Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Health Professionals’ Experiences Regarding Alcohol Consumption and Its Relation to Older Care Recipient’s Health and Well-Being
Authors Johannessen A ![]() , Tevik K
, Tevik K ![]() , Engedal K, Gade Haanes G, Helvik AS
, Engedal K, Gade Haanes G, Helvik AS ![]()
Received 11 March 2021
Accepted for publication 2 June 2021
Published 12 July 2021 Volume 2021:14 Pages 1829—1842
DOI https://doi.org/10.2147/JMDH.S310620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Aud Johannessen,1,2 Kjerstin Tevik,3 Knut Engedal,1 Gro Gade Haanes,2 Anne-Sofie Helvik1,3
1Norwegian National Advisory Unit on Ageing and Health, Vestfold Hospital Trust, Tønsberg, Norway; 2University of South-Eastern Norway (USN), Department of Nursing and Health Sciences, Kongsberg, Norway; 3General Practice Research Unit, Department of Public Health and Nursing, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trondheim, Norway
Correspondence: Aud Johannessen
Norwegian National Advisory Unit on Ageing and Health, Vestfold Hospital Trust, P.O. Box 2136, Tønsberg, NO-3103, Norway
Tel +47 97547979
Email [email protected]
Background: Alcohol consumption among older people is expected to increase in the years ahead. Health professionals’ experiences of, and reflections on, alcohol consumption and its relation to well-being are thus important to the provision of adequate and high-quality treatment and care.
Aim: To investigate health professionals’ experiences and reflections about alcohol consumption among older people and how it is related to their health and well-being.
Methods: A case study design approach was adopted, incorporating three qualitative studies involving Norwegian health professionals. The health professionals interviewed included workers in nursing homes, home care professionals and general practitioners.
Results: The study revealed a diversity of views and reflections on alcohol consumption, its facilitation, and the impact on the health and well-being of older patients and care recipients. Six themes were revealed by the three studies: (i) the facilitation of alcohol consumption to promote and normalize life in nursing homes, (ii) the restriction of unhealthy alcohol consumption, (iii) attempts to discuss alcohol consumption with care recipients, (iv) the initiation of collaboration with informal caregivers in restricting alcohol consumption, (v) minimalizing the dialogue regarding alcohol consumption to guard patient privacy and (vi) a desire for joint action and a national political strategy.
Conclusion: Health professionals working in NHs, in-home and GPs find it difficult to discuss the use and elevated use of alcohol with older people for whom they have care and treatment responsibilities. In general, they are concerned that such conversations infringe on the principles governing an individual’s autonomy. However, because they are aware that elevated alcohol intake may have a negative impact on health and well-being, they also express a need for guidelines how they in a better and open minded way can discuss the use and elevated use of alcohol with the patients they care for.
Keywords: case-study, elderly, harmful use of alcohol, narrative interviews, municipality staff, older adult, older oldest
Introduction
In most western countries, alcohol consumption is a normal part of adult social life. For all adults, including older people older people aged 65 years and above, the serving of alcohol and its intake are linked to special occasions, functions and recreational events involving social interaction promoting joy, pleasure and general well-being. Opinions about alcohol consumption are influenced by the social norms and regulations prevailing in wider society, and may differ between countries and regions across the world.1
In the Nordic countries, both alcohol intake volumes and frequency of consumption decrease with increasing age in both genders.2–4 However, in recent years, the decrease in alcohol consumption with age among older people has been less prominent than in the 1970s, and the proportion of older people currently abstaining entirely has decreased since.3,5,6 A epidemiological study in Norway reported that about 28% of community-living men and women 65 years or older drank alcohol once a week or more often, but only 11% of those drinking weekly drank 4 times a week or more often.7 In Norway, among the current generation of older people born in the period following the Second World War, alcohol consumption is now expected to increase in the years to come.8
Alcohol consumption comprises a health risks that are linked to drinking patterns, the amount of alcohol consumed, and the vulnerability of the individual user of alcohol. Research suggests that, in general, older people are more vulnerable to the negative health impacts of alcohol than younger people, primarily due to age-related changes.9,10 On the basis of generally greater vulnerability in old age, some countries have introduced guidelines for alcohol consumption.11,12 However, no standardized international guidelines have been established for consumption among older people.11 In the United States (US), older people are recommended to drink no more than one unit of alcohol per day, or no more than seven units per week. These recommendations apply to healthy individuals who are not taking medication; older people with health problems or who are taking certain medications should drink less or not at all.11,13 In the USs, the term “elevated consumption” is used to describe levels of consumption that exceed recommended domestic guidelines. Alcohol guidelines developed specifically for older people are recently developed in Canada too, and the recommendations are a bit higher than in US.14 Although, there are indeed a dearth of guidelines for older people, in the general population alcohol guidelines still differ markedly between countries, with different levels of suggested “safe” consumption and with/without gendered guidelines, and as such achieving international consensus may be particularly challenging.
The World Health Organization (WHO) has reported that elevated alcohol consumption is negatively linked to more than 200 health conditions15 and that a possible connection exists between a lifetime of elevated consumption and reduced cognitive function in old age.16–18 In addition, numerous studies have reported that elevated consumption and mental illness among older people are often reported simultaneously, although it is not always easy to determine which occurred first.19 Moreover, depending on the level of drinking and an older individual’s health status, alcohol consumption may increase the risk of falls,20 cardiovascular disease,21,22 cancer,22 hospitalization,23 physical constraints24 and reduced quality of life or well-being.25 Alcohol interacts with many of the medications commonly prescribed to older people,10,26 and may increase the risk of adverse effects, such as increased sedation, dizziness, fall-related injuries and overdose-related mortality.9,10
For some older people, alcohol consumption may represent a means of coping with their life and health situation.27 Psychosocial risk factors that may promote elevated consumption among older people include the onset of retirement, boredom, loneliness, isolation and homelessness,24,28,29 while others drink to reduce anxiety and depression and increase their sense of well-being.30–32 Alcohol consumption may thus be viewed as a form of psychotropic drug that requires control by public health clinicians.1 However, in some countries, alcohol consumption is regarded as a private matter, both regarding drinkers among older people and abstainers, and is only discussed in general terms, if at all.33–35 A recent study has shown that older people tend to trivialize or dismiss their alcohol consumption, regarding it simply as something that “old people do”.34
Alcohol consumption is therefore regarded both as a normal part of social life and as a potential threat to the health and well-being of older people—in the latter case, alcohol represents a drug that requires regulation.1 These competing views constitute two paradigms and thus also two coexisting realities for those public health clinicians, health service planners, managers and politicians who are responsible for providing health and social services to older people. Nurses and nurses’ aides working NHs and in municipality in-home care services do not consider that they should screen for alcohol misuse among older care recipients in Norway. Only the GPs are normally involved in screening of alcohol misuse and interventions to reduce or stop drinking, but such screening is scarce among GPs.36,37 The GPs may also refer patients to treatment in specialized health care. Recently, a review was published regarding health personals view of barriers to address harmful alcohol consumption in older adults.38 The review reported the following barriers: 1) uncertainty about legitimacy of drinking as a concern for health professionals 2) pre-existing stereotypes of older adults drinking and 3) sensitivity surrounding drinking in old age and 4) older adults own right to decide to drink. However, the review38 did not explore how alcohol consumption was related to health and well-being by the perspective of individual categories of health professionals. Health professionals’ experiences of and reflections on alcohol consumption among older people are therefore crucial to the quality of treatment and care provided to older people and may have consequences for their health and well-being. The terms “well-being” or “wellness” are used here to refer to the diverse and interconnected dimensions of physical, mental and social well-being that extend beyond the traditional definition of the term “health”.39 They encompass choices and activities aimed at achieving physical vitality, mental alacrity, social satisfaction, a sense of accomplishment and personal fulfilment. Thus, the definition of a “good life” is said to entail participation in activities and experiences that involve meaningfulness and inclusion. The WHO has previously highlighted key values, such as participation, justice, equality and independence, as well as the right to health.40 So far as we are aware, there is a general absence of such values linked to policy regarding both the use of alcohol as a social beverage for recreational occasions, and its consumption in the context of personal safety and within the health services sector. In our study we therefore, wanted to investigate health professionals’ experiences of and reflections regarding alcohol consumption among older people and how they relate alcohol consumption to the care recipients’ health and well-being.
