Back to Journals » Clinical Ophthalmology » Volume 17
Heads-Up Three-Dimensional Viewing Systems in Vitreoretinal Surgery: An Updated Perspective
Authors Razavi P ![]() , Cakir B, Baldwin G, D’Amico DJ
, Cakir B, Baldwin G, D’Amico DJ ![]() , Miller JB
, Miller JB ![]()
Received 3 June 2023
Accepted for publication 14 August 2023
Published 28 August 2023 Volume 2023:17 Pages 2539—2552
DOI https://doi.org/10.2147/OPTH.S424229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Peyman Razavi,1 Bertan Cakir,2 Grace Baldwin,2 Donald J D’Amico,1 John B Miller2
1Department of Ophthalmology, Weill Cornell Medical College, New York-Presbyterian Hospital, New York, NY, USA; 2Harvard Retinal Imaging Lab, Boston, MA, USA
Correspondence: John B Miller, Harvard Retinal Imaging Lab, 243 Charles St, Boston, MA, 02114, USA, Tel +1 617 573-3750, Fax +1 617 573-3698, Email [email protected]
Abstract: Three-Dimensional (3D) heads-up visualization systems have significantly advanced vitreoretinal surgery, providing enhanced detail and improved ergonomics. This review discusses the application of 3D systems in vitreoretinal surgery, their use in various procedures, their combination with other imaging modalities, and the role of this technology in medical education and telementoring. Furthermore, the review highlights the benefits of 3D systems, such as improved ergonomics, reduced phototoxicity, enhanced depth of field, and the use of color filters. Potential challenges, including the learning curve and additional costs, are also addressed. The review concludes by exploring promising future applications, including teleophthalmology for remote assistance and specialist availability expansion, virtual reality integration for global clinical education, and the combination of remotely robotic-guided surgery with artificial intelligence for precise, efficient surgical procedures. This comprehensive review offers insights into the current state and future potential of 3D heads-up visualization systems in vitreoretinal surgery, underscoring the transformative impact of this technology on ophthalmology.
Keywords: three-dimensional viewing system, 3D visualization, heads-up display, vitreoretinal surgery, three-dimensional surgery
Introduction
Three-dimensional (3D) heads-up viewing systems have enabled a major visualization advancement in vitreoretinal surgery. Developed initially to provide surgeons with an improved view of the surgical field, these systems consist of two separate optical channels which produce two slightly different images and are combined to create a 3D picture. TrueVision (Santa Barbara, CA) initially developed a digital camera that could attach to the standard analog operating microscope and enable displaying the images on a screen.1 After the initial success, TrueVision and Alcon collaborated to produce a system for digitally assisted ophthalmic procedures, the NGENUITY® 3D visualization platform, which was released in 2016.2 To obtain a stereoscopic view of the screen, the surgeons wear passive 3D polarized glasses. Additionally, the Artevo 800 3D Heads-up Display System (Carl Zeiss Meditec, USA) was introduced more recently and delivers real-time, high-resolution stereoscopic images of the operating area in true-to-life colors on an advanced display screen.3,4 Other systems, such as Sony’s HMS-3000 MT (Sony Electronics Inc., Tokyo, Japan), have attempted to bring the monitor closer to the operator and embed the video into a head-mounted unit.1 With the continued evolution of this technology, the use of 3D surgical viewing systems is likely to become even more widespread in vitreoretinal surgery.
Use and Outcomes in Vitreoretinal Surgery
Pars Plana Vitrectomy
Three-dimensional heads-up systems have found extensive use in vitreoretinal surgery. Surgeons have expressed positive experiences with this technology, citing ease of use, superior comfort, visibility, picture clarity, maneuverability, and improved depth perception compared to traditional microscopy.5 A retrospective review of 272 vitreoretinal surgeries, including treatments for a wide variety of vitreoretinal pathologies, found no complications attributed to the use of the 3D heads-up system.6 Moreover, no cases required conversion to an operating microscope.6 International studies likewise reported favorable outcomes. A retrospective, descriptive, comparative study in France found no differences in visual and anatomical results when employing the 3D heads-up systems compared to the conventional microscopy.7 Specifically, postoperative rates of retinal detachment (RD) recurrence, macular hole closure rates, epiretinal membranes (ERM) surgical times, and visual prognoses were comparable.7 Another retrospective study conducted in China reported no appreciable difference in the incidence of complications between 3D and conventional microscopic vitrectomy procedures for treating a wide range of vitreoretinal disorders.8 Similarly, visual and anatomical outcomes were comparable between the two modalities.8 Table 1 summarizes a list of studies comparing the use of 3D heads-up display (HUD) systems with the conventional microscope in treating vitreoretinal diseases. Across various studies, three-dimensional heads-up displays and standard operating microscopes consistently demonstrate comparable effectiveness in surgical outcomes.
