Back to Journals » Journal of Inflammation Research » Volume 19
HDL-Adjusted Inflammatory Ratios and Sequential Graft Configuration are Associated with Mid-Term Saphenous Vein Graft Occlusion in a Post-CABG Angiography Cohort
Authors Hosoglu Y ![]() , Tibilli H, Kavalci V, Hoşoğlu A
, Tibilli H, Kavalci V, Hoşoğlu A
Received 21 December 2025
Accepted for publication 6 March 2026
Published 23 March 2026 Volume 2026:19 590762
DOI https://doi.org/10.2147/JIR.S590762
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Yusuf Hosoglu,1 Hakan Tibilli,2 Veysi Kavalci,3 Ayşe Hoşoğlu4
1Department of Cardiology, Private Koru Sincan Hospital, Ankara, Türkiye; 2Department of Cardiology, Başkent University Adana Hospital, Adana, Türkiye; 3Department of Cardiology, Faculty of Medicine, Adıyaman University, Adıyaman, Türkiye; 4Department of Cardiology, Başkent University Ankara Hospital, Ankara, Türkiye
Correspondence: Yusuf Hosoglu, Department of Cardiology, Private Koru Sincan Hospital, Ankara, Türkiye, Email [email protected]
Background: Saphenous vein graft (SVG) failure limits long-term outcomes after coronary artery bypass grafting (CABG). HDL-adjusted inflammatory ratios, including the neutrophil-to-HDL ratio (NHDLr) and lymphocyte-to-HDL ratio (LHDLr), have emerged as markers of vascular inflammation, but their association with SVG occlusion in the post-CABG setting is unclear. We evaluated whether HDL-adjusted inflammatory ratios and sequential graft configuration are associated with mid-term SVG occlusion.
Methods: This retrospective observational study included 190 post-CABG patients who underwent clinically indicated follow-up coronary angiography. Patients were categorized by the presence (n=72) or absence (n=118) of at least one occluded SVG. HDL-adjusted ratios were calculated from fasting blood tests obtained at the outpatient visit when angiography was planned. Multivariable logistic regression was used to identify independent predictors of SVG occlusion.
Results: Patients with SVG occlusion had higher NHDLr (5.07 vs 4.41, p=0.006) and LHDLr (2.48 vs 2.15, p=0.012). Median time from CABG to index angiography was 40.9 months (IQR 23.5– 66.5). Sequential grafting was more frequent in the occlusion group (33.3% vs 11.9%, p< 0.001). In multivariable analysis, sequential grafting (adjusted OR 3.58, 95% CI 1.63– 7.85), female sex (OR 2.05, 95% CI 1.06– 3.94), NHDLr (OR 1.18, 95% CI 1.01– 1.38), and LHDLr (OR 1.39, 95% CI 1.04– 1.87) were independently associated with SVG occlusion. The combined model showed moderate discrimination (AUC 0.729). SVG occlusion was not associated with all-cause mortality during follow-up (p=0.566).
Conclusion: In a post-CABG cohort undergoing follow-up angiography, elevated NHDLr and LHDLr and sequential grafting were independently associated with mid-term SVG occlusion. These findings support further validation of HDL-adjusted inflammatory ratios as accessible markers related to graft vulnerability in this setting.
Keywords: coronary artery bypass, saphenous vein, inflammation, high-density lipoproteins
Introduction
Coronary artery bypass grafting (CABG) remains a cornerstone revascularization strategy for multivessel coronary artery disease, yet the durability of saphenous vein grafts (SVG) continues to limit long-term outcomes. SVG failure follows a characteristic progression that includes early thrombosis, intimal hyperplasia within the first postoperative year, and the subsequent development of accelerated atherosclerosis.1,2 Clinically, SVG failure is common in mid-term follow-up, with roughly half of grafts failing by 5–10 years in many series, which underscores the value of identifying biological and procedural contributors to graft occlusion.3,4
Traditional cardiovascular risk factors and isolated lipid measures do not always explain SVG patency, suggesting that graft failure reflects mechanisms not captured by standard risk profiling.3 Because implanted vein grafts undergo abrupt hemodynamic and shear-stress changes, and low or disturbed shear is linked to endothelial activation and graft stenosis, inflammatory indices may be particularly relevant in the arterialised graft setting.5,6 These considerations support evaluating inflammation-related biomarkers in a post-CABG setting that is biologically distinct from native coronary atherosclerosis.1
In this context, composite indices integrating circulating leukocyte counts with high-density lipoprotein cholesterol (HDL-C) have been proposed as readily available markers of the balance between systemic inflammatory activity and HDL-mediated vascular protection. HDL-adjusted ratios, including neutrophil-to-HDL (NHR/NHDLr), lymphocyte-to-HDL (LHDLr), and white blood cell–to–HDL (WHDLr) ratios, have shown associations with disease severity and prognosis in native coronary disease cohorts and broader populations.7–9 However, data on these indices in post-CABG cohorts, where the target pathology is arterialised vein-graft disease rather than native-plaque progression, remain limited, and evidence for lymphocyte-to-HDL–based measures is comparatively sparse.
Surgical configuration is another determinant of saphenous vein graft performance. Sequential grafting can improve conduit efficiency, yet the altered flow patterns may create regions of low shear stress that promote thrombosis, intimal hyperplasia and accelerated atherosclerosis.1 Prior studies have reported conflicting findings regarding whether sequential grafts outperform or underperform individual anastomoses, with some showing superior patency and others demonstrating equivalent or inferior outcomes.10–12 These inconsistencies highlight the need to clarify both biological and technical determinants of mid-term graft deterioration. Accordingly, the present study evaluated, within a contemporary post-CABG cohort undergoing clinically indicated follow-up angiography, whether HDL-adjusted inflammatory indices (NHDLr, LHDLr, and WHDLr) and procedural characteristics are associated with angiographically confirmed SVG occlusion. We also assessed the relationship between graft occlusion and long-term survival.
Methods
This retrospective observational study included patients who underwent CABG at a tertiary university hospital between January 2013 and January 2024 and later underwent invasive coronary angiography (CAG) for clinical indications included recurrent or progressive angina, abnormal findings on noninvasive stress testing. Patients with missing laboratory data, previous cardiac surgery, congenital heart disease, active malignancy, chronic inflammatory or infectious conditions, or incomplete angiographic records were excluded. After applying these criteria, 190 patients were included in the final analysis (Figure 1. Flowchart of the study). Ethical approval was obtained from the institutional review board, and all procedures complied with the Declaration of Helsinki. This study is reported in accordance with the RECORD guideline for observational studies using routinely collected health data.
