")
Back to Journals » Clinical Ophthalmology » Volume 15
Hand-Held Nidek versus Table-Mounted Huvitz Autorefractors and Their Agreement with Subjective Refraction in Adults
Authors Sayed KM , Alsmman AH , Mostafa EM
Received 30 May 2020
Accepted for publication 17 March 2021
Published 1 April 2021 Volume 2021:15 Pages 1391—1401
DOI https://doi.org/10.2147/OPTH.S263667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Khulood Muhammad Sayed, Alahmady Hammad Alsmman, Engy Mohammed Mostafa
The Department of Ophthalmology, Sohag Faculty of Medicine, Sohag University, Sohag, Egypt
Correspondence: Alahmady Hammad Alsmman
The Department of Ophthalmology, Sohag Faculty of Medicine, Sohag University, Sohag, 82524, Egypt
Tel +20-1111-428-635
Email [email protected]
Objective: To compare the agreement between commercially available table mounted and a hand-held autorefractors and their agreement with subjective refraction. The effect of different body position with the handheld autorefractometer was also evaluated.
Methods: A prospective study was performed on 253 healthy eyes. Refraction was acquired by a table-mounted Huvitz and hand-held Nidek autorefractometer, subjective refraction was acquired. Refractive errors were compared in terms of spherical equivalent (SE), cylinder power, and the J0 and J45. The level of agreement was evaluated by Bland–Altman plots.
Results: There was a significant difference in SE measurements between both devices and between them and subjective refraction (P=0.00). The Huvitz SE readings tended to be less myopic. However, limits of agreement (LOA) for SE were narrowest for Nidek sitting vs supine followed by Huvitz vs subjective SE refraction. The LOA for SE for Nidek sitting vs subjective SE were of wider range. For cylinder values, LOA were similar for all devices and positions and between them and subjective cylinder refraction.
Conclusion: Table mounted Huvitz and Nidek portable autorefractor cannot be used interchangeably in clinical practice except for estimation of the cylinder power. No difference in refraction between sitting and supine positions for portable Nidek autorefractor but with caution in cylinder axis. High agreement was achieved between subjective refraction and Huvitz readings but not with Nidek hand-held autorefractor. A highly reliable spectacle prescription could be done based on Huvitz readings. Both devices and positions could be used interchangeably in estimation of K-readings.
Keywords: Huvitz, Nidek, portable, autorefractometer, subjective refraction
Introduction
Subjective refraction continues to be the gold standard practice for accurately prescribing glasses,1 and not to be replaced by autorefraction. Yet autorefraction can be used to set a starting point for subjective refraction.2 Autorefraction also plays a major role in following the progress of refractive errors as well as its value in screening for refractive errors in children.3–5
Cyclotorsions occur when the eye rotates around the optical axis6,7 and depend on the orientation of the body.8 One type of cyclotorsion is the static type which occurs when the patient changes position from an upright or sitting position to supine position.6
Assessing the agreement between 2 different-commercially available-autorefractometers would be of value in clinical practice so as to know if they could be used interchangeably or not. Previous studies comparing hand-held to table-mounted autorefractors did not include comparison with subjective refraction nor the effect of changing body position.9,10 So we planned to put the different body position effect on refraction onto test, then all findings were compared with the subjective refraction that acquired the best-corrected visual acuity. To the best of our knowledge, comparing the agreement between Huvitz table mounted and a handheld Nidek autorefractors in different body positions was not studied before.
Methods
A prospective cross-sectional study was done on 253 eyes of 253 healthy population collected from the outpatient clinic of Ophthalmology department in Sohag university hospital. The study was conducted from January 2019 to November 2019. The study population was - to a large extent- the relatives of patients or the workers in the department. Data were collected from 350 subjects but only 253 patients fit the inclusion criteria. All participants underwent refraction measurement with the table mounted autorefractometer (Huvitz autoref/keratometer HRK-7000A Huvitz Co. Ltd., Republic of Korea) followed by the hand held autorefractometer Nidek ARK-30 (Nidek Co. Hiroishi, Japan) in both sitting and supine position. Subjective refraction was determined by the spherical and cylinder lenses that could achieve the best-corrected distance visual acuity (BCDVA). It was performed by a single physician. Subjects were informed about the measurements and informed consent was obtained. This study was approved by the ethical committee of the Sohag faculty of medicine, Sohag, Egypt. The study adhered to the tenets of the Declaration of Helsinki.
Inclusion criteria were subjects older than 18 years and a best-corrected visual acuity (VA) better than 0.1 logarithm of the minimum angle of resolution (6/7.5). Exclusion criteria included: any ocular condition that interfered with autorefractometer performance and any previous ocular surgery. Eyes with retinal pathology and amblyopic eyes were also excluded.
Refraction measurements of the subjects were performed by one investigator and were repeated at least 3 times with the average values of the obtained results recorded. As the two eyes were strongly related, only refractive readings of one eye of each patient were used for statistical analysis. The included eye was chosen randomly except when one of them did not fit the inclusion criteria.
Nidek ARK-30 hand-held autoKeratorefractometer works with the Scheiner’s double pinhole principle. This device has an autofogging mechanism to relax accommodation. It consists of 2 parts: the main body and the hand-held measurement device which is connected wirelessly to the main body (same as a video camera in size and weight (980 g)). It measures monocularly and the measurement distance should be 6 cm from the eye. It automatically records 10 measurements from each eye and gives a single best result. It has a measurement range of −20.00 to +22.00 D for spheres and 12 D for cylinders.
