")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Health Literacy and Anxiety Among Hemodialysis Patients During the Coronavirus Disease Pandemic
Received 8 November 2022
Accepted for publication 28 March 2023
Published 4 April 2023 Volume 2023:16 Pages 1051—1061
DOI https://doi.org/10.2147/PRBM.S395479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
In Ju Yoon,1 Su Jung Lee2
1Graduate School of Nursing Science, Hallym University, Hallym University Sacred Heart Hospital, Anyang, South Korea; 2School of Nursing, Research Institute of Nursing Science, Hallym University, Chuncheon, South Korea
Correspondence: Su Jung Lee, Tel +82-33-248-2722, Fax +82-33-248-2734, Email [email protected]
Background and Purpose: The COVID-19 pandemic can cause psychological distress, and hemodialysis patients with chronic kidney disease may be particularly vulnerable. The aim of this study is to investigate anxiety levels among patients undergoing hemodialysis during the COVID-19 pandemic and to explore the relationship between health literacy and anxiety.
Methods: This study recruited 149 hemodialysis patients from two hospitals between July 16th and July 31st, 2021. Patient data were collected using questionnaires on general characteristics, health literacy, generalized anxiety, and coronavirus disease-related anxiety. We used the Coronavirus Anxiety Scale (CAS) and the Korean version of the Generalized Anxiety Disorder (GAD) scale to evaluate the anxiety symptoms of the patients. Statistical analyses were performed using descriptive statistics, t-test, Mann–Whitney U-test, one-way ANOVA, Kruskal-Walli’s test and Spearman’s rank correlation.
Results: The results showed that health literacy increased with decreasing age and increasing educational level among patients who source health information from the internet and among patients without comorbidities. Patients with comorbidities showed high levels of general anxiety. Patients who search for health information for ≥ 1 hour had high levels of coronavirus disease-related anxiety. Both CAS and GAD showed a significant negative correlation with the sub-domains of health literacy, except for critical health literacy.
Conclusion: The results of this study highlight the need for a follow-up study on whether health literacy programs will reduce the anxiety levels of patients undergoing hemodialysis during infectious disease outbreaks. In addition, provision of social support for patients with comorbidity is essential for reducing their anxiety levels during disease outbreaks.
Keywords: end-stage kidney disease, anxiety, health literacy, coronavirus disease-19, pandemics
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Djaafar has been published for this article.
Introduction
The number of Korean hemodialysis patients with chronic kidney disease has tripled from 33,427 in 2008 to 117,398 in 2019. This is expected to continue increasing due to the aging population and a rise in chronic diseases such as hypertension and diabetes.1 Hemodialysis patients have higher risk of mental health issues like depression and anxiety due to restricted physical activity2 and lack of social support.3 Previous studies indicate anxiety rates of 13–41%, more than double that of the general population.4,5
The coronavirus disease (COVID-19) pandemic has a huge impact on patients with chronic disease.6 The period during which infectious diseases occur widely, such as COVID-19, may be closely related to psychological and mental illness symptoms.7 Patients undergoing hemodialysis are vulnerable to COVID-19 infection owing to a combination of several risk factors, including reduced immune function due to uremia, high blood pressure, underlying diseases such as diabetes, and old age. In addition, regardless of whether there is an outbreak of infectious diseases or not, patients who require hemodialysis need to visit medical institutions regularly and receive treatment for about 4 hours in a dialysis room. This increases their risk for anxiety and elevates their psychological burden.8 Therefore, it is important to identify mental instability in patients undergoing hemodialysis during a pandemic and relieve their mental stress.
As social distancing continues to mitigate the spread of COVID-19, the public is increasingly acquiring information through non-face-to-face media such as television, radio, smartphones, and computers.9 Recent reports have indicated that during a pandemic, media reports tend to focus more on the damage caused by the spread of the infectious disease than on providing accurate information on the symptoms of the disease.10,11 This trend often aggravates public anxiety and panic. Therefore, healthcare professionals emphasize the importance of an individual’s ability to obtain and understand accurate health information.11,12 Previous studies have demonstrated that health literacy affects health behavior.13 In addition, it has been reported that patients with low health literacy who have chronic diseases show poor self-management of the diseases and have high levels of depression and anxiety.14,15 Additionally, increasing age is associated with increased difficulty in reading and understanding health information. It has been reported that people with underlying chronic diseases need more information and understanding of health behavior than those without.16 It is very important for CKD patients undergoing hemodialysis during a pandemic to understand dialysis-related information, such as regular dialysis treatment, dietary management, medication, and dialysis blood vessel management, as well as COVID-19 infection prevention measures, to make appropriate health-related decisions. This means that patients undergoing hemodialysis require a higher level of health literacy than the general population.17 However, the average age of hemodialysis patients in Korea is 62 years old, with a high proportion of elderly patients.18 And it could be expected that there will be difficulties in understanding health information due to various physical symptoms caused by chronic kidney disease.2,19
Several previous studies have confirmed the correlation between different variables and the anxiety and health literacy levels of patients undergoing hemodialysis8,17,20–22 However, the health literacy and anxiety levels of patients undergoing hemodialysis during the pandemic were not investigated in these studies. Therefore, the aim of the present study was to investigate the anxiety and health literacy levels of patients undergoing hemodialysis during the COVID-19 pandemic, and to confirm the relationship between anxiety and health literacy among them. We believe that the results of this study could be used as evidence for the establishment of psychological and social support programs for patients undergoing hemodialysis during the other pandemic.
Materials and Methods
Study Design
This was a cross sectional survey study conducted to determine the health literacy and anxiety levels of patients undergoing hemodialysis during the COVID-19 pandemic, and to analyze the correlation between health literacy and anxiety.