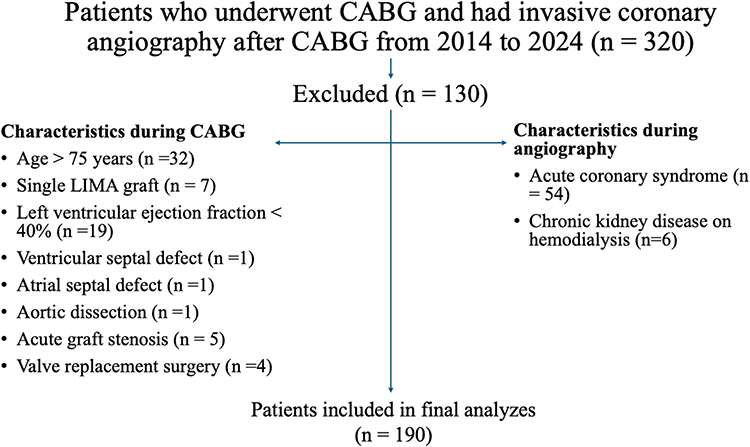 |
Figure 1 Flow diagram of patient selection. |
Demographic characteristics, comorbidities, operative details, and medications were collected from electronic medical record, surgical operative notes, catheterization/angiography reporting system, and laboratory information system. No linkage to external databases was performed. Comorbidities were abstracted from clinician-documented diagnoses in the electronic record. All laboratory measurements were obtained from a single 8-hour fasting venous blood sample drawn during the outpatient visit in which elective angiography was planned. These values therefore reflect the concurrent inflammatory and metabolic status at the time of graft evaluation rather than preoperative or longitudinal biomarker levels. CRP/hs-CRP values were available only in a small, non-systematically tested subset of patients and were therefore not analyzed due to substantial missingness and high risk of selection bias. Hematologic variables included WBC, neutrophil, and lymphocyte counts. Because both systemic inflammation and HDL-associated vascular protection are implicated in the biological processes that contribute to graft degeneration, we calculated HDL-adjusted leukocyte ratios such as the neutrophil to HDL ratio (NHDLr), lymphocyte to HDL ratio (LHDLr), and WBC to HDL ratio (WHDLr) as novel inflammatory and atherogenic indices. These ratios were selected a priori based on biological rationale and prior literature; however, the analysis was not prospectively registered and should be considered hypothesis-generating. Biochemical parameters including lipid profile, glucose, creatinine, electrolytes, and liver enzymes were analyzed using standard automated methods. Lipid concentrations were obtained in mg/dL and converted to mmol/L using standard conversion factors. Neutrophil, lymphocyte, and total WBC counts were recorded as ×109/L. Based on these measurements, we calculated three HDL-adjusted inflammatory indices consistent with published definitions. The NHDLr was defined as neutrophil count (×109/L) divided by HDL cholesterol (mmol/L). Similarly, the LHDLr was calculated as lymphocyte count (×109/L) divided by HDL cholesterol (mmol/L), and the WHDLr as total WBC count (×109/L) divided by HDL cholesterol (mmol/L).
All angiograms were reviewed by two interventional cardiologists who were blinded to clinical and laboratory data. The patency of each bypass graft was evaluated, and SVG occlusion was defined as complete obstruction with TIMI 0 flow or graft stenosis greater than 50%, consistent with the widely adopted Fitzgibbon classification.13 Disagreements between reviewers were resolved by consensus. Inter-observer agreement for identifying SVG occlusion was high, with a kappa coefficient of 0.82, indicating substantial reliability. Patients were categorized according to the presence or absence of at least one occluded SVG. Data were extracted by the study team and cleaned by range and consistency checks prior to analysis; no imputation was performed.
The primary endpoint was the presence of SVG occlusion on angiography. The secondary endpoint was all-cause mortality during follow-up. Survival time was measured from the date of the index angiography to the date of death or last clinical contact. Because the number of events was low and the median survival time was not reached, restricted mean survival time was also evaluated.
Statistical Analysis
The sample size was assessed for adequacy based on the conventional requirement of at least 10 outcome events per predictor variable in logistic regression. With four variables planned for inclusion in the multivariable model, a minimum of 40 SVG occlusion events was required. Mid-term angiographic studies report SVG occlusion rates of approximately 20% within 24 to 60 months after CABG, and our cohort included 72 patients with at least one occluded graft, indicating that the study had sufficient power to evaluate the independent associations of inflammatory indices and operative variables with graft failure.
Data distribution was evaluated using Shapiro–Wilk tests and Q-Q plots. Continuous variables are presented as mean with standard deviation or as median with interquartile range, and were compared using the Student’s t test or the Mann–Whitney U-test as appropriate. Categorical variables were compared using the chi-square test or Fisher exact test. Because HDL-adjusted leukocyte ratios reflect integrated inflammatory and lipid-related pathways, as outlined in the Introduction, the NHDLr, LHDLr and WHDLr were included as candidate inflammatory indices in the statistical analysis.
To identify predictors of SVG occlusion, variables with a p value below 0.10 in univariable analyses and clinically relevant covariates were entered into a multivariable binary logistic regression with backward likelihood ratio selection. To address collinearity, correlation coefficients among leukocyte-based variables and HDL-adjusted ratios were examined, and variables demonstrating strong collinearity were excluded from the multivariable model. Model calibration was evaluated with the Hosmer–Lemeshow test, and discriminative performance was quantified with the area under the receiver operating characteristic curve. Odds ratios were reported with 95% confidence intervals. Missing data were assessed for randomness, and variables with fewer than five percent missing values were handled using complete case analysis. No variable required imputation, and the final multivariable models included only patients with complete data for all covariates.
Long-term all-cause mortality was analyzed from the date of the index coronary angiography using Kaplan-Meier curves, and groups were compared with the Log rank test. Survival analyses were exploratory. Information on post-angiography revascularization procedures, including PCI or repeat CABG, was not collected, and survival findings may therefore be influenced by unmeasured therapeutic decisions. Two-sided p values below 0.05 were considered statistically significant. All analyses were conducted using IBM SPSS Statistics version 31 and RStudio version 2025.05.1.
Results
A total of 190 post-CABG patients were analyzed, of whom 72 had at least one occluded saphenous vein graft and 118 had only patent grafts. The median time from CABG to index angiography for the entire cohort was 40.9 months (IQR 23.5–66.5), and the median follow-up duration from CABG was 98.1 months (IQR 70.7–120.0). Age at surgery, age at angiography, and the interval between procedures were similar in both groups, and conventional cardiovascular risk factors and medication use showed no meaningful differences. Female sex tended to be more frequent in the occluded group (47.9% vs. 33.6%, p = 0.051). Sequential SVG grafting was significantly more common among patients with occlusion (33.3% vs. 11.9%, p < 0.001), while other baseline variables were comparable as shown in Table 1.
