Back to Journals » International Journal of Women's Health » Volume 18
Global Disability and Economic Burden Caused by Rheumatoid Arthritis, Osteoarthritis, Neck Pain, and Low Back Pain in Women of Childbearing Age from 1990 to 2021
Authors Yao Y, Yuan D, Li Y, Wang Y
Received 20 January 2026
Accepted for publication 12 March 2026
Published 25 March 2026 Volume 2026:18 597468
DOI https://doi.org/10.2147/IJWH.S597468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Yuming Yao,1,* Dongliang Yuan,1,* Yusheng Li,1,2 Yaping Wang2,3
1Department of Orthopedics, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 3Teaching and Research Section of Clinical Nursing, Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yaping Wang, Email [email protected]
Background: This study utilized data from the Global Burden of Disease (GBD) to systematically analyze the years lived with disability (YLDs) and direct economic costs attributable to rheumatoid arthritis (RA), osteoarthritis (OA), neck pain (NP), and low back pain (LBP) among women aged 15– 49 between 1990 and 2021, aiming to inform public health intervention strategies.
Methods: Using GBD 2021 data, we reported the YLDs and age-standardized rates (ASYR) for four major musculoskeletal diseases (MSD) in women of childbearing age (WCA) from 1990 to 2021. The temporal trends in disease burden were assessed by estimated annual percentage change (EAPC), and a non-linear frontier model was used to examine the association between the sociodemographic index (SDI) and disease burden. Additionally, the direct economic burden imposed by the four diseases in WCA was estimated.
Results: In 2021, the YLDs among WCA worldwide due to RA, OA, NP, and LBP were 610,000, 1.61 million, 6.35 million, and 19.51 million, respectively, reflecting increases of 86.8%, 111%, 58%, and 40% compared to 1990. The ASYR for RA and OA increased by 13.6% and 11.2%, respectively, while the ASYR for NP and LBP slightly decreased. High SDI regions bear the heaviest burden, but regions with low-middle SDI show a faster growth rate. The global economic burden of these four diseases totaled $43.66 billion, with LBP accounting for the largest portion ($16.7 billion), and about 80% of the expenditure concentrated in high-SDI and high-middle SDI countries.
Conclusion: MSD pose a persistent and growing health and economic challenge for WCA, with RA and OA showing a clear trend toward younger age groups. Although the ASYR for LBP has decreased, its absolute disability burden has still increased due to population growth. High-income countries bear the majority of the economic cost, reflecting the unequal distribution of global health resources.
Keywords: global burden of disease, women of childbearing age, musculoskeletal diseases, years lived with disability, economic burden
Introduction
Musculoskeletal disorders represent a leading cause of global disability, affecting over 1.63 billion individuals. Among these, neck pain (NP), low back pain (LBP), osteoarthritis (OA), and rheumatoid arthritis (RA) are particularly prevalent.1,2 These conditions not only compromise patients’ quality of life and work productivity but also impose a substantial burden on healthcare systems globally, ranking as primary contributors to disability-adjusted life years (DALYs).3 Recent studies indicate a continuous rise in both the incidence and disability burden associated with these disorders.4–7 Notably, women of childbearing age (WCA) exhibit unique epidemiological characteristics and health outcomes, rendering this demographic a critical focus of global health research.8
NP and LBP are characterized by an early onset, profoundly impacting patients’ functional capacity and well-being. Their etiology is closely associated with lifestyle factors, such as prolonged sitting and poor posture, as well as psychological determinants, including stress and chronic pain mechanisms.9,10 The prevalence of NP and LBP is significantly higher in women than in men,6,7 particularly during reproductive years and post-menopause. This disparity is likely attributable to fluctuations in the female physiological cycle and heightened pain sensitivity.11 Regarding OA, a degenerative condition, its burden is exacerbated by population aging and rising obesity rates.12 Conversely, RA, a chronic autoimmune disorder involving systemic inflammation and multi-joint damage, severely diminishes quality of life and escalates healthcare costs.13 The elevated incidence and disability burden of these conditions among women are driven by gender-specific disparities, primarily stemming from hormonal fluctuations (eg, variations in estrogen and progesterone), differences in immune function, and societal role expectations.11,14,15 Furthermore, the post-menopausal decline in estrogen levels further aggravates the risk and severity of these diseases.16–18
Beyond their profound impact on individual health, musculoskeletal disorders impose significant economic strains on healthcare systems, a burden that is particularly acute among WCA. Direct medical costs—encompassing diagnosis, treatment, and rehabilitation—substantially escalate financial pressures on individuals, families, and society at large. Consequently, a comprehensive understanding of the global burden and economic implications of musculoskeletal disorders within this demographic is imperative for effective healthcare resource allocation and evidence-based policy formulation across diverse regions.
The Global Burden of Disease (GBD) study offers vital data for assessing disability burdens across diverse populations by systematically estimating the incidence of diseases, injuries, and risk factors, stratified by age, sex, region, and Socio-demographic Index (SDI). However, to date, there remains a paucity of focused research regarding the global burden, temporal trends, and economic costs of common musculoskeletal disorders, specifically RA, OA, NP, and LBP. To address this gap, the present study leverages the GBD 2021 database to analyze the burden of these four conditions among women aged 15–49 years globally. Specifically, we aim to: (1) investigate the global epidemiological characteristics and analyze long-term trends and variations across multiple levels (global, regional, national, and by SDI); and (2) integrate supplementary databases to evaluate the direct economic costs associated with musculoskeletal disorders in WCA. These findings will provide a robust scientific basis for formulating precise public health policies at global, regional, and national levels to mitigate the burden of musculoskeletal diseases in this vulnerable population.
