Back to Archived Journals » Clinical Audit » Volume 14
Guideline Concordance in Managing Community-Acquired Pneumonia: Room for Improvement
Received 28 June 2022
Accepted for publication 14 October 2022
Published 15 November 2022 Volume 2022:14 Pages 79—88
DOI https://doi.org/10.2147/CA.S377148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zoka Milan
YG Alvin Tan,1,2 Ian A Scott1,2
1Department of Internal Medicine and Clinical Epidemiology, Princess Alexandra Hospital, Brisbane, Queensland, Australia; 2Greater Brisbane School of Clinical Medicine, University of Queensland, Brisbane, Queensland, Australia
Correspondence: YG Alvin Tan, Tel +61 7 3176 2111, Email [email protected]
Objective: To assess contemporary concordance of inpatient management of community-acquired pneumonia (CAP) with guideline recommendations relating to use of severity assessment tools (SAT), antimicrobials and microbiological investigations.
Methods: A single-centre, retrospective audit involving patients admitted with CAP to medical inpatient units of a tertiary hospital between September 2019 and March 2020 using electronic medical record review. SAT scores were retrospectively calculated for all patients, and the appropriateness of interventions determined with reference to local guidelines.
Results: Of 200 patients of mean age 64 years, 58% were admitted to general medicine units and the remainder to other specialties. Treating clinicians recorded a SAT in 9% (18/200) of the patients, with calculated scores rating 58% of all cases as being mild. Antibiotic prescribing on admission was guideline-concordant in 16.0% of the patients, but significantly higher among patients with moderate-to-severe vs mild CAP (24% vs 10%; p=0.01). Step-down oral antibiotic prescribing was guideline-concordant in 39% of the patients, and significantly higher among younger (< 65 years) vs older patients (51% vs 31%; p=0.006) and those with longer (> 7 days) vs shorter length of stay (57% vs 34%; p=0.007). No significant differences in concordance were seen between different specialties. Among patients for whom blood cultures and sputum cultures were requested, only 2% (2/110) and 17% (15/86) respectively yielded a positive result.
Conclusion: This study suggests infrequent use of SATs, low guideline concordance for antibiotic prescribing, and the need for more selective use of blood cultures. Reasons underpinning inappropriate antibiotic prescribing and strategies for reversing it need to be identified.
Keywords: community-acquired pneumonia, guideline concordance, risk stratification, microbiological investigations, antibiotics
Introduction
Community-acquired pneumonia (CAP) is defined as a lower respiratory infection with onset in the community or within 48 hours of hospitalization.1 Respiratory infections are a common cause for hospitalisations and mortality in Australia.2,3 The precise incidence of CAP is uncertain4 but is estimated at about 2 per 1000 people per year and accounts for about 2% of hospital admissions.5
Clinical guidelines from various jurisdictions help guide management of patients with CAP1,6,7 regarding the choice of initial antibiotics and use of severity assessment tools (SATs) that risk stratify patients in determining need for admission or likelihood of death or other adverse outcomes. The SMART-COP (systolic blood pressure, multi-lobar chest radiography involvement, albumin level, respiratory rate, tachycardia, confusion, oxygenation, and arterial pH) score, with a range 0 to 11, is one such tool that is commonly used and validated in Australian settings for identifying patients likely to require intensive respiratory or vasopressor support, as well as estimating 30-day mortality.8 Other SATs include the Pneumonia Severity Index (PSI) in the US7 and the CURB-65 (confusion, urea, respiratory rate, systolic or diastolic blood pressure, and age ≥65 years) in the UK.6
Adherence to clinical guidelines has been shown to decrease patient mortality, reduce duration of hospital stay,9 and improve cost-effectiveness of patient care.10 Despite these benefits, concordance with guideline recommendations in the care of CAP patients is often poor,11 and varies in Australian hospitals between 5% and 59%12 based on studies performed more than 7 years ago.
This study aimed to provide a contemporary review of the management of CAP in a tertiary hospital and determine concordance with local guidelines regarding 1) use of SMART-COP; 2) use of antibiotics; and 3) use and yield of microbiological investigations.
Materials and Methods
A single centre, retrospective cohort study was undertaken of consecutive patients admitted to inpatient wards of Princess Alexandra Hospital over the period between September 1, 2019 and March 31, 2020, and who had a discharge diagnosis of pneumonia coded as International Classification of Diseases version 10 (ICD-10) code J09-J19. These records were identified through the hospital’s health information management system and corresponding electronic medical records were retrieved. Selection criteria were derived from the International Community-acquired Pneumonia Organisation (CAPO) study protocol.13 Inclusion criteria comprised 1) radiological evidence (chest X-ray or computed tomography [CT] imaging) 48 hours before or after admission demonstrating new pulmonary infiltrate; and 2) one of the following clinical signs and symptoms: fever ≥38°C or hypothermia ≤35.5°C, changes in white cell count (leucocytosis or leukopenia) or new or increased cough and/or new or increased sputum. Exclusion criteria comprised 1) provisional diagnosis of hospital acquired pneumonia (defined as new onset pneumonia that occurred more than 48 hours after being hospitalised and not incubating at time of admission); 2) discharge diagnosis not consistent with CAP; 3) alternative diagnosis that adequately explained the clinical findings; and 4) palliative patients with pre-existing expressed wishes for no active intervention.
