Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
Health status and lung function in the Swedish alpha 1-antitrypsin deficient cohort, identified by neonatal screening, at the age of 37-40 years
Authors Piitulainen E, Mostafavi B, Tanash HA
Received 20 August 2016
Accepted for publication 30 October 2016
Published 2 February 2017 Volume 2017:12 Pages 495—500
DOI https://doi.org/10.2147/COPD.S120241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Eeva Piitulainen, Behrouz Mostafavi, Hanan A Tanash
Department of Respiratory Medicine and Allergology, Skåne University Hospital, Lund University, Malmö, Sweden
Background: Severe alpha 1-antitrypsin (AAT) deficiency (genotype PiZZ) is a well-known risk factor for COPD. A cohort of PiZZ and PiSZ individuals was identified by the Swedish national neonatal AAT screening program in 1972–1974 and followed up regularly since birth. Our aim was to study the lung function, respiratory symptoms and health status at the age of 38 years in comparison with a random sample of control subjects selected from the population registry.
Methods: The study group included 120 PiZZ, 46 PiSZ and 164 control subjects (PiMM), who answered a questionnaire on smoking habits and symptoms and the Saint George Respiratory Questionnaire (SGRQ) on quality of life. A total of 89 PiZZ, 33 PiSZ and 92 PiMM subjects underwent spirometry.
Results: Four percent of the PiZZ, 2% of the PiSZ and 12% of the control subjects were current smokers (P=0.008), and 17% of the PiZZ, 9% of the PiSZ and 21% of the control subjects had stopped smoking. The PiZZ current smokers had a significantly higher (ie, poorer) median activity score according to the SGRQ than the PiZZ never-smokers (P=0.032). The PiMM current smokers had significantly higher activity score (P<0.001), symptom score (P<0.001), and total score (P=0.001) according to the SGRQ than the PiMM never-smokers. The PiZZ current smokers had a significantly lower postbronchodilator forced expiratory volume in 1 second (FEV1)% of predicted value (P=0.019) and FEV1/forced vital capacity (FVC) ratio (P=0.032) than the PiZZ never-smokers. The proportion of subjects with a FEV1/FVC ratio of <0.70, indicating COPD, was significantly higher in the PiZZ current smokers than in the PiZZ never-smokers (P=0.001). Among the PiSZ and PiMM subjects, the differences in lung function between the smoking subgroups were insignificant.
Conclusion: PiZZ current smokers were found to have signs of COPD before 40 years of age. Smoking is less common among the AAT-deficient subjects identified by neonatal screening than among their peers in the general population.
Keywords: alpha 1-antitrypsin deficiency, health status, lung function, COPD, screening, smoking
Introduction
Severe alpha 1-antitrypsin (AAT) deficiency (PiZZ) is a well-known risk factor for developing COPD and liver disease.1 Moderate AAT deficiency, PiSZ, is also considered a risk factor for the development of COPD in smokers. Despite the fact that this genetic codominant, autosomal disorder, characterized by low plasma levels of circulating AAT was discovered more than 50 years ago, its natural course has still not been elucidated.2
The Swedish national neonatal AAT screening study was carried out in 1972–1974, when all 200,000 newborn children were screened for AAT deficiency.3 A total of 127 PiZZ, 2 PiZ-null, 54 PiSZ and 1 PiS-null infants were identified. The cohort has been followed up frequently during infancy, then every second year up to the age of 18 years, and every fourth year in adulthood. A series of reports on the prospective follow-ups of the cohort have been published till their 34 years of age.4–9 Since the age of 30 years, a randomly selected, age-matched control group has been followed up in order to compare the results with the Swedish general population. Five PiZZ children and 1 PiSZ child died before the age of 8 years. During the follow-up, five new PiZZ individuals, born abroad during the screening period, have been identified and added to the cohort.8,9 Thus, the cohort still included 127 PiZZ and 2 PiZ-null subjects at the age of 34 years.
Our aim was to study the smoking habits, health status including respiratory symptoms, quality of life and lung function at the age of 38 years in the cohort of the AAT-deficient subjects identified by the Swedish neonatal screening program in comparison with an age-matched control group randomly selected from the population registry.
