Back to Journals » Cancer Management and Research » Volume 14
HBV Infection Status Indicates Different Risks of Synchronous and Metachronous Liver Metastasis in Colorectal Cancer: A Retrospective Study of 3132 Patients with a 5-Year Follow-Up
Authors Zhou J, Guo X, Huang P, Tan S, Lin R, Zhan H, Wu X, Li T, Huang M, Huang M
Received 9 December 2021
Accepted for publication 20 April 2022
Published 27 April 2022 Volume 2022:14 Pages 1581—1594
DOI https://doi.org/10.2147/CMAR.S350276
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Jiaming Zhou1,2 *, Xiaoyan Guo3 *, Pinzhu Huang1,2 *, Shuyun Tan,1,2 Rongwan Lin,4 Huanmiao Zhan,5 Xiaofeng Wu,6 Tuoyang Li,1,2 Mingzhe Huang,1,2 Meijin Huang1,2
1Department of Colon and Rectum Surgery, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China; 2Guangdong Provincial Key Laboratory of Colorectal and Pelvic Floor Disease, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Infectious Diseases, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China; 4Department of Clinical Laboratory, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China; 5Department of Pathology, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China; 6Department of Medical Records Management, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China
* These authors contributed equally to this work
Correspondence: Meijin Huang, The Sixth Affiliated Hospital of Sun Yat-sen University, No. 26 Yuancun Erheng Road, Tianhe District, Guangzhou, Guangdong, People’s Republic of China, Tel +8613924073322, Fax +8620-38254221, Email [email protected]
Purpose: Previous studies on the effect of hepatitis B virus (HBV) infection on colorectal liver metastasis (CRLM) are contradictory. This study revealed different, more specific impacts of HBV on CRLM.
Patients and Methods: A total of 3132 colorectal cancer patients treated from 2013 to 2015 were analyzed retrospectively and followed up for five years. The patients were divided into three groups: group A (chronic HBV infection, CHB); group B, (occult HBV infection, OHB) and group C (no HBV infection, NHB). The risk factors for CRLM, 5-year overall survival (OS), and liver disease-free survival (LDFS) were analyzed.
Results: A total of 905 patients (28.9%) had CRLM, with poor survival compared to those without CRLM (P < 0.01). The incidence of CRLM was 33.41% (138/413) in group A, 21.63% (138/638) in group B and 30.23% (629/2081) in group C (P < 0.05). Synchronous colorectal cancer liver metastasis (SYN-CRLM) was found in 425 patients (13.57%). CHB increased the risk of SYN-CRLM (P < 0.01), with a worse prognosis (P < 0.05). Metachronous colorectal cancer liver metastasis (MET-CRLM) was found in 480 patients (15.33%). OHB decreased the risk of MET-CRLM after surgery (P = 0.02), with a better 5-year LDFS (P = 0.01). Even without surgery, patients with OHB showed a lower incidence rate of MET-CRLM (P < 0.01).
Conclusion: The incidence of CRLM in this study was approximately 28.9%. Surgery and different HBV infection statuses affected the occurrence of CRLM. Chronic HBV infection increased the risk of SYN-CRLM with poor prognosis. Occult HBV infection reduced the risk of MET-CRLM with better LDFS after surgery.
Keywords: colorectal cancer, liver metastasis, hepatitis B virus, chronic HBV infection, occult HBV infection
Introduction
In recent years, the global incidence of colorectal cancer (CRC) has continued to rise. CRC is the third most common malignant tumor with the second-highest mortality rate.1 In China, the incidence and mortality of CRC are ranked fourth and fifth, respectively.2,3 The majority of CRC patients who died had distant metastasis, and liver metastasis was the most common. Synchronous CRC liver metastasis (SYN-CRLM) was evident in 14–20% of CRC patients at the time of diagnosis.4–6 Nearly 17% of patients without SYN-CRLM suffered from metachronous CRC liver metastasis (MET-CRLM), even after resection of the primary tumor.7,8 According to statistics, the SYN-CRLM rate of CRC in China is approximately 25–30%, and the MET-CRLM rate is approximately 12–21%.
Hepatitis B virus (HBV) infection is the most common chronic liver disease in humans. It is estimated that approximately 2 billion people worldwide have been infected with HBV, and more than 350 million people have chronic hepatitis B (CHB).9 Approximately 120 million people in China are chronic HBV carriers, accounting for approximately one-third of the world’s total population, and 30 million of them have HBV virus replication throughout their life.10,11 Hepatitis B is one of the causes of hepatocellular carcinoma, increasing the risk of intrahepatic metastasis.12–14 In addition, it has been reported that HBV infection also increases the risk of liver metastasis in pancreatic cancer, B-cell lymphoma, and other malignant tumors.15–17
Several previous studies have reported the risk of HBV for CRC liver metastasis, but the findings have differed. Utsunomiya et al suggested that the risk of CRLM is lower in patients with HBV and HCV infections.18 Song et al suggested that HBV replication can reduce the incidence of CRLM.19 Augustin et al and Cai et al reported in a meta-analysis that the risk of liver metastasis in CRC patients with CHB was reduced.20,21 Zhao et al suggested that HBV infection is a good predictor of prognosis after liver metastasis resection.22 However, in recent years, scholars have raised different objections. Huo et al indicated that HBV surface antigen (HBsAg) positivity is an independent risk factor for SYN-CRLM.23 All of the above studies have some limitations. There were no analyses of CRLM in different periods based on different HBV results and HBV infection statuses. At present, there is still a lack of large samples, comprehensive retrospective studies, and studies with support from laboratory data. Therefore, this study reviewed the data of 3132 patients treated at the Sixth Affiliated Hospital of Sun Yat-sen University from 2013 to 2015 and analyzed the relationship between HBV infection and CRLM.