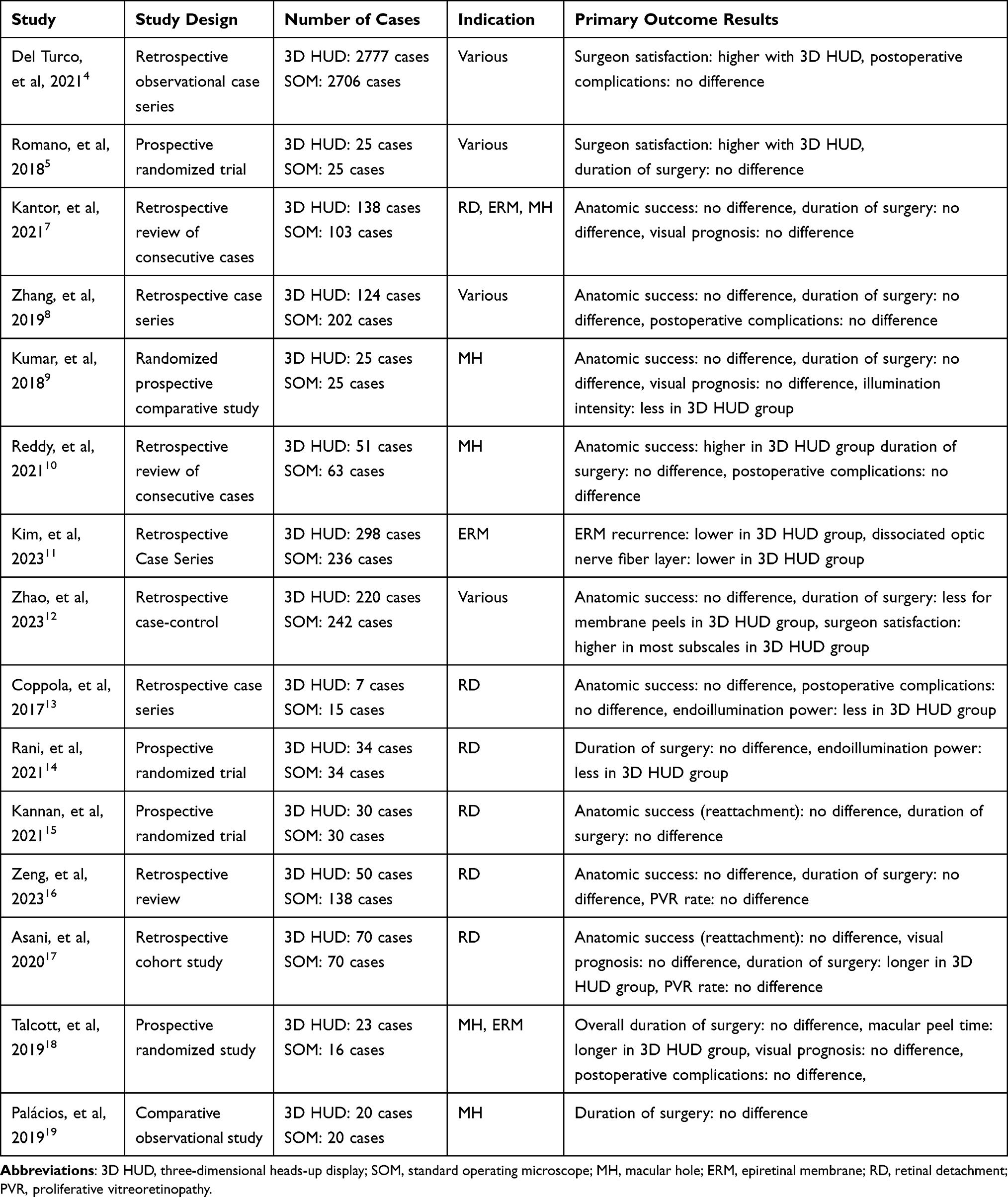 |
Table 1 Studies Comparing Outcomes with Three-Dimensional Heads-Up Display and Standard Operating Microscope |
In terms of its effectiveness in vitrectomy, a laboratory study compared vitreous removal using the NGENUITY® 3D heads-up viewing system to a standard surgical microscope.20 It was found that the application of the 3D heads-up viewing system resulted in significantly less residual vitreous in porcine eyes.20 The authors posited that the 3D heads-up viewing system enhances the vitreous gel removal process by improving the visualization of the peripheral vitreous via the blue color channel.20
Another area where 3D visualization technology can make a significant impact is endoscope-assisted vitrectomies. In the conventional setup, surgeons must switch between a microscope and a small monitor for the endoscopy, which is cumbersome and time-consuming. In contrast, 3D technology facilitates the simultaneous display of two viewpoints on a single large screen, streamlining the process.21
Peripheral Vitrectomy and Scleral Depression
Peripheral vitreous removal with scleral depression is commonly performed with the help of a skilled assistant who provides scleral indentation for vitreous base shaving, while the primary surgeon uses a widefield viewing system. A case series introduced a novel technique for visualizing the retina and vitreous during vitrectomy, employing a transscleral illuminated light pipe and a digital camera with heads-up display technology.22 This technique allows a single surgeon to perform peripheral vitrectomy and scleral depression without needing a skilled assistant. In this method, the light pipe is adjusted to 100% power on the vitrectomy machine and is placed externally on the sclera just posterior to the vitreous base insertion. It is used to gently indent the sclera to perform a peripheral vitrectomy. The digital camera and heads-up display system are used to improve visualization of the vitreous cavity, with the light amplification settings increased to near-maximal gain to enhance the view of areas with low luminance.22 Using the digital camera and heads-up display system in this technique has several advantages over a traditional operating microscope. The high-definition camera with a high dynamic range improves the display quality by combining multiple images with different exposures. This provides a better view compared to the traditional microscope. Additionally, the system’s digital image processing can significantly amplify endogenous luminance, improving visualization of areas of the vitreous cavity with low luminance.
Internal Limiting Membrane and Epiretinal Membrane Peeling
Macular holes are characterized by a defect in the center of the fovea, resulting in significant vision impairment and patient morbidity. The surgical method to treat macular holes generally involves a pars plana vitrectomy, induction of a posterior vitreous detachment, internal limiting membrane (ILM) peel, and fluid gas exchange. This is typically followed by one week of post-operative face-down positioning, resulting in a high macular closure rate.23 The ILM peeling stage, in particular, requires exceptional stereopsis and hand-eye coordination, given its delicacy. A randomized prospective comparative study evaluated the clinical outcomes of patients undergoing macular surgery with a 3D heads-up viewing system and conventional microscopic surgery performed by a single surgeon.9 The study reported comparable results concerning surgical time and macular hole closure rates.13 Further, a retrospective study conducted with vitreoretinal surgical fellows in India found that the use of the 3D heads-up display system yielded significantly greater closure rates than traditional microscopy (86.3% vs 60.3%).10 This highlights the potential role the system could have in surgical training.
The application of 3D heads-up visualization systems has also been investigated in other instances of ILM peels. A retrospective case series, consisting of 14 consecutive patients who underwent ILM peeling for proliferative vitreoretinopathy, found that most eyes had anatomic success with just one procedure, and all eyes attained success.24 This observation suggests that the 3D visualization system can be effectively used in the treatment of proliferative vitreoretinopathy.
