Back to Journals » Risk Management and Healthcare Policy » Volume 19
Health Equity Barriers to Accessing Vaccination and Screening Services in Low- and Middle-Income Countries: A Narrative Review
Authors Sinuraya RK ![]() , Postma MJ, Puspitasari IM
, Postma MJ, Puspitasari IM ![]() , Suwantika AA
, Suwantika AA ![]()
Received 27 March 2026
Accepted for publication 11 June 2026
Published 22 June 2026 Volume 2026:19 612390
DOI https://doi.org/10.2147/RMHP.S612390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Rano K Sinuraya,1,2 Maarten J Postma,3,4 Irma M Puspitasari,1,2 Auliya A Suwantika1,2
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Department of Health Sciences, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands; 4Department of Economics, Econometrics & Finance, Faculty of Economics & Business, University of Groningen, Groningen, the Netherlands
Correspondence: Rano K Sinuraya, Email [email protected]
Abstract: Vaccination and screening services are essential components of preventive care, yet access to these services remains unequal in many low- and middle-income countries (LMICs). This narrative review examines health equity barriers affecting access to vaccination and screening services in LMICs, with screening evidence drawn predominantly from cervical cancer/HPV-related programs and selected other preventive screening contexts, and identifies strategies to improve equity in preventive care. Relevant English-language literature was identified through PubMed and Scopus and synthesized thematically. The review examined cross-cutting equity barriers across vaccination and the screening contexts represented in this evidence base. Barriers operated across individual and household, community and sociocultural, health system, and policy and structural domains. Common barriers included poverty, transportation costs, low health literacy, stigma, weak primary care, workforce shortages, and inadequate financing. Vaccination-specific challenges included weak cold-chain systems, reliance on campaign-based delivery, vaccine hesitancy, and missed immunization schedules, whereas screening-specific challenges included repeated visits, weak referral and follow-up systems, stigma related to cancer and reproductive health screening, and delayed diagnosis. These barriers disproportionately affected rural populations, low-income households, women and girls, migrants, ethnic minorities, people with disabilities, and other marginalized groups, contributing to persistent inequities by income, gender, education, and rural–urban residence. Advancing equity in preventive care requires strengthening primary health care, reducing financial and geographic barriers, improving culturally responsive communication, using disaggregated data for equity-focused planning, and investing in workforce and service delivery improvements.
Keywords: health equity, vaccination, screening services, preventive care, low- and middle-income countries, access barriers
Introduction
Vaccination and screening services are among the most effective preventive health interventions for reducing avoidable morbidity and mortality.1 Vaccination helps prevent the spread of infectious diseases and protects both individuals and communities, while screening services support earlier detection and management of disease before complications arise.1,2 In low- and middle-income countries (LMICs), where health systems often face the combined challenges of infectious diseases, rising noncommunicable diseases, and persistent maternal and child health needs, these services are especially important.2 Beyond improving population health, they can also reduce the long-term burden on already constrained health systems.1–3
Despite their importance, access to vaccination and screening services remains uneven across many LMICs.4 Increases in national service coverage have not always translated into equitable access across population groups.2 Disparities persist by income, education, gender, geography, and other dimensions of social disadvantage.5 People living in rural or underserved areas may face long travel distances, limited service availability, and weak infrastructure, while low-income households may struggle with both direct and indirect costs of care.4,6 Marginalized groups may also experience low health literacy, stigma, discrimination, and limited trust in health services, all of which can reduce uptake of preventive interventions.7
These persistent gaps underscore the need to examine preventive care through a health equity lens.8 In this context, the issue is not only whether services are available, but whether different groups are equally able to reach, afford, accept, and benefit from them.9 Barriers to access are often interconnected and may arise from socioeconomic disadvantage, geographic isolation, sociocultural influences, health system weaknesses, and broader policy or structural conditions.8,9
Reviewing vaccination and screening services together offers a useful perspective because, although these interventions differ in delivery and follow-up requirements, they share a common preventive purpose and are shaped by many of the same equity-related constraints. Both depend on awareness, affordability, physical accessibility, trust, and health system readiness. In this review, screening services are understood as preventive services aimed at early detection across the screening contexts represented in the literature reviewed, rather than as a comprehensive synthesis of all screening programs. The screening evidence included in this review is more heavily concentrated in cervical cancer/HPV-related screening and a limited number of other preventive screening contexts. Bringing vaccination and screening services into one discussion allows identification of cross-cutting barriers that may be less visible when these services are examined separately. This integrative focus also distinguishes the present review from much prior work, which has typically examined either vaccination equity or barriers to a single screening programme in isolation, and has often emphasized differences in service coverage rather than equity-stratified access.4,10,11
This narrative review therefore examines health equity barriers affecting access to vaccination and screening services in LMICs. It focuses on socioeconomic, geographic, sociocultural, health system, and policy-related influences that shape unequal access to these essential preventive services. By synthesizing these barriers within a single framework, the review aims to provide a clearer understanding of inequities in preventive care and to inform more inclusive and equitable strategies for improving population health in LMICs.
Conceptualizing Health Equity in Preventive Care
Health equity provides an important lens for examining access to preventive care in low- and middle-income countries (LMICs).8 In the context of vaccination and screening services, the central issue is not only whether services are available, but whether different population groups are able to reach, use, and benefit from them equitably.8–10 This perspective draws attention to the social, economic, geographic, and structural conditions that shape unequal access.
An equity perspective is especially important because equal provision does not necessarily result in fair access.10 Preventive services may be formally available, yet remain less accessible in practice for people affected by poverty, low education, gender inequality, geographic isolation, disability, or social exclusion.9,10 Access should therefore be understood as multidimensional, involving not only service availability, but also affordability, physical accessibility, awareness, acceptability, and the appropriateness of service delivery.12 These dimensions align with established conceptualizations of access as a multidimensional, patient-centred process that spans perceiving a need and seeking, reaching, obtaining, and ultimately benefiting from care.13
In this review, barriers to vaccination and screening services are understood as operating across four interconnected levels. At the individual and household level, access may be influenced by income, education, health literacy, perceived risk, time constraints, and prior experiences with care.11,14,15 At the community and sociocultural level, social norms, gender expectations, religious beliefs, stigma, trust, and family and community influences may shape uptake.16–19 At the health system level, service availability, workforce capacity, stock-outs, waiting times, provider communication, and continuity of care affect whether preventive services can be used in practice.19–21 At the policy and structural level, financing arrangements, insurance coverage, governance, public health priorities, and broader patterns of inequality shape the conditions under which access is enabled or constrained.22–24
Together, these four levels provide the framework for this review and guide the analysis of barriers to equitable access to vaccination and screening services in LMICs. This framework is illustrated in Figure 1.