Materials and Methods
Patients
From January 1, 2013, to December 31, 2015, a total of 3914 newly admitted and confirmed CRC patients were analyzed retrospectively. The inclusion criteria were as follows: (1) pathological diagnosis of colorectal adenocarcinoma; (2) no current or previous history of other malignant tumors; (3) no viral coinfection of the liver, except HBV; and (4) absence of drug hepatitis, alcoholic liver disease, fatty liver disease, autoimmune liver disease, and pregnancy with CHB. Patients who died within 30 days after surgery were excluded. Patients without HBV serological markers (HBVM) or liver examination results at the first diagnosis of CRC were excluded. A total of 3132 patients were included in this study; see Figure 1. The study protocol was approved by the Ethics Committee of the Sixth Affiliated Hospital of Sun Yat-sen University (approval number 2020ZSLYEC-101), which waived the requirement for written informed consent due to the retrospective nature of the study. The confidentiality of patient data was guaranteed, as required by the Ethics Committee, and the study was conducted in accordance with the Declaration of Helsinki.
 |
Figure 1 The flow chart of this study. |
Data Collection
The data included sex, age, tumor location, differentiation degree, HBVM and serum HBV-DNA results at first admission, carcinoembryonic antigen (CEA), carbohydrate antigen 19–9 (CA19-9), aspartate aminotransferase (AST), alanine aminotransferase (ALT), fibrosis index based on the four factors (FIB-4), chemotherapy (including neoadjuvant or adjuvant chemotherapy), tumor, node, metastasis (TNM) stage (according to American Joint Committee on Cancer [AJCC], version 7 of CRC), liver disease-free survival (LDFS) and overall survival (OS) during follow-up.
Judgment of CRLM
Variable definitions of synchronous and metachronous CRLM have been reported in the literature. According to the statements from the Expert Group on OncoSurgery management of Liver Metastases group (EGOSLIM), SYN-CRLM should be termed “synchronously detected liver metastases”.24 We diagnosed the intrahepatic nodule as SYN-CRLM at the first diagnosis of CRC and MET-CRLM at any time after that.
In this study, for intrahepatic nodules, after the first diagnosis of CRC, we examined the patient’s radiology images, detected the serum CEA and alpha-fetoprotein (AFP) levels, and performed ultrasound-guided biopsy and pathological diagnosis when necessary. After excluding primary liver cancer, hemangioma, and liver cyst, all of the results were judged by two radiologists who had more than 5 years of experience in specifically diagnosing CRLM.
Judgment of HBV Infection
All patients were tested for HBV using HBVM (five items of hepatitis B) at the first diagnosis of CRC as follows: HBsAg; hepatitis B surface antibody (anti-HBs); hepatitis B e antigen (HBeAg); hepatitis B e antibody (anti-HBe); and hepatitis B core antibody (anti-HBc). We divided patients into three groups: groups A, B, and C. Group A (chronic hepatitis B virus infection, CHB) included patients with HBsAg-positive HBV infection. Group B (occult hepatitis B virus infection, OHB) included patients with HBsAg-negative HBV infection who were positive for anti-HBe or anti-HBc. Group C included patients who were negative for HBVM or were only anti-HBs-positive. Serum HBV-DNA was determined quantitatively by PCR in HBsAg-positive patients included in the study.
Follow-Up
The time between the first diagnosis of CRC and the diagnosis of MET-CRLM was defined as LDFS, and the time between the first diagnosis of CRC and death was defined as OS. CT or B-ultrasound examinations were performed every 6–12 months after the operation. If abnormal nodules in the liver were found, the diagnosis of CRLM was made by contrast-enhanced ultrasonography or MRI. If necessary, a biopsy was performed for pathological diagnosis. The follow-up office of the Sixth Affiliated Hospital of Sun Yat-sen University followed up all patients. We collected and recorded the follow-up data through the patients’ return visit. For the patients who were examined in a local hospital due to living in a remote area, if there was suspected tumor recurrence or progression, the patients were required to return to our hospital for further evaluation.
Statistical Analysis
Categorical variables are shown as the number and percentage of patients. For binary variables, baseline categorical clinical parameters were compared by χ2-test or Fisher’s exact test, and numerical values were compared using Student’s t test. Significant risk factors for SYN-CRLM and MET-CRLM were analyzed by logistic regression analysis. A Log rank test was used to determine OS and LDFS in each group. The hazard ratio (HR) and the corresponding 95% confidence interval (CI) were estimated with a mixed effects Cox regression model. Statistical analysis was performed using SPSS 22 (IBM company) and GraphPad Prism 8. All survival curves were analyzed and displayed using GraphPad Prism 8. A two-tailed P value less than 0.05 was considered significantly different.
Results
Baseline Characteristics
From January 1, 2013, to December 31, 2015, 3914 CRC patients were confirmed to have CRLM in our hospital. A total of 782 patients were excluded because of the lack of HBVM results and the inability to evaluate preoperative liver metastasis. A total of 3132 patients were included in the final analysis, which included 1922 males and 1210 females. The median age was 56 years (±11.17; range from 17 to 95). There were 1526 patients with rectal cancer and 1606 patients with colon cancer. According to the HBVM results, the patients were divided into groups A, B or C. Group A was the CHB group, with a total of 413 (13.19%) patients. Group B was the OHB group, with a total of 638 (20.37%) patients. Group C was the noninfection group, with a total of 2081 (66.44%) patients. A total of 2893 patients underwent surgery for primary tumor resection during their treatment, while the other 239 did not. SYN-CRLM was found in 425 (13.57%) patients at their first diagnosis, while MET-CRLM was found in 483 (15.42%) patients during treatment and follow-up. Among the 2707 patients without SYN-CRLM, 2615 patients underwent surgery, while MET-CRLM occurred in 404 patients. In 92 patients without either SYN-CRLM or surgery, MET-CRLM occurred in 79 patients. CRLM was not found in 2224 (71.01%) patients during follow-up. See Table 1.
