Back to Journals » Nursing: Research and Reviews » Volume 15
Health Literacy Mediates Racial Differences in Cognitive Functioning Among African American/Black and White People with and without HIV in the Deep South
Authors Delgadillo JD ![]() , Beltran-Najera I, Long AR
, Beltran-Najera I, Long AR ![]() , Haase SR, Vickers JK, Woods SP, Vance DE
, Haase SR, Vickers JK, Woods SP, Vance DE ![]() , Fazeli PL
, Fazeli PL ![]()
Received 30 April 2025
Accepted for publication 4 November 2025
Published 13 November 2025 Volume 2025:15 Pages 177—191
DOI https://doi.org/10.2147/NRR.S520064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Ferry Efendi
Jeremy D Delgadillo,1 Ilex Beltran-Najera,2 Alexis R Long,3 Shakaye R Haase,1 Jasmine K Vickers,3 Steven Paul Woods,2 David E Vance,3 Pariya L Fazeli3
1University of Alabama at Birmingham, Department of Psychology, Birmingham, AL, USA; 2University of Houston, Department of Psychology, Houston, TX, USA; 3University of Alabama at Birmingham, School of Nursing, Birmingham, AL, USA
Correspondence: Pariya L Fazeli, University of Alabama at Birmingham, School of Nursing, NB 470C, 1720 2nd Avenue South, Birmingham, AL, 35294-1210, USA, Email [email protected]
Purpose: Disparities in cognition among middle-aged and older African American/Black adults are evident, especially among people living with HIV (PLWH). Though disparities in health literacy among African American/Black adults impact health outcomes across clinical populations, its role in racial differences in cognition among PLWH is not well understood. This study aimed to determine if health literacy mediated racial differences in cognition among PLWH and people living without HIV (PLWoH).
Patients and Methods: Measures of oral word literacy (Wide Range Achievement Test-3rd Edition), health literacy (Test of Functional Literacy in Adults – Reading Comprehension subtest, Rapid Estimate of Adult Literacy in Medicine, Newest Vital Sign, Expanded Numeracy Scale), and cognition (gold standard neurocognitive battery) were examined in 273 participants (170 PLWH: 86% African American/Black; 103 PLWoH: 65% African American/Black) via secondary analysis. Multivariable linear regressions (MLRs) among PLWH and PLWoH examined associations between health literacy and cognition, accounting for relevant covariates, followed by adjusted bootstrap confidence interval mediation analyses to determine whether health literacy mediated the association between race and cognition.
Results: In both samples, White people scored higher than African American/Black people on measures of cognition, health literacy, oral word literacy, and SES. Adjusted MLRs in PLWH and PLWoH separately showed health literacy was associated with cognition (PLWH: b =0.205, p =0.007; PLWoH: b = 0.354, p =0.002). Health literacy significantly mediated the association between race and cognition, independent of covariates (PLWH: effect =0.055, 95% CI [0.0048, 0.1973]; PLWoH: effect =0.093, 95% CI [0.0276, 0.1827]).
Conclusion: These results underscore the importance of health literacy in explaining racial disparities in cognition among African American/Black PLWH and PLWoH in the Deep South. Findings have implications for guiding the development of health literacy interventions, which may have downstream positive impacts on cognition.
Keywords: health disparities, neurocognitive disorders, infectious disease, race and ethnicity, cultural psychology, neuropsychological assessment
Introduction
Race and HIV
The United States (US) Deep South (a region including the following states: AL, FL, GA, LA, MS, NC, SC, TN, TX), is an epicenter of the US HIV epidemic, where people living with HIV (PLWH) experience the poorest outcomes compared to PLWH in other US regions. In addition to the Deep South contributing to over 52% of HIV diagnoses in 2022,1 the US Deep South also has the highest rates of infection and HIV-related deaths.2 The primary contributor to the US Deep South having the worst HIV outcomes is attributed to the racial disparities in HIV outcomes among certain populations, particularly African Americans/Black people. Even though African American/Black people made of 13% of the US population in 2019, African American/Black people made up 40% of PLWH.3 Despite HIV incidence rates having decreased by approximately 18% from 2018 to 2022 among African American/Black people, they were nearly 8 times more likely to receive an HIV diagnosis compared to White people in 2022.1 Further, African American/Black PLWH also have significantly worse HIV care continuum compared to White PLWH (ie, receive care, care retention, viral suppression), highlighting the significant racial disparities in HIV outcomes among African American/Black PLWH.1–4
HIV, Race, and Cognition
These health disparities among African American/Black PLWH may ultimately increase the risk for developing HIV-associated neurocognitive disorder (HAND), a spectrum of cognitive impairment ranging from mild to severe impairments disrupting functional independence, which have an estimated prevalence of 30–50%5,6 and can present even among PLWH with well-control HIV.7 HIV damages the central nervous system via several mechanisms including release of viral proteins and neuroinflammation.8 A meta-analysis on the global HAND prevalence indicated it to be highest among people with more severe history of HIV (ie, low nadir CD4).9 As PLWH age, they are also at risk for other neurodegenerative disorders such as Alzheimer’s disease and related dementias (ADRD). In fact, dementia incidence rates have been estimated to be 1.2–3.7 times higher among PLWH than people living without HIV (PLWoH).10
The higher prevalence and incidence rates of ADRD among African American/Black people compared to Whites has been well-established in the general population.11,12 Research in PLWH has shown that African American/Black people and Hispanics have significantly worse cognitive outcomes compared to Non-Hispanic Whites. In a sample of African American/Black PLWH (N = 116) and White PLWH (N = 105) aged 50 and older, African American/Black PLWH had significantly worse memory and learning performance compared to White PLWH.13 Another study14 found that Non-Hispanic African American/Black PLWH had significantly worse global and domain (eg, learning, executive functioning) cognitive functioning than Non-Hispanic White and Hispanic PLWH. Another study found that African American/Black PLWH were more likely to meet criteria for neurocognitive disorders than White PLWH (45% vs 17%, respectively).15 Increased rates of HAND among African American/Black people may partially be attributed to the greater prevalence of risk factors for HAND, including but not limited to cardiometabolic disorders (eg, diabetes and hypertension),16 psychiatric comorbidities (eg, anxiety and depression, HIV disease severity),17 and social comorbidities (eg, low education, poverty, trauma).18 Understanding factors associated with poorer cognitive outcomes among African American/Black PLWH is challenging given issues related to culturally relevant cognitive tests and psychometrics/norming. Furthermore, examination of the influence of social determinants of health on cognitive outcomes among African American/Black PLWH is needed.19
Health Literacy
Unequal quality in primary schooling provided to African American/Black populations in the Deep South has played a role in the current literacy disparities that are present in older African American/Black PLWH and PLWoH alike.20,21 Disparities in health literacy are one potential mechanism leading to poorer health outcomes and cognitive function among African American/Black PLWH. Health literacy can be understood as, “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions”.22 African American/Black PLWH are at particular risk for low health literacy,23 which may be attributable to various social determinants of health.
Health literacy has shown to influence ethnoracial disparities in neuropsychological functioning in other populations,24 but we know little about its influence in HIV disease. One study25 found in a sample of African American/Black and White PLWH that health literacy significantly mediated the association between race and global and domain (eg, attention/working memory) cognitive functioning. These findings converge with studies showing that general language literacy is associated with cognitive outcomes among African American/Black PLWH. For example, one study26 found that lower scores on the HIV Dementia Scale (a cognitive screener) among African American/Black PLWH were partially explained by reading scores from the Weschler Test of Adult Reading (WTAR), an accepted measure of literacy that serves as a proxy for quality of education.27
Despite the evidence that there are racial disparities among African American/Black PLWH in HIV outcomes as well as non-HIV-related comorbidities16–18 and that health literacy that may have downstream impacts on cognitive functioning, little research has examined if health literacy explains racial differences in cognitive functioning in PLWH. Of the two studies that have examined how health literacy and oral word literacy mediate racial differences in cognitive functioning in African American/Black and White PLWH,25,26 both studies lacked HIV-negative comparison groups, and included samples of PLWH that were relatively young (mean ages ~40–50), not representing older adulthood where declines in cognitive functioning are most pronounced. Furthermore, no studies have investigated these relationships within samples from the US Deep South, a population of PLWH that are largely African American/Black and that present with the worst HIV outcomes of any US region. Our study also uniquely expands upon previous research by examining specific components of health literacy that may drive racial differences. Thus, the purpose of the current study was to understand the relationship between health literacy and cognitive functioning among a sample of middle-aged and older African American/Black and White PLWH and PLWoH from the Deep South. The first aim was to determine if health literacy was associated with cognitive functioning when accounting for relevant covariate(s) among PLWH and PLWoH separately. The second aim was to determine if health literacy mediated racial differences in cognitive functioning, when accounting for relevant covariate(s). Inverse mediation models were also performed to confirm directionality (ie, examine whether cognitive functioning explains racial differences in health literacy), as various conceptual models have suggested that cognitive functioning may have upstream effects on health literacy,28 and that the relationship between health literacy and cognitive functioning may also be reciprocal.29 Post-hoc analyses from the mediation models performed for aim 2 were conducted to determine which specific health literacy domains (ie numeracy and reading) uniquely mediated the relationship between race and global cognitive function.