Table-mounted Huvitz HRK-7000A has a refractive range of −25.00 to +22D and cylinder 10D. It uses color picture slide with autofogging technique for measurement. Its principle is based on wavefront aberrometry (Hartmann shack).11
For spherical equivalence, the following formula was used:

Vector analysis is used to compare the magnitude and direction of two cylinders.12 So the axis values were converted to the power vector coordinates J0, and J45 using the following equations13 where C is the cylindrical component, and α is the axis in radians:


Subjective Refraction
Meticulous subjective refraction was performed by determination of BCDVA and using the Jackson’s cross-cylinder technique for checking the cylindrical power and axis. The final spherical power was defined as the highest plus value or the lowest minus value that gave the best visual acuity. Refraction of each eye was done separately followed by binocular balancing. Subjective refraction was done before autorefraction to maintain masking, but any previous spectacles were available to the ophthalmologist at the time of testing and were usually used as a starting point of subjective refraction.
Statistical Analysis
Data were analyzed using MedCalc version 18.1. Quantitative data were represented as mean±standard deviation. Data were analyzed using ANOVA with Bonferroni post hoc test for comparison of the means of three groups. A probability of less than 5% (p<0.05) was considered statistically significant. Agreement between both devices was compared using Bland–Altman analysis scatter plots.
When the data were not normally distributed Kruskal Wallis test was used for comparison of three groups and Mann–Whitney test was used to compare two groups.
The Scatter plots of differences between the device measurements against the mean of the measurements are used to assess the agreement between these devices. The 95% limits of agreement (LoA) were calculated using the mean difference ±1.96 standard deviation (SD). The smaller the range between these two limits the better the agreement is.
Positive J0 values represent with-the-rule astigmatism, and negative values correspond to against-the-rule astigmatism, and J45 represents oblique astigmatism.
Results
The study started by 350 subjects yet 97 did not fit the inclusion criteria due to the presence of cataract surgery, retinal pathology and amblyopia.
So the total sample size in our study was 253 eyes of 253 subjects with mean age of 35.05±11.76 years, 106 patients were females (41.9%) and 125 were right eyes (49.4%).
The SE of the study population ranged from (−9.25 to +11.50 D) and cylinder error ranged from (−5.00 to 0.00 D).
Mean (±SD) of SE refraction, cylinder power, the J0 and J45 vector component and keratometric measurements obtained using the Huvitz, Nidek sitting and Nidek supine position and subjective refraction are shown in Tables 1 and 2.
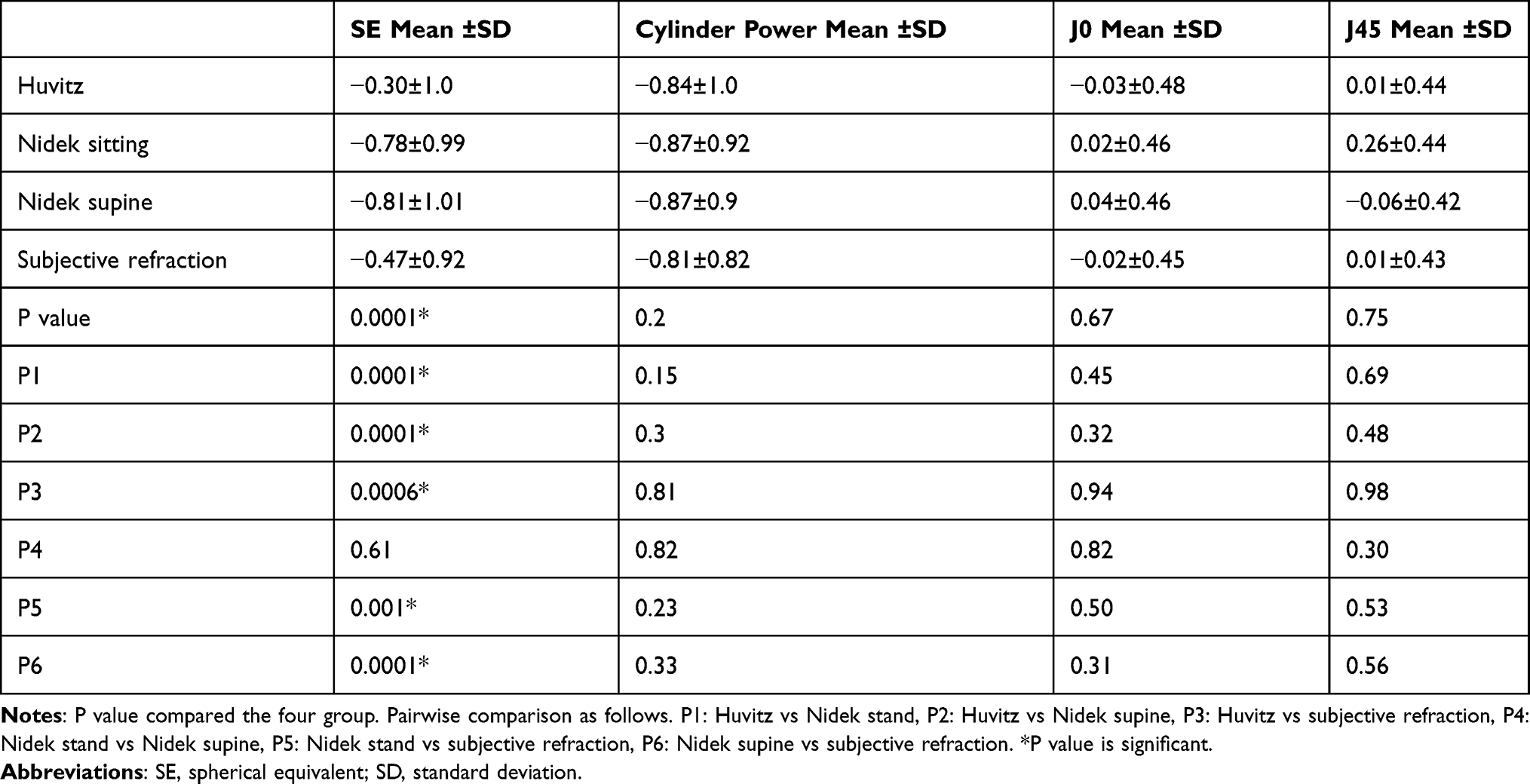 |
Table 1 Comparison of Mean Values of Refractive Measurements Between Autorefractometers |
 |
Table 2 Comparison of Mean Keratometric Values Between Both Devices |
There was a statistically significant difference in mean SE between both instruments in both positions and between both of them and subjective refraction (p<0.001) with the Huvitz SE readings tended to be less myopic (less minus) than both the sitting and supine positions of the Nidek and also less myopic than subjective refraction. No significant difference was found between both instruments in any other parameter or between any of the devices and subjective refraction regarding cylinder power cylinder, J0 and J45 and K-readings.