Sample
The participants were patients aged ≥19 years old who receive dialysis in the hemodialysis rooms of two general hospitals located in two cities in Korea and agreed to participate in this study. We conveniently recruited patients who receive hemodialysis twice a week. Patients who were hospitalized or had a history of psychiatric illness, patients who tested positive for COVID-19, and patients with a history of COVID-19 infection were excluded. Regarding the number of participants, the minimum number of samples required for correlation was calculated using the G power software (version 3.1.9.4, Department of Psychology, University of Düsseldorf, Düsseldorf, Germany, 2019). Based on the information on previous studies,3,22,23 we performed a two-sided calculation at a significance level of 0.05, using an effect size of 0.3 and a power of 0.95. The results indicated that the required sample size was 143 participants. Considering a 20% dropout rate, we distributed the survey questionnaire to 180 patients.
Data Collection Procedures and Ethical Considerations
This study was conducted from 16 July 2021 to 31 July 2021 after receiving institutional review board approval from the two medical institutions (Hallym University Kangnam Sacred Heart Hospital; HKS 2021-06-010, Hallym University Sacred Heart Hospital; HALLYM 2021-06-006-001). The lead researcher for this study and head nurse of the institutions provided explanations and distributed consent forms to the eligible patients. After receiving sufficient explanation of the study, patients who agreed to participate in the study signed and submitted the consent forms. Information that could identify the patients were not collected. The collated data were kept in a file with a separate lock, restricting access to non-researchers.
Measures
Demographic and Clinical Characteristics of the Participants
The general characteristics questionnaire consisted of questions on 10 items, including gender, age, type of household, education level, employment status, mode of commute to the hospital, COVID-19 related quarantine experience, status of completion of secondary COVID-19 vaccination, main source of health information, including those related to COVID-19, and time spent acquiring health information. We classified the age of the participants into < 60, 60–69, and ≥70 years old age groups, whereas type of household was classified into single-person households and households with cohabitants. We also investigated employment status and mode of commute to the hospital (including public transportation) at the time of the survey. In addition, we investigated whether the participants experienced quarantine due to COVID-19 or not. Regarding COVID-19 vaccination status, the participants were classified into those who completed the second COVID-19 vaccination and those who did not. The main sources of health information were classified into four categories: television and/or radio, internet, paper prints (newspapers, books, magazines), and healthcare workers such as doctors and nurses. Time spent acquiring health information was classified into an average of less than 1 hour and more than 1 hour per day. Regarding clinical characteristics, hemodialysis maintenance period and comorbidities were analyzed. Hemodialysis maintenance period was classified as < 3 years, 3–7 years, and ≥ 7 years. Regarding comorbidities, patients diagnosed with a disease other than the cause of CKD were classified as patients with a comorbidity.
Health Literacy
We used the 14-item Functional, Communicative, and Critical Health Literacy (FCCHL) tool, which was developed by Ishikawa24 for the measurement of health literacy in patients with diabetes, and modified by Kristian,20 to measure the health literacy of the participants in terms of function, communicative, and critical thinking. Linguistic validation was achieved by having two nursing professors translate Kristian’s revised FCCHL tool into Korean. The researchers reviewed and supplemented the translation by examining whether there were any items that needed to be corrected owing to the loss of meaning in translation and cultural differences, and whether the items were composed of clear sentences that are easily understood.25 The Korean version of the FCCHL was then translated back into English by a nursing professor and a linguist fluent in Korean and English. To check the validity of the questions in the Korean version of the FCCHL tool, we checked the validity index of the questions by presenting them to three adult nursing doctors, one doctor of nephrological medicine, and two head nurses in the hemodialysis department. Five evaluators evaluated the 14 items using a 4-point Likert scale. Four points indicated “very valid”, whereas 1 point indicated “not valid”. The item content validity index, which evaluates the ratio of items rated 3 or 4 points, was found to be 0.80 or higher for all items.26
In the FCCHL, functional literacy is measured using five questions and responses are provided using a 4-point Likert scale, with answers ranging from “not at all” (4 points) to “frequently” (1 point). Communicative literacy (CmHL) and critical health literacy (CHL) are measured using five and four questions, respectively, and responses are provided using a 4-point Likert scale. The responses range from “easy” (4 points) to “difficult” (1 point). Higher scores indicate higher health literacy. Cronbach’s α related to function, communicative, and critical thinking, which are the sub-domains of health literacy, were 0.84, 0.77, and 0.65, respectively, at the time of the development of the FCCHL, whereas that for the FCCHL was 0.78. In the present study, Cronbach’s α for health literacy related to function, communicative, and critical thinking were 0.88, 0.89, and 0.94, respectively, whereas that for FCCHL was 0.93.
Anxiety
Coronavirus Anxiety Scale
We used the Coronavirus Anxiety Scale (CAS) created by Lee27 to measure COVID-19-related anxiety. CAS is a tool developed for the measurement of physical dysfunction associated with COVID-19. The Korean version of this tool has been validated.28 The CAS includes responses to questions regarding experiencing physical symptoms, such as dizziness, sleep disturbance, lethargy, decreased appetite, and abdominal pain, when media information about COVID-19 is received over the past two weeks. The CAS includes five questions, and each item was measured using a 5-point Likert scale. Responses range from “no” (0 points) to “almost every day for the past 2 weeks” (4 points). A total score of 9 or more indicates dysfunctional anxiety. Cronbach’s α for the CAS at the time of development was 0.93, whereas that in the present study was 0.88.
Generalized Anxiety Disorder
The Korean version of the Generalized Anxiety Disorder (KGAD), which was developed by Spitzer29 and translated by Seo et al,30 was used for the screening and diagnosis of generalized anxiety disorder in the present study. The KGAD focuses on how disturbed a patient has been by anxiety over the past two weeks. Each item is measured using a 4-point Likert scale, with answers ranging from 0 for “not at all disturbed” to 3 for “disturbed almost every day”. The total score ranges from a minimum of 0 to a maximum of 21, with higher scores indicating higher levels of anxiety. The cut-off value for generalized anxiety is 10 points, with a score of 5 or higher indicating mild anxiety, 10 or higher indicating moderate anxiety, and 15 or higher indicating severe anxiety. Cronbach’s α for the KGAD at the time of development was 0.92, and whereas that in the present study was 0.89.