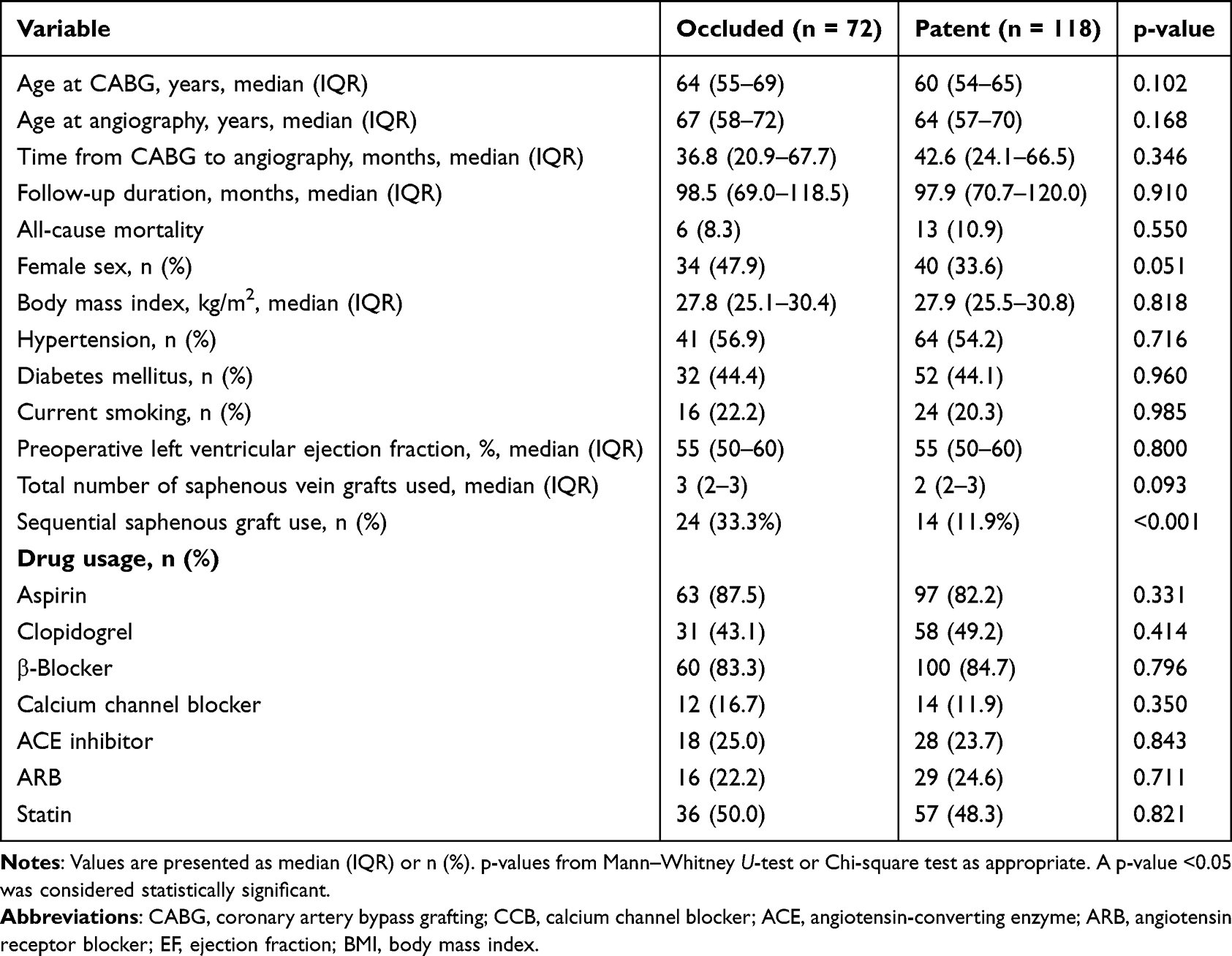 |
Table 1 Baseline Characteristics and Clinical Data of Patients with and without SVG Occlusion |
Laboratory findings are presented in Table 2. Patients with occluded grafts demonstrated significantly higher WBC (8.7 vs. 7.7 × 109/L, p < 0.001), neutrophil counts (5.3 vs. 4.5 × 109/L, p = 0.012), and lymphocyte counts (2.5 vs. 2.2 × 109/L, p = 0.016). HDL-adjusted leukocyte ratios were significantly higher in patients with occlusion, including NHDLr (5.07 vs. 4.41, p = 0.006), LHDLr (2.48 vs. 2.15, p = 0.012), and WHDLr (8.51 vs. 7.56, p = 0.001). Lipid parameters, renal function, electrolytes, and neutrophil to lymphocyte ratio (NLR) did not differ significantly between groups. Graft-level analysis demonstrated the highest SVG occlusion rate in the right coronary artery (RCA) territory (31.1%), followed by circumflex artery-obtuse marginalis 1 (21.8%), whereas left internal mammary artery- left anterior descending artery (LIMA–LAD) grafts had the lowest occlusion rate (9.7%) (Table 3).
