Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Healthcare Utilization and Cost in the Two Years Before Neuromodulation Implantation Among Medicaid Enrollees with Drug-Resistant Epilepsy
Authors Evans K, Li Q, Zhang L ![]() , Lam S
, Lam S ![]() , Do Rego B, Danielson V, Lassagne R, Berger A
, Do Rego B, Danielson V, Lassagne R, Berger A
Received 3 July 2025
Accepted for publication 14 August 2025
Published 28 August 2025 Volume 2025:17 Pages 571—583
DOI https://doi.org/10.2147/CEOR.S551202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Kathryn Evans,1 Qian Li,1 Lu Zhang,2 Sandi Lam,2 Bronwyn Do Rego,3 Vanessa Danielson,3 Reginald Lassagne,3 Ariel Berger1
1Thermo Fisher Scientific, Waltham, MA, USA; 2Department of Neurosurgery, Division of Pediatric Neurosurgery, Ann and Robert H. Lurie Children’s Hospital of Chicago, Northwestern University Feinberg School of Medicine, Chicago, IL, USA; 3LivaNova, London, UK
Correspondence: Ariel Berger, Email [email protected]
Background: Current treatment guidelines recommend consideration of neurostimulators and other alternative treatments to antiseizure medications in patients with drug-resistant epilepsy (DRE). This study assessed patterns of utilization and cost of healthcare services and prescription pharmacotherapies during the 2-year period before neurostimulator implantation among Medicaid enrollees with DRE.
Methods: This retrospective, observational cohort study used healthcare claims and enrollment data obtained from the US Centers for Medicare and Medicaid Services. Medicaid enrollees who met study selection criteria (ie, evidence of DRE and neurostimulator implantation) between January 1, 2011, and December 31, 2020, were included. Those without antiseizure medication (ASM) dispenses within 12 months of their implantation date or continuous enrollment for the 24-month period before this date were excluded. Demographic/clinical characteristics, utilization and cost of healthcare services, and prescription pharmacotherapies were assessed over the 2-year period before implantation. Care was designated as all-cause or epilepsy-related; the latter was defined as all ASM dispenses and all claims for medical care (ie, inpatient or outpatient) with a diagnosis code (any position) of epilepsy.
Results: In total, 2469 patients met the selection criteria. Mean age at implantation was 20.8 years. Comorbidities were common. Over the 2-year period before implantation, patients were prescribed a mean of 4.4 unique ASMs. Fifty-seven percent had at least one all-cause hospital admission, and 82.9% had at least one all-cause emergency department visit; corresponding epilepsy-related values were 55.3% and 66.1%. Less than half of patients received specific cranial imaging, including video electroencephalographs. Total mean all-cause healthcare costs were $117,013; epilepsy-related healthcare costs accounted for $48,169 (41.2%).
Conclusion: Medicaid enrollees with DRE experience high use and cost of healthcare services and pharmacotherapy over the 2 years before neurostimulator implantation. Further research is needed to understand the impacts associated with broader access to specialized epilepsy care, such as cranial imaging and neurostimulators.
Keywords: drug-resistant epilepsy, neuromodulation, medicaid, antiseizure medications, neurostimulator implantation, healthcare costs
Introduction
Around 40% of patients with epilepsy do not achieve adequate seizure control from antiseizure medications (ASMs).1–4 Patients who fail to achieve sustained seizure freedom with at least two different ASMs (either monotherapies or in combination) are considered to have drug-resistant epilepsy (DRE).5 Patients with DRE experience greater levels of comorbidities as well as higher utilization and cost of healthcare services than patients with epilepsy who respond to ASMs. Further, those with DRE also experience social stigmatization and greater dependence on family and caregivers, some having reported feeling a sense of “loss of control”.5
There is a low likelihood of response to subsequent ASMs following transition to DRE. In one relatively large (N=459) study, between 5.4% and 0.5% of patients attain seizure freedom with the third and sixth ASM regimens, respectively, versus 67.1% and 39.1% of those receiving their first and second such regimens, respectively.6 Accordingly, alternative nonpharmacological treatments exist and should be considered in patients with DRE. These include resective surgeries such as corpus callosotomy, hemispherectomy, temporal lobectomy, and laser ablation as well as nonresective surgeries such as neurostimulator implantation. The approach to treatment of a patient with DRE is by necessity individualized and should be informed by patient history, personal circumstance, treatment preference, and other factors.
With respect to nonresective approaches, three neurostimulator devices have been approved by the United States (US) Food and Drug Administration (FDA) for the treatment of epilepsy refractory to ASMs: vagus nerve simulation (VNS), which involves implantation of stimulating electrodes around the left vagus nerve in the carotid sheath and the placement of a pulse generator in the left anterior chest wall; responsive nerve stimulation (RNS), a closed-loop system in which electrodes are placed intracranially in the skull at the seizure foci and the pulse generator placed under the scalp; and deep brain stimulation (DBS), which is another closed-loop system in which electrodes are placed into the anterior nucleus of the thalamus, and the pulse generator is placed in the pectoral muscle.7–9 While all three devices are FDA-approved for patients aged ≥18 years, only VNS is currently approved for patients aged ≥4 years.10–12 All three devices have demonstrated efficacy and safety for the treatment of DRE in both clinical trial and real-world settings.13–16
Despite this, less than 1% of patients with DRE complete presurgical evaluations, and even fewer undergo surgery.17 For those who do, the process may seem disproportionately extensive: up to 20 years may lapse from the initial DRE diagnosis to surgical intervention.2,18,19 While more recent data suggest that this timespan may have decreased to about 10 years,20 this remains a lengthy and highly burdensome ordeal, as during this time patients (and their families and caregivers) experience continued disruption in their ability to live their lives because of inadequately controlled seizures, which negatively affect their ability to perform daily activities and their quality of life and also result in substantial medical expenses. For patients with DRE, these medical visits and expenses typically increase over time.21
Information regarding the clinical and economic “journey” to neuromodulation may help identify areas to improve care for this vulnerable and underserved population. We previously examined this issue among patients with DRE identified in a large US healthcare claims database comprising individuals with commercial (ie, private) insurance.22 Results of that study found that during the 2-year period immediately prior to implantation, patients with DRE have substantial levels of comorbidities, including physical ailments (eg, chronic pulmonary disease, cerebrovascular disease, hemiplegia/paraplegia) and mental health disorders (eg, depression, anxiety); they also have high levels of utilization and cost of healthcare services and pharmacotherapies that increase over this 2-year interval.22
Although the previous study shed light on the journey to neuromodulation, it was limited to patients with DRE who were covered by private (ie, commercial) insurance, and there are other health insurance options in the US that should be considered. One such alternative US payer is Medicaid, which is the single largest source of health coverage in the US, providing healthcare coverage to over 72 million Americans. It is a joint state and federal program that covers specific groups of individuals, including those in low-income families, qualified pregnant women and children, individuals on Supplemental Security Income, and disabled or medically needy individuals.23 Some eligibility requirements may differ by state. Prior research has found an association between epilepsy and Medicaid coverage, although it is possible that the toll of the disease—particularly among those who are refractory to ASMs—may result in circumstances that qualify an individual (and/or their family) for Medicaid insurance. It is therefore important to assess the experiences of Medicaid enrollees with DRE to fully understand the toll of this disease in the US.24 This study used data from the US Centers for Medicare and Medicaid Services (CMS) to assess patterns of healthcare utilization and cost among Medicaid enrollees with DRE to better understand their journey during the 2 years before neurostimulator implantation.