Another vitreoretinal surgery wherein the utilization of 3D heads-up visualization systems has demonstrated significant benefits over standard microscopy is epiretinal membrane (ERM) peeling, a procedure demanding a degree of dexterity and stereopsis similar to ILM peeling and can be performed with or without ILM peeling. In a retrospective evaluation of 534 consecutive ERM peeling procedures performed in South Korea, the use of this system was associated with a substantially lower incidence of ERM recurrence and dissociated optic nerve fiber layer rates than the standard microscopy.11 In this study, logistic regression analysis identified the use of conventional microscopy as the sole significant risk factor for ERM recurrence (adjusted odds ratio: 12.86, p=0.02).11 The authors suggested that leveraging digital image processing in a 3D heads-up system can enhance visualization and magnification without sacrificing resolution. This enhanced surgical view may facilitate a less traumatic and more complete ERM removal, possibly resulting in a lower rate of ERM recurrence and dissociated optic nerve fiber layer. Additionally, the visual acuity and central macular thickness improvement achieved with the 3D heads-up system in this study was comparable to that attained with standard microscopy.11
Three-dimensional heads-up systems also support a faster peeling time for surgeons. In a retrospective case-control study involving 462 eyes, the procedures done with the 3D display resulted in a significantly shorter ERM or ILM peeling period for eyes affected by ERM and idiopathic MH compared to those performed with conventional microscopy.12 The same study did not find a shorter procedure time in other vitreoretinal procedures, such as complete vitrectomy or retinal detachment repair. Overall, from the surgeon’s perspective, the 3D system received significantly higher ratings in several areas, such as comfort level, resolution, depth of field, and magnification.12
Retinal Detachment Repair
Rhegmatogenous retinal detachment (RRD) is a serious medical condition that can lead to permanent vision loss if not promptly addressed. The application of the 3D heads-up visualization system in RRD repair via pars plana vitrectomy (PPV) can deliver satisfactory anatomical and functional results, parallel to those attained with traditional microscopy.13,14 A prospective interventional study of 60 eyes undergoing RRD repair found that the use of a 3D heads-up display and the standard microscope led to similar rates of final retinal attachment and significant improvement in visual acuity.15 The duration of surgery was also similar for both methods.15 Moreover, a retrospective review of 188 eyes undergoing RRD repair, comparing the use of the NGENUITY® 3D heads-up display and traditional microscope, found no significant difference between the two groups regarding anatomic success rates, postoperative complications, or surgical duration.16 The authors of these studies detailed that 3D head-up visualization systems provided improved ergonomics, increased depth of field, and a greater field of view. Similarly, a retrospective cohort study of 140 surgeries, comparing 3D heads-up to the standard microscope, found that both groups had similar outcomes regarding the primary retinal reattachment rate, the incidence of postoperative proliferative vitreoretinopathy, and the final best-corrected visual acuity (BCVA).17 However, the duration of surgery was longer in the 3D HUD group, an outcome ascribed to the learning curve.17
During the RRD repair, perfluorocarbon liquid (PFCL) is often utilized to facilitate the drainage of subretinal fluid (SRF). However, the retention of PFCL inside the eye can cause unintended toxicity to the retina and lead to various postoperative complications. To address this issue, a consecutive series of RRD surgical patients assessed whether PFCL could be excluded from PPV surgery with the aid of the NGENUITY® 3D Visualization System.25 The study comprised 60 cases, with half utilizing PFCL and the other half not. The findings revealed that by excluding PFCL, the operation time was significantly reduced, and visual acuity outcomes were slightly better while achieving a 100% retinal reattachment rate.25 Consequently, the 3D visualization system can be used to perform PPV surgery without PFCL, resulting in a simpler operation and avoiding PFCL-related complications. When performing PPV surgery for RRD without PFCL, one of the main challenges is poor visualization under a microscope in air-filled eyes. However, the authors argue that this challenge can be overcome by using a 3D visualization system, which provides better intraoperative visualization, a wider field of view, and improved resolution by using real-time digital signal processing and allows for sharper, clearer images at lower endo-illumination levels.25 The 3D visualization system provides an excellent view in an air-filled eye, making it possible to perform intraocular manipulations under air and complete the necessary steps of the surgery, such as laser photocoagulation in the degenerative area within the attached retina, aspiration of SRF by fluid-air exchange, and laser photocoagulation in the detached region.
Moreover, heads-up 3D systems have been utilized during scleral buckling. Endoillumination systems, such as a chandelier or a guarded light pipe, can be used with 3D heads-up visualization during scleral buckling to enable direct visualization of the procedure’s intraocular steps rather than an indirect ophthalmoscope.26 A novel method for intraocular viewing during primary scleral buckling for RRD repair was recently described.27 This approach involves using a guarded light pipe – a light pipe encased in a silicone sleeve – for comprehensive illumination of the retina using the 3D heads-up system. The guarded light pipe is placed in a vitrectomy port. The sleeve prevents advancing the light pipe too far through the cannula into the posterior segment and dragging the vitreous. The light pipe aids in visualizing retinal breaks, guiding cryotherapy, adjusting the height of the buckle, and completing subretinal fluid drainage and enhances teaching primary scleral buckling to trainees. With the integrated visualization, everyone in the room can witness the surgical steps. The video processor of the 3D heads-up display allows the surgeon to open the iris aperture and allow more light from the eye to reach the camera and, by extension, the surgical display. This action ensures sufficient light for effective surgical performance, which can be more challenging with the standard microscope. A comparative study evaluating the guarded light pipe technique against traditional scleral buckling found analogous anatomical and visual outcomes, as well as comparable operative times.28
Use in Combination with Other Intraoperative Imaging Modalities
Intraoperative Three-Dimensional Fluorescein Angiography
Intraoperative fluorescein angiography (FA) involves the utilization of a fluorescent dye which, once introduced into the bloodstream, illuminates retinal blood vessels. This process enables surgeons to evaluate blood flow within the retina during surgery, a feature that can be highly beneficial in the management of retinal vascular disorders, such as proliferative diabetic retinopathy (PDR).
Two case series reported the application of three-dimensional-FA-guided PPV in addressing PDR and retinal vein occlusion.29,30 Employing a high-resolution 3D visualization system, surgeons can obtain real-time information on blood flow within the retina and closely examine the peripheral retina, a task that has been challenging with standard FA approaches in outpatient settings. A key benefit of this approach is the immediate access to angiographic data during surgery, a feature not feasible with traditional surgical techniques. By visually identifying the non-perfusion areas on the same screen, surgeons can ensure that the retinal photocoagulation treatment is precise, minimizing the risk of over- or under-treatment. Furthermore, it was reported that the fibrovascular proliferative membrane (FVPM) position could be easily pinpointed, enabling surgeons to execute the segmentation and removal of the FVPM using the same display.29
Additionally, when retinal vein occlusion is incidentally discovered during PPV for vitreous hemorrhage, it can be difficult to decide the extent of photocoagulation needed and to fully remove FVPM during surgery.30 This difficulty arises from the complications inherent in accurately determining the size and orientation of neovascularization and predicting its adhesion to the vitreoretinal interface, particularly in eyes with incomplete posterior vitreous detachment. 3D-FA can help address these issues by verifying the size and location of neovascularization in real time during surgery.30 Combining intraoperative 3D-FA with optical coherence tomography may provide additional precise information about the vitreoretinal interface surrounding the neovascularization, as well as any intraretinal or subretinal pathological changes. This approach can potentially lead to safer and less invasive PPV procedures.
Intraoperative Optical Coherence Tomography
Intraoperative optical coherence tomography (OCT) is a relatively recent development in ophthalmic surgery, offering real-time, high-resolution imaging of ocular structures during surgical procedures. Intraoperative OCT enables the detection of pathological conditions and alterations in vitreoretinal structures during surgery, thereby enhancing understanding of the anatomy and promoting informed surgical decisions grounded on real-time input.31–33 Conventional viewing systems, like traditional microscopes, have visualization quality and ergonomics limitations. They necessitate beam splitters and laser filters for secure and efficient functioning and fail to offer the same level of detail or adaptability as digital displays.