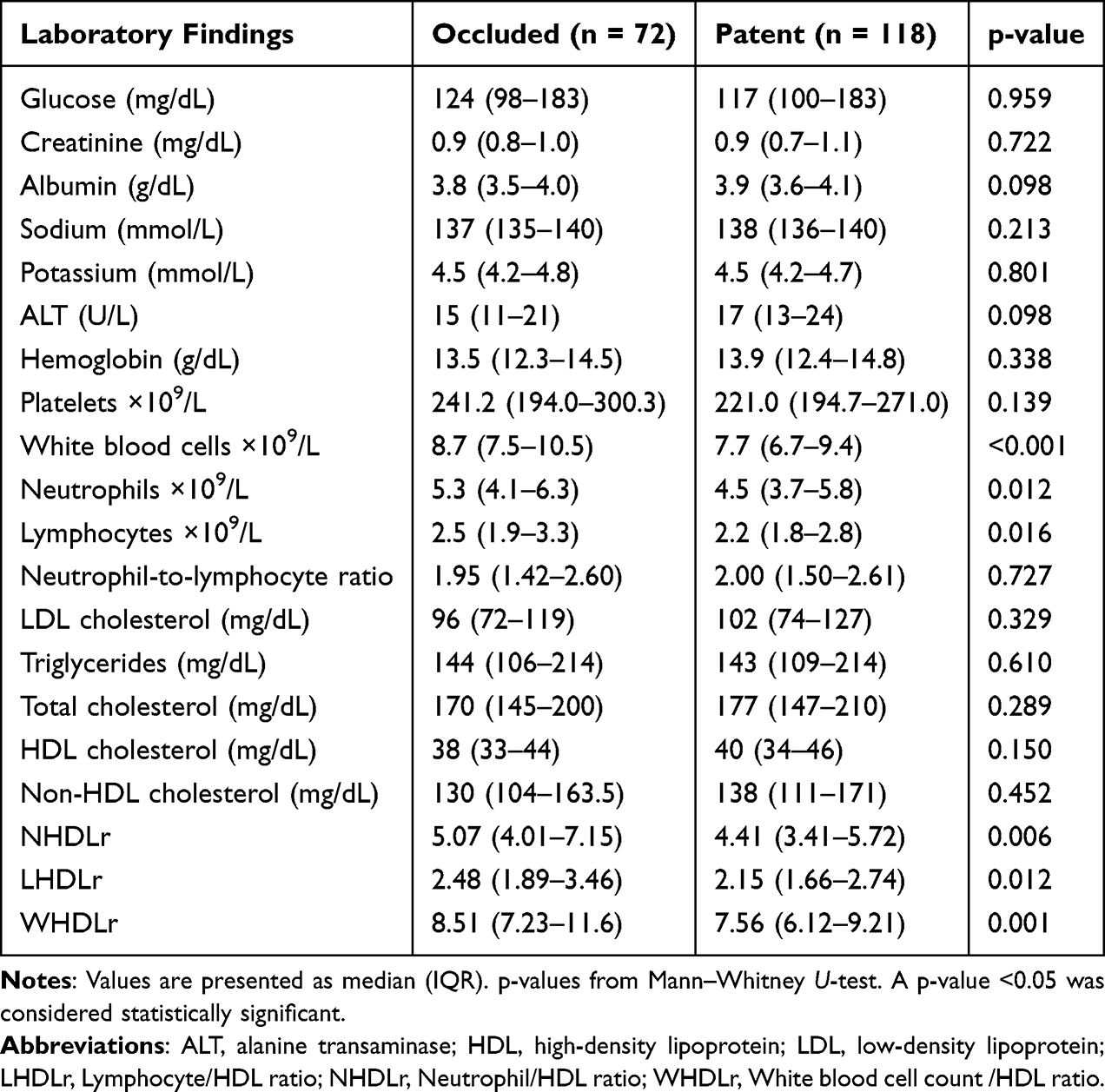 |
Table 2 Laboratory Findings of Patients with and without SVG Occlusion |
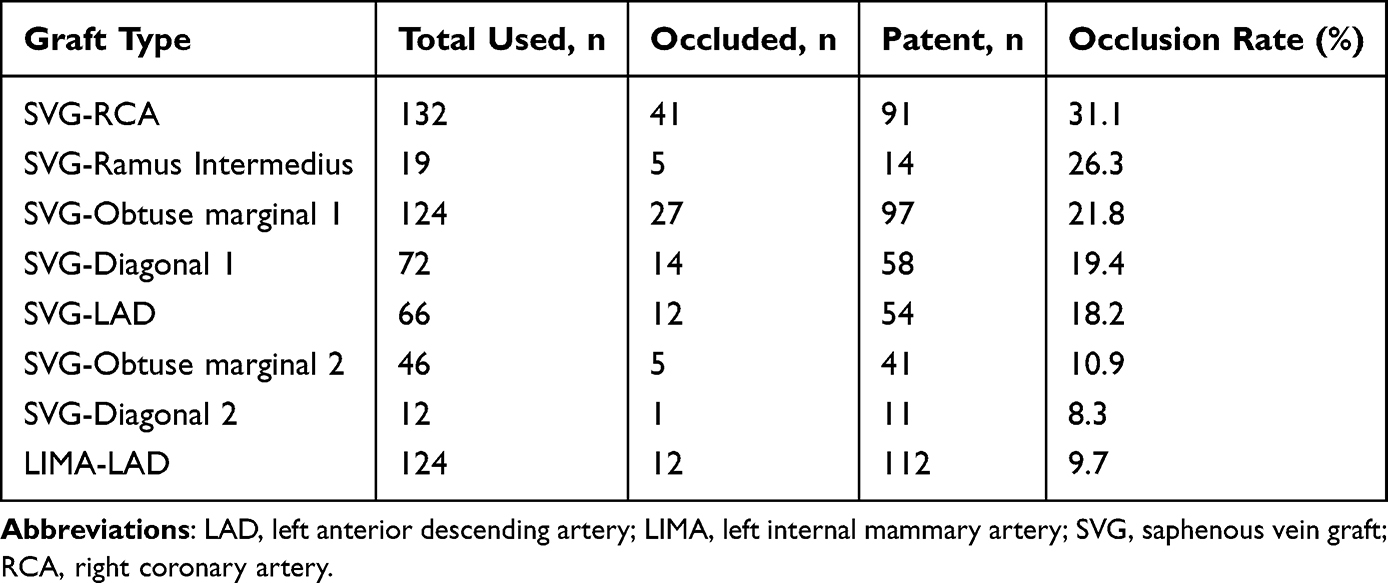 |
Table 3 The Patency Status of Individual Graft Type |
Univariate logistic regression identified several variables associated with SVG occlusion (Table 4). Sequential grafting showed the strongest association (OR 3.71, 95% CI 1.77–7.81), followed by the HDL-based ratios (NHDLr, LHDLr) and leukocyte measures (WBC, neutrophil, lymphocyte counts). Female sex demonstrated a borderline association in univariate analysis, but became a significant independent predictor in the multivariate model. Four variables remained independently associated with SVG occlusion: sequential grafting (adjusted OR 3.58, 95% CI 1.63–7.85), female sex (adjusted OR 2.05, 95% CI 1.06–3.94), NHDLr (adjusted OR 1.18, 95% CI 1.01–1.38), and LHDLr (adjusted OR 1.39, 95% CI 1.04–1.87). WBC, neutrophil count, lymphocyte count, and WHDLr did not enter the multivariate model due to collinearity and absence of additional independent predictive value. The multivariable model demonstrated modest explanatory power (Nagelkerke R2 = 0.087) and acceptable calibration, with a non-significant Hosmer–Lemeshow test (p = 0.46).
