Back to Journals » Clinical Ophthalmology » Volume 15
Healthcare Resource Utilization and Costs in Patients with Geographic Atrophy Secondary to Age-Related Macular Degeneration
Authors Kim A, Devine B ![]() , Campbell J, Shirneshan E, Zhao C, Bansal A
, Campbell J, Shirneshan E, Zhao C, Bansal A
Received 26 February 2021
Accepted for publication 1 June 2021
Published 23 June 2021 Volume 2021:15 Pages 2643—2651
DOI https://doi.org/10.2147/OPTH.S307603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ashley Kim,1– 3 Beth Devine,1 Joanna Campbell,2 Elaheh Shirneshan,2 Changgeng Zhao,2 Aasthaa Bansal1
1The Comparative Health Outcomes, Policy, and Economics (CHOICE) Institute, Department of Pharmacy and The Department of Health Services and Economics, University of Washington, Seattle, WA, USA; 2Allergan, an AbbVie company, Irvine, CA, USA; 3GRAIL, Inc, Menlo Park, CA, USA
Correspondence: Ashley Kim Email [email protected]
Purpose: Geographic atrophy (GA) is an advanced form of nonexudative age-related macular degeneration (AMD) that lacks treatment options. With considerable interpatient variability in the rate of GA progression due to lesion characteristics, information characterizing the disease burden is limited. The aim of this study was to describe the healthcare resource utilization (HCRU) and costs associated with increasing severity levels of GA.
Patients and Methods: A retrospective analysis was conducted using claims data from IQVIA’s PharMetrics Plus database. Patients with a prevalent GA diagnosis were identified between October 1, 2016 and June 30, 2017 and classified by disease severity and laterality. Disease-specific HCRU and costs by disease severity were assessed during the 12-month follow-up period, with multivariable analyses performed adjusting for baseline characteristics.
Results: A total of 28,773 GA cases were identified (mean age = 68.7; 58.5% female), of which 24% and 76% had unilateral and bilateral GA, respectively, with varying levels of recorded severity (in increasing order): early or intermediate (EI) AMD, GA without subfoveal involvement (GAwoSF), and GA with subfoveal involvement (GAwSF). Patients with greater baseline severity in the bilateral group had a significantly higher number of outpatient (OP) visits per year (1.98 EI AMD; 2.57 for GAwoSF; 2.63 for GAwSF). Increasing disease severity was associated with higher patient-related costs in the outpatient setting (mean [SD] of $82 [$157], $110 [$559] for unilateral EI AMD and GAwSF, respectively, and $56 [$94], $64 [$97], $59 [$85] for bilateral EI AMD, GAwoSF, GAwSF, respectively). Similarly, higher payer-related costs were seen in patients with bilateral GAwSF compared to bilateral EI AMD (mean [SD] $280 [$325]; $198 [$262]).
Conclusion: Study findings demonstrate that patients, with more severe GA at baseline, experience greater HCRU and costs in the outpatient setting. Further research should explore specific contributing factors to the long-term economic burden of GA.
Keywords: age-related macular degeneration, geographic atrophy, healthcare resource utilization, healthcare costs
Introduction
Geographic atrophy (GA) is a late-stage manifestation of nonexudative age-related macular degeneration (AMD) that affects nearly 1 million people in the United States (US) and 5 million people worldwide, and leads to significant visual function impairment and eventual blindness.1 Characterized by the formation of drusen, or pigmentary changes at the macula, AMD is the most common cause of irreversible central vision loss in elderly patients in the US,2 and consists of 2 major advanced forms that are not mutually exclusive: dry, atrophic, or nonexudative AMD and wet, neovascular, or exudative AMD.3 The nonexudative form is more prevalent, with nearly 85% of patients with AMD having the dry form,1 and involves a slow progressive degeneration of the retina, whereas the exudative form is less frequent but is responsible for 90% of acute blindness due to choroidal neovascularization (CNV).4 Patients with CNV may develop atrophy after a few years, and similarly, patients with atrophy can also eventually develop CNV.5
Although advanced stages of AMD consisting of geographic atrophy and neovascular AMD can coexist due to common risk factors, GA occurs specifically through the loss of the retinal pigment epithelium with associated loss of thermocapillary, and scotomas, or blind spots, can develop.5 Strong risk factors for GA include advanced age, history of smoking, and high levels of oxidative stress damaging the macula.1
Geographic atrophy can be categorized into 3 main levels of severity, in increasing order: early to intermediate AMD (EI AMD), advanced atrophic nonexudative AMD without subfoveal involvement (GAwoSF), and advanced atrophic nonexudative AMD with subfoveal involvement (GAwSF).6 Patients with EI AMD may progress to GAwoSF, which does not involve the center of the fovea, or GAwSF, which does involve the center of the fovea. Whereas severe visual acuity loss occurs more slowly and less commonly in patients with GA, and the fovea is spared until late in the course of the disease, GA involving the foveal center causes approximately 10% of all AMD-related visual loss.7 Patients whose GA does not involve the central fovea may have relatively good distance visual acuity yet manifest a substantially decreased ability to perform near visual tasks, such as reading.6
Unlike exudative AMD, which can effectively be treated with anti-vascular endothelial growth factor (VEGF) drugs,3 there are currently no approved treatments to prevent the onset and progression of GA.1 Patients are given non-drug–related treatments, including nutritional supplements, vitamins, and advice on lifestyle modifications, such as quitting smoking, and none of these treatments have established effectiveness. Previous research has suggested that GA is associated with a significant decline in vision-related quality of life in patients, in areas such as driving, reading, recognizing faces, and watching television, and a greater risk for developing or experiencing cognitive dysfunction.1,8–14 Disease progression has also been shown to be associated with increased annual Medicare expenditures.15 However, the current literature describing GA, specifically, is sparse; with many existing studies in late AMD lacking discrimination between neovascular and non-exudative AMD.
