")
Back to Journals » Patient Preference and Adherence » Volume 15
Health-Related Perceptions of Older Adults/Patients with Degenerative Lumbar Diseases (ODLs) are associated with their Quality of Life: a Mixed-Methods Study
Authors Ruan Y, Chen W, Zhuang C, Lin H
Received 8 July 2021
Accepted for publication 24 September 2021
Published 8 October 2021 Volume 2021:15 Pages 2303—2311
DOI https://doi.org/10.2147/PPA.S328532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Yuhui Ruan,1 Weisin Chen,2 Chenyang Zhuang,2 Hong Lin2,3
1School of International and Public Affairs, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Department of Orthopaedic Surgery, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 3Institute of Medical Science Popularization, Fudan University, Shanghai, People’s Republic of China
Correspondence: Hong Lin
Department of Orthopaedic Surgery, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China
Tel +86 13636526656
Email [email protected]
Purpose: This study aimed to elucidate the quality of life of older adults/patients with degenerative lumbar diseases (ODLs) and analyse its association with some of their health-related perceptions.
Materials and Methods: This mixed-methods study consisted of a questionnaire survey and an in-depth interview, which was designed within this study. ODLs were recruited from January 12, 2017 to June 27, 2018. The independent sample t-test and grounded theory coding method were employed for data analysis.
Results: Of the 125 participants who returned valid questionnaires, 18 were included in the in-depth interviews. ODLs’ quality of life was associated with the following health-related perceptions: “life barriers”, “subjective health status”, and “treatment outcomes” across the domains of physiology, psychology, social relations, and environment.
Conclusion: Our findings indicate that ODLs’ quality of life is associated with their health-related perceptions. Thus, to improve older adults’ quality of life, more attention should be paid to enhancing non-medical factors such as their health-related perceptions.
Keywords: life barriers, subjective health status, treatment outcomes
Introduction
Degenerative lumbar diseases are “essential illnesses” that are associated with poorer quality of life (QOL) in the elderly.1,2 Many degenerative changes are found to be risk factors of their QOL, such as related changes in plain radiography, osteoporosis, muscle strength, and physical ability.3 Thus, surgery-related factors are emphasized in major biomedical reports as the key points of improving their QOL.4,5 But social risk determinants, such as perceived social support and level of education,6,7 have been proved as predictors of elderly patient’s QOL in some studies. Thus, this study was designed to examine the relationship of some social risk determinants and QOL of the older adults/patients with degenerative lumbar diseases (ODLs).
Generally, degenerative lumbar diseases are associated with severe pain and difficulties in activities of daily living.8 They often result in disability and even death for affected patients.9 Thus, increasing awareness regarding degenerative lumbar diseases and its effects on the QOL of ODLs has become necessary for current public healthcare systems.10 It is also desirable for patients to understand the relationship of their QOL (including regarding postoperative complications, pain, timed up and go, sit-to-stand, daily life, etc.) with some health-related perceptions, to foster health-promoting behaviours.11
To date, there is limited information about these diseases. The primary prevention and treatment of degenerative lumbar diseases remain difficult. However, as a key part of the spine, the lumbar is essential for many activities. Thus, the patient’s QOL is greatly impacted by related diseases. Generally, with increasing age, the lumbar ages too.12,13 Related symptoms, such as pain, numbness, sensory disturbance, and dyskinesia, can result in great difficulty for patients, especially older adults.
A few non-biomedical studies of pain, appetite, fatigue, and confidence reported that patients’ health-related perceptions might be an important indicator of their health-related behaviours and that these perceptions are associated with their QOL.14–17 Many patients’ health information is influenced by related perceptions that are important for the way they feel in daily life. Patients’ QOL is impacted during their activities, emotional states, and important decision-making processes. For example, pain is one of the most common factors that trigger individuals, especially older adults, to perceive an illness and seek health services.18 Furthermore, fatigue is considered a health risk factor because it correlates with depression symptoms in patients, which in turn can affect their health-related QOL.17 Besides, low self-confidence or self-esteem are strongly associated with patients’ QOL.19 Race, genes, age, gender, and some unhealthy lifestyle or habits are also important factors associated with the QOL of patients with degenerative lumbar diseases.20–22
Although the current body of evidence suggests an association between patients’ QOL and certain genetic or environmental factors, limited studies have focused on the relationship between ODLs’ health-related perceptions and their QOL. An understanding of the relationship between ODLs’ health-related perceptions and their QOL is meaningful. Thus, this study aimed to explore ODLs’ QOL across the domains of physiology, psychology, social relations, and environment, to determine related relationships.
Materials and Methods
Study Design
A mixed-methods study, combining both quantitative and qualitative processes, was designed. This was a two-stage process, conducted through a questionnaire survey and an in-depth interview (Figure 1). Participants in the first stage were recruited through convenience sampling and they completed the questionnaire either independently or with the help of researchers who interpreted the questions. Subsequently, based on the information provided by the participants, some ODLs from the first stage were selected and invited to participate in the in-depth interview in the second stage. Although these two stages were designed to overlap, the second stage started in the second half of the questionnaire survey period. Generally, with the ongoing questionnaire survey process, a trend was gradually identified in this study that “perceived life barriers”, “subjective health status”, and “corresponding treatment outcomes” showed some association with ODLs’ QOL. Further, this study designed the open questions and recruited related participants for the in-depth interviews (stage 2) during a later questionnaire survey process (stage 1). When the participants were obtained for interviews, stage 2 was initiated immediately. Meanwhile, new participants for stage 1 continued to be recruited.