Subjects and methods
Study population
When the cohort population reached the age of 38 years, all 127 PiZZ, 2 PiZ-null, 53 PiSZ and 1 PiS-null individuals were invited to participate in a health checkup to assess their health status and lung function. The same randomly selected group of 300 individuals as in the 30-year and 34-year follow-ups identified from the Swedish population registry served as control group.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Regional Ethical Review Board of Lund, Sweden. All study participants gave their signed, informed consent.
Questionnaires
A questionnaire was sent to all study participants. It included questions on occupation, occupational exposure, smoking habits, respiratory symptoms and medication. A smoker was defined as a person having smoked at least one cigaret per day for 1 year. The following symptoms were included in the questionnaire: wheezing, cough with sputum production for at least 3 months over 2 consecutive years (ie, chronic bronchitis) and dyspnea when walking 100 m on level ground. The Medical Research Council (MRC) dyspnea scale was also included in the questionnaire. The disease-specific questionnaire on quality of life, the Saint George Respiratory Questionnaire (SGRQ), was also sent to the study participants.10
Spirometry and physical examination
All AAT-deficient individuals visited either their local hospitals or the Department of Respiratory Medicine, Malmö, Sweden. During their visit, spirometry was performed according to the European Respiratory Society/American Thoracic Society recommendations. A reversibility test 15 minutes after inhaling beta-2-agonist was requested. The results of the spirometry were expressed as a percentage of the European Respiratory Society reference values.11 The forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratios were presented as decimals. Postbronchodilator results of spirometry in the smoking subgroups were analyzed, because COPD is defined based on postbronchodilator values. Measurement of the fractional exhaled nitric oxide (FENO) level was requested.12 The results of spirometry, physical examination and diagnoses of respiratory and other diseases were reported by a study protocol. All control subjects performed spirometry and the FENO test at the Department of Respiratory Medicine, Malmö, Sweden.
Statistical analyses
Statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS version 22.0) software. Because of skewed distribution of the continuous variables, we used nonparametric tests (the Mann–Whitney U test and the Kruskal–Wallis test). Categorical values were analyzed by the χ2 test. The Pearson correlation coefficient was calculated to assess correlations. A P-value <0.05 was considered significant.
Results
Study population
Three PiSZ subjects and one PiZZ subject died before carrying out the checkup. A total of 120 PiZZ, 46 PiSZ and 164 control subjects answered the questionnaire. The demographic data of the study participants are presented in Table 1. The proportion of women was higher in the control group than in the AAT-deficient groups. Smoking was significantly more common among the control subjects than among the AAT-deficient subjects (P=0.008).
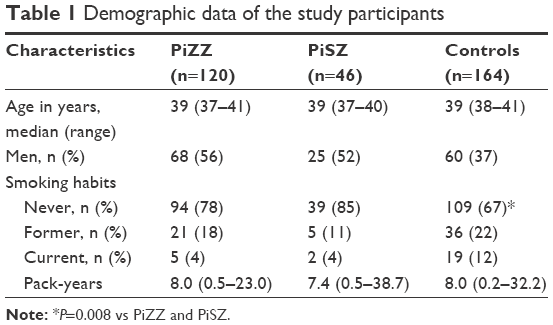 | Table 1 Demographic data of the study participants |
Spirometry
A total of 89 PiZZ, 33 PiSZ and 98 PiMM subjects underwent spirometry. The results for the Pi subgroups are shown in Table 2. No significant differences were found in FEV1 or FVC between the Pi subgroups. The postbronchodilator results of spirometry, stratified by smoking habits, are shown in Table 3. The PiZZ current smokers had a significantly lower postbronchodilator FEV1% of predicted value (P=0.019) and FEV1/FVC ratio (P=0.032) than the PiZZ never-smokers. The proportion of subjects with a FEV1/FVC ratio of <0.70, indicating COPD, was significantly higher among the PiZZ current smokers than among the PiZZ never-smokers (P=0.001). The results were similar when prebronchodilator values were analyzed (data not shown). The differences in the results of the pulmonary function tests among the corresponding smoking subgroups in the PiSZ and PiMM subjects were nonsignificant.