 |
Figure 1 Conceptual framework of health equity barriers to vaccination and screening services in low- and middle-income countries. Note: Equitable access to preventive care is shaped by interacting barriers at the individual and household, community and sociocultural, health system, and policy and structural levels. These barriers influence whether different population groups can access, use, and benefit from vaccination and screening services in LMICs. |
Health Equity Barriers to Vaccination and Screening Services in LMICs
Socioeconomic Barriers
Socioeconomic disadvantage is one of the most persistent barriers to equitable access to vaccination and screening services in low- and middle-income countries (LMICs). Although preventive services are often described as low-cost or free at the point of delivery, access is rarely cost-free in practice.4,25 Many individuals and households still face direct and indirect expenses, including transport costs, consultation fees, lost wages, and time away from work or caregiving. For economically vulnerable populations, these burdens can make preventive care difficult to prioritize, especially when more immediate household needs take precedence over services perceived as non-urgent.26
Across the literature, poverty shapes not only whether preventive services are used, but also when and how consistently they are used.27,28 Even small out-of-pocket costs may delay vaccination or discourage participation in screening services.23 This burden is often more pronounced for screening, which may require repeated visits, follow-up testing, referral, and treatment. Financial hardship can therefore disrupt the entire continuum of preventive care rather than only the initial point of access.29
Education and health literacy also play an important role in uptake. Individuals with limited formal education may have fewer opportunities to understand the purpose, timing, and value of vaccination and screening services, and may be less able to navigate complex health systems.4,30 Limited health literacy can reduce awareness of available services, weaken confidence in prevention, and increase vulnerability to misinformation. In many settings, these disadvantages intersect with poverty, gender inequality, and rural residence, creating compounded barriers to access.30
Digital exclusion is also becoming more relevant within this broader socioeconomic landscape.31 As appointment systems, reminders, health messaging, and service information become increasingly dependent on mobile phones and internet access, people without reliable digital access may face additional obstacles to accessing preventive care.32 Socioeconomic barriers therefore extend beyond income alone and include the wider material and informational conditions that shape whether preventive services are feasible, understandable, and accessible in everyday life.33
Geographic and Infrastructural Barriers
Geographic location remains a major determinant of access to preventive care in LMICs. People living in rural, remote, or otherwise underserved areas often face greater difficulty reaching health facilities, especially where services are concentrated in urban centers.34 Long travel distances, limited transport options, and poor road conditions can make vaccination and screening services physically difficult to access, particularly for populations already facing financial hardship.4,34
These disadvantages are often intensified by infrastructure limitations. In many LMIC settings, rural and peripheral areas are marked by shortages of health facilities, weak referral networks, and insufficient numbers of trained health workers.4 Such constraints reduce the availability of both routine vaccination and screening services and limit the continuity of care needed for follow-up, diagnosis, or treatment.4,34 Geographic inequity is therefore not simply a matter of distance, but also of uneven service capacity across places.34
The specific effects of these constraints differ somewhat by service type. In vaccination, weak cold-chain infrastructure can disrupt the storage and delivery of temperature-sensitive products, particularly in hard-to-reach areas.35 In screening, limited laboratory and diagnostic capacity may delay or prevent early detection altogether.36 Outreach approaches that could help reduce these gaps, such as mobile clinics or community-based preventive services, are often underdeveloped or inconsistently implemented. As a result, geographic and infrastructural barriers continue to shape who can realistically access preventive care and who remains excluded.4,34,36
Gender and Sociocultural Barriers
Gender norms and broader sociocultural conditions strongly influence the demand for, acceptance of, and engagement with preventive care. In many LMICs, women’s access to health services is shaped by restricted mobility, unequal decision-making power within households, limited control over financial resources, and social expectations surrounding caregiving and respectability.37,38 These constraints may affect women’s ability to seek vaccination for themselves or their children, as well as their participation in screening services, particularly those related to sexual and reproductive health.
Stigma is another important barrier. Some forms of screening, especially those associated with sexual health, reproductive health, or cancer, may be avoided because they are linked to shame, immorality, or social judgment.38,39 Adolescent girls and unmarried women may face especially strong stigma when seeking preventive services.39 At the same time, men may avoid care because prevailing norms of masculinity discourage help-seeking and reinforce the view that preventive care is unnecessary unless illness is already present.38,39
Trust, beliefs, and local health narratives also shape uptake. Mistrust of vaccines or screening services may arise from previous negative experiences, misinformation, low confidence in institutions, or community-level skepticism toward formal health care.40 Religious and cultural beliefs may further influence how prevention is understood, including whether vaccination is accepted, whether screening is considered necessary, and whether health care providers are seen as appropriate sources of care.41 These influences rarely operate in isolation; they interact with education, gender, language, and social position to shape how preventive services are interpreted and used.41,42
Language can also function as a barrier when services are not delivered in linguistically accessible or culturally responsive ways.43,44 Poor communication between providers and service users may reduce understanding, trust, and continuity of care.45 Taken together, these patterns show that access to preventive care depends not only on service availability, but also on whether services are socially acceptable, culturally meaningful, and trusted by the communities they are intended to serve.43–45
Beyond cultural acceptability, discrimination within health care settings can itself operate as a barrier to preventive care. Ethnic minorities, indigenous peoples, populations affected by histories of colonialism, and migrants frequently report experiences of disrespect, bias, and unequal treatment when interacting with health services, and such experiences can erode trust and discourage future engagement with vaccination and screening programs.46,47 These dynamics are not only a matter of individual provider attitudes; institutional racism, expressed through routine practices, organizational norms, and structural arrangements that systematically disadvantage particular groups, can shape who feels welcome, who is treated with dignity, and who ultimately returns for follow-up care.47,48 For migrant and post-colonial minority populations in particular, perceived or experienced discrimination in medical settings may compound language barriers, legal insecurity, and economic hardship, reducing continued attendance at appointments and contributing to lower uptake of preventive services.46,48 Addressing these patterns requires more than culturally sensitive communication alone; it calls for explicit attention to anti-discriminatory practice, respectful and equitable treatment, and organizational accountability so that preventive services are genuinely accessible to historically marginalized communities.46,48
Health System Barriers
Health system weaknesses can reproduce inequity even where preventive services are formally available.9 One of the most persistent challenges in LMICs is the shortage and uneven distribution of trained health workers. Workforce deficits often increase waiting times, reduce service quality, and limit the availability of vaccination and screening, particularly in rural and underserved settings.49 Under these conditions, preventive care may be delayed, inconsistently delivered, or deprioritized in favor of more immediate clinical demands.9,49
Provider training and service organization also affect access.50 When health workers are insufficiently trained in preventive care, communication, or follow-up procedures, patients may receive incomplete information, poor-quality counseling, or inconsistent care. This can weaken trust in services and reduce future uptake.50,51 These problems are especially significant in screening services, where the value of screening depends not only on initial access but also on timely diagnosis, referral, treatment, and continuity of care.24,52
Supply-side failures create further obstacles. Stock-outs of vaccines, test kits, and essential supplies can interrupt service delivery and discourage communities from returning for care.53 Long waiting times, inconvenient clinic schedules, overcrowding, and poor patient provider communication may further reduce the usability of services, especially for people already facing financial or social barriers.54 In practice, the existence of a formal service does not guarantee meaningful access if the health system lacks the capacity, reliability, or responsiveness needed to deliver it equitably.53,54
Policy, Governance, and Financing Barriers
Access to preventive care is also shaped by broader policy and structural conditions. Weak national strategies for preventive health can leave vaccination and screening fragmented, under-prioritized, or unevenly implemented across regions and population groups.55 Where planning is not explicitly equity-oriented, preventive services may expand overall while still failing to reach those facing the greatest disadvantage.55,56
Financing arrangements are particularly important. In many LMICs, inadequate insurance coverage, user fees, and reliance on out-of-pocket spending create financial barriers that discourage preventive care use.55,56 Even when services are nominally subsidized, the absence of broader financial protection may leave households exposed to transport costs, follow-up expenses, and treatment costs that make prevention less accessible in practice. Donor dependence may further complicate service delivery by creating instability, vertical programming, or misalignment between funding priorities and local needs.24,50,55
Governance and resource allocation also influence who is reached and who is left behind. Urban bias in infrastructure, staffing, and program investment can disadvantage rural and peripheral populations, while weak information systems may obscure inequities among marginalized groups.56 Without reliable data on coverage, uptake, and unmet need across different social groups, inequities are difficult to identify and address. Policy choices therefore do not simply determine whether preventive services exist, but how fairly they are distributed across populations.8,56
How Barriers Accumulate Among Marginalized Groups
Although many barriers to preventive care are widely shared, they are not distributed evenly across populations. In practice, socioeconomic, geographic, sociocultural, and health system barriers often accumulate within the same groups, producing compounded disadvantage in access to vaccination and screening services.4,34 Rural populations, for example, may encounter long travel distances, limited service availability, workforce shortages, and weak infrastructure at the same time.57 The urban poor may live closer to facilities but still face financial exclusion, overcrowded services, insecure employment, and poor living conditions that limit their ability to prioritize preventive care.57,58 Migrants, displaced populations, and ethnic or linguistic minorities may face exclusion related to legal status, mobility, language, discrimination, or mistrust of institutions. People with disabilities may encounter physical inaccessibility, limited accommodation, and services that are not designed to meet their needs.59,60
Women and adolescent girls may experience particularly layered forms of disadvantage, as gender norms often intersect with poverty, restricted mobility, stigma, and limited control over household resources.60 Children in underserved communities may miss vaccination or screening opportunities because of household poverty, low caregiver awareness, or weak service delivery systems.60,61 These examples illustrate that inequities in preventive care are not random; rather, they are concentrated among groups already affected by social, economic, geographic, or political marginalization.59,60
An equity-focused analysis must therefore consider not only general barriers, but also how those barriers combine within specific populations and settings. This is essential for understanding who is most likely to be left behind and for designing more targeted and inclusive preventive care strategies in LMICs.