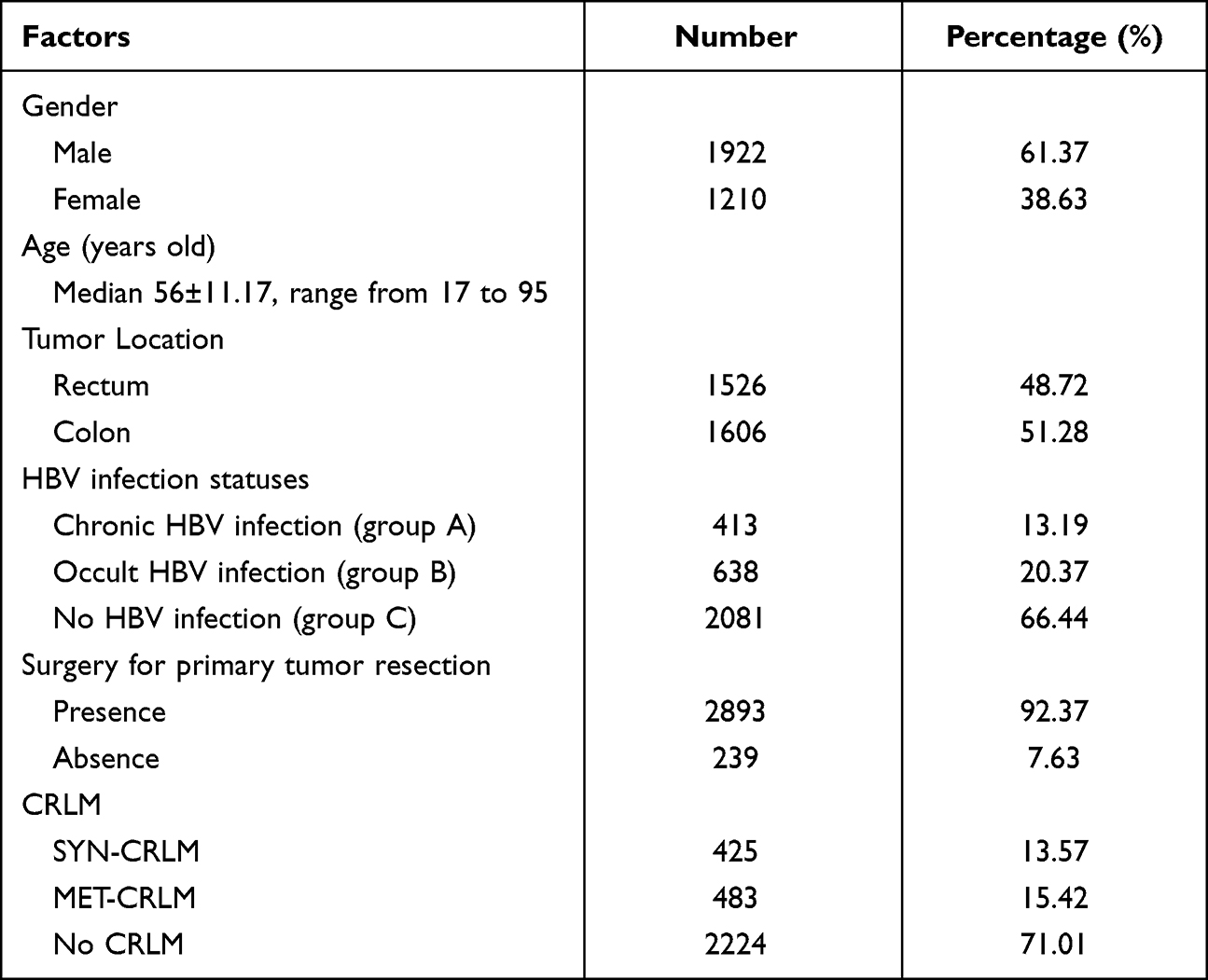 |
Table 1 Baseline Characteristics of Patients |
Differences Between HBV Infection Groups
Among the 3132 patients with CRC (before surgery), a total of 425 (13.56%) patients were found to have SYN-CRLM at the first diagnosis of CRC before surgery. The incidence of SYN-CRLM in groups A, B and C was 16.95% (70/413), 11.60% (74/638) and 13.50 (281/2281), respectively, with a significant difference (P=0.05). The incidence of MET-CRLM in groups A, B and C was 16.46% (68/413), 10.03% (64/638) and 16.72% (348/2081), respectively, with a significant difference (P=0.01). There was a significant difference between group A, group B and group C in sex (P = 0.04) and age (P < 0.01) proportions. The abnormal proportions of AST (P < 0.01), ALT (P < 0.01) and FIB-4 (P < 0.01) in group A were significantly higher than those in groups B and C. The statistical results showed that there was no difference in tumor location, tumor differentiation, T stage, N stage, CEA or CA19-9 in the different HBV infection groups. See Table 2.
 |
Table 2 Difference Between HBV Infection Groups |
Chronic Hepatitis B Virus Infection Increased the Incidence Rate of SYN-CRLM
In multivariate analysis, CHB was an independent risk factor for SYN-CRLM (P < 0.01). Compared with that in CHB, the relative risk of SYN-CRLM in OHB was 0.19 (0.11–0.34), while that in NHB was 0.29 (0.18–0.47). Moreover, the independent risk factors for SYN-CRLM were T stage of 3 or 4 (P<0.01, HR = 3.94 [2.08–7.48]), N stage of 1 or 2 (P<0.01, HR = 1.83 [1.38–2.46]), CEA>5 ng/mL (P<0.01, HR=3.85 [2.84–5.22]), CA19-9>37 U/mL (P<0.01, HR=2.18 [1.59–2.98]), AST>40 (P<0.01, HR=3.85 [2.84–5.22]), and ALT>40 U/L (P<0.01), HR=2.15 [1.49–3.10]). On the other hand, high or moderate differentiation (P=0.01, HR = 0.62 [0.44–0.87]) was an independent protective factor for SYN-CRLM. See Table 3.
