Back to Journals » Clinical Interventions in Aging » Volume 18
Grip Strength is a Predictor for Subsyndromal Delirium Among Older Adults Following Joint Replacement
Authors Qian J ![]() , Shen X
, Shen X ![]() , Gao X, Sun Q
, Gao X, Sun Q
Received 1 June 2023
Accepted for publication 22 September 2023
Published 3 October 2023 Volume 2023:18 Pages 1675—1685
DOI https://doi.org/10.2147/CIA.S423727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Jiawei Qian,1,2 Xiulan Shen,3 Xin Gao,3 Qiuhua Sun2
1Department of Nursing, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2School of Nursing, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 3Emergency and Trauma Center, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
Correspondence: Qiuhua Sun, Email [email protected]
Background: Delirium is common in older patients during the postoperative period, increasing the number of adverse events, and grip strength is associated with delirium. Subsyndromal delirium (SSD) is a prostate of clinical delirium; nevertheless, the relationship between grip strength and SSD has not been elucidated. This study aimed to examine the association between grip strength and SSD in the elderly after arthroplasty.
Methods: A total of 181 patients were recruited from two Chinese hospitals. SSD and delirium were evaluated before the surgery and the first week after surgery using the confusion assessment method. The Mini-mental State Examination was used to assess patients’ cognitive function, and their grip strength was evaluated with an electronic hand dynamometer before surgery. Logistic regression and ROC curve analysis were conducted to determine the odds ratio and predictive value of grip strength for SSD.
Results: The incidence of SSD and postoperative delirium (POD) was 41.44% and 14.36% for the elderly following arthroplasty respectively, and approximately 1/3 of SSD progressed into POD. Older age, declined cognitive function, fall history, and lower grip strength were risk factors for SSD (P< 0.05). The area under the ROC curve of grip strength was 0.863 and 0.900 for males and females respectively, and the cut-off point of it was determined to be 22.050 kg for men and 18.050 kg for women.
Conclusion: SSD and POD are common among older people. Decreased grip strength, advanced age, lower cognitive function, and fall history were independent risk factors for SSD, and grip strength was a significant predictor for SSD in aged patients after the arthroplasty.
Keywords: subsyndromal delirium, delirium, grip strength, risk factor, joint replacement
Introduction
Delirium is an acute neurocognitive dysfunction characterized by fluctuating consciousness and obvious impairment of cognition, such as inattention, disorientation, disorganized thinking, agitation, and delusions1 This condition commonly occurs in older patients during the postoperative period (Postoperative delirium, POD) with a combined incidence of 24%.2 Delirium is recognized as a serious adverse event closely related to various negative consequences, including prolonged hospital admissions, cognitive function decline, and higher mortality, significantly undermining both life span and quality.3 In addition to full delirium syndromes, subsyndromal delirium (SSD), a milder form of delirium has been a topic of interest in recent decades.4,5 SSD is defined by the presence of partial delirium symptoms or a precursory state of clinical delirium but does not yet meet the full diagnostic criteria of delirium.6,7 The incidence of SSD can be highly variable, ranging from 0.9% to 36.5%, and close to delirium, patients who develop SSD are associated with unfavorable outcomes as well, such as extended duration of hospitalization, long-term functional disability, and cognitive impairment.8 Not only that, in previous studies, risk factors of SSD have also been identified as similar to those associated with delirium, like advanced age, preoperative fasting times, psychotropic medications, cognitive impairment, acute stroke, hearing and visual impairment, and frailty.9,10 Consequently, it could be considered that risk factors of delirium could also be intrinsic factors in those of subsyndromal delirium.
Hand grip strength is a very simple and inexpensive way to assess muscle capacity, it has been used widely in recent clinical studies to estimate frailty or muscle mass in older adults.11,12 Although it is generally accepted as a measure of physical or motor function, a growing number of studies have demonstrated its statistically significant relationship to cognition in the elderly.13,14 Moreover, some published studies have shown that low preoperative hand grip strength was an independent predictor of delirium after surgery.15,16 However, there has been a paucity of research on the effect of grip strength before surgery on the occurrence of SSD in older patients undergoing joint replacement so far. Therefore, this study aimed to investigate the association between grip strength and SSD in older patients after joint replacement surgery.
Materials and Methods
Participants
This prospective observational study was undertaken in the orthopedics department of the 903rd Hospital of PLA, Hangzhou, China, and the First Affiliated Hospital of Zhejiang Chinese Medicine University, Hangzhou, China. A total of 181 adults were recruited to complete the research between May 2019 and February 2021. The inclusion criteria for patients were as follows: (1) aged ≥65 years; (2) scheduled to undergo hip or knee joint replacement surgery, both total joint replacement and hemiarthroplasty were involved; (3) able to communicate with the researchers and complete study questionnaires or measurements; (4) voluntarily participated in the study. (5) expected a postoperative hospital stay of at least one week. The exclusion criteria were as follows: (1) patients with severe physical illness and psychiatric disorders, or unstable postoperative vital signs; (2) with SSD, delirium symptoms, or cognitive impairment before the operation; (3) duration of hospital stay less than one week after surgery; (4) dropped out halfway for reasons including death, referring to another department.