Data Analysis
Data analysis was performed using SPSS version 22 (IBM Corp., Armonk, NY, USA). Patient characteristics, health literacy, CAS and KGAD score were analyzed and the results are presented as percentages, mean standard deviations, medians and interquartile ranges (25th to 75th percentile). We confirmed the normality of the distribution of continuous variables using the Kolmogorov–Smirnov test. Differences in health literacy and anxiety levels were analyzed according to the characteristics of the participants using the t-test, Mann–Whitney U-test, one-way ANOVA, Kruskal–Wallis test. The correlation between health literacy and anxiety was analyzed using Spearman’s rank correlation coefficients.
Results
Demographic and Clinical Characteristics of the Participants
The questionnaires were distributed to a total of 180 patients. Of these, 31 returned questionnaires with incomplete responses. Thus, a total of 149 patients were finally analyzed. The average age of the respondents was 63.93 years and 50.3% of them were male. Regarding the type of household, 22.1% of the respondents were from single-person households. Regarding the education level, the highest percentage of participants had 10–12 years of education. Regarding employment status and mode of commute, 81.2% of the respondents were unemployed, whereas 55.7% used public transportation to commute to the hospital. Regarding COVID-19-related variables, 8.1% of the respondents experienced quarantine due to COVID-19, whereas 55.5% of them completed the second COVID-19 vaccination. Regarding the acquisition of health information, 72.5% of the respondents answered that they use the television or radio, whereas 59.7% spend less than 1 hour acquiring health information. The average hemodialysis maintenance period of the respondents was 6.22 years, and 79.9% of them had comorbidities (Table 1).
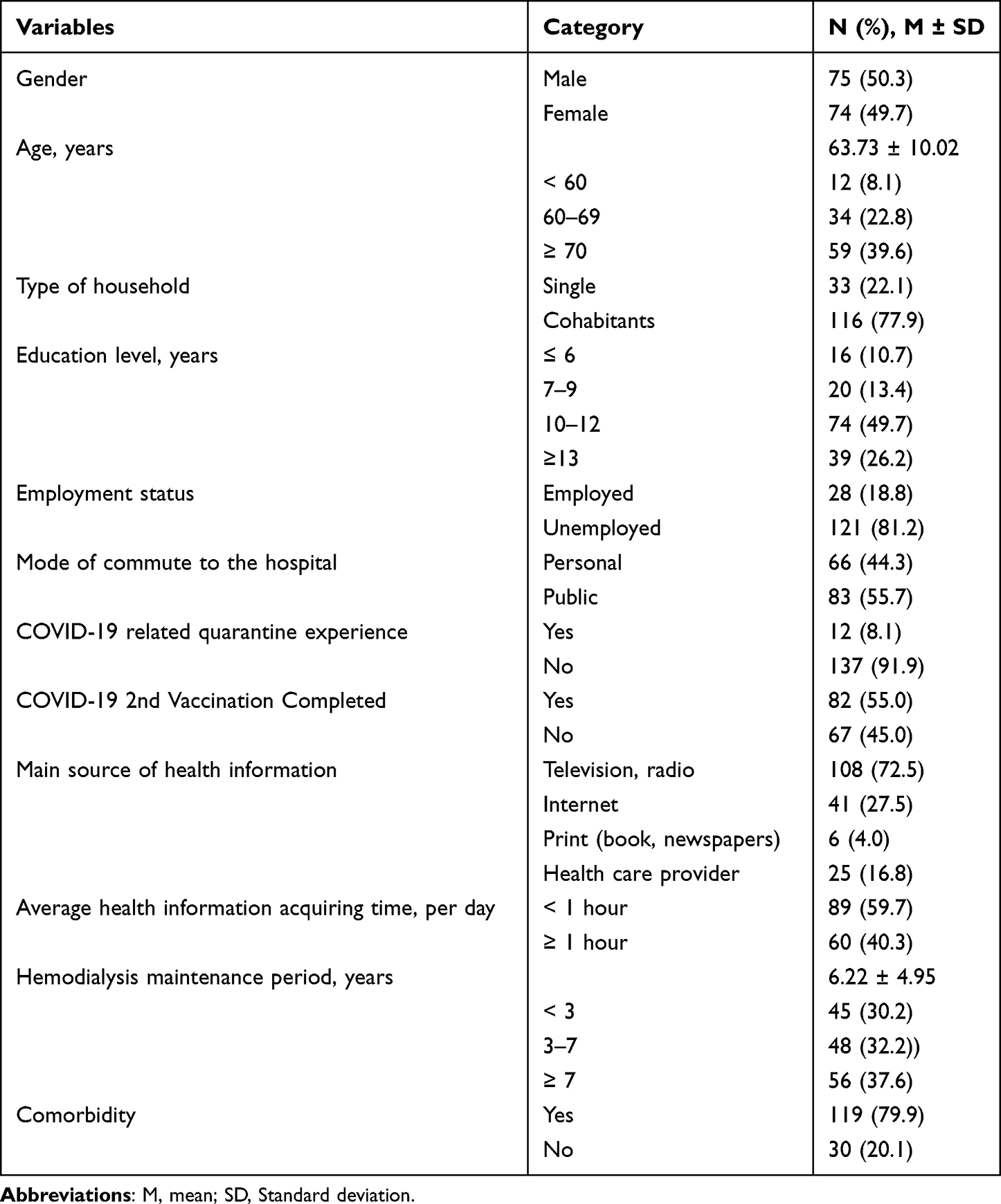 |
Table 1 Demographic and Clinical Characteristics of the Participants (n= 149) |
Health Literacy and Anxiety Levels
Regarding health literacy, the literacy score for the functional health literacy sub-domain was 14.03± 4.52, that for CmHL was 14.01±4.13, and that for CHL 9.97±3.77.