In contrast, one of the most promising applications of 3D visualization technology is its use in conjunction with intraoperative optical coherence tomography (OCT). A small prospective pilot study reported surgeons’ affirmation that displaying OCT data on a large screen through 3D technology enhanced the examination and analysis of OCT data, improving comfort and efficiency.34 By projecting the OCT on a high-resolution screen, surgeons could scrutinize the data without reverting to the microscope’s external display system. This practice led to a considerable decrease in OCT scanning times compared to another study that employed intraoperative OCT with a conventional microscopy system.33 A recent case report describes the potential of OCT integration in 3D head-up imaging systems in myopic macular schisis repair.35 The technology verified the absence of an iatrogenic macular hole during the repair process, thus empowering surgeons to conduct foveal-sparing ILM peeling without the need for gas tamponade.35
Broader Advantages
Impact on Medical Education
In a standard setup, typically only surgeons operating the microscope can attain stereopsis and adequate visualization. However, a 3D viewing system allows everyone in the operating room to access the same high-definition 3D image. The system has significant educational value, particularly for providing feedback to fellows and residents and teaching medical students. For instance, a pointer can be used by the surgical teacher to guide surgical maneuvers and point out important pathology to the trainee in real time.
Further, the recordings of high-definition 3D videos offer an excellent teaching tool for reviewing surgeries. For viewers who are learning ophthalmic procedures, 3D videos are more instructive than two-dimensional videos. For instance, one prospective randomized study revealed that on anatomy comprehension questions, students who watched 3D video recordings of certain vitreoretinal procedures performed better than those who watched 2D videos of the same procedures.36 In a cross-sectional survey, most medical students reported higher accuracy in identifying the anatomy with the 3D head-up viewing system NGENUITY®, and they preferred this platform over the 2-dimensional display and standard microscopy as their desired learning modality.37 Likely, medical students who work with a surgeon who uses 3D heads-up visualization systems have a more positive experience in the operating room as they can better visualize the steps of the intraocular procedure. Residents also reported greater anatomical knowledge and improved ergonomics with the 3D heads-up system.37 It was also reported that the operation room nurses had an enhanced ability to monitor the case development and foresee which tools might be required.37 This could potentially lead to reduced operating times and minimize errors. Additionally, a questionnaire-based study that assessed the satisfaction levels of surgeons and trainees with 3D HUD compared to the traditional microscope found that both surgeons and trainees were more satisfied with 3D surgery.38 Notably, the trainees reported better satisfaction levels with 3D in various subcomponents, such as visualization, physical aspects, ease of use, and education.38
Telementoring
Telementoring in ophthalmology involves the use of technology to offer remote guidance and supervision to trainees and peers. With telementoring, experienced ophthalmologists can remotely observe and provide real-time feedback to trainees during surgical procedures, diminishing the necessity for trainees to be physically co-located with their mentors. This can improve the accessibility and efficiency of training, particularly for trainees in remote or underserved areas. Additionally, this tool can be employed to teach new techniques and deliver continuing surgical education for seasoned surgeons.
The integration of 3D visualization systems on ophthalmology telementoring potentially elevates the training experience for both trainees and mentors. It does this by offering a more immersive and lifelike view of the surgical field, enabling better visualization and comprehension of the anatomical structure, a feature particularly beneficial for intricate ophthalmic procedures. A recent report revealed that using affordable video-capturing hardware and a streaming application, live, low-latency 3D streaming of vitreoretinal procedures is possible.39 The inclusion of 3D visualization systems in telementoring programs allows trainees to receive more effective and individualized guidance, potentially enhancing surgical outcomes.
Improved Ergonomics
Musculoskeletal problems are common among ophthalmologists due to the nature of their work, which involves long hours of sitting or standing, repetitive movements, and prolonged use of instruments such as microscopes. These conditions can exert strain on different body parts, and over time, culminate in musculoskeletal disorders such as neck and lower back pain. A survey of eye care specialists revealed that compared to family medicine doctors, ophthalmologists and optometrists have a higher prevalence of neck, wrist, and lower back discomfort.40 Contributing factors were identified as repeated work, extended or awkward positions, and bending of the joints. Additionally, an online survey of 127 ophthalmologists found that 66% of respondents experienced work-related pain.41 Time spent in surgery was significantly associated with musculoskeletal symptoms.41 Notably, 14% of the participants stated that they intended to retire early due to the symptoms they experienced.41 Considering these facts, it is important to consider improving the work settings of eye care practitioners to avoid musculoskeletal problems and associated personal and economic costs.
The 3D visualization systems help improve ergonomics by providing surgeons with a more comfortable and efficient working environment and reducing physical strain. According to a survey of ophthalmic surgeons, heads-up displays improved posture and increased general comfort.42 A majority of the respondents who experienced pain or discomfort during procedures reported less discomfort since employing heads-up displays. Intriguingly, those who used heads-up displays for over half of their cases had approximately five times higher likelihood of reporting pain reduction.42 Another survey also found that the device improved symptoms, especially in the cervical and lumbar areas, for more than half of the users.43 A report also indicates that performing procedures with 3D technology and positioning can be more manageable when the patient has a spinal malformation or needs surgery in the Trendelenburg position.44
Reduction in Phototoxicity
Phototoxicity is a potential complication during ophthalmic microsurgery, which can cause retinal damage due to prolonged exposure to intense light from sources. Phototoxicity from endo-illumination during vitreoretinal surgery is well-described in the literature.45 In 3D viewing systems, the image is created by putting together inputs from two cameras, and it is subsequently processed by algorithms that enable the detection and magnification of light levels lower than those easily detectable by the human eye. Hence, this process improves the image brightness, leading to lower illumination levels.46 An initial comparative study on 3D visualization reported that light intensity had to be set at 100% for certain procedures without a 3D system. However, with the 3D system, such a high setting was never necessary.2 This study also reported that certain vitreoretinal procedures could be completed with 20% less light intensity due to the signal amplification.2 Moreover, a prospective, observational surgical case series of 10 patients investigated the minimal endo-illumination levels required to perform 3D heads-up vitreoretinal surgery.47 The surgeons found that they could comfortably work at an endo-illumination level of 10% of maximum output or less with 3D heads-up setups, compared to standard operating microscopes in which the endo-illuminator was set to 40% of the maximum output.47 Recent studies have further confirmed a considerable decrease in light intensity during different ophthalmic procedures, which can lower the risk of phototoxicity and increase patient comfort.48,49
Improved Depth of Field
Depth of field refers to the range of distances within which objects appear in focus, and it directly affects the clarity of the surgeon’s vision during the procedure. A narrow depth of field can make it difficult for the surgeon to maintain focus on the critical structures within the eye, while a larger depth of field can provide a more detailed and accurate view. On a conventional microscope, the accommodative capabilities of each surgeon can affect the depth of field. In contrast, the depth of field on 3D displays is unaffected by the user’s capacity to accommodate. Reduced eye strain can be a benefit of 3D systems because they do not require near vision. Therefore, the surgeon does not have to accommodate while looking through the eyepiece for an extended period.