Data Collection
Demographic Characteristics and Grip Strength Assessment
In this study, the nursing staff enrolled patients and recorded their demographic data throughout their hospital stay. All participants’ demographic information was collected from the electronic medical records on the day before the surgery, including age, gender, body mass index (BMI), previous medical history, and prior medication use. In addition, surgical sites and anesthesia modes were also recorded. Grip strength assessment: The nursing staff assessed the participants’ hand grip strength before surgery with an electronic hand dynamometer (CAMRY, EH101, SENSSUN, China) with a cut-off point grip strength adjusted for gender and body mass index (BMI), and is defined as the maximum value from 3 attempts with the dominant hand privileged.17
SSD and Delirium Assessment
This research used the Chinese version of the confusion assessment method (CAM) to determine the incidence of SSD and POD. This version has a good intraclass correlation coefficient of 0.91, a sensitivity of 0.90, a specificity of 0.94, and a sensitivity of 0.90, in the cross-validity test, the Kappa value is 0.83 (P<0.01).18 Delirium was diagnosed if CAM criteria were met: (a) acute onset or fluctuating course; (b) impairment of attention; and either (c) disturbing consciousness; or (d) disorganized thinking. While a diagnosis of SSD is based on at least one of the CAM symptoms but does not meet the complete diagnostic criteria for Delirium.19 As part of this study, four psychiatry-trained research nurses assessed SSD and delirium in patients on the day before surgery and 1–7 days after surgery.
Cognitive Function Assessment
The Mini-Mental State Examination (MMSE) was used to detect patients’ cognitive impairment. MMSE consists of 11 items testing five aspects of cognitive function: orientation, registration, attention and calculation, recall, and language. The scale has 30 questions with a maximum score of 30, of which 27–30 is considered normal, and 27 is determined as cognitive impairment.20 The reliability and validity of the Chinese version are excellent, the Cronbach alpha coefficient was 0.833, and the test–retest reliability was 0.924,21 which has been widely used for screening older adults for cognitive impairments in China. The trained nurses assessed cognition levels by MMSE in participants before surgery.
Basic Activities of Daily Living Measurement
The Barthel Index (originally called the Maryland Disability Index) was introduced by Mahoney and Barthel in 1955 and has been widely used for the evaluation of patients’ ability to perform basic activities of daily living.22 The Barthel Index measures 10 items, including bathing, dressing, feeding, personal hygiene, using the toilet, bladder, and bowel control, walking on a level surface, and transfer from chair to bed, giving a total score ranging from 0 (fully dependent) to 100 (fully independent). The structural validity and reliability of the Chinese version were shown to be robust, with kappa statistics ranging from 0.63 to 1.00.23 The research nurses used the Barthel Index to assess patients’ basic activities of daily living before surgery.
Ethical Consideration
The study was approved by the ethics committee of the 903rd hospital of PLA, Hangzhou, China (ethical register number: 201907300401023) and the first affiliated hospital of Zhejiang Chinese Medicine University (ethical register number: 2019-KL-014-01). The procedures for the study were explained to all participants and their relatives, and all the participants provided their written informed consent on the day before the operation.
Statistics
SPSS software version 25.0 was used to analyze the data. Continuous variables were reported as means and standard deviations, while categorical variables were expressed as absolute values and percentages. Continuous variables were analyzed using independent t-tests; non-normal data were compared with Mann–Whitney’s U-test; while categorical data were assessed using chi-squared tests. In univariate analysis, factors with P < 0.05 were included in the multivariate analysis. Then, bivariate logistic regression analyses were conducted to estimate the odds ratio for each independent variable, and the significant risk factors for the occurrence of SSD were investigated. Finally, a ROC curve analysis was used to evaluate the predictive value of grip strength for SSD. A two-sided P<0.05 was considered statistically significant.
Results
Demographic Characteristics and Perioperative Factors
A total of 196 patients who met the inclusion were enrolled in this study, among them, 15 met the exclusion criteria; hence, 181 patients without delirium symptoms and cognition impairment before the operation were thus included in the analysis (Figure 1). All participants were aged ≥ 65 years old, the average age was 75.15 ± 7.54 years, and most were women, accounting for 65.75% (n = 119) of the total. Regarding the surgical sites, 46.41% (n = 84) of patients received knee replacement, and 53.59% (n = 97) received hip replacement. The average grip strength for male and female were 22.66 ± 6.60 kg and 17.50 ± 5.48kg, respectively. At the end of observation, a total of 58.56% (n = 106), 41.44% (n = 75), and 14.36% (n = 26) patients were classified as non-delirious (ND), with SSD (SSD from ND), and with Postoperative delirium (POD from SSD), respectively. In this study, approximately one-third (n = 26, 34.67%) of SSD cases were observed with a status of POD. The demographic characteristics and perioperative factors are summarized in Table 1.