Materials and Methods
Data Source
This was a retrospective, observational database study using healthcare claims and enrollment data on patients insured by Medicaid across the US obtained from CMS. The Medicaid database contains administrative healthcare data for millions of Americans who meet the aforementioned criteria. The database includes demographic data (including eligibility periods for medical and pharmacy benefits), claims for medical encounters (inpatient and outpatient), claims for outpatient prescription drug dispenses, and financial information.25 Medical claims include diagnoses (in International Classification of Diseases, 9th and 10th Revisions, Clinical Modification [ICD-9-CM and ICD-10-CM, respectively] formats), procedures (in ICD-9-CM; ICD-10-CM; Current Procedural Terminology, 4th Edition; and Healthcare Common Procedural formats), place(s) and date(s) of service, and reimbursed amounts by Medicaid. Payments made out of pocket or through other insurers are not available in this data set. Pharmacy claims include medications dispensed (in National Drug Code format), therapy-days and number of pills dispensed, and total reimbursed amounts. The database is compliant with the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and spanned the 10-year period from January 1, 2011, to December 31, 2020 (ie, the study period), which represents a duration 2 years longer than that in our original research, which focused on the period from January 1, 2012, to December 31, 2019.
Standard Protocol Approvals, Registrations, and Patient Consents
Institutional review board (IRB) assessment determined that this study was exempt from IRB oversight based on the US Department of Health and Human Services regulations found at 45 CFR 46.104(d)(4).
Study Selection Criteria
As with the previous study,22 we identified all patients with evidence of receipt of VNS, RNS, or DBS during the period between January 1, 2011, and December 31, 2020. Among all such patients, the earliest date on which one of these devices was identified was deemed the index date. As with the prior research, all patients were also required to (1) have a diagnosis of epilepsy on a medical (inpatient or outpatient) claim (in any position) on their index date, (2) have at least one ASM dispensed within the 12-month period immediately prior to index date, and (3) be continuously enrolled over the 2-year period prior to index date. Because our goal was to focus on a DRE cohort undergoing initial neurostimulation device implantation, patients were excluded if they had evidence of neuromodulation implantation, programing, maintenance, removal, or replacement over the period prior to the index date or multiple devices (ie, VNS, RNS, DBS) implanted on this date. Patients with Parkinson’s disease, a condition that may also be treated with neurostimulation, were also excluded.
Measures
Demographic characteristics (eg, age, gender, race) were assessed as of index date; clinical characteristics, including comorbidities, were based on all information available over the 2-year period immediately prior to index date. Patterns of use and cost of healthcare services and prescription pharmacotherapy were examined over the entire 2-year preindex period. Healthcare services and costs were assessed alternatively employing an all-cause and epilepsy-related focus, the latter of which was defined to include all medical claims with a diagnosis code (any position) of epilepsy and all ASM dispenses. Utilization and cost data were examined over the aggregate preindex period and within each month (ie, 24 months in total).
Data were summarized using descriptive statistics (eg, means, medians, percentages) and presented in tabular and graphical formats. There were no prespecified hypotheses, and analyses were purely descriptive; therefore, no comparisons were undertaken, and no statistical significance testing was performed.
Results
Sample Attrition
A total of 40,890 patients underwent VNS, RNS, or DBS implantation between January 1, 2011, and December 31, 2020. Of these, 36,566 (89.4%) had a diagnosis of epilepsy on the index date. A large number of patients, 21,948 (53.7% of all patients with evidence of neurostimulator implantation during the study period) were excluded because of lack of continuous enrollment over the 2 years prior to implantation (Table 1). A total of 2469 patients (6.0% of those with evidence of neurostimulators) met all selection criteria and constituted the study sample.