Methods
Data Sources and Definitions
GBD data are collected through systematic assessments of various surveys, censuses, civil registrations, population monitoring, and other health-related data sources. After data collection, DisMod-MR 2.1 (a Bayesian meta-regression tool) is used to assess and adjust for bias risks in each data source using standardized statistical methods. Detailed methods regarding data collection, processing, and generation are extensively described in the GBD 2021 study,19 with related publicly available estimated figures accessible at http://ghdx.healthdata.org/gbd-results-tool. The disability and prevalence data used in this study are from the GBD 2021 dataset, which covers global disease burden data for 204 countries and territories from 1990 to 2021, involving 811 locations, 371 diseases and injuries, and 88 risk factors.19,20 The GBD study divides 204 countries and territories into 21 regions, further categorized into 7 super-regions. This study extracts years lived with disability (YLDs) and prevalence data for women aged 15–49 in RA, OA, NP, and LBP, categorized by age groups (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49 years), with specific data download details in Supplementary Method 1. Moreover, healthcare expenditure data for four common musculoskeletal diseases among WCA are available at https://vizhub.healthdata.org/dex/, with ICD codes and case definitions provided in Supplementary Methods 2–3.
Statistical Analysis
To adjust for age structure differences among populations, we calculated the age-standardized YLD rate (ASYR) using the direct standardization method based on the global standard population defined in the GBD 2021 study. This method assumes that YLDs are the weighted sum of independent Poisson random variables.21,22 All rates are calculated per 100,000 population, with the 95% uncertainty interval (UI) computed for each variable to reflect the uncertainty of the estimates. Furthermore, to assess the temporal trends in disability burden among WCA, we calculated the estimated annual percentage change (EAPC) and its 95% confidence interval (CI). When both the EAPC and its 95% CI are greater than zero, it indicates an increasing trend in disease burden; when both are less than zero, it indicates a decreasing trend; if the 95% CI of the EAPC includes zero, it suggests that the disability burden remained stable during the period.23,24 The specific calculation method for the EAPC is described in Supplementary Method 4.
To assess the relationship between sociodemographic development levels and the burden of four musculoskeletal diseases among WCA, we utilized frontier analysis to construct a nonlinear frontier model, which describes the optimal YLD burden achievable by a country or region at a certain development level. We define “effective difference” as the absolute gap between the ASYR caused by RA, OA, NP, and LBP in WCA and the frontier model, thereby revealing the potential for health improvements not yet achieved by specific countries or regions at their current development levels (see Supplementary Method 5). Additionally, we investigated the correlation between SDI and ASYR across 21 regions through Spearman correlation analysis.25
We used extrapolation to estimate the economic costs of four common musculoskeletal diseases among WCA in various countries for 2021, a method widely applied in previous economic analyses.26–29 Initially, we calculated the direct medical expenditures for each disease case in seven age groups in the United States for 2021 (ages 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, and 45–49 years). Subsequently, by comparing the total medical expenditures of each country with those of the United States, we estimated a correction factor.30 Lastly, we multiplied the number of women with musculoskeletal diseases in each age group in various countries by the cost of medical expenditures per case in the United States, then multiplied by the correction factor, to estimate the economic burden of these four common diseases in each country. Detailed analytical methods are described in Supplementary Method 6. Data analysis and visualization were performed using R statistical software (version 4.4.0). The R packages utilized in the analysis included “dplyr”, “tidyverse”, “data.table”, “ggplot2”, and “maps”. Statistical significance was set at a P-value of less than 0.05.
Results
Global Burden and Temporal Trends
In 2021, the global YLDs for WCA caused by RA reached 606,536 (95% UI 397,295–893,380), an increase of 86.8% since 1990, with an estimated annual growth rate of 2.15% (95% CI 2.05–2.25). The YLDs associated with OA were 1.61 million (0.75–3.24), growing 1.11 times since 1990, with an EAPC of 2.67% (2.48–2.86). The YLDs associated with NP and LBP were 6.35 million and 19.51 million respectively in 2021, with estimated annual growth rates of 1.47% and 1.18%. Regarding age-standardized rates, the 2021 ASYRs for RA and OA were 30.22 and 77.86 per 100,000 respectively, increasing by 13.6% and 11.2% since 1990. In contrast, the YLDs caused by NP and LBP showed a declining trend from 1990 to 2021, with their EAPCs being −0.05% (−0.13 to 0.04) and −0.28% (−0.34 to −0.22) respectively (Tables 1–2 and Tables S1-S2).