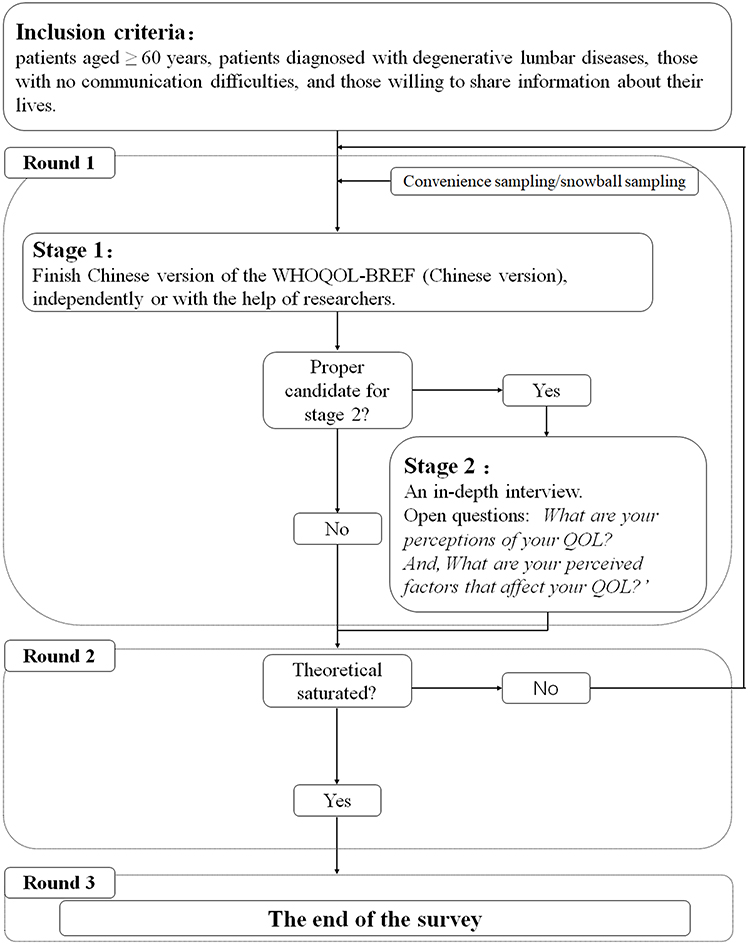 |
Figure 1 Study design. |
Inclusion Criteria
The inclusion criteria for the study participants were: patients aged ≥ 60 years; patients diagnosed with degenerative lumbar diseases including degenerative lumbar spinal stenosis, lumbar disc herniation, and degenerative lumbar spondylolisthesis using clinical and radiological evidence; those with low back pain history for over three months; those with no communication difficulties; and those willing to share information about their lives. All potential participants were briefed on the study aims before they decided to participate, and their consent was obtained.
Sampling of Participants
Sampling Process
Participants were recruited from the hospitalized patients receiving conservative treatments including physiotherapy and drug medications at the Department of Orthopaedic Surgery and “blinded for review” by the researchers through face-to-face communication (patients who received surgery were not included). Questionnaires with >20% questions unanswered were excluded. When less than two questions were unanswered in one of three domains (physiology, psychology, and environment), the missing scores were replaced by the average score of related domains. However, if more than two questions were unanswered in one domain, the score of the related domain was omitted (for the “social relations” field, only one question could be left unanswered). After excluding 14 questionnaires with missing data, 125 valid questionnaires were analysed from January 12, 2017 to June 27, 2018. Of the 125 participants, finally, 18 of them were invited and participated in in-depth interviews. Participants who were included in stage 2 were designated with an anonymized code.
Questionnaire Survey in Stage 1
The World Health Organization’s Quality of Life Instrument-Short Version (WHOQOL-BREF) is a simplified version of the WHO Quality of Life-100 (WHOQOL-100).23 The comprehensiveness of the WHOQOL-100 is retained by the WHOQOL-BREF. At least one question in each domain related to QOL and the most general question in each domain (ie, the ones with the highest correlation with the total score) were included. The Chinese version of the WHOQOL-BREF, which was used in this study, has been used extensively for its excellent reliability and validity.24,25
The WHOQOL-BREF comprises 26 questions, rated on a five-point Likert scale from 1 to 5 (the degree of positivity increased with the ratings from 1 to 5). The total scores were calculated for each domain, and higher scores indicated higher QOL.