Materials and Methods
Participants and Procedure
The current study is a cross-sectional secondary analysis of observational data collected from September 2016 through July 2019. Participants in the current study included 273 middle-aged and older PLWH (n = 170; 86% African American/Black) and PLWoH (n = 101; 65% African American/Black) from Birmingham, Alabama. PLWH were recruited from a parent RCT (after completing the baseline assessment for that study, they were invited to do the additional study measures used in the current study),30 which had the following inclusion criteria: aged 40+ years, a patient at the university HIV/AIDS clinic, not having a major health condition(s) that may affect cognitive function (eg, Alzheimer’s disease, schizophrenia), no major vision or hearing impairments, no prior head injury with loss of consciousness greater than 30 minutes, and not undergoing radiation or chemotherapy at the time of the study. PLWoH were recruited for a parent observational study via flyers in the community and a university online ad listing studies. Inclusion criteria were the same as for PLWH, with the exception that PLWoH were aged 50+ years. The rationale for the different age cut-off between PLWH and PLWoH was due to aims of the parent studies and because cognitive declines may have an earlier onset in PLWH. This study was funded by the National Institute on Aging, was approved by the UAB Institutional Review Board (protocol # 160601006), and was conducted in accordance with the Declaration of Helsinki. After written informed consent was obtained, participants completed questionnaires and measures, including a comprehensive neurocognitive battery, and measures of demographic characteristics, health literacy, and oral word literacy.
Measures
Sociodemographic Characteristics
Sociodemographic characteristics were obtained via self-report questionnaire and consisted of: age, race/ethnicity, sex, total years of education, and annual household income (ie 1 = $0 – $10,000 to 11 = $100,000 and above). Oral word literacy was determined from the reading subtest of the Wide Range Achievement Test-3rd Edition (WRAT-3),31 an established proxy for quality of education.27 A socioeconomic status (SES) composite Z-score was created given the conceptual overlap and collinearity between total years of education and annual household income (PLWH: Spearman’s r =0.476, p <0.001; PLWoH: Spearman’s r =0.571, p <0.001).32,33 Sample descriptive and clinical characteristics across the HIV and racial groups are displayed in Table 1.
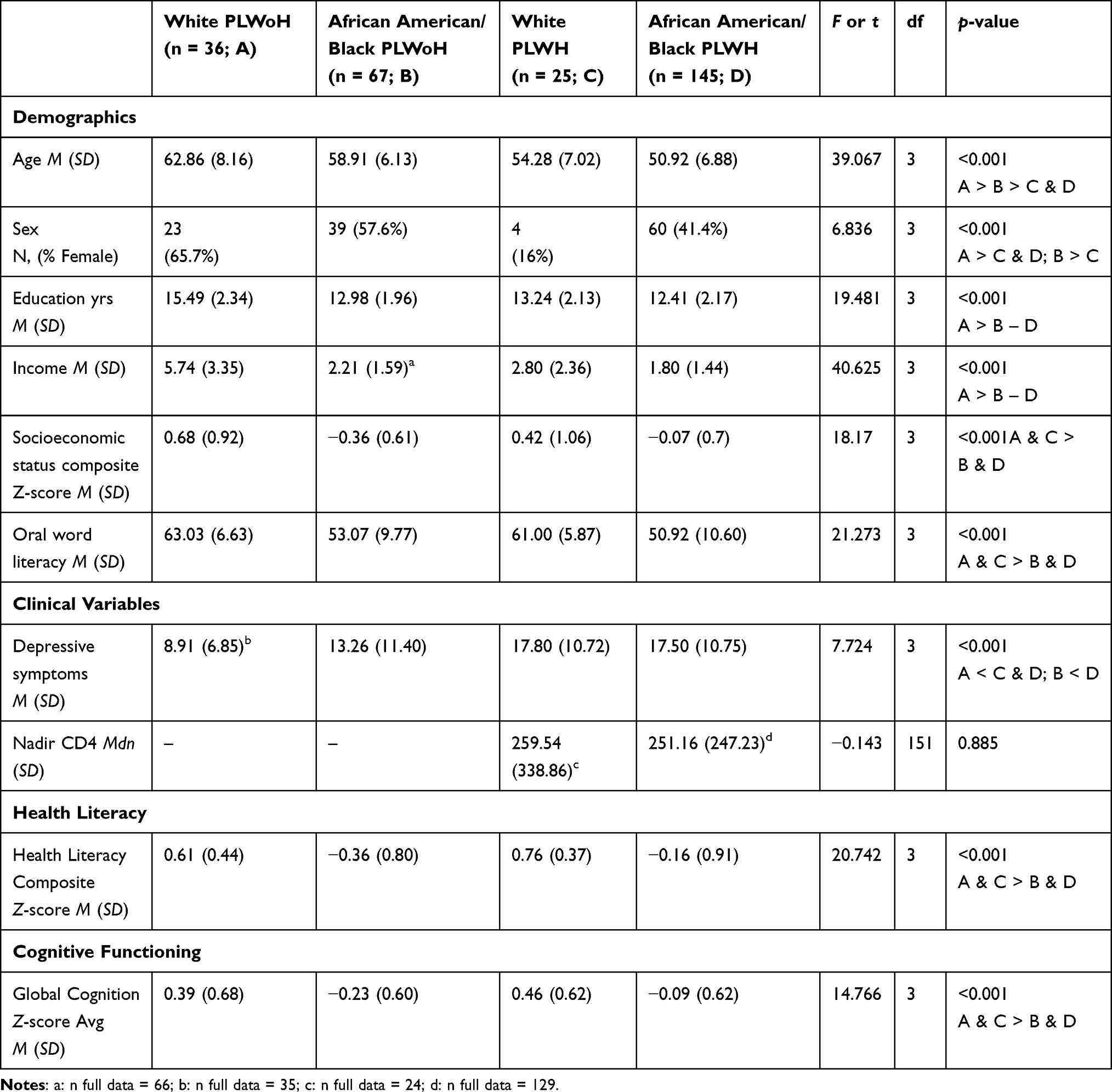 |
Table 1 Demographic and Clinical Statistics by HIV Status and Race |
Neurocognitive Functioning
The neurocognitive battery assessed seven major cognitive domains, including speed of information processing, learning, memory, executive functioning, verbal fluency, attention and working memory, and motor functioning5 (see Table 2). A sample-based global cognition Z-score composite was calculated from the raw scores, with higher scores reflecting better functioning. The rationale for using a sample-based Z-score for global cognition functioning instead of a normed T score was to have a clearer comparison of racial difference in cognitive functioning, given the known norming issues among African American/Black adults.34
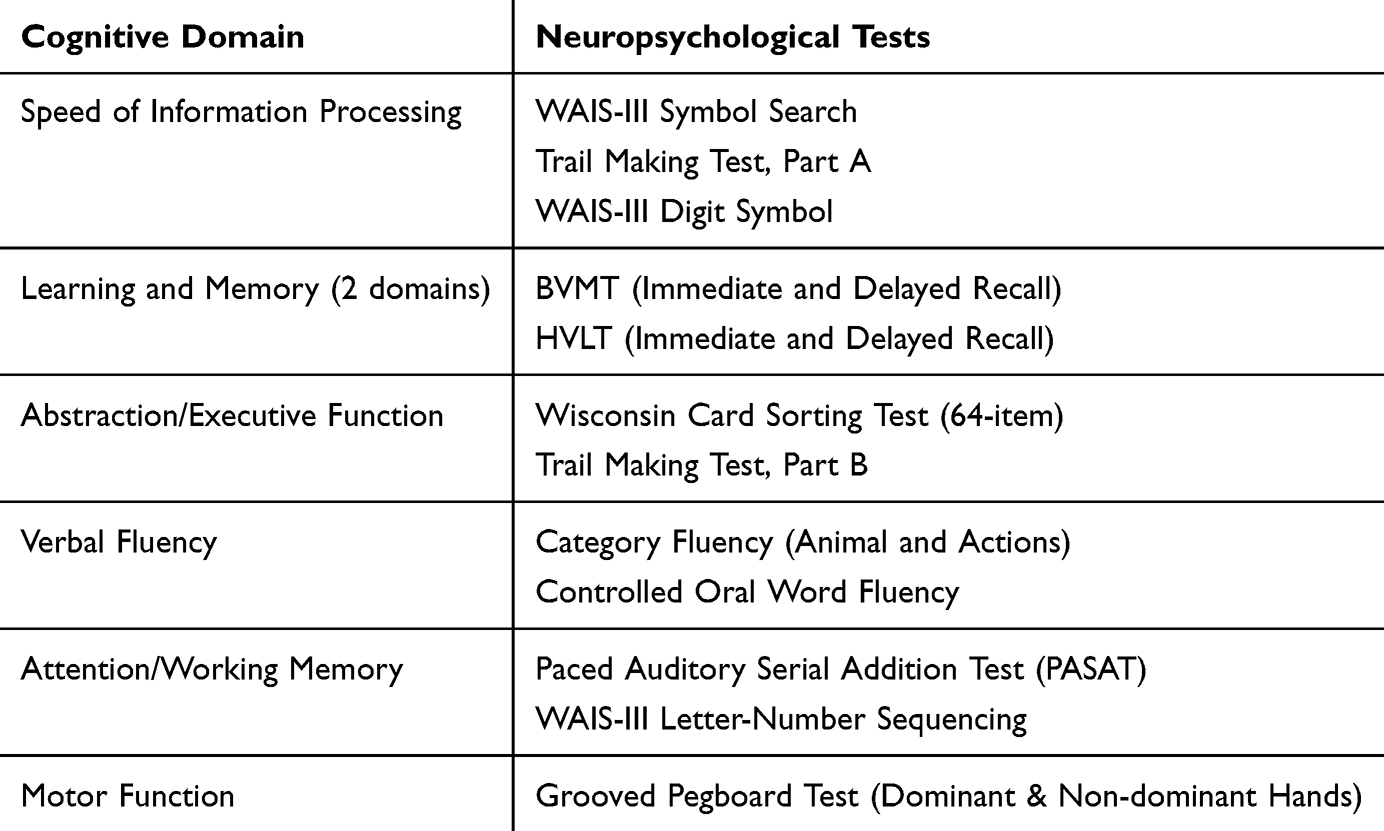 |
Table 2 Neuropsychological Test Battery by Cognitive Domain |
Health Literacy
The following health literacy measures were administered to ensure there were two reading measures and two numeracy measures: the Test of Functional Literacy in Adults (TOFHLA) Reading Comprehension subtest,35 the Rapid Estimate of Adult Literacy in Medicine (REALM),36 the Newest Vital Sign (NVS),37 and the Expanded Numeracy Scale (ENS).38 The TOFHLA Reading Comprehension subtest includes 50-items, with high higher scores indicating greater health literacy (scores ranging between 16 and 50). The REALM is a 66-item measure used to assess the capacity to recognize and accurately pronounce health-related words (eg, “jaundice”, “colitis”, “impetigo”). The total scores range from 0 to 66, with scores ≤ 60 used to indicate limited health literacy. The NVS is a 6-item measure of health literacy (numeracy) that is performance-based, requiring participants to answer questions about an ice cream nutrition label (eg, “If you are allowed to eat 60 grams of carbohydrates as a snack, how much ice cream could you have?”). Scores can range from 0 to 6, with higher scores indicating greater health literacy. Lastly, the ENS is a 7-item activity designed to assess one’s fundamental competency with mathematical concepts in the context of perceived health risks (eg “Which of the following numbers represents the biggest risk of getting a disease: 1%, 10%, or 5%?”). Scores range between 0 and 7, with higher scores indicating greater understanding of health risks. After calculating sample-based Z-scores for each of the health literacy measures, a health literacy Z-composite score was created, following the approach suggested by Matchanova et al.39 We also examined individual domain (numeracy vs reading) Z-scores of the health literacy measures in subanalyses.40
Clinical Variables
The Center for Epidemiological Studies – Depression41 was used to assess depressive symptoms, with scores of 16 or greater considered as clinically relevant. HIV disease characteristics were derived from interview and clinic records, and included current and nadir CD4 count, estimated duration of HIV disease, plasma viral load, and treatment status. Participants also provided urine samples for toxicology (TransMedR) for five illicit substances (ie marijuana, amphetamines, cocaine, methamphetamine, and opiates).