Taken together, these barriers show that inequities in preventive care arise through the interaction of multiple forms of disadvantage, reinforcing the need for context-sensitive and equity-oriented strategies in LMICs.
Common and Distinct Equity Challenges in Vaccination and Screening Services
Although vaccination and screening services differ in their delivery models, follow-up requirements, and target conditions, they are shaped by many of the same equity barriers in low- and middle-income countries (LMICs). Both depend on people being able to reach services, understand their value, trust providers, and engage with health systems that are often under-resourced and unevenly distributed. At the same time, each service presents distinct operational challenges. Vaccination depends heavily on reliable supply chains, cold-chain systems, and sustained public confidence, whereas screening often requires repeated visits, timely diagnosis, referral, and treatment after the initial test. Distinguishing between shared and service-specific barriers helps clarify where integrated strategies may be effective and where more tailored responses are needed.
Shared Barriers
Vaccination and screening services are both shaped by broader social and health system inequities. Across the literature, common barriers include poverty, geographic isolation, low health literacy, weak primary care systems, workforce shortages, and social exclusion. These constraints rarely operate independently. Rather, they often overlap and reinforce one another, making preventive care especially difficult to access for populations already facing disadvantage (Table 1).
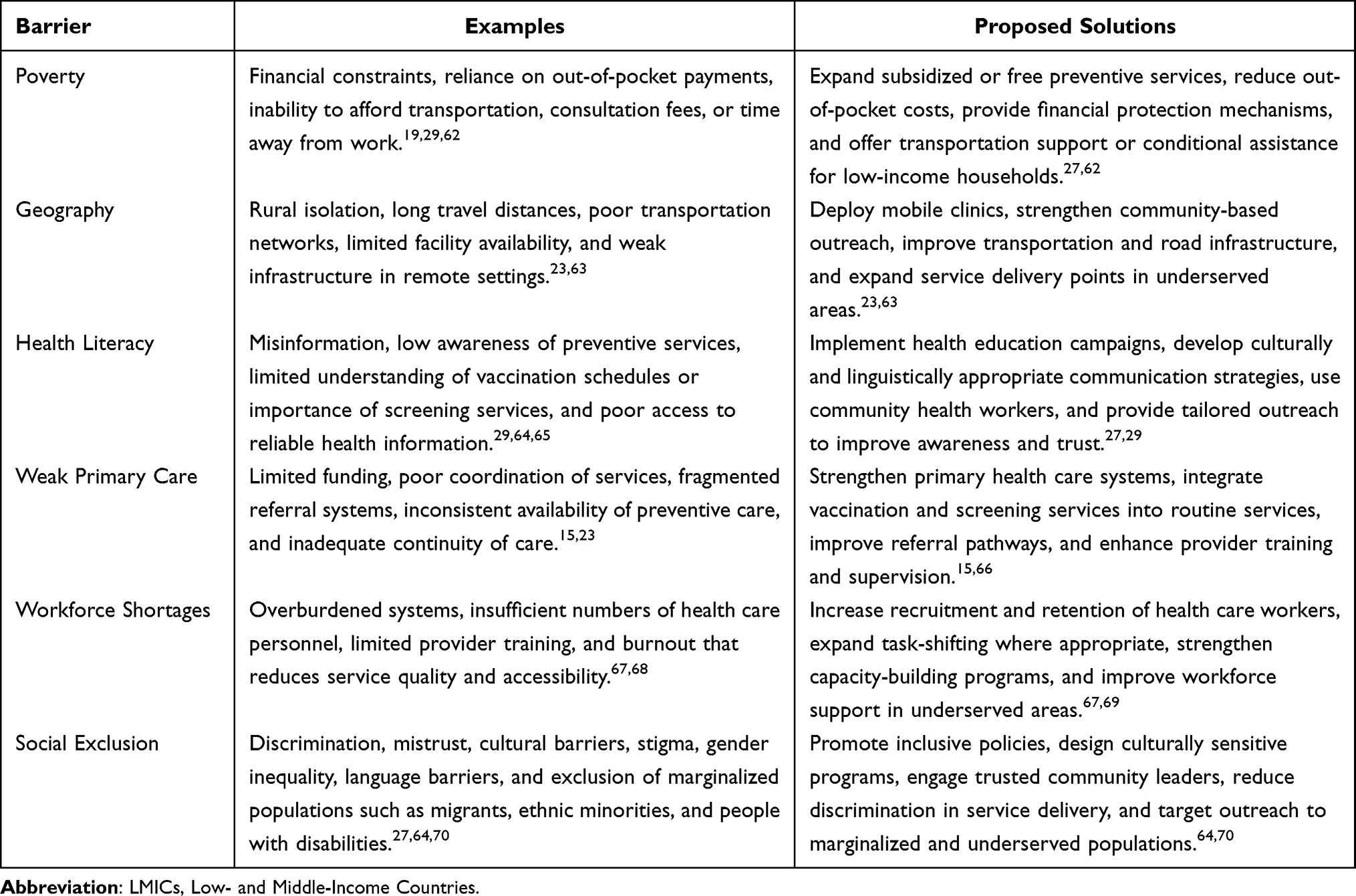 |
Table 1 Summary of Major Barriers to Equitable Access to Vaccination and Screening Services in LMICs |
While these barriers affect both services, their practical consequences are not always the same. Vaccination is particularly sensitive to supply continuity, cold-chain function, and public confidence, whereas screening depends more heavily on follow-up capacity, diagnostic pathways, and continuity of care after the initial encounter.
Vaccination-Specific Issues
Several equity challenges are especially pronounced in vaccination programs. One of the most important is cold-chain logistics. Vaccines depend on uninterrupted temperature control, which can be difficult to maintain in rural and remote settings where electricity is unreliable, storage capacity is limited, and transportation systems are weak.71 These infrastructure constraints can disproportionately affect populations living far from health facilities and contribute to uneven vaccine availability.71,72
A second challenge is reliance on campaigns rather than strong routine immunization systems. Mass campaigns may improve short-term coverage, but they do not always provide consistent access for underserved populations between campaign periods.4 Service disruptions during emergencies, pandemics, or logistical breakdowns can further interrupt continuity and widen inequities in access. Vaccine hesitancy and rumors also remain a distinct challenge, as concerns about safety, mistrust of authorities, and misinformation can directly reduce uptake.4,40 In addition, missed vaccination schedules are common where follow-up systems are weak, caregiver awareness is limited, or households face continuing access barriers (Table 2).
 |
Table 2 Vaccination-Specific Barriers to Equitable Access in LMICs: Key Challenges and Proposed Solutions |
Screening-Specific Issues
Screening presents a different set of equity challenges because access does not end with the initial test. In many LMIC contexts, screening services require repeated visits for testing, confirmatory diagnosis, referral, treatment, and follow-up. This creates a heavier burden on patients, especially those facing transportation costs, lost wages, long waiting times, and competing household or work responsibilities.82 As a result, even where initial screening is available, many individuals may be unable to complete the full pathway of care.
Diagnostic follow-up gaps are another major challenge. Weak referral systems, poor care coordination, stock-outs of diagnostic supplies, delays in laboratory processing, and loss to follow-up after abnormal results can all prevent timely diagnosis and treatment.11 Screening is also particularly sensitive to stigma, especially when related to cancer, sexual health, or reproductive health. Fear of positive results, embarrassment, concerns about privacy, and mistrust of services may discourage participation. Late presentation and weak referral pathways further reduce the effectiveness of screening services, especially where awareness of early detection is low and higher-level services remain difficult to reach11,83 (as shown in Table 3).