Further, based on the results of literature analysis and two rounds of expert consultation (six scholars in related fields, as well as seven chief doctors of orthopedic departments of tertiary hospitals were involved), three other questions were added to this survey. Participants used a five-point scale to rate the themes on “life barriers”, “subjective health status”, and “treatment outcomes”. Barriers study is essential to supporting the QOL of patients.26 As the result of expert consultation, also as reported in many studies, patients’ QOL is affected by various life barriers, including environment-related,27,28 physical activity-related,29 and other practical barriers.30 QOL and health status are considered the most important aspects for patients. Self-perceived health status is empirically estimated as the way health to affect QOL.31 Treatment outcomes also showed a strong association with the QOL of the elderly32 Thus, three related questions were added to study their influence on ODLs’ QOL. As designed, lower scores indicated positive health-related perceptions (fewer barriers, feeling healthy, satisfied with treatment outcomes), while higher scores indicated negative feelings (several barriers, feeling unhealthy, unsatisfied with treatment outcomes). ODLs who rated the items “1”, “2”, or “3” were categorised into the “positive” group, while those who rated the items “4” or “5” were categorised into the “negative” group.
Data on participants’ demographic characteristics were also collected; these included age, gender, native place, address, education level, marital status, occupation, and living arrangements. The independent sample t-test using STATA 10.0 was performed to assess the factors associated with the QOL of ODLs.
In-Depth Interviews
As previously noted, a total of 18 participants were included in the in-depth interviews, and data were gathered until data saturation was reached. Each participant was briefed on the study aims before they decided to engage.
The grounded theory coding method was employed for the qualitative analysis in this study,33–35 similar to our previous study.36 By comparing, memo-writing, and immediate data analysis, themes were explicated and analysed from interviews until saturation was reached.37 In this study, data saturation was defined as a point when data from participants no longer revealed new information on the existing theoretical categories extracted from related processes.38 The length of the in-depth interviews was flexible, varying from 30 to 60 minutes.