Our aim was to expand the scope of previous studies to better understand the burden of GA in a nationally representative sample of Americans aged 50 years and older, as AMD is a significant cause of blindness in people age 50 and older.1 Accordingly, this study was designed to characterize the incidence and prevalence of GA and examine prevalent cases of GA across the different severity levels, by assessing the association of severity level with healthcare resource utilization (HCRU) and cost. We hypothesized that patients with more severe GA will have significantly higher rates of healthcare resource utilization and total direct health care costs.1
Methods
Data Source
Data were obtained from IQVIA PharMetrics Plus claims database, which captures fully adjudicated pharmacy and medical claims data for more than 130 million unique enrollees across the US with commercial insurance, Medicare, and Medicaid. PharMetrics Plus provided de-identified patient-level data on patient demographics, comorbidities, healthcare resource utilization, and costs in compliance with the patient confidentiality requirements of the Health Insurance Portability and Accountability Act of 1996. The current study did not require Institutional Review Board (IRB) review and approval, as the study protocol did not meet the federal definition of “human subjects research,” as determined by the University of Washington Human Subjects Division IRB.
Study Design
This observational, retrospective cohort study consisted of an analysis time frame that ranged from October 1, 2015 to June 30, 2018. The date of first diagnosis of GA during the period from October 1, 2016 through June 30, 2017 (deemed the enrollment period) was defined as the index date. Patients were required to be at least 50 years of age as of the index date, and were excluded if they had GA with unspecified severity level or eye.
The 12-month period before the index date was defined as the pre-index period, when patients’ baseline characteristics and comorbidities were assessed. In addition, the 12-month period after the index was defined as the post-index, or follow-up, period, in which the patients’ healthcare resource utilization and costs were recorded. All patients were required to be continuously enrolled for 12 months before and following the index date.
Study Population
The study population was classified into 6 patient cohorts stratified by disease severity and laterality. The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes for GA specify both laterality and severity (Supplementary Table 1); as such, the cohorts were organized into 3 different severity levels within the unilateral and bilateral groups to ensure accurate documentation and characterization. The cohorts, in increasing order of severity, were: (1) unilateral EI AMD, (2) unilateral GAwoSF, (3) unilateral GAwSF, (4) bilateral EI AMD, (5) bilateral GAwoSF, and (6) bilateral GAwSF.
Unilateral GA was defined as having a claim history specifying GA in one eye only during the entirety of the follow-up period, with the index date set as the first date or claim of diagnosis of unilateral GA during the index period. Similarly, bilateral GA was defined by claims indicating GA in both eyes, with severity classified based on the more severe eye. For instance, if a patient had EI AMD in the left eye and GAwoSF in the right eye, then the patient would be classified as having bilateral GAwoSF, and all outcomes would be calculated as such. Additionally, if a patient were diagnosed with GAwoSF in both eyes, then the patient would simply be classified as having bilateral GAwoSF and outcomes would be measured identically, regardless of progression in the post-index period.
Patient Characteristics
Baseline characteristics, including age, sex, geographic location, and health plan type, were reported as of the index date. Charlson Comorbidity Index (CCI) scores, which predict mortality risk and are defined by 22 medical conditions, were calculated for each patient, with a higher CCI score indicating greater comorbidity burden. The prevalence of specific comorbid ocular (eg, wet AMD, diabetic retinopathy, glaucoma) and psychological (eg, anxiety, depression) conditions was collected for all patients.