Methods
A case study design, as recommended by Yin41 (2003) and42 Berg and Lune (2012), represents one approach to the development of knowledge on relatively complex issues by collecting data from different sources. Such an approach is recommended in situations where it is desirable to include contextual relationships.41,43,44 The use of case studies also facilitates access to several data sources—for example by triangulating sources and methods as a methodological approach, as shown in a study by45 Thorsen and Johannessen (2018). In Norway, little is known how health professionals’ experience older care recipients’ alcohol consumption and how they view the relation between alcohol consumption and the older people’s health and well-being. Health professionals’ experiences of and reflections on alcohol consumption among older people and how they judge alcohol consumption to be related to older people’s health and well-being are little explored. We felt it would therefore be of particular interest to compile the opinions of a broad range of health professionals with diverse work experiences. Following Berg and Lune,42 to conduct this case study, we included empirical data from three earlier qualitative studies that met these requirements (references to the studies will be included later). The three original studies represent three cases and included nurses, occupational therapists (OTs), physical therapists (PTs) and social educators (a person that contribute to help people to prevent, solve and reduce social problems) working in NHs and the in-home care sector. In addition, opinions of general practitioners (GPs) were included in the present study (see Table 1 for details about the informants).
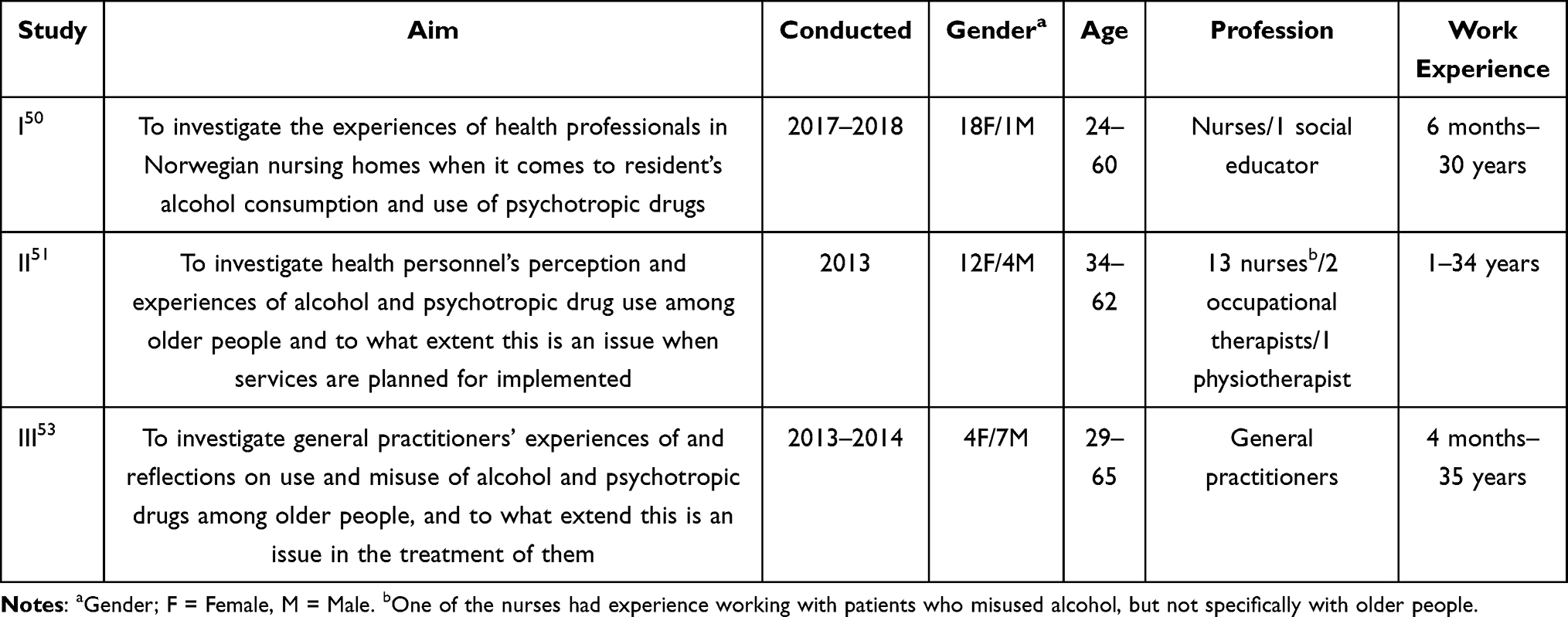 |
Table 1 Overview of Studies I, II and III, and Information Relating to the Informants Involved in This Case Study |
Material
The aforementioned studies (I, II and III) all had qualitative designs.46 Such an approach is well-suited to obtaining knowledge of poorly documented conditions, and to grasping the meaningful content of recorded experiences.46 Experience from other studies47 shows that the views of different sources—and in this case, different health professionals—should not be overlooked, because these can facilitate a “bottom-up perspective”48 or experiences from different sources.45 The three cases collected data by using Norwegian language.
The Three Cases
Study I was an investigation of the experiences of nurses and a social educator related to NH residents’ use of alcohol and psychotropic drugs. The study employed a combination of focus group and semi-structured in-depth interviews. The focus group interviews were conducted by ZZ and XX, while all other interviews were conducted by XX. The study involved the participation of 19 health professionals working in NHs in six Norwegian counties. Six of the 19 worked in care units, 5 had special responsibilities for quality development, 5 were unit leaders and 3 held other responsibilities within the NHs. (Further information is provided in Table 1.) The informants were initially contacted by telephone or letter, or during face-to-face conversations at professional conferences. All the interviews were audio-recorded, transcribed by a professional typist and checked by the interviewer (XX). The material was analyzed using the content analysis approach.49 The analysis was carried out in three steps by the authors XX and ZZ. Findings revealed two themes based on the NH informants’ opinions and experiences: 1) the balancing of alcohol use is needed to improve quality of life and provide good quality of care, and 2) the use of psychotropic drugs, practice and changes related to treatment and care. The two major themes encompassed four subthemes: (i) alcohol may contribute to pleasure and better quality of life, (ii) alcohol needs to be restricted if alcohol consumption is harmful, (iii) practice and collaboration related to residents’, use of psychotropic drugs and (iv) changes in use of psychotropic drugs as a part of treatment and care.50
Study II was an investigation of nurses’, OTs’ and PTs’ perceptions and experiences of alcohol and psychotropic drug use among older people and the extent to which this was an issue in terms of the planning and implementation of in-home health services. The study was conducted using individual in-depth interviews with 16 health professionals working in the home care sector. The interviews employed semi-structured thematic questions and were conducted by XX. in order to create a heterogeneous group hoping to maximize diversity of experiences. Initially, 14 heads of home care sectors in urban and rural municipalities in southern Norway were contacted by telephone and asked to recruit informants. Sixteen informants were then deliberately selected by XX in order to create a heterogeneous group. (Further information is provided in Table 1.) All the interviews were audio-recorded, transcribed by a professional typist and checked by the interviewer (XX). The data were analyzed using a content analysis approach,49 and the analysis was carried out in three steps by author XX. and ZZ. Two categories of informants’ experiences emerged, described here as: 1) state of practice and. 2) a desire to improve services.” These categories included four subcategories, described as: (i) legitimacy and attention to substance use and misuse, (ii) competence and knowledge in practice, (iii) improving collaboration and (iv) changing routines.51
Study III was an investigation of GPs’ experiences of and reflections on older peoples’ use and misuse of alcohol and of psychotropic drugs, and the extent to which such use was an issue in the treatment of older people. Eleven GPs were recruited by telephone from urban and rural municipalities in Norway. (Further details of the GPs are provided in Table 1.) Nine of the interviews were conducted by XX, and two by UU. All interviews were audio-recorded, transcribed by a professional typist and checked by the interviewer (XX). The data were analyzed using the phenomenological-hermeneutic method developed specifically for research into informants’ life experiences.43,52 This method has the advantage of shifting dialectically between explanations and understanding and was therefore suitable for these data collected. The analysis was carried out by the first author XX and the last author VV. Two themes emerged. The first theme encompassed on the GPs’ opinions of older people’s alcohol and psychotropic drug use. This theme included three subthemes: (i) older people’s situations, (ii) older people’s alcohol use, and (iii) older people’s psychotropic drug use. The second theme described the GPs’ practice, and was divided into two subthemes addressing (i) assessment of alcohol consumption and (ii) prescription of psychotropic drugs.53
In the following text
Analysis
The aim of the analysis in the present case study was to illustrate the experiences of health professionals with diverse backgrounds and work experience working in the Norwegian health service at the municipal level. The research question we asked before re-analyzing all original material was how due health professionals from several settings in the municipality health services experience and reflect upon alcohol consumption in older adults and the health and well-being consequences of alcohol consumption?