Depth perception is crucial for most vitreoretinal procedures, which demand accurate hand-eye coordination.50 The spacing between the optical beams in the 3D system is larger than in the standard surgical microscope. Moreover, there is an option to select among lenses with multiple different objective working distances.5 A physician questionnaire survey evaluating the depth of field, lateral resolution, and image quality of a heads-up 3D visualization system found that, based on subjective assessments, surgeons preferred the digital 3D system over the traditional eyepiece, especially at high magnifications.51 Another report stated that if the aperture of the 3D system camera is decreased to 30%, the depth of field is up to three times larger than the standard microscope.46
Color Filters
Indocyanine green (ICG) preferentially stains the ILM and aids in the visualization and removal of the membrane from the retina. Toxicity and retinal damage from the dye have been described in vitro and in vivo, as well as following macular surgery.52 The 3D visualization systems enable surgeons to apply color filters, potentially limiting the need for dye and thereby reducing both the amount and duration of dye exposure, thus mitigating the risk of toxicity. A prospective comparative observational study demonstrated that during ILM peeling, customized settings on digitally assisted vitreoretinal surgery allowed surgeons to employ an ICG concentration that was three times lower compared to that used with a standard operating microscope.53
In addition to the black and white filter, which is often used to achieve contrast in ILM peeling, other color filtering options are available. According to a survey of surgeons in France, some of the most commonly used filters, following the black and white filter, include the red-free filter for hemorrhage suppression and the yellow filter for fluid-air exchange.54
Visualization of Details and Integration with Operating Systems
Our experience demonstrates that 3D systems deliver sharp focus and reveal a broader range of details. In addition to offering up a high-depth resolution, high dynamic range imaging merges underexposed and overexposed images, resulting in superior detail recognition and contrast. Additionally, 3D heads-up visualization systems can facilitate seamless integration with operating systems. The key to the seamless integration of Alcon’s CONSTELLATION® Surgical system with NGENUITY® lies in a software solution that combines these systems to manage crucial data parameters seamlessly, such as intraocular pressure, flow velocities, infusion pressures, and laser intensity. This specialized software enhances the surgical experience by offering customization features, preset imaging modes, advanced video recording options, and improvements to the user interface, including procedural flow enhancements for improved white balance. Figure 1 summarizes some of the advantages of 3D heads-up visualization systems.
 |
Figure 1 Advantages and applications of 3D heads-up visualization systems. |
Potential Drawbacks
The Experience of the Assistant Surgeon
Despite its overall positive impacts on ergonomics, some reports have indicated that in certain cases, the use of a 3D heads-up system may have the opposite outcome on ergonomics for members of the care team. A questionnaire-based study revealed that the second assistant might need to adopt uncomfortable or awkward postures if the room design requires perpendicular positioning to the primary surgeon.55 This positioning can make it uncomfortable for them to keep turning their heads to the monitor.55 However, with appropriate room setup, this discomfort can likely be avoided, and the positioning may still be preferable to the neck and back strain associated with the assistant peering into microscope oculars.
The Experience for the Anesthesia Team
Although 3D monitors improve the experience of most personnel in the operating room, this setup can be more unfavorable for the anesthesia team. For example, in a cross-sectional survey of care team members, anesthesiologists reported that 3D displays did not lead to greater engagement in the surgical case, likely because it is typically impossible to view both the 3D display and the anesthesia monitors simultaneously.37 However, it is still possible to simultaneously project the case onto 2D monitors.
Setup and Operating Room Space
Three-dimensional surgical viewing systems require a substantial setup process. The combination of multiple technological components, such as stereoscopic displays and recording devices, necessitates a meticulous assembly procedure, which can be complex and time-consuming. The large monitors in the operation room may also limit the anesthetist’s access to the patient.55 The system requires more space than just a standard microscope. The operating room must be sufficiently large to accommodate the extensive viewing display, enabling non-operating personnel to move around and perform their tasks.6
The Learning Curve
The learning curve for using a 3D heads-up system may pose a challenge, particularly for surgeons who are accustomed to traditional microscopes. For instance, a prospective randomized study of 39 cases of PPV for epiretinal membrane or macular hole discovered that with a 3D heads-up system, macular peel times were longer and associated with reduced surgeon-reported ease of use.18 This finding may be partially attributable to the learning curve that accompanies this new technology. Despite this, studies have found that the use of 3D systems has a relatively brief learning curve. In a comparative observational study that analyzed the required time for PPV and ILM peels using traditional microscopy and a 3D visualization system, one experienced surgeon and three fellows performed macular hole surgeries, completing five procedures with traditional microscopy and five with the 3D system.19 The study found no significant difference in the duration of surgery between using the 3D system and the traditional microscopy.19 This finding can be attributed to the short learning curve associated with the 3D system. To attain confidence in using this technology, the surgeons needed to perform only five surgeries using the 3D system. Moreover, a first-year retina fellow carried out the first surgery using the 3D system, further supporting a brief learning curve.19 With adequate practice and experience, all vitreoretinal surgeons should be able to become proficient in using the system.
Financial Costs
The use of 3D heads-up systems constitutes an additional expense in comparison to traditional microscopes. These costs may encompass the purchase of specialized equipment, including the 3D monitor and stereo viewing glasses, as well as the cost of maintenance and repairs. Another drawback involves the large data files 3D imaging systems create; these can complicate data processing and lead to higher storage costs. Additionally, training may be necessary for the surgical team, leading to further expenses. It should be noted, however, that while there may be some initial costs associated with the adoption of a 3D heads-up system, potential benefits exist. These include enhanced visualization and ergonomics during surgery, which can lead to superior outcomes for both patients and surgeons and may ultimately reduce the overall costs of use.
Refocusing of the Microscope
While the systems obviate the need for eye accommodation, they also introduce their own challenges. The absence of natural eye accommodation means that surgeons must frequently refocus the microscope throughout the procedure. This necessity can be cumbersome and interrupt the surgical flow. Careful calibration for depth perception is essential to tailor the system to the surgeon’s visual needs, ensuring an optimal 3D view that alleviates eye strain or visual fatigue. Thus, the implementation and effective use of 3D viewing systems in vitreoretinal surgery demand a balance of effort, expertise, and continual adjustments.
Future Directions
Teleophthalmology is a promising application of 3D visualization technology. The recent demonstration of live webcasting of 3D retina surgery in 4K over a 5G network serves as a proof of concept with significant implications for the field.56 With the assistance of intraoperative high-definition streams, experienced surgeons may be able to offer live remote assistance and recommendations, especially for more complex cases. In underserved countries, this technology could expand the availability of specialists and improve surgical training. The military or any facilities in remote locations that lack access to specialty care may also derive benefits from this technology.