Two open questions were asked: “What are your perceptions of your QOL?” and “What do you think have affected your QOL?” A series of relevant probe questions on “life barriers”, “health status”, and “treatment outcomes” were also included.
In principle, this study employed the combination coding method, including both line-by-line coding, and sentence-by-sentence coding. In some conditions, integrated coding for sentences or even paragraphs with similar or related meanings was allowed. Special consideration was given to some sensitive actions, events, and processes, especially the observed “vivid” words. Then, the abstract concepts in the conceptual level were extracted (codes). The codes were fixed, integrated, and even traded offs with the supplement of the follow-up material. After repeated deliberations and comparisons, the final codes were obtained. Subsequently, a series of initial codes and focused codes were generated. The relationship of ODLs’ health-related perceptions with their QOL was studied.
Results
A total of 125 valid questionnaires were collected from participants (Table 1), including 45 (36.0%) male and 80 (64.0%) female participants. Many of them had degenerative lumbar diseases for more than 10 years.
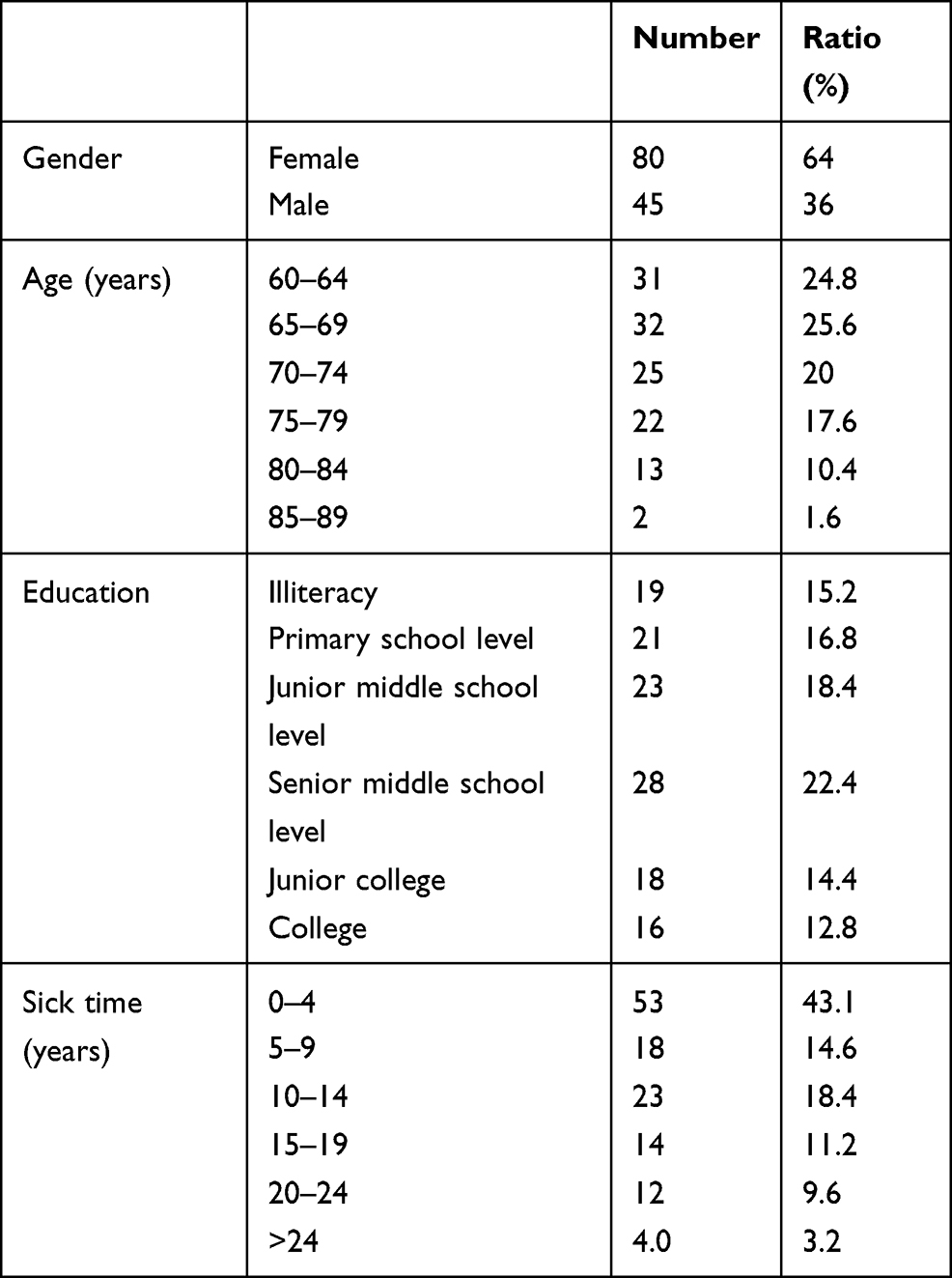 |
Table 1 Socio-Demographic Information of the Participants |
ODLs’ QOL and Associated Factors
All ODLs were required to evaluate their related health status in the preceding two weeks. The mean QOL scores on the four domains were 11.02±2.44 for physiology, 13.09±2.16 for psychology, 14.66±2.59 for social relations, and 6.27±1.07 for environment.
ODLs’ QOL was significantly associated with their perceived “life barriers” (Table 2). ODLs with lower scores on “life barriers” also reported better QOL on physiology, psychology, and social domains than those with higher scores (p<0.05). But this association was not significant in the environment domain (p=0.051, p<0.10).
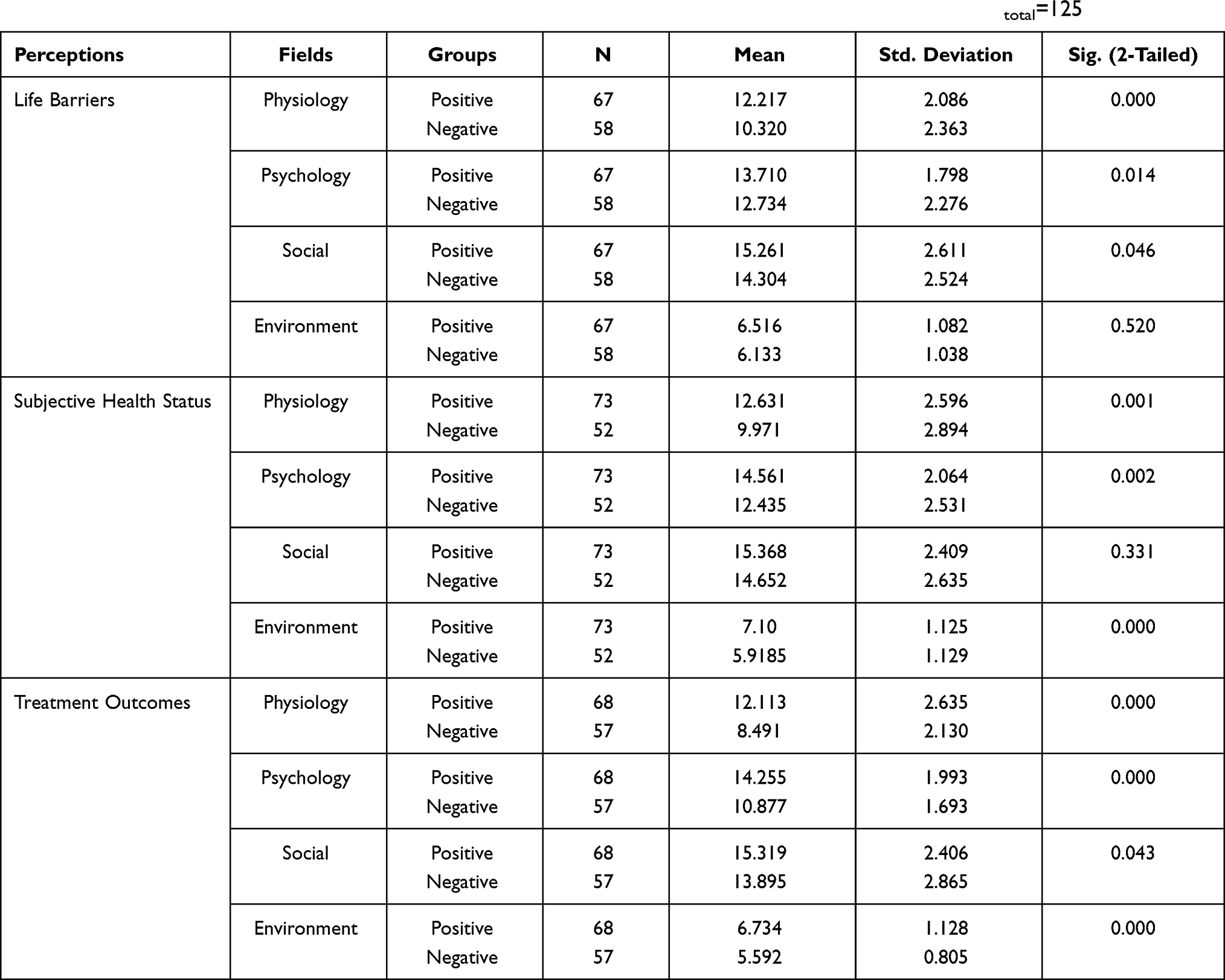 |
Table 2 Independent Sample t-Test Results of ODLSs’ QOL with Perceptions (95% Confidence Interval), Ntotal=125 |
Likewise, ODLs with higher scores on “subjective health status” reported a significantly worse QOL in physiology, psychology, and environment domains (p<0.05; Table 2). Meanwhile, those who reported lower scores on “treatment outcomes” showed significantly better QOL scores in all four domains (p<0.05) (Table 2).