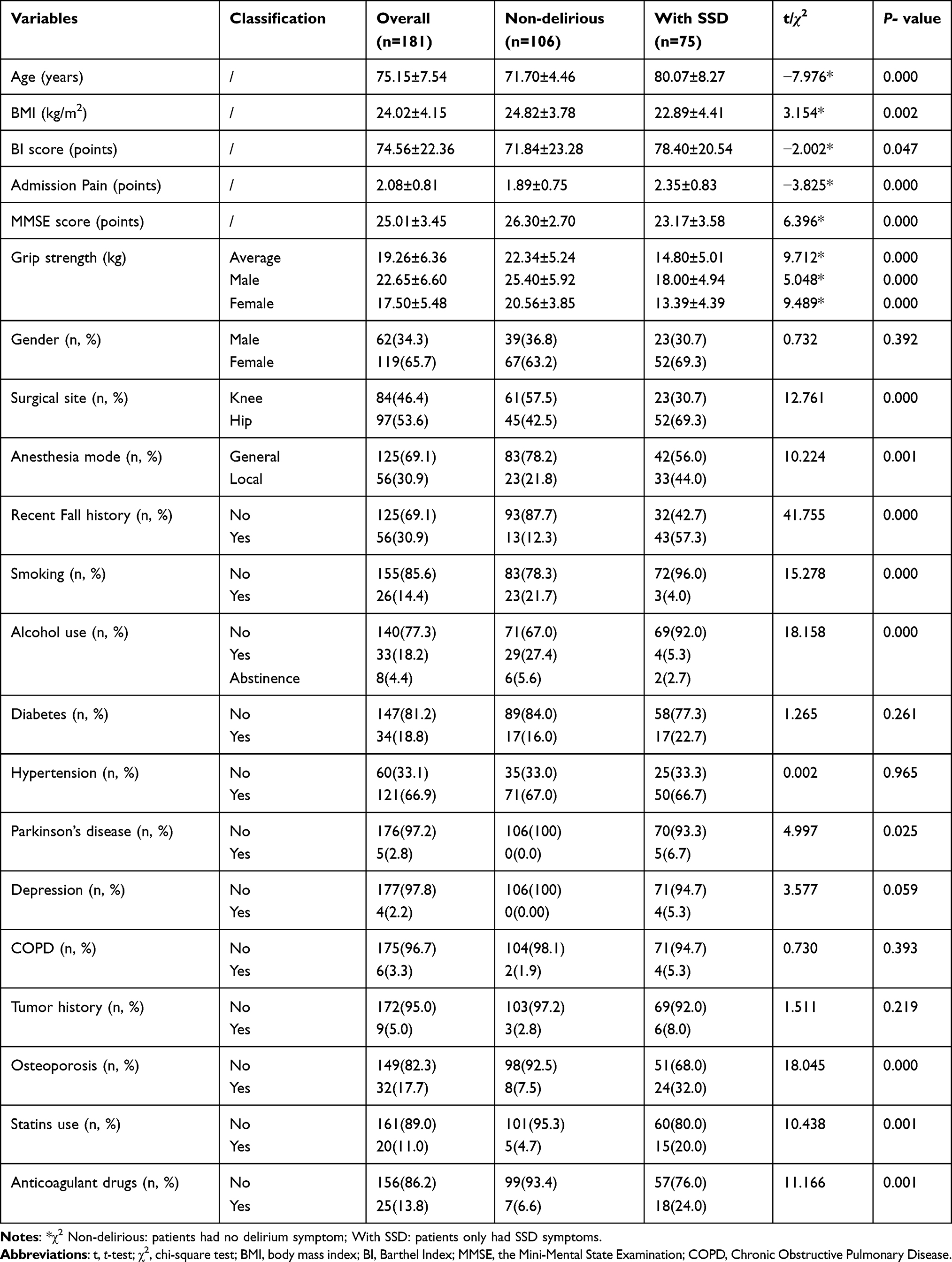 |
Table 1 The Demographic Characteristics and Perioperative Factors |
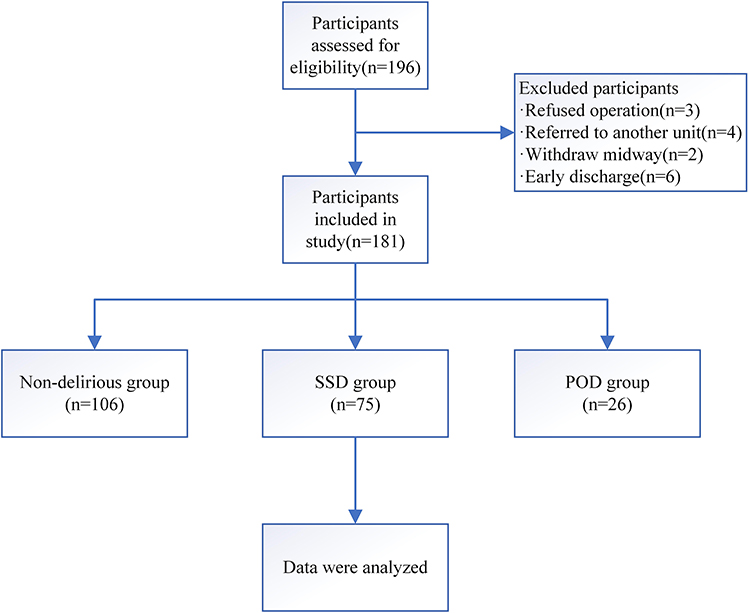 |
Figure 1 Flow diagram of the patient selection process. |
The Risk Factors of Postoperative Subsyndromal Delirium
Significant differences were observed in demographic data between the no delirious and SSD groups, including grip strength, age, BMI, admission pain, MMSE, and BI score (P<0.05). Concerning medical history and prior medication use, fall history, smoking, Parkinson’s disease, osteoporosis, as well as the use of alcohol, statins, and anticoagulant drugs were found to be associated with SSD as well (P<0.05). In addition, operation-related factors are also significantly associated with postoperative SSD according to the surgical site and anesthesia mode (P < 0.01). In this study, multivariate analysis showed that grip strength (P = 0.001), advanced age (P = 0.018), preoperative cognitive function (P=0.006), and fall history within 6 months (P = 0.003) were statistically significant risk factors for the incidence of SSD in elderly after surgery (Table 2).