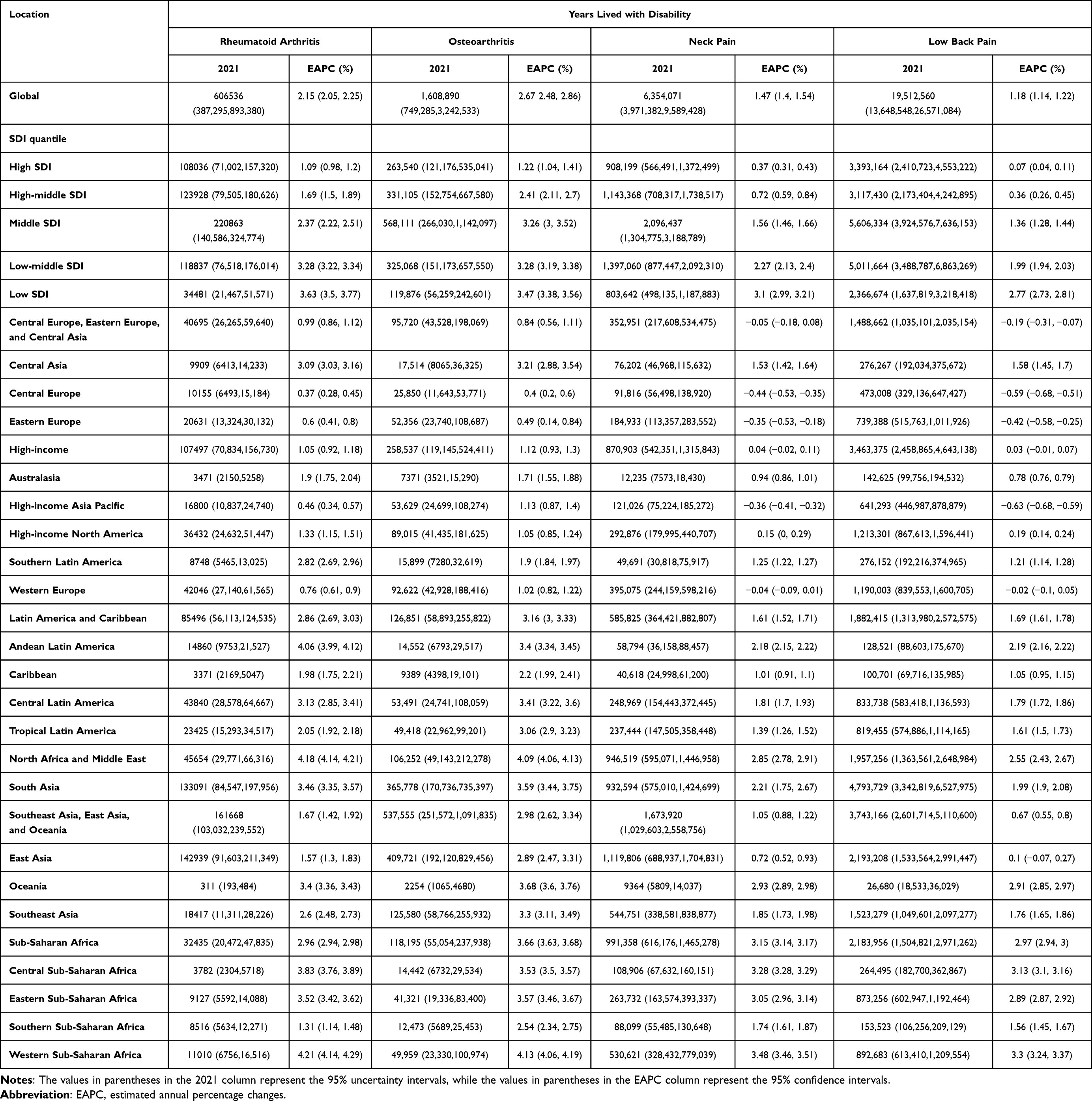 |
Table 1 In 2021, years Lived with Disability for Women of Reproductive Age Globally, Caused by Rheumatoid Arthritis, Osteoarthritis, Neck Pain, and Low Back Pain, Categorized by SDI and Region, Along with Estimated Annual Percentage Changes from 1990 to 2021 |
 |
Table 2 In 2021, Age-Standardized Years Lived with Disability Rate for Women of Reproductive Age Globally, Caused by Rheumatoid Arthritis, Osteoarthritis, Neck Pain, and Low Back Pain, Categorized by SDI and Region, Along with Estimated Annual Percentage Changes from 1990 to 2021 |
Regional Burden and Temporal Trends
The four musculoskeletal disorders exhibited the highest burden of YLD in middle SDI quantiles. Apart from NP, the ASYR of the other three musculoskeletal diseases increased with rising SDI. In 2021, the heaviest ASYR burden among WCA caused by RA was in the high SDI quantiles (39.52 per 100,000), followed by the high-middle SDI quantiles (35.05 per 100,000). However, from 1990 to 2021, the fastest average annual growth rate was in the low-middle SDI quantiles (EAPC = 0.96%), while the growth rate was the slowest in the middle SDI quantiles (EAPC = 0.60%). Similar to RA, OA posed the greatest burden on WCA in the high SDI quantiles (85.79 per 100,000), with a slower growth rate (EAPC = 0.49%). Regarding the burden of NP in WCA, except for a 0.08% annual decline in the high-middle SDI quantiles over the past 32 years, the other SDI quantiles remained stable or showed slight increases. From 1990 to 2021, the burden of LBP on WCA showed a declining trend across all five SDI quantiles, with the fastest decline in the high-middle SDI quantiles (EAPC = −0.31%) (Tables 1–2 and Figure S1).
