Back to Journals » Patient Preference and Adherence » Volume 19
Health-Related Quality of Life Among Patients Living with HIV/AIDS in Vietnam: A Cross-Sectional Study
Authors Vo LT, Nguyen PH, Nguyen HTN ![]() , Phan DQ, Vo XTT
, Phan DQ, Vo XTT ![]() , Vo LY, Nguyen YNT
, Vo LY, Nguyen YNT ![]() , Huynh G
, Huynh G ![]()
Received 24 December 2024
Accepted for publication 21 April 2025
Published 30 April 2025 Volume 2025:19 Pages 1197—1210
DOI https://doi.org/10.2147/PPA.S514101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Johnny Chen
Ly Trieu Vo,1 Phi Hoang Nguyen,2 Han Thi Ngoc Nguyen,3 Dung Quoc Phan,4 Xuan Thi Thanh Vo,1 Lan Y Vo,2 Yen Nhi Thi Nguyen,5 Giao Huynh2
1Infectious Disease E Department, Hospital for Tropical Diseases, Ho Chi Minh City, Vietnam; 2Faculty of Public Health, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 3Infection Control Department, University Medical Center Ho Chi Minh City, Ho Chi Minh City, Vietnam; 4Faculty of Control Disease, Health Center District 8, Ho Chi Minh City, Vietnam; 5Department of Obstetrics & Gynecology, Stanford University School of Medicine, Stanford, CA, USA
Correspondence: Giao Huynh, Faculty of Public Health, University of Medicine and Pharmacy at Ho Chi Minh City, 217 Hong Bang, District 5, Ho Chi Minh City, 700000, Vietnam, Tel +84 90 860 8338, Email [email protected]
Background: HIV/AIDS remains a major public health concern in Vietnam. While advancements in antiretroviral therapy (ART) have significantly enhanced survival rates and transformed HIV into a manageable chronic condition, the health-related quality of life (HRQL) of people living with HIV/AIDS (PLHA) often falls short of optimal levels.
Purpose: This study aims to evaluate the HRQL of HIV/AIDS outpatients at the Hospital for Tropical Diseases in Vietnam and identify key factors impacting their well-being.
Methods: A cross-sectional study was conducted among 328 PLHA receiving care at the Hospital for Tropical Diseases between March 2023 to March 2024. Data was collected using the World Health Organization Quality of Life-HIV Brief Version (WHOQOL-HIV BREF) instrument and included socio-demographic, clinical, and treatment-related variables. Descriptive statistics were utilized to summarize the data. Inferential statistical analyses, including independent t-test, one-way ANOVA, Kruskal–Wallis tests, and linear regression, were performed to evaluate the relationships between HRQL domains and participant characteristics. Statistical significance was set at p < 0.05.
Results: The mean overall quality of life score was 14.6 ± 2.2. The highest domain scores were observed in spirituality (15.1 ± 3.5) and environment (15.1 ± 2.9), while the lowest was in the physical domain (14.1 ± 2.0). Significant determinants of overall quality of life included age, marital status, employment type, income, financial difficulties, chronic diseases, and CD4 counts (all p < 0.05).
Conclusion: This study highlights the multifaceted challenges affecting the quality of life of PLHA, emphasizing the need for a holistic care approach. Being married, having stable employment, and having higher CD4 counts were associated with better quality of life, whereas older age, unstable income, financial struggles, and comorbidities were linked to poorer outcomes. Interventions addressing these determinants, including chronic disease management, social and mental health support are crucial for enhancing overall well-being.
Keywords: CD4 count, chronic disease, HIV/AIDS, health-related quality of life, WHOQOL-HIV BREF
Introduction
HIV/AIDS continues to be a global health issue that imposes considerable strain on public health systems and influences economic growth, cultural progress, and social stability. By the end of 2023, an estimated 39.9 million people were living with HIV worldwide, with 1.3 million new infections and 630,000 AIDS-related deaths reported that year.1 In Vietnam, 249,000 hIV infections have been documented since the first identified case in 1990, with 114,195 deaths attributed to the disease.2 In 2023 alone, Vietnam reported 6,883 new HIV cases and 1,260 AIDS-related deaths. These numbers reflect the ongoing challenges posed by this epidemic. In particular, infection rates are increasing among young populations and men who have sex with men, while stigma, and limited access to healthcare remain issues in these populations.2 In response, Vietnam has implemented national antiretroviral therapy guidelines aligned with World Health Organization recommendations, as outlined in the Ministry of Health’s 2021 guidelines. The preferred first-line ART regimen consists of tenofovir/lamivudine/dolutegravir (TDF/3TC/DTG) due to its high efficacy and tolerability, while second-line therapy includes protease inhibitors for cases of treatment resistance. Vietnam has made notable progress toward the UNAIDS 95–95-95 targets, with 88% of people living with HIV aware of their status, 80% receiving ART, and 98.3% achieving viral suppression by 2023.2 However, challenges remain in early diagnosis, timely treatment initiation, and retention in care. Addressing stigma, expanding community-based testing, and improving linkage to care will be essential for Vietnam to achieve the 95–95-95 goals.
Despite the severity of HIV/AIDS, the introduction of antiretroviral therapy has brought about significant improvements for PLHA. The chronic condition is increasingly manageable as ARV medications effectively suppress the progression and rapid transmission of HIV.1,3–5 As a result, people living with HIV/AIDS can now achieve a life expectancy that is comparable to that of the general population in many settings. However, this narrowing of the gap in life expectancy is not absolute, as disparities remain due to late diagnosis, limited access to healthcare services, socioeconomic inequalities, and the burden of chronic comorbidities.6,7 This shift has led to growing interest in factors beyond medical treatment, with health-related quality of life emerging as a major focus for researchers and healthcare providers in recent years.4
Quality of Life, as defined by the World Health Organization (WHO), refers to an individual’s perception of their position in life within the context of their culture, value systems, and in relation to their goals, expectations, standards, and concerns.6 When assessed in terms of health and illness, this concept reflects a patient’s subjective evaluation of how their condition and its treatment impact the physical, psychological, and social dimensions of their life.8–10 To evaluate HRQL in PLHA, various tools have been developed, including both generic and disease-specific instruments. Among the generic measures, the EuroQol 5 Dimensions (EQ-5D), the Short Form-36 (SF-36) Health Survey, and the World Health Organization Quality of Life-Brief Version (WHOQOL-BREF) are widely employed due to their ability to compare HRQL across different disease populations.11,12 However, these tools may lack the sensitivity required to detect nuances specific to HIV or its treatments. Conversely, HIV-specific tools, such as the WHOQOL-HIV BREF, are tailored to capture the unique experiences of PLHA.11
Previous research worldwide has identified numerous factors influencing the quality of life among PLHA. Socio-demographic variables such as gender, education, cultural beliefs, employment, income, smoking status, and social support from family and friends are commonly associated with quality of life outcomes.8 Among these factors, spirituality and religious practices play an increasingly significant role in Vietnam, where approximately 95% of the population engages in some form of faith, belief, or religious activity.13 The country’s spiritual landscape is characterized by a blend of Buddhism, Confucianism, Taoism, and folk beliefs with many individuals participating in spiritual practices without formally, affiliating with a special religion. Additionally, clinical determinants, including comorbidities, disease stage, CD4 count, and adherence to antiretroviral therapy, also affect quality of life.8,14 Despite extensive research, there remains no consensus on the primary determinants of quality of life for PLHA. Several studies have highlighted the low quality of life in Vietnam among PLHA.15–18 A recent meta-analysis by Thai et al reported that the quality of life scores of Vietnamese HIV/AIDS patients averaged 13.0 on the WHOQOL-BREF and 13.9 on the WHOQOL-HIV BREF.19 This population’s overall quality of life was estimated to range between 50% and 75%.19 Despite multiple studies conducted over the past decade, this meta-analysis reveals that the quality of life among PLHA in Vietnam has remained moderate, suggesting limited sustained improvement. To address this gap, this study provides an updated assessment of the quality of life among HIV-infected outpatients in recent years and supports ongoing efforts to improve their well-being. By using the WHOQOL-HIV BREF and a large sample from a major outpatient clinic in southern Vietnam, the study provides timely and context-specific evidence to support more effective, better patient-centered HIV care. The findings of this study offer important insights for developing targeted interventions to improve treatment outcomes and enhance the overall well-being of PLHA in Vietnam.