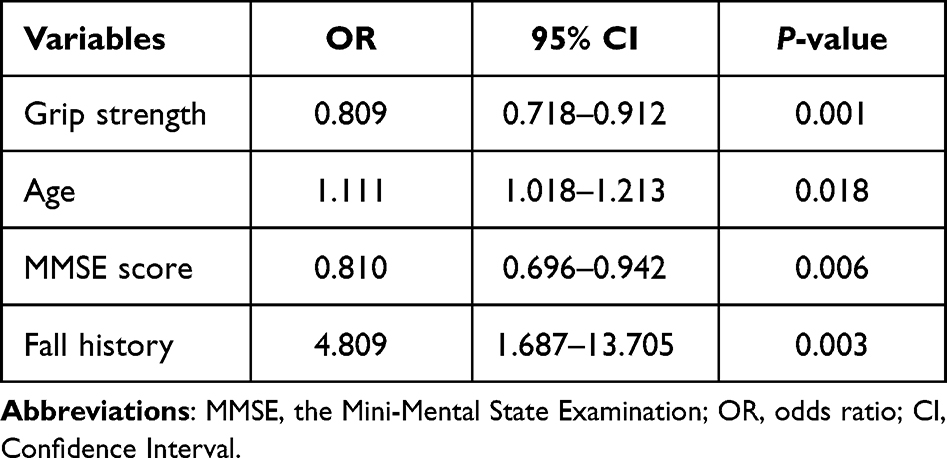 |
Table 2 The Risk Factors of Postoperative Subsyndromal Delirium |
The ROC Curve Analysis for Grip Strength
ROC curve analysis of grip strength showed the area under the ROC curve was 0.863 [95% CI:0.763 to 0.964] (P < 0.001) and 0. 900 [95% CI:0. 846 to 0.954] (P < 0.001) for males and females respectively. The quality of the ROC curve analysis was judged based on the area under the ROC curve value (<0.7, indicating low accuracy; 0.7–0.9, indicating moderate accuracy; >0.9, indicating high accuracy). The cut-off point was determined to be 22.050 kg (men) and 18.050 kg (women) by calculating the maximum of the Youden index, with a sensitivity of 0.744 and a specificity of 0.913 for male patients, and a sensitivity of 0.761 and a specificity of 0. 904 for females. Therefore, in this case, the grip strength has a medium diagnostic value for predicting SSD after the operation (Figures 2 and 3).