In 2021, the regions with the lowest YLDs from four types of musculoskeletal disorders in WCA were in Oceania, while the highest burdens were observed in East Asia, South Asia, and North Africa and Middle East. In terms of ASYR, RA, OA, NP, and LBP caused the greatest disability burden respectively in Andean Latin America (85.01 per 100,000), High-income Asia Pacific (91.61 per 100,000), North Africa and Middle East (588.7 per 100,000), and Australasia (1892.02 per 100,000). Between 1990 and 2021, the High-income Asia Pacific, Central Europe, and Eastern Europe experienced the quickest increase in YLDs from musculoskeletal diseases among WCA, with sub-Saharan Africa exhibiting a slower average annual growth rate (Tables 1–2).
National Burden and Temporal Trends
In 2021, the highest YLDs caused by musculoskeletal disorders among WCA were recorded in China, India, and the United States. However, significant geographical differences exist in the ASYR. The highest ASYR for RA, OA, NP, and LBP were observed in Peru (111.54 per 100,000), Taiwan (a province of China) (108.76 per 100,000), Iran (659.53 per 100,000), and New Zealand (2004.9 per 100,000), respectively. From 1990 to 2021, the fastest increase in YLDs due to musculoskeletal disorders among WCA in the Middle East was observed, particularly in Qatar, the United Arab Emirates, and Kuwait. In Equatorial Guinea, WCA show the greatest annual increase in ASYR due to RA and OA, while the highest annual increases in ASYR for NP and LBP are found in Finland and Sweden, respectively (Table S3-S4 and Figures 1–2).
 |
Figure 1 Age-standardized YLD rates among women of childbearing age caused by rheumatoid arthritis (A), osteoarthritis (B), neck pain (C), and low back pain (D) in 2021. Abbreviation: YLD, years lived with disability. |
 |
Figure 2 Estimated annual percentage change in age-standardized YLD rates among women of childbearing age caused by rheumatoid arthritis (A), osteoarthritis (B), neck pain (C), and low back pain (D) from 1990 to 2021. Abbreviation: YLD, years lived with disability. |
Analysis by Time, Age, and Region
The crude YLD rate for RA in women aged 30–34 showed the most significant increase, rising from 25.95 per 100,000 in 1990 to 30.46 in 2021, an increase of 17.36%. In women under 30, OA did not contribute to the YLD burden; however, in women aged 30–49, the YLDs caused by OA remained stable, at about 10%. The YLD burden caused by NP decreased in women aged 20–39, while it increased by 3.1% in women aged 45–49 over these 32 years. Moreover, all childbearing age groups saw a significant reduction in the YLD burden from LBP, particularly in the 30–34 age group, where the reduction was most pronounced (−13.57%) (Figure 3).
 |
Figure 3 Crude YLD rates among women of childbearing age by age group caused by rheumatoid arthritis (A), osteoarthritis (B), neck pain (C), and low back pain (D) in 1990 and 2021. Abbreviation: YLD, years lived with disability. |
The study results indicate that there are significant age-related differences in the disability burden caused by various types of musculoskeletal disorders among WCA. Among WCA in each age group, the highest proportion of YLDs is caused by LBP, followed by NP, OA, and RA. It is important to note that OA typically does not occur in individuals under 30 years old, hence the proportion of YLDs due to OA is zero in the 15–29 age group. Additionally, as age increases, the proportion of YLDs caused by RA and OA gradually rises, whereas in 2021, YLDs related to NP peaked in the 30–34 age group, and those caused by LBP progressively decreased with age. Compared to 1990, in 2021, the proportion of disability burden caused by RA, OA, and NP among WCA in all age groups has increased (Figures 4–5 and Table S5).