The interviews from the three studies were recoded and re-analyzed by separated reading54 and via content analysis49 aiming at identifying, describing and thematizing the compiled data. The analysis was carried out in three stages. First, the authors XX and ZZ carefully re-read the interviews several times to gain an overall impression, identified words and sentences expressing a central meaning, and systematically condensed the data while being careful not to alter the original meaning. In the next stage, the authors assigned a code to the relevant phrases that identified their content. In the third and final stage, the categories were created: these consisted of groups of codes corresponding to the themes in the interviews. Quotations from interviews conducted in the three studies are presented in the following to assist readers in evaluating the integrity of the findings.
Ethics
The present study adhered to the ethical principles outlined in the Helsinki Declaration.55 The scope of the study was presented to the Norwegian Data Protection Authority and was shown not to infringe on the provisions of the Norwegian Act relating to medical and health research. As such, it did not require approval from a regional ethics committee.
Results
An overview of the themes extracted from the material of each study are illustrated in Table 2.
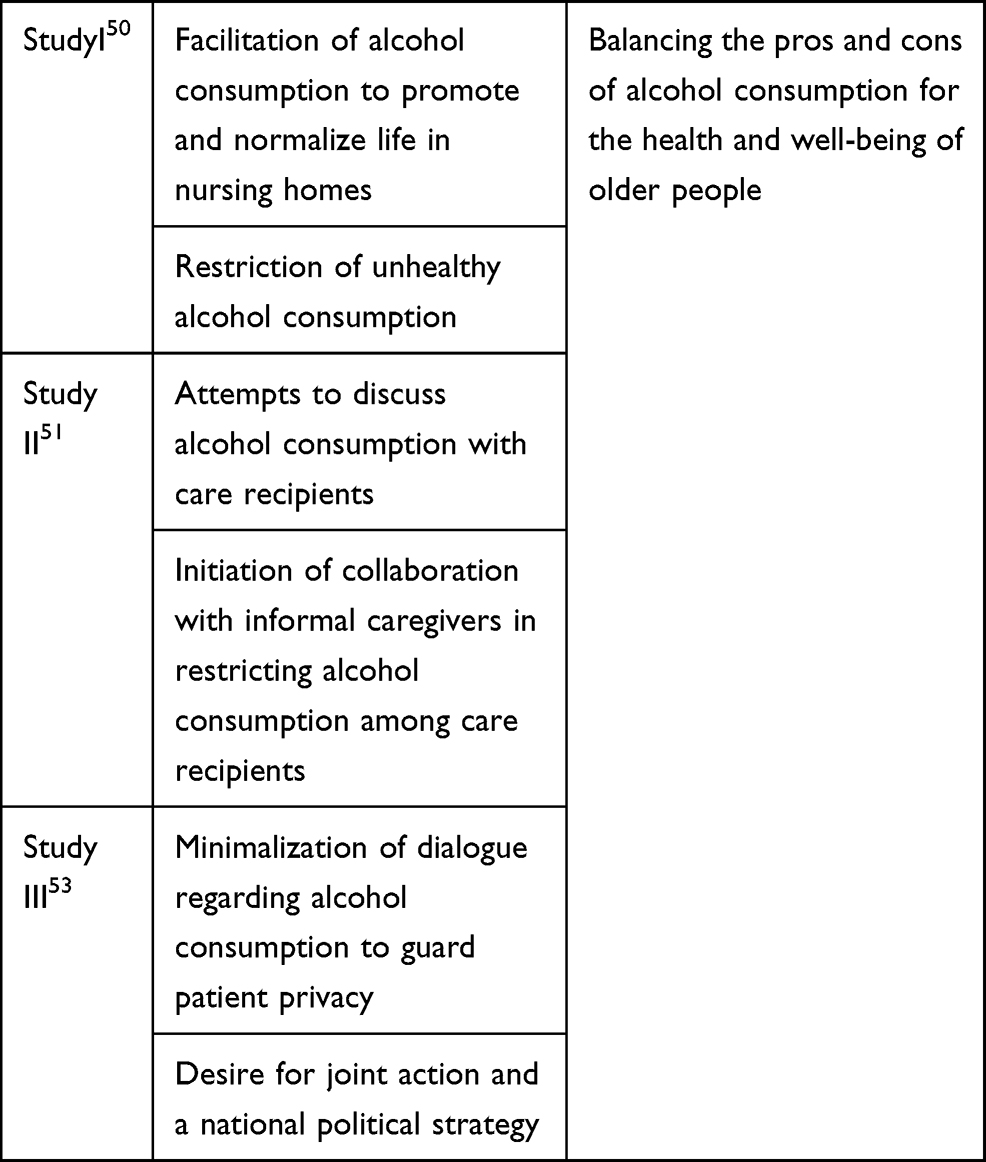 |
Table 2 Overview of the Six Themes That Emerged from these Three Included Studies, and a Sum-Up of the Three Original Cases |
Study I: The findings of this study show that health professionals exhibited a variety of experiences of and reflections on alcohol consumption in NHs. Two themes were revealed: (i) facilitation of alcohol consumption to promote and normalize life in NHs, and (ii) restriction of unhealthy alcohol consumption.
Facilitation of Alcohol Consumption to Promote and Normalize Life in NHs
The informants discussed to varying degrees whether it was right to facilitate alcohol consumption in a NH. Some considered such facilitation to be a positive contribution to the residents’ quality of life. It was also thought to have a nurturing effect and that it promoted joy and pleasure. Serving alcohol on weekends was a way of differentiating the weekend from the rest of the week. Moreover, the informants suggested that NH residents should experience a life that was as normal as possible, and that drinking alcohol was an issue of self-determination. In some situations, where the serving of alcohol was available on weekends, informants said that residents were often too tired to want it. Others expressed the view that having a single glass of wine was acceptable, even for those residents taking a variety of medications; it was just a matter of evaluating doses relative to the amount of alcohol. Other informants said that the serving of alcohol-free beer and wine was a valid option in such cases. In one of the NHs, a user survey on the serving of alcohol was conducted, about which one of the informants stated:
In one unit, the residents said that serving alcohol, or having a cart available from which they could buy alcohol, was not important. They would rather have a chocolate cart. However, in another unit, they thought that it was nice to enjoy wine on Saturdays. So, is the desire among the residents so great? I am uncertain as to whether alcohol contributes to a better quality of life. I am uncertain! It doesn’t seem like that when you ask the older people!