Association of ODLs’ QOL with Perceived Factors
ODLs’ QOL was associated with perceived “life barriers”, “subjective health status”, and “treatment outcomes”.
Perceived “Life Barriers”
Identifying the main life barriers and their underlying mechanisms are important, which can affect patients’ perceptions of difficulties in daily life and in turn affect their QOL. The life barriers that were mentioned the most in this study were summarised as “physical pain/discomfort”, “inconvenience related to self-care/work/family-life”, “economic burden”, and “mental pressure”, among others.
Except for wasting money on medicine, extra help from others is needed when performing heavy labour work. Thus, it is difficult for me to take part in family outings because it is inconvenient. Such life barriers remind me that I am a useless person who always brings trouble to others. (97-11-L)
ODLs who reported more “life barriers” were more easily unmotivated about various aspects of their daily life, such as “daily activities”, “working”, “providing intergenerational support to their children”, and “interaction between friends”. There was a higher possibility of encountering difficulties in related processes. Such life barriers can result in mixed results that covered more than one of the four mentioned fields.
No mention about going out for work; even helping to take care of my granddaughter or serving myself was difficult. Though others never complain about my uselessness, I am unsatisfied with myself. (49-6-M)
My interactions with friends have been decreasing greatly since my degenerative lumbar disease worsened. (65-8-X)
Life barriers can impede ODLs’ ability to take care of themselves and others and increases their difficulties in interpersonal communication and environmental interactions, thus having a considerable negative effect on their QOL.
Perceived “Subjective Health Status”
ODLs’ “subjective health status” were associated with their subjective life experiences. The most mentioned subjective health status was about “pain”, “sleep”, “appetite”, “energy”, etc., which played an essential role in their perceptions of health. ODLs’ positive “subjective health status” was strongly associated with “lack of pain” and “good sleep/appetite/drinking/activities”, which represented being “full of energy”.
I am satisfied with how I feel about my health. I can eat and sleep well. They (children/spouse) are worried more than I am. I cannot wait to meet my good friends who had telephoned me and requested me to go fishing after my discharge. (107-12-B)
Compared with ODLs who reported positive “subjective health status”, those who reported negative feelings were more easily unmotivated with their daily lives. They reported more negative feelings, such as “lack of cure”, “discomfort”, “worry”, “fear”, and “confusion”. As a result, many negative behavioural reactions were reported, which included “being unmotivated about planning daily activities”, “being unmotivated about pursuing a higher QOL”, “less confidence in improving QOL”, etc. Thus, such ODLs had relatively poorer QOL.
My subjective health status is bad. I still feel pain and can’t sleep well, which make me very restless with anxiety for a long time. But I dare not always tell my children about my real feelings, because I am afraid to complain that I am having troubles. Thus, I simply hide my feelings and make as few requests as possible. Recently, I have been gradually reducing my daily activities and visiting fewer friends. (78-9-Q)
Perceived “Treatment Outcomes”
Degenerative lumbar diseases are irreversible in some ways. Thus, many patients have to live with such diseases for the rest of their lives, which results in negative perceptions of “treatment outcomes”. Several ODLs stated that their perceived “treatment outcomes” were not only based on their physicians’ evaluations but also their subjective perceptions. The latter refers to their own experience and feelings, which can influence their health-related decision-making in daily life, such as “health management”, “living arrangements”, and “expectation of future”. Many of these were closely associated with their QOL. ODLs who reported positive “treatment outcomes” also reported relatively better QOL.