Outcome Measures
Disease-specific healthcare resource utilization and costs, which were defined by the presence of a diagnosis of procedure code for nonexudative AMD or GA, were evaluated for the 12-month post-index period by type of service: outpatient, emergency department, and inpatient. Average inpatient length of stay (LOS) was also reported. Direct healthcare costs were examined from the payer perspective, which included the contracted or accepted reimbursable amount for covered medical services that the health plan agrees to pay to service providers; and from the patient perspective, which included any copays, coinsurance, and deductibles. All costs were adjusted to 2019 US dollars using the medical care component of the Consumer Price Index.16 In addition, the incidence and prevalence of GA in the follow-up period were calculated. In addition to disease-specific healthcare resource utilization and costs, all-cause healthcare resource utilization and costs were also evaluated and are included in Supplementary Tables 2 and 3.
Statistical Analysis
Standard summary descriptive statistics were used to evaluate differences in baseline characteristics including demographics among all study cohorts. To characterize the incidence and prevalence of GA, new incident cases were identified within the index period by identifying newly diagnosed patients and excluding individuals with a history of GA in the pre-index period. Prevalent cases were simply calculated as the total number of patients with GA in the index period, regardless of previous diagnoses.
Multivariable analyses were conducted on the prevalent cases, and to assess the association between GA severity level and healthcare resource utilization, using EI AMD as the reference group. A negative binomial regression model was used to estimate the association between severity level and rates of outpatient, emergency department, and inpatient admissions, as this model accounts for overdispersion in count data.17 We adjusted for age, sex, geographic region, insurance type, CCI, and both ocular and psychological comorbidities, separately for unilateral and bilateral patients.