The CAS median and quartile range were 0 (0–1.0) and the proportion of patients with physical dysfunctional anxiety (score ≥ 9 points) was 1.4%. The average KGAD median and quartile range were 0 (0–4.0) and the proportion of patients with anxiety (score ≥ 10 points) was 4.7% (Table 2).
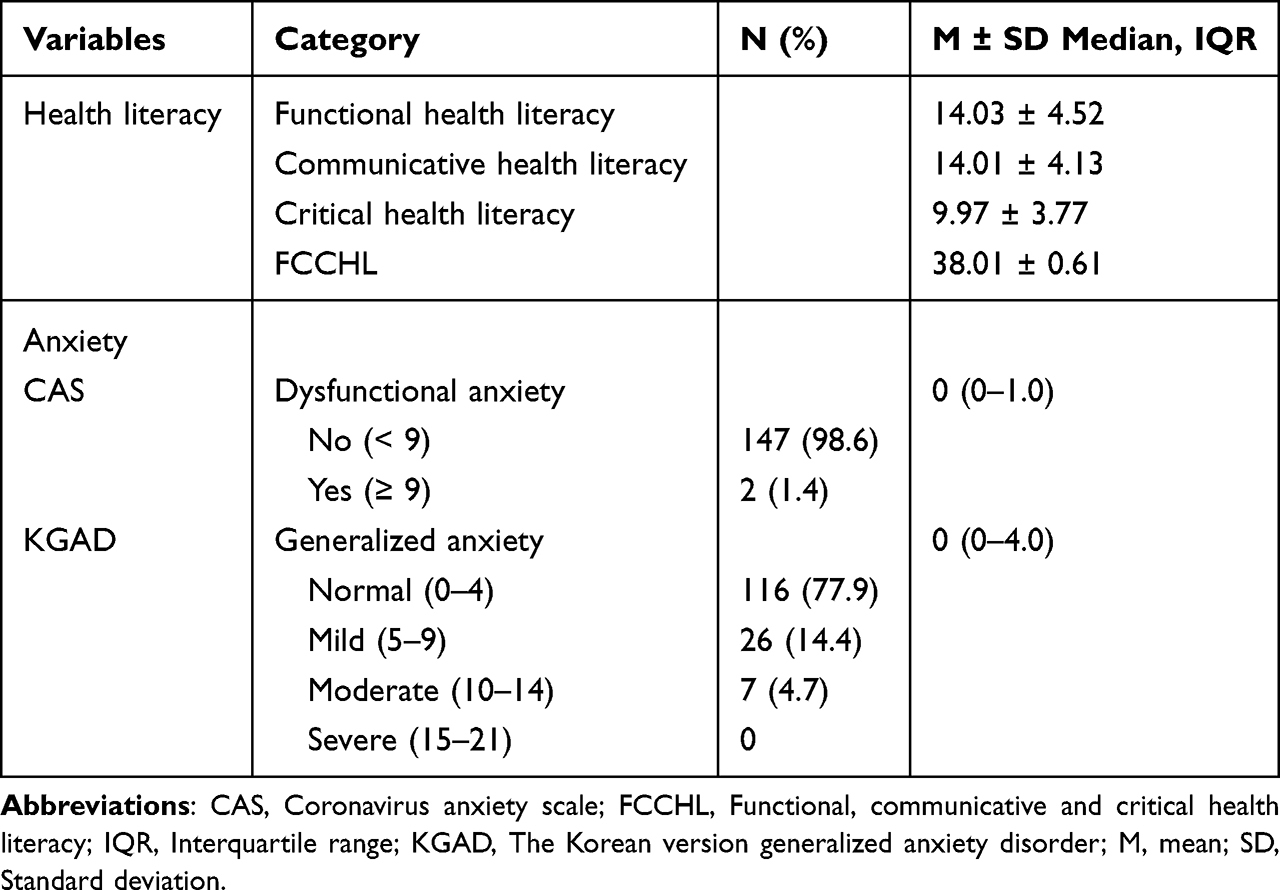 |
Table 2 Subject’s Health Literacy and Anxiety Level (n= 149) |
Differences in Health Literacy and Anxiety Levels According to the General Characteristics of the Participants
There were significant differences in the FCCHL scores of the participants according to age (F=8.085, p < 0.001), educational level (F=11.163, p < 0.001), acquisition of information through the internet (F= −3.254, p < 0.001), and presence or absence of comorbidities (t=3.143, p=0.002) (Figure 1). Functional health literacy, CmHL, CHL levels were higher when the age of participants was lower; the higher the education level, the higher the health literacy level in all sub-domains. The group obtaining health-related information through the internet and that without comorbid diseases showed high health literacy levels in all sub-domains (Supplementary Table 1).
