Back to Journals » Cancer Management and Research » Volume 18

Haploidentical Allogeneic Cell Transplantation in Relapsed/Refractory Multiple Myeloma
Authors Frimmel J ![]() , Morgner A, Brogsitter C, Trautmann-Grill K, Kunadt D, Teipel R, Röllig C, Hänel M, Schetelig J, Stölzel F
, Morgner A, Brogsitter C, Trautmann-Grill K, Kunadt D, Teipel R, Röllig C, Hänel M, Schetelig J, Stölzel F ![]() , Bornhäuser M
, Bornhäuser M ![]()
Received 1 September 2025
Accepted for publication 14 January 2026
Published 4 February 2026 Volume 2026:18 564588
DOI https://doi.org/10.2147/CMAR.S564588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bilikere Dwarakanath
Julia Frimmel,1 Anke Morgner,2 Claudia Brogsitter,3 Karolin Trautmann-Grill,4 Desiree Kunadt,4 Raphael Teipel,4 Christoph Röllig,4 Mathias Hänel,2 Johannes Schetelig,4,5 Friedrich Stölzel,1,6 Martin Bornhäuser4,7,8
1Division of Stem Cell Transplantation and Cellular Immunotherapies, Department of Internal Medicine II, University Hospital Schleswig Holstein, University Kiel, Kiel, Germany; 2Department for Internal Medicine II, Klinikum Chemnitz, Chemnitz, Germany; 3Department of Nuclear Medicine, University Hospital Dresden, University Dresden, Dresden, Germany; 4Department of Internal Medicine I, University Hospital Dresden, University Dresden, Dresden, Germany; 5DKMS Clinical Trials Unit, Dresden, Germany; 6Faculty of Medicine Dresden, University Dresden, Dresden, Germany; 7German Cancer Consortium (DKTK) Partner Site Dresden, Dresden, Germany; German Cancer Research Center (DKFZ), Heidelberg, Germany; 8National Center for Tumor Diseases (NCT) Dresden, Dresden, Germany
Correspondence: Julia Frimmel, Rosalind-Franklin-Straße 12, Kiel, 24105, Germany, Email [email protected]
Purpose: Although emerging therapies for multiple myeloma (MM) have improved treatment options, long-term disease control in relapsed/refractory (r/r) MM remains a challenge. While the effect of natural killer cell alloreactivity in haploidentical allogeneic hematopoietic cell transplantation (HCT) with post-transplantation cyclophosphamide (PTCy) as graft-versus-host disease (GvHD) prophylaxis is considered a standard treatment option for several hematologic neoplasms, its use in MM is controversial. In this retrospective analysis, we evaluated a small cohort of consecutive patients with MM who underwent haploidentical allogeneic HCT with PTCy.
Patients and Methods: With a median follow-up of 68 months (range, 2– 109 months), seven consecutive patients with r/r MM underwent haploidentical HCT. All were heavily pre-treated, having received proteasome inhibitors, anti-CD38 antibody, immunomodulatory drugs, and at least one autologous HCT. Three patients received a chemotherapy-based reduced-intensity conditioning regimen combined with radioimmunotherapy. GvHD prophylaxis in all patients consisted of PTCy in combination with tacrolimus and mycophenolate mofetil.
Results: All patients showed stable engraftment with complete donor chimerism. Haploidentical HCT resulted in initial response in all patients, with four patients achieving a complete remission (CR) and three a very good remission (VGPR) at first disease assessment post- HCT. All individuals surviving beyond day +100 experienced disease relapse or progression. Among the six surviving patients median time to relapse was 26.5 months (range, 5– 81 months). At last follow-up, four of five surviving patients maintained a CR, while one patient remained in a very good partial remission, all following subsequent individualized therapies. Acute GvHD grades III–IV were observed in two patients, while four developed mild-to-moderate chronic GvHD, with no GvHD-related deaths at the last follow-up.