In addition, generalized linear models were used to compare cost outcomes in patients with GA. The models used a gamma-distributed error and log link to account for the right-skewed distribution of cost data.18–21 We adjusted for patients’ baseline characteristics and comorbidities. The marginal or incremental costs between cohorts were obtained by applying the method of recycled predictions to the model.22 For both healthcare resource utilization and costs, we conducted multivariate generalized linear models to explore effect modification by including an interaction term between GA severity and laterality. All data management and statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and STATA 15 software (StataCorp LP Lakeway, TX, USA).
Results
Baseline Characteristics
A total of 28,773 patients with GA were included in the study (Figure 1). The mean age was 69 years, and 59% were female. The most common clinical form of GA was EI AMD, regardless of laterality (95% of all patients). The impact of comorbidity was greater in individuals with more severe GA. Demographic and clinical characteristics are shown in Table 1 and Figure 1. Nearly 30% of patients had a baseline ocular comorbidity, with the most common being wet, exudative AMD. Patients with unilateral GA had higher rates of nonexudative AMD, compared to patients with bilateral GA, although the rates increased proportionally with severity.
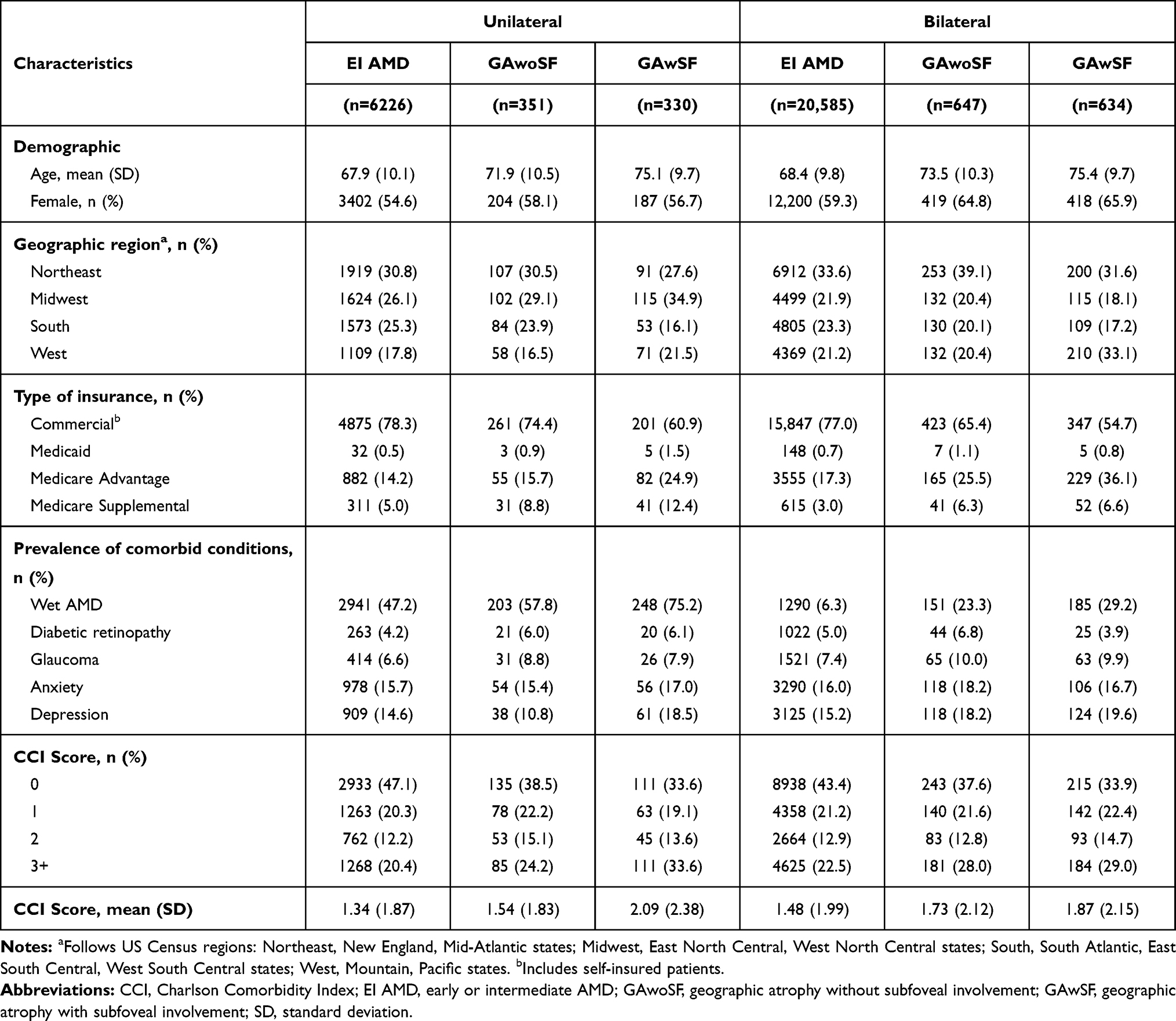 |
Table 1 Baseline Demographic and Clinical Characteristics by GA Severity at Baseline |
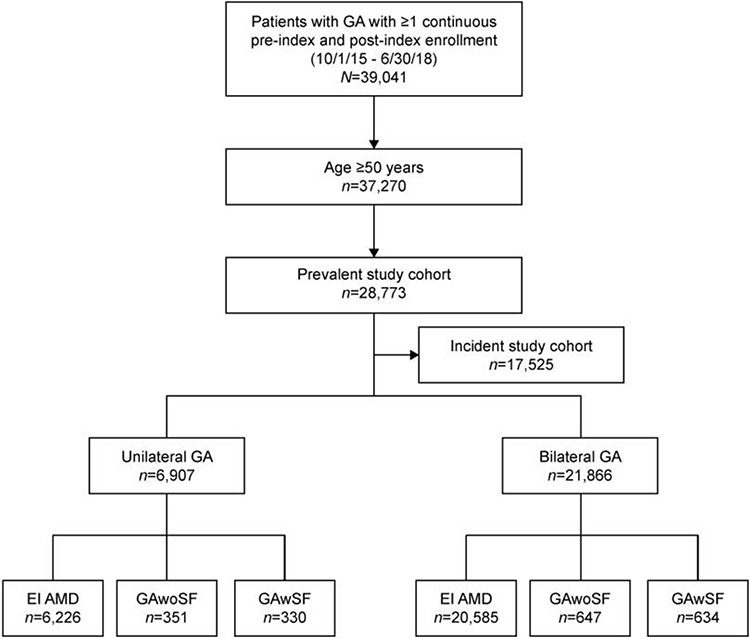 |
Figure 1 Flow chart of cohort identification. Abbreviations: EI AMD, early or intermediate AMD; GA, geographic atrophy; GAwoSF, geographic atrophy without subfoveal involvement; GAwSF, geographic atrophy with subfoveal involvement. |
Incidence and Prevalence of GA
The prevalence of GA was 2.88 cases per 10,000 individuals, and there were 1.75 new incident cases per 10,000 individuals in 1 year.
Health Care Resource Utilization
The mean number of GA-specific outpatient, emergency department, and inpatient visits in the 1-year follow-up period is shown across severity and laterality in Figure 2. Of note, approximately 83% and 9% of patients with GA were seen in the outpatient and inpatient setting, respectively. No emergency department claims specifying a GA diagnosis were reported.