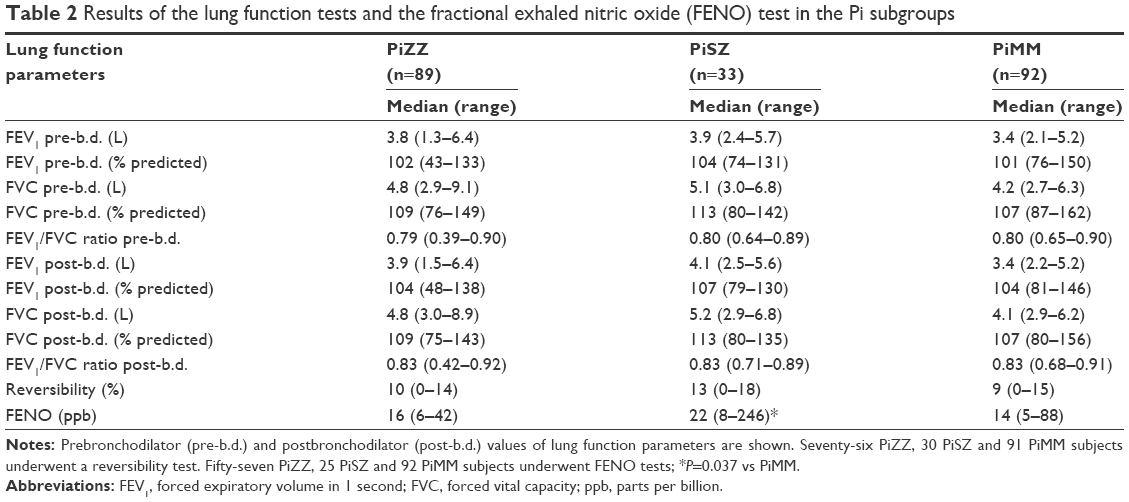 | Table 2 Results of the lung function tests and the fractional exhaled nitric oxide (FENO) test in the Pi subgroups |
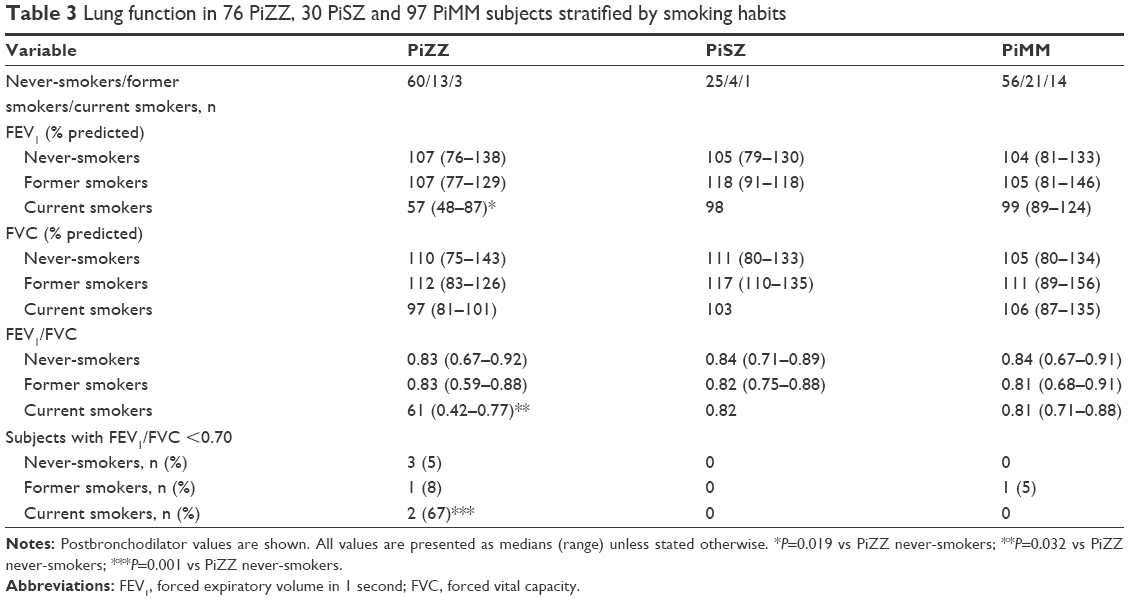 | Table 3 Lung function in 76 PiZZ, 30 PiSZ and 97 PiMM subjects stratified by smoking habits |
Occupational exposure
Forty-nine (42%) of 118 PiZZ, 15 (32%) of 47 PiSZ and 42 (26%) of 164 PiMM subjects reported occupational exposure to airway irritants (P=0.019). No significant differences in lung function tests were found between the subjects reporting occupational exposure to airway irritants and those not exposed.