Data Collection
Data were collected on the following variables:
Patient characteristics: age, gender, place of residence; length of hospital stay (LOS); pre-existing co-morbidities (pulmonary conditions, obstructive sleep apnoea [OSA], heart failure, diabetes, chronic kidney disease, renal replacement therapy, rheumatoid arthritis, immunodeficiency state, chronic liver disease, or motor neuron disease); pneumococcal vaccination status if known; smoking status; alcohol misuse; need for domiciliary oxygen; SAT documented by treating team with severity scores; data required to calculate the SMART-COP score for each patient; cardiac complications including acute myocardial infarction and/or presence of cardiac arrhythmia; in-patient death; and readmissions to Queensland public hospitals with CAP within 30 days of discharge, ascertained by reviewing the state-wide Viewer software program.
Clinical care: intensive care unit admission (ICU) and ICU LOS; use of invasive or non-invasive ventilation (NIV); microbiological investigations for CAP including blood cultures, sputum cultures, urinary antigen tests, atypical organism serology, yield of pathogenic organisms and changes in antibiotic therapy according to pathogen and sensitivities; antibiotic use prior to admission; penicillin allergy status and drug reactions during hospitalisation; initial (empirical) antibiotics use; duration of intravenous (IV) antibiotic therapy; subsequent oral antibiotics prescribed, which took account of microbiological results; and time to conversion to oral therapy following onset of clinical stability, defined as resolution of fever/hypothermia for at least 48 hours, improvement in clinical signs and symptoms (including hypotension, tachycardia, oxygen saturation, respiratory rate, symptomatic improvement) and ability to tolerate oral intake.
Vaccination information was derived from available Medicare-recorded immunisation records via My Health Record. Scores for SMART-COP were calculated retrospectively for every patient by one investigator (AT) using extracted data. Variables used to calculate the scores were considered to have normal values if relevant data were not available. De-identified data were collated into an Excel spreadsheet and the SMART-COP score (with range 0 to 11) was calculated automatically. Depending on the severity scores, the cases were classified mild (score 0–2), moderate (score 3–4) or severe (score 5 to 11).
Reference Standard
The Metro-South Health (MSH) antibiotic guidelines14 issued in 2020 were used as the reference for determining guideline concordance for antibiotic prescribing, and which recommend a beta-lactam as the mainstay antibiotic for mild or moderate severity CAP, with a macrolide or doxycycline added to cover for atypical organisms, including gentamicin in severe cases to provide gram-negative cover (Appendix 1). Amoxycillin, with or without doxycycline or roxithromycin, was recommended as step-down oral therapy. Variations in recommended antibiotics and duration of therapy were considered acceptable (ie, guideline-concordant) on a case-by-case basis according to documented penicillin allergy/drug reactions, recommendations of attending Infectious Disease specialists and patient-specific clinical factors: febrile neutropenia, receiving immunosuppressive therapy, currently enrolled in clinical trials, clinical concerns about route of administration (eg, dysphagia) or comorbid conditions influencing antibiotic use (eg, renal insufficiency).
Outcome Measures
Whole cohort analyses were undertaken in defining patient characteristics, use of, and calculated scores for, SMART-COP, guideline concordance in choice, dose, duration, and route of administration of initial and subsequent antibiotics, and choice and yield of microbiological investigations. Additional subgroup analyses were performed comparing A) SMART-COP scores for 1) patients admitted to ICU/receiving NIV/dying in hospital versus scores for remaining patients and 2) patients undergoing microbiological investigations versus none; and B) guideline-concordant antibiotic prescribing in patients: 1) ≥65 years versus <65 years of age; 2) admitted to general medicine units versus other specialty units; 3) with SMART-COP scores for mild disease vs moderate-to-severe disease; 4) with pre-existing pulmonary disease vs no disease; 5) with diabetes or immunodeficiency vs none; 6) with LOS ≤7 days vs >7 days; and 7) readmitted at 30 days vs no readmission.
Statistical Analyses
Analyses were completed in Excel and descriptive statistics were used to present means (standard deviations [SD]), medians (interquartile range [IQR]) and proportions. Comparisons of proportions and means used chi-square tests (or Fisher’s exact tests for small samples) and Student’s t-test respectively. De-identified data were stored in a password-protected Microsoft Excel file only accessible to the investigators. Ethics approval was granted by the Metro South Human Research Ethics Committee (LNR/2020/QMS/60898). A waiver of consent was granted, given that the retrospective collection of data carries no foreseeable risk of harm to the participants.
Results
A total of 349 patient records were retrieved from the hospital database of which 200 admissions met selection criteria and were included for analysis.
Patient Characteristics
Mean age was 64 (± SD 18.9) years, 61% were male, and 15% were living in a residential age care facility at the time of admission (Table 1). The admitting unit was general medicine for 56.5% of the patients.