Materials and Methods
Study Design and Population
This cross-sectional study examines health-related quality of life among PLHA undergoing ART at the Infectious Disease E Department of the Hospital for Tropical Diseases (HTD) in Ho Chi Minh City, Vietnam, from March 2023 to March 2024. The hospital is a high-level tertiary referral hospital specializing in the diagnosis, treatment, counseling, and management of infectious diseases in southern Vietnam, especially PLHA. It is dedicated to providing long-term antiretroviral therapy for HIV/AIDS patients and manages an average of 40 to 60 cases daily and 800 to 1,000 cases annually.20
The sample size was calculated using the formula for estimating a mean,21 based on the following assumptions: a population standard deviation (σ) of the overall quality of life score of 2.1 as reported in prior research,22 a Z-score  of 1.96 corresponding to a Type I error (α) of 0.05 for a 95% confidence level, and an estimation error (d) of 0.3.17
of 1.96 corresponding to a Type I error (α) of 0.05 for a 95% confidence level, and an estimation error (d) of 0.3.17

Thus, the required sample size was rounded up to 189 participants to ensure adequate statistical power. However, to accommodate a 20% non-response rate, the total minimum sample size for the study was 237 participants. In practice, the study successfully recruited 328 eligible participants.
The inclusion criteria were 18 years or older at the start of the study and with a confirmed HIV diagnosis. Patients with significant cognitive impairments or reading comprehension difficulties were excluded.
Data Collection
A pretested, structured questionnaire was used to assess quality of life among study participants. The questionnaire consisted of three components: socio-demographic information, medical history, and the short version of the WHOQOL-HIV BREF instrument (Supplementary Figures 1 and 2). The Vietnamese version of the WHOQOL-HIV BREF, previously validated for use in Vietnam, was used for data collection.16,17,22 Socio-demographic data was collected through face-to-face interviews. Interviews were conducted in private counseling rooms to ensure patient confidentiality. Medical history data covered variables such as the duration of time elapsed since diagnosis, route of transmission, duration of ART, ART regimen (first-line regimen: INSTI-based therapy, specifically tenofovir/lamivudine/dolutegravir; second-line regimen: protease inhibitors (PI), including lopinavir/ritonavir (LPV/r) or lopinavir/ritonavir (ATV/r), in combination with nucleoside reverse transcriptase inhibitors (NRTIs); and third-line regimen: PIs such as LPV/r or darunavir/ritonavir (DRV/r), in combination with one to two NRTIs, with or without DTG),23 compliance with ART (evaluated by frequency and adherence to ARV intake in the past three months), smoking status, comorbidities, and CD4 count.
The WHOQOL-HIV BREF questionnaire includes 31 facets grouped into six domains: physical, psychological, level of independence, social relationships, environment, and spirituality/religion/personal beliefs.24 The first two items assess overall quality of life: Q1 evaluates the general perception of quality of life, while Q2 assesses overall health status. Participants were asked to reflect on their experiences over the past two weeks for their response. Most items were rated on a Likert scale, where 1 represents the lowest or most negative perception and 5 represents the highest or most positive perception. Six negatively phrased questions were reverse-scored before analysis. Domain scores were calculated by averaging the facet scores within each domain, multiplying the mean by four to align with the scoring system of the WHOQOL-100. This results in domain scores ranging from 4 (lowest quality of life) to 20 (highest quality of life).
Before the primary data collection, a pilot study was conducted with 20 patients to pretest the questionnaire and resolve any ambiguities or inconsistencies. The reliability of the instrument in this sample was confirmed with a high Cronbach’s α of 0.92, indicating high internal consistency.25
Data Management and Data Analysis
Analysis was done using Stata version 17.0. Descriptive statistics were used to analyze all variables. Categorical variables were reported as frequencies (percentages), while continuous variables were reported as means (± standard deviation). An independent t-test was used for dichotomous variables with homogeneous variances, while Welch’s t-test was used for dichotomous variables with heterogeneous variances. One-way ANOVA was used for nominal variables when the dependent variable was quantitative, normally distributed, and had homogeneous variance. When the dependent variable was quantitative but not normally distributed, the Kruskal–Wallis test was used instead. Linear regression analysis was conducted to assess the association between independent variables (year of birth, gender, residence, highest education level, marital status, occupation, stable income, religious affiliation, and family economic status, HIV infected time, HIV transmission route, duration of ART, forgotten to take any ART, smoking, any chronic disease, CD4 counts) and each quality of life domain and overall quality of life. All variables with a p-value < 0.2 from the univariate analysis were included in the model. A stepwise method was employed to select the final model. Multicollinearity among independent variables was assessed using the Variance Inflation Factor (VIF). A VIF value greater than 10 was considered indicative of high multicollinearity, while values below 5 were interpreted as negligible.26 Prior to conducting multivariable linear regression, all independent variables were tested for collinearity. When any variable exhibited substantial collinearity, it was considered for exclusion or further adjustment. In this study, no variable exceeded the acceptable VIF threshold. Statistical significance for the final model was determined at a p-value < 0.05 and a 95% confidence level for the adjusted coefficients.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of the Hospital for Tropical Diseases in Ho Chi Minh City, Vietnam (737/QĐ-BVBNĐ, 17 March, 2023). This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was secured from each participant after they were thoroughly informed about their rights and the study’s purpose and procedures. Participants were assured they could have a confidential discussion with the investigators regarding any concerns related to the study and were free to withdraw at any point without repercussions. Each participant was assigned a unique study code.