Another exciting advancement in the use of 3D visualization technology occurs in the realm of virtual reality. Academic conferences, which are vital for disseminating novel research findings and advancing the field, have increasingly utilized digital solutions since the onset of the COVID-19 pandemic to conduct scientific meetings.57 These technologies have predominantly relied on video conferencing applications. Virtual meetings have addressed long-standing challenges associated with traditional in-person conferences, such as balancing clinical responsibilities, mitigating financial costs, and minimizing disruptions to sleep habits caused by time zone differences.
Virtual reality has emerged as a new frontier in scientific collaboration within this innovative ecosystem. The virtual reality environment leverages numerous benefits of both in-person and remote conferences. This system allows remote check-in, making it more accessible, cost-effective, and flexible for attendees. Attendees may navigate the conference setting in a manner akin to a real-world event, allowing them to efficiently attend multiple sessions.58 Recently, the 2022 Digital Ophthalmic Society meeting was held in a virtual reality space, offering a more immersive interaction than traditional video conferencing platforms.59 The virtual environment also incorporates spatial audio, enabling users to concentrate on proximate sounds without distraction from noise elsewhere in the digital space.59 The 3D visualization systems’ ability to record surgery in 3D makes it particularly suitable for virtual reality viewing.
When 3D surgical recordings are integrated into virtual reality, they can present a superior experience compared to the two-dimensional capabilities of traditional systems. As the usage of virtual reality expands, ophthalmic specialists may participate in clinical education and provide live feedback for operations. Similarly, trainees from around the world may learn from live procedures conducted by retina experts. The virtual reality space provides a dynamic setting in which inquiries may be posed live. These educational experiences may complement the training of residents and fellows, particularly in atypical or challenging cases that are typically treated in specialized facilities. Although live broadcasting has not yet been integrated into virtual reality platforms, the proof of concept for merging live 3D streams with virtual reality has already been described in vitreoretinal procedures.39
Another potential future application of 3D visualization technology is its use in remotely guided robotic surgery. A crucial step in enabling this type of surgery is the transition to high-definition, three-dimensional live imaging. It has been demonstrated that ocular surgeries can be performed with the da Vinci robot.60 Robotics can increase dexterity, eliminate tremors, and enable remote surgery thanks to their high precision and exquisite mechanical control.61 This technology can provide novel treatment options for specific conditions, such as retinal vein cannulation, where surgical alternatives are restricted by the physiological limitations of the human hand.62 However, the adoption of robotics in ophthalmology presents challenges, such as the fragile nature of the eye and unanticipated movements of the patient’s head.
Lastly, the further integration of artificial intelligence (AI) represents an exciting development in ophthalmology. Live operator support and the combined use of AI with robotic advancements can lead to semi-autonomous robotic interventions. This collaboration may result in more precise and efficient surgical procedures, allowing surgeons to perform complex operations with greater ease and accuracy.
Conclusion
In conclusion, 3D visualization technology has revolutionized vitreoretinal surgery, providing surgeons with numerous advantages, including enhanced visualization, ergonomics, and depth perception. Although the technology may present potential drawbacks, such as a learning curve and increased costs, its benefits are poised to improve both patient outcomes and satisfaction within the surgical team. Future research could focus on the long-term effects of 3D visualization technology on surgical outcomes, further exploring the role of virtual reality and teleophthalmology in surgical education, remote surgical assistance, and the development of robotics and artificial intelligence in surgeries. By persisting in the investigation and development of 3D visualization technology in ophthalmology, the field can continue to evolve and enhance, ultimately leading to improved outcomes.
Data Sharing Statement
Unpublished data, available upon request from the corresponding author.
Funding
This research received no external funding.
Disclosure
D.J.D is a consultant for Alcon. J.B.M. is a consultant for Alcon, Allergan, Topcon, Carl Zeiss, Sunovion, and Genentech. The authors report no other conflicts of interest in this work.
References
1. Agranat JS, Miller JB. 3D surgical viewing systems in vitreoretinal surgery. Int Ophthalmol Clin. 2020;60:17–23. doi:10.1097/iio.0000000000000291
2. Eckardt C, Paulo EB. Heads-up Surgery for Vitreoretinal Procedures: an experimental and clinical study. Retina. 2016;36:137–147. doi:10.1097/iae.0000000000000689
3. Kelkar JA, Kelkar AS, Bolisetty M. Initial experience with three-dimensional heads-up display system for cataract surgery - A comparative study. Indian J Ophthalmol. 2021;69:2304–2309. doi:10.4103/ijo.IJO_231_21
4. Del Turco C, D’AmicoRicci G, Dal Vecchio M, et al. Heads-up 3D eye surgery: safety outcomes and technological review after 2 years of day-to-day use. Eur J Ophthalmol. 2021;11206721211012856. doi:10.1177/11206721211012856
5. Romano MR, Cennamo G, Comune C, et al. Evaluation of 3D heads-up vitrectomy: outcomes of psychometric skills testing and surgeon satisfaction. Eye. 2018;32:1093–1098. doi:10.1038/s41433-018-0027-1
6. Agranat JS, Miller JB, Douglas VP, et al. The scope of three-dimensional digital visualization systems in vitreoretinal surgery. Clin Ophthalmol. 2019;13:2093–2096. doi:10.2147/OPTH.S213834
7. Kantor P, Matonti F, Varenne F, et al. Use of the heads-up NGENUITY 3D visualization system for vitreoretinal surgery: a retrospective evaluation of outcomes in a French tertiary center. Sci Rep. 2021;11:10031. doi:10.1038/s41598-021-88993-z