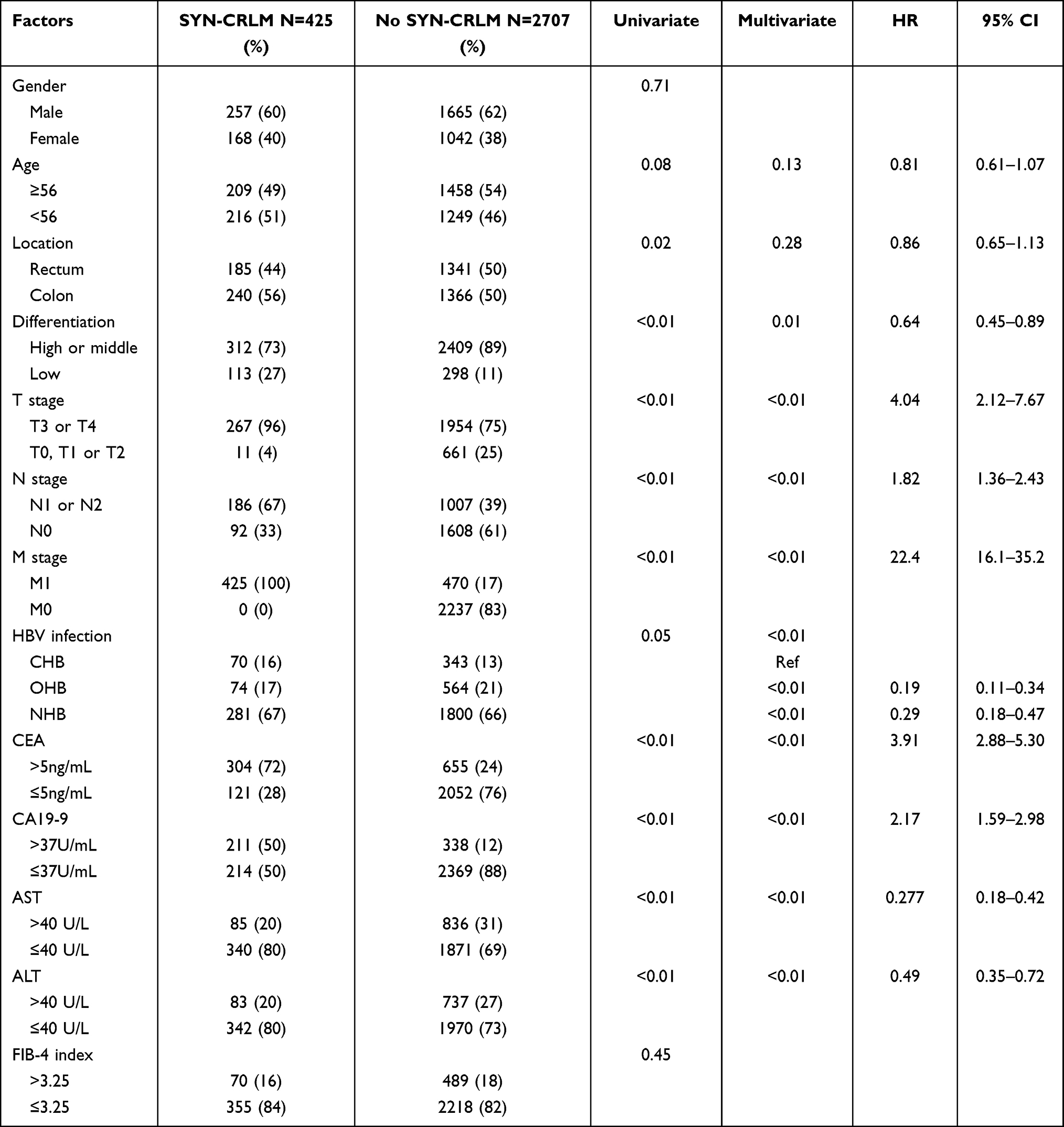 |
Table 3 Risk Factors of SYN-CRLM N=3132 |
Occult Hepatitis B Virus Infection Decreased the Incidence Rate of MET-CRLM
A total of 2615 patients underwent surgery for primary tumor resection and were followed up. Of these patients, 404 developed MET-CRLM, accounting for 15.44% of patients. There were also differences in the HBV infection groups (P=0.02). In contrast to SYN-CRLM, we found that occult HBV infection (group B) decreased the incidence rate of MET-CRLM (relative to CHB, P=0.04, HR= 1.47 (1.02–2.10) and NHB, P<0.01, HR=1.49 (1.14–1.95)) in the Cox regression analysis. Our analysis also showed that better pathological differentiation (P=0.04, HR=0.77 [0.61–0.99]) was an independent protective factor against MET-CRLM. In contrast, the presence of extrahepatic organ metastasis (P<0.01, HR=10.12 [7.90–12.95]), initial CA19-9 level at the first diagnosis of CRC (P<0.01, HR=1.50 [1.19–1.89]) and chemotherapy (P<0.01, HR=3.11 [1.91–5.04]) were independent risk factors. See Table 4.