Results
During the study period, 328 eligible PLHA were included in the study. Table 1 provides an overview of sociodemographic and health-related characteristics. The majority of respondents were male (79%) and over 35 years old (60.7%). 41.8% of respondents reside in Ho Chi Minh City. 35.4% had completed secondary education, and 49.4% identified as single. Freelance work was the most common occupation (37.8%), and most participants reported having a stable income (78.7%). The majority of those surveyed (76.8%) did not identify with any religion, and 74.1% were not experiencing financial difficulties. When the participants were asked about their health status, 28% had been diagnosed with HIV within the past year, with unprotected sex being the primary mode of transmission (58.8%). Around one-third (36.6%) had been on ART for less than a year. Almost all participants were on a first-line ART regimen, took ART once daily, and reported no missed doses (99.7%, 99.4%, and 85.7%, respectively). Over half (54%) had CD4 levels of ≥ 500 cells/mm3, while only 17% had CD4 counts below 200 cells/mm3. Additionally, 19.5% of the participants were smokers, and 12.5% had any chronic disease.
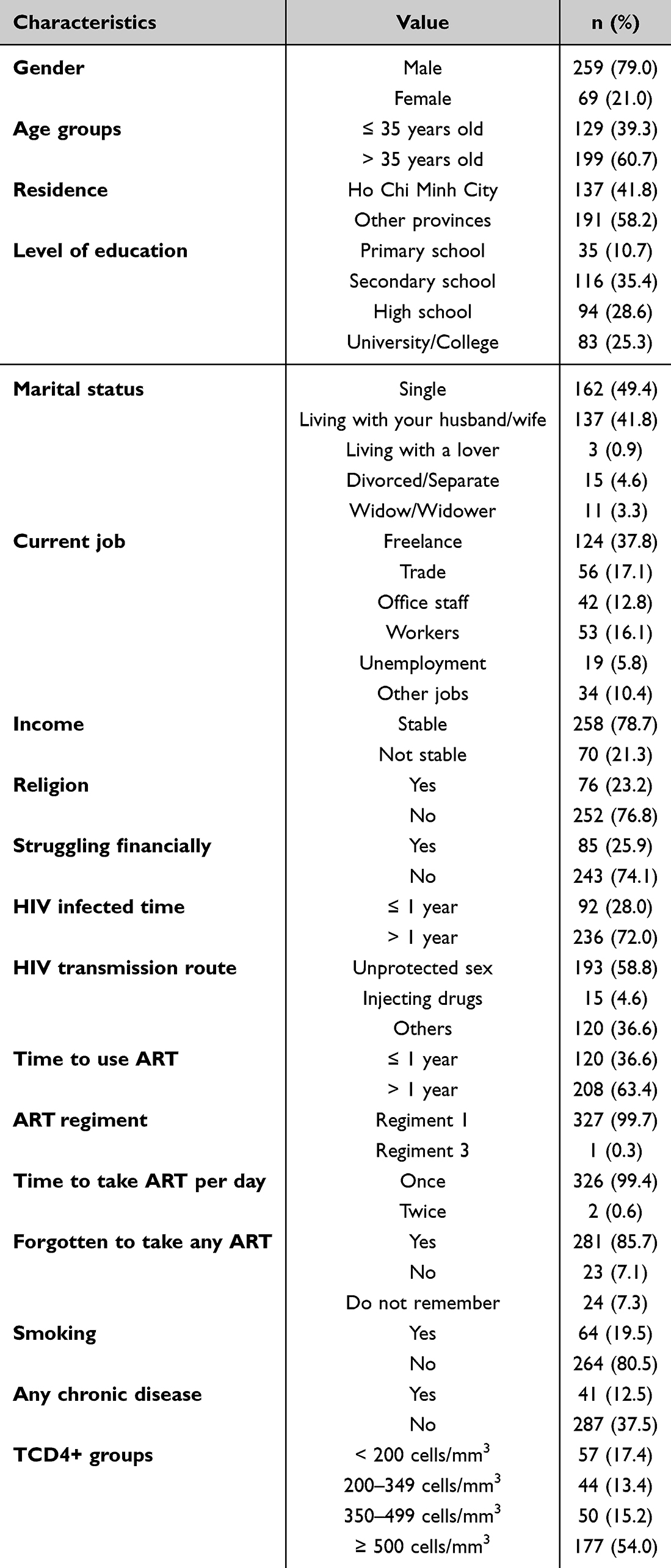 |
Table 1 Characteristics of the Participants (n = 328) |
The score distributions for each WHOQOL-HIV BREF item and domain are shown in Tables 2 and 3. The lowest individual item scores were symptoms of HIV (2.5 ± 1.0), dependence on medication (2.7 ± 1.2), and concentration ability (2.9 ± 1.1), while the highest scores were negative feelings (4.5 ± 0.8) and mobility (4.2 ± 1.0) (Table 2). As can be seen from Table 3, the overall mean score across all domains was 14.6 ± 2.2. The highest mean scores were observed in the spiritual (15.1 ± 3.5) and the environment domains (15.1 ± 2.9), whereas the physical domain had the lowest score (14.1 ± 2.0).