FENO test
The amount of NO exhaled was analyzed in 57 PiZZ, 25 PiSZ and 92 PiMM subjects. The median amount of NO exhaled was significantly higher in the PiSZ subjects than in the control subjects (Table 2). Fourteen of the control subjects who underwent FENO test were current smokers. On excluding the current smokers from the analysis, the difference became insignificant.
Respiratory symptoms
No significant differences in respiratory symptoms were found among the Pi subgroups. The respiratory symptoms in the smoking subgroups are shown in Table 4. Recurrent wheezing was more prevalent among the PiZZ current smokers than among the PiZZ never-smokers and former smokers but the difference was not statistically significant. Chronic bronchitis was more prevalent among the PiSZ current smokers than among the PiSZ never-smokers and former smokers (P=0.042). Among the PiMM subjects, the current smokers reported significantly more recurrent wheezing than the never-smokers and former smokers (P=0.004; Table 4). The score of the MRC dyspnea scale was also higher (worse) among the PiMM current smokers than among the never-smokers (P=0.026; Table 5).
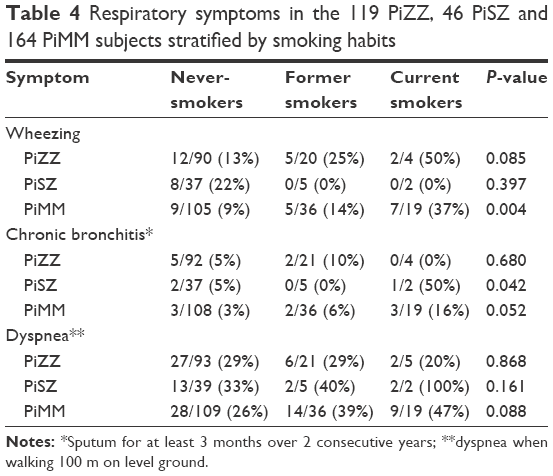 | Table 4 Respiratory symptoms in the 119 PiZZ, 46 PiSZ and 164 PiMM subjects stratified by smoking habits |
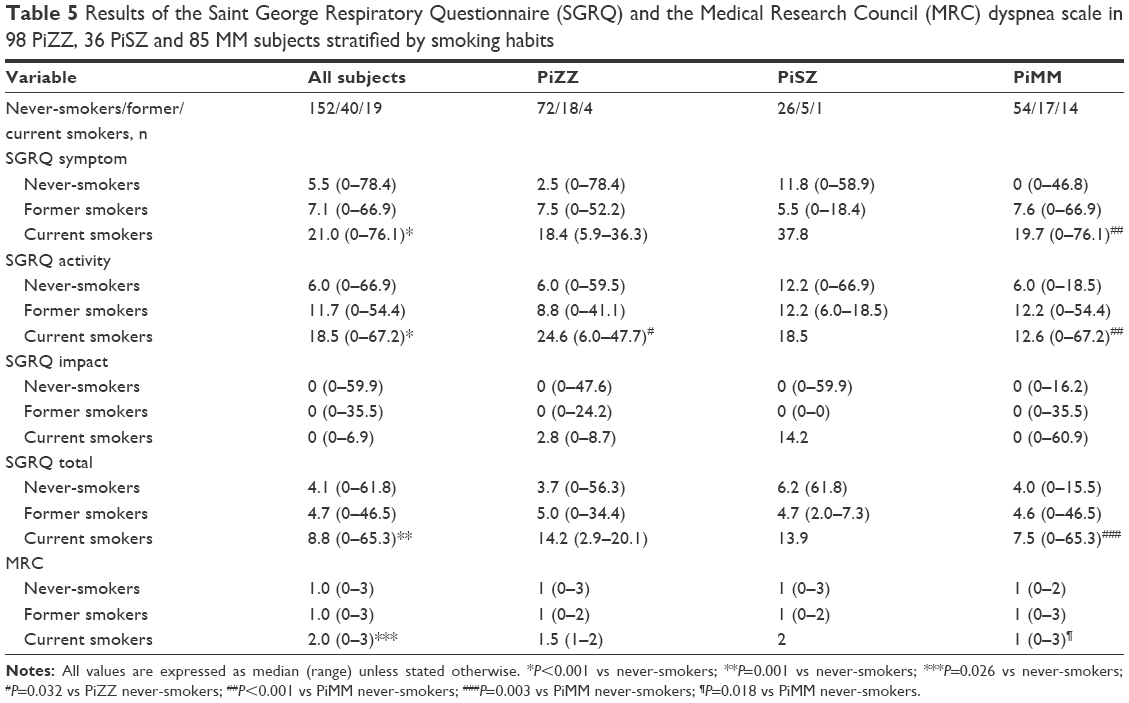 | Table 5 Results of the Saint George Respiratory Questionnaire (SGRQ) and the Medical Research Council (MRC) dyspnea scale in 98 PiZZ, 36 PiSZ and 85 MM subjects stratified by smoking habits |
Quality of life
The results of SGRQ in the smoking subgroups are shown in Table 5. When all study participants were analyzed together, the current smokers had, on SGRQ, a significantly higher, that is, poorer activity score (P<0.001), symptom score (P<0.001) and total score (P=0.001) than the never-smokers. The PiZZ current smokers had a significantly higher activity score than the PiZZ never-smokers (P=0.032). In the PiSZ subjects, no significant differences were found in SGRQ. The PiMM current smokers had a significantly higher activity score (P=0.005), symptom score (P=0.001) and total score (P=0.002) than the PiMM never-smokers.