Correlations
There were strong positive correlations between both devices in sphere and cylinder values and strong correlation between both devices and subjective refraction in sphere and cylinder values (Table 3).
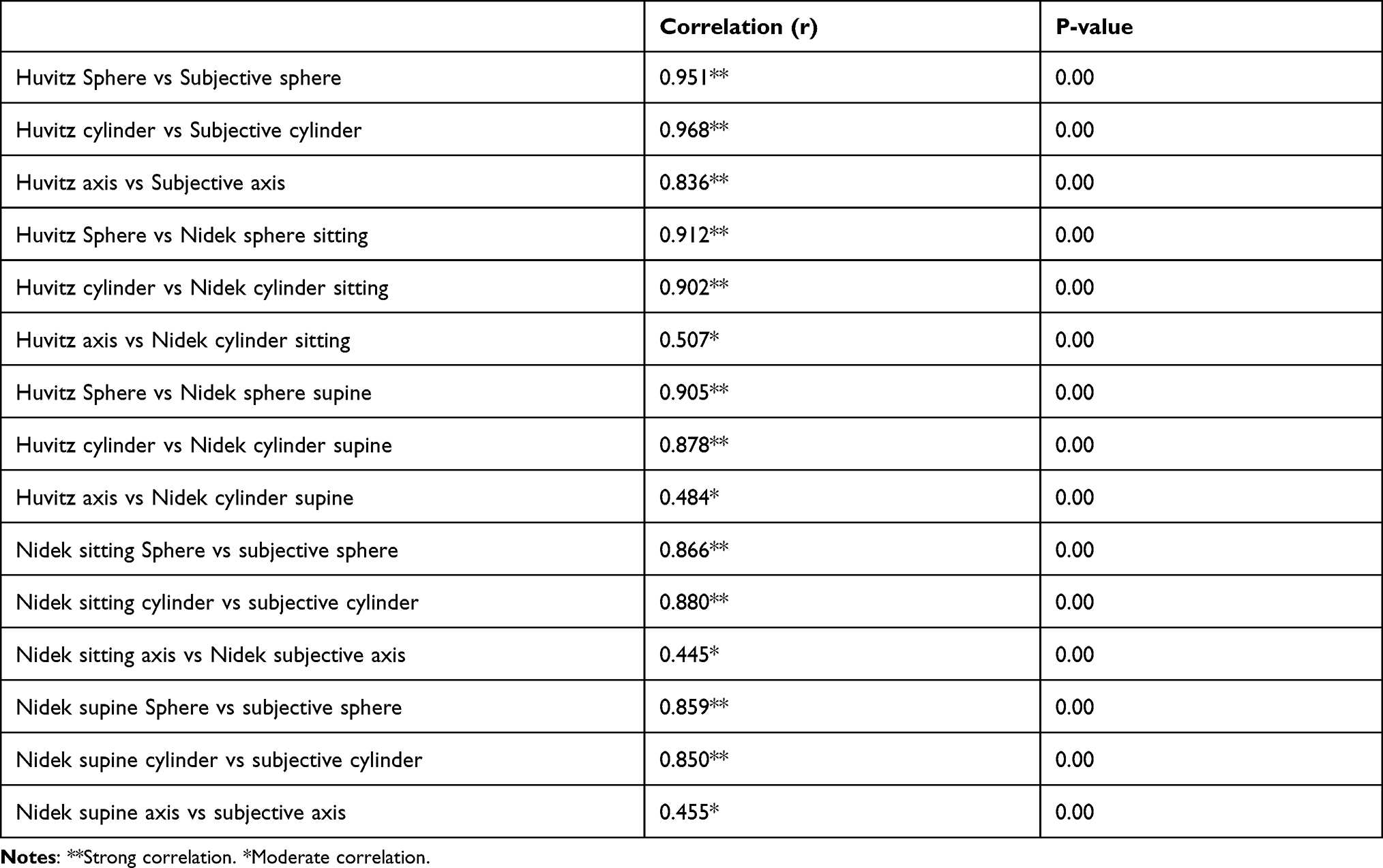 |
Table 3 Correlations Between Variables of Both Devices in Both Positions and Subjective Refraction |
Multivariate Predictors
When variables were entered in a regression models; the most predictive variable for subjective sphere was Huvitz sphere measurements. r2 = 0.905, P=0.00. The most predictive variable for subjective cylinder was also Huvitz cylinder measurements. r2 = 0.938, P=0.00. The most predictive variable for subjective axis was Huvitz axis measurements. r2 = 0.699, P=0.00.