 |
Table 2 Descriptive Statistics of the WHOQOL-HIV BREF Facets (n = 328) |
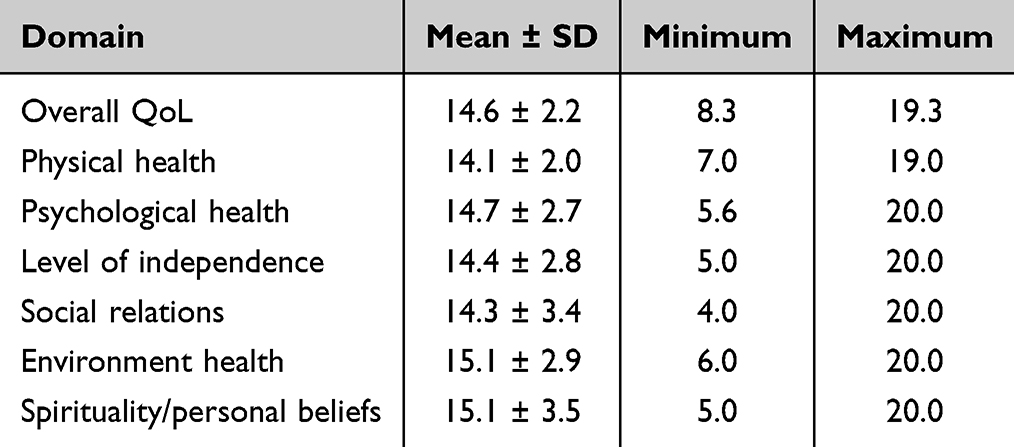 |
Table 3 Descriptive Statistics of the WHOQOL-HIV BREF Domains (n = 328) |
Table 4 summarizes the relationship between quality of life and participant characteristics. A significant association was found between age groups and several quality-of-life domains. Participants over the age of 35 had lower mean scores in the level of independence (p = 0.001), social relations (p = 0.002), environmental health (p = 0.004), and overall quality of life (p = 0.012) compared to those aged 35 and younger. A statistically significant difference was observed between spirituality domain and education level (p = 0.001). Participants living with their spouse had significantly higher mean scores in the psychological, level of independence, social, environmental domains, and overall quality of life compared to other groups (p < 0.05). Similarly, there was a significant difference between profession and the psychological health (p = 0.005), level of independence (p = 0.001), social (p = 0.006), environmental domains (p < 0.001), and overall quality of life (p < 0.001). Participants with stable incomes and those not experiencing financial difficulties had higher mean scores across all domains (p < 0.05). Significantly higher mean scores in psychological health (p = 0.017) and social relations (p = 0.011) were observed in participants without religious affiliation compared to those with religious affiliations. There was a strong association between spirituality (p = 0.030), overall quality of life (p = 0.035), and the time of HIV infection. Likewise, a statistically significant difference was found between physical health (p = 0.011), spirituality (p = 0.017), overall quality of life (p = 0.047), and the time of initiating ART (antiretroviral therapy). No significant differences were found between CD4 count groups and the quality-of-life domains. However, the relationship between CD4 count and the overall quality of life was statistically significant (p = 0.030). Participants who did not smoke showed higher mean scores in the level of independence (p = 0.047) and environmental domains (p = 0.016). Additionally, participants without chronic diseases had significantly higher mean scores across all domains compared to others (p < 0.05), except for the physical domain.
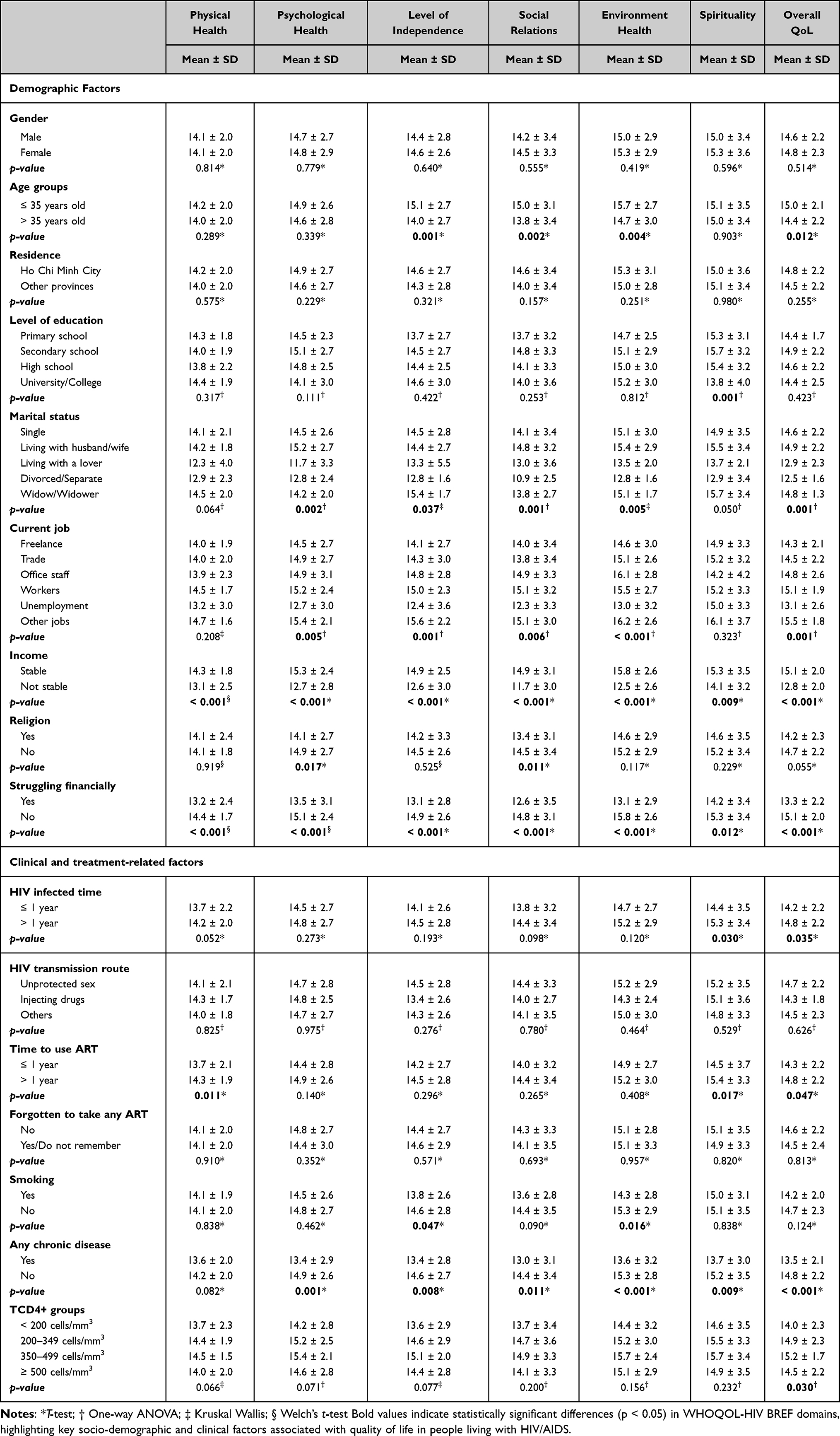 |
Table 4 Factors Related to the Domains of Quality of Life (n = 328) |
Table 5 shows the results of the multiple linear regression analysis and identifies independent predictors of overall quality of life, including age group, marital status, profession, income, financial difficulties, chronic diseases, and CD4 count group. The coefficients reported are unstandardized beta values. Participants over the age of 35 had an overall quality of life score 0.72 points lower than those aged 35 and younger (p = 0.005; 95% CI: 0.18–1.26). Those living with a spouse or who were widowed had an overall quality of life scores of 0.53 (p = 0.042; 95% CI: 0.02–1.05) and 1.56 (p = 0.014; 95% CI: 0.31–2.81) points higher, respectively, than single participants. In contrast, participants living with a partner had overall quality of life scores 2.29 points lower than singles. Participants in occupations outside identified job categories had an overall quality of life score of 0.82 points higher than freelancers (p = 0.029; 95% CI: 0.08–1.55). Those with unstable incomes had overall quality of life scores 1.39 points lower than others (p < 0.001; 95% CI: 0.75–2.02), while participants without financial difficulties had overall quality of life scores 0.96 points higher (p = 0.001; 95% CI: 0.41–1.51). Participants without chronic diseases had an overall quality of life score 0.73 points higher than those with chronic conditions. Additionally, participants in the 350–499 cells/mm³ CD4 group had an overall quality of life score 0.83 points higher than those in the < 200 cells/mm³ group (p = 0.030; 95% CI: 0.08–1.58).