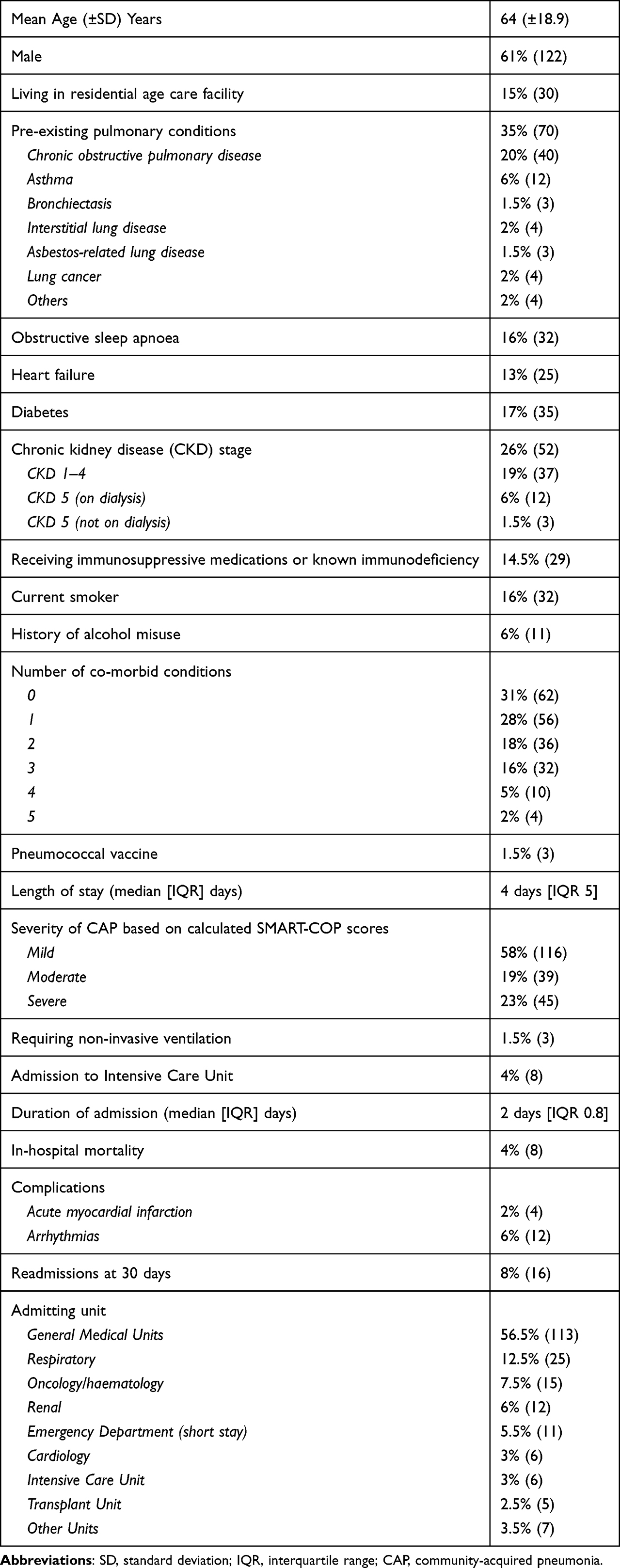 |
Table 1 Patient Characteristics (n=200) |
Pre-existing pulmonary conditions were documented in 70 (35%) patients, although none were receiving domiciliary oxygen. A minority of patients (32 [16%]) were current smokers, 35 (17%) had diabetes and 29 (14.5%) were receiving immunosuppressive medications or had diagnosed immunodeficiency. Only 3 patients had a recorded pneumococcal vaccine status, and 26 patients had a documented penicillin allergy.
Clinical Course
Median length of stay was 4 days (IQR 5) and 8 (4%) patients died in hospital. The mean age of patients that died in hospital was 82 (± SD 6.7) years. Admission to ICU occurred in 8 (4%) patients with median ICU stay of 2 (IQR 0.8) days, and 3 (1.5%) patients received NIV during admission. Complications comprised myocardial infarction in 4 (2%) patients and arrhythmias in 12 (6%), and 16 (8%) were readmitted at 30 days with CAP.
Severity Assessment
Use of a SAT was documented for 18 (9%) patients, SMART-COP in 15 and CURB-65 in 3. Most patients (96%) had data available on the variables used to retrospectively calculate a SMART-COP score; in the remaining 8 (4%) patients, pH was not available in the absence of blood gas analyses at presentation. Among those with a SMART-COP score documented by the admitting unit, 3 underestimated severity compared with the calculated score, 9 were concordant and 1 overestimated severity. The calculated SMART-COP score for all patients categorised the cohort as having mild disease in 116 (58.0%), moderate disease in 39 (19.5%) and severe disease in 45 (22.5%).
Microbiological Investigations
The most frequent investigation and corresponding yield was a blood culture (n=109, 54.5%; yield 2%), followed by Pneumococcus and Legionella urine antigen tests (n=88, 44%; 7%), sputum culture (n=86, 43%; 17%) and atypical pneumonia serology (n=73; 34%; 14%) (Table 2). Equal numbers of tests per patient (1.8) were performed in those with mild versus moderate-to-severe disease, and there were no differences between groups in frequency or yield of each type of investigation. A positive yield was seen in 33 of 356 investigations (9.3%). The frequency and corresponding proportion of a positive test that led to a change in therapy were blood cultures (n=2; 100%), sputum cultures (n=15; 53%), urine antigens (n=6; 50%) and atypical pneumonia serology (n=10; 20%). The most common causative organisms identified were Haemophilus influenzae and Streptococcus pneumoniae (5 cases each). Among 24 patients receiving antibiotics prior to admission, 11 had blood cultures (all negative) and 16 had sputum cultures of which two were positive.