Conclusion: In this small, selected cohort, haploidentical allogeneic HCT with individualized pre-treatment and conditioning regimens was associated with disease control in heavily pretreated patients with r/r MM.
Keywords: haploidentical transplantation, multiple myeloma, PTCy, cyclophosphamide
Introduction
The outcome of patients with multiple myeloma (MM) has improved significantly in recent years due to new treatment options, such as proteasome inhibitors, anti-CD38 antibody treatment, and immunomodulation.1,2 Furthermore, bispecific antibodies and chimeric antigen receptor (CAR) T-cell therapies are now widely available and represent highly effective, well-established immunotherapeutic options. They have become integral to the treatment algorithm for r/r MM and are increasingly being incorporated into earlier lines of therapy.3,4 However, especially in multiple relapsed or refractory (r/r) situations with increased resistant tumor biology, it is still challenging to achieve disease control.2 In this setting, particularly in younger patients, allogeneic HCT may be considered a therapeutic option for selected patients aiming to achieve sustained remission.3 The observation of prolonged remissions in heavily pretreated patients has led to the assumption of a graft-versus-myeloma effect, suggesting a potential for long- term disease control or even cure in some cases.5,6 At the same time, these studies have documented high rates of treatment-related mortality while these therapeutic modality carries additional risks, including the development of secondary malignancies, which continue to render this approach controversial.5–8 Due to recent advances in the field of allogeneic HCT with improved supportive measures, the introduction of a broader range of conditioning protocols and adaption of several regimens inducing alloreactivity, thus preserving effective graft-versus-tumor effectivity and reducing graft-versus-host disease, transplantation-associated mortality, and non-relapse associated mortality has been reduced.9–11 In the absence of a well-matched donor, the use of post-transplantation cyclophosphamide (PTCy) in haploidentical allogeneic HCT, thus lowering the incidence of GvHD while preserving graft-versus-tumor effects, is undisputed.12,13 However, the use of haploidentical allogeneic HCT in MM in general, especially in the absence of a well-matched donor, and in r/r patients has been a matter of ongoing debate.5,6,14 Therefore, we aimed to report our experience by retrospectively analyzing a small consecutive cohort of selected, yet heavily pretreated patients with r/r MM who underwent haploidentical allogeneic HCT with PTCy in order to evaluate the feasibility of this approach in this patient population and to assess whether PTCy can be used without abrogating the graft-versus-myeloma effect.
Patients and Methods
This study is a small retrospective, single-center analysis of all consecutive patients with MM who were undergoing haploidentical HCT in our center between January 2015 and February 2019. At the time of treatment, CAR-T cell therapies and bispecific antibodies were not yet available outside of clinical trials for patients with multiple myeloma. All individuals fulfilled the eligibility criteria regarding organ function to undergo allogeneic HCT. Due to the unavailability of a matched donor in all cases, haploidentical transplantation was pursued as an alternative donor strategy. The response to treatment was assessed in accordance with the International Myeloma Working Group response criteria.15,16 Relapse was defined as increase of serum paraprotein or occurrence of extramedullary disease. OS was calculated as time from allogeneic HCT to death from any cause. Patients were extensively pretreated (including at least one autologous HCT after high-dose therapy) before haploidentical HCT (Table S1 in the Supplementary Appendix). All patients received salvage therapy prior to haploidentical HCT to be preferentially transplanted in complete remission (CR, n = 2) or very good partial remission (VGPR, n = 3), as with one patient undergoing allogenic HCT in partial remission (PR). In another case, only stable disease (SD) was achieved prior to haploidentical transplantation. Patients received RIC conditioning with fludarabine/melphalan (one patient with one autologous HCT with melphalan-based conditioning), fludarabine/treosulfan (n = 5 patients with two autologous HCTs with melphalan-based conditioning), or fludarabine/cyclophosphamide/TBI 2 Gy for one patient deemed for non-myeloablative conditioning. Three patients were additionally offered and supplemented with Re-188-anti CD66 radioimmunotherapy after exclusion of contraindications (ie, grade 2 or higher chronic renal insufficiency).17 All patients received PTCy-based GvHD prophylaxis with 50 mg/kg on days +3/+4 in conjunction with tacrolimus and mycophenolate mofetil (MMF), both commencing on day +5 after haploidentical HCT. This regimen was applied as described by Luznik et al13 and has been established for GvHD prophylaxis in the haploidentical transplant setting.18,19 The details of patient characteristics are listed in Table 1. All patients provided written informed consent, and the study was approved by the Ethics Committee of the TU Dresden (EK98032010) in accordance with the Declaration of Helsinki.