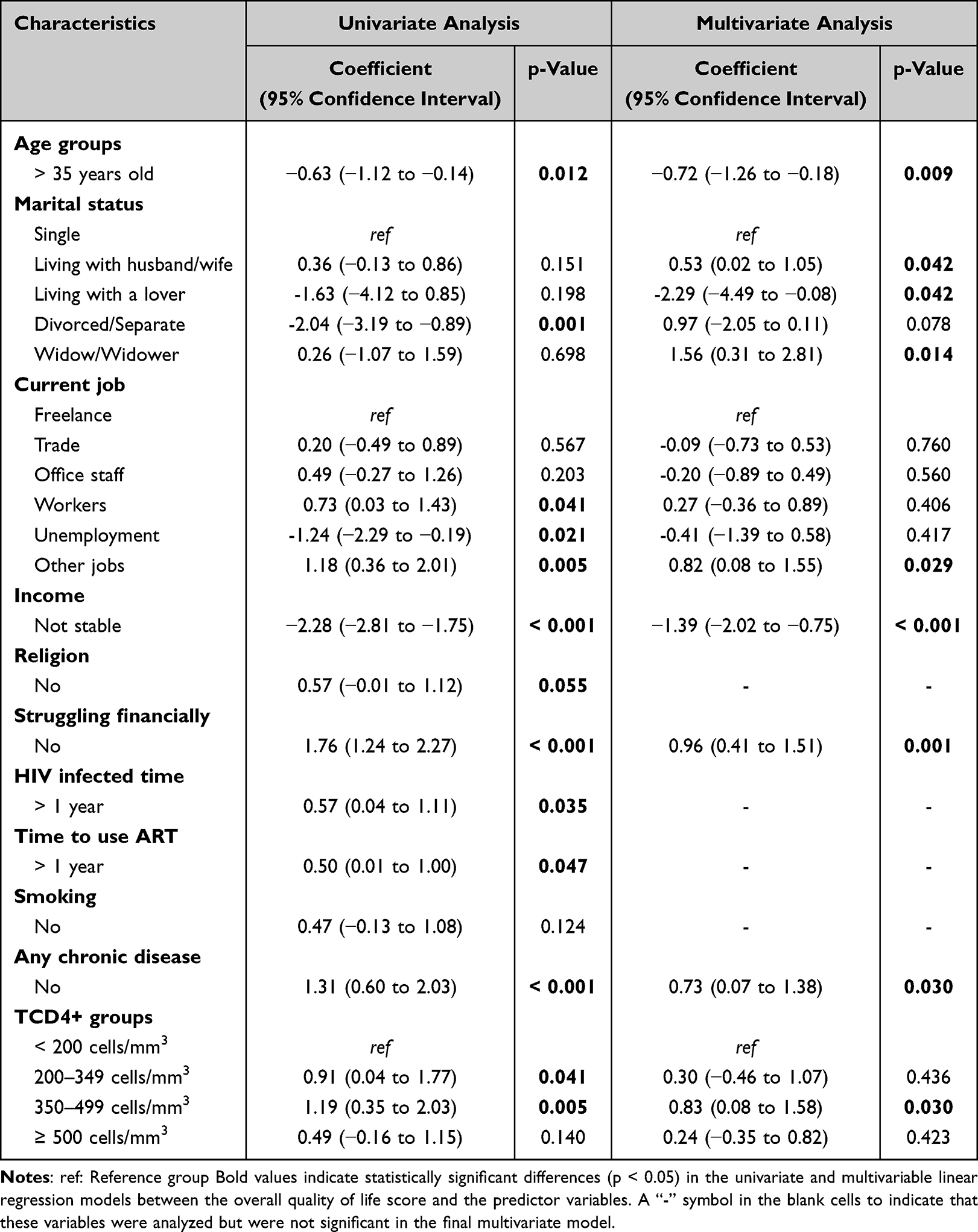 |
Table 5 Multiple Linear Regression Analysis of Overall Quality of Life and Participant Characteristics (n = 328) |
Discussion
This study showed that the mean total quality of life score was 14.6 ± 2.2. This result aligns with findings from Quach et al (2016), who reported a similar mean quality of life score of 14.0 ± 1.9 at the same facility in Vietnam.16 However, it exceeds the mean quality of life score of 12.2 ± 1.7; 12.9 ± 3.2; and 13.6 ± 2.1 reported by Nguyen et al (2016),17 Nguyen and Truong (2021),18 and Duong (2015),22 respectively, among PLHA in Vietnam. These discrepancies may arise from variations in sample demographics, methodological approaches, or improvements in HIV care and societal attitudes over the intervening years.
The assessment of quality of life among PLHA using the WHOQOL-HIV BREF revealed that the spirituality domain had the highest score in this study. This finding is consistent with previous studies conducted in Iran, France, and Burkina Faso.27–29 However, it contrasts with results from Quach et al (2016),16 and Nguyen et al (2016),17 which identified the physical domain as having the highest mean score. This discrepancy may be attributed to cultural and demographic factors specific to Vietnam. Spirituality is deeply integrated in Vietnamese society, with most of the population engaging in religious or spiritual practices with and without formal religious affiliation.13 This pattern is reflected in our study, where only 23.2% of participants reported having formal religious affiliation. A possible explanation for this may be the sex composition of our sample, in which 79% of participants were male. Prior research has suggested that men may be less likely to identify with formal religion while still engaging in spiritual practices such as meditation, mindfulness, or belief in a higher purpose.30 This may explain why participants scored highly in the spirituality domain despite the low reported rate of religious affiliation. Spirituality and personal beliefs are critical coping mechanisms for many individuals living with chronic illnesses, including HIV.31 Religious practices such as prayer can provide a sense of empowerment, reduce feelings of helplessness, and alleviate death anxiety, all of which help individuals feel more optimistic about the future.