Some informants stated that serving alcohol could be an indicator of the quality of the NH service. One said:
Running a bar in an NH has been one of those things that politicians have said could be an NH welfare indicator.
In line with this, it appeared that the NHs had a variety of different arrangements to permit the serving of alcohol. Some NHs employed volunteers or NH support groups, acting almost as servers who sold and served alcohol on the weekends, or served alcohol during parties arranged on a monthly basis. Other NHs ran a soccer-themed or an ordinary pub, also once a month. The soccer-themed pub was reported to be an activity supported by the government-backed “Quality Reform for Older People” initiative. Alcohol carts were made available every Saturday and were given different names, such as the “pleasure cart” or the “welfare cart.” Some informants reported that their NH also sold or served alcohol-free beer and wine in the bars and from the carts. Some said that there were no bars or carts, but that residents could enjoy their own drinks bought in by informal caregivers. One informant said:
The rule is that one glass of alcohol a day is okay—a rule that was also well known to the informal caregivers.
Restriction of Unhealthy Alcohol Consumption
Making alcohol available for consumption does not always increase well-being. The informants expressed that, until quite recently, there had been considerable fear going on about the negative effects of alcohol. Nevertheless, some NH informants had begun reflecting on the alcohol consumption of their residents. This change in focus could be a result of their participation in seminars on topics related to alcohol consumption in old age, and/or experiences of alcohol consumption creating difficult situations for residents or carers who had been threatened or hindered in their work by residents who had been drinking to excess. Alcohol consumption may contribute to poorer health and well-being, and some noted that regular access to and the consumption of alcohol is restricted in their NH. One said:
We’re a NH, and there is no serving of alcohol here at our NH, so consumption should be restricted and controlled for residents at the facility. Of course, we see that friends, family members and acquaintances smuggle in gin and tonics in half-liter bottles.
Informants mentioned that NH professionals tried to restrict the alcohol use of residents who are known as “extensive alcohol consumers.” Restrictions were put in place in collaboration with the residents themselves, their informal caregivers and NH physicians. In some situations, the County Governor’s office has been involved in imposing restrictive regulations on alcohol intake. Moreover, some NHs had removed refrigerators from residents’ rooms as a means of regulating alcohol intake. One informant said:
It’s difficult! To what extent can we regulate? We are in discussions with the County Governor about alcohol regulation. We have arrived at a compromise saying that if they drink, they must do so in their own rooms. But, if so, they do not get their medication. These are psychotropic drugs such as tranquilizers and anti-psychotics that increase the risk of falls and agitation.
Health professionals also reported that they monitored residents who consumed alcohol regularly as part of a patient safety program designed to reduce the incidence of falls and other accidents. They also said that they were in dialogue with residents’ informal caregivers, when the latter brought alcohol to the NH.
Study II: The findings of this study show that in-home care health professionals exhibited a variety of experiences of and reflections on alcohol consumption and its relation to well-being. Two themes emerged from the interviews: (i) attempts to discuss alcohol consumption with care recipients, and (ii) initiation of collaboration with informal caregivers in restricting alcohol consumption among care recipients. These themes cover how the informants dealt with their experiences of alcohol consumption that seemed elevated and risk-full for their health of older care recipients.
Attempts to Discuss Alcohol Consumption with Care Recipients
In general, the informants stated that they enjoyed a healthy dialogue with the older people receiving in-home care services. Nevertheless, when it came to alcohol intake and its potential impact on health and well-being, they reported that they either did not focus greatly on the topic or found it difficult to talk naturally about it. Moreover, in cases of elevated consumption, involving increased health risks to care recipients, informants believed that although such consumption reduced recipients’ quality of life, engaging in dialogue related to alcohol intake was difficult. Informants reported that this was a sensitive subject, and that care recipients expressed surprised if health professionals raised the subject and its effect on their health and well-being. Most care recipients wanted to avoid the topic. As one informant explained:
If we talk to older people about their consumption of alcohol, they tell us that it’s not our business.
Informants also reported that discussing alcohol intake may interfere with the principles of autonomy and their recipients’ right to self-determination. They felt that such conversations impinged on fundamental rights associated with well-being. However, the informants also stated that they rarely observed elevated consumption among their recipients, rendering such conversations unnecessary. Nevertheless, one informant stated the following:
We do raise the issue of alcohol when care recipients apply for an electric wheelchair and talk to them about alcohol consumption. The care recipients have to sign an agreement saying that they are not supposed to drink alcohol when they are out using their wheelchairs.
Initiation of Collaboration with Informal Caregivers in Restricting Alcohol Consumption Among Care Recipients
The informants reported having a healthy dialogue and good collaborative relationships with their patients’ next of kin and informal caregivers. In cases of elevated alcohol consumption among care recipients, they sometimes appealed to informal caregivers to encourage their relatives to drink less, once they noticed that prolonged consumption might be having a negative effect on a patient’s health or well-being. In most cases, caregivers were aware of the alcohol consumption, but were unable to influence the patient’s intake. Moreover, informants noted that sometimes informal caregivers responded that their relative habitually consumed the same amount of alcohol without suffering any harm earlier in life. Thus, in the informants’ experience, while some caregivers exhibited awareness, others did not recognize either the reason to reduce consumption or the potential consequences of drinking for their relative’s health and well-being. As one informant noted:
The informal caregivers do not understand the dangers involved in combining elevated alcohol consumption with the pills being taken by the care recipient.
Moreover, informal caregivers would sometimes bring or buy alcohol and encourage drinking as a means of promoting well-being. One informant said:
I often see that …, and I enjoy a glass of wine myself, so I can understand the old chap sitting there in his living room with a three-liter box [of wine] after a visit from his next of kin.
The informants told that some informal caregivers try to talk about drinking with their parents but are told that it’s just none of their business, so they are they are unable to do any more about it. Informants also experienced having informal caregivers that told them that they are under pressure to buy alcohol for their relative. One of them noted:
These caregivers do so because they are concerned that their relatives might drive to the store themselves, something which they are in no condition to do.
Study III: The findings of this study show that the GPs exhibited a wide variety of experiences of and reflections on alcohol consumption and its relation to well-being among older people. Two themes emerged from the interviews: (i) minimalization of dialogue regarding alcohol consumption to guard patient privacy, and (ii) desire for joint action and a national political strategy.
Minimalization of Dialogue Regarding Alcohol Consumption to Guard Patient Privacy
Some GPs reported that they had observed several “hidden” cases of patients engaging in excessive consumption, and of alcohol addiction. Others reported that drinking to levels that may have a negative impact on health and well-being was rare among their patients, although they admitted to not focusing specifically on the issue. One informant noted:
That I do not see alcohol consumption among my old patients may be because I do not focus on this issue. I am not an expert in alcohol-related histories!
Overall, the GPs reported that this topic was difficult to talk about with an older patient in the absence of a prior alcohol-related history. They explained that references to drinking were often made in a humorous tone, accompanied by laughter, as among “buddies”. The use of screening tools—involving asking a set of detailed questions about drinking frequencies and amounts as a means of assessing the impact on the patient’s physical or mental health—were considered by some GPs to be problematic, because the exercise was experienced by patients as an interrogation. These GPs felt such questions could be experienced as offensive, especially if the patient regarded alcohol consumption as a private matter. As such, exchanges of this type might undermine the trust established between the GP and the patient, which was essential to the optimal treatment and well-being of the latter. Furthermore, GPs worried that raising the issue of alcohol could potentially violate a patient’s rights to privacy, with attendant legal implications.
