Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Health Extension Workers Knowledge and Associated Factors on Child Immunization in Bako Tibe, West Shewa, Oromia, Ethiopia: A Cross-Sectional Study
Received 14 August 2021
Accepted for publication 23 September 2021
Published 7 October 2021 Volume 2021:14 Pages 2827—2832
DOI https://doi.org/10.2147/JMDH.S334230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Belachew Umeta,1 Biniyam Girma2
1School of Pharmacy, Department of Pharmaceutical Sciences, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia; 2School of Pharmacy, Department of Pharmacology, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Belachew Umeta Tel +251901649597
Email [email protected]
Purpose: To assess health extension workers knowledge of child immunization schedules and associated factors.
Methods: A cross-sectional study design was conducted among health extension workers working in Bako Tibe Woreda. The data were collected by using semi-structured questionnaires, and descriptive statistics were used to summarize the data. Chi-square (χ2) was used to identify factors associated with the knowledge of health extension workers on the immunization schedules.
Results: The response rate of the study was 92.1% (58/63). All of the health extension workers included in the study were females. The majority of health extension workers 45 (77.59%) had satisfactory knowledge of the child immunization schedule. Educational status (χ2 = 11.05; P= 0.001), work experience of as health extension workers (χ2 = 6.22; P= 0.045), on job training on immunization (χ2 = 11.12; P= 0.002), marital status (χ2 = 6.30; P= 0.019) were factors associated with health extension workers knowledge.
Conclusion: The majority of health extension workers had satisfactory knowledge of the child immunization schedule. Educational status, work experience as health extension worker, on job training on immunization, and marital status were factors associated with the knowledge of health extension workers on the child immunization schedule.
Keywords: health extension workers, immunization schedule, vaccination, community health workers
Introduction
Since the Alma-Ata Declaration in 1978, community health worker (CHW) cadres have been occurring in many countries. Nowadays, their roles in primary healthcare have been getting recognition due shortage of human resources in low- and middle-income countries. Community health workers (CHWs) are effective in the context of a wide variety of health programs. For effective implementation of their programs, both community health workers (CHW) and their respective supervisors require training that strengthens their skills, knowledge, and attitude towards the program package.1
To improve primary healthcare coverage and ensure accessibility of the community to basic health services, Ethiopia has launched a new community-based initiative called the Health Extension Program (HEP) in the year 2003. Under the program, female community health workers were trained for one year, named health extension workers (HEWs), and deployed to rural areas.2,3 The program has four packages: - disease prevention and control, family health, hygiene and environmental sanitation, health education and communication, and targeted at household and community level.
Health extension workers (HEWs) are secondary school graduates selected from the communities they serve and are supposed to work at the health post level for 25% of their time and in the community for the remaining. Since 2003, over 38,000 health extension workers (HEWs) are employed in Ethiopia. They are accountable for health centers and the administration of kebeles (lowest administrative unit). A health center is linked with five health posts, and together they form a primary healthcare unit. A health post serves 5000 population on average and is staffed by two health extension workers. Health professionals from the health centers supervise HEWs, and therefore the HEWs refer clients in need of upper-level healthcare to health centers. The administrations of the kebeles are responsible for giving support to the HEWs.4–6
Vaccination decreases the burden of infectious disease and health care costs and is successful in the prevention of childhood illness. It is an effective intervention for preventing infectious diseases. An effective vaccination schedule requires essential and good quality vaccines to be available. To deliver an effective and potent vaccine, well-trained professionals, a reliable transport/storage system, and efficient management procedures are required.7,8
In 1974, the WHO launched the expanded program of immunization (EPI). Even though EPI was launched long ago, 29% of child mortality worldwide was due to vaccine-preventable diseases. An assessment carried out in more than 70 countries between 2010 and 2012 found that only 29% of countries meet its minimum recommended standards for temperature control, and merely less than 10% of countries met out of 24 countries in 2013. Maintaining the quality of vaccines has been one of the main challenges of immunization programs in Africa.8,9 Several studies were conducted to estimate health professionals knowledge of immunization programs. A study in the United States indicates a lack of refrigerator temperatures that fell within the acceptable range.10 The other studies from Malaysia and south India reported that only 5.6% of clinics adhere to the guideline.11,12
Different studies reported factors affecting immunization programs. From these, gender, work experience, type and level of professionalism, training on immunization were factors. Although immunization coverage is high in Ethiopia, outbreaks, morbidity, and mortality from vaccine-preventable diseases (like measles, pertussis, and neonatal tetanus (NNT)) are still happening in different parts.13 Studies conducted so far mainly focused on the coverage of the service. However, issues regarding HEWs knowledge on immunization schedules were not as detailed. Therefore, the study aimed to assess knowledge of HEWs on immunization schedules and associated factors. The finding could try to answer the discrepancy between high vaccination coverage, vaccine potency, and the occurrence of frequent outbreaks from vaccine-preventable diseases.
