")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
GPs in UK: From Health Gatekeepers in Primary Care to Health Agents in Primary Health Care
Received 27 April 2023
Accepted for publication 1 September 2023
Published 20 September 2023 Volume 2023:16 Pages 1929—1939
DOI https://doi.org/10.2147/RMHP.S416934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Ying-Nan Bi, Yu-An Liu
School of Political Science and Public Administration, Shandong University, Qingdao, People’s Republic of China
Correspondence: Ying-Nan Bi, Email [email protected]
Abstract: After 75 years of reformed practice, general practitioners (GPs) in the UK have transformed from health gatekeepers who simply provide medical decision-making such as diagnostic and treatment services and referral services, to health agents who proactively provide more relevant health services such as immunizations, health monitoring and health management, etc. In order to discuss this transformation of the role of the general practitioner and the conditions for the evolution of the role, this study chose the documentary analysis method to provide a comprehensive overview of the legal and normative documents related to the general practitioner. Furthermore, this study uses a comparative analysis method to conclude the definition and role characteristics of GPs as health agents. This study summarises the general pattern of evolution of GPs into health agents. The transformation into a health agent relies on the interpersonal trust and rigorous institutional of society on the general practitioner system. The expansion of GPs’ clientele and range of services, together with the motivation to proactively provide services, have combined to push for a “qualitative change” in the GP’s role as health agent. The transformation of the role of the general practitioner to a health agent is a historical necessity. It responds to the evolution of society’s understanding of health and the need for higher levels of health. Therefore, recognizing the role of GPs as health agents is important for optimizing the use of health care resources and improving the health of society by taking advantage of this role.
Keywords: general practitioner, health agent, health gatekeeper
Introduction
As an important providers of primary care services, general practitioners (GPs) are often likened to gatekeepers of health. A gatekeeper is a person or policy that acts as an intermediary, who can control access from one point to another. According to this definition, the GPs as gatekeeper of health is the intermediary between primary-level and secondary-level health care services.1 As the first doctor to see a patient in healthcare, the main job of GPs is to arrange treatment or referral based on the patient’s initial diagnosis. The UK was one of the first countries in the world to establish a system of GPs involvement in primary care.2 In 1948, based on the Beveridge report, the National Health Service (NHS) was established in the UK by implemented the system of first visit by GPs and hierarchical medical system. In the more than 70 years since the founding of the NHS, the principle of first consultation by a general practitioner has been strictly implemented and GPs have always been recognized as the health gatekeepers. However, the fact is that the job description and job duties of GPs are very different from what they were more than 70 years ago. In addition to initial consultation and referral, more duties are required to be exercised by GPs, such as disease prevention,3 chronic disease management,4 health promotion,5 disease screening,6 etc. At this point, it seems that the health gatekeeper in primary care no longer adequately describes the general practitioner,7 which is evolving towards another role - a health agent in primary health care. This paper will reveal the role evolution process of GPs - from the role of health gatekeeper to health agent - through the perspective of responsibility evolution and will discuss the conditions and implications of this evolution.
Materials and Methods
This research is a classic case study. The reason for choosing GPs in the UK to analyse the changing role of the GPs is that the GPs system has been at the heart of the NHS for over 75 years of its existence, and the whole system is well developed and without interruption. In order to discuss the changing role of the GPs, this case study provides a comprehensive review of the history of GPs in the UK and analyses the changing role of GPs from a historical evolutionary perspective. The documentary analysis preferred for this research was a comprehensive review of the legal and regulatory documents dealing with the duties of GPs. These documents were all sourced from the Legislation.gov.uk and England.nhs.uk website, which are managed by the Federation Archives and NHS England board, respectively. Secondly, this study used a comparative analysis to compare the different roles of GPs. From the comparison, characteristics and definitions of the role of the GP as a health agent were generalized.
From Health Gatekeeper in Primary Care to Health Agent in Primary Health Care
Agent is a proper noun derived from principal-agent relationship which widely discussed and studied in different fields such as law, finance, accounting and economics,8 and even in the field of medical decision-making.9 In a principal-agent relationship, which usually occurs in specialized areas where there is a knowledge gap, the agent acts on behalf of the principal and should represent the principal’s interests. So, what is a health agent? And what are the duties of a health agent? The following will discuss health agents by analyzing the evolution of the role of GPs in NHS reform.
Since the establishment of the NHS in 1948, GPs have played the role of health gatekeepers providing treatment and referral services to patients.10 It is much easier for patients to access treatment from GPs than from other doctors such as specialists in NHS, which means that GP services are much more accessible than others.11 As the first point of contact with medical services, they are entrusted by patients with the legal framework to make medical decisions such as treatment and referrals. But recently, the role of the GPs as health gatekeeper has been questioned. Some believe that GPs can lose the best time to save lives and increase the cost of treatment by delaying diagnosis; that the GP system can exacerbate inequalities in the distribution of health resources, etc.12,13 An increasing number of people are deliberately avoiding GP services at the point of the first visit, choosing to access health services through other ways such as Accident and Emergency (A&E) departments, Minor injuries and Walk in Centers, NHS 111 and palliative care teams, etc.14 Has the role of the GPs as health gatekeeper really been diminished? There have even been calls to rethink the role of gatekeepers in primary care.12,15 Obviously, this is not the case. After 75 years of evolution, GPs have transformed from health gatekeepers to health agents. Current dissatisfaction with the work of GPs stems from the perception that they are health gatekeepers rather than the health agents. The role of the health agent has been neglected in the NHS. Following the path of reform in the NHS, it is possible to find out how the role of GPs has changed.