Statistical Analyses
Statistical analyses were conducted in JMP Pro Version 1442 and R version 4.1.43 In order to calculate the sample-based composite Z-scores for the cognitive domains, we used the following equation for each neurocognitive measure:  [eg, individual score on Controlled Oral Word Fluency (COWF) subtracted by the average score on COWF all divided by the standard deviation of COWF; individual scores on Category Fluency – Animal and Actions (CF-AA) subtracts by the average score on the CF-AA all divided by the standard deviation of CF-AA]. Afterwards, we obtained the mean z-score for each of the cognitive domains by taking the mean from the previously calculated z-scores (eg Verbal Fluency
[eg, individual score on Controlled Oral Word Fluency (COWF) subtracted by the average score on COWF all divided by the standard deviation of COWF; individual scores on Category Fluency – Animal and Actions (CF-AA) subtracts by the average score on the CF-AA all divided by the standard deviation of CF-AA]. Afterwards, we obtained the mean z-score for each of the cognitive domains by taking the mean from the previously calculated z-scores (eg Verbal Fluency  ). We then created the global cognitive functioning Z-score by obtaining the mean Z-score from all of the cognitive domains Z-scores. One-way ANOVAs were performed to determine if there were significant differences by race/HIV-status groups (ie, four groups) and to characterize the sample. To determine covariates for the multiple linear regressions and mediation analyses as well as confirm conditions for mediation were met, correlation analyses were performed among PLWH and PLWoH separately, determining which demographic and clinical variables listed in Table 1 were associated with race, health literacy, and global cognitive functioning.44 Variables that were associated with race, health literacy, and global cognitive functioning were entered as covariates in the linear regression and mediation analyses. For the linear regression analyses, we examined within PLWH and PLWoH separately whether health literacy was associated with cognitive functioning. Specifically, for the mediation, we examined within PLWH and PLWoH separately whether health literacy mediated the association between race and cognitive functioning (see Figure 1), followed by inverse mediation models where we examined within PLWH and PLWoH separately whether cognitive functioning mediated the association between race and health literacy. For the post hoc analyses, mediation analyses were performed to determine which specific domains of health literacy (ie, numeracy and reading) mediated the association between race and cognitive functioning among PLWH and PLWoH separately. Post hoc power calculations were conducted per Fritz and MacKinnon’s specifications45 and determined that for PLWH (n = 170) the sample size has approximately 80% power to detect combinations a*b of at least H*H in magnitude, where H stands for Halfway between small and medium effect (ie, each standardized coefficient (a and b), of at least 0.26 in magnitude in the population). The post hoc power calculation for PLWoH (n=103) indicated it would be approximately 80% power to detect a*b combinations slightly higher in magnitude than H*M where H is as above and M is a medium effect (ie, a standardized coefficient of at least 0.39 in magnitude in the population).
). We then created the global cognitive functioning Z-score by obtaining the mean Z-score from all of the cognitive domains Z-scores. One-way ANOVAs were performed to determine if there were significant differences by race/HIV-status groups (ie, four groups) and to characterize the sample. To determine covariates for the multiple linear regressions and mediation analyses as well as confirm conditions for mediation were met, correlation analyses were performed among PLWH and PLWoH separately, determining which demographic and clinical variables listed in Table 1 were associated with race, health literacy, and global cognitive functioning.44 Variables that were associated with race, health literacy, and global cognitive functioning were entered as covariates in the linear regression and mediation analyses. For the linear regression analyses, we examined within PLWH and PLWoH separately whether health literacy was associated with cognitive functioning. Specifically, for the mediation, we examined within PLWH and PLWoH separately whether health literacy mediated the association between race and cognitive functioning (see Figure 1), followed by inverse mediation models where we examined within PLWH and PLWoH separately whether cognitive functioning mediated the association between race and health literacy. For the post hoc analyses, mediation analyses were performed to determine which specific domains of health literacy (ie, numeracy and reading) mediated the association between race and cognitive functioning among PLWH and PLWoH separately. Post hoc power calculations were conducted per Fritz and MacKinnon’s specifications45 and determined that for PLWH (n = 170) the sample size has approximately 80% power to detect combinations a*b of at least H*H in magnitude, where H stands for Halfway between small and medium effect (ie, each standardized coefficient (a and b), of at least 0.26 in magnitude in the population). The post hoc power calculation for PLWoH (n=103) indicated it would be approximately 80% power to detect a*b combinations slightly higher in magnitude than H*M where H is as above and M is a medium effect (ie, a standardized coefficient of at least 0.39 in magnitude in the population).