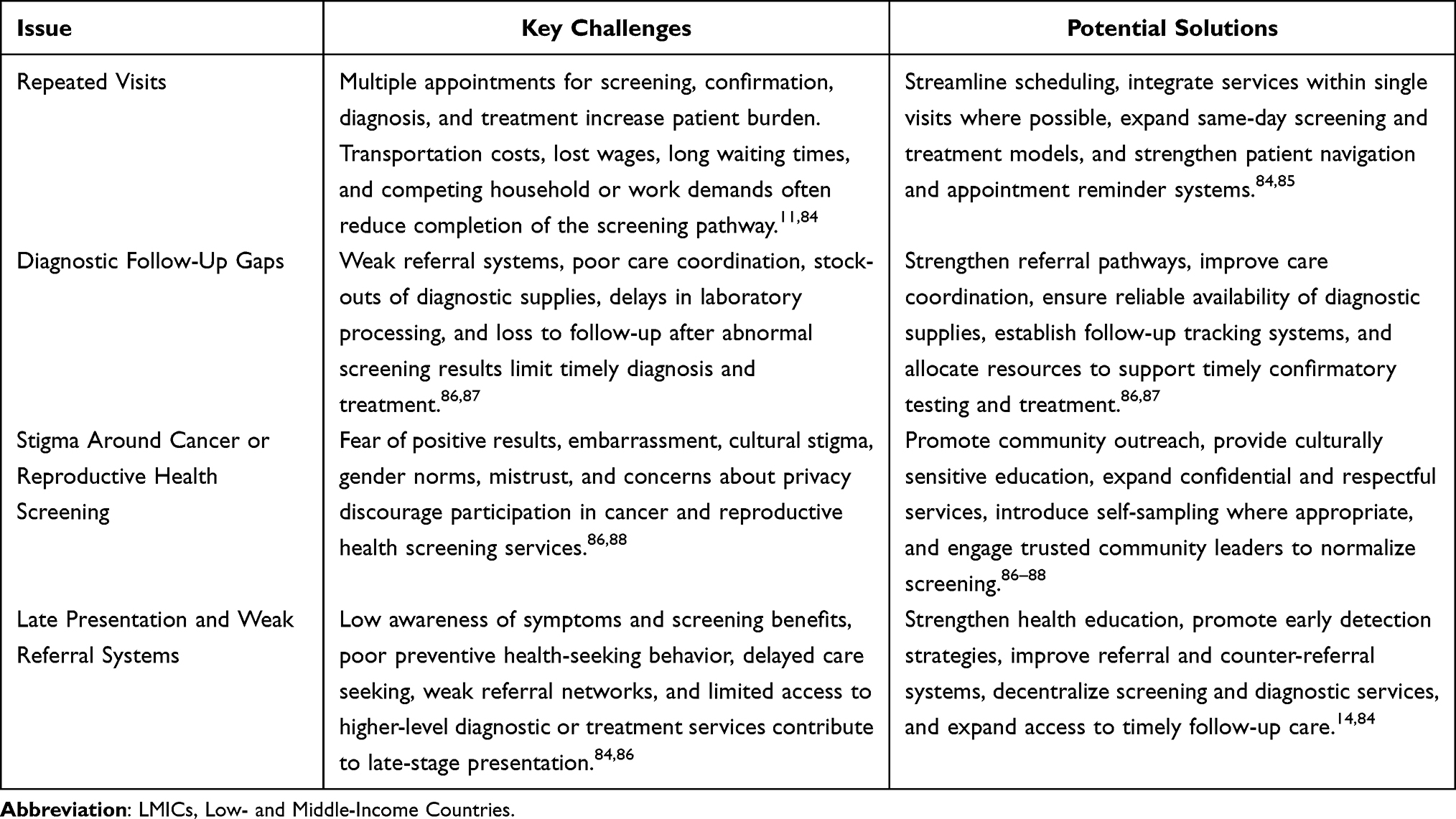 |
Table 3 Screening-Specific Barriers and Potential Solutions in LMICs |
Taken together, this comparison highlights both convergence and divergence in equity challenges across preventive services. Vaccination and screening services share many underlying barriers rooted in poverty, geography, exclusion, and weak health systems, but they differ in the operational demands they place on both patients and services. Recognizing these common and distinct challenges is important for designing responses that are both integrated and appropriately tailored to the specific requirements of each preventive intervention.
Strategies to Advance Equity in Preventive Care
Improving equitable access to vaccination and screening services in LMICs requires more than expanding the nominal availability of services. As this review has shown, barriers to preventive care are rooted in broader socioeconomic disadvantage, weak health systems, and structural inequities that limit whether underserved populations can benefit from available services. Advancing equity therefore requires coordinated action across multiple levels, including service delivery, financing, community engagement, governance, and workforce capacity.
Strengthening Primary Health Care
Strong primary health care systems are central to equitable preventive care because they provide the most accessible platform for routine vaccination and screening services.89 Integrating preventive services into primary care can reduce fragmentation and increase the likelihood that individuals encounter vaccination and screening services during regular contact with the health system, rather than only through stand-alone campaigns or episodic interventions.89–91 This is particularly important in LMICs, where reliance on vertical programs may create gaps in continuity of care.
Continuity and outreach within primary health care are equally important. Preventive care is most effective when services are delivered consistently and supported by reminders, referrals, and repeat visits where needed.92 Community health workers, local clinics, and satellite health posts can extend the reach of preventive services to rural and marginalized populations that might otherwise face long travel distances or irregular access to care.93 Decentralizing service delivery through community-based and lower-level facilities can reduce missed opportunities for prevention and make services more accessible to populations that are routinely underserved.92,93
Reducing Financial and Geographic Barriers
Financial hardship remains a major barrier to preventive care in LMICs. Even when vaccination or screening services are offered free of charge, patients may still face indirect costs such as transport expenses, lost wages, child care needs, or fees related to follow-up visits.94 Reducing out-of-pocket costs is therefore essential to improving equitable access. Policies that provide preventive services free at the point of care, particularly for low-income and high-risk populations, can reduce financial exclusion and encourage service use.94,95
Geographic barriers also require more flexible and locally responsive delivery models. Mobile clinics can extend preventive services to remote communities where fixed facilities are limited or difficult to reach.96 Transport vouchers and similar support mechanisms may help offset travel costs for patients who need to attend clinics for vaccination, rescreening, or diagnostic follow-up. School-based and community-based delivery models may also help reach children, adolescents, and other groups who do not regularly use formal health facilities. By reducing both financial and physical distance from services, these strategies can improve access for populations that are systematically underserved.96,97
Community Engagement and Culturally Responsive Communication
Equity in preventive care depends not only on service availability, but also on whether communities trust, understand, and accept those services. In many settings, misinformation, stigma, cultural norms, and mistrust of health systems can reduce uptake of both vaccination and screening services.98 Community engagement is therefore essential for strengthening demand and ensuring that interventions are locally acceptable.99
Partnerships with trusted local leaders, community health workers, religious figures, women’s groups, and other respected actors can improve the credibility of health messages and strengthen public confidence in services.40,99 Communication strategies should be tailored to local beliefs, concerns, and social contexts rather than relying on generic messaging alone. Engaging religious and community leaders is valuable, but it is most effective when paired with genuine efforts to understand the specific concerns that underlie religious or cultural objections, so that responses address the actual basis of hesitancy rather than assuming that endorsement by trusted leaders alone will change behaviour. Providing information in local languages and using culturally responsive education can improve understanding and reduce misinformation.98,99 These efforts are especially important in relation to vaccine hesitancy and to screening services affected by stigma, including cancer and reproductive health screening.
Equity-Focused Policy and Planning
Policy and planning processes play a decisive role in determining whether preventive services reach those who need them most. Equity-focused planning requires health systems to look beyond average national coverage levels and identify which populations remain excluded.2,40,100 Explicit attention to rural populations, low-income households, migrants, ethnic minorities, people with disabilities, and other marginalized groups can help ensure that preventive care programs reduce rather than reproduce disparities.2,100,101 These priorities are reflected in major equity-oriented programmatic initiatives, including pro-equity immunization strategies in Gavi-supported countries80 and global efforts to eliminate cervical cancer as a public health problem,82,85 which illustrate how active implementation actors are translating equity goals into practice and offer evaluable models for reaching underserved populations.
Disaggregated data are central to this effort. Monitoring uptake by income, gender, geography, education, ethnicity, disability status, or other markers of disadvantage can reveal inequities that remain hidden in aggregate coverage figures.2,9,100 These data can inform planning, resource allocation, and quality improvement. Equity-oriented planning also requires financing arrangements that prioritize underserved areas and reduce reliance on household spending. Without deliberate policy action, preventive care programs may continue to benefit those already better positioned to access services.66,100
Health Workforce and Service Delivery Improvement
The health workforce is a critical determinant of equitable preventive care delivery. Shortages of trained personnel, provider burnout, inconsistent service quality, and weak referral systems can all reduce the accessibility and effectiveness of vaccination and screening services.102 Strengthening provider training is therefore important not only for technical competence, but also for communication, counseling, and culturally sensitive care. Well-prepared providers are better equipped to address vaccine hesitancy, explain screening procedures, and support patients through follow-up processes.100,102
Task shifting can also improve equity by expanding service capacity in under-resourced settings. Community health workers, nurses, midwives, and other non-physician providers can contribute to health education, reminders, basic screening, and follow-up support when appropriately trained and supervised.102 Reminder systems, whether paper-based, phone-based, or community-led, can reduce missed appointments and incomplete care pathways. Better referral and follow-up mechanisms are especially important for screening, where continuity of care after an abnormal result is essential.103 Strengthening coordination across levels of care can therefore reduce loss to follow-up and improve outcomes for vulnerable populations.