 |
Table 4 Risk Factors of MET-CRLM After Surgery N=2615 |
After SYN-CRLM was excluded, 92 patients did not undergo surgery because of multiple organ metastasis or refusal of further treatment. MET-CRLM was found in 79 patients, and MET-CRLM was not found in the remaining 13 patients before death. The incidence rate of MET-CRLM in group B was lower than that in groups A and C (P<0.01). See Table 5.
 |
Table 5 Incidence Rate of MET-CRLM in Different HBV Infection Statues without Surgery N=92 |
5-Year OS and LDFS Between Different HBV Infection Statuses
In this study, the follow-up period ended on January 1, 2020. A total of 2985 patients were followed up with a median follow-up time of 43 months (range, 0–73); 147 patients were lost. A total of 666 patients died, and 2319 survived during the follow-up period. The 5-year survival rate was 79.71%. The 5-year survival rates of patients with SYN-CRLM, MET-CRLM and without CRLM were 50.08%, 42.41% and 86.25%, respectively (P<0.001, Figure 2A). The 5-year survival rates of patients with and without surgery were 78.38% and 7.56%, respectively (P<0.001, Figure 2B). The 5-year survival rates of group A, group B and group C were 71.76%, 77.10% and 75.69%, respectively (P=0.049, Figure 2C).
 |
Figure 2 The 5-year overall survival (A) between SYN-CRLM, MET-CRLM and no CRLM; (B) between patients with and without surgery; (C) between CHB, OHB and NHB; (D) between CHB, OHB and NHB in patients with SYN-CRLM; (E) between CHB, OHB and NHB in patients with MET-CRLM; and (F) between CHB, OHB and NHB in patients without CRLM. |
Among 425 patients with SYN-CRLM, the 5-year OS rates of CHB, OHB and NHB were 45.88%, 38.10% and 54.01%, respectively (P=0.12, Figure 2D). Among 480 patients with MET-CRLM, the 5-year survival rates of CHB, OHB and NHB were 42.39%, 39.14% and 43.63%, respectively (P=0.232, Figure 2E). Among 2227 patients without CRLM, the 5-year survival rates of CHB, OHB and NHB were 83.64%, 85.52% and 86.93%, respectively (P = 0.366, Figure 2F).
During the follow-up, among the 2707 patients without SYN-CRLM, a difference in 5-year LDFS was observed between patients with and without surgery (P < 0.001, Figure 3A). Of the 2615 patients who underwent surgery, the MET-CRLM rates of CHB, OHB, and NHB were 16.51% (54/327), 11.53% (64/555), and 16.50% (286/1733), respectively, with a significant difference in the 5-year LDFS (P=0.013, Figure 3B). Of the 92 patients who did not receive surgery, the MET-CRLM rates of CHB, OHB, and NHB were 81.3% (13/16), 44.4% (4/9), and 92.5% (62/69), respectively, with no significant difference in the 5-year LDFS (P=0.119, Figure 3C).
 |
Figure 3 Liver disease-free survival (A) between patients with and without surgery; (B) between CHB, OHB and NHB in patients with surgery; (C) between CHB, OHB and NHB in patients without surgery. |
Relationship Between CRLM and Serum HBV-DNA Level
Among the 413 patients in group A, 344 were tested for serum HBV-DNA levels. In 34 patients with HBV-DNA > 1000 copies/mL, SYN-CRLM was found in 4 patients, and MET-CRLM was found in 5 patients. In 310 patients with HBV-DNA < 1000 copies/mL, SYN-CRLM was found in 49 patients, and MET-CRLM was found in 40 patients. There was no significant correlation between HBV DNA level and CRLM (P=0.81, see Table 6), and there was no significant difference in LDFS and OS. See Figure 4A and 4B.
 |
Table 6 Incidence Rate of CRLM in Different Serum HBV-DNA Copies N=344 |
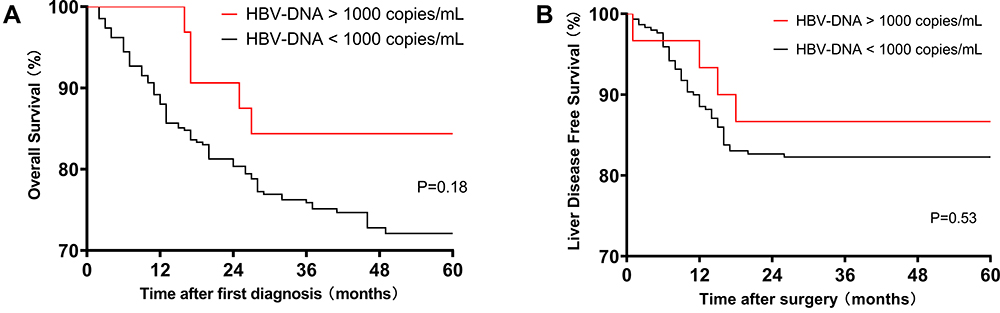 |
Figure 4 (A) The 5-year overall survival and (B) liver disease-free survival between different serum HBV-DNA levels in HBsAg-positive patients. |
Discussion
The liver is the most likely organ and site of CRC metastasis.25 According to the literature, the incidence of SYN-CRLM is 14–20%, and the incidence of MET-CRLM is approximately 17%. At present, there are no reports in the literature on the incidence of CRLM in Chinese CRC patients. Our data suggest that the SYN-CRLM rate is 13.57%, and the MET-CRLM rate is 15.42%, which are the first retrospective cohort study data from China.