The Responsibilities of GPs are Expanding from Providing Diseases Treatment to Integrating Treatment, Prevention and Health Promotion
The struggle between humans and diseases is a gradual history, which is continuously progressing step by step with the advancement of science under the impetus of people’s health needs. From GPs splitting off from the ancient community of apothecaries in the mid-17th century in response to a sudden outbreak of infectious disease in London, to the recognition of GPs as legal practitioners under the Medical Act 1858 (S.I. 1858 c.90),16 to the National Health Service Act (S.I. 1946 c.81)17 set out the system of first visit by GPs and hierarchical medical system as the basic framework for the operation of the NHS in 1946, the historical origins of the GP can be seen in the fact that it emerged as a solution to the problem of seeking medical care for ordinary patients. From fighting infectious diseases with a legal capacity to being the main provider of primary care, the role of the GPs has not been static for the past two hundred years. It has changed in response to the needs of the public, society and the times, especially from the 1970s onwards.
The National Health Service Act 1946 divided the provision of healthcare services. Public health services such as immunization, home nursing and home midwifery services are provided by local authorities. On the other hand, general medical, dental service, ophthalmic and pharmacy services, which are directly related to the treatment of patients, are provided by executive committees and local representative committees responsible for GP consultations. Therefore, when the NHS was first established, GPs were limited to being entrusted by patients to provide treatment and referral services. As gatekeepers to the NHS, GPs exercised medical decision-making powers on behalf of patients and played the role of medical decision-making agents. As a public information leaflet about the NHS from 1948 states
You and everyone in your family will be entitled to all usual advice and treatment from a family doctor.…Your doctor will give you a prescription for any medicines and drugs you need.…
Benefiting from the post-war economic recovery, there had been few reforms that occurred in the first 20 years of the NHS. In the 1970s, the economic downturn caused by the oil crisis hindered the development of the NHS. To solve the problems faced by the NHS, the NHS first ushered in a restructuring of the organization in 1974. The reform addresses the fragmentation of the health care process between hospital services, primary care, community care, and public health services that have existed through organizational restructuring since the establishment of the NHS in 1948.18 The organizational restructuring strategy transferred the responsibility of providing facilities for the prevention of illness has originally undertaken by the local health authorities to the Secretary of State and it is stipulated that the Secretary of State can arrangement the vaccination or immunization of persons against disease by the general practitioner (S.I. 1973 c.32).19
The 1974 National Health Service Law (General Medical and Pharmaceutical Services) Regulations (S.I. 1974/160)20 included maternity medical services that were originally in charge of regional health authority into the scope of services provided by GPs. The Family Practitioner Committee is required to publish the list on those doctors who have undertaken to provide either general medical services including maternity medical services or general medical services limited to maternity medical services. In 1975, in England and Wales, GPs who provided contraceptive services to women were able to receive a certain number of subsidies from the government (S.I. 1975/719).21 Later, GPs have gone on to provide other services including the child health surveillance, the minor surgery and the health management (S.I. 1989/1897).22 By the end of the 1980s, the categories of medical and health services mentioned above had become like the current statutory duties of the GPs and were included as part of the GPs' essential services, alongside the original basic duties (Table 1).
 |
Table 1 History of Changes in GPs’ Statutory Duties |
When society enters the 21st century, the advancement of the aging population structure, obvious changes in the spectrum of human diseases, and the continuous application of new diagnosis and treatment technologies have changed people’s understanding of disease treatment and health.23 Chronic, non-communicable diseases have replaced infectious diseases as the main killers of human health.24 Health is not just the absence of disease. It is also about moving from symptomatic treatment to early detection and prevention of disease. The 2023/24 NHS Standard Contract in England,25 in addition to providing basic general outpatient treatment and referrals, the services provided by GPs already cover public health such as health education, health screening, family planning services, child health care, chronic disease management, pregnancy care and immunization, etc. At this time, the duties of GPs were very different from those required by the NHS Act 1948 to provide treatment and referral services only. With the addition of public health service duties such as health screening, health education, immunization, and family planning, their job was not only to provide medical decision-making services to patients, but also to promote health knowledge among registered residents, advocate healthy lifestyles, physical monitoring, and other primary prevention of diseases, as well as to monitor epidemics and prevent their occurrence. It should be noted that the enrichment of statutory duties has helped GPs to gradually move from health gatekeepers to health agents. Therefore, in terms of the changes in the content of GP services, we can easily distinguish the difference between a gatekeeper and a health agent: the former provides medical services to patients, while the latter provides medical and health services to all registered residents.