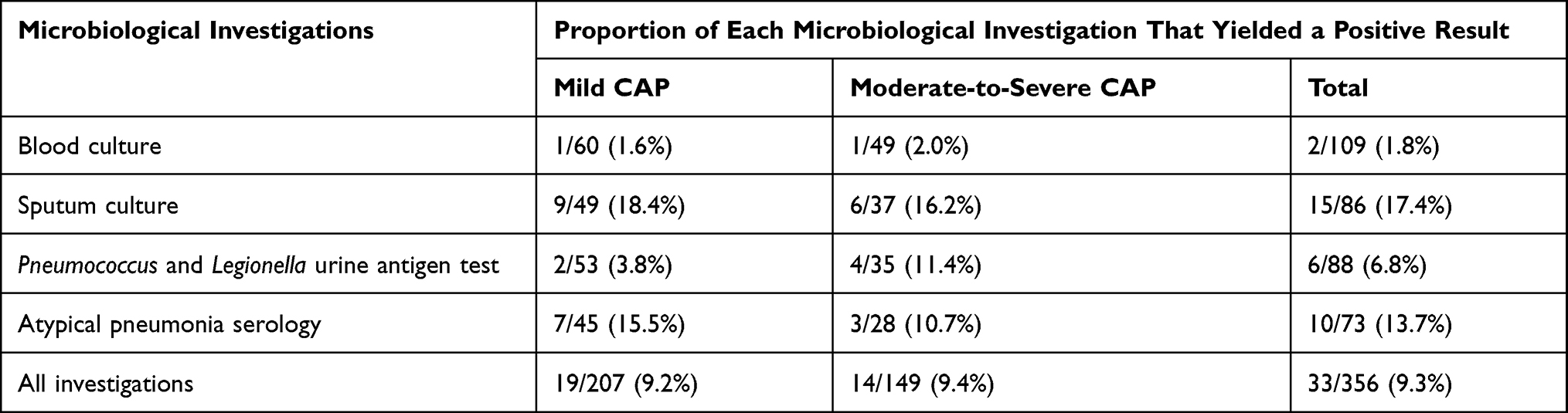 |
Table 2 Yield of Microbiological Investigations According to CAP Severity |
Antibiotic Prescribing
Initial antibiotic prescribing was guideline concordant in 32 of 200 patients (16.0%) (Table 3). On admission, the most frequently prescribed initial antibiotic regimes were IV benzylpenicillin and oral doxycycline (n=51, 26%), piperacillin–tazobactam (n=30, 15%) and ceftriaxone and azithromycin in (n=30, 15%). Among 30 patients receiving ceftriaxone, only 16 (53%) had a documented penicillin allergy to account for its use. Guideline concordance within each antibiotic group ranged from as low as 2.5% for piperacillin–tazobactam to 100% for amoxycillin. Acceptable deviations from guidelines comprised penicillin allergy (n=6/32; 19%), concerns about dysphagia (n=2/32; 6%) and chronic kidney disease (n=1/32; 3%). Among the 168 patients with guideline-discordant initial antibiotic prescribing, 163 (97%) had incorrect antibiotics prescribed and 5 patients (3%) had incorrect dose charted. The mean duration of IV antibiotics was 3.5 (± SD 2.5) days. Most of the patients (n=144; 72%) patients were switched appropriately to oral therapy following determination of clinical stability. For the remaining 56 (28%) patients with delayed switch to oral antibiotics, reasons for this could not be ascertained from medical records.
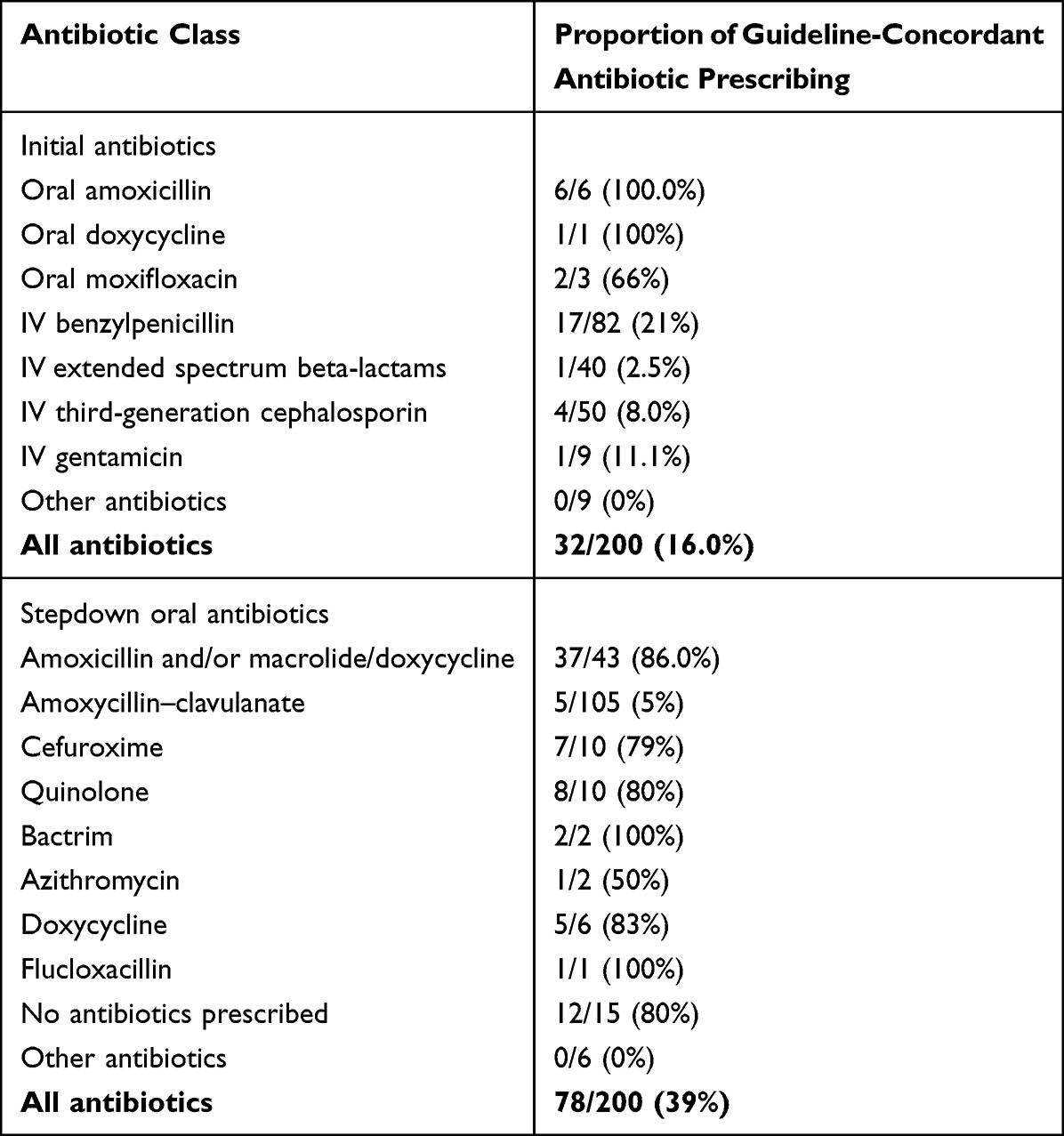 |
Table 3 Proportion of Guideline-Concordant Prescribing in Each Antibiotic Class |
Step-down antibiotic prescribing was guideline concordant in 78 of 200 patients (39.0%) (Table 3). The most frequently prescribed oral antibiotics comprised amoxycillin–clavulanate (86; 43%), amoxycillin and doxycycline combination (34; 17%) and amoxycillin–clavulanate with doxycycline (22; 11%). Guideline concordance ranged from as low as 5% for amoxycillin–clavulanate to 86% for amoxycillin with macrolide or doxycycline. Acceptable deviations comprised ID specialist recommendations (n=13/78, 16%), penicillin allergy (n=11/78, 14%), immunosuppression (n=1/78, 1%) and clinical trial enrolment (n=1/78, 1%). Among the 122 patients with guideline-discordant step-down oral antibiotic prescribing, 115 (94%) had incorrect antibiotics prescribed, 5 (4%) had incorrect dose and 2 (2%) had incorrect duration of therapy (too short or long duration).