A study showed that the occurrence of CRLM is mainly related to CEA level, tumor depth, positive lymph nodes, node metastasis, positive vascular invasion and other factors.26 At present, the “seed soil hypothesis” is considered to be the main mechanism of CRLM.27 According to the hypothesis and the anatomical characteristics of CRC, when cancer cells from the primary sites in the colon escape into the bloodstream, the most likely location where they lodge is the liver. Kelly et al suggested that micrometastasis occurs when cancer cells from the primary CRC escape from the primary location into the portal circulation.28 Even though the liver immune system removes tumor cells at the beginning of metastasis, when a suitable liver immune microenvironment is met, the colonization, replication and proliferation of CRC cells cause CRLM.29 Therefore, exploring the immune environment of the liver is of great significance to prevent CRLM, especially in China, which has the largest number of HBV-infected patients in the world.
HBV infection is the most common liver disease in China. Chronic HBV infection has a complicated course with three phases (immune tolerant phase, immune active phase and inactive phase). In this process, HBsAg is positive, and HBV-DNA can be detected, which represents the replication and reproduction of HBV.30 However, not all people infected with HBV develop CHB, and some people can recover. Among these patients, the long-lasting persistence of HBV genomes in the liver (with detectable or undetectable HBV DNA in the serum) of individuals testing negative for HBsAg is termed occult HBV infection.31 Therefore, according to the HBV infection status, in this study, we divided the patients with CRC into CHB, OHB and NHB for analysis.
SYN-CRLM was found in 425 patients, accounting for 13.57%. The incidence of SYN-CRLM in OHB (P<0.01, HR=0.19, 95% CI (0.10–0.33)) and NHB (P<0.01, HR=0.28, 95% CI (0.17–0.46)) was significantly lower than that in CHB. This finding indicates that the active replication of HBV may increase the risk of SYN-CRLM, which is the same result as that found by Huo et al.23 Before surgery, when the primary tumor continues to enter the liver through blood flow, the consumption of the immune system in the liver is intensified, and the incidence of SYN-CRLM is increased. Similar phenomena were observed in primary liver cancer with HBV infection.32,33 CHB and tumorigenesis have similar immune mechanisms. Peng et al observed the upregulation of the PD-1/PD-L1 pathway in patients with CHB, thereby inhibiting the function and expression of interferon-r (INF-r) and CD8+ T cells, resulting in sustained liver cell damage.34 Previous studies have suggested that the pathogenesis and metastasis of CRC are related to the upregulation of the PD-1/PD-L1 negative regulatory signaling pathway, which leads to immune escape.35–37 Therefore, we believe that in CRC patients with CHB, whose liver immune function is impaired, CRLM is more likely to occur.
MET-CRLM was found in 404 (15.45%) patients after resection of the primary tumor during follow-up. However, unlike the effect on SYN-CRLM, OHB was an independent protective factor relative to CHB and NHB in the Cox regression analysis. The 5-year LDFS rate of OHB was 88.47%, which was significantly better than that of CHB (83.49%) and NHB (83.50%) (P=0.01). This result suggested that the liver’s immune status may reduce the risk of CRLM in patients who do not have HBV replication or have recovered from HBV infection. A number of studies have noted that HBV-related immune function is enhanced in patients recovered from HBV infection, and its antiviral function is better than that of patients with chronic hepatitis B infection. Wu et al noted that PD-1 expression in HBeAg-negative HBV patients was significantly lower than that in HBeAg-positive HBV patients.38 Penna showed that the frequency of HBV-specific T cells in self-limited acute hepatitis B was comparable to that observed in the acute stage of infection and was usually higher than that in patients with chronic HBV infection.39 Zhang et al noted that PD-1 expression was significantly upregulated on HBV-specific CD8 T cells in the early phase of acute HBV infection, and successful viral clearance correlated with a subsequent decrease in PD-1 expression.40 This finding indicates that there may be some immune response related to HBV infection, which enhances the clearance of tumor cells in the liver.
There have been several previous studies on the relationship between HBV and CRLM, but the conclusions are contradictory.23,41–43 None of the above studies considered that HBV infection might have different effects on CRLM before and after surgery, and these studies did not analyze the effects caused by different HBV infection statuses independently. We believe that these differences are why the studies have different conclusions.
It is generally believed that HBV replication activity is high in HBsAg-positive patients whose serum HBV-DNA is more than 1000 copies/mL.44 We also compared the incidence of CRLM, LDFS and OS in HBsAg-positive patients with different serum HBV-DNA levels. The findings suggested that high-level replication of HBV is not directly related to the occurrence of CRLM.
The results showed that chronic HBV infection increased the risk of SYN-CRLM before surgery, probably by damaging hepatocytes and the liver immune system. Occult HBV infection decreased the risk of MET-CRLM after surgery, probably due to a good liver immune response. Compared to previous studies, our results can better explain the relationship between HBV infection and CRLM in the same cohort. However, this study is a single-center retrospective analysis and lacks biopsy tissue evidence. The occurrence of CRLM may be related to the primary tumor, HBV infection status, and liver immunology, but the mechanism remains unknown. Therefore, we will carry out a multicenter prospective observational study in future work, collect complete clinical and experimental data, and further study the mechanism of how HBV infection affects the occurrence of CRLM.
Conclusion
The incidence of CRLM in this study was approximately 28.9%. Surgery and different HBV infection statuses affected the occurrence of CRLM. Chronic HBV infection increased the risk of SYN-CRLM with poor prognosis. Occult HBV infection reduced the risk of MET-CRLM with better LDFS after surgery.
