Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Granular Parakeratosis of the Eccrine Ostium: A Case Report
Authors Sriprachya-anunt S, Rutnin S ![]() , Suchonwanit P
, Suchonwanit P ![]()
Received 12 May 2023
Accepted for publication 4 July 2023
Published 13 July 2023 Volume 2023:16 Pages 1807—1810
DOI https://doi.org/10.2147/CCID.S421152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Sittha Sriprachya-anunt, Suthinee Rutnin, Poonkiat Suchonwanit
Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Poonkiat Suchonwanit, Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Ratchathewi, Bangkok, Thailand, 10400, Tel +66-2-2011141, Fax +66-2-201-1211 ext 4, Email [email protected]
Abstract: Granular parakeratosis (GP) is a unique keratotic disorder that often affects the intertriginous areas. GP usually presents as erythematous or brownish hyperkeratotic papules or plaques and can be further classified into five types. GP of the eccrine ostium is a rare subtype; its pathological defects are mainly localized to the stratum corneum of the eccrine ostia. Due to its rarity, there is usually a delay in diagnosing GP, and these patients are often misdiagnosed with other dermatological conditions. In this report, we present the case of a 64-year-old Thai female who presented with recurrent pruritic erythematous rashes on her neck since approximately 40 years. She was previously diagnosed with eczema or folliculitis. Histopathological examination confirmed a final diagnosis of GP of the eccrine ostium. She was advised to avoid excessive heat and keep her intertriginous areas dry. Her condition improved significantly during the follow-up visit.
Keywords: flexural area, granular parakeratosis, hyperkeratosis, keratinization disorder, keratotic papules, sweat gland
Introduction
Granular parakeratosis (GP) is an uncommon dermatological disorder due to abnormal keratinization, with an incidence of 0.005%.1,2 The clinical presentations include brownish to erythematous papules that sometimes coalesce into plaques, mainly on the intertriginous areas.3 Because of its clinical characteristics and benign nature, GP is usually misdiagnosed, and the correct diagnosis may be delayed for up to 20 years.4 In this case report, we present a case of GP of the eccrine ostium, a rare type of GP, which was definitely diagnosed almost four decades after the initial presentation of the disease.
Case Presentation
A 64-year-old Thai female visited the dermatology clinic with a 4-day history of an itchy erythematous rash on her neck. She reported experiencing the same manifestations since her twenties, with a frequency of up to three to four episodes in some years. The lesions tended to be stimulated by hot climate and profuse sweating and resolved spontaneously or after the application of topical medications. Having been previously diagnosed with either eczema or folliculitis with similar presentations, she initially received topical and oral medications from a local pharmacy to manage her symptoms. However, the lesions did not improve despite a 3-day treatment with topical pimecrolimus and oral clindamycin 300 mg twice daily. She reported that her mother also suffered from the same condition but to a milder degree. The underlying conditions included hypertension, dyslipidemia, type-2 diabetes mellitus, allergic rhinitis, major depressive disorder, non-alcoholic steatohepatitis, and myasthenia gravis.
Dermatological examination revealed multiple discrete brownish spiny keratotic papules and scaly erythematous papules on the neck (Figure 1A and B). No obvious skin lesions were observed on the axillae of the patient. Histological analysis revealed a mild epidermal hyperplasia with focal mound parakeratosis. Higher magnification showed that parakeratotic corneocytes contain multiple basophilic granules, similar to keratohyalin granules. These features were prominent in the stratum corneum of the eccrine ostia (Figure 2A and B).
 |
Figure 1 Clinical presentations: multiple erythematous to brownish spiny keratotic papules on the neck at the initial visit (A and B). |
 |
Figure 2 Histopathology: (A) mild epidermal hyperplasia with focal mound parakeratosis (hematoxylin-eosin, x100). (B) Higher magnification showed parakeratotic corneocytes with retained keratohyalin granules, which were more prominent around the eccrine ostia (hematoxylin-eosin, x400). |
Based on the clinical manifestations and histopathological findings, the patient was diagnosed with GP of the eccrine ostium. She was advised to avoid excessive heat and keep her intertriginous areas dry. At the 2-week follow-up visit, the lesions significantly improved (Figure 3A and B).