Materials and Methods
Study Design and Setting
The institutional-based descriptive cross-sectional study design was employed. Bako is located West of Addis Ababa and is Located in the western margin of the West Shewa Zone. The Woreda have a total population of 123,558. Of which 81.5% (100,709) in rural, whereas the remaining was an urban population. As per the Woreda health bureau, there were 32 health posts during the data collection, of which 28 of them were in rural parts of the Woreda. The study was conducted from April to May 2019.
Participants and Sampling Technique
Each health posts in the Woreda have two health extension workers except one health post. Sixty-three (63) health extension workers were working in both rural and urban health posts of the Woreda. All Health extension workers who were volunteers to participate were included in the study. Health extension workers who were unavailable during the data collection period were excluded. Since all of the HEWs working in the study setting were eligible, we did not use any specific sampling technique. Rather, the focus was on ensuring the participation of as many HEWs as possible. Trained graduating pharmacy students collected the data. The data were collected by interviewing all the health extension workers during their annual meeting at the Woreda Health bureau.
Data Collection Tools and Techniques
Semi-structured questionnaires were used for the data collection from the health extension workers. The questionnaires were prepared in English by reviewing the World Health Organization (WHO) guideline for children immunization schedule (https://www.who.int/countries/eth/areas/immunization/routine/en/index3.html) and Ethiopian Federal Ministry of Health (FMOH) guidelines for the national expanded program on immunization
The questionnaires consist of the following parts: Socio-demographic characteristics (sex, marital status, educational status, years served as health extension workers, on the job training on vaccination use and schedule, days of participation in training, and need of HEWs for training on immunization schedule), knowledge about immunization schedule (vaccine given at birth, vaccine given orally, vaccine given at six weeks, vaccine given at ten weeks, vaccines given at 14th weeks, vaccines given at 9th months, and storage temperature of vaccines) and availability of infrastructures (power supply/electricity, refrigerator, EPI guideline).
Main Outcome Variable Measurement
We did not get a standardized guideline to evaluate the knowledge of health extension workers. We used previous literature reporting systems to assess the knowledge of health professionals.13 Accordingly, the knowledge was reported as if the HEWs had satisfactory knowledge or not satisfactory knowledge on the immunization schedule. Seven items were included under the knowledge part, and the maximum knowledge score is 7, and the minimum was 0. The HEWs who answered half of the questions under knowledge parts are classified as they had satisfactory knowledge.
Data Management and Analysis
Data were entered and cleaned using Epi Info software and exported to SPSS version 20 for further analysis. Descriptive statistics were used for organizing, describing, and summarizing the data. Chi-square (χ2) was used to check the association of independent variables with the dependent variable. P-value <0.05 was used to declare significance.
Ethical Consideration
The study protocol was reviewed and approved by the Ethical Review Committee of Jimma University Institute of Health. Verbal informed consent was approved by the Ethical review committee and obtained from the health extension workers after the purpose and methods of the study had been explained in detail. And their response kept anonys.
Results
Socio Demographic Characteristics
Out of 63 HEWs working in Bako Tibe Woredas, 58 (92.1%) had participated in the study. All of the HEWs were females, and all of them had EPI books for Immunization use and schedule. The majority, 39 (62.24%), were unmarried/single. Nearly half of respondents, 27 (46.5%), served as HEWs for 4–6 years; the majority, 30 (51.7%) them had 10+2+ educational status, and 43 (74.1%) of them took on job training given on immunization use and schedule. Of these participating in the training, 37 (72.5%) participated for less than four days. All of the HEWs reported they need refresher training on the immunization schedule. All of the health extension workers participated in the study had EPI guideline for immunization schedule supplied by Ethiopian Federal Ministry of Health (Table 1).