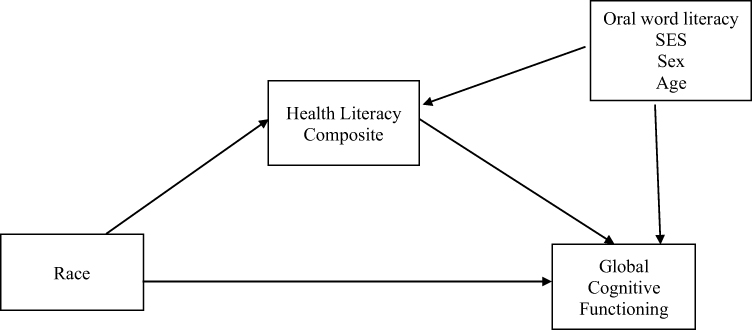 |
Figure 1 Mediation Pathway. |
Results
PLWoH were significantly (p’s <0.01) older, had greater representation of females and Whites, had more years of education, higher annual income, higher oral word literacy, and fewer depressive symptoms than PLWH. When examining racial differences within PLWH and PLWoH separately, White PLWoH were significantly (p’s <0.01) older, had higher SES (ie, more years of education and higher annual income), higher oral word literacy, higher health literacy, and higher global cognitive functioning than African American/Black PLWoH. Similarly, within PLWH, White PLWH had higher SES, higher oral word literacy, higher health literacy, and higher global cognitive functioning than African American/Black PLWH. More details on the specific differences found between the four groups are shown in Table 1. Descriptive analyses revealed few instances of missingness. One data point on income was missing among African American/Black PLWoH, one data point on depressive symptoms was missing among White PLWoH, 16 data points on Nadir CD4 were missing among African American/Black PLWH, and one data point on Nadir CD4 was missing among White PLWH. Therefore, missingness was handled with listwise deletion.
To determine which variable(s) to include in the multiple linear regression and mediation models as covariates, correlation analyses were performed. Variables correlated with all three primary variables of interest (ie, race, health literacy, cognitive functioning) were included as covariates. Correlation analyses among PLWH revealed SES and oral word literacy to be the only variables that correlated with race (SES: r =0.205, p <0.01; oral word literacy: r =0.336, p <0.01), health literacy (SES: r =0.451, p <0.01; oral word literacy: r =0.834, p <0.01), and cognitive functioning (SES: r =0.460, p <0.01; oral word literacy: r =0.627, p <0.01). Similar to PLWH, correlation analyses among PLWoH revealed SES and oral word literacy to be correlated with race (SES: r =0.563, p <0.01; oral word literacy: r =0.478, p <0.01), health literacy (SES: r =0.649, p <0.01; oral word literacy: r =0.859, p <0.01), and cognitive functioning (SES: r =0.650, p <0.01; oral word literacy: r =0.609, p <0.01). Thus, oral word literacy and SES were selected as covariates due to the above-mentioned associations, while age and sex were included as covariates given their conceptual relevance.
The linear regression in PLWH showed higher health literacy was significantly associated with higher cognitive functioning [R2 =0.517, F(6, 163) = 29.100, p <0.001; b =0.205, p =0.007], when accounting for race, age, sex, SES, and oral word literacy. The linear regression in PLWoH showed that higher health literacy was significantly associated with higher cognitive functioning [R2 =0.618, F(6, 96) = 25.905, p <0.001; b =0.354, p =0.003], when accounting for race, age, sex, SES, and oral word literacy. See Table 3 for full results.
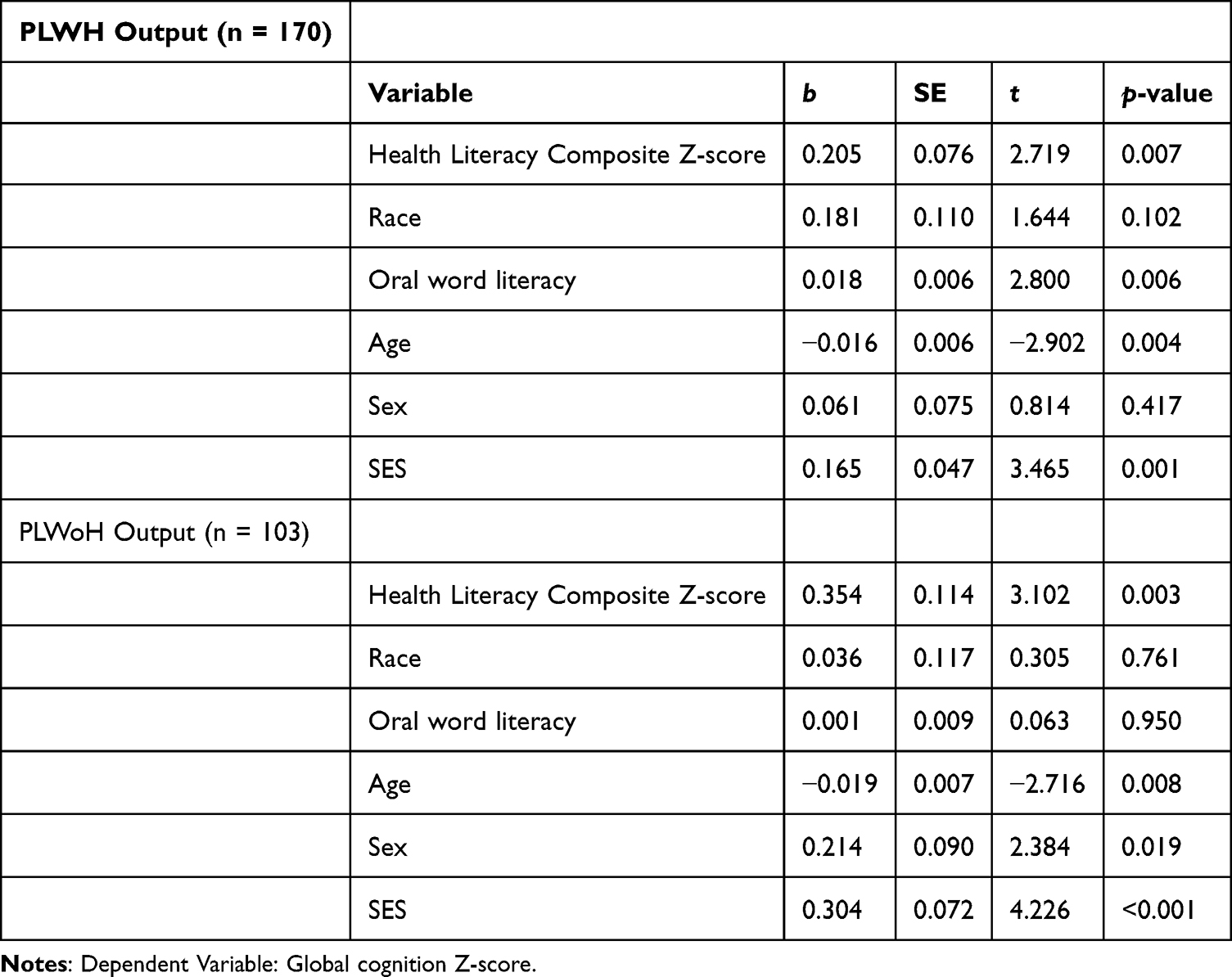 |
Table 3 Health Literacy Predicts Global Cognitive Function |
The mediation analysis in PLWH showed that health literacy (indirect effect =0.055, 95% CI [0.0048, 0.1973]; partially standardized mediated effect =0.084) significantly mediated the association between race and global cognitive functioning, independent of oral word literacy, age, sex, and SES (see Figure 2), with 23.3% [indirect effect (0.055) divided by the total effect (indirect effect + direct effect)] of the total variance in global cognitive functioning being explained by the mediating effect of health literacy. The indirect pathways indicated that the association between race and health literacy was significant (b =0.267, 95% CI [0.0467, 0.4882], p =0.018), as well as the association between health literacy and global cognitive functioning (b =0.205, 95% CI [0.0562, 0.3546], p =0.007). While higher oral word literacy, younger age, and higher SES were associated with higher global cognitive functioning (oral word literacy: b =0.018, 95% CI [0.0052, 0.0301], p =0.006; age: b = −0.016, 95% CI [−0.0269, −0.0051], p =0.004; SES: b =0.164, 95% CI [0.0708, 0.2582], p <0.001), the direct effect of race was not significantly associated with global cognitive functioning (b =0.181, 95% CI [−0.0364, 0.3473], p =0.102) nor was sex significantly associated with global cognitive functioning (b =0.061, 95% CI [−0.0876, 0.2103], p =0.417). The inverse mediation analysis in PLWH showed that global cognitive functioning (indirect effect =0.049, 95% CI [−0.0000, 0.1225]) did not mediate the association between race and health literacy, independent of oral word literacy, age, sex, and SES. The indirect pathways indicated that the association between race and global cognitive functioning was significant (b =0.236, 95% CI [0.0182, 0.4536], p =0.034), as well as the association between global cognitive functioning and health literacy (b =0.211, 95% CI [0.0578, 0.3645], p =0.007). While higher oral word literacy and younger age were associated with higher health literacy (oral word literacy: b =0.059, 95% CI [0.0504, 0.0685], p <0.001; age: b = −0.017, 95% CI [−0.0282, −0.0062], p =0.002), the direct effect of race on health literacy approached significance (b =0.218, 95% CI [−0.0019, 0.4372], p =0.052). Sex was not significantly associated with health literacy (b = −0.004, 95% CI [−0.1551, 0.1475], p =0.960), while the association between SES and health literacy approached significance (b =0.096, 95% CI [−0.0017, 0.1930], p =0.054). In summary, mediation findings indicated that White PLWH were expected to obtain higher global cognitive functioning than African American/Black PLWH through the partial mediating effect of higher health literacy, and that the inverse mediating effect of global cognitive functioning on racial differences in health literacy among PLWH was not observed.