Mean Difference
The mean SE difference between the measurements taken with the Huvitz table-mounted autorefractor and those taken using the portable Nidek sitting were significantly different: 0.48±0.39. The Nidek consistently recorded more minus values than its table-mounted Huviz. Nidek also consistently recorded more myopic SE measurements than subjective refraction, with a mean difference of −0.31±0.48D. The least mean SE differences were reported between Nidek sitting vs supine (0.03 D) followed by Huvitz vs subjective refraction (0.18D), No significant differences were observed in mean differences of cylinder, J0 and J45 measurements between both devices and both positions and between both of them and subjective refraction.
Mean differences between Huvitz and Nidek sitting, Huvitz and Nidek supine and Nidek sitting and supine and subjective refraction for all variables are shown in Table 4. The J0 and J45 showed smaller mean difference than cylinder power but with a wider confidence interval. The 95% confidence interval of upper and lower limits of agreement for spherical equivalent, and J0 and J45 vector components were demonstrated in Table 4.
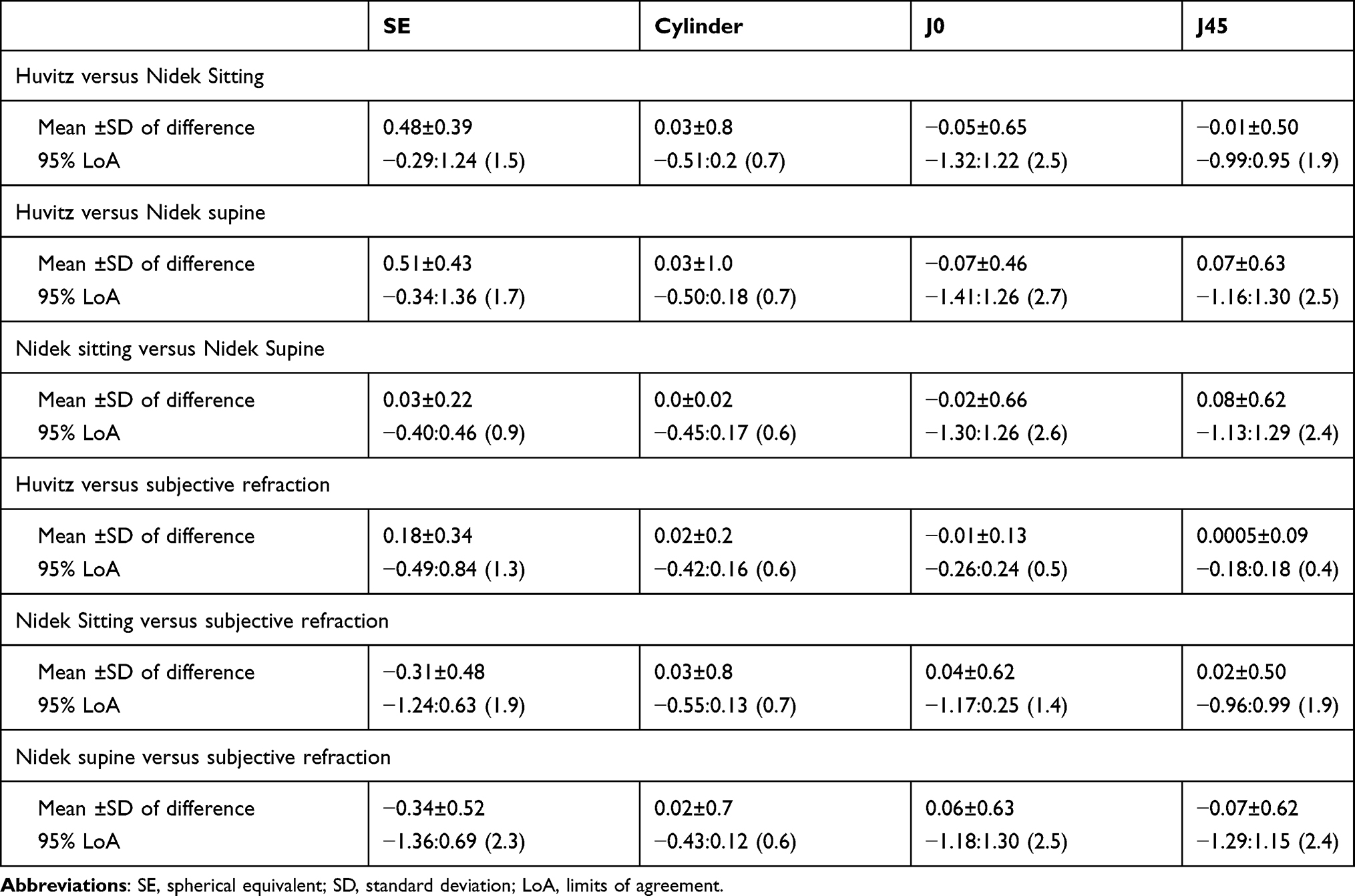 |
Table 4 Differences in Mean Refractive Components Between Autorefractometers |
Mean difference ± SD in SE measurements was the least for Nidek sitting vs Nidek supine (0.03±0.22) followed by Huvitz vs subjective SE (0.18±0.34). For Cylinder measurements, mean difference was minimal for both devices and positions (0.02–0.03). Mean difference ± SD of J0 measurements was the least for Huvitz vs subjective J0 (−0.01±0.13), the same was for J45 measurements (0.0005±0.09).
Bland–Altman Plots
Bland–Altman plots are shown in Figure 1A–C. The 2 dotted lines represent the lower and upper 95% limits of agreement (LoA). The vertical axis represents the difference between both devices measurements; the horizontal axis shows the arithmetic mean values for SE, J0 and J45 in Figures 1–3 respectively.