Similarly, the environment domain scored highly in this study and surpassed previously reported values in Vietnam.16–18 Social development and improved public awareness have significantly enhanced the understanding of factors contributing to HIV transmission. This enhanced knowledge has helped alleviate stigma and overprotective attitudes toward PLHA, meaning that these individuals are better able to integrate into their communities and workplaces and experience less discrimination.32
The physical domain had the lowest mean score in this study. This finding aligns with the results of studies by Barger et al (2020),28 and Handayani et al (2019).32 However, it is lower than the scores reported by Quach et al (2016),16 and Nguyen et al (2021),18 but higher than those reported by Tran et al (2012),15 and Nguyen et al (2016).17 Several factors may account for the low physical domain score. First, the majority of participants in this study were older, with 60.7% being over 35 years old. Older age is typically associated with declining physical health due to natural aging processes.29 Second, while ART has significantly improved HIV management, it can cause side effects such as nausea, diarrhea, fatigue, and metabolic disturbances, which can negatively affect physical well-being and daily functioning.33 Third, HIV itself, along with its complications and comorbidities, particularly in cases of advanced disease or inconsistent treatment, can result in chronic fatigue, pain, and other physical symptoms that impair quality of life.34 This is further supported by the high mean score for the “pain and discomfort” facet in this study, which was 4.1 ± 1.1.
In the multivariate analysis by using linear regression, seven factors had an impact on the overall quality of life of PLHA (p < 0.05). The present study found a significant association between age and the quality of life among PLHA, consistent with findings from studies conducted globally.3,8 Participants over 35 years old were more likely to have lower quality of life compared to those aged 35 years and younger. As individuals age, they undergo natural physiological changes such as reduced immunity and diminished physical strength. They also experience increased vulnerability to comorbidities and opportunistic infections and are less adherent to treatment. These factors collectively contribute to a decline in quality of life.8
In this study, marital status had a statistically significant impact on overall quality of life, which was also reported by Khademi et al (2021),27 Handayani et al (2019),32 Nguyen et al (2016).17 Participants living with spouses reported higher quality of life scores compared to single individuals, aligning with previous research that associates marriage with improved quality of life. This can be explained by the consistent emotional, financial, and practical support provided by spouses, which alleviates stress and promotes better health outcomes. Such partnerships often enhance adherence to medical treatments and foster resilience when coping with chronic illnesses like HIV/AIDS, thereby reducing psychological distress and improving well-being.27 Interestingly, the study also found that respondents living with a partner (outside of marriage) had lower quality of life scores than single participants, while widowed individuals reported higher quality of life scores compared to singles. These results may reflect cultural and social dynamics, particularly in settings like Vietnam, where cohabiting relationships without formal marital status are often viewed as less stable or lacking legal and social recognition. As a result, individuals in such relationships may receive less formal support, both socially and institutionally, compared to their married counterparts. In contrast, previous studies have suggested that widowed individuals may develop greater emotional resilience over time as they adapt to the loss of a spouse through adaptive coping mechanisms and strong social networks.35,36 However, as this study did not collect qualitative data to explore the underlying mechanisms driving these findings, further research is needed to confirm these associations.
The findings of this study align with existing literature highlighting the influence of employment on the overall quality of life among PLHA. This finding reflects that of Rueda et al (2011),37 who also found that employment status was strongly related to quality of life, particularly in physical health outcomes. In this study, participants working as freelancers reported lower quality of life scores compared to those in other occupations. This may stem from the inherent challenges of freelance work, such as income fluctuations, which can heighten anxiety and hinder effective financial planning. These stressors are likely to contribute negatively to overall well-being. In our sample, a higher proportion of freelancers (29.0%) reported unstable income compared to traders (10.7%), office staff (4.8%), workers (13.2%), and individuals categorized under “other jobs” (17.6%). However, after adjusting for potential confounders in the multivariate analysis, no significant differences in overall quality of life were observed between freelancers and individuals in other employment categories, including trade, office staff, and workers (p > 0.05). The only group that demonstrated a statistically significant difference compared to freelancers was those categorized under “Other jobs” (p = 0.029). This suggests that while financial instability is more common among freelancers, its direct impact on quality of life may be influenced by additional factors not captured in this study, such as job flexibility, sense of autonomy, personal coping mechanisms, and access to social support. Moreover, previous research has suggested that the relationship between employment and health-related quality of life remains complex and likely bidirectional.37,38 While good HRQL may be necessary for maintaining employment based on the selection hypothesis, stable employment could enhance well-being by providing structure, financial security, and social interaction based on the causation hypothesis. Consequently, these findings should be interpreted cautiously.
In addition to employment, financial stability and individual income were significant determinants of quality of life in this study. Participants with stable incomes exhibited higher quality of life scores than those with unstable income. Similarly, those free from financial struggles had better quality of life scores compared to individuals facing financial hardships. These findings align with previous research, by Tran et al (2012),15 Quach et al (2016),16 Nguyen et al (2016),17 and Fuster-Ruiz de Apodaca et al (2019).39 Stable economic conditions enable individuals to meet basic needs essential for sustaining health and well-being, such as access to nutritious food and healthcare services.40 Conversely, financial instability often exacerbates stress, limits participation in social activities, and strains professional and personal relationships. These results highlight the importance of addressing socio-economic factors to enhance the quality of life among PLHA through targeted interventions and support systems.
The current investigation highlights the negative impact of comorbidities on the overall quality of life among PLHA. Patients with chronic diseases had significantly poorer quality of life compared to those without chronic conditions, consistent with findings from Nguyen et al (2016),17 and Ghiasvand et al (2019).14 The study of Barber et al (2023) further illustrated the cumulative effect of comorbidities, showing that individuals with three or more chronic conditions experienced significantly worse physical, psychological, social, and environmental quality of life, while those with two comorbidities reported declines in psychological and environmental quality of life.41 Non-communicable diseases (NCDs) present significant challenges in managing HIV. Treatments for NCDs alongside antiretroviral therapy increase the risk of polypharmacy-related complications, such as higher pill burden, drug-drug interactions, and adverse effects. These issues can exacerbate fatigue, pain, and adherence difficulties, potentially compromising virological control and worsening health outcomes. The findings underscore a critical concern for HIV care, as projections suggest that by 2030, 84% of PLHA will have at least one NCD, with 28% experiencing three or more. These trends threaten the physical, psychological, social, and environmental quality of life, emphasizing the urgent need for integrated care strategies.34
Regarding immunological status, Quach et al (2016),16 Tran et al (2012),15 Fuster-Ruiz de Apodaca et al (2019),39 and Ghiasvand et al (2019),14 have consistently shown that low CD4 counts are associated with diminished quality of life, particularly in physical health, functional abilities, and symptom management. This aligns with our findings, which revealed that participants with CD4 counts below 200 cells/mm³ had significantly lower overall quality of life scores compared to those in the 350–499 cells/mm³ group. CD4 counts is a critical marker of HIV progression, with levels below 200 cells/mm³ signifying advanced disease as defined by WHO.42 At this stage, individuals face a heightened risk of opportunistic infections and AIDS-related complications, which dramatically impact both physical health and psychological well-being. Interestingly, our study did not detect a significant difference in quality of life scores between participants with CD4 counts below 200 cells/mm³ and those above 500 cells/mm³. This unexpected result may stem from a phenomenon where individuals with higher CD4 counts perceive their health as less satisfying due to their heightened expectations of recovery and well-being.43 As such, despite their better clinical outcomes, these individuals might report lower subjective satisfaction with their health, resulting in a weaker association between high CD4 counts and perceived quality of life. Further investigation into patient perceptions and expectations is needed to better understand this paradox.