Taken together, these strategies suggest that advancing equity in preventive care requires both shared and service-specific responses. Many priorities, including stronger primary health care, reduced financial and geographic barriers, community engagement, equity-focused planning, and workforce investment, are relevant across both vaccination and screening services. At the same time, some challenges require more tailored action, such as strengthening cold-chain and routine delivery systems for vaccination or improving referral, follow-up, and diagnostic continuity for screening.
Implications and Future Directions
This review shows that inequities in access to vaccination and screening services in low- and middle-income countries (LMICs) cannot be understood only in terms of whether preventive services are formally available.8–10 Across both interventions, access is shaped by overlapping socioeconomic, geographic, sociocultural, health system, and structural barriers that influence whether individuals are able to reach, use, and benefit from care.11,14–16,18,20,26,27,29,30,34–37,51–53,64,70,104 These patterns suggest that inequities in preventive care are rarely the result of a single obstacle. Rather, they emerge through the accumulation and interaction of disadvantage across multiple levels.4,8,10,56,60
A central implication of this review is that formal service availability should not be mistaken for meaningful access. Vaccination and screening services may be included in national programs and offered at low or no direct cost, yet still remain inaccessible in practice because of transport burdens, indirect expenses, weak follow-up systems, stigma, limited trust, poor service quality, or lack of continuity of care.11,18–21,26,27,29,86,88 This distinction is especially important in LMICs, where improvements in aggregate coverage may obscure persistent disparities affecting rural populations, low-income households, women and girls, migrants, ethnic minorities, people with disabilities, and other marginalized groups.56–61,95 An equity perspective therefore requires attention not only to overall service expansion, but also to who continues to be left behind and why.
The review also shows the value of examining vaccination and screening services together. These services share many underlying barriers, including poverty, geographic exclusion, weak primary care, limited health literacy, and social marginalization.23,27,29,30,63–65 At the same time, they differ in ways that matter for implementation. Vaccination is especially sensitive to supply continuity, cold-chain reliability, and public confidence, whereas screening depends more heavily on repeated contact, referral systems, diagnostic follow-up, and continuity of care after the initial test.11,72,73,75,77,78,86,103 Bringing these services into the same analytical frame helps identify where integrated strategies are appropriate and where more tailored responses are needed.
Another important insight is that inequities in preventive care reflect broader social determinants of health.8–10,22–24,56 Poverty, low educational attainment, gender inequality, poor infrastructure, insecure livelihoods, and social exclusion shape health-seeking behavior long before individuals arrive at a health facility.29,30,88 Expanding equitable access to vaccination and screening services therefore requires action beyond the health sector alone.89–93 Although health system reforms remain essential, their effects may be limited if wider structural disadvantages continue to constrain people’s ability to seek and sustain care.57,58,60,61 Preventive care strategies should therefore be linked to broader efforts to reduce social and geographic inequalities.
These findings have several implications for policy and practice. Most importantly, equity should be treated as a core objective of preventive care policy rather than as a secondary outcome of coverage expansion. Efforts to improve vaccination and screening services will be more effective when they are embedded within stronger primary health care systems, supported by equity-oriented planning, and informed by disaggregated data that make underserved populations more visible. In this context, reducing inequities will require coordinated demand-side and supply-side action, including financial protection, decentralized delivery, culturally responsive communication, workforce strengthening, and stronger continuity of care.
Future research should build on these findings by examining which equity-focused interventions are most effective across different LMIC contexts. More evidence is needed on integrated primary care models, mobile and community-based services, reminder systems, self-sampling approaches, and culturally tailored communication strategies, particularly among underserved populations.89–93 Future studies should also pay closer attention to intersectionality, recognizing that disadvantage is often layered across poverty, gender, rural residence, disability, migration status, and minority identity.56–58,60,61 In addition, stronger implementation research is needed to clarify how referral systems, supply chains, workforce models, and financing arrangements can be improved in real-world settings.100–103 Future work should move beyond measuring initial service uptake alone and place greater emphasis on continuity of care, including completion of vaccine schedules, attendance at repeat screening visits, timely diagnostic confirmation, and access to treatment after abnormal findings.
Limitations
This review has several limitations. First, the evidence spans diverse LMIC contexts with substantial variation in health systems, infrastructure, financing arrangements, and sociocultural conditions. This heterogeneity limits the extent to which the findings can be generalized across all settings. Second, although the review considers vaccination and screening services within a single preventive care framework to identify shared equity barriers, these services differ in delivery models, service organization, and follow-up requirements, and some intervention-specific nuances may not have been fully captured. In addition, the screening literature was not evenly distributed across screening programs and was concentrated mainly in cervical cancer/HPV-related screening, with more limited evidence from other preventive screening contexts. Findings related to screening should therefore be interpreted within that narrower scope. Third, the review was limited to English-language sources and selected databases, which may have resulted in the omission of relevant studies published in other languages or indexed elsewhere. Fourth, as a narrative rather than systematic review, study identification and selection were guided by the authors’ judgement rather than a predefined protocol, and the synthesis is interpretive in nature. This approach may have introduced selection bias, including possible over-representation of certain regions or disease areas, and the conclusions reflect the authors’ reading of a heterogeneous body of work. Relatedly, much of the underlying empirical literature operationalizes equity through differences in coverage or uptake rather than through deeper structural determinants, which may constrain the depth of equity-related inferences that can be drawn. Because of this heterogeneity and the conceptual focus of the review, no formal meta-analysis or quantitative inequality metrics (such as concentration indices) were attempted, and the analysis was limited to thematic synthesis of existing evidence. Despite these limitations, the review provides a useful synthesis of cross-cutting barriers and highlights priority areas for policy, practice, and future research.
Conclusion
Equitable access to vaccination and screening services remains a major challenge in LMICs. This review shows that barriers to preventive care are multidimensional and interconnected, shaped by socioeconomic disadvantage, geographic inaccessibility, sociocultural exclusion, health system weaknesses, and broader structural constraints. While vaccination and screening services share many common equity challenges, they also differ in the operational and follow-up demands they place on health systems and service users. Advancing equity in preventive care therefore requires coordinated, context-sensitive strategies that address both immediate barriers to access and the wider social and structural conditions that shape who benefits from prevention and who is left behind. Ultimately, addressing these equity barriers is essential for progress toward universal health coverage and the health-related Sustainable Development Goals, including SDG 3 targets on reducing preventable morbidity and mortality.
Acknowledgments
This publication charge is funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025). The authors also acknowledge PresentationGO (www.presentationgo.com) as the source of the template used in the design of Figure 1.
Funding
This study was funded by the grant Enhancing Quality Education for International University Impacts and Recognition – World Class University (EQUITY-WCU) for RKS, grant number 3969/UN6.3.1/PT.00/2025.
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this manuscript.
References
1. Argento VS. Health screening and disease prevention. In: Pignolo RJ, Crane MK, Forciea MA, editors. Classic Papers in Geriatric Medicine with Current Commentaries. Totowa, NJ: Humana Press; 2008:113–16.