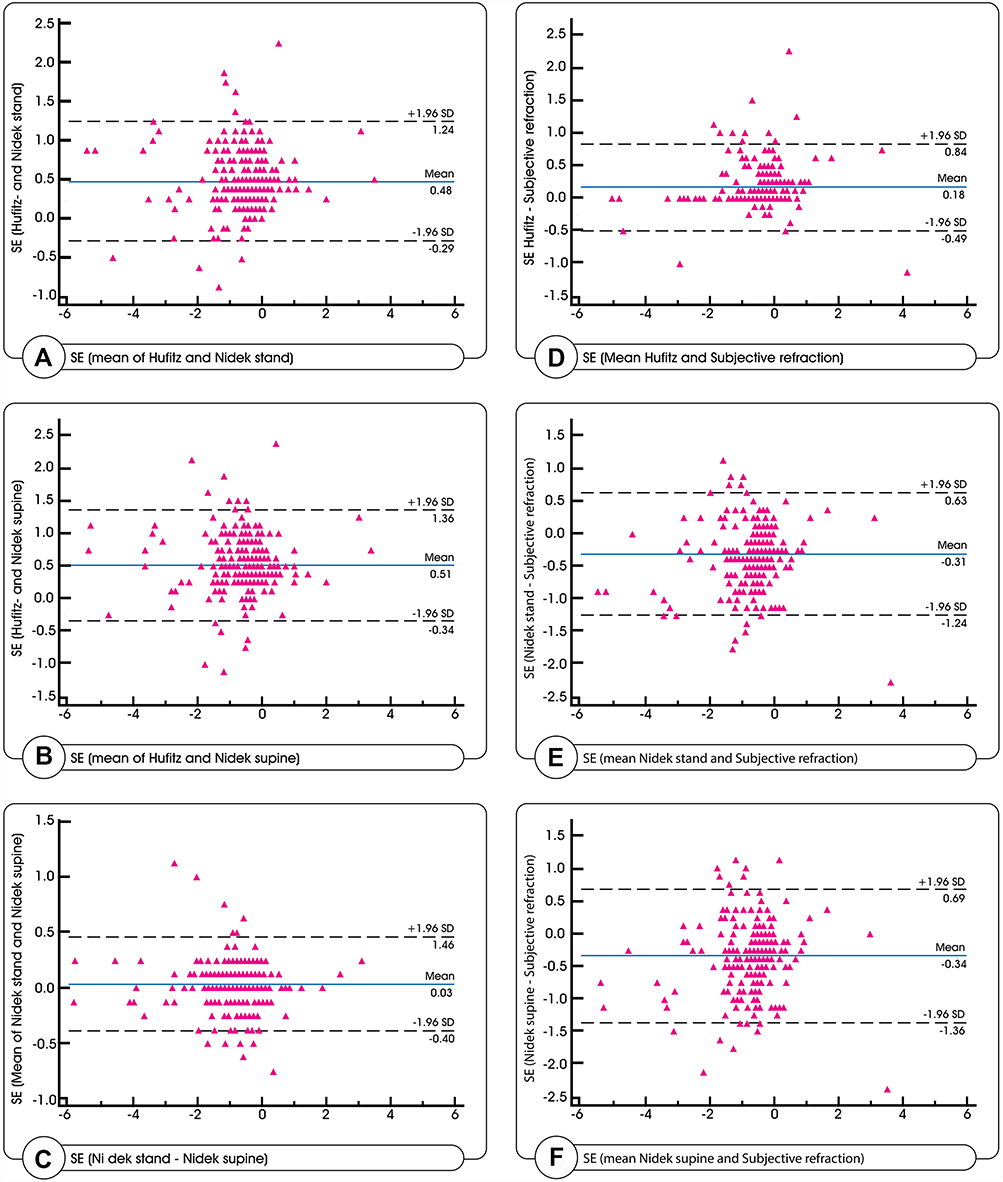 |
Figure 1 Bland–Altman plots of the differences in spherical equivalence (SE) between Huvitz and Nidek sitting (A), Huvitz and Nidek supine (B), and Nidek sitting and Nidek supine (C). Huvitz and subjective refraction. (D). Nidek sitting and subjective refraction (E). Nidek supine and subjective refraction (F). |
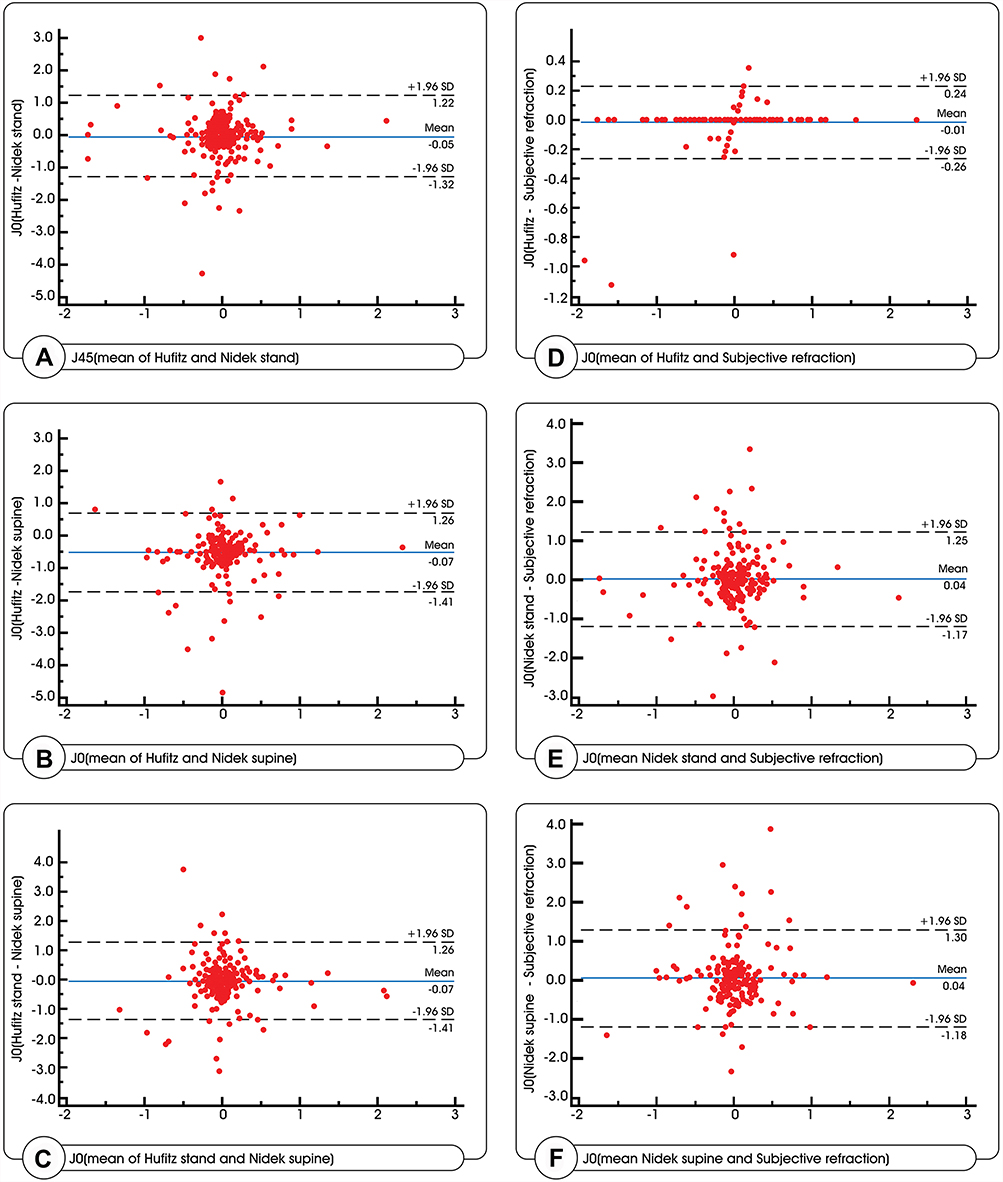 |
Figure 2 Bland–Altman plots of the differences in J0 between Huvitz and Nidek sitting (A), Huvitz and Nidek supine (B), and Nidek sitting and Nidek supine (C). Huvitz and subjective refraction. (D). Nidek sitting and subjective refraction (E). Nidek supine and subjective refraction (F). |