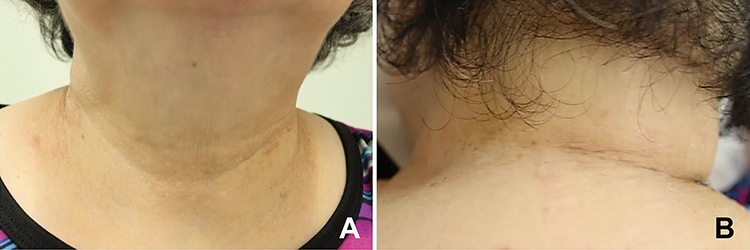 |
Figure 3 Significant improvement of the lesions at the 2-week follow-up visit (A and B). |
Discussion
First described by Northcutt in 1991, GP is a rare acquired disorder of epidermal keratinization.2,3 It is usually found in the adult population, although children as young as 3 months of age have been reported to have such a condition.5,6 Females are more commonly affected than men.1 GP usually presents as erythematous to brownish hyperkeratotic papules or plaques, mainly affecting intertriginous areas. In a recent systematic review of 129 patients with GP from 60 studies, the axilla was found to be the most commonly affected area (56.5%), followed by the groins (31.8%), inter/submammary areas (10.9%), and anogenital areas (10.1%). The neck, as in our case, was affected in 7% of all cases.4
GP has been found to be associated with obesity, heat, sweating, friction, and topical agents such as zinc oxide, deodorants, and benzalkonium chloride.7–9 In terms of pathogenesis, the primary defect is in the processing of profilaggrin to filaggrin during keratinocyte cornification, resulting in failure to degrade keratohyalin granules.2 Altered proliferation and maturation of the epidermis are thought to be triggered and stimulated by the aforementioned factors.10,11 GP is also reported to be associated with other dermatological and systemic conditions such as ichthyosis, atopic dermatitis, dermatomyositis, molluscum contagiosum, fungal infection, and cancers.9,12–18
A recent report by Chirasuthat et al proposed the classification of GP into 5 types based on clinical presentations and histopathological findings. These include intertriginous GP, GP of the eccrine ostium, follicular GP, GP acanthoma, and incidental GP. As in our case, GP of the eccrine ostium usually presents with multiple brownish spiny keratotic papules on the neck with a tingling sensation when sweating. This is generally triggered by hot environments and excessive sweating. A histopathological study demonstrated parakeratotic corneocytes containing keratohyalin granules, which usually localize to the stratum corneum of the eccrine ostia.12
Owing to its diverse clinical presentations, GP may be misdiagnosed as other dermatological conditions, such as eczema, contact dermatitis, Darier’s disease, confluent and reticulated papillomatosis, epidermal nevus, folliculitis, or fungal infection. Moreover, routine biopsy may not be performed in such patients because of the benign nature of GP. As a result, GP is thought to be underrecognized. There is usually a delay in diagnosis, with a mean duration of 19.2 months and a range of up to 20 years from the first presentation of the condition.4,19 In our case, the patient reported experiencing itchy erythematous lesions similar to her current presentation since the age of 25 years. A review of her dermatologic outpatient visits revealed diagnoses of either eczema or folliculitis on multiple occasions, which were subsequently treated with topical corticosteroids or antifungals. Due to multiple recurrences of her condition, a skin biopsy was eventually performed, which revealed a diagnosis of GP.
In terms of prognosis, GP is usually self-limiting and improves after discontinuation or avoidance of the triggering factors. A recent systematic review reported that the condition spontaneously resolves in 4.7% of cases.4 Several treatment options have been attempted with variable responses. These include topical corticosteroids, vitamin D analogues, retinoids, ammonium lactate, antifungals, oral isotretinoin, cryotherapy, and laser therapy.2,3,20–25 Our patient’s lesions resolved spontaneously. She was prescribed topical corticosteroids when she experienced itchiness, advised to avoid excessive sweating, and was kept dry. However, it is important to note that this case report has some limitations, including relying on anecdotal evidence from a single case and lacking generalizability.
Conclusion
We present a case of granular parakeratosis of the eccrine ostium, a rare keratotic disorder, in a patient who had suffered from the condition for almost 4 decades before the correct diagnosis was confirmed. Its recurrent and benign nature often results in GP being under-recognized and misdiagnosed as other conditions such as eczema or folliculitis. This report also highlights the importance of histopathological examination, which can help distinguish GP from other dermatological disorders with similar presentations and prevent delays in establishing a correct diagnosis.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical review and approval were not required to publish case details in accordance with local legislation and institutional requirements. Written informed consent was obtained from the patient for publication of this case report and any accompanying images according to our standard institutional rules.
Funding
No sources of funding were used to prepare this manuscript.
Disclosure
The authors declare that this article was prepared in the absence of any commercial or financial relationships that could be construed as potential conflict of interest.