Subgroup Analyses
Patients admitted to ICU, receiving NIV or dying in hospital had significantly higher SMART-COP scores compared to other patients (mean [SD] 5.8 [2.8] vs 2.3 [1.9]; p<0.001). In contrast, scores for patients undergoing microbiological investigations were similar to those of non-investigated patients (mean [SD] 2.5 [2.2] vs 2.6 [2.3]; p=0.74). Among patient subgroups (Table 4), initial antibiotic prescribing was more guideline-concordant in those with moderate-to-severe CAP than in mild CAP (20/84, 24% vs 12/116, 10%; p=0.01). Step-down oral antibiotic prescribing was more guideline-concordant in younger than in older patients (40/79, 51% vs 38/121, 31%; p=0.006) and in those with longer than shorter LOS (23/40, 57% vs 55/160, 34%; p<0.001). No significant differences were seen between general medicine and other specialty units in guideline-concordant use of antibiotics.
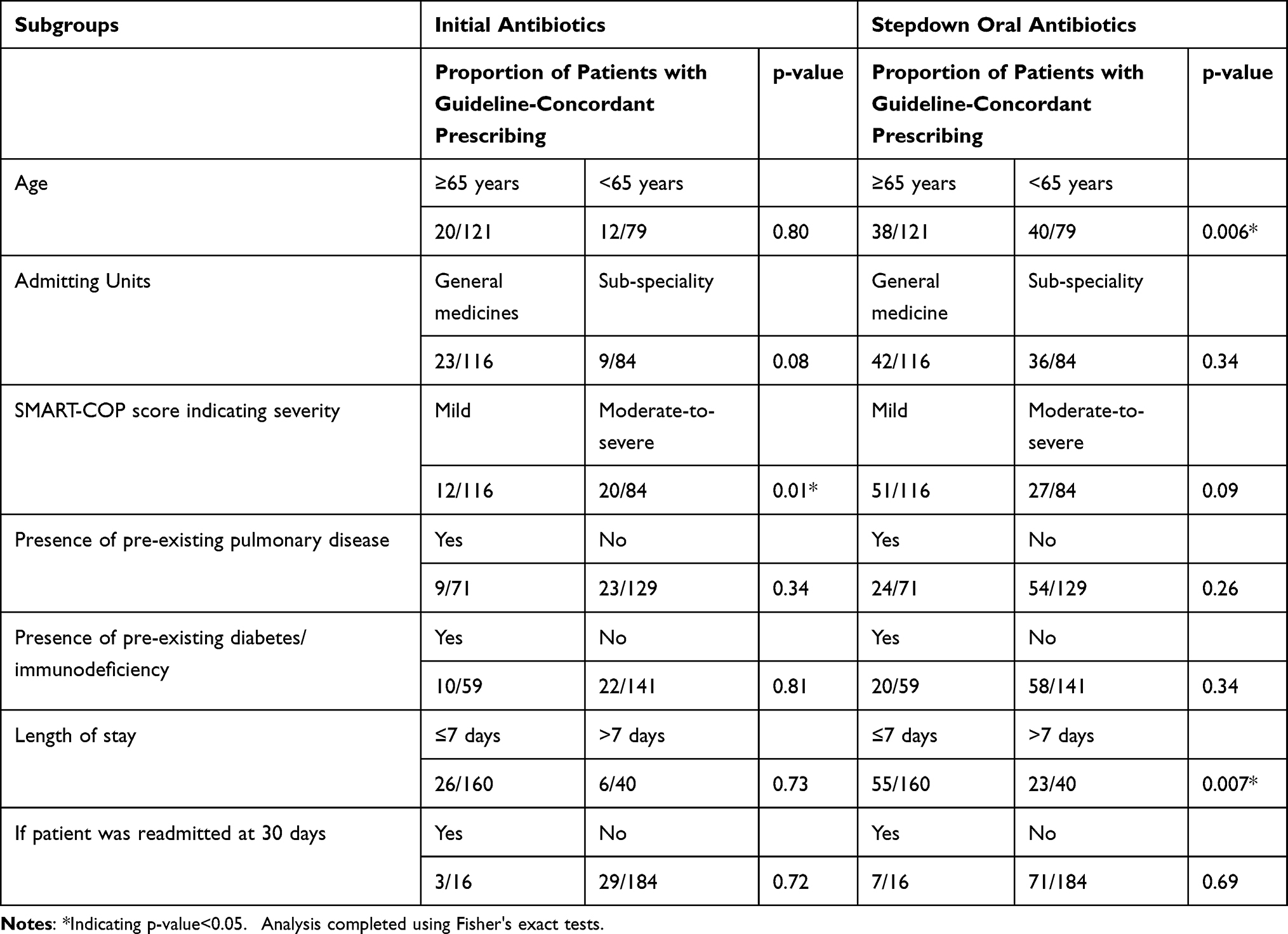 |
Table 4 Subgroup Analyses of Guideline-Concordant Antibiotic Prescribing |
Discussion
The management of CAP is challenging for various reasons. In older, multi-morbid patients, accurate assessment of disease severity may be difficult because of the absence of classical features of high fever or clear-cut radiological signs used to calculate SATs. There is also an array of potential pathogens, more so in older or immunocompromised patients, that can be treated with different antibiotics associated with variable antimicrobial resistance patterns, as indicated by local antibiograms.