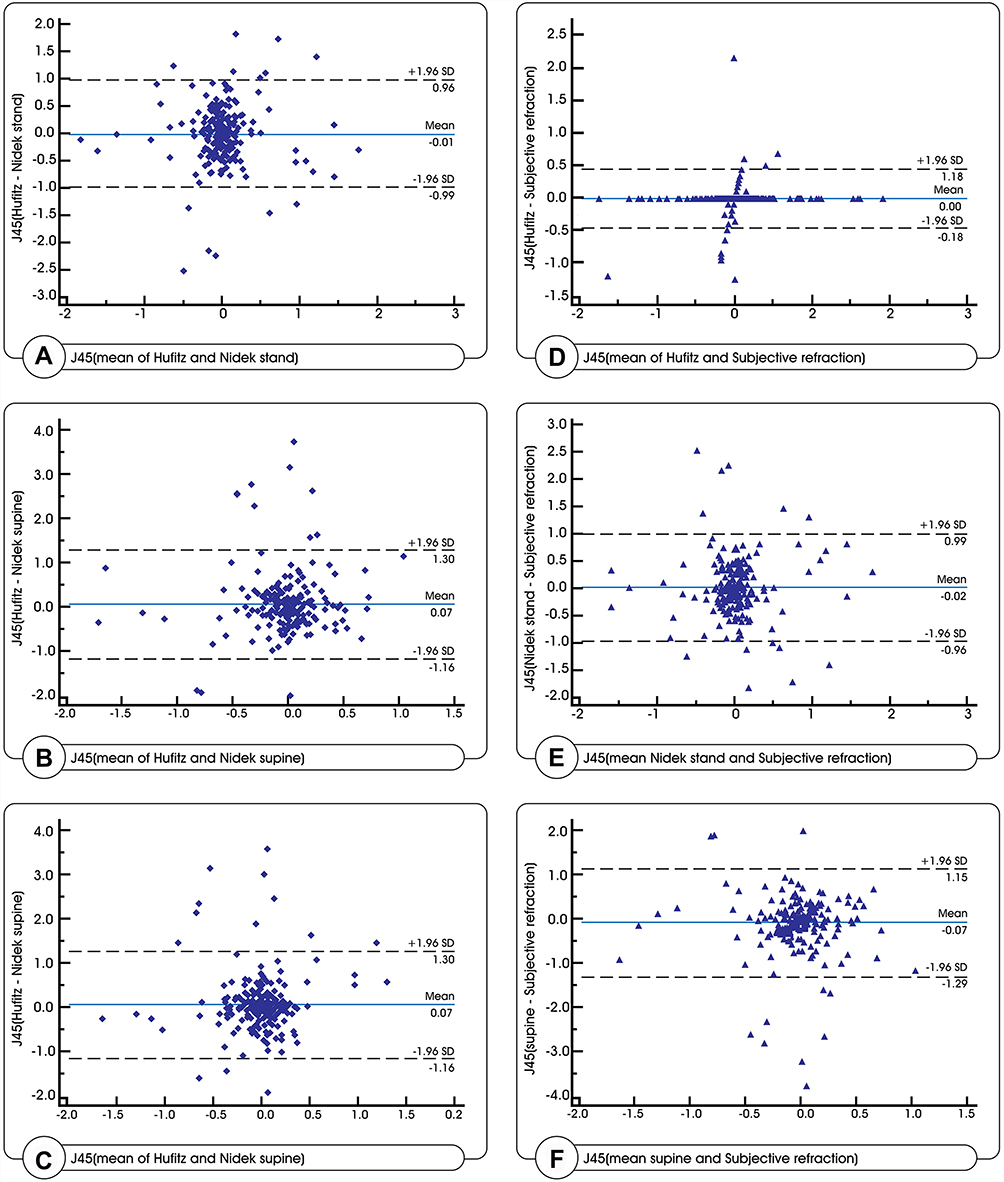 |
Figure 3 Bland–Altman plots of the differences in J45 between Huvitz and Nidek sitting (A), Huvitz and Nidek supine (B), and Nidek sitting and Nidek supine (C). Huvitz and subjective refraction. (D). Nidek sitting and subjective refraction (E). Nidek supine and subjective refraction (F). |
Subjective Refraction
The narrowest 95% LOA was achieved between subjective refraction and Huvitz measurements (SE, cylinder, J0 & J45), much more wider 95% LOA was found between it and Nidek measurements in both positions.