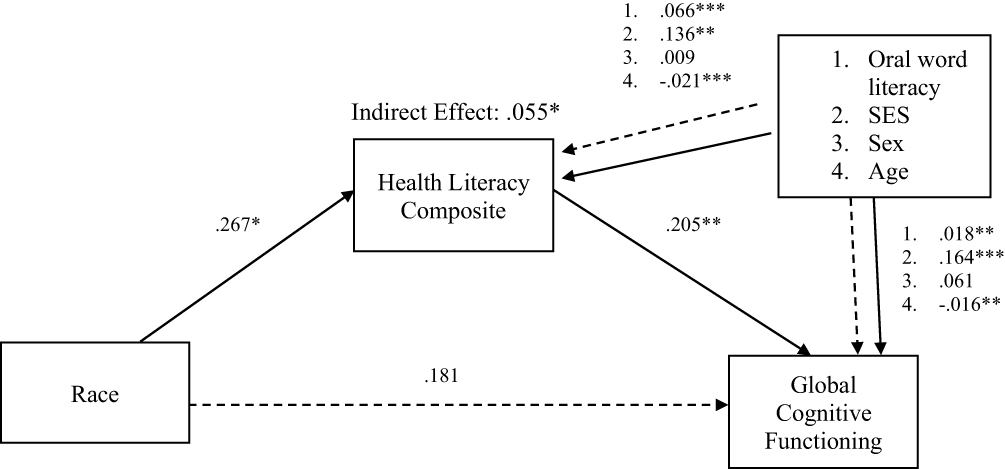 |
Figure 2 Mediation among PLWH. Notes: * p <0.05, ** p <0.01, *** p <0.001. |
Similarly, the mediation analysis in PLWoH showed that health literacy (indirect effect =0.093, 95% CI [0.0276, 0.1827]; partially standardized mediated effect =0.134) significantly mediated the association between race and global cognitive functioning, independent of oral word literacy, age, sex, and SES (see Figure 3), with 72.1% of the total variance being in global cognitive functioning explained by the mediating effect of health literacy. The indirect pathways indicated that the association between race and health literacy was significant (b =0.263, 95% CI [0.0628, 0.4633], p =0.011), in addition to the association between health literacy and global cognitive functioning (b =0.354, 95% CI [0.1275, 0.5805], p =0.002). While oral word literacy and the direct effect of race were not associated with global cognitive functioning (oral word literacy: b =0.001, 95% CI [−0.0175, 0.0187], p =0.949; race: b =0.036, 95% CI [−0.1971, 0.2686], p =0.761), the other covariates were significantly associated with global cognitive functioning (age: b = −0.019, 95% CI [−0.323, −0.0050], p =0.008; sex: b =0.214, 95% CI [0.0358, 0.3918], p =0.019; SES: b =0.304, 95% CI [0.1610, 0.4462], p <0.001). The inverse mediation analysis in PLWoH showed that global cognitive functioning (indirect effect = 033, 95% CI [−0.0223, 0.1081]) did not mediate the association between race and health literacy, independent of oral word literacy, age, sex, and SES. While the indirect pathways indicated that the association between race and global cognitive functioning was not significant (b =0.129, 95% CI [−0.1060, 0.3637], p =0.279), the association global cognitive functioning and health literacy was significant (b =0.257, 95% CI [0.0927, 0.4221], p =0.002). While higher oral word literacy, younger age, and the direct effect of white race were significantly associated with higher health literacy (oral word literacy: b =0.056, 95% CI [0.0452, 0.0663], p <0.001; age: b = −0.013, 95% CI [−0.0250, −0.0014], p =0.028; race: b =0.229, 95% CI [0.0368, 0.4230], p =0.020), sex and SES were not significantly associated with health literacy (sex: b = −0.014, 95% CI [−0.1697, 0.1426], p =0.863; SES: b =0.033, 95% CI [−0.0992, 0.1653], p =0.621). Thus, much like the findings among PLWH, White PLWoH were expected to obtain higher global cognitive functioning than African American/Black PLWoH through the partial mediating effect of higher health literacy, and the inverse mediating effect of global cognitive functioning on racial differences in health literacy among PLWoH was not observed.
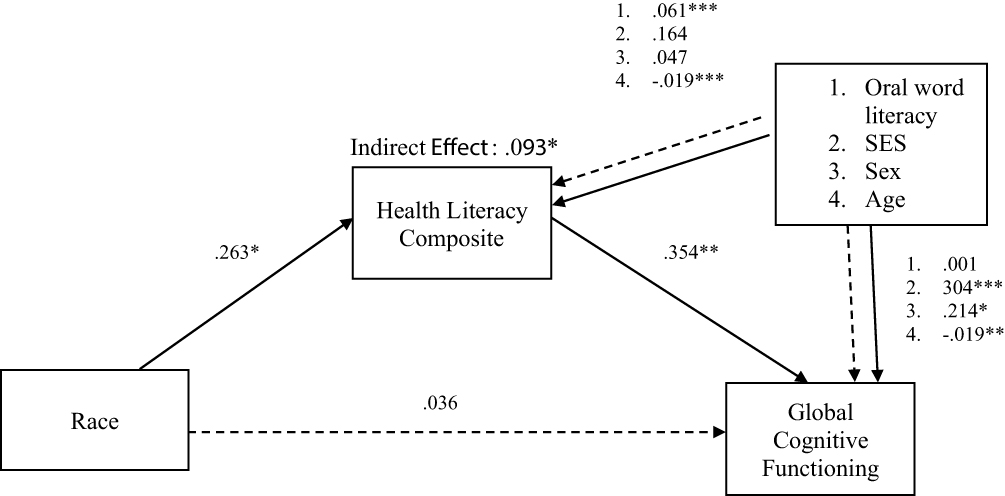 |
Figure 3 Mediation among PLWoH. Notes: * p <0.05, ** p <0.01, *** p <0.001. |
Finally, we conducted post-hoc analyses to examine which domains of health literacy uniquely mediated the associations between race and global cognitive functioning while covarying for oral word literacy, age, sex, and SES in PLWH and PLWoH alike. Among PLWH, numeracy (indirect effect =0.102, 95% CI [0.0248, 0.2576]; partially standardized mediated effect =0.156) significantly mediated the association between race and global cognitive functioning, independent of oral word literacy, age, sex, and SES, with 42.9% of the total variance in global cognitive functioning being explained by the mediating effect of the numeracy domain of health literacy. The indirect pathways indicated that the association between race and numeracy was significant (b =0.457, 95% CI [0.1645, 0.7505], p =0.002), as well as the association between numeracy and global cognitive functioning (b =0.222, 95% CI [0.1128, 0.3321], p <0.001). While sex and the direct effect of race were not associated with global cognitive functioning (sex: b =0.087, 95% CI [−0.0586, 0.2329], p =0.239; race: b =0.134, 95% CI [−0.0802, 0.3483], p =0.218), higher oral word literacy (b =0.020, 95% CI [0.0114, 0.0296], p <0.001), younger age (b = −0.015, 95% CI [−0.0254, −0.0044], p =0.006), and higher SES (b =0.133, 95% CI [0.0387, 0.2267], p =0.006) were significantly associated with higher global cognitive functioning. However, an indirect effect of reading on global cognitive functioning was not observed among PLWH (b =0.007, 95% CI [−0.0152, 0.0395]). The indirect pathways indicated that the association between race and reading was not significant (indirect effect =0.109, 95% CI [−0.1024, 0.3204], p =0.310) nor was there an association between reading and global cognitive functioning (b =0.061, 95% CI [−0.0983, 0.2213], p =0.448). While the direct effect of white race (b =0.226, 95% CI [0.0068, 0.4450], p =0.043), higher oral word literacy (b =0.027, 95% CI [0.0122, 0.0418], p <0.001), younger age (b = −0.019, 95% CI [−0.0305, −0.0086], p <0.001), and higher SES (b =0.189, 95% CI [0.0963, 0.2835], p <0.001) were associated with higher global cognitive functioning, sex was not significantly associated with global cognitive functioning (b =0.047, 95% CI [−0.1081, 0.2025], p =0.549). The findings among PLWH indicated that White PLWH were expected to obtain higher global cognitive functioning than African American/Black PLWH through the partial mediating effect of higher numeracy, while the association between race and global cognitive functioning among PLWH was not mediated by the reading domain of health literacy.