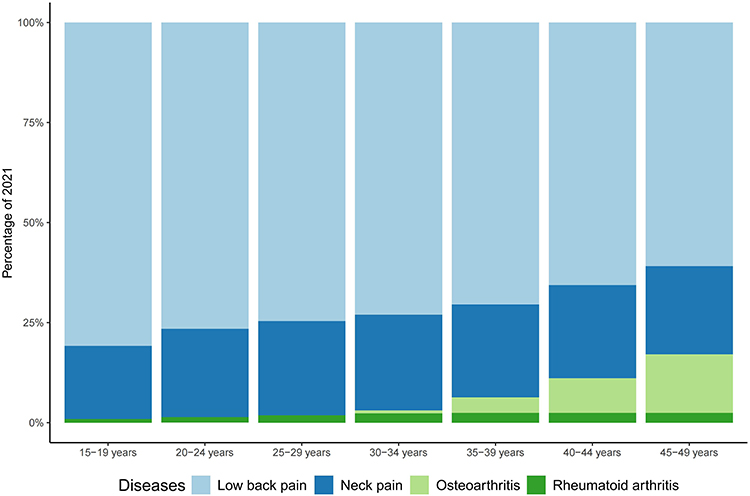 |
Figure 4 Stacked bar chart of disability burden caused by four common musculoskeletal disorders among women of childbearing age globally in 2021. |
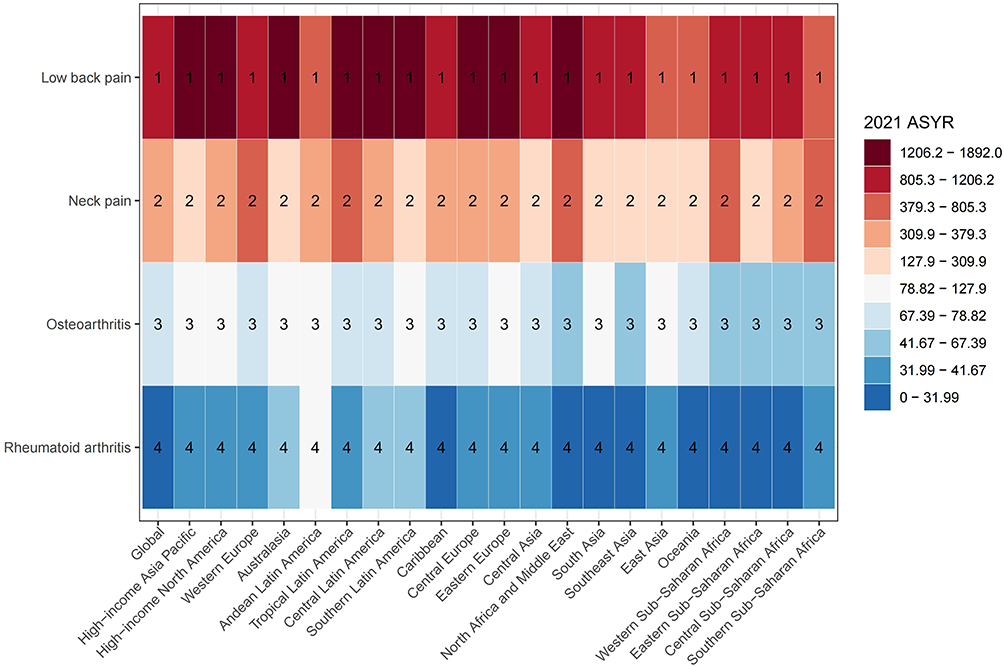 |
Figure 5 Heatmap of disability burden caused by four common musculoskeletal disorders among women of childbearing age across global and 21 regions in 2021. |
Frontier Analysis
Between 1990 and 2021, except for NP, the ASYR of other musculoskeletal disorders in WCA were positively correlated with SDI (Figure 6). Frontier analysis across 204 countries and territories indicated that ASYR associated with RA and OA in WCA increase with rising SDI, while YLDs related to NP tend to decrease as SDI increases (Figure S2). Regarding the YLD burden caused by RA, in 2021, WCA in low SDI countries such as Somalia, Niger, Chad, Papua New Guinea, and Timor-Leste showed the smallest effective difference from the frontier; while the largest gaps were seen in countries like Peru, Kuwait, and Mexico. In terms of YLD burden caused by OA in WCA, African countries with low SDI such as Somalia, Niger, and Burundi are closest to the frontier, while high SDI Asian countries or territories like Taiwan (a province of China), South Korea, and Singapore exhibit larger effective differences. The YLD burden associated with NP and LBP follows a similar trend, where the burden related to NP among WCA in Iran is furthest from the frontier, while New Zealand shows the largest effective difference in LBP-related disability burden among such women (Figure 7 and Table S6).
 |
Figure 6 Relationship between age-standardized YLDs rates and socio-demographic index (SDI) for rheumatoid arthritis (A), osteoarthritis (B), neck pain (C), and low back pain (D) among women of childbearing age across 21 regions from 1990 to 2021. Each point represents the observed ASYR value for a specific region in a given year, while the solid line indicates the expected value calculated based on SDI and disease rate models for all regions. Points above the solid line indicate regions with disease burdens higher than expected, whereas points below the line indicate lower-than-expected burdens. Abbreviation: YLD, years lived with disability. |
 |
Figure 7 Frontier analysis of age-standardized YLD rate caused by rheumatoid arthritis (A), osteoarthritis (B), neck pain (C), and low back pain (D) among women of childbearing age across 204 countries or territories from 1990 to 2021. Each point represents a specific country or territory in 2021, with the top 15 countries showing the largest deviations from the frontier marked in black. Countries with low SDI (≤0.455) and minimal deviation from the frontier are shown in blue, while those with high SDI (≥0.805) but significant deviations relative to their development level are highlighted in red. Point colors also reflect trends in ASYR changes (decline or increase) from 1990 to 2021. Abbreviation: SDI, socio-demographic index. |
Economic Burden
In 2021, the direct economic burden attributed to RA, OA, NP, and LBP among WCA worldwide was respectively $8.25 billion (95% UI: 6.42–10.31 billion), $5.07 billion (4.21–6.02 billion), $13.64 billion (7.94–22.00 billion), and $16.7 billion (12.71–21.46 billion). There is significant inequality in the geographic and socioeconomic distribution of the economic burden caused by these four diseases: WCA in high and high-middle SDI regions bear over 80% of the direct global economic burden, while those in low SDI regions account for less than 1% (see Table 3). LBP causes the highest direct costs among WCA in high SDI quintiles, amounting to $8.39 billion, which represents 50% of the global burden. The other three musculoskeletal disorders mainly impose a substantial economic strain on WCA in high-middle SDI quintiles. Geographically, aside from OA, which imposes the highest economic burden on women in High-income regions (50.78%), the remaining three conditions predominantly affect women in Southeast Asia, East Asia, and Oceania. Specifically, the direct economic burdens of RA, OA, and NP are most significant in East Asia, High-income North America, South Asia, and Western Europe; whereas the economic impact of LBP is primarily concentrated in High-income North America ($7.21 billion), East Asia ($4.9 billion), South Asia ($2.1 billion), and Western Europe ($0.6 billion). In comparison, the direct economic burdens caused by WCA in Oceania, Sub-Saharan Africa, and the Caribbean are relatively smaller. At the national level, the countries with the greatest economic burden on WCA due to RA, OA, and NP are China, the United States, India, Japan, Brazil, and Germany; for LBP, the United States faces the highest economic costs ($7.16 billion), followed by China, India, Japan, Brazil, and Germany (Table S7-S14).