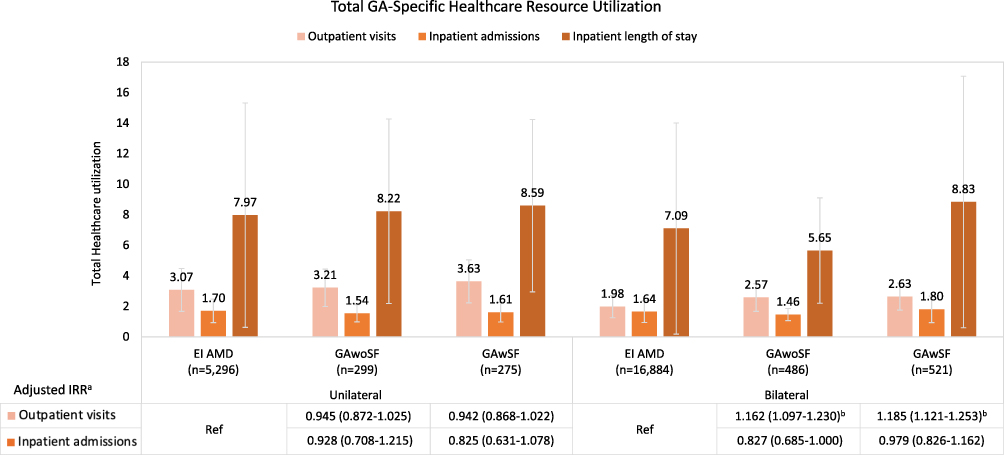 |
Figure 2 Total GA-Specific Healthcare Resource Utilization.Notes:aAdjusted for age, gender, region, insurance type, Charlson Comorbidity Index, and baseline comorbidities. bp<0.05, using “early/intermediate AMD” as the referent category. Abbreviations: EI AMD, early or intermediate AMD; GA, geographic atrophy; GAwoSF, geographic atrophy without subfoveal involvement; GAwSF, geographic atrophy with subfoveal involvement. |
Patients with bilateral GAwoSF and GAwSF had, on average, 2.57 and 2.63 outpatient visits per year, compared with 1.98 outpatient visits per year in patients with EI AMD. Results of the adjusted healthcare resource utilization from the negative binomial model, which computes inter-cohort differences as incident rate ratios, suggest that compared with those who have bilateral EI AMD, individuals with bilateral GAwoSF and GAwSF had a 16% higher rate of GA-specific outpatient visits (incident rate ratios 1.16 [95% confidence interval (CI) 1.10–1.23], p=0.001) and a 19% higher rate of GA-specific outpatient visits (incident rate ratios 1.19 [95% CI 1.12–1.25], p=0.001), respectively, after adjusting for baseline characteristics. No statistically significant differences were found in GA-specific inpatient visits or hospitalizations among patients with more severe unilateral and bilateral GA, when compared with those with EI AMD. Moreover, the interaction between disease severity and laterality with respect to healthcare resource utilization was not significant. The mean number of all-cause outpatient, emergency department, and inpatient visits are shown in Supplementary Table 2.
Total Cost of Care
The mean GA-specific healthcare costs by increasing severity and laterality across all healthcare settings are shown in Figure 3. In unilateral GA, the mean patient-related costs in the outpatient setting were significantly higher in patients with GAwSF compared to those with EI AMD ($30, [95% CI $4–$56], p=0.024), after adjusting for baseline characteristics and comorbidities. Similarly, in bilateral GA, the mean patient-related costs in the outpatient setting were significantly higher in patients with both GAwoSF ($13, [95% CI $3–$22], p=0.008) and GAwSF ($13, [95% CI $4–$22], p=0.007) compared to those with bilateral EI AMD, and the mean payer-related costs were higher in patients with GAwSF ($44, [95% CI $19–$69], p=0.001), compared to those with bilateral EI AMD.