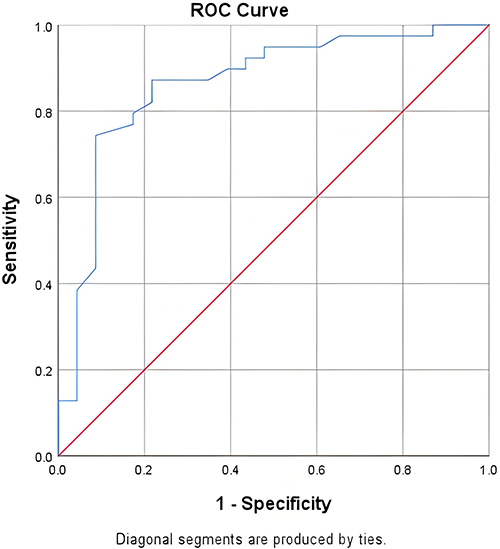 |
Figure 2 ROC curve of male patients. |
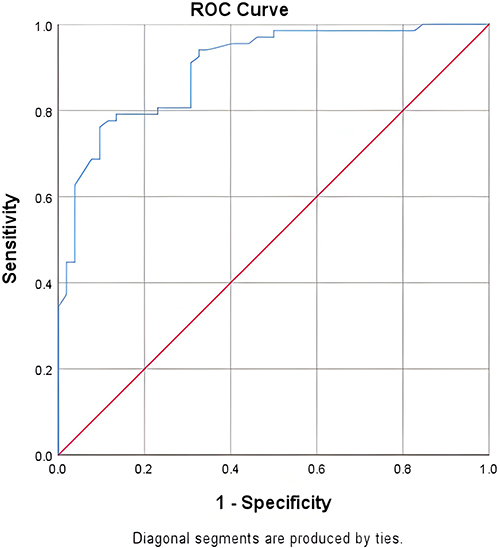 |
Figure 3 ROC curve of female patients. |
Discussion
The current study aimed to investigate the association between preoperative hand grip strength and the occurrence of SSD in older adults after joint replacement. The results indicated that the incidence of SSD and POD after surgery was 41.44% and 14.36% among older adults respectively, with hand grip strength, older age, lower cognition function, and a recent fall history being identified as significant risk factors for the prevalence of postoperative SSD. Furthermore, the ROC curve illustrated that the cutoff point of grip strength could be used to predict a diagnosis of SSD in older patients after joint replacement surgery.
Incidence of SSD and POD in Older Patients After Joint Replacement
The results of the present study showed that the incidence of SSD was 41.44%, which was lower than the rate of 68% reported in another study of patients who underwent total joint replacement (TJR).24 Meanwhile, 26 out of 181 cases (14.36%) were diagnosed with POD, which is comparable to the previous report that 17% of patients developed POD after total joint replacement during hospital admission.25 The lower incidence rate of SSD and POD detected in this study may have been because some participants accepted hemiarthroplasty or minimally invasive surgery instead of TJR, which might decrease the occurrence of SSD or POD after an operation. Besides, a total of 26 (34.67%) patients eventually progressed to POD, and all of them progressed from a state of SSD (POD from SSD). According to the available literature, about 9.5% of patients have been reported progressed from a state of SSD to full delirium.26 This might be due to the differences in diseases, treatment, screening frequency, etc. across the studies. Although SSD is not clinically diagnostic, it has currently been considered a prodromal state of full delirium with a particularly high risk for clinical delirium. This may also imply an increase in morbidity, length of hospital stays, new-onset dementia, and economic and human costs.27,28 Hence, further attention is deserved and early intervention strategies are crucial to reverse the progression from SSD to POD.
The Predictive Value of Grip Strength at the Diagnosis of Postoperative SSD
To the best of our knowledge, this study was probably the first to explore the association between grip strength and SSD in patients after joint replacement. Hand grip strength was evidenced as an independent risk factor for postoperative SSD in this study (P=0.001), which was similar to those of previous studies. Past research has revealed that grip strength was associated with the decline of the aging population’s verbal ability, spatial ability, processing speed, and memory.13 More than that, older people with better grip strength were expected to have less incidence of POD and cognitive impairment, while lower hand grip strength was significantly associated with the development of total dementia or delirium.15,29 This could be due to motor or physical function and certain cognitive functions sharing overlapping neurological processes, or even involving similar physiological mechanisms.11 For instance, lower hand grip strength may reflect systemic inflammation, which has been linked to cognitive decline such as delirium and dementia.29,30 Correspondingly, grip strength testing could be considered a discriminating measurement for neuromuscular function or cognitive decline.14,31 Given that SSD is a prostate of full delirium and acute brain dysfunction associated with long-term cognitive impairment,32 the grip strength could be used as a predictive tool for postoperative SSD in older patients.
In addition to these, the ROC curve analysis revealed that the cut-off point of grip strength was 22.050 kg and 18.050 kg for males and females, respectively. For the relative study was rare, data from an older Japanese group who underwent colorectal cancer surgery were compared. In that study, the cutoff values of grip strength for POD were 21.8 kg for men and 15.4 kg for women, respectively,15 which were partially in line with the present results. This was perhaps because most patients in the current study were people who just needed selective arthroplasties. However, patients in the Japanese report all had cancers, and their general conditions were worse than those patients of in this study. Based on this, women’s hand grip strength seemed more likely to be affected by their poor physical conditions when compared to men. Thus, the cutoff values of the grip strength of female participants in this study were higher than the Japanese data, while men’s were more comparable. Nevertheless, grip strength has a significant diagnostic value both for men and women, and has the potential to be used as a diagnostic marker for the occurrence of SSD after the operation.