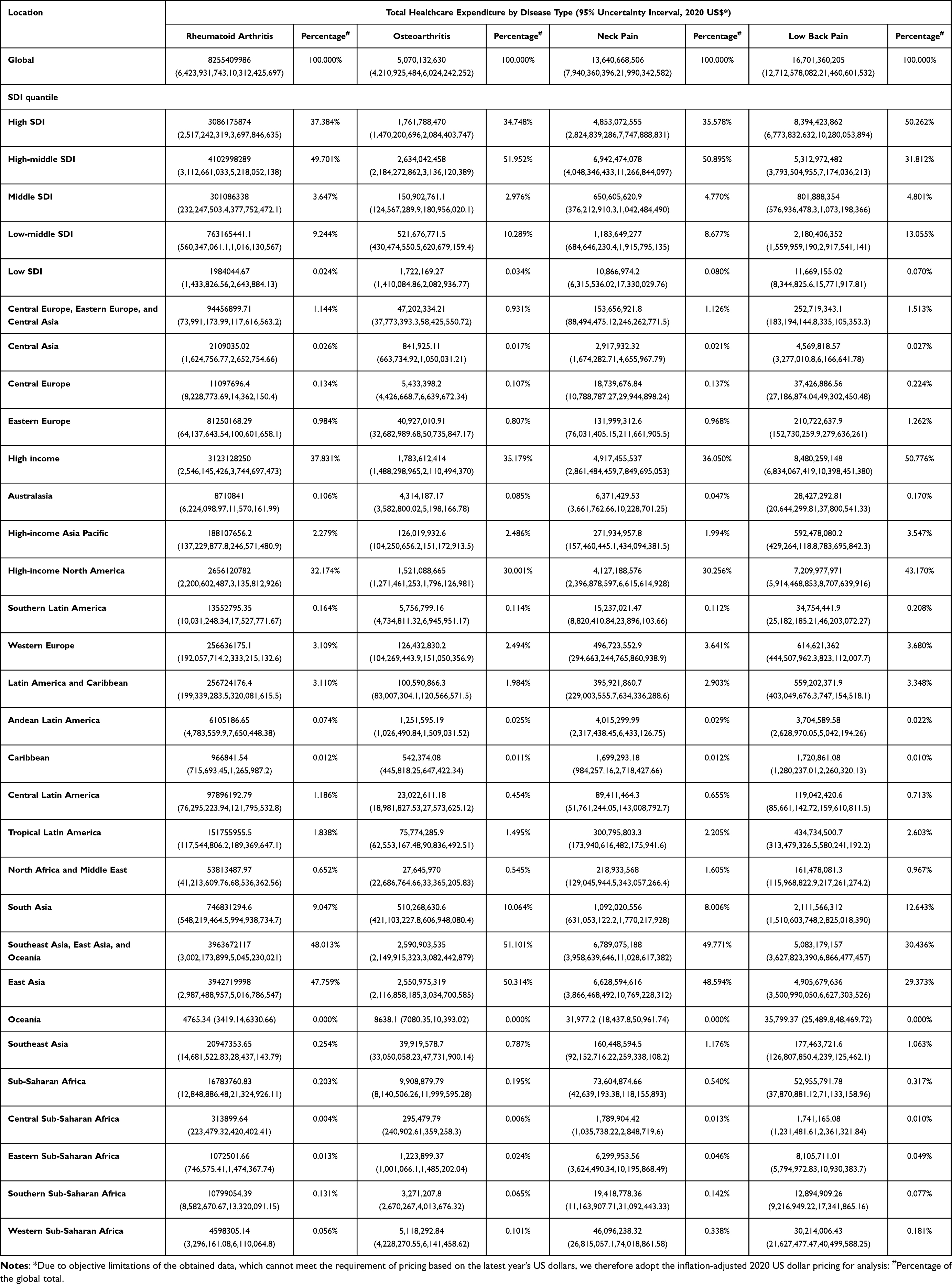 |
Table 3 Total Healthcare Expenditure for Women of Reproductive Age (15–49 Years) Due to Rheumatoid Arthritis, Osteoarthritis, Neck Pain, and Low Back Pain Globally and Across Regions in 2021 |
Discussion
Our analysis reveals that over the past 32 years, the global ASYR due to RA and OA among WCA has exhibited an upward trend. In contrast, the ASYR for NP has remained stable, while that for LBP has demonstrated a declining trajectory. Notably, despite the stability in NP rates and the decrease in LBP rates, the absolute global YLDs attributable to NP and LBP among WCA in 2021 were 1.58 and 1.4 times higher, respectively, than in 1990, reflecting the impact of population growth and aging. Collectively, these four musculoskeletal disorders incurred a global direct expenditure of $43.66 billion, with LBP imposing the most substantial economic burden ($16.7 billion). Furthermore, a pronounced disparity exists in the economic burden across nations with varying levels of socio-economic development; countries with high and high-middle SDI scores accounted for over 80% of the global direct economic burden. Distinct from prior research, this study represents the inaugural systematic exploration of the YLD burden of RA, OA, NP, and LBP among WCA utilizing the latest GBD 2021 data.8 Crucially, it provides the first comprehensive assessment of both YLD and economic burdens associated with these conditions at global, regional, and national levels.