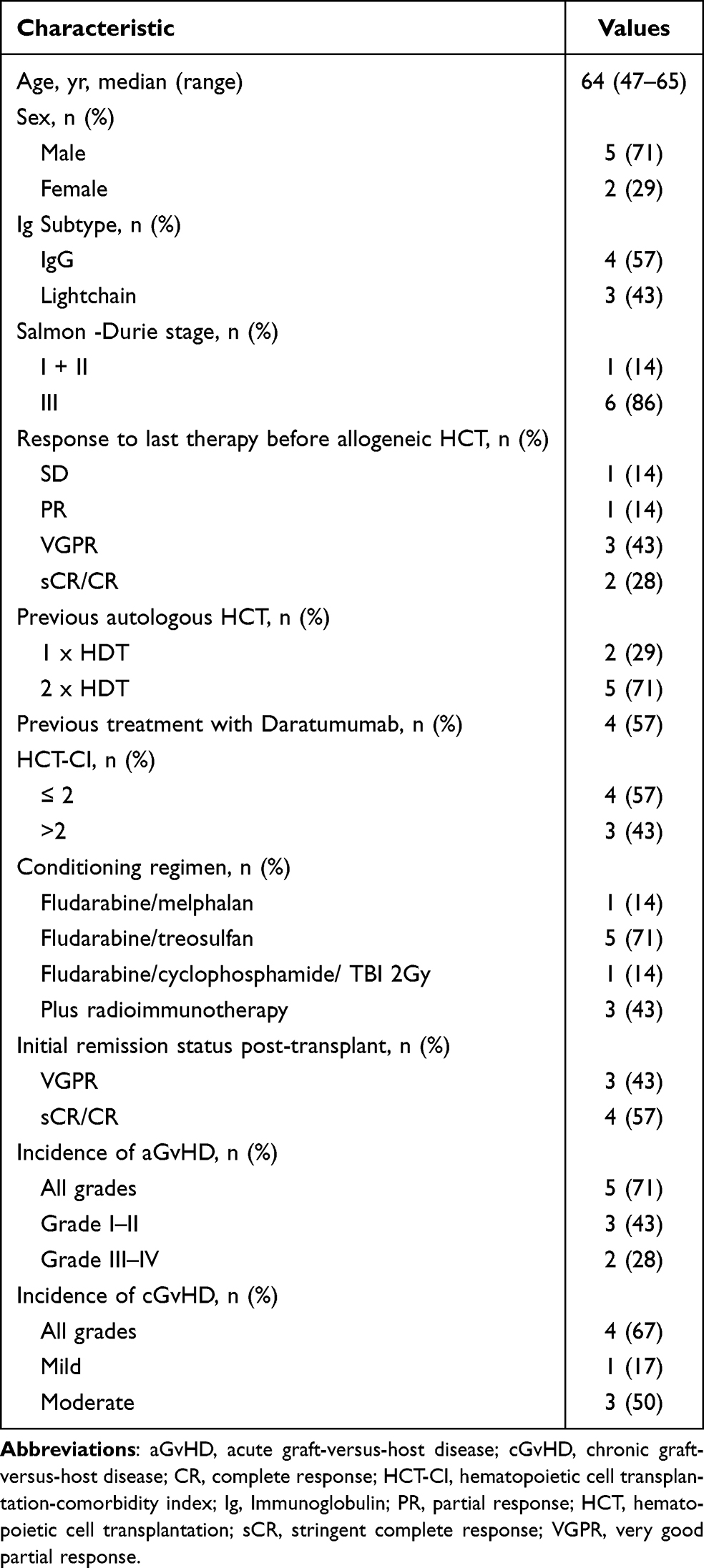 |
Table 1 Patients Characteristics |
Results
The median duration of follow-up for the entire cohort was 68 months (range, 2–109 months), while the median follow-up among surviving patients was 70 months (range, 60–109 months). The median time to reach > 500/µL neutrophils was 19 days (range, 17–28 days) and the median time to platelet engraftment (> 50 GPT/L) was 44 days (range, 12–71 days). All patients had a complete donor chimerism of > 95% within day +20 after allogeneic HCT. The treatment, survival, and response data are shown in Figure 1. The five-year overall survival was 71%. One patient died after successful engraftment and was discharged on day +64 due to Clostridiodes difficile associated enterocolitis with subsequent septic multiorgan failure, resulting in a treatment-related mortality rate of 14%. The overall incidence of aGvHD was 71% (five out of seven patients). Severe aGvHD (grades 3–4) occurred in 28% (two out of seven patients) of the treated patients. The overall incidence of cGvHD was 67% (four out of seven patients). Moderate cGvHD occurred in 50% (three out of six surviving patients) of the patients, while one patient had only mild symptomatic cGvHD. No GvHD-associated deaths occurred during the last follow-up.
 |
Figure 1 Time to progression and OS of patients after haploidentical HCT. Boxes indicate pre-transplant therapy with daratumumab (red), combination with radioimmunotherapy (RIT) as part of conditioning therapy (blue). Arrows: therapy after relapse; pomalidomide (pom); dexamethasone (dex); ixazomib (ixa); lenalidomide (len); daratumumab (dara); carfilzomib (car); cyclophosphamide (cyclo). Last response at last follow-up is depicted as complete remission (CR), stringent complete remission (sCR) or very good partial remission (VGPR) at the end of each bar. |