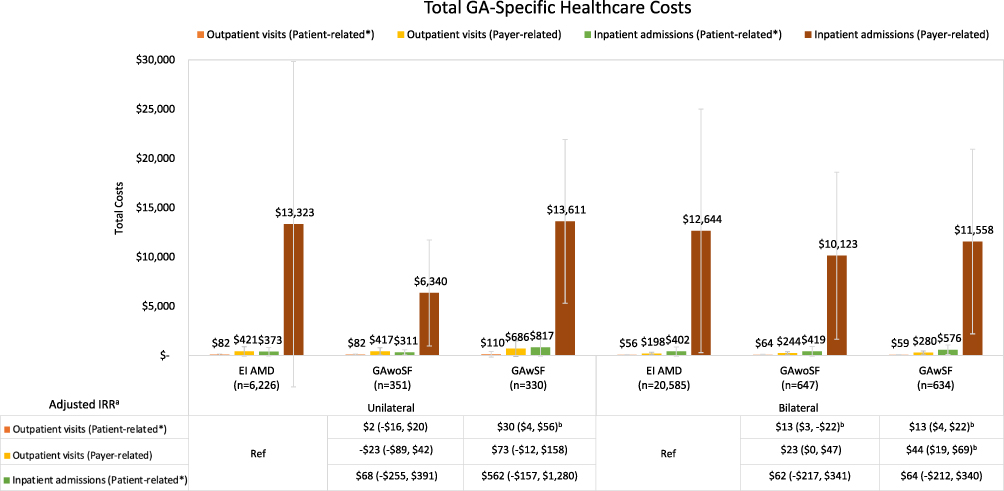 |
Figure 3 Total GA-Specific Healthcare Costs.Notes: Costs are shown in 2019 US dollars. *Patient-related costs include patient copay, coinsurance, deductible. aAdjusted for age, gender, region, insurance type, Charlson Comorbidity Index, and baseline comorbidities. bp<0.05, using “early/intermediate AMD” as the referent category. Abbreviations: EI AMD, early or intermediate AMD; GA, geographic atrophy; GAwoSF, geographic atrophy without subfoveal involvement; GAwSF, geographic atrophy with subfoveal involvement. |
For both unilateral and bilateral GA, no statistically significant differences were seen in the inpatient setting when comparing patients with more severe GA to those with EI AMD. In addition, after adjusting for all possible confounders, the interaction between disease severity and laterality with respect to costs was not significant. The mean all-cause healthcare costs are shown in Supplementary Table 2.
Discussion
This retrospective claims-based study evaluated the relationship between increasingly severe forms of GA and disease burden in a primarily commercially insured US population. The study findings provide insight into the economic dimensions of the recognized clinical unmet need.
Our study found that the vast majority of patients with GA was seen exclusively in the outpatient setting, which was expected, as there are no current treatments available for GA. Patients with more severe bilateral GA had more outpatient visits per year, at about 2.5 visits compared to 2 visits in those with less severe bilateral GA. This finding is significant, given the only treatment available is best supportive care, and the American Academy of Ophthalmology recommends follow-up at 6–24 months.23 In addition, we saw no GA-specific utilization of the emergency department and a small number of hospitalizations across all patients, the latter of which may result from comorbidities that are associated with older age and disease progression.
With respect to costs, we found that the mean GA-specific costs were higher in patients with more severe GA in the outpatient setting. Also, patients with unilateral GA had slightly higher mean costs than those in bilateral GA. Overall, however, the actual costs were not large, ranging from $56–$110, given that these were disease-specific, and not all-cause, costs and thus, we would be capturing outpatient visits that do not require any active therapy. Although the incidence of baseline exudative AMD was higher at 49.1% in patients with unilateral GA, compared with 7.4% in bilateral GA, and thus a higher proportion of unilateral patients would likely be treated with more costly anti-VEGF agents, we would not expect to see these costs reflected in the GA-specific costs.
There are very few studies that have examined the burden of GA or nonexudative AMD. One United Kingdom multicenter retrospective cohort study using an electronic medical record database suggested that high levels of visual impairment are associated with losses in mobility and independence in patients with bilateral GA, and patients with milder levels of impairment at the time of GA diagnosis have a high risk of vision loss over time.1 This study, however, did not compare patients by laterality but assessed disease-specific burden. Our findings are consistent with this study as we observed patients with milder disease at baseline to significantly use healthcare resource utilization over the follow-up period.
Furthermore, another retrospective study using Medicare claims data examined the cost of disease progression among individuals with AMD over time.15 Schmier et al defined disease progression as having an incident diagnosis of either exudative or non-exudative AMD. Patients with non-exudative AMD had annual Medicare ophthalmic expenditures that were at least 3 times higher than those without AMD, and those with exudative AMD had costs at least 5-fold more than those with non-exudative AMD. These findings are not comparable with those in our current study because patients with nonexudative AMD were compared to those without AMD and were not stratified further by severity.
Further research is warranted to assess outcomes in patients with bilateral but asymmetric disease, as well as specific drivers of healthcare resource utilization and costs. Also, it may be worth investigating the risk of falls and fractures in this population, given the literature surrounding the relationship between AMD and falls is scarce, as well as the advanced age of GA patients.
Strengths of this study include the use of real-world data to identify patients with differing severity and laterality levels of GA. This is the first study to profile the GA population in the US and assess the economic burden of GA. In addition, the PharMetrics Plus claims data provide visibility into the full 7-digit ICD-coding, which allows for clear distinction between patients who are unilaterally and bilaterally affected.
The results of this study should be interpreted cautiously due to several limitations. This study used claims data from a primarily commercial insurance database, despite the average age at baseline of 68.7. As such, the costs associated with GA may not fully be captured from this study.