Internal Market Reforms - Motivation for GPs to Become Health Agents
Reform of the NHS internal market began in the late 1980s, following the recommendations of the Conservative government’s “Services for Patients” report, which removed the government from the burden of overwhelming health care and separated the providers from the purchasers of health care services. While the main aim of this reform was to improve the efficiency of increasingly criticized hospital services by introducing competition, the reform was a double-edged sword that also changed the way GPs worked and the role they performed in the health care service.26–28
Towards a Health Agent Motivation for the First Time
Before the implementation of the internal market reforms, the basic structure of the NHS was relatively simple, with GPs seeing patients and managing their conditions, and referring those who needed further treatment to hospitals or senior doctors for treatment. Patients were in the hands of GPs and senior medical resources were in the hands of hospitals, and as separate sectors of the healthcare chain, they worked closely together to keep the NHS running.29 In this relationship, the two show only a direct working relationship, without any financial conflict of interest. The income of the GPs as independent self-employed professionals was determined by the number of patients served and the additional services they could provide and was paid by the government. Although in the 1960s and 1970s government funding for GPs began to cover the costs of building repairs (S.I. 1966 c.8),30 support staff,31 etc. the funding was only used for GP consultations and not for referrals. Prior to the 1990s, the lack of financial incentives for GPs meant that GPs, who acted as gatekeepers responsible for primary care decision-making, had no motivation to proactively seek further referrals for their patients to specialist medical services. When healthcare resources were limited and the demand for referrals increased, waiting times for referrals became increasingly long. For example, waiting times for elective orthopaedic surgery range from 18 months to three years.32 Over time, how to improve efficiency has become an urgent issue for the NHS to address.
In 1990, the Conservative Party government opened the prelude to the NHS “internal market” reform. The core content of the reform is to separate the buyers and providers of medical and health service and introduce competition into medical and health services. After the reform, the general practitioner is no longer only a provider of primary medical services. His role has undergone some subtle changes, and the key to this change is the emergence of service contracts. Due to the separation of buyers and providers of medical and health services, there are mainly two types of contractual relationships in the NHS.33,34 The first is the primary healthcare contract. Some general practitioner groups or GPs can apply to become General Practitioners Fundholders (GPs Fund holders) and apply for independent budget support for the services they can provide.26 Local medical administrations can sign service contracts with GPs fund holders on behalf of nationals to purchase general practitioner services in the form of fund allocation (S.I. 1990 c.19).35 This kind of contract not only continues the “capitation” remuneration but also stipulates the types of services that should be provided. The other type of contract is a medical purchase contract between the general practitioner and the hospital.36 The general practitioner accepts the government’s entrustment to purchase medical services from the hospital on behalf of the patient.37 The referral process is based on the principle of “money goes with the patient”, realizing the transfer of medical expenses. This kind of contract is controlled by the payment system of “total budget control”, which has a positive effect on GPs who become GPs fund holders. They can proactively provide and purchase high-quality and low-cost medical services for patients, and put the money saved as a result into the improvement of primary care service.
In this kind of contract-centric medical system, for the first time, GPs have been promoted to the role of agent. The general practitioner is not only the executor (for the first type of contract) and client (for the second type of contract) of the contract but also the health agent representing the interests of patients. If the previous diagnosis and treatment work of GPs mostly relied on the professional experience of GPs and the stable working relationship of consultants, then the current service motivation has more consideration as an agent. In order to get more money saved, they have competed for service contracts with an “economic man” mindset, to proactively provide patients with the better services. However, the reform of the Conservative Party is not thorough. This GPs fund holder system is not mandatory. GPs can participate in it according to their wishes. As there is no budgetary support or incentives to encourage non-participating GPs to join the group, they lack the economic incentive to become agents. Therefore, some people believe that this GPs fund holder system will cause inequality among GPs, divide the two levels of primary care, and affect the general practitioner system.38,39
Towards a Health Agent Motivation for the Second Time
The Primary Care Trusts (PCTs) established by the Labor Party government in 1999 replaced GPs fund holders as purchasers of medical services. It abolished the GPs fund holder system, changed the contract provision system of general practitioner’s medical and health services to direct supply, and purchased services from hospitals with the support of GPs.40–42 Although the Labor Government’s PCTs plan abolished competition for contracts for GPs, a broader competition plan was released in 2004 - Opening up GPs registrations. From the beginning of the establishment of the NHS to 2004, the area of residence was the main reference factor for people to choose GPs for registration. That is, residents living in area A can choose GPs registered in area A to register. In addition, for a long period of time, there is a clear limit on the number of people served by each general practitioner. For example, in the 1972 law, it was stipulated that each independent general practitioner can serve no more than 3500 registered people. Each partner general practitioner can serve no more than 4500 registered persons. If he employs assistants, no more than 2000 persons can be added for each additional assistant (S.I.1972/1602).43 Although this kind of legal setting stipulates that people can choose GPs voluntarily and can also change GPs according to the change of residence, because of the service ceiling, especially in densely populated areas, it is virtually impossible for people to want to freely choose GPs who serve themselves. Until 2004, the PCTs contract provided to GPs abolished the clause restricting the number of registrations of GPs, and the saturation of the number was no longer a reason for GPs to reject applicants for registration and decide whether to close and open patient registration requires PCTs approval (S.I.2004/291).44 Such a policy arrangement means that the initiative to select GPs is given to residents, and an internal competition among GPs is formed in a certain area. Since the payment per capita is still implemented, those GPs who have more registrations will have higher incomes. It is therefore necessary to improve their services to win more registrations proactively. In addition, the related institutional arrangements occurred in the early 21st century. Since January 2006, GPs have been required to provide their patients with a list of 4-5 candidate hospitals, including an independent institution, when providing referrals.45 The introduction of this policy has added another consideration factor to patients - who provides a better referral service - when choosing GPs, and for GPs, there is an additional element of competition.