These findings highlighted that enhancing the quality of life for PLHA remains a priority in the development and implementation of comprehensive healthcare strategies. In addition to clinical management, social factors such as stable employment, financial security, and psychological well-being play critical roles in shaping health outcomes. Participants with stable income and those without financial difficulties reported significantly better quality of life across multiple domains, suggesting that economic interventions should be integrated into HIV care strategies. Such interventions may include vocational training programs, financial support initiatives, and improved access to medical assistance programs, health insurance, and hospital fee support for individuals facing economic hardship.
This study has several strengths. The high response rate and the absence of missing data in the regression analyses enhance the robustness of the findings. Furthermore, the use of an internationally recognized and validated instrument for measuring health-related quality of life in the Vietnamese context improved the reliability and comparability of the results.
However, there are also several limitations. As a cross-sectional design, it cannot capture longitudinal changes in quality of life related to adherence to antiretroviral therapy or other interventions over time. Additionally, as WHOQOL-HIV BREF assesses experiences over the past two weeks, the findings may be subject to recall bias, particularly for domains influenced by recent emotional or situational changes. Some key factors influencing quality of life, such as self-care practices, social support systems, and family involvement, were not examined in detail. Moreover, income stability and financial difficulties were self-reported and therefore subjective. Participants may have applied different personal thresholds or interpretations to these concepts, potentially introducing variability or bias in the analysis. Finally, as this study was conducted in a single tertiary hospital in southern Vietnam, the findings may not be fully generalizable to the broader population of people living with HIV/AIDS across the country. Future research should consider multi-center or population-based designs to improve the generalizability of findings.
Conclusion
Although the average overall quality of life score among participants was moderate, notable variations were observed across different domains. The highest scores were recorded in the spirituality and environmental domains, whereas the physical domain scored the lowest. Key socio-demographic and clinical determinants of quality of life include age, marital status, employment type, income stability, financial difficulties, the presence of chronic conditions, and CD4 count levels. Notably, our study population included both individuals living with HIV and those with AIDS. As expected, those with lower CD4 count, which is commonly associated with AIDS, tended to report poorer overall quality of life scores. These findings highlight the complex challenges faced by people living with HIV/AIDS and emphasize the importance of adopting comprehensive care strategies to improve their well-being. Comprehensive care strategies should integrate financial and employment support, psychological counseling, and social assistance to address the broader determinants of health. By incorporating these elements into HIV care, healthcare systems can enhance patient well-being and foster long-term improvements in quality of life.
Data Sharing Statement
Available upon request to the corresponding author.
Acknowledgments
The authors extend their gratitude to the healthcare workers at Hospital for Tropical Diseases in Ho Chi Minh City, particularly the Infectious Disease E Department, for facilitating data collection. We deeply appreciate the participation of all people living with HIV/AIDS who contributed their time and insights to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests.
References
1. Joint United Nations Programme on HIV/AIDS (UNAIDS). The urgency of now: AIDS at a crossroads. 2024.
2. Ministry of Health. National Plan for HIV/AIDS Prevention and Control. 2024.
3. Zhong H, Wei F, Song Y, Chen H, Ni Z. Health-related quality of life and associated factors among people living with HIV/AIDS in Sichuan, China: a cross-sectional study. Front Public Health. 2023;11:1133657. doi:10.3389/fpubh.2023.1133657
4. Garrido-Hernansaiz H, Heylen E, Bharat S, Ramakrishna J, Ekstrand ML. Stigmas, symptom severity and perceived social support predict quality of life for PLHIV in urban Indian context. Health Qual Life Outcomes. 2016;14(1):152. doi:10.1186/s12955-016-0556-x
5. Kanters S, Vitoria M, Doherty M, et al. Comparative efficacy and safety of first-line antiretroviral therapy for the treatment of HIV infection: a systematic review and network meta-analysis. Lancet HIV. 2016;3(11):e510–e520. doi:10.1016/s2352-3018(16)30091-1
6. Harris RM, Xavier Hall CD, Mills JC, Pence BW, Bgneris J, Wong FY. Beyond Viral Suppression-The Impact of Cumulative Violence on Health-Related Quality of Life Among a Cohort of Virally Suppressed Patients. J Acquired Immune Deficiency Syndromes. 2023;92(1):59–66. doi:10.1097/qai.0000000000003099
7. Lazarus JV, Safreed-Harmon K, Barton SE, et al. Beyond viral suppression of HIV - the new quality of life frontier. BMC Med. 2016;14(1):94. doi:10.1186/s12916-016-0640-4
8. Mohammed SA, Yitafr MG, Workneh BD, Hailu AD. Health-related quality of life and associated factors among people living with human immunodeficiency virus on highly active antiretroviral therapy in North East Ethiopia: cross-sectional study. PLoS One. 2021;16(3):e0247777. doi:10.1371/journal.pone.0247777
9. Dennison CR. The role of patient-reported outcomes in evaluating the quality of oncology care. Am J Manag Care. 2002;8(18 Suppl):S580–6.
10. Mengistu N, Hareru HE, Shumye S, et al. Health related quality of life and its association with social support among people living with HIV/AIDS receiving antiretroviral therapy in Ethiopia: a systematic review and meta-analysis. Health Qual Life Outcomes. 2022;20(1):77. doi:10.1186/s12955-022-01985-z
11. Cooper V, Clatworthy J, Harding R, Whetham J. Measuring quality of life among people living with HIV: a systematic review of reviews. Health Qual Life Outcomes. 2017;15(1):220. doi:10.1186/s12955-017-0778-6
12. Wen H, Yang Z, Han S, Zhang L, Hu Y, Hu Y. Psychometric properties of self-reported measures of health-related quality of life in people living with HIV: a systematic review. Health Qual Life Outcomes. 2022;20(1):5. doi:10.1186/s12955-021-01910-w
13. The Government Committee for Religious Affairs. Beliefs, Religions, and the Implementation of Policies and Laws on Beliefs and Religions in Vietnam. Available from:https://btgcp.gov.vn/.