Among PLWoH, numeracy (indirect effect =0.155, 95% CI [0.0556, 0.3012]; partially standardized mediated effect =0.223) significantly mediated the association between race and global cognitive functioning, independent of oral word literacy, age, sex, and SES. Since the signs of the indirect effect (positive) and the direct effect (negative) were not consistent, calculation of the total variance in global cognitive functioning being explained by the mediating effect of the numeracy domain of health literacy was not appropriate. The indirect pathways indicated that the association between race and numeracy was significant (b =0.502, 95% CI [0.2040, 0.8000], p =0.001), as well as the association between numeracy and global cognitive functioning (b =0.308, 95% CI [0.1611, 0.4550], p <0.001). While the direct effect of race was not associated with global cognitive functioning (b = −0.026, 95% CI [−0.2553, 0.2037], p =0.824), higher oral word literacy (b =0.013, 95% CI [0.0008, 0.0249], p =0.037), younger age (b = −0.020, 95% CI [−0.0332, −0.0079], p =0.002), female sex (b =0.249, 95% CI [0.0768, 0.4203], p =0.005), and higher SES (b =0.249, 95% CI [0.1060, 0.3919], p <0.001) were significantly associated with higher global cognitive functioning. However, an indirect effect of reading on global cognitive functioning was not observed among PLWoH (indirect effect < −0.001, 95% CI [−0.0220, 0.0243]). The indirect pathways indicated that the association between race and reading was not significant (b =0.034, 95% CI [−0.2226, 0.289], p =0.795) nor was there an association between reading and global cognitive functioning (b = −0.004, 95% CI [−0.1915, 0.1834], p =0.966). While higher oral word literacy (b =0.024, 95% CI [0.0011, 0.0461], p =0.039), younger age (b = −0.026, 95% CI [−0.0406, −0.0117], p <0.001), female sex (b =0.236, 95% CI [0.0445, 0.4283], p =0.016), and higher SES (b =0.341, 95% CI [0.1915, 0.4915], p <0.001) were associated with higher global cognitive functioning, the direct effect of race was not significantly associated with global cognitive functioning (b =0.130, 95% CI [−0.1070, 0.3674], p =0.279). The findings among PLWoH indicated that White PLWoH were expected to obtain higher global cognitive functioning than African American/Black PLWoH through the partial mediating effect of higher numeracy, while the association between race and global cognitive functioning among PLWH was not mediated by the reading domain of health literacy. In summary, the mediating effects of general health literacy on the association between race and global cognitive functioning among PLWH and PLWoH was driven by the numeracy domain of health literacy, and not the reading domain of health literacy.
Discussion
As the average age of HIV population in the United States continues to increase, the need to understand how to mitigate declines in cognitive functioning is apparent. The goal of the current study was to examine the mediating role health literacy plays in racial disparities in cognitive functioning in a sample of middle-aged and older White and African American/Black PLWH and PLWoH from the Deep South. In our sample, White PLWH and PLWoH demonstrated greater global cognitive functioning, health literacy, and higher oral word literacy and SES than African American/Black counterparts, confirming racial disparities previously reported.13–15,23,25,26,46,47 Our findings for aim one were confirmed, such that health literacy was significantly associated with cognitive functioning among PLWH and PLWoH separately. Consistent with our second aim, health literacy was found to partially mediate racial differences in global cognitive functioning in PLWH and PLWoH, while the inverse mediation model was not supported (cognitive function as the mediator). Lastly, our post-hoc analyses based on the analyses for aim 2 indicated that the health literacy domain of numeracy drove the racial differences in global cognitive functioning in both samples. It should be noted that the while partially standardized indirect effects, a recommended effect size measure for indirect effects when the independent variable (ie, race) is dichotomous,48,49 do not have benchmarks for small, medium, or large effect sizes like Cohen’s d and ƒ2, the partially standardized indirect effects increased for PLWH and PLWoH after post hoc analyses were performed (PLWH: 0.084 to.156; PLWoH: 0.134 to.223). These observed increases in effect size when examining the mediating effects of the numeracy domain of health literacy on racial differences in global cognitive functioning among PLWH and PLWoH alike emphasizes the role that numeracy may have in global cognition among these aging populations.
Prior work among PLWH and PLWoH demonstrates that health literacy is a key social determinant of health that contributes to racial disparities in neurocognitive functioning,23,46,47,50,51 indicating a concern about the quality of education that ethnic/racial minorities receive, and how poor literacy translates to poor health literacy.22 Furthermore, as health literacy encompasses oral word literacy and applies it to health and medical contexts, it has been found to predict cognitive functioning above and beyond oral word literacy,23,46,47,50,51 as was the case in the current study. These findings are consistent with data from younger PLWH25 and represent the first study to examine this mediation among middle-aged and older PLWH and PLWoH, and to demonstrate the effect of health literacy is not dependent on oral literacy and SES. Our findings also highlight the unique role that numeracy skills may play in explaining racial differences in cognitive function.
There are several potential interpretations of the mediating effect of health literacy on racial differences in cognitive function. It is possible that poorer health literacy is associated with worse cognitive performance among African American/Black people in part due to the downstream impact of general literacy. Indeed, oral reading is often considered a proxy for quality of education,27 and African American/Black people may have different educational experiences (eg, lower quality teaching leading to differences in knowledge acquisition and application, familiarity/comfortability with standardized testing) that may impact their performance on cognitive tests. Yet our adjustment for oral reading suggests that the health literacy mechanism is likely more complex than this. There are several potential mediators and moderators that may explain the impact of health literacy with cognitive function, which should be explored in future work. For example, HIV management (as well as management of other comorbidities among PLWoH, such as diabetes and hypertension) may be one pathway whereby health literacy explains poorer cognitive outcomes among African American/Black people. In other words, poorer health literacy drives poorer HIV disease management (including attitudes related to HIV care)23,39,52 and outcomes among African American/Black people (particularly in the Deep South) which can directly cause central nervous system impairment and cognitive decline. Similarly, there are several positive health behaviors that are putative predictors of cognitive decline and dementia (eg, physical activity, cognitive activity), and race and health literacy may impact engagement in these behaviors, thereby impacting cognitive function. Our finding that numeracy measures (with complex applied questions requiring critical thinking skills) were driving racial differences in cognition also supports this hypothesis that such higher-order decision making skills (ie, executive function) are a pathway potentially leading to better health behaviors and cognitive function. The finding that numeracy explained racial differences in cognition above and beyond oral reading measures also suggests that health numeracy measures may simply be a better proxy for quality of education than oral reading measures, and that numeracy skills may be more directly relevant to cognitive testing performance.
Implications for Clinical Practice and Research
Assessing health numeracy skills in clinical settings may provide an indication of PLWH that may be at risk for poorer cognitive outcomes. Conversely, having high health numeracy may serve as an individual buffer whereby some PLWH may be better able to compensate for cognitive functioning (and/or brain pathology) and perform better on cognitive (and perhaps everyday function) assessments. Future research should determine whether health literacy interventions may have secondary downstream effects on cognitive function. There also may be factors not examined here that may further explain why health literacy mediates racial differences in cognitive function, such as disease management and health behaviors, which should be examined in future studies.
Furthermore, given the graying of the HIV population, it is important to address the medical needs of PLWH through a gerontological perspective. Given the growing concerns with the early onset of cognitive decline and development of related dementias among middle aged and older PLWH,7 clinicians should be informed on predictors and potential signs of HAND among PLWH, in addition to holistically monitoring any changes in patients, especially cognitive-related health changes. Brief measures are available to assess a patient’s current level of everyday function difficulties as well as cognitive functioning, such as the Montreal Cognitive Assessment (MOCA).53 Healthcare providers can also implement strategies to increase the health literacy of their patients as has been shown by previous interventions,54 including but not limited to increasing engagement in self-management practices, increasing understanding and knowledge about HIV-related health implications (eg, CD4 count, viral load), and teaching behavioral skills that PLWH can implement in their daily lives (eg, coping strategies to manage HIV-related stigma, develop routines that increase medication adherence).