If a GP considered that a patient’s levels of consumption were elevated, a common strategy among the informants was to take blood tests and use the results as a starting point for initiating a conversation about alcohol and its relation to health and well-being. One informant said:
I’m not good asking about alcohol, but if I take blood tests and find that ALAT, gamma-GT and ferritin levels are a bit too high, then I’ll ask about consumption.
Other informants reported that it was easier to talk with patients about alcohol consumption following an accident, such as a fall, a broken leg or arm, or in connection with issues potentially linked to alcohol, such as stomach complaints. At times, it was easier for informants to raise the subject if they received information about the patient’s alcohol consumption and life situation from other family members.
The informants noted that it was common for both patients and their next of kin to experience a feeling of shame linked to problematic relations with alcohol. Some informants stated that sometimes it was possible to motivate patients to seek support and change their habits. The reasons for alcohol consumption among older people could be existential, related to life crises, mental health problems and, in many cases, loneliness. One GP said:
I had a patient who had lost his wife and was drinking because of this crisis. I had regular meetings and talks with him, and after half a year he totally abstained.
Desire for Joint Action and a National Political Strategy
The informants reported that alcohol consumption and its potential consequences for health and well-being is an important topic within wider society, and that the issue should receive increased attention. One informant was keen to discourage media statements such as “two glasses of wine is good for your heart.” Another informant stated the following:
Wider society needs to be more aware. I believe that GPs, informal caregivers, health professionals in general and the media need to be more aware of alcohol consumption and its risks. Information about the risks should be disseminated throughout society—not in a condescending way, but via the popular media that everyone reads.
Informants also reported that health professionals in general should be more aware of alcohol consumption among older people, including themselves, in consultations with their patients. They recommended that the subject be highlighted in education programs and other arenas, in a similar way to that employed in connection with the risks of smoking. Some stated that health professionals should be reminded to initiate conversations about alcohol consumption and health and well-being. One informant said:
I have received an information card about alcohol consumption and have placed it on my desk to remind me to take the issue up with my patients.
Balancing the Pros and Cons of Alcohol Consumption for the Health and Well-Being of Older People
In general, alcohol consumption was seen both as a normal part of life contributing to well-being and a treat to health and well-being. The health professionals were balancing the pros and cons of alcohol consumption for the health and well-being of their older care recipients and patients, independent of their work experience and workplace, but the actions taken differed considerably. Nursing home personal more clearly than the others weighted the pro et cons of alcohol use. The cons of alcohol consumption for care recipients and patients’ health and well-being were often brought up when elevated alcohol was obvious and negative health consequences were emerging.
Discussion
This study describes a diversity of experiences and reflections reported by NH, home care professionals and GPs regarding alcohol consumption and the facilitation of such consumption among older people and the implications for their health and well-being. In the following, the findings will be discussed in the order they were presented in the preceding section.
Health professionals working in NHs facilitated the consumption of alcohol as a means of promoting a sense of pleasure and to increase their residents’ quality of life and well-being. Alcohol was utilized as a nurturing treatment, and also as a means of promoting a sense of joy and pleasure in a social interaction context.1 Some NH informants reported that user surveys had been conducted in their NHs, asking questions about the serving of alcohol to their residents; the surveys found that some residents wanted alcohol to be served, while others did not. There are different habits among older people currently living at home or in NHs are, but older people are more accustomed to drinking, and this is supported by studies that demonstrate that alcohol consumption in this group has increased during the last decade.1,4,56 Older people themselves have also stated in a study that consumption of alcohol is just something “older people do”,34 it is a part of normal life.
The staff facilitated the serving of alcohol in different ways, and the availability and serving of alcohol in NHs are considered to constitute essential features of enjoying a normal life.1 However, this positive aspect of the serving and consumption of alcohol is at odds with the health risks associated with combining alcohol with medication.1,10,26,57,58 In addition, a liberal attitude towards availability will also tends to increase consumption.56
Nursing home informants also reported that facilitating alcohol consumption did not always necessary increase NH residents’ quality of life in NHs, and that it may in fact be detrimental to health and well-being. The informants’ awareness that alcohol consumption in later years may create difficult situations for some residents was mostly a result of their participation in seminars, but in some cases, informants drew on their own clinical experience. Also, other studies underline that knowledge and training intervention skills is need.38,59,60 One study has also pointed out that key changes take place when health professionals begin showing an interest in patients’ alcohol consumption in the same way they do with other lifestyles diseases.61 This assertion has been supported by another study,51 and other authors have demonstrated that, currently, both ordinary and elevated consumption are more likely to be observed among the oldest older people in Norway and among older NH residents.1,62,63
In the wake of experience in recent years indicating that levels of alcohol intake among some residents is a risk to their health, the environment within NHs, and the well-being of others. The nursing home staff experience of coexisting realities, alcohol both being a normal part of social life and a potential threat to the health and well-being. Nursing home professionals reported that they, when alcohol consumption was elevated and seen as a treat to health, attempted to restrict alcohol consumption, for some residents in collaboration NH with NH physicians and the residents themselves. To regulate consumption, at admission interviews, they have invited residents and their informal caregivers to discuss the NH’s attitudes and procedures related to alcohol consumption. Informants also explained that caregivers who were allowed to bring alcohol into the NH for residents, were also encouraged to engage in discussions with their next of kin and the staff regarding the regulation of alcohol intake. This is in line with Norwegian regulations64 promoting a person-centered care approach combined with person-directed care.65–68
In some situations, the County Governor’s office had become involved in introducing regulations and restrictions in relation to alcohol intake, also in line with Norwegian regulations.64 Moreover, the WHO40 has highlighted key values, such as participation, justice, equality and independence, but also the right to health.69 The NH managers and health professionals in the present study encountered directives whilst also attempting to balance the interests of residents’ rights to self-determination with the treatments they felt were essential for health and well-being.1
Further, our study has shown that the home care health professionals enjoyed a healthy dialogue with their care recipients, but found it difficult to engage them in a relaxed manner about their alcohol intake and its potential impacts on their health and well-being. This was true even in situations where care recipients had increased health risks, or in cases where elevated consumption was reducing their quality of life. Alcohol consumption was regarded as a private matter, and most care recipients avoided the topic. This opinion of the professionals working in in-home care service was differed from what was seen among professionals in NHs, who discussed the serving of alcohol on a regular basis while the in-home care service professionals often overlooked or avoided the topic. The GPs also demonstrated an aversion towards discussing the use of alcohol with their older patients. It might be that the autonomy of older people living at home is more respected, because the informants expressed concern that a discussion of alcohol consumption might interfere with principles of patient autonomy and thus fundamental rights associated with well-being. However, why should such a concern not be evident in NH settings? As mentioned earlier health professionals need support and knowledge to intervene to avoided risks associated with drinking among older people.38,59,60
The health professionals both in NHs and in-home care services and the GPs in this study did not appear to focus much on the causes of elevated consumption, despite it being well known that poor emotional and physical well-being are associated with excessive drinking in old age.24,27–30,32 Our informants seemed to focus more on the actions that could be taken to improve conditions resulting from physical illness, rather than on the causes of elevated consumption. As noted previously, liberal attitudes towards alcohol consumption also contribute to increased consumption.34,56
Municipal in-home care professionals would enter into dialogue with informal caregivers about care recipients’ alcohol intake if they recognized that consumption levels might be having a negative impact on their health and well-being; they would appeal to these caregivers to encourage their relatives to drink less. We believe that this strategy was used because the professionals working in in-home care sought to avoid having this discussion with the care recipients. We do not know the reasons behind this aversion, as they never spoke about it—moreover, while some informal caregivers exhibited an awareness of these issues, not all of them acknowledged the reasons behind the professionals’ recommendation that intake be reduced for the sake of their relatives’ health and well-being. This latter was expressed in attitudes centered on the foolishness of depriving older people of “one last pleasure,” which has also been reported in connection with other older and vulnerable persons.1 Since we know that elevated alcohol use among older people has increased in recent years, and that many are able to reduce their consumption,8,61 it is important to inform informal caregivers not only about the consequences of elevated consumption, but also to encourage both caregivers and care recipients to take action to promote change. Such an initiative is in line with current Norwegian legislation.64 However, the professional in-home care service should be encouraged to talk directly with the care recipients—not just with the informal caregivers—about the negative effects of elevated alcohol consumption.