Other diseases
The other diagnoses reported by the study participants are presented in Table 6. No significant differences were found in prevalence in the diagnoses among the Pi subgroups.
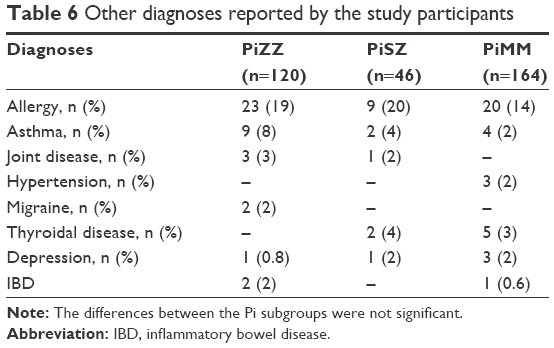 | Table 6 Other diagnoses reported by the study participants |
Discussion
Our results show that the majority of the PiZZ current smokers (2 of the 3 PiZZ current smokers) identified by screening at birth have COPD at the age of 37–40 years. In contrast, the PiMM subjects do not present the changes in lung function parameters indicating COPD. These results confirm that PiZZ individuals are more vulnerable to smoking than the general population.
The AAT-deficient subjects in this study form the only existing population-based cohort of PiZZ and PiSZ individuals, identified by a national neonatal screening, and were followed up since birth. Since the age of 30 years, the results have been compared with those of age-matched control subjects who were randomly selected from the population registry.8,9 At all health checkups, smoking was found to be less common among the AAT-deficient subjects than among the control subjects. The present checkup shows that at 37–40 years of age, smoking continues to be less common among the cohort than among the controls. This is probably due to the continuous antismoking campaign since childhood. The control subjects were identified at the age of 30 years, and they were personally counseled to stop smoking at the time of their participation in the checkups at the age of 30, 34 and 38 years.
Since the age of 34 years, the cohort and the controls have answered the SGRQ, which is a disease-specific questionnaire on quality of life. Similar to the results at the previous checkup, the smokers, independent of Pi group, had a significantly poorer quality of life than the never-smokers.9 Thus, in the general population, smoking has already a negative impact on the quality of life before the age of 40 years, and before the decrease in lung function occurs. The differences in quality of life between current and never-smokers were more apparent among the control subjects than among the AAT-deficient subjects, probably due to the insufficient power of the statistical analyses because of a small number of current smokers among the cohort. Furthermore, many of the AAT-deficient, former smokers had smoked only a few cigarets per day for a short time at a young age. This fact may also explain why no significant differences in lung function were found between the AAT-deficient never-smokers and former smokers. Our results show that antismoking campaign at an early age prevents the occurrence of respiratory symptoms and COPD in the AAT-deficient individuals. Therefore, one of the most important tasks is early identification of the deficiency state, possibly by screening before the age at which smoking is initiated, that is, in adolescence.