Other Risk Factors for SSD in Older Patients Undergo Arthroplasty
A multivariate analysis was conducted to determine the effect of grip strength and other risk factors on the incidence of SSD in older patients undergoing arthroplasty. The results revealed that older age, MMSE score, and fall history are also independent risk factors for SSD with the exception of grip strength. Similar to delirium, SSD is a common geriatric syndrome with a significant negative impact on the health status of older patients.8 The prevalence of SSD was high (36.4%) among older adults in hospital or long-term care (LTC) settings with advanced age has been a well-known independent predictor for SSD.33 In the present study, the average age of the SSD group was relatively high (80.07 ± 8.27 years), almost 10 years older than no delirious patients (71.70 ± 4.46 years), which provided strong supporting evidence for previous research.
In parallel, past research has determined that the onset of SSD is often significantly associated with lower cognitive function5 and that dementia and cognitive impairment were strong pre-disposing factors for SSD or delirium following surgery.34,35 However, patients with severe cognitive impairment were all excluded before surgery in this study. Thus, it can be stated that even a mild decline in cognitive level could deteriorate the brain function of older patients who underwent joint replacement.36 Additionally, some published reports have indicated that a recent fall history was thought to be one of the most frequently occurring risk factors for persons with cognitive impairment like SSD and delirium.24,37 What’s more, the incidence of hospital falls varies between 5.71% and 18%,38 and are generally induced by a decline in lower muscle power and decreased balance control.39 It is partially in line with the finding as was mentioned above that decreased hand grip strength was a strong predictor for postoperative SSD. Concerning falls, unfortunately, more than 30% of inpatient falls result in injuries such as bleeding, swelling, and fractures.40 In this study, approximately 57.3% (43 out of 75 cases) of SSD patients experienced a history of falls in the last 6 months, contributing to a higher possibility of femoral neck and pelvic fractures. The consequent symptoms, such as pain, sedative, trauma, and inflammation could foster the development of SSD and cognition decline.41–43
In addition to these risk factors, other variables, such as pain, low BI score, and chronic alcohol use, are known to increase the risk of POD.34,41,44 However, most of the risk factors for delirium were not associated with SSD in the present study, it could be relevant to advancements in medical technologies, Chinese traditional attitude toward illness, and different healthy habits. For instance, timely analgesia or other analgesic programs have been widely applied to relieve acute pain that may reduce the effect of admission pain on SSD.45 Simultaneously, traditional Chinese culture insists that patients, especially older patients need more care and attention from their family and society, making most patients less preferred to do daily living activities by themselves, which could explain why BI score was not significantly associated with SSD. Further, although chronic alcohol use might increase the risk of delirium symptoms, the rate of heavy drinking seemed very low among older patients in the current survey. These may partially explain why some variables in this study were not risk factors for postoperative SSD.
Limitations
This study has several limitations. Firstly, although the study was conducted in two independent hospitals, it had a limited number of patients due to insufficient research staff and a relatively short study period, which may influence the study results. Furthermore, according to the inclusion criteria, both hemiarthroplasty and total joint replacement surgery were included, resulting in a mixed population of patients. However, the surgical types were not discussed in this study; Besides, the perioperative factors included in the current analysis were also restricted, especially the intraoperative factors. That may have led to the omission of potentially valuable information. Finally, hospital outcomes, such as hospital stays, and postoperative cognition status, were not calculated or assessed in the present study, nor neither long-term neurological function outcomes. Nonetheless, the points mentioned above will be considered in a future study and the results should be further validated through multicenter studies with larger sample sizes.
Conclusion
This study revealed the incidence of SSD and POD was 41.44% and 14.36% among older adults following joint arthroplasty respectively, and nearly 34.67% of SSD patients progressed into POD. Besides, the current study outlined the risk factors for the development of SSD, which were lower hand grip strength, older age, declined cognitive function, and fall history within 6 months. Moreover, the diagnostic value of hand grip strength was examined and the results showed grip strength could be used as a diagnostic marker for postoperative SSD in aged patients independently. These findings indicated the importance of SSD prediction for older patients, providing new ideas for early diagnosis and intervention strategies for the occurrence of SSD among older patients following joint replacement surgery.
Compliance with Ethical Standards
The study has been performed in accordance with the ethical standards as laid down in the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Ethical Approval
The study was approved by the ethics committee of the 903rd hospital of PLA, Hangzhou, China (ethical register number: 201907300401023) and the first affiliated hospital of Zhejiang Chinese Medicine University (ethical register number: 2019-KL-014-01).
Informed Consent
Written informed consent for the publication of their clinical details was obtained from the patients or their families.