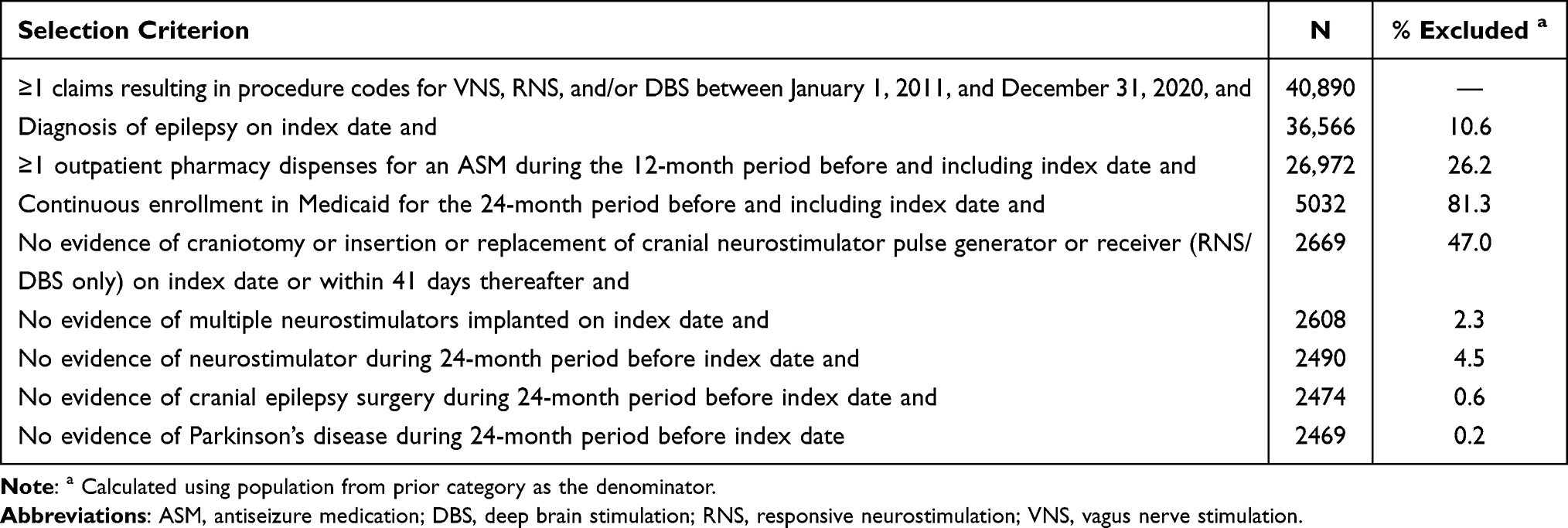 |
Table 1 Sample Attrition |
Patient Demographic and Clinical Characteristics
Mean (standard deviation [SD]) age at implantation was 20.8 (14.1) years; 52.2% of patients were under 18 years of age as of their index date (Table 2). Just over one-half of patients (52.9%) were male. Forty-nine percent of patients were non-Hispanic White, 12.7% were Black, 10.9% were Hispanic, 1.6% were American Indian/Alaska Native, 1.5% were Asian/Pacific Islander, 1.6% were designated of “other” race/ethnicity, and 23.0% had unknown race/ethnicity status. The majority of patients (97.0%) were designated ineligible for Medicare. Mean (SD) Charlson Comorbidity Index was 1.3 (1.5). Comorbidities were common over the preindex period and included respiratory infections/sinusitis/bronchitis (this condition was identified in 48.7% of the sample during preindex), learning disabilities (41.0%), hemiplegia or paraplegia (31.8%), abdominal/chest pain (31.6%), chronic pulmonary disease (26.3%), anxiety (20.2%), and depression (16.9%).
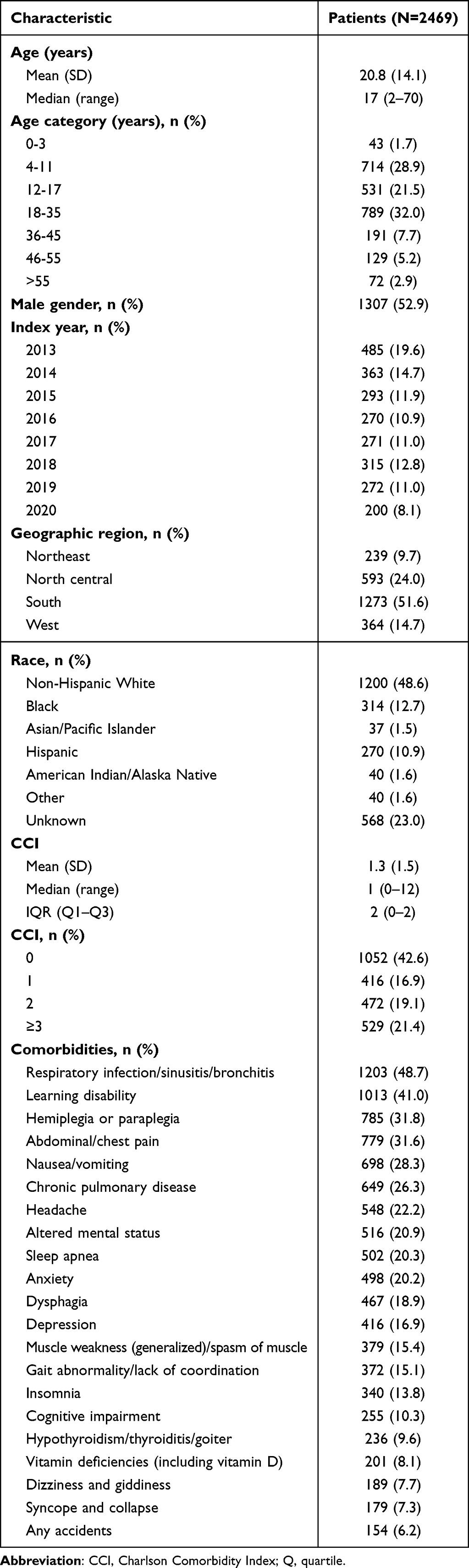 |
Table 2 Demographic and Clinical Characteristics of Medicare Enrollees With DRE Who Underwent Neurostimulator Implantation |
Patterns of Use of ASMs and Other Prescription Pharmacotherapies
Patients were prescribed a mean (SD) of 4.4 (1.7) unique ASMs over the 2-year period prior to implantation; 44.9% of patients received five or more ASMs (Figure 1). The most commonly prescribed ASM was levetiracetam (prescribed to 55.9% of patients), followed by diazepam (51.6%), lacosamide (36.7%), and clobazam (35.9%) (polypharmacy was common; accordingly, numbers sum to >100%). Twenty-seven percent of patients were dispensed antidepressants, and 10% were dispensed anxiolytics.