Documented use of a SAT to risk stratify patients in this study was low, with the SMART-COP score used in less than 1 in 10 patients. This is similar to observations in other Australian studies.12,15 Explanations may include clinician perceptions of low utility or being unaware of the tools or doubting their predictive accuracy. Notably, the American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA) 2019 guidelines7 and the NICE 2014 guidelines16 recommend their use in conjunction with clinical judgement, and the current Australian Therapeutic Guidelines1 primarily recommend a “red flags” system, while mentioning SMART-COP can also be used.
The SMART-COP score was originally intended to predict the need for respiratory or vasopressor support in admitted patients, with high sensitivity (92%) and negative predictive value (99%).8 However, among older, multi-morbid populations, its predictive accuracy is lower when compared to CURB-65,17 and many of these patients who may not benefit from ICU admission can usually be identified by clinical judgement. The SMART-COP is potentially more useful in younger patients in whom it performs better than the PSI and CURB-65 which tend to underestimate severity.18 While accepting the importance of clinical judgement,19 cognitive bias or other extraneous factors can predispose a clinician to misclassify the disease severity during initial triage.20 In this study, patients with a worse prognosis did demonstrate higher SMART-COP scores and initial antibiotic prescribing was more guideline-concordant among those with moderate-to-severe disease. More consistent use of a SAT in categorising CAP severity may promote higher guideline concordant initial IV antibiotic prescribing, as recommended in several guidelines.1,6,14
In regard to the choice of initial and subsequent antibiotics, our study revealed low concordance with local guidelines: 16% and 39%, respectively, considerably lower than the average 75% of all antibiotic prescribing in patients with CAP observed in a recent Australia-wide hospital survey.21 This significant disparity may relate to more in-depth analysis of medical records, use of more prescriptive local guidelines as the reference standard, and tertiary setting attracting a more at-risk population. However, similar results have been reported elsewhere,12,15 although use of ceftriaxone was much less in our study compared to other reports.15,22 Preferential use of extended spectrum penicillin in the absence of supporting clinical indications, such as febrile neutropenia, is of concern. The overuse of IV antibiotics in mild cases of CAP may relate to clinician misconception of oral antibiotics being less effective, despite evidence of similar efficacy in patients who tolerate oral administration.1
Amoxycillin–clavulanate was frequently used as a step-down oral antibiotic despite its tendency to select out resistant organisms and having more adverse effects than amoxicillin.1 In addition, as strains of S. pneumonia highly resistant to penicillin are seen in less than 2% of the cases,21 its indiscriminate use is unnecessary. The frequent use of amoxycillin–clavulanate as a step-down oral antibiotic might be attributed to clinicians wanting to cover aspiration pneumonia or a perceived increased patient adherence given the reduced frequency (twice daily versus three times daily) compared with amoxicillin. While the choice of antibiotics will depend on local resistance patterns, a penicillin and doxycycline or macrolide are regarded as the most appropriate therapy.1,23 Our observation that older patients received less guideline-concordant oral antibiotics may reflect a clinician perception that “stronger” broad spectrum antibiotics are needed in such patients, as reported in other studies.24,25 The same may apply to patients with shorter LOS in whom clinicians may “play safe” in light of reduced time available to confirm continued clinical stability.
In terms of microbiological investigations, less than 1 in 11 returned a positive result, and only 4 in 100 led to a change in antibiotic therapy. Guideline recommendations for such tests vary considerably (Table 5), with consensus being to reserve blood cultures for patients with fever or other features suggesting moderate-to-severe CAP and to reserve sputum cultures for those productive of purulent phlegm. Serological tests for atypical organisms are not warranted due to long turnaround times and little impact on acute management.