Acknowledgment
An unauthorized version of the Chinese MMSE was used by the study team without permission, but has been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Field RR, Wall MH. Delirium: past, present, and future. Semin Cardiothorac Vasc Anesth. 2013;17(3):170–179. doi:10.1177/1089253213476957
2. Ho MH, Nealon JR, Igwe E, et al. Postoperative delirium in older patients: a systematic review of assessment and incidence of postoperative delirium. Worldviews Evid Based Nurs. 2021;18(5):290–301. doi:10.1111/wvn.12536
3. Rollo E, Callea A, Brunetti V, et al. Delirium in acute stroke: a prospective, cross-sectional, cohort study. Eur J Neurol. 2021;28(5):1590–1600. doi:10.1111/ene.14749
4. Qian J, Sun Q. Bibliometrics analysis of subsyndromal delirium. Chin J Pract Nurs. 2019;35(25):1990–1995. doi:10.3760/cma.j.issn.1672-7088.2019.25.014
5. Heesung H, Kwang-Min L, Kyung-Lak S, et al. Incidence and risk factors of subsyndromal delirium after curative resection of gastric cancer. BMC Cancer. 2018;18(1):765. doi:10.1186/s12885-018-4681-2
6. Sepulveda E, Leonard M, Franco JG, et al. Subsyndromal delirium compared with delirium, dementia, and subjects without delirium or dementia in elderly general hospital admissions and nursing home residents. Alzheimers Dement Diagn Assess. 2017;7:1–10. doi:10.1016/j.dadm.2016.11.002
7. Klimiec-Moskal LIS, Lis A, Pera J, et al. Subsyndromal delirium is associated with poor functional outcome after ischaemic stroke. Eur J Neurol. 2019;26:927–934. doi:10.1111/ene.13912
8. Cole MG, Ciampi A, Belzile E, et al. Subsyndromal delirium in older people: a systematic review of frequency, risk factors, course and outcomes. Int J Geriatr Psychiatry. 2013;28(8):771–780. doi:10.1002/gps.3891
9. Denny DL, Lindseth GN. Pain, opioid intake, and delirium symptoms in adults following joint replacement surgery. West J Nurs Res. 2020;42(3):165–176. doi:10.1177/0193945919849096
10. Yam KK, Shea YF, Chan TC, et al. Prevalence and risk factors of delirium and subsyndromal delirium in Chinese older adults: delirium and subsyndromal delirium. Geriatr Gerontol Int. 2018;18:1625–1628. doi:10.1111/ggi.13545
11. Hooyman A, Malek‐Ahmadi M, Fauth EB, et al. Challenging the relationship of grip strength with cognitive status in older adults. Int J Geriatr Psychiatry. 2021;36(3):433–442. doi:10.1002/gps.5441
12. Fried LP, Tangen CM, Walston J. Frailty in older adults evidence for a phenotype. J Gerontol. 2001;56(3):M146–M157. doi:10.1093/gerona/56.3.M146
13. Stern NGO, Reynolds CA, Finkel D, et al. Grip strength and cognitive abilities: associations in old age. J Gerontol Seri B. 2016;71(5):841–848. doi:10.1093/geronb/gbv017
14. Sprague BN, Phillips CB, Ross LA. Age-varying relationships between physical function and cognition in older adulthood. J Gerontol. 2019;74(5):772–784. doi:10.1093/geronb/gbx126
15. Asami A, Hidekazu T, Takayuki O, et al. Grip strength as a predictor of postoperative delirium in patients with colorectal cancers. Anna Gastroenterol Surg. 2021;6(2):265–272. doi:10.1002/ags3.12519
16. Kotani T, Ida M, Inoue S, et al. Association between preoperative hand grip strength and postoperative delirium after cardiovascular surgery: a retrospective study. J Clin Med. 2023;12(7):2705. doi:10.3390/jcm12072705
17. Wirth R, Klimek CN, Lueg G, et al. Acute disease induced cognitive dysfunction in older patients – an unrecognized syndrome. BMC Geriatr. 2022;22(1):1–7. doi:10.1186/s12877-022-03323-w
18. Qian J, He M, Zhan X, et al. Transcutaneous electrical acupoint stimulation combined with an integrated perioperative nursing program prevents subsyndromal delirium in older patients after joint replacement. Geriatr Nurs. 2023;49:199–206. doi:10.1016/j.gerinurse.2022.12.010
19. Adamis D, Treloar A, Martin FC, et al. A brief review of the history of delirium as a mental disorder. Hist Psychiatry. 2007;18(4):459–469. doi:10.1177/0957154X07076467
20. Folstein MF, Folstein SE, Mchugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
21. Zhou X. A Preliminary Study of the Validity and Reliability of the Chinese Version of Mini-Mental State of Examination in Stroke Patients. Fujian Chinese Medical University; 2015. doi:10.7666/d.Y2807907