At first disease assessment following haploidentical transplantation, four of the seven patients achieved a complete remission (CR), while the remaining three achieves a very good partial remission (VGPR). Despite these initial remission rates, all patients who survived beyond day + 100 post- allogeneic HCT experienced disease progression or relapse. Among the six surviving patients median time to relapse after allogeneic HCT was 26.5 months (range, 5–81 months). Four patients (67%) remained free of disease progression at two years after haploidentical HCT and two patients (33%) maintained remission beyond four years. Subsequent treatment was administered on an individual basis according to physicians’ choice, resulting at last follow-up in a CR in four of the five surviving patients and VGPR in one. UPN1 showed progression of MM 29 months after haploidentical HCT. The patient was initially treated with carfilzomib/dexamethasone and subsequently with lenalidomide/daratumumab/dexamethasone and currently has an sCR of 81 months after progression and reinitiation of therapy. UPN5 had disease progression at 24.5 months after haploidentical HCT and received treatment with daratumumab/lenalidomide/dexamethasone for 18 months, which achieved a VGPR as the best response after an intolerable single cycle of pomalidomide/daratumumab/dexamethasone. After evidence of disease progression, the patient was treated with teclistamab, which was switched to talquetamab owing to poor tolerability. Durable and ongoing CR was achieved using this therapy. UPN6 received a single cycle of pomalidomide/cyclophosphamide/dexamethasone and is currently 50 months in sCR at the last follow-up. UPN7 underwent haploidentical HCT with SD and VGPR. After 4.8 months, the patient relapsed, was treated with pomalidomide/dexamethasone/carfilzomib, and achieved a PR. He died of disease progression on day +382 after haploidentical HCT. Two patients were diagnosed with cutaneous basal cell carcinoma as a secondary malignancy during follow-up.
Discussion
The present study demonstrated that haploidentical HCT can induce long-term disease control in a small cohort of heavily pretreated and selected patients with r/r MM.