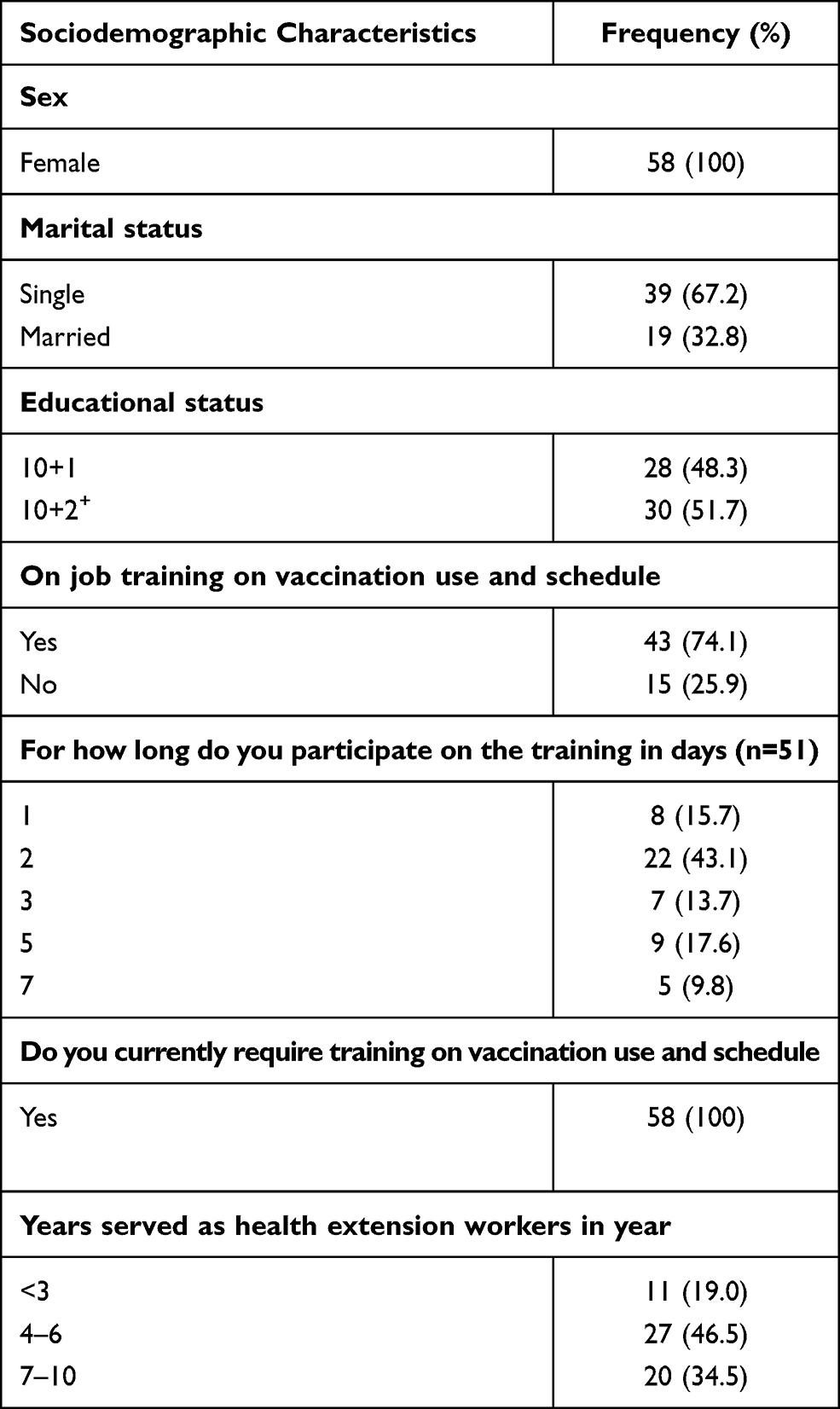 |
Table 1 Sociodemographic Characteristics of Health Extension Workers Working in Bako Tibe Woreda |
Availability of Infrastructure
From 32 health posts included in the study, only 8 (27.59%) of them had a refrigerator. Of those, only 3 (37.5%) of them had a functional refrigerator, and nearly one-fourth 6 (10.34%) of the health posts had a power supply and/electricity (Table 2).