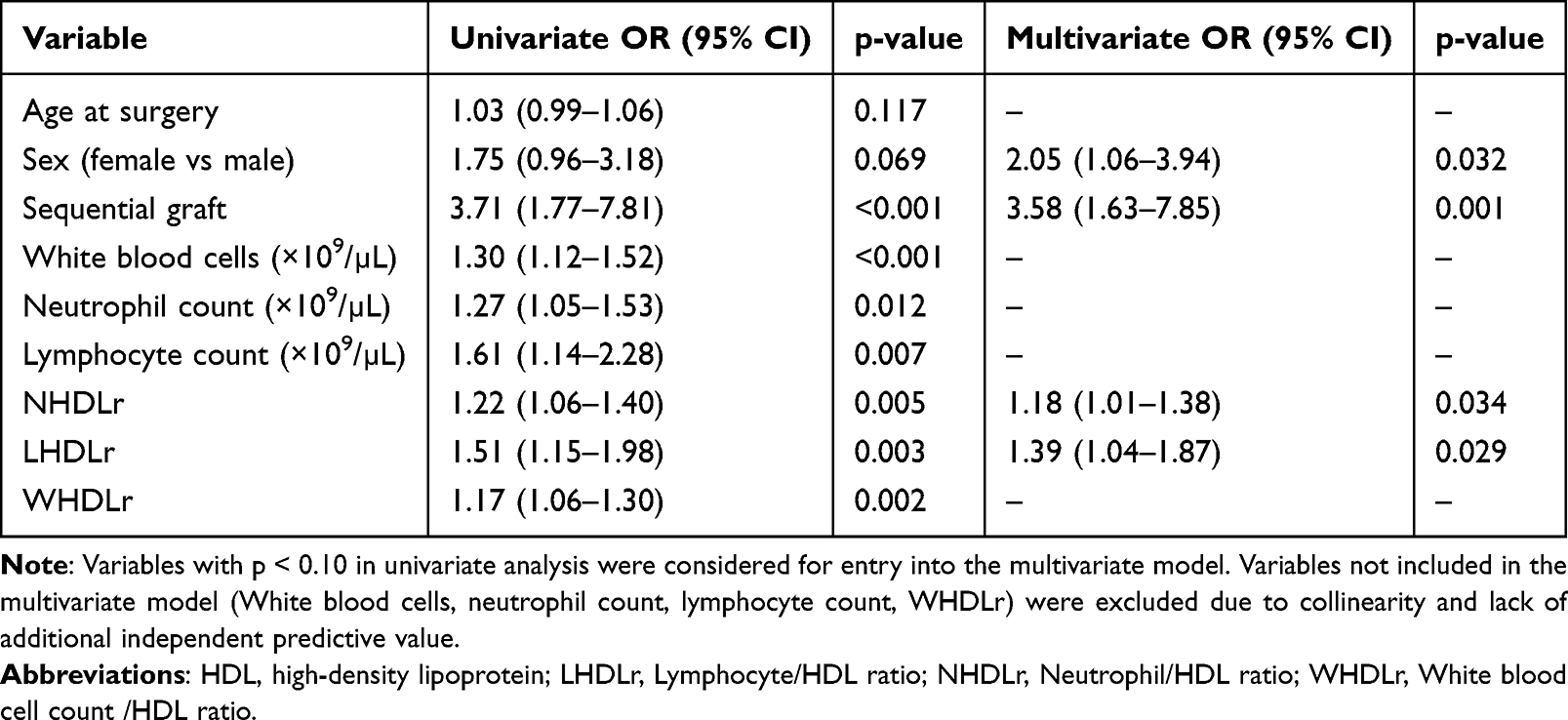 |
Table 4 Univariate and Multivariate Logistic Regression Predictors of SVG Occlusion at Patient Level |
ROC analysis demonstrated modest discriminatory ability for individual predictors. NHDLr, LHDLr, and sequential grafting achieved AUC values between 0.60 and 0.63, whereas female sex provided limited discrimination (AUC 0.57). The combined multivariate model incorporating the four independent predictors significantly improved performance, yielding an AUC of 0.729 (95% CI 0.654–0.804, p<0.001) and clearly outperforming individual predictors (Figure 2).
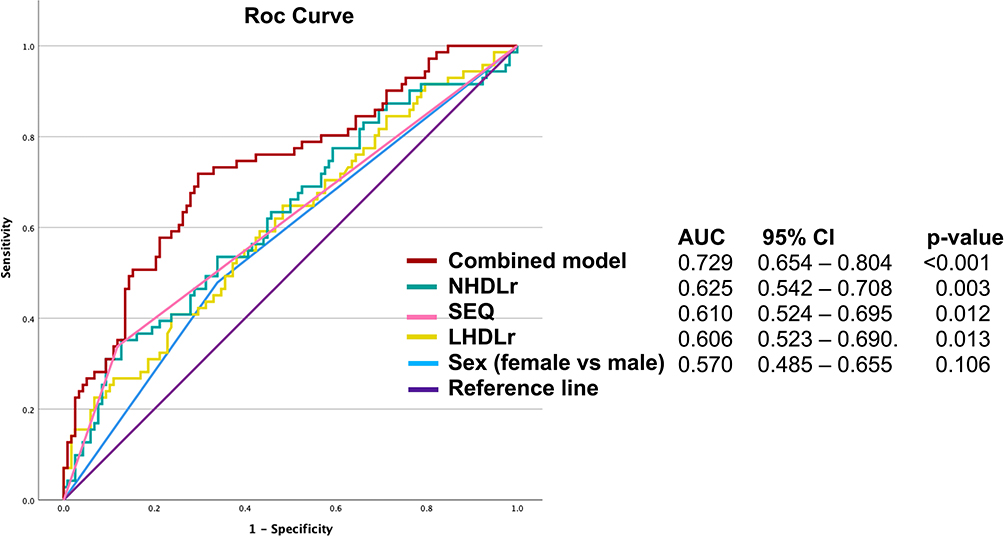 |
Figure 2 ROC curves comparing single inflammatory markers and the combined predictive model for SVG occlusion. |
Kaplan–Meier analysis showed no significant difference in long-term all-cause mortality between patients with occluded and patent SVGs (Figure 3). Median survival was not reached in either group because of low event rates and right-censoring. The restricted mean survival time was 112.8 ± 2.0 months in the patent group and 114.4 ± 2.4 months in the occluded group, with overlapping 95% confidence intervals. Over the follow-up period, mortality occurred in 6 patients (8.3%) with SVG occlusion and 13 patients (10.9%) with patent grafts (Table 1), and the survival curves demonstrated near-complete overlap throughout follow-up. Consistently, the Log rank test showed no statistically significant difference between groups (log-rank χ2 = 0.329, p = 0.566). Given the low number of deaths, these survival findings should be interpreted as exploratory.