Although the number of patients analyzed is limited, the observation that the majority achieved a CR, a well-established prognostic factor for long-term survival,20,21 is notable A recent analysis of a comparable, though larger, cohort of relapsed/refractory MM patients reported a median PFS of 13 months and a median OS of 51.4 months.22 Another small retrospective single-center study described a cohort of MM patients who underwent allogeneic HCT from HLA-matched sibling donors, reporting a median OS of 6.7 years and a 5-year OS of 62.5%. Among the patients who relapsed, the median time to relapse was 3.64 years (range, 0.21–9.33 years).23 Despite these favorable data, one clinical trial was discontinued due to failure to reach the projected PFS of 50% in an interim analysis with eight out of nine patients relapsing within 90 days after haploidentical transplantation. Schmidt et al reported outcomes from a much larger retrospective cohort of 85 MM patients undergoing allogeneic HCT between 2000 and 2022, with a median OS of 1.7 years, five-year OS of 22.2%, and a one-year TRM of 23.5%.24 Whether this difference in OS in previously published studies and our data are due to selection bias, different donor type allogeneic HCT (haploidentical HCT vs matched- or partially mismatched unrelated donor HCT), or availability of more recent therapeutic options prior to and after allogeneic HCT is unclear.5,6,22 Here, we report promising results with a five-year OS of 71%, despite one early death due to CDI which is a frequent complication after allogeneic HCT.25 This corresponds to a treatment-related mortality rate of 14%, which is comparable to other previous reported rates for allogeneic HCT in multiple myeloma.7,22 Among the six surviving patients median time to relapse was 26.5 months (range, 5–81 months). Four patients (67%) remained free of disease progression at two years after haploidentical HCT and two patients (33%) maintained remission beyond four years. A rather high rate of a/cGVHD was observed but no GVHD associated deaths occurred. Of note, the interpretation of our results is limited due to low patient numbers and its unicentric and retrospective nature.
At present, CAR-T cell therapies and bispecific T cell engagers are the preferred options for triple-class refractory r/r MM patients.2 When these modalities have been exhausted or are not accessible, haploidentical HCT appears to be a feasible salvage therapy option for severely pretreated r/r MM patients. Notably, even in the setting of relapse/progressive disease, patients undergoing haploidentical HCT demonstrate superior post-relapse responses compared with those previously treated with autologous transplantation.12,22 Following relapse after haploidentical HCT, CR or at least VGPR could be achieved using immunomodulatory agents and combinations such as pomalidomide, carfilzomib, and daratumumab. A possible explanation for this effect is the avoidance of an immune escape by the combination of the persisting graft-versus-myeloma- effect and immunomodulatory substances.11 At last follow-up, four of the five surviving patients were in CR and one in VGPR; this favorable disease control reflects the efficacy of the subsequent post-transplant treatment regimens and represents an important contributor to the overall survival observed in this cohort. Thus far, limited experience has been acquired with BCMA-, or GPRC5D- targeted CAR-T cell therapy and bispecific antibodies following allogeneic HCT. However, existing data indicate comparable efficacy and favorable tolerability in patients after allogeneic HCT.26–28 In line with these observations, one patient in our cohort received idecabtagene vicleucel and another patient was treated with a bispecific antibody following allogeneic HCT. Neither patient developed GvHD or experienced unexpected adverse events, supporting the notion that these therapies may be feasible in the post-transplant setting.
Although there is a possible selection effect to consider in our cohort, as fit patients are more likely to be offered allogeneic HCT, fulminant progressive patients are less likely to undergo allogeneic HCT and the availability of a haploidentical donor is necessary.
In our small cohort, we can confirm the previously published data reporting promising OS and subsequent disease control of r/r MM patients after haploidentical allogeneic HCT and see this overall as a valid and safe option for selected patients. Nevertheless, prospective randomized studies are warranted to further evaluate its efficacy, feasibility, safety and to identify which patient subgroups are most likely to benefit from haploidentical HCT.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
This paper was presented at the 50th annual meeting of the European society for Blood and Marrow Transplantation (EBMT) as abstract with interim findings.