8. Zhang T, Tang W, Xu G. Comparative analysis of three-dimensional heads-up vitrectomy and traditional microscopic vitrectomy for vitreoretinal diseases. Curr Eye Res. 2019;44:1080–1086. doi:10.1080/02713683.2019.1612443
9. Kumar A, Hasan N, Kakkar P, et al. Comparison of clinical outcomes between “heads-up” 3D viewing system and conventional microscope in macular hole surgeries: a pilot study. Indian J Ophthalmol. 2018;66:1816–1819. doi:10.4103/ijo.IJO_59_18
10. Reddy S, Mallikarjun K, Mohamed A, et al. Comparing clinical outcomes of macular hole surgeries performed by trainee surgeons using a 3D heads-up display viewing system versus a standard operating microscope. Int Ophthalmol. 2021;41:2649–2655. doi:10.1007/s10792-021-01792-3
11. Kim DJ, Kim DG, Park KH. Three-dimensional heads-up vitrectomy versus conventional microscopic vitrectomy for patients with epiretinal membrane. Retina. 2023;43:1010–1018. doi:10.1097/iae.0000000000003762
12. Zhao XY, Zhao Q, Li NN, et al. Surgery-related characteristics, efficacy, safety and surgical team satisfaction of three-dimensional heads-up system versus traditional microscopic equipment for various vitreoretinal diseases. Graefes Arch Clin Exp Ophthalmol. 2023;261:669–679. doi:10.1007/s00417-022-05850-z
13. Coppola M, La Spina C, Rabiolo A, Querques G, Bandello F. Heads-up 3D vision system for retinal detachment surgery. Int J Retina Vitreous. 2017;3:46. doi:10.1186/s40942-017-0099-2
14. Rani D, Kumar A, Chandra P, Chawla R, Hasan N, Agarwal D. Heads-up 3D viewing system in rhegmatogenous retinal detachment with proliferative vitreoretinopathy - A prospective randomized trial. Indian J Ophthalmol. 2021;69:320–325. doi:10.4103/ijo.IJO_1720_20
15. Kannan NB, Jena S, Sen S, Kohli P, Ramasamy K. A comparison of using digitally assisted vitreoretinal surgery during repair of rhegmatogenous retinal detachments to the conventional analog microscope: a prospective interventional study. Int Ophthalmol. 2021;41:1689–1695. doi:10.1007/s10792-021-01725-0
16. Zeng R, Feng Y, Begaj T, Baldwin G, Miller JB. Comparison of the safety and efficacy of a 3-dimensional heads-up display vs a standard operating microscope in retinal detachment repair. J Vitreoretin Dis. 2023;7:97–102. doi:10.1177/24741264221150074
17. Asani B, Siedlecki J, Schworm B, et al. 3D heads-up display vs. Standard operating microscope vitrectomy for rhegmatogenous retinal detachment. Front Med. 2020;7:615515. doi:10.3389/fmed.2020.615515
18. Talcott KE, Adam MK, Sioufi K, et al. Comparison of a three-dimensional heads-up display surgical platform with a standard operating microscope for macular surgery. Ophthalmol Retina. 2019;3:244–251. doi:10.1016/j.oret.2018.10.016
19. Palácios RM, Maia A, Farah ME, Maia M. Learning curve of three-dimensional heads-up vitreoretinal surgery for treating macular holes: a prospective study. Int Ophthalmol. 2019;39:2353–2359. doi:10.1007/s10792-019-01075-y
20. Mura M, Martin W, Williams KK, Abulon DJK. Comparison of 3D digitally assisted visualization system with current standard visualization for the removal of vitreous in a preclinical model. Clin Ophthalmol. 2021;15:4499–4505. doi:10.2147/opth.S327570
21. Kita M, Mori Y, Hama S. Hybrid wide-angle viewing-endoscopic vitrectomy using a 3D visualization system. Clin Ophthalmol. 2018;12:313–317. doi:10.2147/opth.S156497
22. Todorich B, Stem MS, Hassan TS, Williams GA, Faia LJ. Scleral transillumination with digital heads-up display: a novel technique for visualization during vitrectomy surgery. Ophthalmic Surg Lasers Imaging Retina. 2018;49:436–439. doi:10.3928/23258160-20180601-08
23. Xia S, Zhao X-Y, Wang E-Q, Chen Y-X. Comparison of face-down posturing with nonsupine posturing after macular hole surgery: a meta-analysis. BMC Ophthalmol. 2019;19(1):34. doi:10.1186/s12886-019-1047-8
24. Francone A, Charles M. Extensive internal limiting membrane peeling for proliferative vitreoretinopathy. Int Ophthalmol. 2023;43:147–153. doi:10.1007/s10792-022-02397-0
25. Guan L, Chen J, Tang Y, et al. 3D visualization system-assisted vitrectomy for rhegmatogenous retinal detachment: leave out the perfluorocarbon liquid. Ophthalmol Ther. 2023;12:1611–1619. doi:10.1007/s40123-023-00692-2
26. Nam KY, Kim WJ, Jo YJ, Kim JY. Scleral buckling technique using a 25-gauge chandelier endoilluminator. RETINA. 2013;33:880–882. doi:10.1097/IAE.0b013e31827e2602
27. Agranat JS, Douglas VP, Douglas KAA, Miller JB. A guarded light pipe for direct visualization during primary scleral buckling on the Ngenuity platform. Int J Retina Vitreous. 2020;6:42. doi:10.1186/s40942-020-00246-9
28. Baldwin G, Sokol JT, Ludwig CA, Miller JB. A Comparative study of traditional scleral buckling to a new technique: guarded light pipe with heads-up three-dimensional visualization. Clin Ophthalmol. 2022;16:3079–3088. doi:10.2147/opth.S378179
29. Imai H, Tetsumoto A, Inoue S, et al. Intraoperative three-dimensional fluorescein angiography-guided pars plana vitrectomy for the treatment of proliferative diabetic retinopathy: the maximized utility of the digital assisted vitrectomy. Retina. 2023;43:359–362. doi:10.1097/iae.0000000000002805
30. Imai H, Tetsumoto A, Yamada H, et al. Intraoperative three-dimensional fluorescein angiography-guided pars plana vitrectomy for branch retinal vein occlusion. Retin Cases Brief Rep. 2022;16:802–805. doi:10.1097/icb.0000000000001091
31. Ehlers JP, Goshe J, Dupps WJ, et al. Determination of feasibility and utility of microscope-integrated optical coherence tomography during ophthalmic surgery: the DISCOVER Study RESCAN Results. JAMA Ophthalmol. 2015;133:1124–1132. doi:10.1001/jamaophthalmol.2015.2376
32. Ray R, Barañano DE, Fortun JA, et al. Intraoperative microscope-mounted spectral domain optical coherence tomography for evaluation of retinal anatomy during macular surgery. Ophthalmology. 2011;118:2212–2217. doi:10.1016/j.ophtha.2011.04.012
33. Ehlers JP, Dupps WJ, Kaiser PK, et al. The prospective intraoperative and perioperative ophthalmic ImagiNg with optical CoherEncE TomogRaphy (PIONEER) study: 2-year results. Am J Ophthalmol. 2014;158:999–1007. doi:10.1016/j.ajo.2014.07.034
34. Ehlers JP, Uchida A, Srivastava SK. The integrative surgical theater: combining intraoperative optical coherence tomography and 3D digital visualization for vitreoretinal surgery in the DISCOVER study. Retina. 2018;38(1):S88–s96. doi:10.1097/iae.0000000000001999