In 2012, the Cameron coalition government initiated what is known as the most thorough reform since the establishment of the NHS. The coalition government replaced the PCTs with the Clinical Commissioning Groups (CCGs) and required all GPs to become members of the CCGs (S.I. 2012/2996).46 CCGs provides two types of contracts that is one is to provide GPs with a contract to purchase primary medical and health services, and the other is to purchase referral medical services from a hospital.47 In other words, the reform policy adopted by the coalition government combines the advantages of the Conservative Party government’s GPs participating in medical service procurement and the Labor Party government’s strengthening internal competition in medical and health services. Although the NHS is more in favor of collaboration following the replacement of CCGs by Integrated Care Systems (ICSs) in 2022, the choice is still in the hands of residents, so collaboration is built on competition. Currently, GPs already have play two roles, one is to provide patients with primary medical services and become the gatekeepers; and the other is, in a competitive environment, they have become agents who proactively provide high-quality and low-cost health care services to registered residents.
From GPs fund holders to PCT, to CCG, and then to ICSs, although the name of purchasing medical and health services on behalf of the government in various government periods in the UK is not the same, the direction of providing “internal marketization” medical reform with competition as the core has not changed. The right of patients to vote with their feet for their GP's services dictates that competition exists. It is precisely the competition that makes the group of GPs take the initiative to assume the role of health agent. Obviously, gatekeepers and health agents are easily differentiated by the motivation for providing services, the former passively provide medical services when patients seek help, while the latter proactively provide medical and health services to registered residents (Table 2).
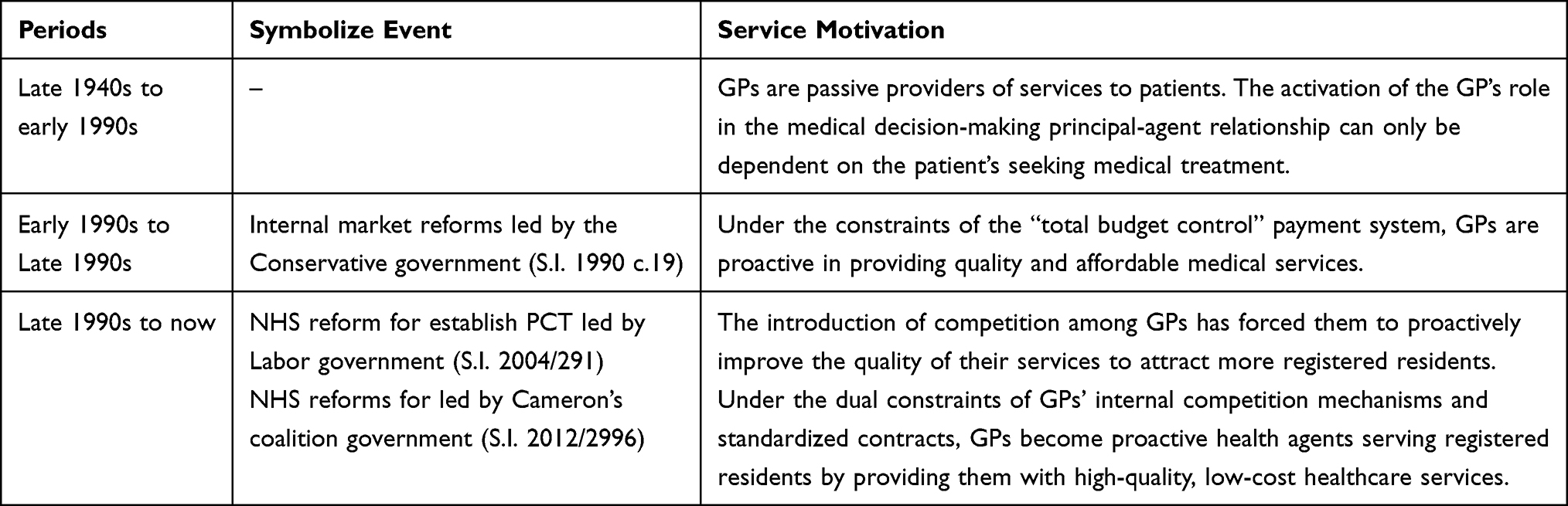 |
Table 2 History of Changes in the Motivation to Serve in GP |
Definition of the Health Agent Role of the GP
In contrast to the gatekeeper who provide medical decision-making with a single duty, the GP, as a health agent, usually has several typical characteristics (Table 3).
 |
Table 3 The Difference Between a Health Gatekeepers and a Health Agent |
Firstly, the services provided are more abundant. The GP’s service already covers both clinical and public health services. According to the latest general medical services contract25 provided by the NHS in England, in addition to providing basic general outpatient treatment and referrals, the services provided by GPs already cover health education, health screening, family planning services, child health care, outpatient surgery, chronic disease management, pregnancy care and immunization, etc.