M.B. reports lecture fees and honoraria from Jazz Pharmaceuticals and MSD, and service on advisory boards for ActiTrexx. K.T.G. has received consulting fees from Sanofi, Takeda, Novartis, Amgen, GSK, and Janssen, and honoraria from Novartis, Amgen, and GSK. M.H. reports honoraria from Sobi, Novartis, Gilead, Falk Foundation, Bristol Myers Squibb (BMS), and Kite, and consulting fees from Pfizer, Incyte, Sanofi, Roche, Amgen, Sobi, Janssen, Kite, Bristol Myers Squibb (BMS), and BeiGene. F.S. has received honoraria and travel support from medac. All other authors declare no conflicts of interest.
References
1. Röllig C, Knop S, Bornhäuser M. Multiple myeloma. Lancet. 2015;385(9983):2197–7. doi:10.1016/S0140-6736(14)60493-1
2. Dimopoulos MA, Terpos E, Boccadoro M, et al. EHA-EMN evidence-based guidelines for diagnosis, treatment and follow-up of patients with multiple myeloma. Nat Rev Clin Oncol. 2025;22(9):680–700. doi:10.1038/s41571-025-01041-x
3. Mohty M, Bruno B, Gagelmann N, Mateos MV. Multiple Myeloma. In: Sureda A, Corbacioglu S, Greco R, Kröger N, Carreras E, editors. The EBMT Handbook. Springer International Publishing; 2024:741–749. doi:10.1007/978-3-031-44080-9_81
4. Rasche L, Hudecek M, Einsele H. CAR T-cell therapy in multiple myeloma: mission accomplished? Blood. 2024;143(4):305–310. doi:10.1182/blood.2023021221
5. Van Elssen C, van Gorkom G, Voorter C, et al. Haploidentical transplantation in patients with multiple myeloma making use of natural killer cell alloreactive donors. Ann Hematol. 2021;100(1):181–187. doi:10.1007/s00277-020-04303-z
6. Sahebi F, Garderet L, Kanate AS, et al. Outcomes of haploidentical transplantation in patients with relapsed multiple myeloma: an EBMT/CIBMTR Report. Biol Blood Marrow Transplant. 2019;25(2):335–342. doi:10.1016/j.bbmt.2018.09.018
7. Greil C, Engelhardt M, Ihorst G, et al. Allogeneic transplantation of multiple myeloma patients may allow long-term survival in carefully selected patients with acceptable toxicity and preserved quality of life. Haematologica. 2019;104(2):370–379. doi:10.3324/haematol.2018.200881
8. Maffini E, Storer BE, Sandmaier BM, et al. Long-term follow up of tandem autologous-allogeneic hematopoietic cell transplantation for multiple myeloma. Haematologica. 2019;104(2):380–391. doi:10.3324/haematol.2018.200253
9. Granot N, Storb R. History of hematopoietic cell transplantation: challenges and progress. Haematologica. 2020;105(12):2716–2729. doi:10.3324/haematol.2019.245688
10. Htut M, D’Souza A, Krishnan A, et al. Autologous/allogeneic hematopoietic cell transplantation versus tandem autologous transplantation for multiple myeloma: comparison of long-term postrelapse survival. Biol Blood Marrow Transplant. 2018;24(3):478–485. doi:10.1016/j.bbmt.2017.10.024
11. Magrangeas F, Avet-Loiseau H, Gouraud W, et al. Minor clone provides a reservoir for relapse in multiple myeloma. Leukemia. 2013;27(2):473–481. doi:10.1038/leu.2012.226
12. Gahrton G, Iacobelli S, Garderet L, Yakoub-Agha I, Schönland S. Allogeneic transplantation in multiple myeloma—does it still have a place? JCM. 2020;9(7):2180. doi:10.3390/jcm9072180
13. Luznik L, O’Donnell PV, Symons HJ, et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol Blood Marrow Transplant. 2008;14(6):641–650. doi:10.1016/j.bbmt.2008.03.005