I feel the treatment outcomes are OK. On the advice of my physicians, I have increased my activities and do some exercises under the supervision of my family. I feel I am more popular in my family and have more energy. I even feel I can ride my bike again someday in the future. (32-4-Z)
On the contrary, ODLs who reported negative treatment outcomes were more likely to report worse QOL, even if their real health status was better than their perceptions. Such perceived “treatment outcomes”, especially negative perceptions, influenced ODLs’ QOL by causing “interpersonal troubles about communication/trust”, “worry/low self-confidence”, “negative attitude about treatment/exercise/health management”, etc., all of which are important for their QOL.
I feel the treatment outcomes are negative. But they (children/spouse/friends) never believe me. My children told me the treatment outcomes were good. Others told me to stop thinking that I will never be as good as before just because I am an older person. But I know better because the terrible feelings related to my body are mine, not theirs. Then I always get worried. (118-17-N)
Discussion
Although degenerative lumbar diseases have always had negative effects on older adults and been studied for many years, they are difficult to cure.24 The current general treatment purpose for degenerative lumbar diseases is to relieve their unpleasant symptoms. Surgical interventions are not considered unless the symptoms are severe. Therefore, ODLs’ QOL is often reduced by non-medical factors pertaining to their daily lives, among which health-related perceptions play an important role.
Degenerative lumbar diseases can result in an increased risk of fragility fractures.39,40 But most related clinical degenerative symptoms do not manifest until one becomes older.41,42 Moreover, as found in this study, ODLs’ QOL is closely associated with their health-related perceptions, including “life barriers”, “subjective health status”, and “treatment outcomes”. ODLs’ QOL scores in “positive” and “negative” groups showed significant differences in all four domains. Higher QOL scores tended to be more strongly associated with positive perceptions.
Fewer life barriers can provide ODLs more comfort or convenience, both practically and psychologically, which are important for a better QOL. ODLs tend to be troubled by the central activity structures in daily life.13 In this study, many perceived barriers affected their daily life distinctively and repeatedly. Severe discomfort and inconvenience were associated with such perceived “life barriers”. Activities and individuals that the ODLs cared about (to provide material and labour help) were also associated with such perceived “life barriers”. They are important for ODLs’ QOL. Meanwhile, perceived “life barriers” were also experienced in their interactions with society and the environment. The negative effects of perceived barriers on patients’ interaction with society and environment may also greatly affect their QOL.43
ODLs experience several diseases and related symptoms in their everyday lives. Thus, their subjective perceptions accumulate over time, which are then reflected in various experiences and impact their “subjective health status.”44 In this study, negative “subjective health status” were associated with some common factors. For example, pain is one of the first indicators of health-related QOL.45 Poor appetite can influence their “subjective health status” by affecting the hypothalamus through the cerebral cortex.46 Patients with poor sleep, especially those who have had poor sleep habits for a long period of time, tend to display negative emotions, such as anxiety, worry, and uneasiness.47 In this study, these negative “subjective health status” were mentioned frequently by ODLs who also reported poorer QOL, indicating that ODLs’ QOL is associated with their “subjective health status.”
Further, perceived positive “treatment outcomes” showed a positive association with ODLs’ health-related decision-making processes in daily life, while perceived negative “treatment outcomes” negatively influenced their QOL and behaviour patterns. For an individual’s bounded rationality and behavioural psychology, an individual’s health-related behavioural reaction is associated with their perceptions.48 A negative perception of “treatment outcomes” can result in limitations to ODLs’ daily life, extra requirements for medical service, constraints in ODLs’ interactions with the society and environment, and behavioural restrictions on life arrangements and expectations. These limitations are closely associated with ODLs’ QOL.
Limitations
Although this study has some strengths, it has several limitations. First, ODLs were recruited from a general hospital in Shanghai. Therefore, the limited sample size and sampling method limit the generalisability of the findings to all ODLs in Shanghai or all of China. Second, the study’s qualitative design precludes causal inferences of ODLs’ QOL and their perceived factors. Third, the reliability and validity to these themes might need to be demonstrated further in a broader context using the relevant questionnaire. Finally, a possible self-selection bias might mislead our consideration if participants in this study tried to emphasise some positive or negative perceptions of QOL.
Conclusion
In this study, ODLs’ QOL was examined across the four domains of physiology, psychology, social relation, and environment. The findings showed that their perceptions, including perceived “life barriers”, perceived “subjective health status”, and perceived “treatment outcomes” were associated with their QOL. Thus, to improve ODLs’ QOL, more attention should be paid to improving their perceptions, which implies that non-medical factors should also be emphasised.
Ethical Approval
This study was approved by the School of International and Public Affairs, Shanghai Jiao Tong University. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). Informed consent was obtained from all patients prior to their participation in the study. All the participants consent included publication of anonymized responses.
Acknowledgments
The authors appreciate all participants of this study for their selfless participation and dedication.