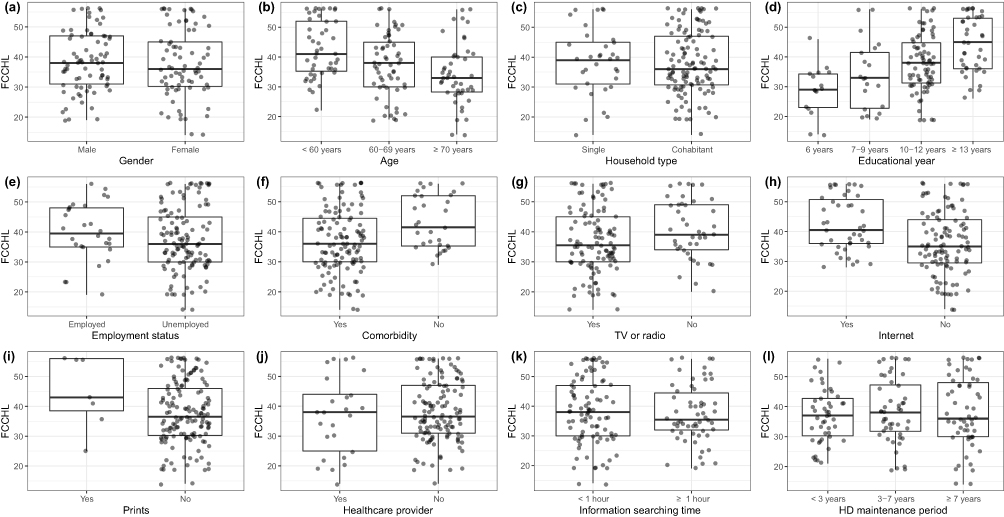 |
Figure 1 Comparison of health literacy according to the general characteristics of the participants (n= 149). Boxplot showing the comparison of health literacy between (a) Gender, (b) Age, (c) Household type, (d) Educational year, (e) Employment status, (f) Comorbidity, the main source of information (g) TV or radio, (h) Internet, (i) Prints, (j) healthcare provider, (k) information searching time, and (l) Hemodialysis maintenance period. The p values of independent variables significant in t-test or one-way analysis of variance were shown in the figure. All data points can be seen as scattered dots overlying the boxplot. Abbreviations: FCCHL, functional, communicative and critical health literacy; HD, hemodialysis. |
The CAS of the respondents differed according to time spent acquiring health information. Patients who spent >1 hour acquiring health information had high levels of anxiety (z = −2.472, p = 0.013). The level of generalized anxiety significantly differed according to the presence or absence of comorbidities (z= −2.384, p = 0.017). However, there was no difference in the other general characteristics of the respondents (Table 3).
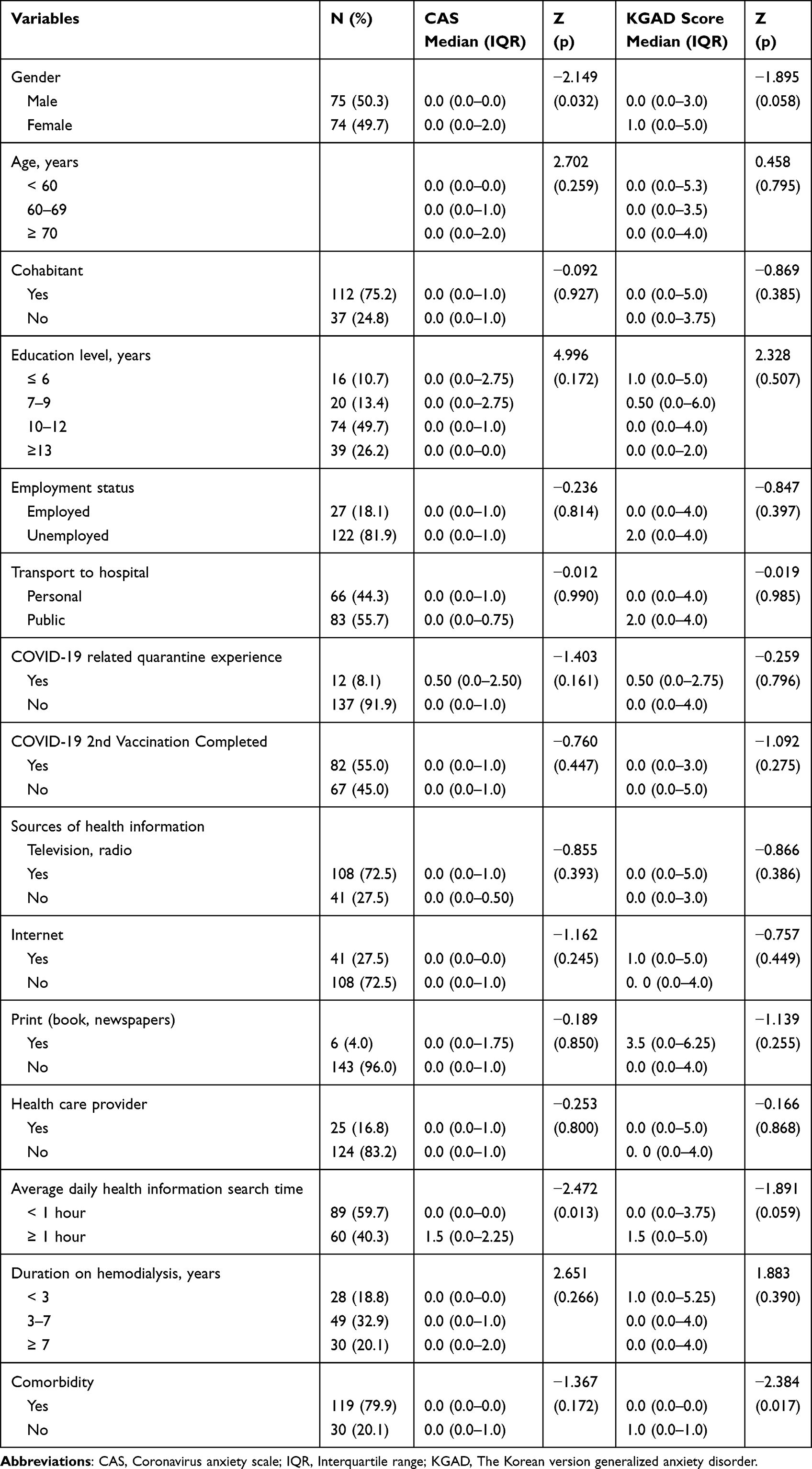 |
Table 3 Differences in Coronavirus Anxiety Scale and General Anxiety Disorder According to Generalized Characteristic (n= 149) |
Correlation Between Health Literacy and Anxiety
Both the CAS and general anxiety of the respondents showed a significant negative correlation with the health literacy sub-domains except for CHL (Table 4).