2. Piot P, Caldwell A, Lamptey P, et al. Addressing the growing burden of non-communicable disease by leveraging lessons from infectious disease management. J Glob Health. 2016;6(1):010304. doi:10.7189/jogh.06.010304
3. Boccalini S. Value of vaccinations: a fundamental public health priority to be fully evaluated. Vaccines. 2025;13(5):479. doi:10.3390/vaccines13050479
4. Ali HA, Hartner AM, Echeverria-Londono S, et al. Vaccine equity in low and middle income countries: a systematic review and meta-analysis. Int J Equity Health. 2022;21(1):82. doi:10.1186/s12939-022-01678-5
5. Wang Q, Leung K, Jit M, Wu JT, Lin L. Global socioeconomic inequalities in vaccination coverage, supply, and confidence. NPJ Vaccines. 2025;10(1):91. doi:10.1038/s41541-025-01143-8
6. Wenang S, Schaefers J, Afdal A, et al. Availability and accessibility of primary care for the remote, rural, and poor population of Indonesia. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.721886
7. Senteio C, Fields SD, Pritam Singh RK, et al. Overcoming health misinformation in marginalized groups: a systematic review. Int J Equity Health. 2025;24(1):323. doi:10.1186/s12939-025-02657-2
8. Persaud N, Sabir A, Woods H, et al. Preventive care recommendations to promote health equity. Cmaj. 2023;195(37):E1250–e1273. doi:10.1503/cmaj.230237
9. Orach CG. Health equity: challenges in low income countries. Afr Health Sci. 2009;9(Suppl 2):S49–51.
10. Nelson HD, Cantor A, Wagner J, et al. Achieving health equity in preventive services: a systematic review for a national institutes of health pathways to prevention workshop. Ann Internal Med. 2020;172(4):258–271. doi:10.7326/M19-3199
11. Srinath A, van Merode F, Rao SV, Pavlova M. Barriers to cervical cancer and breast cancer screening uptake in low- and middle-income countries: a systematic review. Health Policy Plan. 2023;38(4):509–527. doi:10.1093/heapol/czac104
12. Palagyi A, Dodd R, Jan S, et al. Organisation of primary health care in the Asia-Pacific region: developing a prioritised research agenda. BMJ Global Health. 2019;4(Suppl 8):e001467. doi:10.1136/bmjgh-2019-001467
13. Levesque JF, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12:18. doi:10.1186/1475-9276-12-18
14. Chidyaonga-Maseko F, Chirwa ML, Muula AS. Underutilization of cervical cancer prevention services in low and middle income countries: a review of contributing factors. Pan Afr Med J. 2015;21:231. doi:10.11604/pamj.2015.21.231.6350
15. Otaigbe I. A narrative review of strategies to improve childhood vaccination coverage in low- and middle-income countries: improvement of childhood vaccination coverage. Babcock Univ Med J. 2023;6(2):202–214. doi:10.38029/babcockuniv.med.j.v6i2.323
16. Dhanasekaran K, Tamang H, Pradhan S, Lhamu R, Hariprasad R. Challenges in setting up a primary human papillomavirus-DNA testing facility in a lower and middle income country: lessons learned from a pilot programme. Ecancermedicalscience. 2022;16:1492. doi:10.3332/ecancer.2022.1492
17. Eide AH, Mannan H, Khogali M, et al. Perceived barriers for accessing health services among individuals with disability in four African Countries. PLoS One. 2015;10(5):e0125915. doi:10.1371/journal.pone.0125915
18. Musuka G, Cuadros DF, Miller FD, et al. Immunization coverage, equity, and access for children with disabilities: a scoping review of challenges, strategies, and lessons learned to reduce the number of zero-dose children. Vaccines. 2025;13(4):377. doi:10.3390/vaccines13040377
19. Omohwovo EJ, Omojuyigbe JO, Adegbenro TI, et al. Barriers to HPV vaccination and cervical cancer screening in developing countries. J Glob Health Sci. 2025;7(1). doi:10.35500/jghs.2025.7.e5
20. Waterworth CJ, Marella M, O’Donovan J, Bright T, Dowell R, Bhutta MF. Barriers to access to ear and hearing care services in low- and middle- income countries: a scoping review. Glob Public Health. 2022;17(12):3869–3893. doi:10.1080/17441692.2022.2053734
21. von Schoen-Angerer T, Love JP. Equitable access to medicines, vaccines, and medical devices. In: Raviglione MCB, Tediosi F, Villa S, Casamitjana N, Plasència A, editors. Global Health Essentials. Cham: Springer International Publishing; 2023:327–332.
22. Salman AA, Whyle E, de Oliveira LC, Olivier J. Access barriers to healthcare for undocumented migrants in low- and middle-income countries: a qualitative systematic review. J Immigr Minor Health. 2025;27(4):595–608. doi:10.1007/s10903-025-01693-y
23. de-Abreua AJL, Sato APS, Waldman EA. Equal access to vaccines: lessons learned and future perspectives. Saúde Soc São Paulo. 2023;32(3):e230486pt.
24. Asante AD, Price J, Hayen A, et al. Assessment of equity in healthcare financing in Fiji and Timor-Leste: a study protocol. BMJ Open. 2014;4(12):e006806. doi:10.1136/bmjopen-2014-006806
25. Tagoe ET, Sheikh N, Morton A, et al. COVID-19 vaccination in lower-middle income countries: national stakeholder views on challenges, barriers, and potential solutions. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.709127
26. Russell S. The economic burden of illness for households in developing countries: a review of studies focusing on malaria, tuberculosis, and human immunodeficiency virus/acquired immunodeficiency syndrome. In: Breman JG, Alilio MS, Mills A, editors. The Intolerable Burden of Malaria II: What’s New, What’s Needed. Northbrook (IL): American Society of Tropical Medicine and Hygiene; 2004. Supplement to Volume 71(2) of the American Journal of Tropical Medicine and Hygiene.
27. Li C, Thapa D, Mi Q, Gao Y, Fu X. Disparities in hepatitis B virus healthcare service access among marginalised poor populations: a mixed-method systematic review. Infect Dis Poverty. 2024;13(1):58. doi:10.1186/s40249-024-01225-0
28. Coley RL, McCoy DC, Hatch SF. How poverty shapes children’s home, neighborhood, and school environments: an integrative conceptual framework and review. Am Psychol. 2025. doi:10.1037/amp0001573
29. Karasiewicz M, Chawłowska E, Lipiak A, Więckowska B. A step towards understanding and tackling health inequalities: the use of secondary prevention services and the need for health promotion in a rural setting. Int J Environ Res Public Health. 2021;18(16):8492. doi:10.3390/ijerph18168492
30. Lorini C, Santomauro F, Donzellini M, et al. Health literacy and vaccination: a systematic review. Hum Vaccin Immunother. 2018;14(2):478–488. doi:10.1080/21645515.2017.1392423
31. Iqbal MU, Javed MR, Hajj F. Bridging the digital health divide: telemedicine accessibility in low- and middle-income countries during post-pandemic recessions. Ann Med Surg. 2026;88(1):993–994. doi:10.1097/MS9.0000000000004350
32. Yao R, Zhang W, Evans R, Cao G, Rui T, Shen L. Inequities in health care services caused by the adoption of digital health technologies: scoping review. J Med Internet Res. 2022;24(3):e34144. doi:10.2196/34144
33. Macharia J, Wambua R, Oduor C. Digital health for equitable access to universal health coverage: lessons from Makueni county in Kenya. In: Esen Koç H, Öztürk N, Huttunen-Lenz M, editors. Patient Experience and Satisfaction - Evolving Landscape of Healthcare. London: IntechOpen; 2025.