Secondly, to serve a wider range of clients. The diversity of services provided by GPs dictates that they serve a wider range of clients. With the addition of public health responsibilities such as immunization and health education, it means that GPs no longer serve only patients, but also provide services to the residents, who are both the patient and the healthy.
Thirdly, service delivery is more proactive. With competition, GPs have to be more proactive in providing optimal care to registered residents in order to compete for more enrollments, and thus earn a stable and higher income.
Based on the above characteristics, the health agent role of the GP can be defined in this way: entrusted by the individual and the state, in addition to providing disease treatment and referral services to patients, the GP also takes the initiative to provide health-related public health services, such as disease prevention, health education, health management and health monitoring services etc., to healthy registered residents.
Conditions for GPs to Become Health Agents
In the process of reforming the UK healthcare system, GPs have completed the transformation from health gatekeepers to health agents by continuing to enrich their statutory duties, because GPs’ work is highly recognized by UK society. Since the launch of the British Social Attitudes Survey in 1983, public support for a nationalized health system in the UK has been over 90%.48 In 2017, The Commonwealth Found assessed the healthcare systems of 11 high-income countries, including the UK, the US, and Germany, across 72 indicators in five main areas: access, accessibility, the efficiency of management, equity and output of healthcare services, and the results showed that the UK’s NHS ranked first in terms of overall performance and its healthcare system best-reflected equity.49 Such high levels of satisfaction are the result of the full trust that British society has in the NHS and GPs. In terms of the structure of trust, this trust can be described in terms of both interpersonal trust and institutional trust.
Interpersonal Trust: Have the Mass Base
The mass base of GPs stems from the historical roots of their group. GPs come from the group of surgeons-pharmacists, and the emergence of this group has greatly solved the problem of general public visits. It can be said that GPs serve the general public mainly. Before the 20th century, there was a clear hierarchical order for British health care practitioners.50 Physicians are the first rank in this order, they are gentlemen in the medical profession, with a high social reputation; they have the right to prescribe, brain rather than manually treat patients; this group has a small number of practitioners, according to the relevant literature, the total number of physicians in the 16th century is 31, the end of the 17th century about 80 people, the total number of 19th century did not exceed 100 people, so the scarcity of such practitioners determines their main service to the nobles and the rich. Surgeons in the second grade, mainly responsible for dealing with trauma, do not have the right to prescribe the medicine, they use a manual operation to relieve the patient’s pain.50 At the bottom of this order is the pharmacist community. The group has a large number of practitioners, mostly from the civilian class. Because medicines can only be configured according to prescriptions issued by physicians, these people are like physician assistants and cannot participate in medical activities independently. This gold tower-shaped hierarchical order made the distribution of medical resources in early Britain extremely uneven, with only a few nobles and the rich having access to medical services, while the medical needs of the majority, especially the civilian population, could not be met. Under the internal causes of the absolute shortage of physicians and the imbalance in the distribution of medical resources, coupled with the outbreak of infectious diseases in London in the mid-17th century, the hierarchical order of health care providers, which had existed for hundreds of years, had been broken. The bottom group of pharmacists had become the main force in the fight against the epidemic, gradually moving away from physicians and carrying out independent medical activities to take on the responsibility of protecting the health of the general public. The civilian-born group of pharmacists not only self-administered and drug-using but also focused on developing clinical manual skills, creating a whole new group of medical practitioners in British society - GPs (surgeons-pharmacists). Their presence solves the problem of access to medical services for the general public. It should be noted that GPs, who came from and served the civilians, have the broadest and strongest mass base in the UK. This is precisely the reason why, in the subsequent reforms, GPs were selected by the government to perform additional duties, such as providing public health services, and the population accepted that these services would be provided by GPs.
Institutional Trust: Have Stable Legal Support
Stable legal support is reflected in the legal professional qualifications and statutory duties of GP. The first is that GPs have a legal professional qualification. Section 52 of the Medical Act 1858, which explicitly does not allow restrictions on the practice of doctors in a clinical drug or surgical practice, eradicates the order of medical practitioners and legally recognizes the practice status of GPs. In 1911, David Lloyd George, then chancellor of the exchequer, built on the German social security system to promote the creation of the National Insurance Act 1911, which for the first time legally recognized the form of contracted medical services for Medicare insured persons, laying the foundation for the subsequent establishment of a primary health care system dominated by GPs services. Until 1946, under the influence of the Beveridge Report, the NHS Act identified the core elements of the NHS, namely that citizens over the age of 16 can choose a doctor to serve themselves, using a wide range of taxes as a source of expenditure at no cost. At this point, GPs have a full professional qualification as the main provider of primary care in the NHS.