Funding
This research received no specific grant from any funding agency in public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Wang YX, Wang JQ, Kaplar Z. Increased low back pain prevalence in females than in males after menopause age: evidences based on synthetic literature review. Quant Imaging Med Surg. 2016;6(2):199–206. doi:10.21037/qims.2016.04.06
2. Ishimoto Y, Kawakami M, Nakagawa Y. The impact of lumbar spinal stenosis, knee osteoarthritis, and loss of lumbar lordosis on the quality of life: findings from the Katsuragi Low Back Pain Study. Spine Surg Relat Res. 2019;3(2):157–162. doi:10.22603/ssrr.2018-0051
3. Imagama S, Ando K, Hasegawa Y. The relationship between neuropathic pain and spinal alignment independent risk factors for low quality of life in middle-aged and elderly people. Spine. 2019;44(19):E1130–E5. doi:10.1097/BRS.0000000000003073
4. Makino T, Kaito T, Yonenobu K. Risk factors for poor patient-reported quality of life outcomes after posterior lumbar interbody fusion an analysis of 2-year follow-up. Spine. 2017;42(19):1502–1510. doi:10.1097/BRS.0000000000002137
5. Inose H, Hirai T, Yoshii T, et al. Predictors for quality of life improvement after surgery for degenerative cervical myelopathy: a Prospective Multi-Center Study. Health Qual Life Outcomes. 2021;19(1):150. doi:10.1186/s12955-021-01789-7
6. Carpenter CJ. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010;25(8):661–669. doi:10.1080/10410236.2010.521906
7. Ghiasvand H, Higgs P, Armoon B. Social and demographical determinants of quality of life in people who live with HIV/AIDS infection: evidence from a meta-analysis. Biodemography Soc Biol. 2020;65(1):57–72. doi:10.1080/19485565.2019.1587287
8. Albert HB, Sorensen JS, Christensen BS, Manniche C. Antibiotic treatment in patients with chronic low back pain and vertebral bone edema (Modic type 1 changes): a double-blind randomized clinical controlled trial of efficacy. Eur Spine J. 2013;22(4):697–707. doi:10.1007/s00586-013-2675-y
9. Brinjikji W, Luetmer PH, Jarvik JG. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811–816. doi:10.3174/ajnr.A4173
10. Reginster JY, Burlet N. Osteoporosis: a still increasing prevalence. Bone. 2006;38(2 Suppl 1):S4–9. doi:10.1016/j.bone.2005.11.024
11. Parker SL, Adogwa O, Paul AR, et al. Utility of minimum clinically important difference in assessing pain, disability, and health state after transforaminal lumbar interbody fusion for degenerative lumbar spondylolisthesis. J Neurosurg Spine. 2011;14(5):598–604. doi:10.3171/2010.12.SPINE10472
12. Parker SL, Grahovac G, Vukas D, Ledic D, Vilendecic M, Mcgirt MJ. Cost savings associated with prevention of recurrent lumbar disc herniation with a novel annular closure device: a Multicenter Prospective Cohort Study. J Neurol Surg a Cent Eur Neurosurg. 2013;74(5):285–289. doi:10.1055/s-0033-1341416
13. Jing S, Yin A, Shi L, Liu J. Whether new cooperative medical schemes reduce the economic burden of chronic disease in rural China. PLoS One. 2013;8(1):e53062. doi:10.1371/journal.pone.0053062
14. Kim YW, Baik YH, Yun YH, et al. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg. 2008;248(5):721–727. doi:10.1097/SLA.0b013e318185e62e
15. Quinten C, Coens C, Mauer M, et al. Baseline quality of life as a prognostic indicator of survival: a meta-analysis of individual patient data from EORTC clinical trials. Lancet Oncol. 2009;10(9):865–871. doi:10.1016/S1470-2045(09)70200-1
16. Neogi T. The epidemiology and impact of pain in osteoarthritis. Osteoarthritis Cartilage. 2013;21(9):1145–1153. doi:10.1016/j.joca.2013.03.018
17. Kim SH, Son BH, Hwang SY, et al. Fatigue and depression in disease-free breast cancer survivors: prevalence, correlates, and association with quality of life. J Pain Symptom Manage. 2008;35(6):644–655. doi:10.1016/j.jpainsymman.2007.08.012
18. Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology. 2012;143(5):1179–87 e3. doi:10.1053/j.gastro.2012.08.002
19. Williamson D, Gonzalez M, Finlay A. The effect of hair loss on quality of life. J Eur Acad Dermatol Venereol. 2001;15(2):137–139. doi:10.1046/j.1468-3083.2001.00229.x
20. Alemo S, Sayadipour A. Sources and patterns of pain in lumbar disc disease: revisiting Francis Murphey’s theory. Acta Neurochir. 2010;152(9):1555–1558. doi:10.1007/s00701-009-0315-4
21. Phillips FM, Slosar PJ, Youssef JA, Andersson G, Papatheofanis F. Lumbar spine fusion for chronic low back pain due to degenerative disc disease: a systematic review. Spine. 2013;38(7):E409–22. doi:10.1097/BRS.0b013e3182877f11
22. Tang DH, Gilligan AM, Romero K. Association of patient demographics on quality of life in a sample of adult patients with cardiac arrhythmias. Qual Life Res. 2014;23(1):129–134. doi:10.1007/s11136-013-0445-2
23. van Vegchel N, de Jonge J, Bosma H, Schaufeli W. Reviewing the effort-reward imbalance model: drawing up the balance of 45 empirical studies. Soc Sci Med. 2005;60(5):1117–1131. doi:10.1016/j.socscimed.2004.06.043
24. Siegrist J, Siegrist K, Weber I. Sociological concepts in the etiology of chronic disease: the case of ischemic heart disease. Soc Sci Med. 1986;22(2):247–253. doi:10.1016/0277-9536(86)90073-0