34. Evans MV, Andréambeloson T, Randriamihaja M, et al. Geographic barriers to care persist at the community healthcare level: evidence from rural Madagascar. PLOS Glob Public Health. 2022;2(12):e0001028. doi:10.1371/journal.pgph.0001028
35. Awoh AB, Plugge E. Immunisation coverage in rural–urban migrant children in low and middle-income countries (LMICs): a systematic review and meta-analysis. J Epidemiol Community Health. 2016;70(3):305. doi:10.1136/jech-2015-205652
36. Mupunga I, Dimech W, Izumi K, et al. A qualitative evaluation of access to essential laboratory services for communicable diseases at the primary health care level in the Western Pacific Region. Trop Med Health. 2025;53(1):156. doi:10.1186/s41182-025-00797-3
37. Terefe B, Workneh BS, Zeleke GA, et al. Uncovering women’s healthcare access challenges in low- and middle-income countries using mixed effects modelling approach: insights for achieving the sustainable development goals. PLoS One. 2025;20(1):e0314309. doi:10.1371/journal.pone.0314309
38. Azad AD, Charles AG, Ding Q, Trickey AW, Wren SM. The gender gap and healthcare: associations between gender roles and factors affecting healthcare access in Central Malawi, June-August 2017. Arch Public Health. 2020;78(1):119. doi:10.1186/s13690-020-00497-w
39. Plesons M, Bastien S, Dyalchand A, Mehta R, Speizer IS, Chandra-Mouli V. Updated world health organization guideline on preventing early pregnancy and poor reproductive outcomes among adolescents in low- and middle-income countries. J Adolesc Health. 2025;77(5):803–809. doi:10.1016/j.jadohealth.2025.07.024
40. Sinuraya RK, Nuwarda RF, Postma MJ, Suwantika AA. Vaccine hesitancy and equity: lessons learned from the past and how they affect the COVID-19 countermeasure in Indonesia. Global Health. 2024;20(1):11. doi:10.1186/s12992-023-00987-w
41. Melillo S, Strachan R, O’Brien CJ, Wonodi C, Bormet M, Fountain D. Effects of local faith-actor engagement in the uptake and coverage of immunization in low- and middle-income countries: a literature review. Christian J Glob Health. 2022;9(1):2–32. doi:10.15566/cjgh.v9i1.587
42. Hindi Albalawi HM, Rezq KA. Influences of Cultural Factors on Vaccination Practices Among Parents Prior to School Age: a Systematic Review and Meta-Analysis. Cureus. 2024;16(12):e75845. doi:10.7759/cureus.75845
43. Swartz L, Kilian S, Twesigye J, Attah D, Chiliza B. Language, culture, and task shifting--an emerging challenge for global mental health. Glob Health Action. 2014;7:23433. doi:10.3402/gha.v7.23433
44. Taylor A, Kazembe P. Assessing language barriers in health facilities in Malawi. BMC Health Serv Res. 2024;24(1):1393. doi:10.1186/s12913-024-11901-4
45. Tiwary A, Rimal A, Paudyal B, Sigdel KR, Basnyat B. Poor communication by health care professionals may lead to life-threatening complications: examples from two case reports. Wellcome Open Res. 2019;4:7. doi:10.12688/wellcomeopenres.15042.1
46. Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. Lancet. 2017;389(10077):1453–1463. doi:10.1016/S0140-6736(17)30569-X
47. Hamed S, Bradby H, Ahlberg BM, Thapar-Björkert S. Racism in healthcare: a scoping review. BMC Public Health. 2022;22(1):988. doi:10.1186/s12889-022-13122-y
48. Selvarajah S, Corona Maioli S, Deivanayagam TA, et al. Racism, xenophobia, and discrimination: mapping pathways to health outcomes. Lancet. 2022;400(10368):2109–2124. doi:10.1016/S0140-6736(22)02484-9
49. Agyeman-Manu K, Ghebreyesus TA, Maait M, et al. Prioritising the health and care workforce shortage: protect, invest, together. Lancet Glob Health. 2023;11(8):e1162–e1164. doi:10.1016/S2214-109X(23)00224-3
50. Asante A, Price J, Hayen A, Jan S, Wiseman V. Equity in health care financing in low- and middle-income countries: a systematic review of evidence from studies using benefit and financing incidence analyses. PLoS One. 2016;11(4):e0152866. doi:10.1371/journal.pone.0152866
51. Chu KM, Weiser TG. Real-world implementation challenges in low-resource settings. Lancet Glob Health. 2021;9(10):e1341–e1342. doi:10.1016/S2214-109X(21)00310-7
52. Khatri R, Endalamaw A, Erku D, et al. Continuity and care coordination of primary health care: a scoping review. BMC Health Serv Res. 2023;23(1):750. doi:10.1186/s12913-023-09718-8
53. Ricciardi GE, Cuciniello R, Raimondi V, Vaia F, Signorelli C, Renzi C. Preventive healthcare and disability: challenges and opportunities. Healthcare. 2025;13(17):2099. doi:10.3390/healthcare13172099
54. Yazdi-Feyzabadi V, Sabermahani M, Borhaninejad V, Iranmanesh M. Breaking barriers: challenges faced by the older adults in accessing primary healthcare in a developing country. BMC Geriatr. 2025;25(1):946. doi:10.1186/s12877-025-06712-z
55. Langlois EV, McKenzie A, Schneider H, Mecaskey JW. Measures to strengthen primary health-care systems in low- and middle-income countries. Bull World Health Organ. 2020;98(11):781–791. doi:10.2471/BLT.20.252742
56. Zezai D, van Rensburg AJ, Babatunde GB, et al. Barriers and facilitators for strengthening primary health systems for person-centred multimorbid care in low-income and middle-income countries: a scoping review. BMJ Open. 2024;14(11):e087451. doi:10.1136/bmjopen-2024-087451
57. Jahangir S, Bailey A, Hasan MMU, Hossain S. Inequalities in accessing public transportation and social exclusion among older adults and people with disabilities in Bangladesh: a scoping review. Transp Res Interdiscip Perspect. 2024;26:101138. doi:10.1016/j.trip.2024.101138
58. Domapielle MK, Dassah C, Dordaa F, Cheabu BSN, Sulemana M. Barriers to health care access and utilization among aged indigents under the Livelihood Empowerment Against Poverty Programme (LEAP): the perspective of users and service providers in north-western Ghana. Prim Health Care Res Dev. 2023;24:e48. doi:10.1017/S1463423623000385
59. Zeng Y, Kang X, Yang Y, Hwang E. Barriers and facilitators of preventive healthcare access among immigrants in rural America: a scoping review. Int J Equity Health. 2025;24(1):241. doi:10.1186/s12939-025-02603-2
60. Iezadi S, Kolivand P, Namdar P, Saberian P, Gholipour K, Azari S. Racial and ethnic disparities in COVID-19 vaccination: a systematic review and meta-analysis. Arch Public Health. 2025;83(1):261. doi:10.1186/s13690-025-01740-y
61. Vohra-Gupta S, Petruzzi L, Jones C, Cubbin C. An intersectional approach to understanding barriers to healthcare for women. J Community Health. 2023;48(1):89–98. doi:10.1007/s10900-022-01147-8
62. Tan SHS, Wang D, Tan WJ, Allameen NA, Fong NP. Facilitators and barriers of hepatitis B screening and vaccination. Vaccine. 2020;38(34):5447–5453. doi:10.1016/j.vaccine.2020.06.045
63. McKeirnan KC, Undeberg MR, Zelenko S, Meratnia G. A qualitative analysis of rural community vaccination barriers during the COVID-19 pandemic. Vaccines. 2024;12(12):1442. doi:10.3390/vaccines12121442
64. Muñoz Bohorquez J, Channell Doig A, Goldring S, et al. Access barriers, trusted channels, and misconceptions about the COVID-19 vaccine among rural immigrant farmworkers. Hisp Health Care Int. 2025;23(1):26–34. doi:10.1177/15404153241262050
65. Spees LP, Biddell CB, Angove RSM, et al. Barriers to COVID-19 vaccine uptake among resource-limited adults diagnosed with chronic illness. Front Public Health. 2023;11:1046515. doi:10.3389/fpubh.2023.1046515
66. Alegre JC, Sharma S, Cleghorn F, Avila C. Strengthening primary health care in low- and middle-income countries: furthering structural changes in the post-pandemic era. Front Public Health. 2023;11:1270510. doi:10.3389/fpubh.2023.1270510
67. Noya F, Carr S, Freeman K, Thompson S, Clifford R, Playford D. Strategies to facilitate improved recruitment, development, and retention of the rural and remote medical workforce: a scoping review. Int J Health Policy Manag. 2022;11(10):2022–2037. doi:10.34172/ijhpm.2021.160
68. Miseda MH, Were SO, Murianki CA, Mutuku MP, Mutwiwa SN. The implication of the shortage of health workforce specialist on universal health coverage in Kenya. Hum Resour Health. 2017;15(1):80. doi:10.1186/s12960-017-0253-9
69. Baumgartner L, Wright O, Barne K, et al. What factors affect the recruitment and retention of allied health professionals working in hospitals? A systematic literature review. Aust Health Rev. 2024;49:AH24287.