The second is that the duties of a general practitioner are defined by the law. As the law that defined the legal status of GPs, the National Health Service Act 1946, distinguishes the boundaries between the practice of general practice and the public health sector. Public health services were provided by local authorities, while clinical treatment service, which were directly related to patients, were provided by GPs (S.I. 1946 c.81).17 As can be seen from the previous analysis of the expanded role of the general practitioner, the expansion of the scope of the GP’s duties has been supplemented by a process of legal amendments, such as the provision of immunization services in 1973, obstetric care in 1974, family planning services for women in 1975, and the addition of childcare services, medical consultation services and clinical minor surgery in 1989. The significance of recognizing the professional legitimacy of GPs and changing their duties through a uniform legislative amendment process is that it ensures stability, consistency and fairness in the provision of services by GPs.
Discussion: The Lessons of GPs’ Transition from Health Gatekeepers to Health Agents
Now, after sorting out the transition from health gatekeeper to health agent in the UK, it is easy to distinguish between the concepts of health gatekeeper in primary care and health agent in primary health care. The scope of responsibility of the health agent is more encompassing than that of the health gatekeeper, just as the concept of primary health care is broader than that of primary care. According to the Alma Ata Declaration of 1978 by the WHO, primary health care is a strategy for the whole community to pursue health, including providing promotive, preventive, curative and rehabilitative services accordingly etc., that aims at ensuring the highest possible level of health and well-being. Primary care is only one component of primary health care. In the role of health gatekeeper, the GPs connect the primary care service with the senior medical service (both hospital and specialist doctors) and their main task is to provide an initial consultation to patients and to make referrals depending on the diagnosis. In the role of health agent, the GPs have a much larger scope of services and clients than the health gatekeeper, responding to the requirements of primary health care as advocated in the Declaration of Alma-Ata. Firstly, GPs serve a wide range of registered residents. Secondly, in addition to providing first counseling services, GPs offer residents a multitude of options for health services related to disease prevention, health screening and health promotion etc. If previously, as health gatekeepers, GPs provided disease treatment and referral services to patients, and now, as health agents, they provide health management services to residents.
Based on the above analysis of the process of transition from health gatekeeper to health agent in general practice, there are three important lessons were captured. The first lesson is that the transition of the GP role to health agent needs to be sustained by trust. GPs were born out of deep interpersonal trust and have thrived on a rigorous institutional trust. In the struggle against infectious diseases, the work of GPs has gradually become recognized and trusted by the public. It is on this trust-based choice that GPs have gradually become independent providers of health care. Institutional trust in GPs that consists of two elements: the statutory duties of GPs and the procedural legality. The significance of the statutory duty is that it ensures that GPs provide an equitable, stable and consistent service to registered residents. Procedural legality means that all adjustments concerning general practice are accomplished through the legislative amendment process. Given the rules inherent in the UK legislative amendment process, only what is accepted by most of the population can successfully become a legal provision. This illustrates that institutional trust in GPs is based on interpersonal trust. Therefore, it is possible to conclude that the transition of the role of the GPs relies on the interaction of interpersonal and institutional trust, without either of which the GPs cannot be health agents or even good health gatekeepers.
The second lesson is the competetion is both a label for health agents and a driver for the role transition of GPs. In the process of transitioning the role of the GPs, if the expansion of duties was forced on GPs by law, for GPs the result of the internal market reforms is that they have proactively chosen to become health agents. The internal market reform, while giving patients and registered residents the right to choose, has created competition for GPs. To attract more residents to register, the starting point of GPs’ work has shifted from just seeing patients to proactively providing quality and affordable health care services to registered residents.
The third lesson is the use of medical contracts to bind GPs to their services. In the NHS, GPs are funded through a contract with the NHS for their services. The main difference between this type of medical contract and a normal commercial contract is that although the contract is made between the NHS and the GPs, the contract connects the three parties - the GPs, the residents, and the NHS. The NHS purchases the service from the GPs and the GPs provides the service to the residents, so the GPs are agents of the state and the residents respectively. The contract covers several aspects of services such as the population served, the service contents, the hours of service, the way the service is provided, complaints about the service, and dispute resolution. The existence of the contract not only binds the GPs to the service but also binds competition it ensures that every registrant has access to consistent and high-quality services in primary health care. As a legally protected service contract, the contract has many positive aspects. On the one hand, it imposes statutory requirements on the performance of GPs’ duties and responsibilities by standardizing the content of the services. On the other hand, the disclosure of the terms makes the content of the service transparent between the NHS, the residents, and the GPs, which consolidates trust in the GPs. Obviously, the contract has made competition more transparent by delineating the content of services. As competition is bound by the contract, not only is there greater clarity about the services enjoyed by registered residents, but GPs are also encouraged to proactively improve their services rather than focusing on profitability.
Conclusion
By analyzing the role transition process of GPs, this article answers the current doubts about the GPs as health gatekeepers. That the health agent is an iteration of the gatekeepers. The expansion of GPs responsibilities has provided residents with a wealth of accessible healthcare services, and the introduction of competition led to GPs proactively providing quality and affordable services to the residents. The transition of the GPs to health agents is a historical trend, is the choice of society and the people, which is in line with the evolution of medicine and a positive view of health. As health agents, the GPs combine public health services with clinical services. The advantages of this are that, on the one hand, since the service is provided proactively, the decentralization of public health services to the GPs improves the accessibility of public health services to the residents, thus increasing the utilization of public health services; on the other hand, the overall health of society is improved when disease treatment service provided by health gatekeepers is gradually replaced by health management by health agents.