25. Mulry R. Five steps to controlling back injury costs. Prof Saf. 1992;12:24–26.
26. Borneman T, Koczywas M, Ferrell B. An Interdisciplinary Care Approach for Integration of Palliative Care in Lung Cancer. Clinical lung cancer. 2008;9(6):352-360. doi:10.3816/CLC.2008.n.051
27. Badia M, Orgaz MB, Longo E, Verdugo MA, Ullán AM. Do environmental barriers affect the parent-reported quality of life of children and adolescents with cerebral palsy? Res Dev Disabil. 2016;49–50:312–321. doi:10.1016/j.ridd.2015.12.011
28. Nitsch KP, Stipp K, Gracz K, Ehrlich-Jones L, Graham ID. Integrating spinal cord injury – quality of life instruments into rehabilitation: implementation science to guide adoption of patient-reported outcome measures. J Spinal Cord Med. 2020;23:1–9.
29. Rasmussen J, Primdahl J, Bremander A. Physical activity in people with axial spondyloarthritis and the impact of overall attitudes, barriers, and facilitators: a cross-sectional study. Musculoskelet Care. 2020;18(4):510–518. doi:10.1002/msc.1495
30. Thomson P, Rushworth GF, Leslie SJ, Angus NJ, Mohan AR. Longitudinal study of the relationship between patients’ medication adherence and quality of life outcomes and illness perceptions and beliefs about cardiac rehabilitation. BMC Cardiovasc Disord. 2020;20(1). doi:10.1186/s12872-020-01378-4
31. Karimi M, Brazier J. Health, health-related quality of life, and quality of life: what is the difference? PharmacoEconomics. 2016;34(7):645–649. doi:10.1007/s40273-016-0389-9
32. Mary C, Maria OR, Helen E, Stacey H. The relationship between clinical outcomes and quality of life for residents of aged care facilities. Aust J Adv Nurs. 2009;26(4):49–57.
33. Strauss AL, Corbin J. Pesquisa Qualitativa: Técnicas e Procedimentos Para o Desenvolvimento de Teoriafundamentada[Qualitative research: Techniques and procedures for developing grounded theory].
34. Corbin J, Strauss A. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Newbury Park: Sage; 2007.
35. Sbaraini A, Carter SM, Evans RW, Blinkhorn A. How to do a grounded theory study_ a worked example of a study of dental practices. BMC Med Res Methodol. 2011;11(1). doi:10.1186/1471-2288-11-128
36. Ruan Y, Zhu D, Lu J. Social adaptation and adaptation pressure among the “drifting elderly” in China: a Qualitative Study in Shanghai. Int J Health Plann Manage. 2019;34(2). doi:10.1002/hpm.2750
37. Aldiabat KM, Le Navenec C-L. Data saturation: the mysterious step in grounded theory methodology. Qual Rep. 2017;23(1):245–261.
38. Charmaz K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis. London, UK: Sage; 2006.
39. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
40. Hernlund E, Svedbom A, Ivergard M, et al. Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos. 2013;8(1–2):136. doi:10.1007/s11657-013-0136-1
41. Bharmal M, Thomas J
42. Bauer UE, Briss PA, Goodman RA, Bowman BA. Prevention of chronic disease in the 21st century: elimination of the leading preventable causes of premature death and disability in the USA. Lancet. 2014;384(9937):45–52. doi:10.1016/S0140-6736(14)60648-6
43. You JJ, Downar J, Fowler RA, et al. Barriers to goals of care discussions with seriously ill hospitalized patients and their families: a multicenter survey of clinicians. JAMA Intern Med. 2015;175(4):549–556. doi:10.1001/jamainternmed.2014.7732
44. Hickson L, Meyer C, Lovelock K, Lampert M, Khan A. Factors associated with success with hearing aids in older adults. Int J Audiol. 2014;53(sup1):S18–S27. doi:10.3109/14992027.2013.860488
45. Reeve BB, Hays RD, Bjorner JB, et al. Psychometric evaluation and calibration of health-related quality of life item banks - plans for the patient-reported outcomes measurement information system (PROMIS). Med Care. 2007;45(Suppl 1):S22–S31. doi:10.1097/01.mlr.0000250483.85507.04
46. Wynne K, Stanley S, McGowan B, Bloom S. Appetite control. J Endocrinol. 2005;184(2):291–318. doi:10.1677/joe.1.05866
47. Reeve BB, Mitchell SA, Dueck AC, et al. Recommended patient-reported core set of symptoms to measure in adult cancer treatment trials. J Natl Cancer Inst. 2014;106(7):dju129–dju129. doi:10.1093/jnci/dju129
48. Barberis NC. Thirty years of prospect theory in economic Nicholas C. Barberis: a review and assessment. J Econ Perspect. 2013;27(1):173–195. doi:10.1257/jep.27.1.173
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.