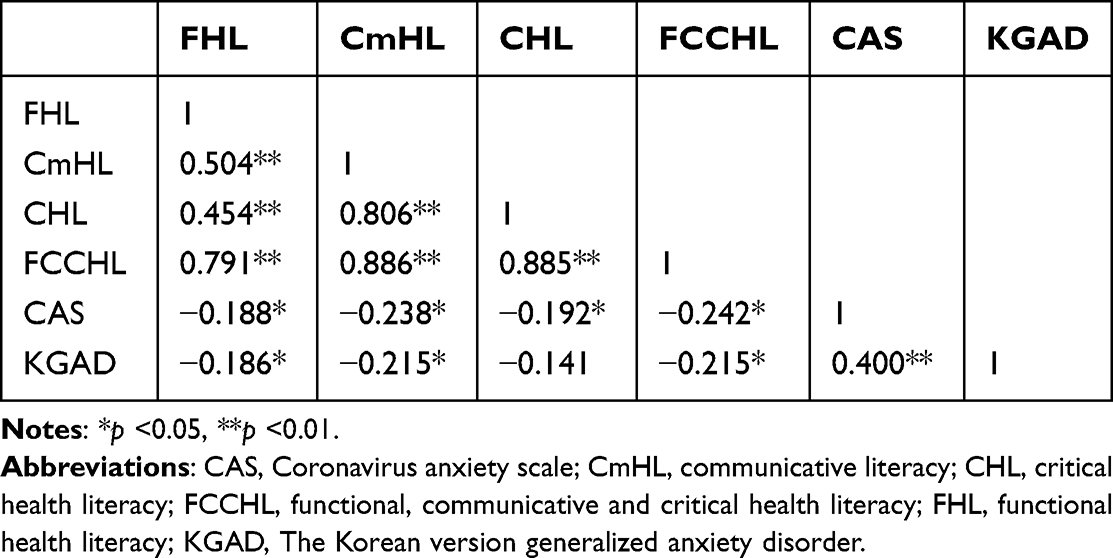 |
Table 4 Spearman Correlation Between Subject’s Health Literacy (Domain; Functional, Communicative and Critical Literacy) and Anxiety (Coronavirus Anxiety Scale, Generalized Anxiety Disorder) |
Discussion
This purpose of this study, which was conducted during the ongoing COVID-19 pandemic (July 2021), was to identify factors that affect the anxiety levels of patients undergoing hemodialysis. The relationship between anxiety and health literacy was analyzed as well. Indino et al20 investigated the health literacy of Austrian patients undergoing hemodialysis. In that study, the CHL score of the participants was 14.0 points, functional health literacy was 15.2 points, and CmHL was 12.3 points. In the present study, the CHL score of the participants was 9.97 points, functional health literacy was 14.03 points, and CmHL was 14.01 points. Health literacy scores related to communicative and critical thinking were higher in the previous study than in the present study. This is attributable to the difference between ages of the participants included in the two studies. The average age of participants in the present study was 63.7 years, whereas that of participants in the Kristian study was 54.4 years, which is significantly younger. In the present study, the health literacy of the patients undergoing hemodialysis during the COVID-19 pandemic differed according to age, education level, source of health information, and the presence or absence of chronic diseases.
The results of the present study showed that health literacy increased with decreasing age and increasing educational level among patients who source health information from the internet and those without comorbidities. Previous studies have also showed a consistent effect of age and education level on health literacy despite the use of various measurement tools as demographic characteristics.31 In other words, the younger the age and the higher the education level, the higher the internet access competency. These results are similar to those of previous studies that indicated that internet access is strongly correlated with health literacy.29,32,33 In addition, several previous studies have demonstrated that health literacy levels differ according to the number of chronic diseases patients have,17,34 and that more health-related information is required for the understanding and improvement of health behavior.16 In the present study, the health literacy level of participants with comorbidities was significantly lower than that of those without comorbidities. However, we did not analyze the difference in health literacy levels according to the number of comorbidities present. Thus, this finding should be interpreted carefully.
The mean CAS of the participants in the present study was 1.05 ± 2.58 and their generalized anxiety score was 2.28 ± 3.28. These results were low compared to the 1.29 ± 2.39-point CAS of the general population measured by Choi et al around mid-July 2020 after the outbreak of COVID-19.28 In a recent longitudinal study, mental health symptoms, such as depression and anxiety, experienced during the COVID-19 pandemic showed a tendency to improve or remain stable over time regardless of the number of COVID-19 outbreaks that occurred.35,36 Therefore, it is important to focus on the development and implementation of mental health programs for high-risk groups that are prone to mental health problems, rather than compare anxiety scores over time.
In the present study, patients that searched for health information, including COVID-19-related information, for more than 1 hour had high CAS. In addition, patients with comorbidities had significantly higher general anxiety scores than those without comorbidities. Hao et al8 suggested that as patients on hemodialysis who have comorbid diseases have a higher risk of developing depression and anxiety than those without comorbid diseases, public health officials should pay more attention to their psychological welfare during the pandemic. In addition, Lee et al suggested that excessive and indiscriminate acquisition of information during an infectious disease epidemic may aggravate public anxiety and stress.37 Therefore, excessive search for information on infectious diseases should be avoided.38
In the present study, the health literacy level of patients undergoing hemodialysis was negatively correlated with their CAS and generalized anxiety scores. In addition, the results of this study confirmed a positive correlation between the time spent acquiring health information and CAS. During the recent COVID-19 pandemic, people with low health literacy level have been reported to have higher levels of anxiety and worry than those with adequate health literacy level. These results are the same for both the general population and patients with moderate renal impairment.39,40 However, previous research on the correlation between health literacy and anxiety levels during the COVID-19 pandemic has been limited. Therefore, further investigation is needed to determine whether interventions for the improvement of health literacy can potentially improve mental health outcomes in public health emergencies, such as a pandemic.