35. Palácios RM, Kayat KV, Farah ME, Devin F. Heads-up digitally assisted surgical viewing with intraoperative optical coherence tomography for myopic schisis repair. J Ophthalmic Vis Res. 2021;16:127–130. doi:10.18502/jovr.v16i1.8259
36. Chhaya N, Helmy O, Piri N, Palacio A, Schaal S. Comparison of 2D and 3D video displays for teaching vitreoretinal surgery. Retina. 2018;38:1556–1561. doi:10.1097/iae.0000000000001743
37. Shoshany TN, Agranat JS, Armstrong G, Miller JB. The user experience on a 3-dimensional heads-up display for vitreoretinal surgery across all members of the health care team: a survey of medical students, residents, fellows, attending surgeons, nurses, and anesthesiologists. J VitreoRet Dis. 2020;4:459–466. doi:10.1177/2474126420929614
38. Cheng TC, Yahya MFN, Mohd Naffi AA, et al. Evaluation of three-dimensional heads up ophthalmic surgery demonstration from the perspective of surgeons and postgraduate trainees. J Craniofac Surg. 2021;32:2285–2291. doi:10.1097/scs.0000000000007645
39. Seddon IA, Rahimy E, Miller JB, Charles S, Kitchens J, Houston SK. Feasibility and potential for real-time 3D vitreoretinal surgery telementoring. Retina. 2022. doi:10.1097/iae.0000000000003656
40. Kitzmann AS, Fethke NB, Baratz KH, Zimmerman MB, Hackbarth DJ, Gehrs KM. A survey study of musculoskeletal disorders among eye care physicians compared with family medicine physicians. Ophthalmology. 2012;119:213–220. doi:10.1016/j.ophtha.2011.06.034
41. Schechet MDSA, DeVience MDE, DeVience PS, Shukla MDS, Kaleem MDM. Survey of musculoskeletal disorders among US ophthalmologists. Digit J Ophthalmol. 2020;26:36–41. doi:10.5693/djo.01.2020.02.001
42. Weinstock RJ, Ainslie-Garcia MH, Ferko NC, et al. Comparative assessment of ergonomic experience with heads-up display and conventional surgical microscope in the operating room. Clin Ophthalmol. 2021;15:347–356. doi:10.2147/opth.S292152
43. Tan NE, Wortz BT, Rosenberg ED, Radcliffe NM, Gupta PK. Impact of heads-up display use on ophthalmologist productivity, wellness, and musculoskeletal symptoms: a survey study. J Curr Ophthalmol. 2022;34:305–311. doi:10.4103/joco.joco_115_22
44. Skinner CC, Riemann CD. “Heads up” digitally assisted surgical viewing for retinal detachment repair in a patient with severe kyphosis. Retin Cases Brief Rep. 2018;12:257–259. doi:10.1097/icb.0000000000000486
45. Postel EA, Pulido JS, Byrnes GA, et al. Long-term follow-up of iatrogenic phototoxicity. Arch Ophthalmol. 1998;116:753–757. doi:10.1001/archopht.116.6.753
46. Franklin AJ, Sarangapani R, Yin L, Tripathi B, Riemann C. Digital vs analog surgical visualization for vitreoretinal surgery. Retinal Phys. 2017;2017:1.
47. Adam MK, Thornton S, Regillo CD, Park C, Ho AC, Hsu J. Minimal endoillumination levels and display luminous emittance during three-dimensional heads-up vitreoretinal surgery. Retina. 2017;37:1746–1749. doi:10.1097/iae.0000000000001420
48. Vélasque L, Arbousoff N, Rigaudier F, et al. Lux study: contribution of a three-dimensional, high dynamic range, ultra-high-definition heads-up visualization system to a significant delivered light intensity decrease during different types of ocular surgeries. J Fr Ophtalmol. 2021;44:1129–1141. doi:10.1016/j.jfo.2021.01.006
49. Horigome Y, Iwashita Y, Hirono K, et al. Evaluation of the retinal hazard with 3D digitally assisted visualization system and conventional microscope in macular surgeries. Retina. 2022;42:2301–2306. doi:10.1097/iae.0000000000003621
50. Bloch E, Uddin N, Gannon L, Rantell K, Jain S. The effects of absence of stereopsis on performance of a simulated surgical task in two-dimensional and three-dimensional viewing conditions. Br J Ophthalmol. 2015;99:240–245. doi:10.1136/bjophthalmol-2013-304517
51. Freeman WR, Chen KC, Ho J, et al. Resolution, depth of field, and physician satisfaction during digitally assisted vitreoretinal surgery. Retina. 2019;39:1768–1771. doi:10.1097/iae.0000000000002236
52. Takayama K, Sato T, Karasawa Y, Sato S, Ito M, Takeuchi M. Phototoxicity of indocyanine green and Brilliant Blue G under continuous fluorescent illumination on cultured human retinal pigment epithelial cells. Invest Ophthalmol Vis Sci. 2012;53:7389–7394. doi:10.1167/iovs.12-10754
53. Park SJ, Do JR, Shin JP, Park DH. Customized color settings of digitally assisted vitreoretinal surgery to enable use of lower dye concentrations during macular surgery. Front Med. 2021;8:810070. doi:10.3389/fmed.2021.810070
54. Palácios RM, Kayat KV, Morel C, et al. Clinical study on the initial experiences of french vitreoretinal surgeons with heads-up surgery. Curr Eye Res. 2020;45:1265–1272. doi:10.1080/02713683.2020.1737136
55. Rizzo S, Abbruzzese G, Savastano A, et al. 3D surgical viewing system in ophthalmology: perceptions of the surgical team. RETINA. 2018;38:857–861. doi:10.1097/iae.0000000000002018
56. Lu ES, Reppucci VS, Houston SKS, Kras AL, Miller JB. Three-dimensional telesurgery and remote proctoring over a 5G network. Digit J Ophthalmol. 2021;27:38–43. doi:10.5693/djo.01.2021.06.003
57. Valenti A, Fortuna G, Barillari C, Cannone E, Boccuni V, Iavicoli S. The future of scientific conferences in the era of the COVID-19 pandemic: critical analysis and future perspectives. Ind Health. 2021;59:334–339. doi:10.2486/indhealth.2021-0102
58. Ong J, Hariprasad SM, Chhablani J. Into the retinaverse: a new frontier of retina in the metaverse. Ophthalmic Surg Lasers Imaging Retina. 2022;53:595–600. doi:10.3928/23258160-20221017-01
59. Young A. Ophthalmology takes the plunge into the metaverse. MetaMed; 2022. Available from: https://www.metamedmedia.com/blog/ophthalmology-takes-the-plunge-into-the-metaverse.
60. Chammas J, Sauer A, Pizzuto J, et al. Da vinci xi robot-assisted penetrating keratoplasty. Transl Vis Sci Technol. 2017;6:21. doi:10.1167/tvst.6.3.21
61. Molaei A, Abedloo E, de Smet MD, et al. Toward the art of robotic-assisted vitreoretinal surgery. J Ophthalmic Vis Res. 2017;12:212–218. doi:10.4103/jovr.jovr_63_17
62. Gijbels A, Smits J, Schoevaerdts L, et al. In-human robot-assisted retinal vein cannulation, A world first. Ann Biomed Eng. 2018;46:1676–1685. doi:10.1007/s10439-018-2053-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.