Data Sharing Statement
Data for this study is available from the corresponding author upon reasonable request.
Ethics Statement
The studies titled “GPs in UK: From Health Gatekeepers in Primary Care to Health Agents in Primary Health Care” was a qualitative study using a documentary analysis method and did not involve an ethical statement.
Funding
The study was funded by an important project “Research on the Transition of Western European Social Democratic Party and New Changes in Social Democracy (grant number: 17JJD710004)” of Ministry of Education of China.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Janssen M, Fluit CRMG, Sagasser MH, Kusters LHJ, Scherpbier-de Haan ND, de Graaf J. Competencies for collaboration between general practitioners and medical specialists: a qualitative study of the patient perspective. BMJ Open. 2020;10(7):e037043. doi:10.1136/bmjopen-2020-037043
2. Grosios K, Gahan PB, Burbidge J. Overview of Healthcare in the UK. EPMA J. 2010;1(4):529–534. doi:10.1007/s13167-010-0050-1
3. Peckham S, Hann A, Kendall S, Gillam S. Health promotion and disease prevention in general practice and primary care: a scoping study. Prim Health Care Res Dev. 2017;18(6):529–540. doi:10.1017/S1463423617000494
4. Blakeman T, Macdonald W, Bower P, Gately C, Chew-Graham C. A qualitative study of GPs’ attitudes to self-management of chronic disease. Br J Gen Pract. 2006;56(527):407–414.
5. Peckham S, Hann A, Boyce T. Health promotion and ill-health prevention: the role of general practice. Qual Prim Care. 2011;19(5):317–23.
6. McCartney M. Prostate cancer screening: what work should GPs stop doing so they can do this work instead? BMJ. 2023;380:284. doi:10.1136/bmj.p284
7. Shi L. The impact of primary care: a focused review. Scientifica (Cairo). 2012;2012:432892. doi:10.6064/2012/432892
8. Waterman RW, Meier KJ. Principal-agent models: an expansion? J Public Admin Res Theory. 1998;8(2):173–202. doi:10.1093/oxfordjournals.jpart.a024377
9. Arrow KJ. Uncertainty and the welfare economics of medical care. In: Uncertainty in Economics. Elsevier; 1978:345–347.
10. Loudon I. The principle of referral: the gatekeeping role of the GP. Br J General Pract. 2008;58(547):128–130. doi:10.3399/bjgp08X277113
11. Goddard M, Smith P. Equity of access to health care services: theory and evidence from the UK. Soc Sci Med. 2001;53(9):1149–1162. doi:10.1016/S0277-9536(00)00415-9
12. Greenfield G, Foley K, Majeed A. Rethinking primary care’s gatekeeper role. BMJ. 2016;354:i4803. doi:10.1136/bmj.i4803
13. Mahase E. GPs are being blamed for government failures in primary care, say doctors. BMJ. 2021;374:n2234. doi:10.1136/bmj.n2234
14. Pope C, McKenna G, Turnbull J, Prichard J, Rogers A. Navigating and making sense of urgent and emergency care processes and provision. Health Expect. 2019;22(3):435–443. doi:10.1111/hex.12866
15. Cox J. GPs can no longer claim to Be the ‘gatekeepers’ of the NHS. Br J General Pract. 2006;56(523):83–84.
16. The National Archives: Medical Act 1858 CHAPTER 90 (S.I. 1858 c.90); 2023. Available from https://www.legislation.gov.uk/ukpga/Vict/21-22/90/enacted
17. The National Archives: National Health Service Act 1946 CHAPTER 81(S.I. 1946 c.81); 2023. Available from https://www.legislation.gov.uk/ukpga/Geo6/9-10/81/contents/enacted.
18. Gorsky M. The British National Health Service 1948–2008: a review of the historiography. Soc Hist Med. 2008;21(3):437–460. doi:10.1093/shm/hkn064
19. The National Archives: National Health Service Reorganization Act 1973 CHAPTER 32 (S.I. 1973 c.32); 2023. Available from https://www.legislation.gov.uk/ukpga/1973/32/contents.
20. The National Archives: The National Health Service (General Medical and Pharmaceutical Services) Regulations 1974 No.160(S.I. 1974/160); 2023. Available from https://www.legislation.gov.uk/uksi/1974/160/contents/made.
21. The National Archives: The National Health Service (General Medical and Pharmaceutical Services) Amendment Regulations 1975 No.719(S.I.1975/719); 2023. Available from https://www.legislation.gov.uk/uksi/1975/719/contents/made.
22. The National Archives: The National Health Service (General Medical and Pharmaceutical Services) Amendment (No. 2) Regulations 1989 No.1897(S.I.1989/1897); 2023. Available from https://www.legislation.gov.uk/uksi/1989/1897/contents/made.
23. Franceschi C, Garagnani P, Morsiani C, et al. The continuum of aging and age-related diseases: common mechanisms but different rates. Front Med (Lausanne). 2018;5: 61 . doi:10.3389/fmed.2018.00061
24. Budreviciute A, Damiati S, Sabir DK, et al. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front Public Health. 2020;8:574111. doi:10.3389/fpubh.2020.574111
25. NHS England: Standard general medical services contract 2023/24; 2023. Available from https://www.england.nhs.uk/publication/standard-general-medical-services-contract-23-24/.