This study has several limitations. First, this study was conducted by conveniently selecting CKD patients receiving dialysis in artificial kidney rooms of two university hospitals when the spread of the mutant variants of COVID-19 and vaccination at the national level began in South Korea. Thus, the generalization of the results of the present study is limited. Second, the data analyzed in this study were collected in July 2021 and do not reflect recent trends attributable to the spread of the Omicron variants. Third, since the CAS is focused on the assessment of physical functional anxiety, it is likely that people with anxiety but without physical dysfunction were excluded from the analysis. Nevertheless, this study is significant in that it provides evidence of the need for the establishment of interventional programs for the improvement health literacy among patients undergoing hemodialysis during an infectious disease outbreak.
Conclusion
This study demonstrated that the health literacy levels of patients with CKD who are undergoing hemodialysis significantly differ according to age, educational level, and the presence of comorbidities. In addition, the results showed that health literacy level is negatively correlated with CAS and generalized anxiety scores. Therefore, it is very important for patients undergoing hemodialysis to find, understand, and apply the right health-related information to reduce anxiety during the outbreak of an infectious disease. Healthcare workers and health managers need to develop programs for the improvement of health literacy in consideration of the age, educational level, and underlying disease of the patient. A follow-up study on whether these educational programs improve health literacy and reduce anxiety in patients undergoing hemodialysis is recommended. In addition, more active social support is essential for patients with underlying diseases during the pandemic period.
Data Sharing Statement
The data that support the findings of this study are available from the first author on special request.
Acknowledgments
This study was conducted after additional research based on the master’s thesis of the first author, In Ju Yoon.
Ethics Approval
This study was conducted after reviewing the exemptions of the institutional review committees of two medical institutions (Hallym University Kangnam Sacred Heart Hospital; HKS 2021-06-010, Hallym University Sacred Heart Hospital; HALLYM 2021-06-006-001) and conducted in line with Helsinki Declaration principles.
Funding
There is no funding to report.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Hong YA, Ban TH, Kang CY, et al. Trends in epidemiologic characteristics of end-stage renal disease from 2019 Korean Renal Data System (KORDS). Kidney Res Clin Pract. 2021;40(1):52. doi:10.23876/j.krcp.20.202
2. Jablonski A. The multidimensional characteristics of symptoms reported by patients on hemodialysis. Nephrol Nurs J. 2007;34(1):29.
3. Gerogianni G, Lianos E, Kouzoupis A, et al. The role of socio-demographic factors in depression and anxiety of patients on hemodialysis: an observational cross-sectional study. Int Urol Nephrol. 2018;50(1):143–154. doi:10.1007/s11255-017-1738-0
4. Cukor D, Coplan J, Brown C, et al. Depression and anxiety in urban hemodialysis patients. Clin J Am Soc Nephrol. 2007;2(3):484–490. doi:10.2215/CJN.00040107
5. Kim SR. Depression and anxiety in maintenance hemodialysis patients: a single center study. Korean J Nephrol. 2010;733–741. doi:10.1186/s12912-021-00584-5
6. Buheji M, da Costa Cunha K, Beka G, et al. The extent of covid-19 pandemic socio-economic impact on global poverty. a global integrative multidisciplinary review. Am J Econ. 2020;10(4):213–224. doi:10.5923/j.economics.20201004.02
7. Bao Y, Sun Y, Meng S, Shi J, Lu L. 2019-nCoV epidemic: address mental health care to empower society. Lancet. 2020;395(10224):e37–e38. doi:10.1016/S0140-6736(20)30309-3
8. Hao W, Tang Q, Huang X, Ao L, Wang J, Xie D. Analysis of the prevalence and influencing factors of depression and anxiety among maintenance dialysis patients during the COVID-19 pandemic. Int Urol Nephrol. 2021;53(7):1453–1461. doi:10.1007/s11255-021-02791-0
9. Dadaczynski K, Okan O, Messer M, et al. Digital health literacy and web-based information-seeking behaviors of university students in Germany during the COVID-19 pandemic: cross-sectional survey study. J Med Internet Res. 2021;23(1):e24097. doi:10.2196/24097
10. Islam MS, Sarkar T, Khan SH, et al. COVID-19–related infodemic and its impact on public health: a global social media analysis. Am J Trop Med Hyg. 2020;103(4):1621. doi:10.4269/ajtmh.20-0812
11. Abel T, McQueen D. Critical health literacy and the COVID-19 crisis. Health Promot Int. 2020;35(6):1612–1613. doi:10.1093/heapro/daaa040
12. Wolf MS, Serper M, Opsasnick L, et al. Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the US outbreak: a cross-sectional survey. Ann Intern Med. 2020;173(2):100–109. doi:10.7326/M20-1239
13. Oldach BR, Katz ML. Health literacy and cancer screening: a systematic review. Patient Educ Couns. 2014;94(2):149–157. doi:10.1016/j.pec.2013.10.001
14. Lincoln A, Paasche MK, Cheng DM, et al. Impact of health literacy on depressive symptoms and mental health‐related: quality of life among adults with addiction. J Gen Intern Med. 2006;21(8):818–822. doi:10.1111/j.1525-1497.2006.00533.x
15. Sudore RL, Mehta KM, Simonsick EM, et al. Limited literacy in older people and disparities in health and healthcare access. J Am Geriatr Soc. 2006;54(5):770–776. doi:10.1111/j.1532-5415.2006.00691.x
16. Lee MS. Health literacy and health behaviors among older adults with cardio-cerebrovascular disease residing in rural areas. Korean J Adult Nurs. 2017;29(3):256–265. doi:10.7475/kjan.2017.29.3.256
17. Cho YM, Seo YH, Park MJ. Relationship between uncertainty in illness, subjective health status, and compliance with sick role behavior according to levels of health literacy in hemodialysis patients. Korean J Adult Nurs. 2018;30(4):437–446. doi:10.7475/kjan.2018.30.4.437
18. Choi HS, Han KD, Oh TR, et al. Trends in the incidence and prevalence of end-stage renal disease with hemodialysis in entire Korean population: a nationwide population-based study. Medicine. 2021;100:13. doi:10.1097/MD.0000000000025293
19. Davison S, Jhangri G, Johnson J. Cross-sectional validity of a modified Edmonton symptom assessment system in dialysis patients: a simple assessment of symptom burden. Kidney Int. 2006;69(9):1621–1625. doi:10.1038/sj.ki.5000184
20. Indino K, Sharp R, Esterman A. The effect of health literacy on treatment adherence in maintenance haemodialysis patients: a cross-sectional study. Ren Soc Australas J. 2019;15(1):11–18.