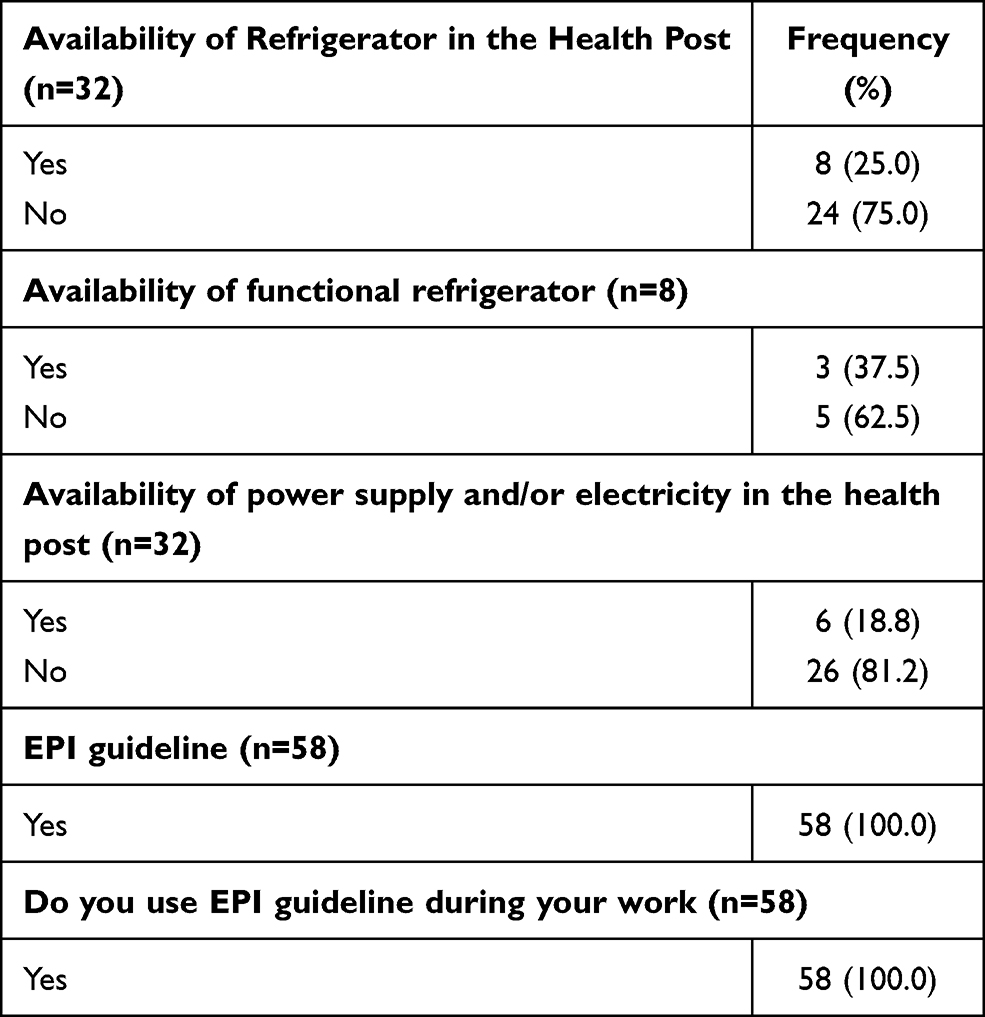 |
Table 2 Availability of Infrastructure in Bako Tibe Woreda Health Posts |
Knowledge of Health Extension Workers About Child Immunization Schedule and Factors Associated with Their Knowledge
More than half, 45 (77.59%) of the health extension workers had satisfactory knowledge of the immunization schedule. Educational status, year of experience as a health extension worker, on job training on immunization schedule and marital status were factors affecting the knowledge of health extension workers on Immunization schedules (Table 3).