14. Ghiasvand H, Waye KM, Noroozi M, Harouni GG, Armoon B, Bayani A. Clinical determinants associated with quality of life for people who live with HIV/AIDS: a Meta-analysis. BMC Health Serv Res. 2019;19(1):768. doi:10.1186/s12913-019-4659-z
15. Tran BX. Quality of life outcomes of antiretroviral treatment for HIV/AIDS patients in Vietnam. PLoS One. 2012;7(7):e41062. doi:10.1371/journal.pone.0041062
16. Quach TMP, Dang TTT, Nguyen HV, Truong TD, Cao NN, Huynh NVA. Quality of life of HIV/AIDS patients who were examined and treated in Hospital for Tropical Diseases in Ho Chi Minh City. Ho Chi Minh City J Med. 2016;20(1):299–305.
17. Nguyen TKT, Huynh NVA, To GK. Quality of life and association factors in people living with HIV/AIDS receiving Antiretrovirus in Center for HIV/AIDS prevention and control in Binh Phuoc Province. Ho Chi Minh City J Med. 2016;20(5):6–12.
18. Nguyen QA, Truong TC. Quality of life of HIV-infected people receiving ARV treatment in outpatient Clinic of Nha Trang Medical Center 2020 and some related factors. J Health Dev Stud. 2021;05(01):1.
19. Thai TT, Huynh NVA, Bui THH, Txu T. Quality of life in HIV/AIDS patients in Vietnam: findings from a meta-analysis. Ho Chi Minh City J Med. 2019;23(2):140–148.
20. Hospital for Tropical Diseases. Hospital Development Strategy to 2030 with a Vision to 2040. 2023.
21. Daniel WW, Cross CL. Biostatistics: A Foundation for Analysis in the Health Sciences.
22. Duong BV, Huynh NVA, To GK, Nguyen TPT. Quality of Life of HIV/AIDS Patients Treated ARV in District 11, Ho Chi Minh City. Ho Chi Minh City J Med. 2015;19(1):14–21.
23. Ministry of Health. Guideline for Treatment and Care of HIV/AIDS. Ministry of Health. 2021;2021:1.
24. Hiv Group W, WHOQOL HIV Group. WHOQOL-HIV for quality of life assessment among people living with HIV and AIDS: results from the field test. AIDS Care. 2004;16(7):882–889. doi:10.1080/09540120412331290194
25. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55. doi:10.5116/ijme.4dfb.8dfd
26. Kutner MH, Nachtsheim CJ, Neter J, Li W. Applied Linear Statistical Models.
27. Khademi N, Zanganeh A, Saeidi S, et al. Quality of life of HIV-infected individuals: insights from a study of patients in Kermanshah, Iran. BMC Infect Dis. 2021;21(1):203. doi:10.1186/s12879-021-05908-z
28. Barger D, Hessamfar M, Neau D, et al. Assessing the psychometric properties of the French WHOQOL-HIV BREF within the ANRS CO3 Aquitaine Cohort’s QuAliV ancillary study. Health Qual Life Outcomes. 2020;18(1):220. doi:10.1186/s12955-020-01451-8
29. Bakiono F, Ouédraogo L, Sanou M, et al. Quality of life in people living with HIV: a cross-sectional study in Ouagadougou, Burkina Faso. SpringerPlus. 2014;3(1):372. doi:10.1186/2193-1801-3-372
30. Pew Research Center. The Gender Gap in Religion Around the World. Pew Research Center. Available from:https://www.pewresearch.org/religion/2016/03/22/the-gender-gap-in-religion-around-the-world/.
31. Vance DE, Brennan M, Enah C, Smith GL, Kaur J. Religion, spirituality, and older adults with HIV: critical personal and social resources for an aging epidemic. Clin Interventions Aging. 2011;6:101–109. doi:10.2147/cia.S16349
32. Handayani S, Ratnasari NY, Husna PH, Marni Susanto T, Susanto T. Quality of Life People Living with HIV/AIDS and Its Characteristic from a VCT Centre in Indonesia. Ethiop J Health Sci. 2019;29(6):759–766. doi:10.4314/ejhs.v29i6.13
33. Oguntibeju OO. Quality of life of people living with HIV and AIDS and antiretroviral therapy. HIV/AIDS. 2012;4:117–124. doi:10.2147/hiv.S32321
34. Smit M, Brinkman K, Geerlings S, et al. Future challenges for clinical care of an ageing population infected with HIV: a modelling study. Lancet Infect Dis. 2015;15(7):810–818. doi:10.1016/s1473-3099(15)00056-0
35. Powers SM, Bisconti TL, Bergeman CS. Trajectories of social support and well-being across the first two years of widowhood. Death Studies. 2014;38(6–10):499–509. doi:10.1080/07481187.2013.846436
36. Kristiansen CB, Kjær JN, Hjorth P, Andersen K, Prina AM. The association of time since spousal loss and depression in widowhood: a systematic review and meta-analysis. Soc Psychiatry Psychiatr Epidemiol. 2019;54(7):781–792. doi:10.1007/s00127-019-01680-3
37. Rueda S, Raboud J, Mustard C, Bayoumi A, Lavis JN, Rourke SB. Employment status is associated with both physical and mental health quality of life in people living with HIV. AIDS Care Apr. 2011;23(4):435–443. doi:10.1080/09540121.2010.507952
38. Worthington C, Krentz HB. Socio-economic factors and health-related quality of life in adults living with HIV. Int J STD AIDS. 2005;16(9):608–614. doi:10.1258/0956462054944408
39. Fuster-RuizdeApodaca MJ, Laguía A, Safreed-Harmon K, Lazarus JV, Cenoz S, Del Amo J. Assessing quality of life in people with HIV in Spain: psychometric testing of the Spanish version of WHOQOL-HIV-BREF. Health Qual Life Outcomes. 2019;17(1):144. doi:10.1186/s12955-019-1208-8
40. Fauk NK, Gesesew HA, Mwanri L, Hawke K, Ward PR. Understanding the quality of life of people living with HIV in rural and urban areas in Indonesia. PLoS One. 2023;18(7):e0280087. doi:10.1371/journal.pone.0280087
41. Barger D, Hessamfar M, Neau D, et al. Factors associated with poorer quality of life in people living with HIV in southwestern France in 2018–2020 (ANRS CO3 AQUIVIH-NA cohort: quAliV study). Sci Rep. 2023;13(1):16535. doi:10.1038/s41598-023-43434-x
42. World Health Organization. Providing care to people with advanced HIV disease who are seriously ill: policy brief. 2023.
43. Degroote S, Vogelaers D, Vandijck DM. What determines health-related quality of life among people living with HIV: an updated review of the literature. Arch Public Health. 2014;72(1):40. doi:10.1186/2049-3258-72-40
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.