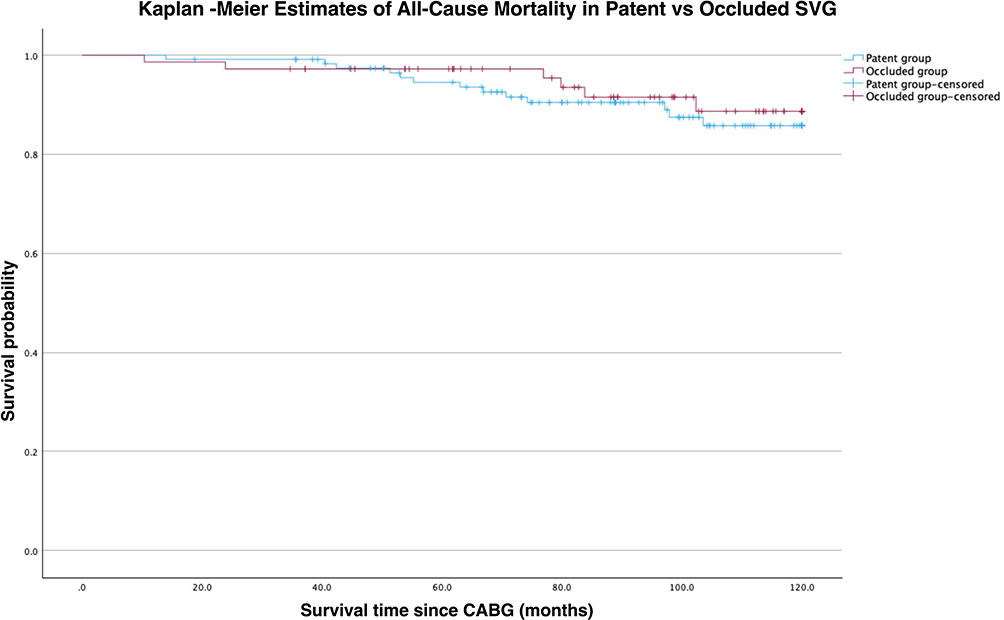 |
Figure 3 Kaplan–Meier survival curves for all-cause mortality according to SVG occlusion status. |
Discussion
In this contemporary post-CABG cohort, we identified two major findings. First, HDL-adjusted inflammatory ratios, particularly the NHDLr and LHDLr, were independently associated with mid-term SVG occlusion. Second, sequential grafting was associated with higher SVG occlusion compared with single-anastomosis grafts, while angiographically confirmed graft occlusion did not translate into higher long-term mortality. Together, these observations highlight the combined influence of systemic inflammation, lipid-immune balance, and surgical flow dynamics on intermediate graft outcomes.
In our cohort, patients with occluded SVGs had higher leukocyte subcomponents, but HDL-adjusted inflammatory ratios showed the most consistent associations with graft occlusion. NHDLr and LHDLr remained independently associated with SVG occlusion, supporting the concept that leukocyte-to-HDL ratios may capture clinically relevant inflammatory burden beyond conventional leukocyte measures. Prior work has proposed leukocyte-to-HDL ratios as inflammatory indicators in native coronary disease settings, with consistent associations reported for NHDLr/NHR and more variable findings for LHDLr/LHR.14 Our findings align with studies linking elevated NHDLr to greater coronary stenosis severity and adverse cardiovascular outcomes7,8,15,16 and with reports associating LHDLr with metabolic-inflammatory stress.17,18 The absence of a significant association with traditional NLR in our cohort is aligned with evidence that NHDLr may outperform NLR for cardiovascular risk prediction.8 An apparent inconsistency is that absolute lymphocyte counts were modestly higher in the occlusion group, whereas lymphopenia has been associated with increased long-term mortality risk in cardiovascular cohorts.19 This likely reflects differences in endpoint and clinical setting, because our outcome was angiographic SVG occlusion in a selected post-CABG population undergoing clinically indicated follow-up angiography with a single timepoint laboratory draw. In multivariable modelling, HDL-adjusted ratios retained independent associations with occlusion, whereas absolute leukocyte components (including lymphocyte count) did not provide incremental independent information once collinearity was considered. In post-CABG angiography cohorts, lymphocyte-based composite indices such as NLR have also been associated with SVG disease,20,21 although these studies evaluate ratios rather than absolute lymphocyte count and use endpoints that differ from our HDL-adjusted indices.
The association of HDL-adjusted ratios with graft occlusion may reflect inflammatory activation in an environment where HDL-mediated vascular protection is attenuated. Experimental and clinical studies suggest that during immune activation HDL can lose vasculoprotective properties, including cholesterol efflux and antioxidative activity, thereby promoting endothelial dysfunction.1,2 In arterialised vein grafts, this may contribute to endothelial injury and downstream pathways that drive intimal hyperplasia and late graft atherosclerosis.22,23 However, HDL functionality (for example cholesterol efflux capacity or antioxidative activity) was not directly measured in this study, so mechanistic inference regarding HDL dysfunction is indirect.
Sequential SVG configuration showed a strong independent association with graft occlusion in our cohort (adjusted OR 3.58). Prior evidence is mixed. A large propensity-matched cohort reported superior patency with sequential SVGs, whereas PREVENT IV found higher 1-year angiographic graft failure (≥75% stenosis) in SVGs with multiple distal targets.11 A meta-analysis also reported differences in perioperative and long-term outcomes between sequential and individual SVG techniques.10 These findings are compatible with hemodynamic explanations whereby disturbed flow and low shear stress in sequential configurations may promote endothelial dysfunction and intimal hyperplasia. However, this is an observational association and should not be interpreted as causal, because sequential grafting may be preferentially used in anatomically complex targets (eg., small or diffusely diseased vessels, poor runoff, competitive flow), and detailed intraoperative flow and anastomotic geometry data were unavailable.
In our cohort, angiographically confirmed SVG occlusion did not translate into higher long-term all-cause mortality, and this finding should be interpreted within the context of contemporary post-CABG management. Effective secondary prevention, including high-intensity statin therapy and antiplatelet treatment, reduces recurrent ischemic events in patients with prior bypass surgery,22,24 and selective repeat revascularization with PCI or redo CABG can further mitigate the clinical impact of graft failure.23 In addition, the near-universal patency of the LIMA to LAD graft in our population provides a form of compensatory graft protection, because a functioning LIMA to LAD remains the major determinant of long-term survival after CABG.25 Together, these factors suggest that while SVG occlusion is an important marker of underlying graft biology and operative technique, its direct influence on mortality may be attenuated in modern practice. This shifts the clinical emphasis from simply detecting SVG occlusion to preventing its downstream consequences, such as recurrent angina or myocardial infarction, through aggressive risk factor modification and timely revascularization when necessary.