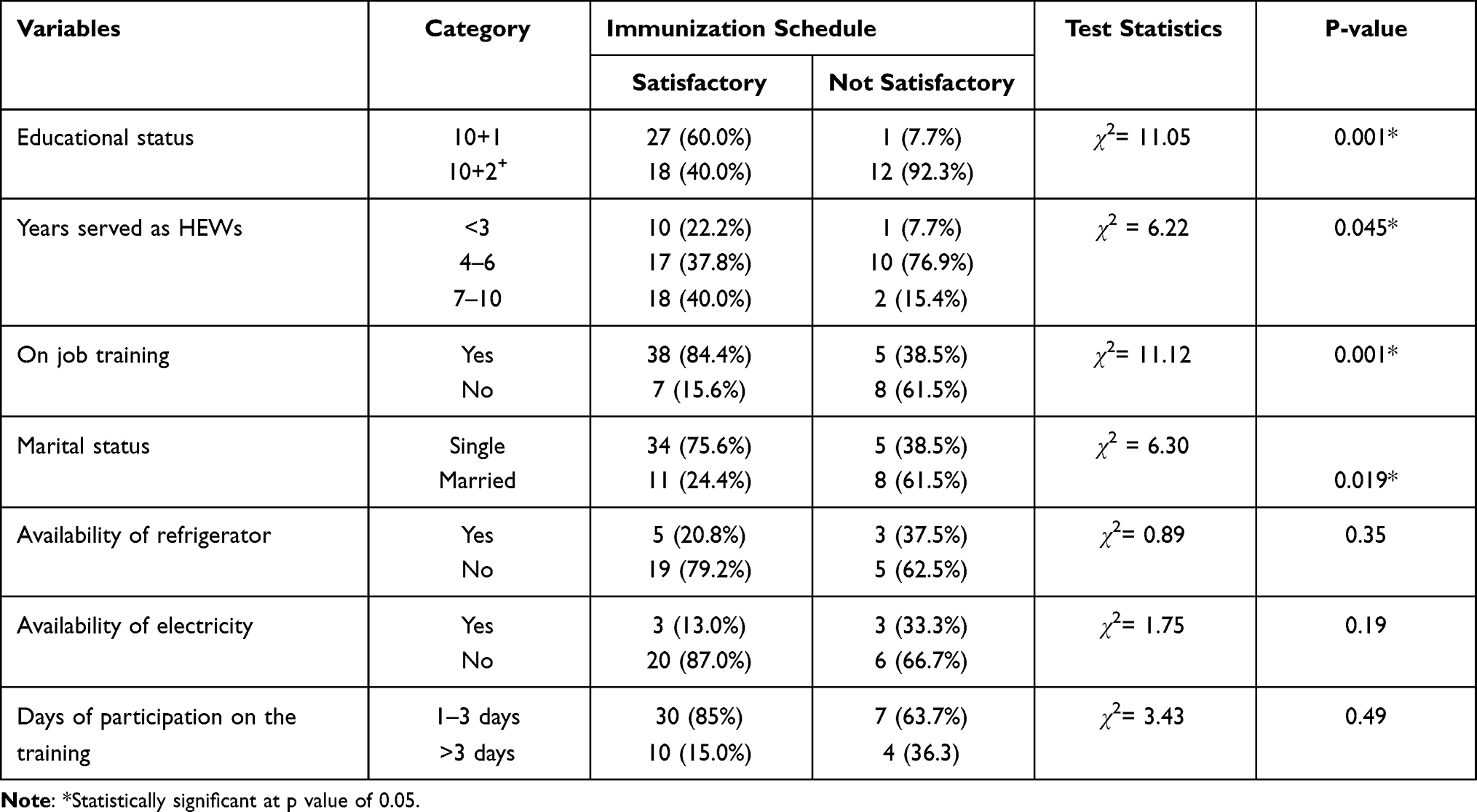 |
Table 3 Factors Associated with the Knowledge of Health Extension Workers on Child Immunization Schedules |
Discussion
Vaccination is one of the most efficient and successful health interventions for the reduction of child morbidity and mortality.14 The Health Extension Program is one of the most innovative community-based health programs in Ethiopia. The program is based on the assumption: access to and quality of primary healthcare in rural communities can be improved by transferring knowledge and skills to households. The program enabled Ethiopia to increase primary health care coverage from 76.9% in 2005 to 90% in 2010.15,16
This study provides insight into Health Extension Workers knowledge of immunization schedules and their related factors. The study showed that 77% of health extension workers had satisfactory knowledge of the child Immunization schedules. Around 79% of the health extension workers described the correct storage temperature range for vaccines. The finding is nearly comparable with the study conducted in Ethiopia Gurage zone in 201913 and western India,17 in which around 71% and 80% of the participants described the correct storage temperature for vaccines, respectively. However, it is different from the study conducted in Bale zone Ethiopia in 2018, in which 67.8% of the respondents were able to describe the correct temperature range for vaccine storage.10 This difference might be due to differences in professional qualifications and availability of infrastructures like electricity and refrigerator.