26. Enthoven AC. Internal market reform of the British National Health Service. Health Aff (Millwood). 1991;10(3):60–70. doi:10.1377/hlthaff.10.3.60
27. Propper C. Agency and incentives in the NHS internal market. Soc Sci Med. 1995;40(12):1683–1690. doi:10.1016/0277-9536(94)00285-2
28. Bramwell D, Checkland K, Shields J, Allen P. 1990s: The introduction of the internal market. In: Community Nursing Services in England: An Historical Policy Analysis. Cham: Springer International Publishing; 2023 doi:10.1007/978-3-031-17084-3:43–59.
29. Piterman L, Koritsas S. Part I. General practitioner–specialist relationship. Internal Medicine Journal. 2005; 35: 430–434. doi: 10.1111/j.1445-5994.2005.00855.x
30. The National Archives: National health service act 1966 CHAPTER 8 (S.I. 1966 c.8); 2023. Available from https://www.legislation.gov.uk/ukpga/1966/8/contents/enacted.
31. Greengross P, Grant K, Collini E. The history and development of the UK National Health Service 1948-1999. Department for International Development Health Systems Resource Centre. 1999.
32. Hart JT. Political Economy of Health Care: A Clinical Perspective. Bristol: Policy Press. 2006:22.
33. Propper C, Wilson D, Söderlund N. The effects of regulation and competition in the NHS internal market: the case of general practice fundholder prices. J Health Econ. 1998;17(6):645–673. doi:10.1016/S0167-6296(98)00029-0
34. Peckham S. The new general practice contract and reform of primary care in the United Kingdom. Healthc Policy. 2007;2(4):34–48.
35. The National Archives: National Health Service and Community Care Act 1990 CHAPTER 19 (S.I. 1990 c.19); 2023. Available from https://www.legislation.gov.uk/ukpga/1990/19/contents.
36. Bennett C, Ferlie E. Contracting in theory and in practice: some evidence from the NHS. Public Adm. 1996;74(1):49–66. doi:10.1111/j.1467-9299.1996.tb00857.x
37. Smith PC, Stepan A, Valdmanis V, Verheyen P. Principal-agent problems in health care systems: an international perspective. Health Policy. 1997;41(1):37–60. doi:10.1016/S0168-8510(97)00012-2
38. Lunt N, Atkin K, Hirst M. Staying single in the 1990s: single-handed practitioners in the new National Health Service. Soc Sci Med. 1997;45(3):341–349. doi:10.1016/S0277-9536(96)00349-8
39. Ali AM. The personalisation of the British National Health Service: empowering patients or exacerbating inequality?. Int J Clin Pract. 2009;63(10):1416–1418. doi:10.1111/j.1742-1241.2009.02152.x
40. Sussex J. Controlling NHS Expenditure: The Impact of Labour’s NHS White Papers. London: Office of Health Economics; 1998.
41. Kay A. The abolition of the GP fundholding scheme: a lesson in evidence-based policy making. Br J General Pract. 2002;52(475):141–144.
42. Bloor K, Maynard A. Reforming the English NHS: a continuing journey. Appl Health Econ Health Policy. 2010;8(6):373–375. doi:10.2165/11586180-000000000-00000
43. The National Archives: The National Health Service (General Medical and Pharmaceutical Services) Regulations 1972 No. 1602(S.I.1972/1602); 2023. Available from https://www.legislation.gov.uk/uksi/1972/1602/contents/made.
44. The National Archives: The National Health Service (General Medical Services Contracts) Regulations 2004 No.291. The National Archives(S.I.2004/291); 2023. Available from: https://www.legislation.gov.uk/uksi/2004/291/contents/made.
45. Kristian Niemietz. Internal Markets, Management by Targets, and Quasi-Markets: An Analysis of Health Care Reforms in the English NHS. Economic Affairs. 2015; 35(1):93–108. doi: 10.1111/ecaf.12115
46. The National Archives: The National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) Regulations 2012 No. 2996(S.I. 2012/2996); 2023. Available from: https://www.legislation.gov.uk/uksi/2012/2996/contents.
47. Reynolds L, Gerada C, McKee M. Ditching the single-payer system in the national health service: how the English Department of Health is learning the wrong lessons from the United States. Int J Health Serv. 2012;42(3):539–547. doi:10.2190/HS.42.3.i
48. Burki T. From health service to national identity: the NHS at 70. Lancet. 2018;392(10141):15–17. doi:10.1016/S0140-6736(18)31513-7
49. Schneider EC, Sarnak DO, Squires D, Shah A, Doty MM. Mirror mirror 2017: international comparison reflects flaws and opportunities for better US health care, the Commonwealth Fund; 2023. Available from: https://www.commonwealthfund.org/publications/fund-reports/2017/jul/mirror-mirror-2017-international-comparison-reflects-flaws-and.
50. Hamilton B. The medical professions in the eighteenth century. Econ Hist Rev. 1951;4(2):141–169. doi:10.2307/2599120
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.