Female sex was independently associated with graft occlusion. Women generally have smaller coronary arteries than men, and a size mismatch between a large vein graft and a small target artery may lead to reduced graft flow, predisposing to occlusion and intimal hyperplasia.26,27 The fact that women often have higher HDL levels but still experienced more occlusions in our study suggests that the anatomical disadvantage may outweigh potential metabolic protection in this context.
The HDL-adjusted ratios are derived from routine, inexpensive laboratory tests and may offer a practical tool for risk stratification after CABG. These indices could help identify patients who require intensified surveillance, more aggressive lipid-lowering or consideration of emerging anti-inflammatory therapies. These results also raise the possibility that HDL-adjusted ratios could enhance existing graft risk assessment frameworks, including tools such as the SAFINOUS score for early SVG failure.28 Prospective studies are needed to validate predictive performance, assess incremental value beyond established clinical predictors, and define clinically useful thresholds. Future work should also evaluate whether serial postoperative measurements improve discrimination and whether incorporating HDL functional assays strengthens mechanistic interpretation. Continued refinement of surgical technique and conduit selection remains essential for improving long-term graft durability.29–31
Limitations of the Study
This study has several limitations. First, its retrospective design and inclusion of only clinically indicated follow-up angiography introduce potential verification bias. Second, laboratory values were obtained at a single timepoint, and CRP/hs-CRP and other inflammatory biomarkers were not available, limiting assessment of inflammatory dynamics and biological triangulation. Third, residual confounding is possible because detailed surgical-technical factors (for example conduit/target quality, anastomotic geometry, graft handling, and intraoperative flow assessment) and postoperative medication adherence were not captured. Fourth, survival analyses were exploratory and limited by few deaths, and data on cause-specific mortality and post-angiography management, including repeat revascularization, were unavailable. The multivariable model showed modest explanatory power (Nagelkerke R2=0.087), consistent with the multifactorial nature of SVG failure and the restricted variable set. Finally, external validation was not performed and is needed before clinical application.
Conclusion
In a contemporary post-CABG cohort undergoing clinically indicated follow-up angiography, higher HDL-adjusted inflammatory ratios (NHDLr and LHDLr) and sequential grafting were independently associated with SVG occlusion. Causality cannot be inferred from this retrospective analysis. SVG occlusion was not associated with all-cause mortality, but survival analyses were exploratory and limited by few events. Prospective studies with external validation and broader inflammatory profiling (including hs-CRP) are needed to confirm these associations and define clinically useful risk thresholds.
Abbreviations
AUC, Area under the receiver operating characteristic curve; CABG, Coronary artery bypass grafting; CAG, Coronary angiography; CI, Confidence interval; HDL, High-density lipoprotein; HDL-C, High-density lipoprotein cholesterol; LAD, Left anterior descending artery; LHDLr, Lymphocyte-to-high-density lipoprotein ratio; LIMA, Left internal mammary artery; NHDLr, Neutrophil-to-high-density lipoprotein ratio; NLR, Neutrophil-to-lymphocyte ratio; OR, Odds ratio; PCI, Percutaneous coronary intervention; PNI, Prognostic nutritional index; RCA, Right coronary artery; ROC, Receiver operating characteristic; SVG, Saphenous vein graft; TIMI, Thrombolysis in Myocardial Infarction; WBC, White blood cell; WHDLr, White blood cell-to-high-density lipoprotein ratio.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional data protection policies but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Adıyaman University Non-Interventional Clinical Research Ethics Committee (Decision Date: 16/04/2024, Decision Number: 2024/4-28). The study was conducted in accordance with the Declaration of Helsinki and institutional research ethics guidelines. Informed consent for participation was waived by the Adıyaman University Non-Interventional Clinical Research Ethics Committee (Decision Date: 16/04/2024, Decision Number: 2024/4-28), as this study was conducted using retrospectively collected and fully anonymized data. No individual patient identifiers, images, or personal information are included in the paper.
Author Contributions
Yusuf Hosoglu.: Conceptualization, Methodology, Formal analysis, Writing – original draft.
Ayse Hosoglu: Conceptualization, Methodology, Formal analysis, Writing – original draft.
Veysi Kavalci: Investigation, Data curation, Visualization, Writing – Review & Editing.
Hakan Tibilli: Investigation, Data curation, Writing – review & editing, Supervision.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest.
References
1. Guida GA, Angelini GD. Pathophysiology and mechanisms of saphenous vein graft failure. Braz J Cardiovasc Surg. 2022;37(Spec 1):32–11. doi:10.21470/1678-9741-2022-0133
2. Owens CD, Gasper WJ, Rahman AS, Conte MS. Vein graft failure. J Vasc Surg. 2015;61(1):203–216. doi:10.1016/j.jvs.2013.08.019
3. Song YQ, Xu Y, Guo ZG. Risk factors and possible mechanisms of saphenous vein graft failure after coronary artery bypass surgery. Chin Med J. 2020;133(13):1606–1608. doi:10.1097/CM9.0000000000000872
4. Hall AB, Brilakis ES. Saphenous vein graft failure: seeing the bigger picture. J Thoracic Dis. 2019;11(Suppl 9):S1441–S1444. doi:10.21037/jtd.2019.03.09
5. Khan MO, Tran JS, Zhu H, et al. Low wall shear stress is associated with saphenous vein graft stenosis in patients with coronary artery bypass grafting. J Cardiovasc Transl Res. 2021;14(4):770–781. doi:10.1007/s12265-020-09982-7
6. McQueen LW, Ladak SS, Zakkar M. Acute shear stress and vein graft disease. Int J Biochem Cell Biol. 2022;144:106173. doi:10.1016/j.biocel.2022.106173