One-tenth (9.34%) of the health post had a functional refrigerator. The finding was different from the study done in the Ethiopia Gurage zone in 2019,13 central Ethiopia in 2016,18 North-West regions of Cameron19 and Ethiopia Bale zone9 in 2018 in which 22.8%, 19%, 95.1% and 62.5 of the health facilities had functional refrigerators, respectively. This difference might be due to the difference in study sites as the above studies include the different types of health facilities. But, the present study only includes the health posts and differences in study purpose.
The majority (77.9%) of the health extension workers had satisfactory knowledge of child immunization. This finding was higher than the study conducted in Thailand to assess health workers knowledge and practice regarding expanded immunization programs, in which 55.6% of the participants had provided the correct answer for immunization schedule.20 And the study was also conducted in India to assess the mother’s knowledge of the immunization schedule of their child and reported 76% of the participants had poor knowledge.21 The discrepancy might be due to differences in the study unit and sample size. The finding was comparable with the study conducted in Nigeria reporting, 76% of the participants had adequate knowledge of the National Immunization Schedule for children with accurate knowledge of vaccine dosages, routes of administration and intervals between doses.22 The finding was lower than the study conducted in Nigeria among pregnant mothers reporting 91.8% of the participants had good knowledge of child immunization schedule.22
Different factors associated with the knowledge of health extension workers on immunization schedules in the study area. From which, educational status, experience, on job training and marital status were the factors determining the knowledge status of health extension workers on immunization schedules. Health extension workers who had an educational status of 10+1 had better knowledge of child immunization schedules than their friends having 10+2 and over. The reason might be because all health extension workers were using EPI guidelines during their work, and 10+2 and above health extension workers might not update themselves. But their friends might update themselves regularly. The other study also showed the association between the knowledge and practice of health extension workers and level of educational, year of experience and training.23 Several studies associated the knowledge of health workers with level of education, year of experience, on the job training and marital status.7,13,18
Limitation of the Study
The study includes the health extension workers working only in Bako Tibe Woreda. Therefore, the finding might not be generalized for all health extension workers working in the country. The study also might have measurement error as their knowledge was measured by categorizing them into two groups of satisfactory and unsatisfactory. In addition, the unavailability of similar literature makes it difficult to compare.
Conclusions and Recommendations
The majority of health extension workers had satisfactory knowledge of the child immunization schedule. Educational status, experience, on the job training, and marital status were factors associated with knowledge on the child immunization schedules. Even though 75% of the health extension workers had satisfactory knowledge of the child immunization schedule, the Federal Ministry of Health (Ethiopia), Woreda Health Bureau, and other stakeholders have to enforce the use of EPI guidelines supplied for the health extension workers.
Data Sharing Statement
The data set used for analysis is available from the corresponding author upon request.
Ethical Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Jimma University Institute of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aitken I. Training community health workers for large-scale community-based health care programs. In: Developing and Strengthening Community Health Worker Programs at Scale: A Reference Guide and Case Studies for Program Managers and Policymakers. Baltimore: Jhpiego; 2014:9.
2. Medhanyie A, Spigt M, Dinant G, Blanco R. Knowledge and performance of the Ethiopian health extension workers on antenatal and delivery care: a cross-sectional study. Hum Resour Health. 2012;10(1):44. doi:10.1186/1478-4491-10-44
3. Mangham-Jefferies L, Mathewos B, Russell J, Bekele A. How do health extension workers in Ethiopia allocate their time? Hum Resour Health. 2014;12(1):61. doi:10.1186/1478-4491-12-61
4. Kok MC, Kea AZ, Datiko DG, et al. A qualitative assessment of health extension workers’ relationships with the community and health sector in Ethiopia: opportunities for enhancing maternal health performance. Hum Resour Health. 2015;13(1):80. doi:10.1186/s12960-015-0077-4
5. Girmay AM, Evans MR, Gari SR, Gebremariam AG, Reta MT. Urban health extension service utilization and associated factors in the community of Gullele sub-city administration, Addis Ababa, Ethiopia. Int J Community Med Public Health. 2019;6(3):976–985. doi:10.18203/2394-6040.ijcmph20190580
6. Tilahun H, Fekadu B, Abdisa H, et al. Ethiopia’s health extension workers use of work time on duty: time and motion study. Health Policy Plan. 2017;32(3):320–328.