In contrast to the PiZZ subjects, no significant differences in lung function were found between the PiSZ smokers and the never-smokers. However, only one PiSZ current smoker underwent spirometry, and for this reason, no conclusions can be drawn from these results. Recently published data from the UK AAT-deficiency register have shown that PiSZ individuals are less susceptible to COPD than PiZZ subjects. They even found that PiSZ index cases have a similar phenotype of emphysema and bronchiectasis as COPD patients with the PiMM phenotype.13 However, no healthy controls from the general population were included in the study and, therefore, no conclusions can be drawn as to whether the PiSZ individuals have an increased risk of developing COPD.
The most important strength of our study is that we followed up only the existing cohort of AAT-deficient individuals, identified in a national neonatal screening program, which provided an opportunity to study the natural course of severe and moderate AAT deficiency. We thank the Swedish system of individual identification numbers; it helped us to know the vital status of all the subjects in the cohort and allowed us to follow the life expectancy of all subjects since birth.
Limitations
The most important limitation of our study is the fact that some AAT-deficient subjects did not participate in the follow-up pulmonary function tests. The most common reason for not participating was lack of time and well-being, that is, lack of symptoms. However, the participation rate of answering the questionnaire was high, more than 90%. The second limitation is the fact that the statistical analyses of this study were weak due to the small number of subjects, especially smokers, in the cohort.
Conclusion
In conclusion, we emphasize that the PiZZ current smokers already have symptoms of COPD at the age of 37–40 years, whereas the never-smoking PiZZ and PiSZ individuals have normal lung function.
Acknowledgments
The authors thank Ewa Ringdahl Szemberg, Isabella Björk and Helene Johansson Kvist for technical and secretarial support. The authors thank all Swedish colleagues for reporting data and Tomas Sveger for his contributions and for his help in improving this paper by providing appropriate criticisms. EP was supported by unrestricted grants from the Swedish Heart-Lung Foundation and Skåne University Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
Stoller JK, Aboussouan LS. A review of α1-antitrypsin deficiency. Am J Respir Crit Care Med. 2012;185(3):246–259. | ||
Laurell CB, Eriksson S. The electrophoretic α1-globulin pattern of serum in α1-antitrypsin deficiency. COPD. 2013;10(Suppl 1):3–8. | ||
Sveger T. Liver disease in α1-antitrypsin deficiency detected by screening of 200,000 infants. N Engl J Med. 1976;294(24):1316–1321. | ||
Sveger T, Piitulainen E, Arborelius M Jr. Lung function in adolescents with alpha1-antitrypsin deficiency. Acta Paediatr. 1994;83(11):1170–1173. | ||
Sveger T, Piitulainen E, Arborelius M Jr. α1-Antitrypsin deficiency: clinical features and lung function in 18-year-old adolescents with α1-antitrypsin deficiency. Acta Paediatr. 1995;84(7):815–816. | ||
Piitulainen E, Sveger T. Respiratory symptoms and lung function in young adults with severe α1-antitrypsin deficiency (PiZZ). Thorax. 2002;57(8):705–708. | ||
Piitulainen E, Carlson J, Ohlsson K, Sveger T. Alpha 1-antitrypsin deficiency in 26-year-old subjects. Lung, liver, and protease/protease inhibitor studies. Chest. 2005;128(4):2076–2081. | ||
Bernspång E, Sveger T, Piitulainen E. Respiratory symptoms and lung function in 30-year-old individuals with alpha-1-antitrypsin deficiency. Respir Med. 2007;101(9):1971–1976. | ||
Tanash HA, Nystedt-Düzakin M, Cano Montero L, Sveger T, Piitulainen E. The Swedish α1-antitrypsin screening study: health status, lung and liver function at age 34. Ann Am Thorac Soc. 2015;12(6):807–812. | ||
Jones PW, Quirk FH, Baveystock CM. The St George’s Respiratory Questionnaire. Respir Med. 1991;85 (Suppl B:25–31); discussion 33–37. | ||
Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J. 1993;6(Suppl 16):5–40. | ||
Turner S. Exhaled nitric oxide in the diagnosis and management of asthma. Curr Opin Allergy Clin Immunol. 2008;8(1):70–76. | ||
Green CE, Vayalapra S, Hampson JS, Mukherjee D, Stockley RA, Turner AM. PiSZ alpha-1 antitrypsin deficiency (AATD): pulmonary phenotype and prognosis relative to PiZZ AATD and PiMM phenotype. Thorax. 2015;70(10):939–945. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.