Among the five musculoskeletal disorders cataloged in GBD 2021, the YLD burden for RA, OA, NP, and LBP is consistently higher in females than in males, with gout being the notable exception.31 This gender disparity likely stems from a complex interplay of multifactorial determinants. Biologically, female sex hormones play a pivotal role in the pathogenesis and pathophysiology of various musculoskeletal degenerative conditions. Particularly in women of reproductive age, hormonal fluctuations can exacerbate the disability burden by modulating inflammatory responses and compromising bone health.32,33 Additionally, inherent anatomical differences in females, such as variations in cervical vertebral dimensions and curvature, may predispose them to the onset and progression of these disorders.34
Beyond biology, sociocultural and psychological factors exert a profound influence on women’s health outcomes.35 Gender inequality often creates barriers to healthcare access in specific cultural contexts. For instance, societal restrictions on female physical activity may deter help-seeking behaviors, while male dominance in controlling economic resources frequently places women at a disadvantage in healthcare decision-making. Furthermore, entrenched societal role expectations often compel women to prioritize familial and communal needs over their own well-being, leading to delayed diagnosis or neglected treatment. Psychologically, social pressures may encourage the endurance of chronic pain, or fear of stigma may discourage treatment-seeking, thereby aggravating the overall disease burden.36,37 In summary, the elevated YLD burden of musculoskeletal diseases among women is driven by the synergistic interaction of biological, social, and psychological factors, which collectively amplify health disparities between sexes.
Although the YLD burden attributable to these four musculoskeletal disorders among WCA generally escalates with advancing age, the trajectory of change across specific age cohorts has varied significantly over the past 32 years. Regarding RA, the 30–34 age group exhibited the most rapid surge in crude YLD rates, whereas the burden of OA increased most markedly among women aged 45–49. For NP, crude YLD rates declined among women aged 20–39, contrasting with an upward trend observed in the 15–19 and 40–49 age groups. By 2021, crude YLD rates for LBP had decreased across all age groups compared to 1990 levels, with the most substantial reduction noted in the 30–34 cohort. These divergent trends likely stem from a complex interplay of biological determinants, lifestyle modifications, advancements in healthcare, and shifting socioeconomic conditions. Specifically, the rising RA burden in younger WCA may be driven by hormone-mediated fluctuations associated with childbirth and heightened inflammatory responses. Conversely, the sharp increase in OA among middle-aged women likely reflects the waning of joint protective mechanisms during the perimenopausal transition, coupled with cartilage degeneration and the cumulative effects of long-term mechanical stress.38 Regarding NP, the decline in the 20–39 age group may be attributed to the widespread implementation of targeted health interventions and elevated health literacy within this demographic. In contrast, the increased burden among adolescents (15–19 years) could be linked to academic stress and prolonged screen time, while for women aged 40–49, occupational demands and sedentary behaviors appear to be the primary contributors.
The YLD burden of RA, OA, NP, and LBP among WCA also exhibits significant heterogeneity across SDI regions. While ASYR for RA, OA, and NP remain highest in high-SDI regions, their growth rates have accelerated notably in low-middle and low-SDI regions over the past three decades. In high-SDI settings, the persistent high burden is largely attributable to population aging, enhanced diagnostic capabilities, and lifestyle-related risk factors. Conversely, the steeper ascent in ASYR observed in low- and low-middle-SDI regions suggests a convergence driven by rapid urbanization, epidemiological transitions, and improving—yet still insufficient—healthcare access and diagnostic capacity. This trend underscores critical gaps in disease prevention and management infrastructure within these developing regions. Globally, although LBP remains the fourth leading cause of YLDs for WCA, its ASYR has demonstrated a general decline across all SDI quintiles. This favorable trend likely reflects heightened awareness of LBP and the widespread adoption of preventive measures facilitated by economic development.39 Notably, the extensive utilization of ergonomic tools, alongside efforts to reduce monotonous labor and correct poor postural habits, has played a pivotal role in mitigating the incidence of LBP.40,41
Notably, certain African nations, such as Somalia and Niger, have demonstrated significant improvements in YLD burdens associated with these four musculoskeletal disorders among WCA. This progress may be attributed to a “catch-up” effect from initially low baseline rates, expanded coverage of basic healthcare services, and sustained international aid. Nevertheless, profound regional disparities persist. For example, in the Andean region of Latin America (eg, Peru), the gap between observed and expected YLD burden (frontier) for RA is the widest, likely reflecting inequitable healthcare resource distribution and inadequate chronic disease management. Similarly, while high-income Asia-Pacific regions (eg, Taiwan, South Korea, Singapore) report substantially higher OA burdens, these estimates should be interpreted with caution; they may partly reflect data availability bias, as the underlying models rely heavily on sparse input data predominantly sourced from high-income settings.4 In Iran, the YLD burden for NP deviates most significantly from the theoretical frontier, a phenomenon potentially driven by the high prevalence of comorbid mental health disorders, such as depression and anxiety. Indeed, existing literature corroborates a strong association between psychological distress and the incidence of neck pain.42,43 Finally, in Oceania (eg, Australia and New Zealand), the LBP burden stands furthest from the frontier, likely exacerbated by the region’s advanced aging population, high obesity prevalence, and sedentary lifestyles.44–46