References
1. Scheinfeld NS, Mones J. Granular parakeratosis: pathologic and clinical correlation of 18 cases of granular parakeratosis. J Am Acad Dermatol. 2005;52(5):863–867. doi:10.1016/j.jaad.2004.12.031
2. Metze D, Rutten A. Granular parakeratosis: a unique acquired disorder of keratinization. J Cutan Pathol. 1999;26(7):339–352. doi:10.1111/j.1600-0560.1999.tb01855.x
3. Northcutt AD, Nelson DM, Tschen JA. Axillary granular parakeratosis. J Am Acad Dermatol. 1991;24(4):541–544. doi:10.1016/0190-9622(91)70078-G
4. Ip HK, Li A. Clinical features, histology, and treatment outcomes of granular parakeratosis: a systemic review. Int J Dermatol. 2022;61(8):973–978. doi:10.1111/ijd.16107
5. Neri I, Patrizi A, Guerrini V, et al. Granular parakeratosis in a child. Dermatology. 2003;206(2):177–178. doi:10.1159/000068454
6. Pimentel DRN, Michalany N, Morgado de Abreu MAM, et al. Granular parakeratosis in children: case report and review of literature. Pediatr Dermatol. 2003;20(3):215–220. doi:10.1046/j.1525-1470.2003.20306.x
7. Ding CY, Liu H, Khachemoune A. Granular parakeratosis: a comprehensive review and a critical reappraisal. Am J Clin Dermatol. 2015;16(6):495–500. doi:10.1007/s40257-015-0148-2
8. Kossard S, White A. Axillary granular parakeratosis. Australas J Dermatol. 1998;39(3):186–187. doi:10.1111/j.1440-0960.1998.tb01280.x
9. Robinson AJ, Foster RS, Halbert AR, et al. Granular parakeratosis induced by benzalkonium chloride exposure from laundry rinse aids. Australas J Dermatol. 2017;58(3):138–140. doi:10.1111/ajd.12551
10. Martorell A, Sanmartin O, Hueso-Gabriel L, et al. Granular parakeratosis: disease or reactive response? Actas Dermosifiliogr. 2011;1(102):72–74. doi:10.1016/j.ad.2010.04.014
11. Wallace CA, Pichardo RO, Yosipovitch G, et al. Granular parakeratosis: a case report and literature review. J Cutan Pathol. 2003;30(5):332–335. doi:10.1034/j.1600-0560.2003.00066.x
12. Chirasuthat P, Chirasuthat S, Suchonwanit P. Follicular granular parakeratosis: a case report, literature review, and proposed classification. Skin Appendage Disord. 2021;7(2):144–148. doi:10.1159/000512950
13. Resnik KS, DiLeonardo M. Incidental granular parakeratosis associated with dermatomyositis. Am J Dermatopathol. 2007;29(3):264–269. doi:10.1097/DAD.0b013e3180465860
14. Suchonwanit P, McMichael AJ. Alopecia in Association with Malignancy: a Review. Am J Clin Dermatol. 2018;19(6):853–865. doi:10.1007/s40257-018-0378-1
15. Pock L, Cermakova A, Zipfelová J, et al. Incidental granular parakeratosis associated with molluscum contagiosum. Am J Dermatopathol. 2006;28(1):45–47. doi:10.1097/01.dad.0000157448.54281.d9
16. Resnik KS, Kantor GR, DeLeonardo M. Dermatophyte-related granular parakeratosis. Am J Dermatopathol. 2004;26(1):70–71. doi:10.1097/00000372-200402000-00011
17. Suchonwanit P, Kositkuljorn C, Pomsoong C. Alopecia areata: an autoimmune disease of multiple players. Immunotargets Ther. 2021;10:299–312. doi:10.2147/itt.S266409
18. Resnik KS, DiLeonardo M. Incidental granular parakeratotic cornification in carcinomas. Am J Dermatopathol. 2007;29(3):264–269.
19. Reddy S, Swarnalata G, Mody T. Intertriginous granular parakeratosis persisting for 20 years. Indian J Dermatol Venereol Leprol. 2008;74(4):405–407. doi:10.4103/0378-6323.42928
20. Chamberlain AJ, Tam MM. Intertriginous granular parakeratosis responsive to potent topical corticosteroids. Clin Exp Dermatol. 2003;28(1):50–52. doi:10.1046/j.1365-2230.2003.01159.x
21. Suchonwanit P, Iamsumang W, Leerunyakul K. Topical finasteride for the treatment of male androgenetic alopecia and female pattern hair loss: a review of the current literature. J Dermatolog Treat. 2022;33(2):643–648. doi:10.1080/09546634.2020.1782324
22. Contreras ME, Gottfried LC, Bang RH, et al. Axillary intertriginous granular parakeratosis responsive to topical calcipotriene and ammonium lactate. Int J Dermatol. 2003;42(5):382–383. doi:10.1046/j.1365-4362.2003.01722.x
23. Brown SK, Heilman ER. Granular parakeratosis: resolution with topical tretinoin. J Am Acad Dermatol. 2002;47(5):s279–280. doi:10.1067/mjd.2002.109252
24. Webster CG, Resnik KS, Webster GF. Axillary granular parakeratosis: response to isotretinoin. J Am Acad Dermatol. 1997;37(5):789–790. doi:10.1016/S0190-9622(97)70119-1
25. Laimer M, Emberger M, Brunasso AM, et al. Laser for the treatment of granular parakeratosis. Dermatol Surg. 2009;35(2):297–300. doi:10.1111/j.1524-4725.2008.01052.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.