Abbreviations
CRC, colorectal cancer; CRLM, colorectal liver metastasis; SYN-CRLM, synchronous colorectal cancer liver metastasis; MET-CRLM, metachronous colorectal cancer liver metastasis; HBV, hepatitis B virus; HBVM, hepatitis B virus serological marker; HBsAg, hepatitis B virus surface antigen; anti-HBs, hepatitis B surface antibody; HBeAg, hepatitis B e antigen; anti-HBe, hepatitis B e antibody; anti-HBc, hepatitis B core antibody; CHB, chronic hepatitis B virus infection; OHB, occult hepatitis B virus infection; NHB, no hepatitis B virus infection; CEA, carcinoembryonic antigen; CA19-9, carbohydrate antigen 19-9; AST, aspartate aminotransferase; ALT, alanine aminotransferase; FIB-4, fibrosis index based on the four factors; OS, overall survival; LDFS, liver disease-free survival; HR, hazard ratio; CI, confidence interval.
Acknowledgments
This work was supported by the Fundamental Research Funds for the Central Universities (Sun Yat-sen University), National Key Clinical Discipline (No. 17ykpy67).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Chen W, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2014. Chin J Cancer Res. 2018;30(1):1–12. doi:10.21147/j.issn.1000-9604.2018.01.01
3. Xie Y, Shi L, He X, Luo Y. Gastrointestinal cancers in China, the USA, and Europe. Gastroenterol Rep. 2021;9(2):91–104. doi:10.1093/gastro/goab010
4. Adam R. Colorectal cancer with synchronous liver metastases. Br J Surg. 2007;94(2):129–131. doi:10.1002/bjs.5764
5. Rees M, Tekkis PP, Welsh FKS, O’Rourke T, John TG. Evaluation of long-term survival after hepatic resection for metastatic colorectal cancer. Ann Surg. 2008;247(1):125–135. doi:10.1097/SLA.0b013e31815aa2c2
6. Favoriti P, Carbone G, Greco M, Pirozzi F, Pirozzi REM, Corcione F. Worldwide burden of colorectal cancer: a review. Updates Surg. 2016;68(1):7–11. doi:10.1007/s13304-016-0359-y
7. McMillan DC, McArdle CS. Epidemiology of colorectal liver metastases. Surg Oncol. 2007;16(1):3–5. doi:10.1016/j.suronc.2007.04.008
8. Manfredi S, Lepage CM, Hatem C, Coatmeur O, Faivre J, Bouvier A. Epidemiology and management of liver metastases from colorectal cancer. Ann Surg. 2006;244(2):254–259. doi:10.1097/01.sla.0000217629.94941.cf
9. Trepo C, Chan HL, Lok A. Hepatitis B virus infection. Lancet. 2014;384(9959):2053–2063. doi:10.1016/S0140-6736(14)60220-8
10. Tanaka M, Katayama F, Kato H, et al. Hepatitis B and C virus infection and hepatocellular carcinoma in china: a review of epidemiology and control measures. J Epidemiol. 2011;21(6):401–416. doi:10.2188/jea.JE20100190
11. Luo Z, Li L, Ruan B. Impact of the implementation of a vaccination strategy on hepatitis B virus infections in China over a 20-year period. Int J Infect Dis. 2012;16(2):e82–e88. doi:10.1016/j.ijid.2011.10.009
12. Bréchot C, Gozuacik D, Murakami Y, Paterlini-Bréchot P Molecular bases for the development of hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC). Semin Cancer Biol. 2000;10(3):211–231. 10.1006/scbi.2000.0321
13. Chuang S, Vecchia CL, Boffetta P. Liver cancer: descriptive epidemiology and risk factors other than HBV and HCV infection. Cancer Lett. 2009;286(1):9–14. doi:10.1016/j.canlet.2008.10.040
14. Levrero M, Zucman-Rossi J. Mechanisms of HBV-induced hepatocellular carcinoma. J Hepatol. 2016;64(1,Supplement):S84–S101. doi:10.1016/j.jhep.2016.02.021
15. Luo G, Hao N, Hu C, et al. HBV infection increases the risk of pancreatic cancer: a meta-analysis. Cancer Cause Control. 2013;24(3):529–537. doi:10.1007/s10552-012-0144-2
16. Wei XL, Qiu MZ, Chen WW, et al. The status of HBV infection influences metastatic pattern and survival in Chinese patients with pancreatic cancer. J Transl Med. 2013;11(1):249. doi:10.1186/1479-5876-11-249
17. Zhou X, Pan H, Yang P, Ye P, Cao H, Zhou H. Both chronic HBV infection and naturally acquired HBV immunity confer increased risks of B-cell non-Hodgkin lymphoma. BMC Cancer. 2019;19(1). doi:10.1186/s12885-019-5718-x
18. Utsunomiya T, Saitsu H, Saku M, et al. Rare occurrence of colorectal cancer metastasis in livers infected with Hepatitis B or C virus. Am J Surg. 1999;177(4):279–281. doi:10.1016/S0002-9610(99)00045-8
19. Song E, Chen J, Ou Q, Su F. Rare occurrence of metastatic colorectal cancers in livers with replicative hepatitis B infection. Am J Surg. 2001;181(6):529–533. doi:10.1016/S0002-9610(01)00634-1
20. Augustin G, Bruketa T, Korolija D, Milosevic M. Lower incidence of hepatic metastases of colorectal cancer in patients with chronic liver diseases: meta-analysis. Hepatogastroenterology. 2013;60(125):1164–1168. doi:10.5754/hge11561
21. Cai B, Liao K, Song XQ, Wei WY, Zhuang Y, Zhang S. Patients with chronically diseased livers have lower incidence of colorectal liver metastases: a meta-analysis. PLoS One. 2014;9(9):e108618. doi:10.1371/journal.pone.0108618