The GPs should also be encouraged to do the same, regardless of their individual experiences of and perspectives on alcohol as a problem among older people; indeed, as found in the present study, while some reported that they knew about cases of “hidden” elevated consumption and addiction among older people, others reported that cases of high levels of consumption that might impact negatively on health and well-being were relatively rare. A common feature among the GPs is that they would only raise these issues if they had information indicating that a patient’s alcohol intake could impact negatively on their health and well-being, from blood test results, existing medical records or information obtained from next of kin. When GPs did raise the issue of alcohol consumption with their patients, it was often done in a humorous tone, which others have also found to be beneficial in therapeutic settings.70 They did not use a screening tool, nor did they ask detailed questions, because they were concerned that patients would be offended regarding discussing such a sensitive topic. Moreover, the GPs felt that, since alcohol consumption is often regarded as a private matter, a conversation on this issue could undermine the trust established between the GP and the patient, which was essential for optimal treatment. Problems associated with health professionals asking patients about alcohol consumption have been highlighted in previous studies.33 This begs the question as to why GPs’ approach to patients’ elevated alcohol consumption is different than their approach to patients’ smoking habits (ie, their willingness to discuss the latter directly with their patients).
In the present study, the GPs would only initiate discussions related to alcohol consumption if a link could be made to existing information about its relevance for their patients’ health and well-being (as described above), or following an accident (such as a fall) or somatic problems that could be affected by alcohol consumption. Some GPs believed that such conversations may motivate patients to decrease their consumption and/or consent to treatment for dependency, as described in a previous study.61 They were concerned that this could create a sense of shame for their patients, as alcohol consumption among older people could be the result of existential problems, life crises, mental health problems and likely also loneliness. Previous studies have also highlighted the feeling of shame linked to elevated alcohol consumption,71 and that such consumption is both caused by, and contributes to, psychosocial circumstances.19,24,32 In the present study, the GPs felt that asking about alcohol use was somewhat embarrassing, as it was considered a private matter. Clearly, they needed support to intervene as stated in other studies.38,59,60 Furthermore, in Norway relatively few treatment options for older persons with such needs are available and thus, the GP has minimal to offer the patient except of in-house counselling. A consequence is that older people are not offered treatment as they are required for.37
Nevertheless, some GPs interviewed in this study also expressed a need to put the issue of alcohol consumption among older people on the political agenda, and that a national strategy is needed due to the important implications for wider society of the potential negative impacts on health and well-being resulting from elevated consumption. It has been argued that, in light of changing drinking patterns among older people, and expectations of increased consumption in the future, alcohol intake should be the subject of greater focus in the years to come.8 Moreover, health professionals in general must be made more aware of alcohol consumption among older people, and the issue should be highlighted in education programs and other relevant arenas, similar to raising awareness around the risks of smoking. This suggestion is also in line with recommendations set out in a previous study.61 However, above all, there needs to be more transparency and openness among health professionals about alcohol consumption habits in general—their own and their patients’ in order to promote health.15
In addition, the study shows also that roles of different health professional in NHs and in-home care are involved in supporting access to alcohol to older people in Norway in different degree. Only the GPs were involved in brief interventions for elevated alcohol consumption. The GPs are also able to refer to treatment in specialist health care services. However, the treatment option is few, and the not easily available. Furthermore, this study and as well as other studies show that there is a need for educational programs on different levels about the topic alcohol related to health and well to contribute to health promotion in the population and also in the older population.15,38,59,60 The study further shows that the barriers for screening, intervening and referring to treatment are different for the various respondents categories of the study. This may be explained by their different roles in providing health and social care to older people, but could also be a results of a general attitude to the use and elevated use of alcohol in the society as a whole. If elevated use and misuse of alcohol among older adults is accepted by the society as a private matter it would be difficult to introduce new screening and treatment programs. Educational programs focusing on the side effects of alcohol use is not enough to change the attitudes. The general awareness of the health problems related to alcohol use among older adults should be raised.
Strengths and Limitations
A strength of the present study is its inclusion of interviews with a broad range of health workers reflecting diversity in terms of workplace and years of experience. Moreover, the case study design facilitated access to different opinions by including data from three qualitative studies as cases; the qualitative research methods indeed proved helpful in providing knowledge on phenomena where knowledge is scarce.36 An additional strength of the study is its spotlight on the need for guidelines to assist health professionals in dealing with questions about elevated alcohol use in the care and treatment of older people, and in overcoming their own barriers around discussing this matter with care recipients. However, the strict descriptive analysis may be a limitation. We could have done a more in-depth analysis that could have cast lighter and insights into the topic, but as the experiences between the various practitioner groups were large it was difficult to find a common denominator. A further limitation is that we could also have added illustrative quotes from non-identifiable participant codes, to ensure that the perspectives of different participants were being presented. Furthermore, we could have missed some valuable experiences and reflections in the translation of the findings and quotes in the writing process. In this re-analysis of the study, we presented it descriptive, because the cases represented very different roles as health professionals. The data of this study was collected during a five years period. During this time period we are not aware of any changes in alcohol legislation in Norway or in any changes of attitudes considering the use of alcohol among people in Norway in general.
Implication for Clinical Praxis
We suggest that health personnel providing health care services to older adults, regardless their role practising as a nurse, a nurse’s aide or a GP should be more aware of alcohol as a potential treat for health and well-being and raise a dialog about use of alcohol in care and counselling situations to avoid dependency and poorer health, and more often refer to or start counselling and treatment, if indicated. Co-operation between the various personnel is recommended. Further we, suggest that the general awareness of side effects of us as well of subtle elevated alcohol use among older adults should be raised in the society and treatment options for older adults increased.
Conclusion
Health professionals working in NHs and in-home care and GPs find it difficult to discuss the use and elevated use of alcohol with older people for whom they have care and treatment responsibilities. In general, they are concerned that such conversations infringe on the principles governing individuals’ autonomy. However, because they are aware that elevated alcohol intake may have a negative impact on health and well-being, they also express a need for guidelines around better and open-minded ways to discuss the use and elevated use of alcohol with the care recipients and patients for whom in their care.
Acknowledgment
The authors wish to thank the health professionals who shared their experiences, the Norwegian National Advisory Unit on Ageing and Health, the Faculty of Medicine at the Norwegian University of Science and Technology (NTNU), and the University of South-Eastern Norway, which supported the study.