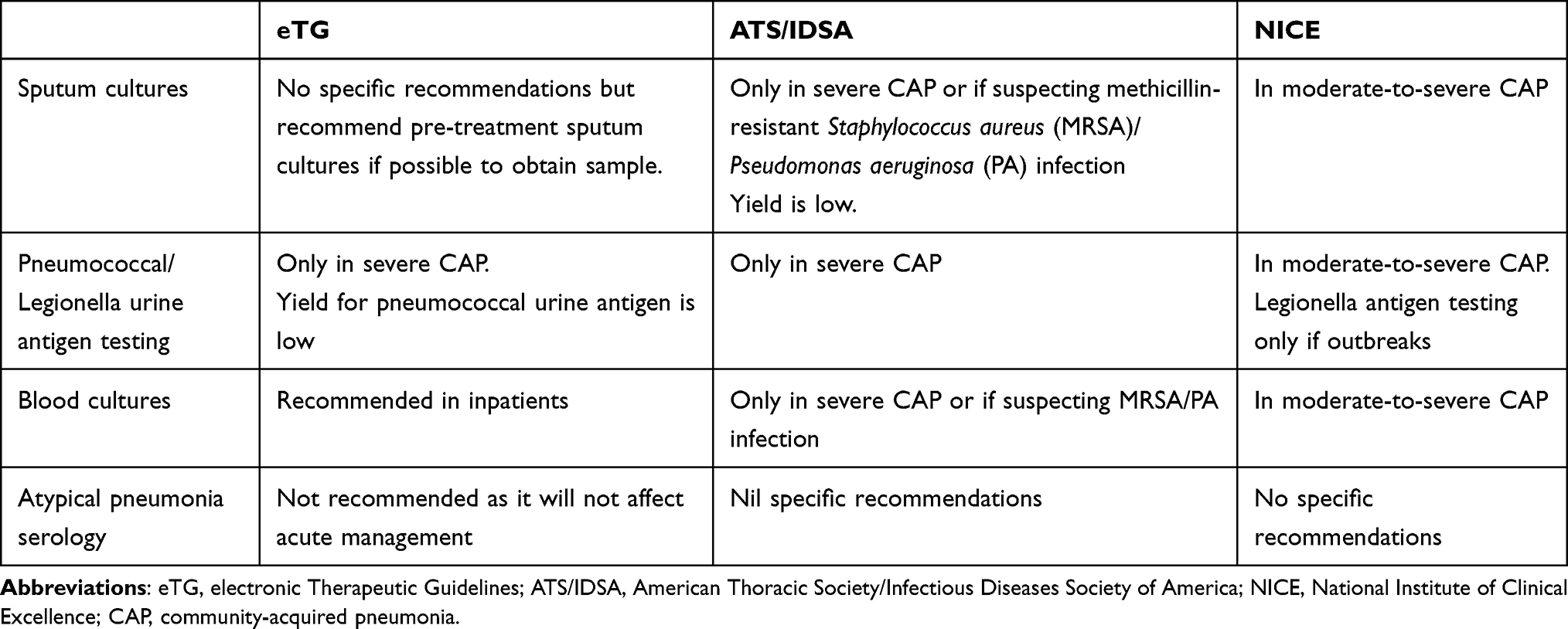 |
Table 5 Guideline Recommendations for Microbiological Investigations |
In this study, both blood and sputum cultures had low yields, consistent with other published data.26–28 Urinary antigen or serological tests were also overused, with half of the tests being ordered in patients with only mild disease. Considering their cost, collection burden for staff, frequently misleading results (eg, false positives from contaminants) and low impact on management, ordering of microbiological investigations should be reserved for more severe CAP or in patients with risk factors.
Study Strengths and Limitations
This study provides a comprehensive analysis of contemporary risk assessment and use of antibiotics and microbial investigations in a large sample of patients with CAP admitted to medical units of a tertiary hospital. Various sub-group analyses have shed additional insights into the differential use of these interventions. It is limited by employing a single centre, retrospective study design reliant on detailed documentation in the medical records and the use of ICD-10 codes to identify suitable patients which may have not captured all cases of CAP. Certain variables (like respiratory rate and presence of confusion) used in the determination of SATs are also highly variable and rely on detailed documentation. Patients who died in the community after discharge from hospital or represented with CAP to private hospitals could not be ascertained. The MSH local antibiotic guidelines, rather than national guidelines, were used as the reference standard for antibiotic concordances as they are heavily promoted to staff, easily accessible electronically, and incorporate local microbiological resistance patterns and epidemiology. However, they do not include recommendations about investigations, and concordance rates for antibiotics might be different if national guidelines had been used.
Implications for Clinical Practice
Standardised, easy-to-implement CAP clinical pathways are needed. They should be based on the current available evidence in the appropriateness of risk assessment, antibiotic use and investigations, but also allow clinicians flexibility according to circumstances, provided justifiable reasons for discordance are documented. Ideally, this pathway should be integrated as a decision support tool into electronic medical records and easily accessible at the point of care to maximise adherence.29,30 Regular audits and peer-referenced feedback on antibiotic use, education campaigns and prompts around the costs of ordering investigations can all promote greater use of pathways31,32 in optimising care and patient safety.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Antibiotic Expert Group. eTG complete. Melbourne: Therapeutic Guidelines Limited; 2019. Available from: http://online.tg.org.au.
2. Australian Institute of Health and Welfare. Hospitals. Canberra: Australian Institute of Health and Welfare; 2021. Available from: https://www.aihw.gov.au/reports-data/myhospitals.
3. Australian Institute of Health and Welfare. Deaths in Australia. Canberra: Australian Institute of Health and Welfare; 2021. Available from: https://www.aihw.gov.au/reports/life-expectancy-death/deaths-in-australia.
4. Johnson PDR, Irving LB, Turnidge JD. Community-acquired pneumonia. Med J Aust. 2002;176(7):341–347. doi:10.5694/j.1326-5377.2002.tb04437.x
5. Tsirgiotis E, Ruffin R. Community acquired pneumonia. A perspective for general practice. Aust Fam Physician. 2000;29(7):639–645.