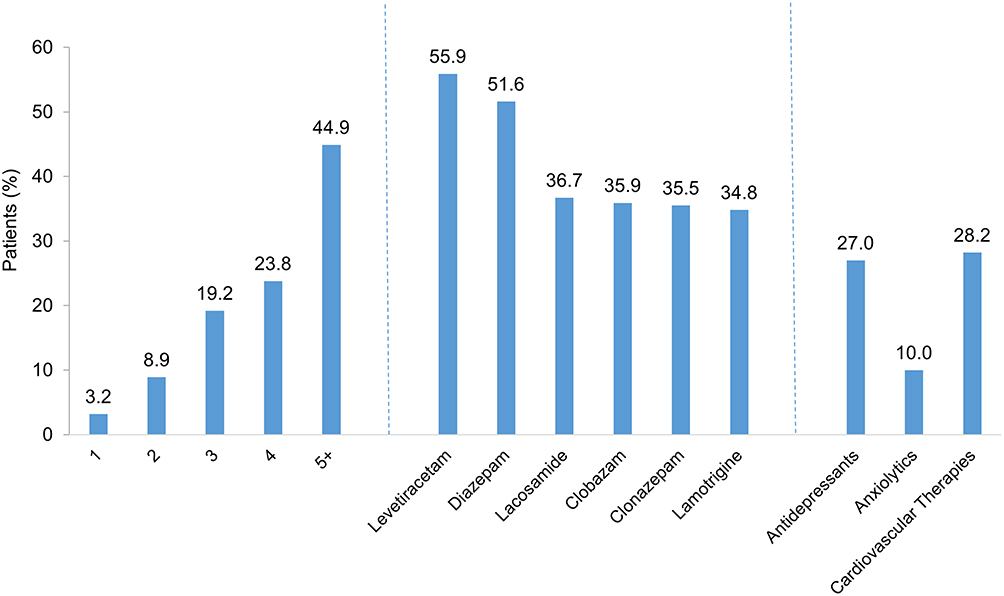 |
Figure 1 Use of ASMs and Other Pharmacotherapies Among Medicaid Enrollees With DRE Who Underwent Neurostimulator Implantation. Abbreviation: ASM, antiseizure medication. |
Patterns of Use and Cost of Healthcare Services
Over the 2-year period prior to implantation, 98.3% of patients had at least one physicians’ office visit; patients experienced a median (Q1, Q3) of 21 (10, 42) office visits during preindex, of which 6 (3, 11) were epilepsy-related. In the first 6 months of the preindex period (ie, the period ending 18 months prior to implantation), approximately 53% of patients experienced at least one physicians’ office visit monthly; in the last 6 months before implantation, this increased to about 60% monthly (Figure 2). Epilepsy-related visits showed a similar pattern—increasing from about 21% of patients with at least one epilepsy-related physicians’ office visit monthly, over the first 6 months of the preindex period, to about 34% monthly during the last 6 months before implantation.
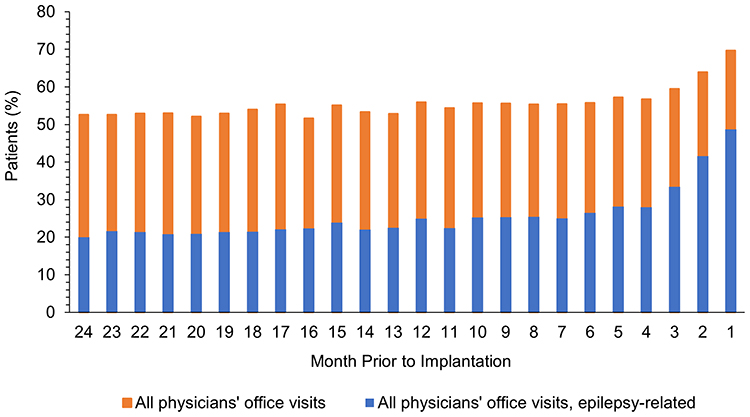 |
Figure 2 All-Cause and Epilepsy-Related Office Visits Among Medicaid Enrollees With DRE During the 2-Year Period Prior to Neurostimulator Implantation. |
More than one-half of patients (57.3%) were hospitalized at least once (all-cause) during the preindex period; 55.3% had at least one epilepsy-related inpatient admission over this period (by definition, epilepsy-related care is a component of all-cause care) (Table 3). Mean (SD) numbers of all-cause and epilepsy-related admissions were 1.5 (2.6) and 1.3 (2.0), respectively; corresponding values for length of stay were 8.1 (18.8) and 7.0 (14.7). Eighty-three percent of patients had at least one all-cause emergency department (ED) visit and 66.1% had at least one epilepsy-related ED visit. The median numbers of computed tomography/magnetic resonance imaging (CT/MRI) scans, electroencephalograms (EEGs), and video EEGs were zero; only 29.5% of patients received at least one CT/MRI scan, and less than one-half (49.0%) received an EEG.
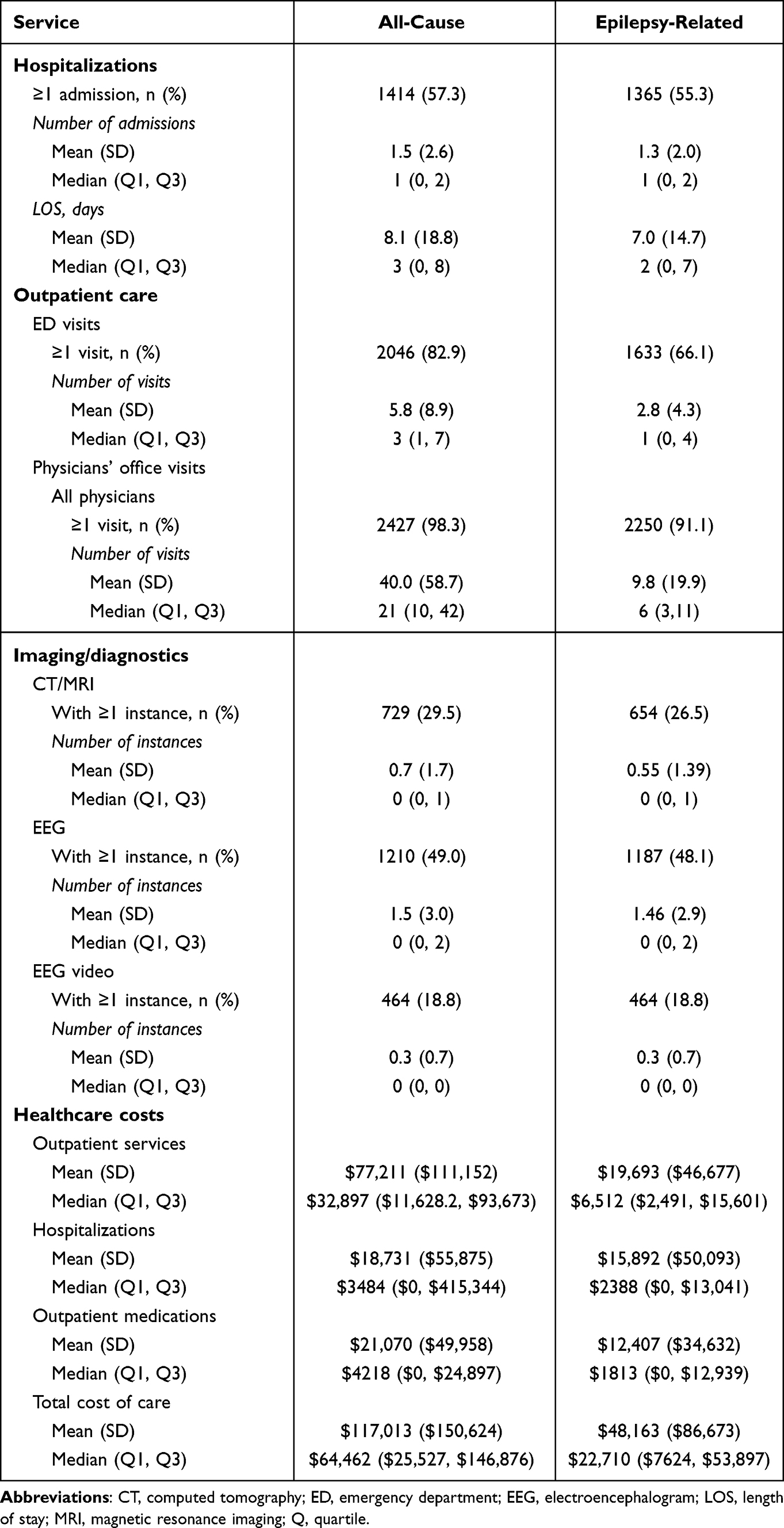 |
Table 3 Use and Cost of Healthcare Services Among Medicaid Enrollees with DRE Who Underwent Neurostimulator Implantation, by Allocation of Care |
Total mean (SD) all-cause healthcare costs were $117,013 ($150,624), and total epilepsy-related healthcare costs were $48,163 ($86,673), or 41.2% of all-cause costs. Corresponding median (Q1, Q3) values were $64,462 ($25,527, $146,876) and $22,710 ($7624, $53,897). Mean monthly all-cause costs increased by 60.8% during preindex (from $4184 during the 24th month before implantation to $6727 in the month prior); mean monthly epilepsy-related costs increased by 155.0% (from $1486 to $3782) (Figure 3). Inpatient care, outpatient care, and prescription pharmacotherapy accounted for 16.0%, 66.0%, and 18.0%, respectively, of all-cause costs during the 24-month period of interest; they accounted for 33.0%, 40.9%, and 25.8%, respectively, of epilepsy-related costs.