7. Ogboghodo EO, Omuemu VO, Odijie O, Odaman OJ. Cold chain management practices of health care workers in primary health care facilities in Southern Nigeria. Pan Afr Med J. 2017;27:34. doi:10.11604/pamj.2017.27.34.11946
8. Bogale HA, Amhare AF, Bogale AA. Assessment of factors affecting vaccine cold chain management practice in public health institutions in east Gojam zone of Amhara region. BMC Public Health. 2019;19(1):1433. doi:10.1186/s12889-019-7786-x
9. Woldemichael B, Bekele D, Esmael A. Cold chain status and knowledge of vaccine providers at primary health care of units Bale Zone, Southeast Ethiopia: cross-sectional study. Immunome Res. 2018;14(1):2. doi:10.4172/1745-7580.1000152
10. Woodyard E, Woodyard L, Alto WA. Vaccine storage in the physician’s office: a community study. J Am Board Fam Pract. 1995;8(2):91–94.
11. Azira B, Norhayati MN, Norwati D. Knowledge, attitude and adherence to cold chain among general practitioners in Kelantan, Malaysia. Int J Collab Res Intern Med Public Health. 2013;5(3).
12. Rao S, Naftar S, Baliga S, Unnikrishnana B. Evaluation, awareness, practice and management of cold chain at the primary health care centers in Coastal South India. J Nepal Paediatr Soc. 2012;32(1):19–22.
13. Yassin ZJ, Yimer Nega H, Derseh BT, Sisay Yehuala Y, Dad AF. Knowledge of health professionals on cold chain management and associated factors in Ezha District, Gurage Zone, Ethiopia. Scientifica. 2019;2019:6937291. doi:10.1155/2019/6937291
14. WHO, UNICEF. Global Immunization Vision and Strategy 2006–2015. Geneva: WHO, Department of Immunization, Vaccines and Biologicals; 2005.
15. Banteyerga H. Ethiopia’s health extension program: improving health through community involvement. MEDICC Rev. 2011;13:46–49.
16. Bilal NK, Herbst CH, Zhao F, Soucat A, Lemiere C. Health extension workers in Ethiopia: improved access and coverage for the rural poor. Yes Afr Can. 2011;24:433–443.
17. Naik AK, Rupani MP, Bansal RK. Evaluation of vaccine cold chain in urban health centers of municipal corporation of Surat city, Western India. Int J Prev Med. 2013;4(12):1395–1401.
18. Rogie B, Berhane Y, Bisrat F. Assessment of cold chain status for immunization in central Ethiopia. Ethiop Med J. 2013;51(Suppl 1):21–29.
19. Yakum MN, Ateudjieu J, Walter EA, Watcho P. Vaccine storage and cold chain monitoring in the North West region of Cameroon: a cross sectional study. BMC Res Notes. 2015;8(1):145. doi:10.1186/s13104-015-1109-9
20. Widsanugorn O, Suwattana O, Harun-Or-Rashid M, Sakamoto J. Healthcare workers’knowledge and practices regarding expanded program on immunization in kalasin, Thailand. Nagoya J Med Sci. 2011;73(3–4):177.
21. Vinish V. Mother’s knowledge on immunization schedule of her child: a descriptive Survey. Manipal J Nurs Health Scie. 2016;2(2):41–45.
22. Awosan KJ, Ibrahim MT, Yunusa EU, Isah BA, Raji MO, Abubakar N. Knowledge, attitude and compliance with full immunization of children against vaccine preventable diseases among pregnant mothers in Sokoto, Nigeria. Int J Contemp Med Res. 2018;5(6):F10–F16.
23. Befekadu A, Yitayal M. Knowledge and practice of health extension workers on drug provision for childhood illness in west Gojjam, Amhara, Northwest Ethiopia. BMC Public Health. 2020;20(1):1. doi:10.1186/s12889-020-08602-y
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.