22. Mahoney FL. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65.
23. Leung SO, Chan CC, Shah S. Development of a Chinese version of the modified Barthel index validity and reliability. Clin Rehabil. 2007;21(10):912–922. doi:10.1177/0269215507077286
24. Denny DL, Lindseth G. Preoperative risk factors for subsyndromal delirium in older adults who undergo joint replacement surgery. Orthop Nurs. 2017;36(6):402–411. doi:10.1097/NOR.0000000000000401
25. Scott JE, Mathias JL, Kneebone AC. Incidence of delirium following total joint replacement in older adults: a meta-analysis. Gen Hosp Psychiatry. 2015;37(3):223–229. doi:10.1016/j.genhosppsych.2015.02.004
26. Yamada C, Iwawaki Y, Harada K, et al. Frequency and risk factors for subsyndromal delirium in an intensive care unit. Intensive Crit Care Nurs. 2018;47:15–22. doi:10.1016/j.iccn.2018.02.010
27. Miller RR, Ely EW. Delirium and cognitive dysfunction in the intensive care unit. Semin Respir Crit Care Med. 2006;27(3):210–220. doi:10.1055/s-2006-945532
28. Greene Nathaniel H, Attix Deborah K, Weldon BC, et al. Measures of executive function and depression identify patients at risk for postoperative delirium. Anesthesiology. 2009;110(4):788–795. doi:10.1097/ALN.0b013e31819b5ba6
29. Hatabe Y, Shibata M, Ohara T, et al. Decline in handgrip strength from midlife to late-life is associated with dementia in a Japanese community: the hisayama study. J Epidemiol. 2020;30(1):15–23. doi:10.2188/jea.JE20180137
30. Munster B, Aronica E, Zwinderman AH, et al. Neuroinflammation in delirium: a postmortem case-control study. Rejuvenation Res. 2011;14(6):615–622. doi:10.1089/rej.2011.1185
31. Li C, Sun L, Shao L. Research progress on physical activity of hospitalized elderly. Chin Nurs Res. 2023;37(7):1181–1185. doi:10.12102/j.issn.1009-6493.2023.07.010
32. Meagher D, O’regan N, Ryan D, et al. Frequency of delirium and subsyndromal delirium in an adult acute hospital population. Br J Psychiatry. 2014;205(6):478–485. doi:10.1192/bjp.bp.113.139865
33. Gao Y, Gao R, Yang R, et al. Prevalence, risk factors, and outcomes of subsyndromal delirium in older adults in hospital or long-term care settings: a systematic review and meta-analysis. Geriatr Nurs. 2022;45:9–17. doi:10.1016/j.gerinurse.2022.02.021
34. Kanno M, Doi M, Kubota K, et al. Risk factors for postoperative delirium and subsyndromal delirium in older patients in the surgical ward: a prospective observational study. PLoS One. 2021;16(8):e0255607. doi:10.1371/journal.pone.0255607
35. Fong TG, Inouye SK. The inter-relationship between delirium and dementia: the importance of delirium prevention. Nat Rev Neurol. 2022;18(10):579–596. doi:10.1038/s41582-022-00698-7
36. Itagaki A, Sakurada K, Matsuhama M, et al. Impact of frailty and mild cognitive impairment on delirium after cardiac surgery in older patients. J Cardiol. 2020;76(2):147–153. doi:10.1016/j.jjcc.2020.02.007
37. Sillner AY, Holle CL, Rudolph JL. The overlap between falls and delirium in hospitalized older adults: a systematic review. Clin Geriatr Med. 2019;35(2):221–236. doi:10.1016/j.cger.2019.01.004
38. C S. Interventions for preventing falls in older people in care facilities and hospitals. Orthop Nurs. 2014;33(1):48–49. doi:10.1097/NOR.0000000000000023
39. W Y, Ge L, Heng BH, et al. Association between patient-reported functional measures and incident falls. Sci Rep. 2021;11(1):5201. doi:10.1038/s41598-021-84557-3
40. Hitcho EB, Krauss MJ, Birge S, et al. Characteristics and circumstances of falls in a hospital setting: a prospective analysis. J Gen Intern Med. 2004;19(7):732–739. doi:10.1111/j.1525-1497.2004.30387.x
41. Feast AR, Nicola W, Kathryn L, et al. Pain and delirium in people with dementia in the acute general hospital setting. Age Ageing. 2018;47(6):841–846. doi:10.1093/ageing/afy112
42. Sugita Y, Miyazaki T, Shimada K, et al. Correlation of nutritional indices on admission to the coronary intensive care unit with the development of delirium. Nutrients. 2018;10(11):1712. doi:10.3390/nu10111712
43. Mller A, Hofen-Hohloch JV, Mende M, et al. Long-term cognitive impairment after ICU treatment: a prospective longitudinal cohort study (Cog-I-CU). Sci Rep. 2020;10(1):15518. doi:10.1038/s41598-020-72109-0
44. Gravante F, Giannarelli D, Pucci A, et al. Prevalence and risk factors of delirium in the intensive care unit: an observational study. Nurs Crit Care. 2021;26(3):156–165. doi:10.1111/nicc.12526
45. Foran SE, Carr DB, Lipkowski AW, et al. A substance P-opioid chimeric peptide as a unique nontolerance-forming analgesic. Proc Natl Acad Sci. 2000;97(13):7621–7626. doi:10.1073/pnas.130181897
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Risk Factors and Development of a Predictive Model for Delirium in ICU Patients: Construction, Validation, and Clinical Implications
Li X, Zhang W, Wang T, Qiu Z, Sun X, Qu W, Zhang G
International Journal of General Medicine 2025, 18:3727-3737
Published Date: 5 July 2025