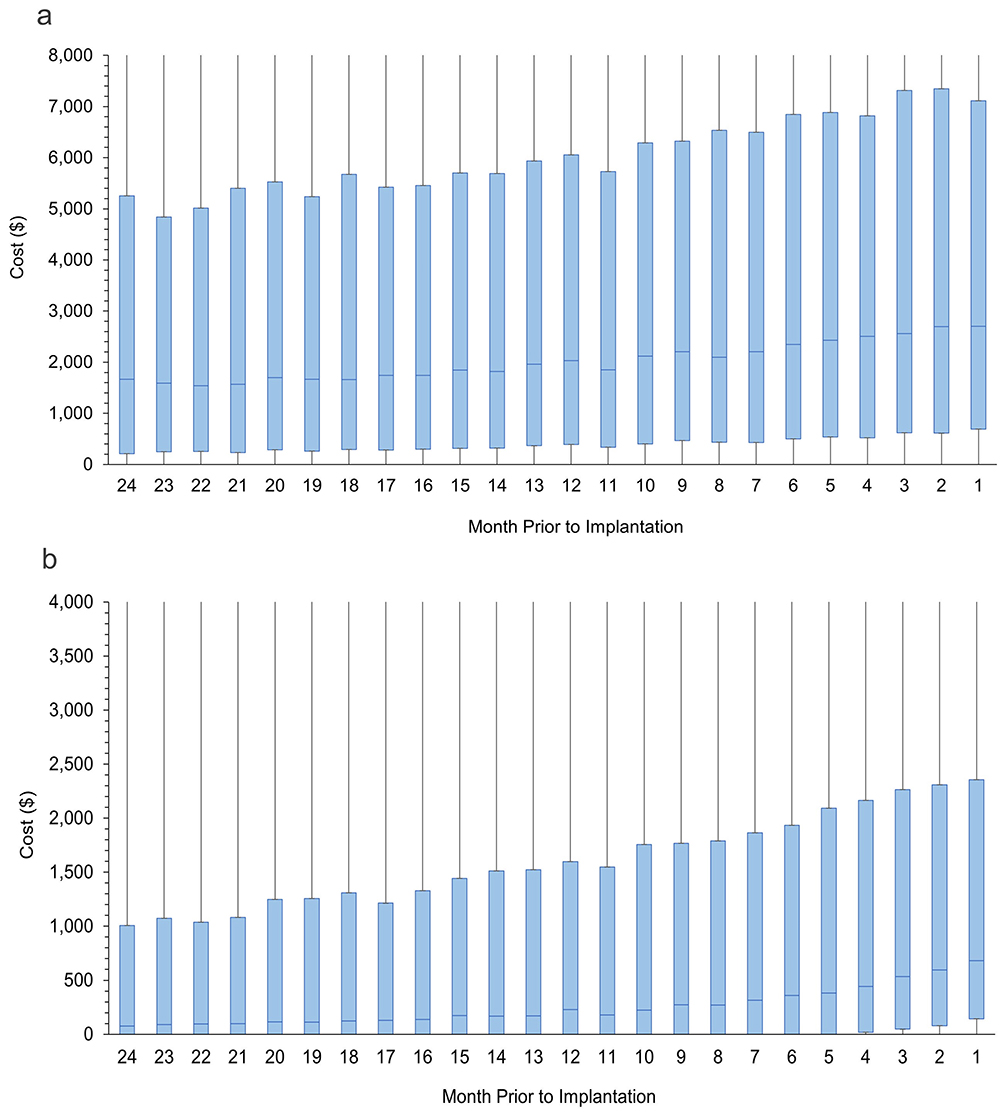 |
Figure 3 All-Cause and Epilepsy-Related Costs Among Medicaid Enrollees With DRE Who Underwent Neurostimulator Implantation, by Month Prior to Implantation. (a) All-Cause. (b) Epilepsy-Related. Notes: For each month, the blue box denotes the interquartile range; the blue line within the blue box, the median cost; black vertical lines indicate minimum and maximum costs. |
Discussion
Results of this study are consistent with those of our prior work and suggest that Medicaid enrollees who suffer from DRE face a high healthcare burden that results in substantial cost over the 2-year period prior to neurostimulator implantation. These patients, who are young (average age: 20.8 years), experience high rates of comorbidities, including learning disabilities, hemiplegia or paraplegia, depression, and anxiety. They are also characterized by high levels of use of pharmacotherapy; just under half of the patients were prescribed at least five ASMs despite the fact that these agents are relatively unlikely to provide adequate seizure control.6 Over the 2-year period prior to implantation, patients averaged about one physician’s visit per month, more than one-half had at least one epilepsy-related hospital admission, and about two-thirds had at least one epilepsy-related ED visit. Healthcare costs were also high—total mean all-cause healthcare costs were $117,013, almost half of which were epilepsy-related. Epilepsy-related healthcare costs increased over time; monthly costs doubled from the beginning of the 2-year preimplantation period to the month prior to implantation. This increase in costs is not fully explained by the costs of presurgical work up. For example, elements required for preoperative clearance for VNS include blood tests, electrocardiograms, chest x-rays, and an office visit.26–31 The average cost of this collection of services in our database was $286. Even after removing the cost of the services most proximal to the index date, epilepsy-related costs still doubled from the beginning of the 2-year preimplantation period to the month prior to implantation. Furthermore, observed healthcare costs during the 2-year period prior to implantation far exceeded reported average annual per-patient costs for Medicaid enrollees ($58,506 in our study vs $6556).32,33 While this example of preoperative care assessed was specific to VNS and may underrepresent comparable costs for RNS and DBS, both of which are more labor-intensive procedures, it is likely that a similar phenomenon would have been observed among patients with RNS or DBS if preclearance utilization specific to those procedures had been removed. Consequently, these findings indicate a need to consider nonpharmacologic interventions such as neurostimulators (where clinically appropriate) earlier in the patient journey.