21. Jeong H, Kim OS. Anxiety, depression and health behavior of elderly with chronic diseases. Nurs Sci. 2013;25(2):35–46.
22. Lee KS, Kim HY, Lee MH. Factors influencing psychosocial adjustment in hemodialysis patients. Korean J Adult Nurs. 2019;31(1):38–49. doi:10.7475/kjan.2019.31.1.38
23. Kang MK, Kang SM, Kim SY. Moderating roles of public services in the quality of life of hemodialysis patients within the context of social support. J Korean Contents Assoc. 2013;13(11):277–287. doi:10.5392/JKCA.2013.13.11.277
24. Ishikawa H, Takeuchi T, Yano E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care. 2008;31(5):874–879. doi:10.2337/dc07-1932
25. Duffy ME. Translating instruments into other languages: basic considerations. Clin Nurse Spec. 2006;20(5):225–226. doi:10.1016/j.ijnurstu.2017.07.015
26. Shi J, Mo X, Sun Z. Content validity index in scale development. J Cent South Univ Med Sci. 2012;37(2):152–155. doi:10.3969/j.issn.1672-7347.2012.02.007
27. Lee SA. Coronavirus anxiety scale: a brief mental health screener for COVID-19 related anxiety. Death Stud. 2020;44(7):393–401. doi:10.1080/07481187.2020.1748481
28. Choi E, Lee J, Lee SA. Validation of the Korean version of the obsession with COVID-19 scale and the Coronavirus anxiety scale. Death Stud. 2022;46(3):608–614. doi:10.1080/07481187.2020.1833383
29. Spitzer RL, Kroenke K, Williams JB; Group PHQPCS. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA. 1999;282(18):1737–1744. doi:10.1001/jama.282.18.1737
30. Seo JG, Park SP. Validation of the Generalized Anxiety Disorder-7 (GAD-7) and GAD-2 in patients with migraine. J Headache Pain. 2015;16(1):1–7. doi:10.1186/s10194-015-0583-8
31. Taylor DM, Fraser S, Dudley C, et al. Health literacy and patient outcomes in chronic kidney disease: a systematic review. Nephrol Dial Transplant. 2018;33(9):1545–1558. doi:10.1093/ndt/gfx293
32. Seo NS, Sim EK. Influence of social support and health literacy on treatment adherence in hemodialysis patients. J Korean Acad Ind Cooperation Soc. 2020;21(7):656–666. doi:10.5762/KAIS.2020.21.7.656
33. Van der Heide I, Wang J, Droomers M, et al. The relationship between health, education, and health literacy: results from the Dutch adult literacy and life skills survey. J Health Commun. 2013;18(sup1):172–184. doi:10.1080/10810730.2013.825668
34. Park E, Jung Y. The association of medical service and medication use information literacy with multi-morbidity. Health Soc Welfare Rev. 2020;40(2):222–243.
35. Rehman U, Yıldırım M, Shahnawaz MG. A longitudinal study of depression, anxiety, and stress among Indians during COVID-19 pandemic. Psychol Health Med. 2022;1–9. doi:10.1080/13548506.2021.2023751
36. Benatov J, Ochnik D, Rogowska AM, Arzenšek A, Mars Bitenc U. Prevalence and sociodemographic predictors of mental health in a representative sample of young adults from Germany, Israel, Poland, and Slovenia: a longitudinal study during the COVID-19 pandemic. Int J Environ Res Public Health. 2022;19(3):1334. doi:10.3390/ijerph19031334
37. Lee DH. The influence of public fear, and psycho-social experiences during the coronavirus disease 2019(COVID-19) pandemic on depression and anxiety in South Korea. Korean J Counsel Psychother. 2020;32:2119–2156. doi:10.23844/kjcp.2020.11.32.4.2119
38. Asmundson GJ, Taylor S. Coronaphobia: fear and the 2019-nCoV outbreak. J Anxiety Disord. 2020;70:102196. doi:10.1016/j.janxdis.2020.102196
39. Tran TV, Nguyen HC, Pham LV, et al. Impacts and interactions of COVID-19 response involvement, health-related behaviours, health literacy on anxiety, depression and health-related quality of life among healthcare workers: a cross-sectional study. BMJ Open. 2020;10(12):e041394. doi:10.1136/bmjopen-2020-041394
40. Dorans KS, Wright-Nunes JA, Schaubel DE, et al. Associations of anxiety during the COVID-19 pandemic with patient characteristics and behaviors in CKD patients: findings from the Chronic Renal Insufficiency Cohort (CRIC) study. Kidney. 2022;3(8):1341–1349. doi:10.34067/KID.00002220
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.