Huvitz vs Nidek
Nearly the same 95% LoA (mean difference ±0.1.96 SD) was achieved between both positions of Nidek and Huvitz measurements except for J0&J45. It was the narrowest for cylinder power.
Nidek Sitting vs Supine
A very narrow range of 95% LOA was achieved in SE (−0.40:0.46 (0.9)) and cylinder readings (−0.45:0.17 (0.6)) but not in J0 (−1.30:1.26 (2.6)) and J45 (−1.13:1.29 (2.4)).
Discussion
The study revealed high agreement – in the vast majority of cases – between subjective refraction and Huvitz table-mounted autorefractor in all parameters of refraction (SE, cylinder power and axis). The narrow 95% limits of agreement demonstrates that the differences among the Huvitz and subjective refraction could be ignored, although they were statistically significant.
Agreement was achieved between subjective refraction and Nidek portable autorefractor only in measuring the cylinder power.
The study also revealed more myopic (more versus) SE values of the Nidek portable autokeratorefractometer in both positions when compared to the table-mounted Huvitz and subjective refraction. The mean difference in SE was significantly different between Huvitz and Nidek in sitting and supine positions (0.48 and 0.51D, respectively) this difference was not found in cylinder power.
Our results are comparable to a previous study by Buchner on 216 children who found that non-cycloplegic handheld autorefraction was comparable to tabletop autorefraction for cylinder power with limitations in accuracy for the SE14 but in contrast to the same study that found the axis of the cylinder was also comparable which was significantly different in our study.
Our results are not in agreement with Wesemann and Dick study who found that the handheld autorefractor (Retinomax) was fairly comparable to subjective refraction results.15 These discrepancies between studies may be due to comparing different devices with different working principles.
The better agreement of cylinder power and the relatively poorer agreement of the J0 and J45 vector components implied discrepancies in axis detection but not in the power of astigmatism using the two refractors and in using 2 different positions.
Thus in the clinical setting; both the Huvitz and Portable Nidek could not be used interchangeably for refraction measurements and more myopic SE readings are evident in the Nidek readings with wide 95% limits of agreement. On the other hand, there is a good agreement achieved regarding the cylinder power between both devices but not in J0 & J45 thus there is interchangeability only in measuring the amount of astigmatism but not its type.
In order to relax accommodation, most autorefractors use a “fogging” target to relax accommodation. Maximum relaxation of accommodation occurred for binocular targets receding into the distance. The hand-held autorefractor tests each eye separately, while the table-mounted autorefractor tests each eye sequentially, but with both eyes open during testing.16 This could explain the more myopic results with Nidek hand-held autorefractor.
High agreement was achieved between sitting and supine positions of Nidek autorefractor in SE and cylinder power but not J0&J45 which express the alignment of the cylinder power. This could be explained by the significant cyclotorsion that occurs in supine position and more with the monocular viewing conditions,17 which was the case with portable Nidek autorefractor.
The error of cylinder power alignment with the handheld autorefractor could be reduced by taking the measurements only when the examined eye is perfectly centralized and the hand of the examiner is highly stabilized with the device is horizontally aligned.
Limits of agreement for myopic side are much more narrow than hyperopic side between Huvitz vs subjective refraction. This is may be explained by the fact that during acquiring subjective refraction for spectacle prescription for the 1st time, myopic patients are comfortable with the least versus power and the hypermetropic patients are not comfortable with full correction of hyperopia. So the range is wider towards the hyperopic side. This can explain the high agreement between Huvitz readings and subjective refraction especially with the less versus readings of Huvitz.
Our study has several limitations including the use of non-cycloplegic refraction which could have led to increased accommodation despite the fogging target of the device while acquiring refraction. Yet our choice of including adult population was to overcome the accommodation issues usually faced with children. Spectacle prescription in adults also depends mainly on non-cycloplegic refraction except in certain situations. In addition, non-cycloplegic refraction can help in screening and categorizing refractive error groups and in determining populations at risk so as to evaluate them further with cycloplegic refraction.18 We also did not use cycloplegia in measurement the refractive values aiming for assessing the potential use of Nidek portable autorefractor as a possible quick screening or diagnostic tool for measuring refraction.
Regarding these points, Nidek portable autorefractor could not be used in children without cycloplegia as it recorded over versus refraction in adults who already have less accommodative power than children. This is in agreement with Iuorno et al study on children who also cautioned the possibility of overdiagnosis of myopia by handheld autorefractor if used alone without cycloplegia19 also cannot be used as a quick diagnostic tool in adults except with extreme caution.
Another limitation is the study assessed two types of commercially available autorefractors; so, the results cannot be applied to other brands of autorefractors or newer technologies of the same principles.