Author Contributions
Anne-Sofie Helvik and Aud Johannessen were responsible for data collection and much of the analytical work, while the process was discussed continuously with Kjerstin Tevik, Gro Gade Haanes and Knut Engedal. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Klein WC, Jess C. One last pleasure? Alcohol use among elderly people in nursing homes. Health Soc Work. 2002;27(3):193–203. doi:10.1093/hsw/27.3.193
2. Bjørk C, Thygesen LC, Vinther‐Larsen M, Grønbæk MN. Time trends in heavy drinking among middle‐aged and older adults in Denmark. Alcohol Clin Exp Res. 2008;32(1):120–127. doi:10.1111/j.1530-0277.2007.00557.x
3. Bratberg GH, Wilsnack SC, Wilsnack R, et al. Gender differences and gender convergence in alcohol use over the past three decades (1984–2008), The HUNT Study, Norway. BMC Public Health. 2016;16(1):723. doi:10.1186/s12889-016-3384-3
4. Tevik K, Selbæk G, Engedal K, Seim A, Krokstad S, Helvik A-S. Factors associated with alcohol consumption and prescribed drugs with addiction potential among older women and men–the Nord-Trøndelag health study (HUNT2 and HUNT3), Norway, a population-based longitudinal study. BMC Geriatr. 2019;19(1):113. doi:10.1186/s12877-019-1114-2
5. Strandberg TE, Strandberg AY, Salomaa VV, Pitkälä K, Tilvis RS, Miettinen TA. Alcoholic beverage preference, 29-year mortality, and quality of life in men in old age. J Gerontol a Biol Sci Med Sci. 2007;62(2):213–218. doi:10.1093/gerona/62.2.213
6. Aira M, Hartikainen S, Sulkava R. Community prevalence of alcohol use and concomitant use of medication—a source of possible risk in the elderly aged 75 and older? Int J Geriatr Psychiatry. 2005;20(7):680–685. doi:10.1002/gps.1340
7. Tevik K, Selbæk G, Engedal K, Seim A, Krokstad S, Helvik A-S. Use of alcohol and drugs with addiction potential among older women and men in a population-based study. The Nord-Trøndelag health study 2006–2008 (HUNT3). PLoS One. 2017;12(9):e0184428. doi:10.1371/journal.pone.0184428
8. Slagsvold B, Hansen T. Morgendagens eldre-betydningen av økt utdanning for mental helse [The elderly tomorrow-The meaning og more education in relation to mental health]. Tidsskrift Psykologi. 2017;55(1):36–45.
9. Weathermon R, Crabb DW. Alcohol and medication interactions. Alcohol Res Health. 1999;23(1):40–54.
10. Moore AA, Whiteman EJ, Ward KT. Risks of combined alcohol/medication use in older adults. Am J Geriatr Pharmacother. 2007;5(1):64–74. doi:10.1016/j.amjopharm.2007.03.006
11. International Alliance for Responsible Drinking (IARD). Drinking guidelines: general population. 2019. Available from: http://www.iard.org/resources/drinking-guidelines-general-population/.
12. Substans Abuse and Mental Health Services (SAMHSA). Older Americans Behavioral Health. Older Adults. 2012. Available from: https://www.samhsa.gov/dbhis-collections/older-adults.
13. National Institute on Alcohol Abuse and Alcoholisme (NIAAA). Older adults. Available from: https://www.niaaa.nih.gov/alcohol-health/special-populations-co-occurring-disorders/older-adults.
14. Canada Go. Government of Canada — action for Seniors report. 2014. Available from: https://www.canada.ca/en/employment-social-development/programs/seniors-action-report.html.
15. World Health Organization (WHO). Global status report on alcohol and health 2018. 2018. Available from: https://www.who.int/publications/i/item/9789241565639.
16. Sabia S, Fayosse A, Dumurgier J, et al. Alcohol consumption and risk of dementia: 23 year follow-up of Whitehall II cohort study. BMJ. 2018;362:k2927. doi:10.1136/bmj.k2927
17. Schwarzinger M, Pollock BG, Hasan OSM, et al. Contribution of alcohol use disorders to the burden of dementia in France 2008–13: a nationwide retrospective cohort study. Lancet Public Health. 2018;3(3):e124–e132. doi:10.1016/S2468-2667(18)30022-7
18. Langballe EM, Ask H, Holmen J, et al. Alcohol consumption and risk of dementia up to 27 years later in a large, population-based sample: the HUNT study, Norway. Eur J Epidemiol. 2015;30(9):1049–1056. doi:10.1007/s10654-015-0029-2
19. Schonfeld L, King-Kallimanis BL, Duchene DM, et al. Screening and brief intervention for substance misuse among older adults: the Florida BRITE project. Am J Public Health. 2010;100(1):108–114. doi:10.2105/AJPH.2008.149534
20. Mukamal KJ, Mittleman MA, Longstreth W
21. Kalla A, Figueredo VM. Alcohol and cardiovascular disease in the geriatric population. Clin Cardiol. 2017;40(7):444–449. doi:10.1002/clc.22681
22. Caputo F, Vignoli T, Leggio L, Addolorato G, Zoli G, Bernardi M. Alcohol use disorders in the elderly: a brief overview from epidemiology to treatment options. Exp Gerontol. 2012;47(6):411–416. doi:10.1016/j.exger.2012.03.019
23. Wadd S, Papadopoulos C. Drinking behaviour and alcohol-related harm amongst older adults: analysis of existing UK datasets. BMC Res Notes. 2014;7(1):741. doi:10.1186/1756-0500-7-741
24. Crome IB, Wu L-T, Crome P, Rao R. Substance Use and Older People. United States: Wiley Online Library; 2015.
25. Ortolá R, García-Esquinas E, Galán I, Rodríguez-Artalejo F. Patterns of alcohol consumption and health-related quality of life in older adults. Drug Alcohol Depend. 2016;159:166–173. doi:10.1016/j.drugalcdep.2015.12.012
26. Johnson I. Alcohol problems in old age: a review of recent epidemiological research. Int J Geriatr Psychiatry. 2000;15(7):575–581. doi:10.1002/1099-1166(200007)15:7<575::aid-gps151>3.0.co;2-0
27. Mauro PM, Canham SL, Martins SS, Spira AP. Substance-use coping and self-rated health among US middle-aged and older adults. Addict Behav. 2015;42:96–100. doi:10.1016/j.addbeh.2014.10.031
28. Epstein EE, Fischer-Elber K, Al-Otaiba Z. Women, aging, and alcohol use disorders. J Women Aging. 2007;19(1–2):31–48. doi:10.1300/J074v19n01_03
29. Gomberg E. Older women and alcohol. Use and abuse. Recent Dev Alcohol. 1995;12:61–79. doi:10.1007/0-306-47138-8_4
30. Haighton C, Kidd J, O’Donnell A, Wilson G, McCabe K, Ling J. ‘I take my tablets with the whiskey’: a qualitative study of alcohol and medication use in mid to later life. PLoS One. 2018;13(10):e0205956. doi:10.1371/journal.pone.0205956
31. Bareham BK, Kaner E, Spencer LP, Hanratty B. Drinking in later life: a systematic review and thematic synthesis of qualitative studies exploring older people’s perceptions and experiences. Age Ageing. 2019;48(1):134–146. doi:10.1093/ageing/afy069
32. Holdsworth C, Frisher M, Mendonca M, De Oliveiria C, Pikhart H, Shelton N. Lifecourse transitions, gender and drinking in later life. Ageing Soc. 2017;37(3):462–494. doi:10.1017/S0144686X15001178
33. Hellum R, Bjerregaard L, Nielsen AS. Factors influencing whether nurses talk to somatic patients about their alcohol consumption. Nord Stud Alcohol Drugs. 2016;33(4):415–436. doi:10.1515/nsad-2016-0034
34. Johannessen A, Helvik A-S, Engedal K, Sorlie VM. Older peoples‘ narratives of use and misuse of alcohol and psychotropic drugs. Scand J Caring Sci. 2016;30(3):586–593. doi:10.1111/scs.12282
35. Johannessen A, Engedal K, Helvik A-S. Use and misuse of alcohol and psychotropic drugs among older people: is that an issue when services are planned for and implemented? Scand J Caring Sci. 2015;29(2):325–332. doi:10.1111/scs.12166