7. Chuang SM, Liu SC, Chien MN, Lee CC, Lee YT, Chien KL. Neutrophil-to-High-Density Lipoprotein Ratio (NHR) and Neutrophil-to-Lymphocyte Ratio (NLR) as prognostic biomarkers for incident cardiovascular disease and all-cause mortality: a comparison study. Am J Prev Cardiol. 2024;20:100869. doi:10.1016/j.ajpc.2024.100869
8. Gao J, Lu J, Sha W, et al. Relationship between the neutrophil to high-density lipoprotein cholesterol ratio and severity of coronary artery disease in patients with stable coronary artery disease. Front Cardiovasc Med. 2022;9:1015398. doi:10.3389/fcvm.2022.1015398
9. Wu T, Zheng YY, Xiu WJ, et al. White blood cell counts to high-density lipoprotein cholesterol ratio, as a novel predictor of long-term adverse outcomes in patients after percutaneous coronary intervention: a retrospective cohort study. Front Cardiovasc Med. 2021;8:616896. doi:10.3389/fcvm.2021.616896
10. Jiao H, Li J, Bai Y, Guo Z. Patency and adverse outcomes of sequential vs. individual saphenous vein grafts in coronary artery bypass: a meta-analysis. Systematic Review. Front Cardiovasc Med. 2022;9:944717. doi:10.3389/fcvm.2022.944717
11. Mehta RH, Ferguson TB, Lopes RD, et al. Saphenous vein grafts with multiple versus single distal targets in patients undergoing coronary artery bypass surgery: one-year graft failure and five-year outcomes from the Project of Ex-Vivo Vein Graft Engineering via Transfection (PREVENT) IV trial. Circulation. 2011;124(3):280–288. doi:10.1161/CIRCULATIONAHA.110.991299
12. Park SJ, Kim HJ, Kim JB, et al. Sequential versus individual saphenous vein grafting during coronary arterial bypass surgery. Ann Thorac Surg. 2020;109(4):1165–1173. doi:10.1016/j.athoracsur.2019.07.094
13. Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper GD, Burton JR. Coronary bypass graft fate and patient outcome: angiographic follow-up of 5,065 grafts related to survival and reoperation in 1,388 patients during 25 years. J Am Coll Cardiol. 1996;28(3):616–626. doi:10.1016/0735-1097(96)00206-9
14. Liu M, Liu X, Wei Z, et al. MHR and NHR but not LHR were associated with coronary artery disease in patients with chest pain with controlled LDL-C. J Invest Med. 2022;70(7):1501–1507. doi:10.1136/jim-2021-002314
15. Huang J-B, Chen Y-S, Ji H-Y, et al. Neutrophil to high-density lipoprotein ratio has a superior prognostic value in elderly patients with acute myocardial infarction: a comparison study. Lipids Health Dis. 2020;19(1):59. doi:10.1186/s12944-020-01238-2
16. Kou T, Luo H, Yin L. Relationship between neutrophils to HDL-C ratio and severity of coronary stenosis. BMC Cardiovasc Disord. 2021;21(1):127. doi:10.1186/s12872-020-01771-z
17. Candido FG, da Silva A, Zanirate GA, Oliveira N, Hermsdorff HHM. Lymphocyte to high-density lipoprotein cholesterol ratio is positively associated with pre-diabetes, metabolic syndrome, and non-traditional cardiometabolic risk markers: a cross-sectional study at secondary health care. Inflammation. 2025;48(1):276–287. doi:10.1007/s10753-024-02063-w
18. Kolahi Ahari R, Akbari N, Babaeepoor N, et al. Association of three novel inflammatory markers: lymphocyte to HDL-C ratio, high-sensitivity C-reactive protein to HDL-C ratio and high-sensitivity C-reactive protein to lymphocyte ratio with metabolic syndrome. Endocrinol Diabetes Metab. 2024;7(3):e00479. doi:10.1002/edm2.479
19. Zafrir B, Hussein S, Jaffe R, Barnett-Griness O, Saliba W. Lymphopenia and mortality among patients undergoing coronary angiography: long-term follow-up study. Cardiol J. 2022;29(4):637–646. doi:10.5603/CJ.a2020.0141
20. Doğan M, Akyel A, Cimen T, et al. Relationship between neutrophil-to-lymphocyte ratio and saphenous vein graft disease in patients with coronary bypass. Clin Appl Thromb Hemost. 2015;21(1):25–29. doi:10.1177/1076029613488935
21. Tasoglu I, Turak O, Nazli Y, et al. Preoperative neutrophil-lymphocyte ratio and saphenous vein graft patency after coronary artery bypass grafting. Clin Appl Thromb Hemost. 2014;20(8):819–824. doi:10.1177/1076029613484086
22. de Vries MR, Simons KH, Jukema JW, Braun J, Quax PH. Vein graft failure: from pathophysiology to clinical outcomes. Nat Rev Cardiol. 2016;13(8):451–470. doi:10.1038/nrcardio.2016.76
23. McKavanagh P, Yanagawa B, Zawadowski G, Cheema A. Management and prevention of saphenous vein graft failure: a review. Cardiol Ther. 2017;6(2):203–223. doi:10.1007/s40119-017-0094-6
24. Guida G, Ward AO, Bruno VD, et al. Saphenous vein graft disease, pathophysiology, prevention, and treatment. A review of the literature. J Card Surg. 2020;35(6):1314–1321. doi:10.1111/jocs.14542
25. Goldman S, Zadina K, Moritz T, et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: results from a Department of Veterans Affairs Cooperative Study. J Am Coll Cardiol. 2004;44(11):2149–2156. doi:10.1016/j.jacc.2004.08.064
26. Gaudino M, Sandner S, An KR, et al. Graft failure after coronary artery bypass grafting and its association with patient characteristics and clinical events: a pooled individual patient data analysis of clinical trials with imaging follow-up. Circulation. 2023;148(17):1305–1315. doi:10.1161/CIRCULATIONAHA.123.064090
27. Harik L, An KR, Dimagli A, et al. Choice of conduit for coronary artery bypass grafting: technical, anatomic, and pharmacologic considerations. Vessel Plus. 2023. doi:10.20517/2574-1209.2023.124
28. Antonopoulos AS, Odutayo A, Oikonomou EK, et al. Development of a risk score for early saphenous vein graft failure: an individual patient data meta-analysis. J Thorac Cardiovasc Surg. 2020;160(1):116–127e4. doi:10.1016/j.jtcvs.2019.07.086
29. Gaudino M, Benedetto U, Fremes S, et al. Radial-artery or saphenous-vein grafts in coronary-artery bypass surgery. N Engl J Med. 2018;378(22):2069–2077. doi:10.1056/NEJMoa1716026
30. Deng MX, Lia H, Lee G, et al. Angiographic patency of coronary artery bypass conduits: an updated network meta-analysis of randomized trials. Braz J Cardiovasc Surg. 2022;37(Spec 1):7–31. doi:10.21470/1678-9741-2022-0142
31. Tian M, Wang X, Sun H, et al. No-touch versus conventional vein harvesting techniques at 12 months after coronary artery bypass grafting surgery: multicenter randomized, controlled trial. Circulation. 2021;144(14):1120–1129. doi:10.1161/CIRCULATIONAHA.121.055525
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.