Only about one-half of patients underwent EEG during the 2-year preindex period; even fewer patients underwent CT/MRI (29.5%) or EEG video (18.8%). By comparison, in our prior analyses of patients with DRE who had commercial (ie, private) insurance, 72.4% underwent EEG; 79.3%, CT/MRI; and 26.6%, EEG video (all over the comparable 2-year period prior to implantation). Previous research indicates that patients with epilepsy who have public health insurance such as Medicaid have less access than their commercially insured counterparts to specialized epilepsy care, such as video EEG monitoring.34 Given that brain imaging is an important tool for the diagnosis and classification of seizure type, which can inform decisions concerning treatment options/regimens, the relatively low levels of use of these procedures highlight a possible gap in care experienced by patients with DRE who have Medicaid insurance. While speculative, it is possible that this gap could be due, at least in part, to an unwillingness of healthcare providers to accept new patients insured by Medicaid. A study based on data from the National Ambulatory Medical Care Survey found that only 74.3% of physicians indicated a willingness to accept new patients with Medicaid insurance versus 96.1% for those with commercial insurance.35 Less willingness to accept new patients may be due in part to lower reimbursement rates and/or difficulty obtaining reimbursement from state Medicaid programs.32 Medicaid has lower reimbursement rates than commercial insurance, in extreme instances resulting in hospital reimbursement at levels approximately one-half of those issued by commercial insurers.32 This cost difference is also illustrated in our data, where epilepsy-related healthcare costs were markedly higher among commercially insured patients ($91,995)22 than among Medicaid enrollees ($48,163). Further study is needed to better understand the underlying reason(s) for these low levels of use of important diagnostic and management tools in DRE and their resulting impacts on patient health, including the rate of referral to surgery centers for initial consultation on the appropriateness of nonpharmacologic treatment options such as neurostimulators.
Many similarities were identified between the commercially insured patients with DRE included in our prior research and the Medicaid enrollees with this condition who constituted the current study population with respect to demographic and clinical characteristics, as well as levels of use and cost of healthcare services and prescription therapies. However, important differences were also identified between the two populations. First, Medicaid enrollees were younger than commercial enrollees at age of implantation (20.8 years vs 26.4 years).22 Second, while both groups of patients had high levels of comorbidities, patients insured by Medicaid were almost twice as likely as commercially insured patients to have hemiplegia or paraplegia or learning disabilities; however, they were slightly less likely to have anxiety or depression. Third, Medicaid enrollees were slightly more likely than commercially insured patients to receive care in EDs on both an all-cause (82.9% vs 68.1%) and epilepsy-related (66.1% vs 55.8%) basis. Furthermore, outpatient visits (including ED visits) accounted for 66% of total all-cause costs for Medicaid enrollees (vs 36% for commercial).22 This difference is consistent with results from previous research that found that, compared with commercially insured patients, patients insured by Medicaid are seven times more likely to have a low-severity visit (ie, a visit that may have been more appropriate in a primary care setting) and four times more likely to have a high-severity ED visit.36
This study has several limitations. First, as with any healthcare claims-based analysis, information is limited to what was entered into the database; consequently, there may be errors of omission and/or commission, without the means to identify or rectify them. For this reason, statistical analyses to address missing data were not performed. However, monthly coverage indicators were available, and only patients who were continuously enrolled and eligible for medical and pharmacy benefits for the entire 2-year follow-up period were included, removing the risk of missing data due to gaps in coverage. Second, clinical symptoms such as seizure frequency and severity are not captured nor are indirect costs, impacts on quality of life, impacts on family and caregivers, the ability to work, or psychosocial impacts such as social stigmatization. As such, results of our work likely underestimate the clinical and economic toll experienced by patients with DRE during the 2-year period before implantation. Geographic residence and types of providers or treatment centers visited are also unavailable, limiting our understanding of the patient journey to implantation and the degree to which observed patterns of utilization and cost of care reflect unfettered access to relevant providers or compromises based on any number of issues (eg, lack of transportation, insufficient funds). Third, the selection criteria have not been formally validated, thus, while somewhat intuitive and consistent with a cohort who undergoes implantation for the treatment of DRE, potential misclassification errors are unknowable. Fourth, while our research enhances generalizability to both commercial and Medicaid insurance populations, the degree to which these findings apply to all individuals with DRE covered by other types of insurance or those undergoing implantation in other countries is unknown.