22. Zhao Y, Lin J, Peng J, et al. Hepatitis B virus infection predicts better survival in patients with colorectal liver-only metastases undergoing liver resection. J Cancer. 2018;9(9):1560–1567. doi:10.7150/jca.24544
23. Huo T, Cao J, Tian Y, et al. Effect of concomitant positive hepatitis B surface antigen on the risk of liver metastasis: a retrospective clinical study of 4033 consecutive cases of newly diagnosed colorectal cancer. Clin Infect Dis. 2018;66(12):1948–1952. doi:10.1093/cid/cix1118
24. Kow AWC. Hepatic metastasis from colorectal cancer. J Gastrointest Oncol. 2019;10(6):1274–1298. doi:10.21037/jgo.2019.08.06
25. Engstrand J, Nilsson H, Strömberg C, Jonas E, Freedman J. Colorectal cancer liver metastases – a population-based study on incidence, management and survival. BMC Cancer. 2018;18(1). doi:10.1186/s12885-017-3925-x
26. Chuang S, Su Y, Lu C, et al. Risk factors for the development of metachronous liver metastasis in colorectal cancer patients after curative resection. World J Surg. 2011;35(2):424–429. doi:10.1007/s00268-010-0881-x
27. Fidler IJ. The pathogenesis of cancer metastasis: the ‘seed and soil’ hypothesis revisited. Nat Rev Cancer. 2003;3(6):453–458. doi:10.1038/nrc1098
28. Kelly RJ, Kemeny NE, Leonard GD. Current strategies using hepatic arterial infusion chemotherapy for the treatment of colorectal cancer. Clin Colorectal Cancer. 2005;5(3):166–174. doi:10.3816/CCC.2005.n.027
29. Pancione M, Giordano G, Remo A, et al. Immune escape mechanisms in colorectal cancer pathogenesis and liver metastasis. J Immunol Res. 2014;2014:1–11. doi:10.1155/2014/686879
30. McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009;49(5 Suppl):S45–S55. doi:10.1002/hep.22898
31. Raimondo G, Caccamo G, Filomia R, Pollicino T. Occult HBV infection. Semin Immunopathol. 2013;35(1):39–52. doi:10.1007/s00281-012-0327-7
32. Liu X, Li M, Wang X, et al. PD-1+ TIGIT+ CD8+ T cells are associated with pathogenesis and progression of patients with hepatitis B virus-related hepatocellular carcinoma. Cancer Immunol Immunother. 2019;68(12):2041–2054. doi:10.1007/s00262-019-02426-5
33. Li Z, Li N, Li F, et al. Genetic polymorphisms of immune checkpoint proteins PD-1 and TIM-3 are associated with survival of patients with hepatitis B virus-related hepatocellular carcinoma. Oncotarget. 2016;7(18):26168–26180. doi:10.18632/oncotarget.8435
34. Peng G, Li S, Wu W, Tan X, Chen Y, Chen Z. PD-1 upregulation is associated with HBV-specific T cell dysfunction in chronic hepatitis B patients. Mol Immunol. 2008;45(4):963–970. doi:10.1016/j.molimm.2007.07.038
35. Kuai W, Xu X, Yan J, et al. Prognostic impact of PD-1 and Tim-3 expression in tumor tissue in stage I–III colorectal cancer. Biomed Res Int. 2020;2020:5294043. doi:10.1155/2020/5294043
36. Goltz D, Gevensleben H, Dietrich J, Dietrich D. PD-L1 (CD274) promoter methylation predicts survival in colorectal cancer patients. Oncoimmunology. 2017;6(1):e1257454. doi:10.1080/2162402X.2016.1257454
37. Chang Y, Ignatova D, Kollmann D, et al. 494 PD1-positive tumor-infiltrating lymphocytes are associated with poor clinical outcome after pulmonary metastasectomy for colorectal cancer. J Invest Dermatol. 2018;138(5,Supplement):S84. doi:10.1016/j.jid.2018.03.501
38. Wu J, Hsu H, Ni Y, Chen H, Wu T, Chang M. Suppression of furin by interferon-γ and the impact on hepatitis B virus antigen biosynthesis in human hepatocytes. Am J Pathol. 2012;181(1):19–25. doi:10.1016/j.ajpath.2012.03.036
39. Penna A, Artini M, Cavalli A, et al. Long-lasting memory T cell responses following self-limited acute hepatitis B. J Clin Invest. 1996;98(5):1185–1194. doi:10.1172/JCI118902
40. Zhang Z, Zhang JY, Wherry EJ, et al. Dynamic programmed death 1 expression by virus-specific CD8 T cells correlates with the outcome of acute hepatitis B. Gastroenterology. 2008;134(7):1938–1949. doi:10.1053/j.gastro.2008.03.037
41. Qiu H. HBV infection decreases risk of liver metastasis in patients with colorectal cancer: a cohort study. World J Gastroenterol. 2011;17(6):804. doi:10.3748/wjg.v17.i6.804
42. Li DG, Castaing M, Ferlito F, Minutolo V, Di Cataldo A, Puleo S. Rare hepatic metastases of colorectal cancer in livers with symptomatic HBV and HCV hepatitis. Ann Ital Chir. 2013;84(3):323–327.
43. Wang FS, Shao ZG, Zhang JL, Liu YF. Colorectal liver metastases rarely occur in patients with chronic hepatitis virus infection. Hepatogastroenterology. 2012;59(117):1390–1392. doi:10.5754/hge11747
44. Nabuco LC, Villela-Nogueira CA, Perez RM, et al. HBV-DNA levels in HBsAg-positive blood donors and its relationship with liver histology. J Clin Gastroenterol. 2007;41(2):194–198. doi:10.1097/01.mcg.0000225575.73385.2b
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.