sourceforge.net/iface/#prev.
15. Bakri FG, Abdelrahim ZM, Alkalbani AS, Khrais GM, Shamroukh DS, Ayajneh MA. Seroprevalence of measles, mumps, rubella, and varicella among physicians and nurses in Jordan. Turkish J Med Sci. 2016;46:614–619. doi:10.3906/sag-1502-115
16. Loulergue P, Moulin F, Vidal-Trecan G, et al. Knowledge, attitudes and vaccination coverage of healthcare workers regarding occupational vaccinations. Vaccine. 2009;27(31):4240–4243. doi:10.1016/j.vaccine.2009.03.039.
17. Hakim S, Mokhtar A. Compliance with vaccination as an occupational safety measure among healthcare workers at Ain shams university hospitals, Cairo, Egypt. Egypt J Occup Med. 2017;41(3):343–355. doi:10.21608/ejom.2017.3925
18. WHO. High-Quality Supplementary Immunization Activities for Injectable Vaccines. Using an Example of Measles and Rubella Vaccines: field guide; 2016. Available from: http://www.who.int/about/licensing/copyright_form/index.html.
19. Amendola A, Bianchi S, Lai A, et al. Measles re-emergence in Northern Italy: pathways of measles virus genotype D8 20132014. Infect Genet Evol. 2017;48:120–126. doi:10.1016/j.meegid.2016.12.013
20. Maltezou HC, Katerelos P, Poufta S, Pavli A, Maragos A, Theodoridou M. Attitudes toward mandatory occupational vaccinations and vaccination coverage against vaccine-preventable diseases of health care workers in primary health care centers. Am J Infect Control. 2013;41:66–70. doi:10.1016/j.ajic.2012.01.028
21. Allam MF. Measles vaccine. J Prev Med Hyg. 2009;50:201–205.
22. Wiedermann U, Garner-Spitzer E, Wagner A. Primary vaccine failure to routine vaccines: why and what to do? Hum Vaccin Immunother. 2016;12(1):239–243. doi:10.1080/21645515.2015.1093263. PMID: 26836329; PMCID: PMC4962729.
23. Urbiztondo L, Borràs E, Costa J, et al.; Working Group for the Study of the Immune Status in Healthcare Workers in Catalonia. Prevalence of measles antibodies among health care workers in Catalonia (Spain) in the elimination era. BMC Infect Dis. 2013;13:391. PMID: 23978316; PMCID: PMC3765384. doi:10.1186/1471-2334-13-391
24. Hahné MS, Nic Lochlainn LM, van Burgel ND, et al. Measles outbreak among previously immunized healthcare workers, the Netherlands, 2014. J Infect Dis. 2016;214(12):1980–1986. doi:10.1093/infdis/jiw480
25. Gohil SK, Okubo S, Klish S, Dickey L, Huang S, Zahn M. Healthcare workers and post-elimination era measles: lessons on acquisition and exposure prevention. Clin Infect Dis. 2016;62(2):166–172. doi:10.1093/cid/civ802
26. Who. Immunization of healthcare workers; 2019. Available from: https://www.who.int/immunization/policy/immunization_tables/en/.
27. Calabrese G, MS G, Tafuri S. Knowledge, attitudes, and practices of occupational health physicians in the promotion of vaccinations recommended for health care workers: an Italian study. Lett Editor/Am J Infect Control. 2016;44(2016):1755–1763.
28. Sabahelzain MM, Moukhyer M, Dubé E, Hardan A, van den Borne B, Bosma H. Towards a further understanding of measles vaccine hesitancy in Khartoum state, Sudan: a qualitative study. PLoS One. 2019;14(6):e0213882. doi:10.1371/journal.pone.0213882
29. Taylor LE, Swerdfeger AL, Eslick GD. Vaccines are not associated with autism: an evidence-based meta-analysis of case-control and cohort studies. Vaccine. 2014;32(29):3623–3629. doi:10.1016/j.vaccine.2014.04.085
30. Karafillakis E, Dinca I, Apfel F, et al. Vaccine hesitancy among healthcare workers in Europe: a qualitative study. Vaccine. 2016;34(41):5013–5020. doi:10.1016/j.vaccine.2016.08.029
31. Alp E, Cevahir F, Gokahmetoglu S, Demiraslan H, Doganay M. Prevaccination screening of health-care workers for immunity to measles, rubella, mumps, and varicella in a developing country: what do we save? J Infect Public Health. 2012;5(2):127–132. doi:10.1016/j.jiph.2011.11.003
32. Russi M, Buchta WG, Swift M, et al. Guidance for occupational health services in medical centers. J Occup Environ Med. 2009;51:1e–18. doi:10.1097/JOM.0b013e3181bb0d7c
33. Maltezou HC, Wicker S. Measles in health-care settings. Am J Infect Control. 2013;41(7):661–663. doi:10.1016/j.ajic.2012.09.017
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.