14. Müller AMS, Kumar SK, Bruno B. The stepchild in myeloma treatments: is allogeneic transplantation not so bad after all? Haematologica. 2019;104(2):222–225. doi:10.3324/haematol.2018.206987
15. Durie BGM, Harousseau JL, Miguel JS, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20(9):1467–1473. doi:10.1038/sj.leu.2404284
16. Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328–e346. doi:10.1016/S1470-2045(16)30206-6
17. International Society of Nephrology. Chapter 1: definition and classification of CKD. Kidney Int Suppl. 2013;3(1):19–62. doi:10.1038/kisup.2012.64
18. Bolaños-Meade J, Hamadani M, Wu J, et al. Post-transplantation cyclophosphamide-based graft-versus-host disease prophylaxis. N Engl J Med. 2023;388(25):2338–2348. doi:10.1056/NEJMoa2215943
19. Desai N, Altareb M, Remberger M, et al. PTCy-based graft-versus-host disease prophylaxis for matched sibling donor allogeneic hematopoietic cell transplantation. Blood Adv. 2025;9(3):660–669. doi:10.1182/bloodadvances.2024014781
20. Kaddoura M, Binder M, Dingli D, et al. Impact of achieving a complete response to initial therapy of multiple myeloma and predictors of subsequent outcome. Am J Hematol. 2022;97(3):267–273. doi:10.1002/ajh.26439
21. Gahrton G, Tura S, Ljungman P, et al. Prognostic factors in allogeneic bone marrow transplantation for multiple myeloma. JCO. 1995;13(6):1312–1322. doi:10.1200/JCO.1995.13.6.1312
22. Strassl I, Nikoloudis A, Machherndl-Spandl S, et al. Allogeneic stem cell transplantation in multiple myeloma: risk factors and outcomes in the era of new therapeutic options—a single-center experience. Cancers. 2023;15(24):5738. doi:10.3390/cancers15245738
23. Vuppala R, Weeks C, Dalgetty M, et al. Allogeneic stem cell transplantation for high-risk multiple myeloma. Blood. 2024;144(Supplement 1):7401. doi:10.1182/blood-2024-211898
24. Schmidt WM, Perera ND, Buadi FK, et al. Long-term outcomes of allogeneic stem cell transplant in multiple myeloma. Blood Cancer J. 2023;13(1):126. doi:10.1038/s41408-023-00900-z
25. Amberge S, Kramer M, Schröttner P, et al. Clostridium Difficile infections in patients with AML or MDS undergoing allogeneic hematopoietic stem cell transplantation identify high risk for adverse outcome. Bone Marrow Transplant. 2020;55(2):367–375. doi:10.1038/s41409-019-0678-y
26. John L, Sauer S, Hegenbart U, et al. Idecabtagene vicleucel is well tolerated and effective in relapsed/refractory myeloma patients with prior allogeneic stem cell transplantation. Transplant Cell Ther. 2023;29(10):609.e1–609.e6. doi:10.1016/j.jtct.2023.06.010
27. Htut M, Dhakal B, Cohen AD, et al. Ciltacabtagene autoleucel in patients with prior allogeneic stem cell transplant in the CARTITUDE-1 Study. Clin Lymphoma Myeloma Leuk. 2023;23(12):882–888. doi:10.1016/j.clml.2023.08.012
28. Amoozgar B, Vesole DH, Donato ML, et al. Impact of Allogeneic Stem Cell Transplant (allo-SCT) on safety and outcomes of Chimeric Antigen Receptor T Cell (CAR-T) therapy in patients with Multiple Myeloma (MM). Transplant Cell Ther. 2024;30(2):S387. doi:10.1016/j.jtct.2023.12.542
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.