Strengths and Limitations
Several limitations should be noted about the current study. First, the sub-sample sizes of the White participants was substantially smaller than the African American/Black participants in both PLWH and PLWoH (though they are representative of the higher burden of HIV among African American/Black in the Deep South), and there was a limited presence of females among the PLWH subsample, limiting generalizability and reproducibility of the results, as well as the power to detect race/sex differences. Additionally, the results may have limited generalizability to PLWH and PLWoH of other geographic regions. Another point regarding generalizability is two inherent biases: 1) volunteer bias such that participants who are interested in research and willing and able to attend the study visit(s) may not generalize to the broader population and 2) although people without HIV were recruited from the community, PLWH were recruited from a University HIV clinic, a sample that is engaged in care and may not represent the broader population with HIV. A second limitation of this study is that analyses were conducted with cross-sectional data, limiting our ability to infer causality. For example, while health literacy and cognitive skills may overlap and have a bidirectional relationship not able to be detected with cross-sectional data, inverse mediation models from the current study and prior research have found that an alternate path for the mediation (cognitive function as the mediator) did not fit the model.25 Similarly, although longitudinal data can better support causal inferences in mediation analysis, with caution applied to interpretation and to provide empirical support of a conceptual model, cross-sectional data is appropriative.55 Further, the post hoc mediation analyses have increased Type I error, as analyses were not controlled for multiple comparisons. Third, although we adjusted for age, sex, education quality, and SES, there are several other factors that may explain the relationships between race and health literacy with cognitive function that were not examined in this study, including cardiometabolic disorders (eg, diabetes and hypertension),16 psychiatric comorbidities (eg, anxiety and depression),17 social comorbidities (eg, discrimination, racism, trauma, access to and quality of health care),18 and health behaviors (eg, HIV management, physical activity). Another related limitation is that the cognitive measures used in this study may not be culturally appropriate for African American/Black people34 vs Whites and thus may have impacted performance and thus study results. However, our use of sample-based Z scores vs normatively corrected scores may have minimized such an impact.
Despite the various limitations to the current study, there were also notable strengths. To our knowledge, this is the first study to explore the mediating role that health literacy has on racial/ethnic disparities on cognitive functioning among middle-aged and older PLWH and PLWoH from the Deep South, with prior studies only having conducted similar analyses among PLWH across the lifespan.25,26 The current study also expanded upon prior research25 by assessing global cognitive functioning through a comprehensive neurocognitive battery, as well as investigating which unique measures of health literacy attributed to the mediating effects found between race and global cognitive functioning.
Conclusion
Findings from the current study provide insight into what future researchers should investigate in middle-aged and older PLWH. Given the relationship between health literacy and cognitive functioning in the current study is consistent with past studies,23,25,46,47 future researchers should assess health literacy when conducting neuropsychological studies. The addition of health literacy measures as a staple to neuropsychological batteries will provide researchers more context on factors that can contribute to cognitive functioning, as well as how other variables can potentially mediate or moderate the relationship between health literacy and cognitive functioning in African American/Black PLWH and other ethnic/racial PLWH. As the PLWH population continues to age and reach older adulthood, future researchers should investigate how health literacy relates to cognitive decline in older PLWH longitudinally, as there are concerns of accelerated and premature aging effects on cognitive functioning in PLWH.56,57 In order to better understand the health disparities among African American/Black PLWH, future research should assess both policy and health behavior changes that are linked to increased health literacy and cognitive functioning, including cognitive and physical activity, dietary habits, and sleep health.58,59
Acknowledgments
This study was funded by National Institutes of Health (NIH) grants K99/R00-AG048762 (PLF) and R01MH106366 (DEV). Jeremy D. Delgadillo was funded by NIH 3R21AG076377-01A1S1 and is now funded by T32HD071866.
Disclosure
The authors report no conflicts of interest in this work.
References
1. CDC. Diagnoses, deaths, and prevalence of HIV in the United States and 6 territories and freely associated states, 2022. Centers for Disease Control and Prevention. Available from: http://www.cdc.gov/hiv-data/nhss/hiv-diagnoses-deaths-prevalence.html.
2. CDC. HIV Surveillance Supplemental Report: estimated HIV Incidence and Prevalence in the United States, 2018–2022. Centers for Disease Control and Prevention. Updated May 2024.2024. Available from: https://www.cdc.gov/hiv-data/nhss/estimated-hiv-incidence-and-prevalence.html.
3. HIV.gov. Impact on Racial and Ethnic Minorities. Vol. 2023. 2023. Available from: https://www.hiv.gov/hiv-basics/overview/data-and-trends/impact-on-racial-and-ethnic-minorities.
4. CDC. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 territories and freely associated states, 2022. Centers for Disease Control and Prevention. Updated May 2024. 2024. Available from: https://www.cdc.gov/hiv-data/nhss/national-hiv-prevention-and-care-outcomes.html.
5. Heaton R, Clifford D, Franklin D, et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER study. Neurology. 2010;75(23):2087–2096. doi:10.1212/WNL.0b013e318200d727
6. Waldrop D, Irwin C, Nicholson WC, et al. The intersection of cognitive ability and HIV: a review of the state of the nursing science. J Assoc Nurses AIDS Care. 2021;32(3):306. doi:10.1097/JNC.0000000000000232
7. Rivera Mindt MG, Byrd DA, Morris EP, et al. Cultural neuropsychology considerations in the diagnosis of HIV-associated neurocognitive disorders. Neurocognitive Complications HIV-Infection. 2019;2020:193–223.
8. Atluri VSR, Hidalgo M, Samikkannu T, et al. Effect of human immunodeficiency virus on blood-brain barrier integrity and function: an update. Front Cell Neurosci. 2015;9:212. doi:10.3389/fncel.2015.00212
9. Wang Y, Liu M, Lu Q, et al. Global prevalence and burden of HIV-associated neurocognitive disorder: a meta-analysis. Neurology. 2020;95(19):e2610–e2621. doi:10.1212/WNL.0000000000010752
10. Lam JO, Lee C, Gilsanz P, et al. Comparison of dementia incidence and prevalence between individuals with and without HIV infection in primary care from 2000 to 2016. AIDS. 2022;36(3):437–445. doi:10.1097/QAD.0000000000003134
11. Cheng Y, Ahmed A, Zamrini E, Tsuang DW, Sheriff HM, Zeng-Treitler Q. Alzheimer’s disease and Alzheimer’s disease-related dementias in older African American and white Veterans. J Alzheimer’s Dis. 2020;75(1):311–320. doi:10.3233/JAD-191188
12. Matthews KA, Xu W, Gaglioti AH, et al. Racial and ethnic estimates of Alzheimer’s disease and related dementias in the United States (2015–2060) in adults aged≥ 65 years. Alzheimer’s Dementia. 2019;15(1):17–24. doi:10.1016/j.jalz.2018.06.3063
13. Thames AD, Nunez R, Slavich GM, Irwin MR, Senturk D. Racial differences in health and cognition as a function of HIV among older adults. Clin Neuropsycholog. 2022;36(2):367–387. doi:10.1080/13854046.2021.1967449
14. Marquine M, Sakamoto M, Dufour C, et al. The impact of ethnicity/race on the association between the Veterans Aging Cohort Study (VACS) Index and neurocognitive function among HIV-infected persons. J Neurovirol. 2016;22(4):442–454. doi:10.1007/s13365-015-0411-6
15. Thompson JL, Beltran-Najera I, Johnson B, Morales Y, Woods SP. Evidence for neuropsychological health disparities in Black Americans with HIV disease. Clin Neuropsycholog. 2022;36(2):388–413. doi:10.1080/13854046.2021.1947387
16. Graham G. Disparities in cardiovascular disease risk in the United States. Current Cardiol Rev. 2015;11(3):238–245. doi:10.2174/1573403X11666141122220003
17. Reif S, Safley D, McAllaster C, Wilson E, Whetten K. State of HIV in the US Deep South. J Commun Health. 2017;42:844–853. doi:10.1007/s10900-017-0325-8
18. Tedaldi EM, Minniti NL, Fischer T. HIV-associated neurocognitive disorders: the relationship of HIV infection with physical and social comorbidities. BioMed Res Int. 2015;2015. doi:10.1155/2015/641913
19. Woods SP, Norman MA. Do Black lives matter to clinical neuropsychologists? An introduction to a special issue. Clin Neuropsychol. 2022;36(2):209–213. doi:10.1080/13854046.2021.2020906
20. Willis AI. Black Literacy Education in the United States. Oxford Research Encyclopedia of Education. 2022.
21. Roets L, Kurtz B, Biraimah K. The Impact Of The Racial and Economic Divides on Access to Quality Education in South Africa and the United States. Bulgarian Comparative Education Society. 2023.