Lastly, this study captured the final stage of a much longer patient journey, which may last up to 20 years from DRE diagnosis to surgical intervention. The high yearly turnover of Medicaid enrollment (only about 20% of patients in our sample were continuously enrolled for the 2-year period of interest) limits the ability to follow patients for longer periods of time. Thus, we opted to focus on the final 2 years before surgery, as this may indicate a period of relatively high cost and potential for earlier intervention (our findings indicated that an average annual per-patient costs for Medicaid enrollees were $58,506). Even with this relatively short period, about 80% of patients with epilepsy who received a neurostimulator were dropped from inclusion due to having less than 2 years of coverage prior to implantation (21,940 of 26,972; Table 1). Further studies are needed to explore patient experiences over the full, protracted course of DRE.
Conclusions
In conclusion, our findings indicate that Medicaid enrollees with DRE who undergo neurostimulator implantation are young and often suffer a substantial comorbidity burden. In the 2-year period before neurostimulator implantation, patients experience relatively high levels of utilization and cost of medical care and prescription pharmacotherapy, a large proportion of which are epilepsy-related. Specific patterns of utilization observed suggest that, relative to commercially insured patients, Medicaid enrollees with DRE are nominally more likely to receive care in the ED and markedly less likely to undergo imaging procedures that are recommended as part of comprehensive management and evaluation in this population.37 The high levels of utilization in the ED and underutilization of imaging may suggest a gap in comprehensive care for Medicaid enrollees with DRE. Further research is needed to better understand the clinical, economic, and psychological impacts associated with neurostimulator implantation in Medicaid enrollees with DRE and whether broader and earlier access to specialized epilepsy care may reduce their disease burden and/or hasten implantation, either or both of which in turn may reduce costs to Medicaid.
Abbreviations
ASM, antiseizure medication; DRE, drug-resistant epilepsy; FDA, Food and Drug Administration; VNS, vagus nerve stimulation; RNS, responsive nerve stimulation; DBS, deep brain stimulation; CMS, Centers for Medicare and Medicaid Services; HIPAA, Health Insurance Portability and Accountability Act; IRB, institutional review board; ICD-9-CM, International Classification of Diseases, 9th Revision, Clinical Modification; ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification; ED, emergency department; CT, computed tomography; MRI, magnetic resonance imaging; EEG, electroencephalogram; N, number; SD, standard deviation; Q1, first quartile; Q3, third quartile.
Data Sharing Statement
This study used healthcare claims and enrollment data on patients insured by Medicaid across the US obtained from the US Centers for Medicare and Medicaid Services (CMS). The anonymized data are not available to the public due to contracting terms with CMS.
Ethics Approval and Informed Consent
Institutional review board (IRB) assessment determined that this study was exempt from IRB oversight based on the US Department of Health and Human Services regulations found at 45 CFR 46.104(d)(4). No new human or animal data were collected during this study.
Consent for Publication
All authors have reviewed the article contents and consent to its publication. All images used in this article are original and can be published.
Acknowledgments
Medical writing support was provided in accordance with Good Publication Practice guidelines by Adam Fix, PhD (PPD clinical research business of Thermo Fisher Scientific) and was paid for by LivaNova.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Author contributions are as follows:
Kathryn Evans: drafting/revising/approving manuscript, study concept and design, analysis and interpretation of data.
Qian Li: revising/approving manuscript, analysis and interpretation of data.
Lu Zhang: drafting/revising/approving manuscript, analysis and interpretation of data.
Sandi Lam: drafting/revising/approving manuscript, analysis and interpretation of data.
Bronwyn Do Rego: drafting/revising/approving manuscript, analysis and interpretation of data.
Vanessa Danielson: revising/approving manuscript, data acquisition, study concept and design.
Reginald Lassagne: revising/approving manuscript, data acquisition, study concept and design.
Ariel Berger: drafting/revising/approving manuscript, study concept and design, analysis and interpretation of data.
Funding
This work was supported by LivaNova PLC, London, UK. In addition to providing the funding that enabled the research, the sponsor was involved in data acquisition, study design, and in the drafting of this article.
Disclosure
At the time, this work was conducted, and Bronwyn Do Rego, Reginald Lassagne, and Vanessa Danielson were paid employees and potential shareholders of LivaNova, a manufacturer of the vagus nerve stimulation device and other medical devices. Kathryn Evans, Ariel Berger, and Qian Li are employees of Thermo Fisher Scientific and members of the PPD™ Evidera™ Real-World Data & Scientific Solutions team, hired by LivaNova to consult on this project. Sandi Lam provides consultancy for LivaNova for scientific advice and serves as a speaker for LivaNova on access to care in epilepsy. She is also a consultant for Brainlab, Ovid Therapeutics, Jaguar Therapeutics, and Encoded Therapeutics, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Behr C, Goltzene MA, Kosmalski G, Hirsch E, Ryvlin P. Epidemiology of epilepsy. Rev Neurol. 2016;172(1):27–36. doi:10.1016/j.neurol.2015.11.003
2. Engel J Jr. What can we do for people with drug-resistant epilepsy? The 2016 wartenberg lecture. Neurology. 2016;87(23):2483–2489. doi:10.1212/WNL.0000000000003407
3. Kobau R, Zahran H, Thurman DJ, et al. Epilepsy surveillance among adults--19 states, behavioral risk factor surveillance system, 2005. MMWR Surveill Summ. 2008;57(6):1–20.
4. Wiebe S, Jette N. Pharmacoresistance and the role of surgery in difficult to treat epilepsy. Nat Rev Neurol. 2012;8(12):669–677. doi:10.1038/nrneurol.2012.181
5. Cramer JA, Wang ZJ, Chang E, et al. Healthcare utilization and costs in adults with stable and uncontrolled epilepsy. Epilepsy Behav. 2014;31:356–362. doi:10.1016/j.yebeh.2013.09.046
6. Hersi H, Saarinen JT, Raitanen J, Peltola J. Response to subsequent antiseizure medications after first antiseizure medication failure in newly diagnosed epilepsy. Front Neurol. 2022;13:1042168. doi:10.3389/fneur.2022.1042168
7. Anyanwu C, Motamedi GK. Diagnosis and surgical treatment of drug-resistant epilepsy. Brain Sci. 2018;8(4):49. doi:10.3390/brainsci8040049
8. NeuroPace. NeuroPace receives IDE approval to initiate NAUTILUS pivotal study of its RNS system for idiopathic generalized epilepsy. Press release. Available from: https://neuropace.com/press-release/neuropace-receives-ide-approval-to-initiate-nautilus-pivotal-study-of-its-rns-system-for-idiopathic-generalized-epilepsy/.