Similarly, claims data is dependent on ICD coding, which can be highly variable and inconsistent. However, in addition to providing granular severity and laterality information for geographic atrophy, ICD-10 codes were used in this study based on existing literature and recommendations to identify patients with geographic atrophy. With regards to the different categories and groups included in this study, the American Academy of Ophthalmology published recommendations for ICD-10 coding in their Preferred Practice Patterns,8 and another study by Fleckenstein et al,6 relied heavily on specific ICD-10 codes to indicate the different severity levels of the disease. Codes pertaining to early/intermediate age-related macular degeneration and advanced dry age-related macular degeneration were explicitly indicated, including those for advanced atrophic age-related macular degeneration with and without subfoveal involvement.
Also, due the asymmetric nature of GA, the baseline severity level at first claim of GA diagnosis for bilateral patients was classified based on the more severe eye in this study, and all outcomes of interest were calculated as such. This is an area for future research to parse out the disease burden on an eye-level.
In regard to the process by which inpatient stays and costs were estimated, the method used to identify costs attributed to hospitalized patients was not standardized and clear in the IQVIA data, where inpatient claims were defined as those with a confinement number. If a patient was hospitalized following an emergency department visit, the emergency department visit would be bundled in and not appropriately separated, and the number of emergency department visits and associated emergency department costs may have been underrepresented. Furthermore, in both patients with unilateral and bilateral GA, 13,847 patients (96%) were classified as having early-intermediate AMD, whereas 574 patients (4%) had more severe forms of GA. Additionally, the 12-month follow-up period may not be long enough to observe changes in costs and outcomes with a slow progressing disease such as GA. The cross-sectional approach of the analysis did not capture those who progressed to more severe forms of GA and the associated healthcare resource utilization and costs associated with progression; however, in our follow-up analyses, we found only 4.8% of incident patients progressing during the follow-up period, thereby supporting the slow progressive nature of GA. Further work is warranted to identify and assess caregiver burden in patients with more severe GA, such as bilateral GAwoSF or GAwSF, who are highly reliant on vision rehabilitation services.
Conclusions
Patients identified as being diagnosed with GA have significantly higher healthcare resource utilization and costs in the first year after diagnosis. Future work, allowing for a longer-term follow-up period, using Medicare data is warranted to better understand the long-term economic burden of GA.
Abbreviations
AMD, age-related macular degeneration; CCI, Charlson Comorbidity Index; CI, confidence interval; CNV, choroidal neovascularization; EI AMD, early or intermediate AMD; GA, geographic atrophy; GAwoSF, geographic atrophy without subfoveal involvement; GAwSF, geographic atrophy with subfoveal involvement; HCRU, healthcare resource utilization; IRR, incident rate ratio; LOS, length of stay; NA, not applicable; SD, standard deviation; US, United States; VEGF, vascular endothelial growth factor.
Acknowledgments
Editorial assistance was provided to the authors by Evidence Scientific Solutions, Inc (Philadelphia, PA) and funded by AbbVie Inc. This study was presented as a virtual poster at the International Society for Pharmacoeconomics and Outcomes Research Meeting; May 18–20, 2020.
Author Contributions
All authors participated in the study conception and design of the study. CZ prepared the analytic data set. AK performed the data analysis and drafted the manuscript. All authors contributed to data interpretation, agreed to the target journal, and revised, critically reviewed, and approved the submission and resubmission versions of the manuscript. All authors also agreed to take responsibility and be accountable for the article contents.
Funding
This study was supported by a training grant to the University of Washington funded by Allergan (prior to its acquisition by AbbVie Inc.).
Disclosure
Dr. Bansal has no conflicts of interest. Dr. Devine has no conflicts of interest. Dr. Campbell, Dr. Shirneshan, and Changgeng Zhao are employees of AbbVie Inc. Dr. Kim was funded by the University of Washington CHOICE Institute Fellowship sponsored by Allergan, an AbbVie company. The authors report no other conflicts of interest in this work.
References
1. Chakravarthy U, Bailey CC, Johnston RL, et al. Characterizing disease burden and progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(6):842–849. doi:10.1016/j.ophtha.2017.11.036
2. Merck. Age-related macular degeneration. The Merck Manual. Available from: https://www.merckmanuals.com/professional/eye-disorders/retinal-disorders/age-related-macular-degeneration-amd-or-armd.