70. Essa-Hadad J, Gorelik Y, Vervoort J, Jansen D, Edelstein M. Understanding the health system barriers and enablers to childhood MMR and HPV vaccination among disadvantaged, minority or underserved populations in middle- and high-income countries: a systematic review. European Journal of Public Health. 2024;34(2):368–374. doi:10.1093/eurpub/ckad232
71. Kitui SK, Juma E, Ndalama MT, et al. Trends in uptake and impact of thermostable vaccines in Africa. Ther Adv Vaccines Immunother. 2025;13:25151355251341662. doi:10.1177/25151355251341662
72. Cattin M, Jonnalagedda S, Makohliso S, Schönenberger K. The status of refrigeration solutions for last mile vaccine delivery in low-income settings. Vaccine X. 2022;11:100184. doi:10.1016/j.jvacx.2022.100184
73. Kapuria B, Sami Hamadeh R, Mazloum F, et al. Achieving sustainable, environmentally viable, solarized vaccine cold chain system and vaccination program-an effort to move towards clean and green energy-driven primary healthcare in Lebanon. Front Health Serv. 2024;4:1386432. doi:10.3389/frhs.2024.1386432
74. Yang X, Zhang L, Staykov K, Wu Z, Jaklenec A. Transforming drug and vaccine delivery for equitable access in global health. Biochem Biophys Res Commun. 2025;779:152415. doi:10.1016/j.bbrc.2025.152415
75. Bulkhi AA, Almoallim HM, Obaid MS, et al. Immunization coverage and barriers among hajj and Umrah pilgrims: insights into vaccine uptake and compliance. J Epidemiol Glob Health. 2025;15(1):104. doi:10.1007/s44197-025-00447-1
76. Kapuria B, Hamadeh RS, Mazloum F, et al. Immunization as an entry point for primary health care and beyond healthcare interventions—process and insights from an integrated approach in Lebanon. Front Health Serv. 2023;3. doi:10.3389/frhs.2023.1251775
77. Edwards KM, Hackell JM; Committee on Infectious Diseases, The Committee on Practice and Ambulatory Medicine. Countering Vaccine Hesitancy. Pediatrics. 2016;138(3). doi:10.1542/peds.2016-2146
78. Nasr R, Swaidan E, Hachem S, et al. Immunization safety monitoring: addressing vaccine hesitancy and enhancing coverage in crisis-affected regions-insights from Lebanon, Ukraine, and Sudan. Ther Adv Vaccines Immunother. 2025;13:25151355251380220. doi:10.1177/25151355251380220
79. Brumbaugh KQ, Gellert F, Mokdad AH. Understanding vaccine hesitancy: insights and improvement strategies drawn from a multi-study review. Vaccines. 2025;13(10):1003. doi:10.3390/vaccines13101003
80. Dadari I, Higgins-Steele A, Sharkey A, et al. Pro-equity immunization and health systems strengthening strategies in select Gavi-supported countries. Vaccine. 2021;39(17):2434–2444. doi:10.1016/j.vaccine.2021.03.044
81. Xie SJ, Mah NR, Chew L, et al. Improving vaccine equity: how community engagement and informatics facilitate health system outreach to underrepresented groups. Appl Clin Inform. 2024;15(1):129–144. doi:10.1055/s-0044-1779258
82. Gravitt PE, Silver MI, Hussey HM, et al. Achieving equity in cervical cancer screening in low- and middle-income countries (LMICs): strengthening health systems using a systems thinking approach. Prev Med. 2021;144:106322. doi:10.1016/j.ypmed.2020.106322
83. Chapola J, Lee F, Bula A, et al. Barriers to follow-up after an abnormal cervical cancer screening result and the role of male partners: a qualitative study. BMJ Open. 2021;11(9):e049901. doi:10.1136/bmjopen-2021-049901
84. Petersen Z, Jaca A, Ginindza TG, et al. Barriers to uptake of cervical cancer screening services in low-and-middle-income countries: a systematic review. BMC Womens Health. 2022;22(1):486. doi:10.1186/s12905-022-02043-y
85. Gopalkrishnan K, Karim R. Addressing global disparities in cervical cancer burden: a narrative review of emerging strategies. Curr HIV/AIDS Rep. 2025;22(1):18. doi:10.1007/s11904-025-00727-2
86. Felisi NM, Oyet D, Yung KMM, Ochola E, Vecchio R, Odone A. Barriers and facilitators to cervical cancer screening in Northern Uganda: qualitative insights from healthcare workers and administrators. Curr Oncol. 2025;32(11):591. doi:10.3390/curroncol32110591
87. Bretsch JK, Wallace AS, McCoy R. Social needs screening in academic health systems: a landscape assessment. Popul Health Manag. 2024;27(5):312–319. doi:10.1089/pop.2024.0111
88. Aldakhil M, Ibrahim Albarrak R, Alharbi RK, et al. Barriers to colorectal cancer screening tests among adults in the Saudi population: a systematic review and meta-analysis. J Taibah Univ Med Sci. 2025;20(5):654–662. doi:10.1016/j.jtumed.2025.09.001
89. Dudley L, Garner P. Strategies for integrating primary health services in low- and middle-income countries at the point of delivery. Cochrane Database Syst Rev. 2011;2011(7):Cd003318. doi:10.1002/14651858.CD003318.pub3
90. van Weel C, Kidd MR. Why strengthening primary health care is essential to achieving universal health coverage. Cmaj. 2018;190(15):E463–e466. doi:10.1503/cmaj.170784
91. Druetz T. Integrated primary health care in low- and middle-income countries: a double challenge. BMC Med Ethics. 2018;19(Suppl 1):48. doi:10.1186/s12910-018-0288-z
92. Sharma N, Harris E, Lloyd J, Mistry SK, Harris M. Community health workers involvement in preventative care in primary healthcare: a systematic scoping review. BMJ Open. 2019;9(12):e031666. doi:10.1136/bmjopen-2019-031666
93. Austin S, Qu H. Community health workers bridging the gap: connecting medicaid members with providers, managed care, and community-based organizations. Risk Manag Healthc Policy. 2024;17:2949–2958. doi:10.2147/RMHP.S482855
94. Farih OA, Mohamed SH, Abdillahi AM, et al. Financial barriers and inequalities in healthcare access across East Africa: evidence from demographic and health surveys. Front Reprod Health. 2025;7:1730560. doi:10.3389/frph.2025.1730560
95. Bolongaita S, Lee Y, Johansson KA, et al. Financial hardship associated with catastrophic out-of-pocket spending tied to primary care services in low- and lower-middle-income countries: findings from a modeling study. BMC Med. 2023;21(1):356. doi:10.1186/s12916-023-02957-w
96. Rabiou LM, Oumarou B, Mor D, et al. Mobile outreach clinics for improving health care services accessibility in vulnerable populations of the Diffa Region in Niger: a descriptive study. Int J Equity Health. 2024;23(1):235. doi:10.1186/s12939-024-02322-0
97. Arenson M, Hudson PJ, Lee N, Lai B. The evidence on school-based health centers: a review. Glob Pediatr Health. 2019;6:2333794x19828745. doi:10.1177/2333794X19828745
98. Prall SP. Quantifiable cross-cultural research on medical mistrust is necessary for effective and equitable vaccination in low- and middle-income countries. J Epidemiol Glob Health. 2024;14(4):1771–1777. doi:10.1007/s44197-024-00319-0
99. Abdullah M, Ahmad T, Kazmi T, et al. Community engagement to increase vaccine uptake: quasi-experimental evidence from Islamabad and Rawalpindi, Pakistan. PLoS One. 2022;17(12):e0274718. doi:10.1371/journal.pone.0274718
100. Phelan H, Yates V, Lillie E. Challenges in healthcare delivery in low- and middle-income countries. Anaesth Intensive Care Med. 2022;23(8):501–504. doi:10.1016/j.mpaic.2022.05.004
101. Serafica R, Reyes AT, Cacciata MC, et al. Bridging the gap: reducing health inequities in access to preventive health care services in rural communities in the Philippines. J Transcult Nurs. 2025;36(1):24–33. doi:10.1177/10436596241271270
102. Tesema AG, Mabunda SA, Chaudhri K, et al. Task-sharing for non-communicable disease prevention and control in low- and middle-income countries in the context of health worker shortages: a systematic review. PLOS Global Public Health. 2025;5(4):e0004289. doi:10.1371/journal.pgph.0004289
103. Brancewicz M, Robakowska M, Śliwiński M, Rystwej D. SMS and telephone communication as tools to reduce missed medical appointments. Appl Sci. 2025;15(17):9773. doi:10.3390/app15179773
104. Chang AY, Riumallo-Herl C, Perales NA, et al. The equity impact vaccines may have on averting deaths and medical impoverishment in developing countries. Health Aff. 2018;37(2):316–324. doi:10.1377/hlthaff.2017.0861
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.