9. Rincon N, Barr D, Velez-Ruiz N. Neuromodulation in drug resistant epilepsy. Aging Dis. 2021;12(4):1070–1080. doi:10.14336/AD.2021.0211
10. Food and Drug Administration. Premarket approval (PMA). VNS therapy system. 2024. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P970003S207.
11. Food and Drug Administration. Premarket approval (PMA). Neuropace RNS system. 2024. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P100026.
12. Food and Drug Administration. Premarket approval (PMA). Medtronic DBS therapy for epilepsy. 2024. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P960009S318.
13. Kuba R, Brazdil M, Kalina M, et al. Vagus nerve stimulation: longitudinal follow-up of patients treated for 5 years. Seizure. 2009;18(4):269–274. doi:10.1016/j.seizure.2008.10.012
14. Markert MS, Fisher RS. Neuromodulation - science and practice in epilepsy: vagus nerve stimulation, thalamic deep brain stimulation, and responsive neurostimulation. Expert Rev Neurother. 2019;19(1):17–29. doi:10.1080/14737175.2019.1554433
15. Nair DR, Laxer KD, Weber PB, et al. Nine-year prospective efficacy and safety of brain-responsive neurostimulation for focal epilepsy. Neurology. 2020;95(9):e1244–e1256. doi:10.1212/WNL.0000000000010154
16. Razavi B, Rao VR, Lin C, et al. Real-world experience with direct brain-responsive neurostimulation for focal onset seizures. Epilepsia. 2020;61(8):1749–1757. doi:10.1111/epi.16593
17. Solli E, Colwell NA, Say I, et al. Deciphering the surgical treatment gap for drug-resistant epilepsy (DRE): a literature review. Epilepsia. 2020;61(7):1352–1364. doi:10.1111/epi.16572
18. Berg AT. Understanding the delay before epilepsy surgery: who develops intractable focal epilepsy and when? CNS Spectr. 2004;9(2):136–144. doi:10.1017/s109285290000849x
19. Mazumder R, Pasqua J, Keselman I. Diagnostic treatment delay in temporal lobe epilepsy. Pract Neurol. 2021;2021(October):36–38,50.
20. Kwan P, Boffini M, Fahoum F, et al. Baseline characteristics and predictors for early implantation of vagus nerve stimulation therapy in people with drug-resistant epilepsy: observations from an international prospective outcomes registry (CORE-VNS). Epilepsia Open. 2024;9(5):1837–1846. doi:10.1002/epi4.13015
21. Sperling MR. The consequences of uncontrolled epilepsy. CNS Spectr. 2004;9(2):98–101,106–109. doi:10.1017/s1092852900008464
22. Evans K, Stamas N, Li Q, et al. Patterns of utilization and cost of healthcare services and pharmacotherapy among patients with drug-resistant epilepsy during the two-year period before neurostimulation: a descriptive analysis of the journey to implantation based on analyses of a large United States healthcare claims database. Epilepsy Behav. 2023;145:109288. doi:10.1016/j.yebeh.2023.109288
23. Centers for Medicare & Medicaid Services. Medicaid eligibility. Available from: https://www.medicaid.gov/medicaid/eligibility/index.html.
24. Thurman DJ, Kobau R, Luo YH, Helmers SL, Zack MM. Health-care access among adults with epilepsy: the U.S. National Health Interview Survey, 2010 and 2013. Epilepsy Behav. 2016;55:184–188. doi:10.1016/j.yebeh.2015.10.028
25. Centers for Medicare & Medicaid Services. Data. Available from: https://www.cms.gov/newsroom/data.
26. Baumgartner C, Koren JP, Britto-Arias M, Zoche L, Pirker S. Presurgical epilepsy evaluation and epilepsy surgery. F1000Res. 2019;8(F1000 Faculty Rev):1818. doi:10.12688/f1000research.17714.1
27. Cedars-Sinai. Vagus nerve stimulator. Available from: https://www.cedars-sinai.org/health-library/tests-and-procedures/v/vagus-nerve-stimulator.html.
28. Epilepsy Foundation. Epilepsy for parents and caregivers. Available from: https://www.epilepsy.com/parents-and-caregivers.
29. Mayfield Brain & Spine. Epilepsy surgery. 2021. Available from: https://mayfieldclinic.com/pe-epilepsysurg.htm.
30. The Royal Children’s Hospital Melbourne. Vagus nerve stimulation. Available from: https://www.rch.org.au/neurology/patient_information/vagus_nerve_stimulation/.
31. UCSF Benioff Children’s Hospitals. Patient education A-Z. Epilepsy presurgical evaluation. Available from: https://www.ucsfbenioffchildrens.org/education/epilepsy-presurgical-evaluation.
32. Joffe M, Chanwong K. Containing Medicaid costs at the state level. 2024. Available from: https://www.cato.org/policy-analysis/containing-medicaid-costs-state-level.
33. KFF. 2022 Employer health benefits survey. 2022. Available from: https://www.kff.org/report-section/ehbs-2022-summary-of-findings/.
34. Schiltz NK, Koroukian SM, Singer ME, Love TE, Kaiboriboon K. Disparities in access to specialized epilepsy care. Epilepsy Res. 2013;107(1–2):172–180. doi:10.1016/j.eplepsyres.2013.08.003
35. Medicaid and CHIP Payment and Access Commission. Physician acceptance of new Medicaid patients: findings from the National Electronic Health Records Survey. 2021. Available from: https://www.macpac.gov/wp-content/uploads/2021/06/Physician-Acceptance-of-New-Medicaid-Patients-Findings-from-the-National-Electronic-Health-Records-Survey.pdf.
36. Kim H, McConnell KJ, Sun BC. Comparing emergency department use among Medicaid and commercial patients using all-payer all-claims data. Popul Health Manag. 2017;20(4):271–277. doi:10.1089/pop.2016.0075
37. Adin ME, Spencer DD, Damisah E, Herlopian A, Gerrard JL, Bronen RA. Imaging of neuromodulation and surgical interventions for epilepsy. AJNR Am J Neuroradiol. 2021;42(10):1742–1750. doi:10.3174/ajnr.A7222
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.