Positive aspects of our study are: The study population consisted only of adults, leading to better analysis of the use of the hand-held portable autorefractor among adults especially being a non-time consuming device, easy to use and also suitable for handicapped and bed-ridden adults. One observer performed all the refraction measurements and thus interobserver bias was eliminated.
The study suggests a high agreement exists between all Huvitz readings and subjective refraction which is the gold standard method for assessment of the refractive error.20 Thus, Huvitz autorefractor can be considered a reliable tool for accurate estimation of refraction and accurate spectacle prescription.
Huvitz table-mounted and Nidek portable autorefractors cannot be used interchangeably for estimation of refraction except for the amount of astigmatism (cylinder power) but not its type (axis of astigmatism). The differences between both autorefractors may be clinically acceptable for screening with tendency for over versus reading for Nidek portable. However, caution should be taken when using these autorefractors for the assessment of the axis of astigmatism.
Both devices and positions could be used interchangeably in estimation of K-readings.
No difference between acquiring refraction with Nidek portable autorefractor in sitting or supine positions except for the axis of astigmatism. The error in cylinder axis could be minimized as discussed above.
Larger studies should be considered to compare the refraction with both devices under the effect of cycloplegia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goss DA, Grosvenor T. Reliability of refraction–a literature review. J Am Optom Assoc. 1996;67(10):619–630.
2. Bullimore MA, Fusaro RE, Adams CW. The repeatability of automated and clinician refraction. Optom Vis Sci. 1998;75(8):617–622. doi:10.1097/00006324-199808000-00028
3. Barry JC, Konig HH. Non-cycloplegic screening for amblyopia via refractive findings with the Nikon Retinomax hand held autorefractor in 3 year old kindergarten children. Br J Ophthalmol. 2001;85(10):1179–1182. doi:10.1136/bjo.85.10.1179
4. Cordonnier M, Dramaix M. Screening for refractive errors in children: accuracy of the hand held refractor Retinomax to screen for astigmatism. Br J Ophthalmol. 1999;83(2):157–161. doi:10.1136/bjo.83.2.157
5. Harvey EM, Miller JM, Wagner LK, Dobson V. Reproducibility and accuracy of measurements with a hand held autorefractor in children. Br J Ophthalmol. 1997;81(11):941–948. doi:10.1136/bjo.81.11.941
6. Smith EM
7. Kara-Junior N, Mourad P, Moraes R, Piva C, Santhiago M. Analysis of ocular cyclotorsion in lying position after peribulbar block and topical anesthesia. Rev Bras Oftalmol. 2014;73(4):199–201. doi:10.5935/0034-7280.20140044
8. Park SH, Kim M, Joo CK. Measurement of pupil centroid shift and cyclotorsional displacement using iris registration. Ophthalmologica. 2009;223(3):166–171. doi:10.1159/000194663
9. Mirzajani A, Qasemi F, Asharlous A, et al. Are the results of handheld auto-refractometer as valid as the result of table-mounted refractometer? J Curr Ophthalmol. 2018;31(3):305–311. doi:10.1016/j.joco.2018.10.012
10. Wosik J, Patrzykont M, Pniewski J. Comparison of refractive error measurements by three different models of autorefractors and subjective refraction in young adults. J Opt Soc Am a Opt Image Sci Vis. 2019;36(4):B1–B6. doi:10.1364/JOSAA.36.0000B1
11. Xiong S, Lv M, Zou H, et al. Comparison of refractive measures of three autorefractors in children and adolescents. Optom Vis Sci. 2017;94(9):894–902. doi:10.1097/OPX.0000000000001113
12. Schimitzek T, Wesemann W. Clinical evaluation of refraction using a handheld wavefront autorefractor in young and adult patients. J Cataract Refract Surg. 2002;28(9):1655–1666. doi:10.1016/S0886-3350(02)01426-8
13. Thibos LN, Wheeler W, Horner D. Power vectors: an application of Fourier analysis to the description and statistical analysis of refractive error. Optom Vis Sci. 1997;74(6):367–375. doi:10.1097/00006324-199706000-00019
14. Buchner TF, Schnorbus U, Grenzebach UH, Stupp T, Busse H. [Examination of preschool children for refractive errors. First experience using a handheld autorefractor.]. Ophthalmologe. 2003;100(11):971–978. German. doi:10.1007/s00347-003-0860-9
15. Wesemann W, Dick B. Accuracy and accommodation capability of a handheld autorefractor. J Cataract Refract Surg. 2000;26(1):62–70. doi:10.1016/S0886-3350(99)00325-9
16. Horwood AM, Riddell PM. Receding and disparity cues aid relaxation of accommodation. Optom Vis Sci. 2009;86(11):1276–1286. doi:10.1097/OPX.0b013e3181bb41de
17. Tjon-Fo-Sang MJ, de Faber JT, Kingma C, Beekhuis WH. Cyclotorsion: a possible cause of residual astigmatism in refractive surgery. J Cataract Refract Surg. 2002;28(4):599–602. doi:10.1016/S0886-3350(01)01279-2
18. Hu YY, Wu JF, Lu TL, et al. Effect of cycloplegia on the refractive status of children: the Shandong children eye study. PLoS One. 2015;10(2):e0117482. doi:10.1371/journal.pone.0117482
19. Iuorno JD, Grant WD, Noel LP. Clinical comparison of the Welch Allyn SureSight handheld autorefractor versus cycloplegic autorefraction and retinoscopic refraction. J AAPOS. 2004;8:123–127. doi:10.1016/j.jaapos.2003.10.006
20. Carracedo G, Carpena-Torres C, Batres L, Serramito M, Gonzalez-Bergaz A. Comparison of two wavefront autorefractors: binocular open-field versus monocular closed-field. J Ophthalmol. 2020:8580471.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.