3. Hernández-Zimbrón LF, Zamora-Alvarado R, Ochoa-de la Paz L, et al. Age-related macular degeneration: new paradigms for treatment and management of AMD. Oxid Med Cell Longev. 2018;2018:8374647. doi:10.1155/2018/8374647
4. Lanchoney DM. A model of the incidence and consequences of choroidal neovascularization secondary to age-related macular degeneration. Comparative effects of current treatment and potential prophylaxis on visual outcomes in high-risk patients. Arch Ophthalmol. 1998;116(8):1045. doi:10.1001/archopht.116.8.1045
5. Sunness JS, Rubin GS, Zuckerbrod A, Applegate CA. Foveal-sparing scotomas in advanced dry age-related macular degeneration. J Vis Impair Blind. 2008;102(10):600–610. doi:10.1177/0145482x0810201004
6. Fleckenstein M, Mitchell P, Freund KB, et al. The progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(3):369–390. doi:10.1016/j.ophtha.2017.08.038
7. Sunness JS, Rubin GS, Applegate CA, et al. Visual function abnormalities and prognosis in eyes with age-related geographic atrophy of the macula and good visual acuity. Ophthalmology. 1997;104(10):1677–1691. doi:10.1016/s0161-6420(97)30079-7
8. American Academy of Ophthalmology. Retina/vitreous panel: preferred practice pattern guidelines: age-related macular degeneration; 2015. Available from: https://www.aao.org/preferred-practice-pattern/age-related-macular-degeneration-ppp.
9. Coleman AL, Yu F, Ensrud KE, et al. Impact of age-related macular degeneration on vision-specific quality of life: follow-up from the 10-year and 15-year visits of the Study of Osteoporotic Fractures. Am J Ophthalmol. 2010;150(5):683–691. doi:10.1016/j.ajo.2010.05.030
10. Xu K, Gupta V, Bae S, Sharma S. Metamorphopsia and vision-related quality of life among patients with age-related macular degeneration. Can J Ophthalmol. 2018;53(2):168–172. doi:10.1016/j.jcjo.2017.08.006
11. Sivaprasad S, Tschosik E, Kapre A, et al. Reliability and construct validity of the NEI VFQ-25 in a subset of patients with geographic atrophy from the Phase 2 Mahalo study. Am J Ophthalmol. 2018;190:1–8. doi:10.1016/j.ajo.2018.03.006
12. Kimel M, Leidy NK, Tschosik E, et al. Functional Reading Independence (FRI) Index: a new patient-reported outcome measure for patients with geographic atrophy. Invest Ophthalmol Vis Sci. 2017;57(14):6298. doi:10.1167/iovs.16-20361
13. Rovner BW, Casten RJ, Massof RW, Leiby BE, Tasman WS; Wills Eye A.M.D. Study. Psychological and cognitive determinants of vision function in age-related macular degeneration. Arch Ophthalmol. 2011;129(7):885–890. doi:10.1001/archophthalmol.2011.146
14. Woo SJ, Park KH, Ahn J, et al. Cognitive impairment in age-related macular degeneration and geographic atrophy. Ophthalmology. 2012;119(10):2094–2101. doi:10.1016/j.ophtha.2012.04.026
15. Schmier JK, Covert DW, Lau EC. Patterns and costs associated with progression of age-related macular degeneration. Am J Ophthalmol. 2012;154(4):675–681.e671. doi:10.1016/j.ajo.2012.04.017
16. U.S. Bureau of Labor Statistics. Medical care in U.S. city average, all urban consumers, not seasonally adjusted. Available from: https://data.bls.gov/timeseries/CUUR0000SAM?output_view=pct_12mths.
17. Deb P, Norton EC. Modeling health care expenditures and use. Annu Rev Public Health. 2018;39(1):489–505. doi:10.1146/annurev-publhealth-040617-013517
18. Mihaylova B, Briggs A, O’Hagan A, Thompson SG. Review of statistical methods for analysing healthcare resources and costs. Health Econ. 2011;20(8):897–916. doi:10.1002/hec.1653
19. Gray A, Clarke PM, Wolstenholme J. Applied Methods of Cost-Effectiveness Analysis in Health Care. Oxford, England: Oxford University Press; 2010.
20. Dodd S, Bassi A, Bodger K, Williamson P. A comparison of multivariable regression models to analyse cost data. J Eval Clin Pract. 2006;12(1):76–86. doi:10.1111/j.1365-2753.2006.00610.x
21. Manning WG, Mullahy J. Estimating log models: to transform or not to transform? J Health Econ. 2001;20(4):461–494. doi:10.1016/s0167-6296(01)00086-8
22. Basu A, Rathouz PJ. Estimating marginal and incremental effects on health outcomes using flexible link and variance function models. Biostatistics. 2004;6(1):93–109. doi:10.1093/biostatistics/kxh020
23. Flaxel CJ, Adelman RA, Bailey ST, et al. Age-related macular degeneration Preferred Practice Pattern®. Ophthalmology. 2020;127(1):P1–P65. doi:10.1016/j.ophtha.2019.09.024
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.