6. Lim WS, Baudouin SV, George RC, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009;64(Suppl3):iii1–iii55. doi:10.1136/thx.2009.121434
7. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Resp Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
8. Charles PG, Wolfe R, Whitby M, et al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis. 2008;47(3):375–384. doi:10.1086/589754
9. Martínez R, Reyes S, Lorenzo MJ, Menéndez R. Impact of guidelines on outcome: the evidence. Semin Respir Crit Care Med. 2009;30(2):172–178. doi:10.1055/s-0029-1202936
10. Egger ME, Myers JA, Arnold FW, Pass LA, Ramirez JA, Brock GN. Cost effectiveness of adherence to IDSA/ATS guidelines in elderly patients hospitalized for Community-Acquired Pneumonia. BMC Med Inform Decis Mak. 2016;16(1):34. doi:10.1186/s12911-016-0270-y
11. Adler NR, Weber HM, Gunadasa I, Hughes AJ, Friedman ND. Adherence to therapeutic guidelines for patients with community-acquired pneumonia in Australian hospitals. Clinical medicine insights: circulatory. Resp Pulmon Med. 2014;8:
12. Maxwell DJ, McIntosh KA, Pulver LK, Easton KL. Empiric management of community-acquired pneumonia in Australian emergency departments. Med J Aust. 2005;183(10):520–524. doi:10.5694/j.1326-5377.2005.tb07153.x
13. Ramirez JA. Fostering international multicenter collaborative research: the CAPO project. Int J Tuberc Lung Dis. 2007;11(10):1062–1065.
14. MSH Medicines Management Committee. MSHPrescribe. Brisbane: Metro South Health; 2020.
15. Trad MA, Baisch A. Management of community-acquired pneumonia in an Australian regional hospital. Aust J Rural Health. 2017;25(2):120–124. doi:10.1111/ajr.12267
16. Eccles S, Pincus C, Higgins B, Woodhead M. Diagnosis and management of community and hospital acquired pneumonia in adults: summary of NICE guidance. BMJ. 2014;349:g6722. doi:10.1136/bmj.g6722
17. Williams E, Girdwood J, Janus E, Karunajeewa H. CORB is the best pneumonia severity score for elderly hospitalised patients with suspected pneumonia. Intern Med J. 2014;44(6):613–615. doi:10.1111/imj.12445
18. Chalmers JD, Singanayagam A, Hill AT. Predicting the need for mechanical ventilation and/or inotropic support for young adults admitted to the hospital with community-acquired pneumonia. Clin Infect Dis. 2008;47(12):1571–1574. doi:10.1086/593195
19. Choudhury G, Chalmers JD, Mandal P, et al. Physician judgement is a crucial adjunct to pneumonia severity scores in low-risk patients. Eur Resp J. 2011;38(3):643–648. doi:10.1183/09031936.00172910
20. Brown SM, Jones JP, Aronsky D, Jones BE, Lanspa MJ, Dean NC. Relationships among initial hospital triage, disease progression and mortality in community-acquired pneumonia. Respirology. 2012;17(8):1207–1213. doi:10.1111/j.1440-1843.2012.02225.x
21. Australian Commission on Safety and Quality in Health Care. Antimicrobial Use and Resistance in Australia Surveillance System (AURA) Sydney. 2021.
22. Wright AA, Maydom BW. Improving the implementation of community-acquired pneumonia guidelines. Intern Med J. 2004;34(8):507–509. doi:10.1111/j.1445-5994.2004.00638.x
23. Charles PG, Whitby M, Fuller AJ, et al. The etiology of community-acquired pneumonia in Australia: why penicillin plus doxycycline or a macrolide is the most appropriate therapy. Clin Infect Dis. 2008;46(10):1513–1521. doi:10.1086/586749
24. Martínez-González NA, Di Gangi S, Pichierri G, Neuner-Jehle S, Senn O, Plate A. Time trends and factors associated with antibiotic prescribing in Swiss Primary Care (2008 to 2020). Antibiotics. 2020;9(11):837. doi:10.3390/antibiotics9110837
25. Orlando V, Monetti VM, Moreno Juste A, et al. Drug utilization pattern of antibiotics: the role of age, sex and municipalities in determining variation. Risk Manag Healthc Policy. 2020;13:63–71. doi:10.2147/RMHP.S223042
26. Benenson RS, Kepner AM, Pyle DN, Cavanaugh S. Selective use of blood cultures in emergency department pneumonia patients. J Emerg Med. 2007;33(1):1–8. doi:10.1016/j.jemermed.2006.12.034
27. Ewig S, Schlochtermeier M, Göke N, Niederman MS. Applying sputum as a diagnostic tool in pneumonia: limited yield, minimal impact on treatment decisions. Chest. 2002;121(5):1486–1492. doi:10.1378/chest.121.5.1486
28. Lidman C, Burman LG, Lagergren Å, Örtqvist Å. Limited value of routine microbiological diagnostics in patients hospitalized for community-acquired pneumonia. Scand J Infect Dis. 2002;34(12):873–879. doi:10.1080/0036554021000026967
29. Buising KL, Thursky KA, Black JF, et al. Improving antibiotic prescribing for adults with community acquired pneumonia: does a computerised decision support system achieve more than academic detailing alone?--A time series analysis. BMC Med Inform Decis Mak. 2008;8:35. doi:10.1186/1472-6947-8-35
30. Mecham ID, Vines C, Dean NC. Community-acquired pneumonia management and outcomes in the era of health information technology. Respirology. 2017;22(8):1529–1535. doi:10.1111/resp.13132
31. Matuluko A, Macdonald J, Ness V, Currie K. Interventions to improve the review of antibiotic therapy in acute care hospitals: a systematic review and narrative synthesis. JAC Antimicrob Resist. 2020;2(3):dlaa065. doi:10.1093/jacamr/dlaa065
32. Bond SE, Boutlis CS, Yeo WW, Miyakis S. Impact of an antimicrobial stewardship intervention on appropriateness of prescribing for community-acquired pneumonia in an Australian regional hospital. Intern Med J. 2017;47(5):582–585. doi:10.1111/imj.13401
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.