22. Berkman ND, Davis TC, McCormack L. Health literacy: what is it? J Health Commun. 2010;15(S2):9–19. doi:10.1080/10810730.2010.499985
23. Walker RL, Hong JH, Talavera DC, Verduzco M, Woods SP. Health literacy and current CD4 cell count in a multiethnic US sample of adults living with HIV infection. Int J STD AIDS. 2018;29(5):498–504. doi:10.1177/0956462417738679
24. Johnson NX, Marquine MJ, Flores I, et al. Racial differences in neurocognitive outcomes post-stroke: the impact of healthcare variables. J Int Neuropsycholog Soc. 2017;23(8):640–652. doi:10.1017/S1355617717000480
25. Beltran-Najera I, Thompson JL, Matchanova A, Sullivan KL, Babicz MA, Woods SP. Neurocognitive performance differences between black and white individuals with HIV disease are mediated by health literacy. Clin Neuropsycholog. 2022;36(2):414–430. doi:10.1080/13854046.2021.1953147
26. Beltran-Najera I, Thompson JL, Matchanova A, Woods SP. Racial differences in scores on the HIV dementia scale: mediating effects of literacy and screening utility among black and white persons with HIV disease. PsyArXiv. 2021;2021:13.
27. Manly JJ, Byrd D, Touradji P, Sanchez D, Stern Y. Literacy and cognitive change among ethnically diverse elders. Int J Psychol. 2004;39(1):47–60. doi:10.1080/00207590344000286
28. Sørensen K, Van den Broucke S, Fullam J, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12(1):80. doi:10.1186/1471-2458-12-80
29. Ettenhofer ML, Foley J, Castellon SA, Hinkin CH. Reciprocal prediction of medication adherence and neurocognition in HIV/AIDS. Neurology. 2010;74(15):1217–1222. doi:10.1212/WNL.0b013e3181d8c1ca
30. Vance D, Fazeli P, Shacka J, et al. Testing a computerized cognitive training protocol in adults aging with HIV-associated neurocognitive disorders: randomized controlled trial rationale and protocol. JMIR Res Protocols. 2017;6(4):e6625. doi:10.2196/resprot.6625
31. Snelbaker AJ, Wilkinson GS, Robertson GJ, Glutting JJ. Wide range achievement test 3 (wrat3). In: Understanding Psychological Assessment. Vol. 2001. Springer; 259–274.
32. Fazeli PL, Waldrop-Valverde D, Yigit I, et al. An exploratory study of correlates of allostatic load in older people living with HIV. JAIDS J Acquired Immune Deficiency Syndromes. 2020;83(5):441–449. doi:10.1097/QAI.0000000000002293
33. Fazeli PL, Marceaux JC, Vance DE, Slater L, Long CA. Predictors of cognition in adults with HIV: implications for nursing practice and research. J Neurosci Nurs. 2011;43(1):36–50. doi:10.1097/JNN.0b013e3182029790
34. Manly JJ. Advantages and disadvantages of separate norms for African Americans. Clin Neuropsycholog. 2005;19(2):270–275. doi:10.1080/13854040590945346
35. Parker RM, Baker DW, Williams MV, Nurss JR. The test of functional health literacy in adults. J Gen Internal Med. 1995;10(10):537–541. doi:10.1007/BF02640361
36. Murphy PW, Davis TC, Long SW, Jackson RH, Decker BC. Rapid estimate of adult literacy in medicine (REALM): a quick reading test for patients. J Reading. 1993;37(2):124–130.
37. Weiss BD, Mays MZ, Martz W, et al. Quick assessment of literacy in primary care: the newest vital sign. Annals Fam Med. 2005;3(6):514–522. doi:10.1370/afm.405
38. Lipkus IM, Samsa G, Rimer BK. General performance on a numeracy scale among highly educated samples. Med Decision Making. 2001;21(1):37–44. doi:10.1177/0272989X0102100105
39. Matchanova A, Babicz M, Medina LD, Fazeli PL, Vance DE, Woods SP. Latent structure of health literacy and its association with health-related management and decision-making in HIV. Psychol Health. 2021;36(8):985–1002. doi:10.1080/08870446.2020.1817453
40. Delgadillo JD, Beltran-Najera I, Long AR, et al. 55 Health literacy mediates racial differences in cognitive functioning among people with and without HIV. J Int Neuropsycholog Soc. 2023;29(s1):51–52. doi:10.1017/S1355617723001376
41. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psycholog Measurement. 1977;1(3):385–401. doi:10.1177/014662167700100306
42. JMP® V. SAS Institute Inc. Cary, NC.
43. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2022.
44. Field-Fote E. Mediators and moderators, confounders and covariates: exploring the variables that illuminate or obscure the “active ingredients” in neurorehabilitation. J Neurologic Phys Ther. 2019;43(2):83–84. doi:10.1097/NPT.0000000000000275
45. Fritz MS, MacKinnon DP. Required sample size to detect the mediated effect. Psycholog Sci. 2007;18(3):233–239. doi:10.1111/j.1467-9280.2007.01882.x
46. Baumann KE, Phillips AL, Arya M. Overlap of HIV and low health literacy in the southern USA. Lancet HIV. 2015;2(7):e269–e270. doi:10.1016/S2352-3018(15)00121-6
47. Osborn CY, Paasche-Orlow MK, Davis TC, Wolf MS. Health literacy: an overlooked factor in understanding HIV health disparities. Am J Preventive Med. 2007;33(5):374–378. doi:10.1016/j.amepre.2007.07.022
48. Ledermann T, Rudaz M, Fritz MS. On partial versus full mediation and the importance of effect sizes. Adv Meth Pract Psychol Sci. 2025;8(3):25152459251355585. doi:10.1177/25152459251355585
49. Miočević M, O’Rourke HP, MacKinnon DP, Brown HC. Statistical properties of four effect-size measures for mediation models. Behav Res Meth. 2018;50(1):285–301. doi:10.3758/s13428-017-0870-1
50. Fleary SA, Ettienne R. Social disparities in health literacy in the United States. HLRP. 2019;3(1):e47–e52. doi:10.3928/24748307-20190131-01
51. Federman AD, Sano M, Wolf MS, Siu AL, Halm EA. Health literacy and cognitive performance in older adults. J Am Geriatrics Soc. 2009;57(8):1475–1480. doi:10.1111/j.1532-5415.2009.02347.x
52. Fazeli PL, Woods SP, Lambert CC, Waldrop-Valverde D, Vance DE. Neurocognitive functioning is associated with self-reported and performance-based treatment management abilities in people living with HIV with low health literacy. Arch Clin Neuropsychol. 2020;35(5):517–527. doi:10.1093/arclin/acaa005
53. Fazeli P, Casaletto K, Paolillo E, Moore R, Moore D, Group H. Screening for neurocognitive impairment in HIV-positive adults aged 50 years and older: montreal Cognitive Assessment relates to self-reported and clinician-rated everyday functioning. J Clin Exp Neuropsychol. 2017;39(9):842–853. doi:10.1080/13803395.2016.1273319
54. Perazzo J, Reyes D, Webel A. A systematic review of health literacy interventions for people living with HIV. AIDS Behav. 2017;21(3):812–821. doi:10.1007/s10461-016-1329-6
55. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford publications; 2017.
56. Aung HL, Aghvinian M, Gouse H, et al. Is there any evidence of premature, accentuated and accelerated aging effects on neurocognition in people living with HIV? A systematic review. AIDS Behav. 2021;25:917–960. doi:10.1007/s10461-020-03053-3
57. Aung HL, Siefried KJ, Gates TM, et al. Meaningful cognitive decline is uncommon in virally suppressed HIV, but sustained impairment, subtle decline and abnormal cognitive aging are not. EClinicalMedicine. 2023;2023:56.
58. Campbell LM, Kohli M, Lee EE, et al. Objective and subjective sleep measures are associated with neurocognition in aging adults with and without HIV. Clin Neuropsycholog. 2022;36(6):1352–1371. doi:10.1080/13854046.2020.1824280
59. Guntzviller LM, King AJ, Jensen JD, Davis LA. Self-efficacy, health literacy, and nutrition and exercise behaviors in a low-income, Hispanic population. J Immigrant Minority Health. 2017;19:489–493. doi:10.1007/s10903-016-0384-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.