36. Lid TG. Addressing Alcohol in General Practice [Doctoral thesis]. Stavanger: University of Stavanger; 2016.
37. Lunde L. Alkoholvaner og problematisk alkoholbruk blant eldre Kunnskapsstatus [Alcohol habits and problematic alcool use among elderly- knowlwdge base]. In: Mobæk R, Nesvåg S, editors. Eldres Rusmiddelbruk. Utredning Til Helse – Og Omsorgsdepartementet [The Elderlies Misuse]. Stavanger: Stavanger KORFOR; 2015;10–31
38. Bareham BK, Kaner E, Spencer L, Hanratty B. Health and social care providers’ perspectives of older people’s drinking: a systematic review and thematic synthesis of qualitative studies. Age Ageing. 2020;49(3):453–467. doi:10.1093/ageing/afaa005
39. Naci H, Ioannidis JP. Evaluation of wellness determinants and interventions by citizen scientists. JAMA. 2015;314(2):121–122. doi:10.1001/jama.2015.6160
40. World Health Organization (WHO). Strategy and Action Plan for Healthy Ageing in Europe, 2012–2020. World Medical Organization; 2012.
41. Yin RK. Case Study Research.
42. Berg BL, Lune H. Qualitative Research Methods for the Social Sciences. California: Pearson; 2017.
43. Lindseth A, Norberg A. A phenomenological hermeneutical method for researching lived experience. Scand J Caring Sci. 2004;18(2):145–153. doi:10.1111/j.1471-6712.2004.00258.x
44. Flyvbjerg B. Five misunderstandings about case-study research. Qual Inq. 2006;12(2):219–245. doi:10.1177/1077800405284363
45. Thorsen K, Johannessen A. Personsentrert omsorg i praksis: fire perspektiver på støttekontakttjenesten i demensomsorgen-en case studie [Person-centred care in practice: four perspectives on the support contact service in dementia care – a case study design]. Nordisk Tidsskrift Helseforskning. 2018;14:2. doi:10.7557/14.4323
46. Kvale S, Brinkmann S. Det Kvalitative Forskningsintervju [The Qualitative Research Interview]. Oslo: Gyldendal akademisk; 2009.
47. Johannessen A. Dementia and Public Health - with Focus on Access to Society [Doctoral thesis]. Gothenborg: Nordic School of Public Health; 2012.
48. Möller A, Nyman E. Why, what and how?–questions for psychological research in medicine. Disabil Rehabil. 2005;27(11):649–654. doi:10.1080/09638280400018551
49. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
50. Johannessen A, Tevik K, Engedal K, Helvik A-S. Health professionals’ experience of nursing home residents’ consumption of alcohol and use of psychotropic drugs. Nord Stud Alcohol Drugs. 2020;1–14. doi:10.1177/1455072520961890
51. Johannessen A, Engedal K, Helvik A-S. Use and misuse of alcohol and psychotropic drugs among older people: is that an issue when services are planned for and implemented? Scand J Caring Sci. 2017;29(2):25–332. doi:10.1111/scs.12166
52. Ricoeur P. Interpretation Theory: Discourse and the Surplus of Meaning. TCU press; 1976.
53. Johannessen A, Helvik A-S, Engedal K, Ulstein I, Sørlie V. Prescribers of psychotropic drugs experiences and reflections on use and misuse of alcohol and psychotropic drugs among older people: a qualitative study. Qual Prim Care. 2015;23(3):134–140.
54. Brown L, Tappan MB, Gillian C, Miller BA, Argyris DE. Reading for self and moral voice: a method of interpreting narratives of real-life moral conflicts and choice. In: Packer MJ, Addison RB, editors. Entering the Circle. Hermenautic Investigation in Psychology. Albany: University of New Yourk Press; 1989:141–154.
55. World Medical Association (WMA). Declaration of Helsinki. 2013. Available from: http://www.wma.net/en/30publications/10policies/b3/index.html.
56. Kelfve S, Agahi N, Mattsson AD, Lennartsson C. Increased alcohol use over the past 20 years among the oldest old in Sweden. Nord Stud Alcohol Drugs. 2014;31(3):245–260. doi:10.2478/nsad-2014-0020
57. Halvorsen KH, Granas AG, Engeland A, Ruths S. Prescribing quality for older people in Norwegian nursing homes and home nursing services using multidose dispensed drugs. Pharmacoepidemiol Drug Saf. 2012;21(9):929–936. doi:10.1002/pds.2232
58. Fog AF, Kvalvaag G, Engedal K, Straand J. Drug-related problems and changes in drug utilization after medication reviews in nursing homes in Oslo, Norway. Scand J Prim Health Care. 2017;35(4):329–335. doi:10.1080/02813432.2017.1397246
59. Dare M, Schirmer J, Vanclay F. Community engagement and social licence to operate. Impact Assess Proj Apprais. 2014;32(3):188–197. doi:10.1080/14615517.2014.927108
60. Henley LJ, O’Donoghue K, Dale M. New Zealand based social worker’s perceptions on assessments of older adults and alcohol use. Practice. 2019;31(2):135–151. doi:10.1080/09503153.2018.1477930
61. Næss O, Nesvåg S. Vurdering av helsetjenester for eldre med alkoholrelaterte problemer: hva virker og hva kan bli bedre? [Consideration of healthcare for elderly with alcohol misuse: what works and what do not?]. Nord Stud Alcohol Drugs. 2017;34(1):91–96. doi:10.1177/1455072516682635
62. Leurs P, Huvent-Grelle D, Lelievre-Leroy S, Roche J, Puisieux F. Alcohol consumption patterns in older people living in nursing homes. Presse Med. 2010;39(12):e280–e288. doi:10.1016/j.lpm.2010.02.054
63. Menecier-Ossia L, Kholler M, Moscato A, Menecier P. Alcohol in care homes for the elderly. Soins Gerontol. 2014;106:34–36. doi:10.1016/j.lpm.2010.02.054
64. Lov om pasient- og brukerrettigheter. Act on Patients- and Users Rights. Oslo: Helse- og omsorgsdepartementet [Health- and Department of Care]; 2020.
65. Kitwood T. Dementia Reconsidered. The Person Comes First. Norfolk: Open University Press; 1997.
66. Edvardsson D, Winblad B, Sandman P-O. Person-centred care of people with severe Alzheimer’s disease: current status and ways forward. Lancet Neurol. 2008;7(4):362–367. doi:10.1016/s1474-4422(08)70063-2
67. McCormack B, Kitson A, Harvey G, Rycroft-Malone J, Titchen A, Seers K. Getting evidence into practice: the meaning of ‘context’. J Adv Nurs. 2002;38(1):94–104. doi:10.1046/j.1365-2648.2002.02150.x
68. McCormack B, McCance T. Person-Centred Practice in Nursing and Health Care: Theory and Practice. West Sussex: John Wiley & Sons; 2016.
69. World Health Organization (WHO). The Global Burden of Disease: 2004 Update. World Health Organization; 2008. https://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/.
70. Leber DA, Vanoli EG. Therapeutic use of humor: occupational therapy clinicians’ perceptions and practices. Am J Occup Ther. 2001;55(2):221–226. doi:10.5014/ajot.55.2.221
71. Lal R, Pattanayak RD. Alcohol use among the elderly: issues and considerations. J Geriatr Ment Health. 2017;4(1):4. doi:10.4103/jgmh.jgmh3416
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.