Several limitations warrant consideration in interpreting our findings. First, while the GBD methodology utilizing the DisMod-MR 2.1 model is recognized for its robustness, the accuracy of its estimates remains contingent upon the quality and availability of source data. Consequently, results at the national or sub-national level should be interpreted with caution, particularly in regions with sparse data. Second, although this study provides a comprehensive macro-level analysis of YLD burdens, it could not account for heterogeneity in clinical treatment protocols and health management systems across countries. This limitation precludes a detailed assessment of variations in resource allocation and rehabilitation accessibility, potentially affecting the external validity of our conclusions regarding specific healthcare interventions. Third, our analytical framework did not incorporate certain contextual determinants, such as sociocultural backgrounds, educational attainment, and specific environmental exposures, which are known to influence disease burden and may limit the comprehensiveness of our etiological interpretations. Finally, our economic analysis was restricted to direct medical costs. Due to data constraints, indirect costs associated with productivity losses and informal care were not included, likely leading to an underestimation of the total socioeconomic impact of these musculoskeletal disorders on WCA.
Conclusion
Musculoskeletal disorders pose a significant health threat to WCA globally, with both disability burden and economic costs continuing to rise. The ASYR for RA and OA has increased significantly among young women, and OA is no longer confined to the elderly population, with the disease burden particularly pronounced among WCA in high-income areas. Although the ASYR for LBP has decreased, the absolute number of YLDs continues to climb with population growth. In 2021, the direct economic costs reached $43.7 billion, with 80% borne by high-middle and high SDI countries, highlighting the global disparity in health resource allocation. There is an urgent need to implement early prevention measures for the youth (such as weight management and occupational protection), optimize the allocation of medical resources, and integrate interventions for mental health and social support. Future efforts should further assess the indirect economic burdens and the drivers of regional disparities to build a more equitable disease prevention and control system.
Abbreviation
ASYR, age-standardized YLDs rate; CI, confidence interval; EAPC, estimated annual percentage change; GBD, global burden of disease; LBP, low back pain; NP, neck pain; OA, osteoarthritis; RA, rheumatoid arthritis; SDI, socio-demographic index; UI, uncertainty interval; WCA, women of childbearing age; YLDs, years lived with disability.
Data Sharing Statement
All data generated or analysed during this study are included in this published article and its supplementary information files.
Ethics Declarations
This research utilized publicly accessible, anonymized, and aggregated data extracted from the GBD 2021 database, with no involvement of identifiable individual-level information. In accordance with the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects of the People’s Republic of China, studies of this nature are exempt from ethical review requirements. The Ethics Committee of Xiangya Hospital, Central South University has verified that neither ethical approval nor informed consent was necessary for this study.
Acknowledgments
This work was supported in part by the High Performance Computing Center of Central South University. We express our sincere gratitude to the Global Burden of Disease research team for providing the data that made this study possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Research on the Integration Innovation and Quality Improvement Pathways of Elderly Care Service Models in the Aging Period (13300-159990011).
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–19.
2. GBDOMD C. Global, regional, and national burden of other musculoskeletal disorders, 1990-2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(11):e670–e82. doi:10.1016/S2665-9913(23)00232-1
3. Kocarnik JM, Compton K, Dean FE, et al. Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: a systematic analysis for the global burden of disease study 2019. JAMA Oncol. 2022;8(3):420–444. doi:10.1001/jamaoncol.2021.6987
4. Collaborators GBDO. Global, regional, and national burden of osteoarthritis, 1990-2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–e22.
5. GBDRA C. Global, regional, and national burden of rheumatoid arthritis, 1990-20 20, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(10):e594–e610.
6. GBDLBP C. Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(6):e316–e29.
7. Collaborators GBDNP. Global, regional, and national burden of neck pain, 1990-2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2024;6(3):e142–e55. doi:10.1016/S2665-9913(23)00321-1
8. Cao F, Li D-P, Wu G-C, et al. Global, regional and national temporal trends in prevalence for musculoskeletal disorders in women of childbearing age, 1990-2019: an age-period-cohort analysis based on the Global Burden of Disease Study 2019. Ann Rheum Dis. 2024;83(1):121–132. doi:10.1136/ard-2023-224530
9. Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. Low back pain. Lancet. 2021;398(10294):78–92. doi:10.1016/S0140-6736(21)00733-9
10. Kazeminasab S, Nejadghaderi SA, Amiri P, et al. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord. 2022;23(1):26. doi:10.1186/s12891-021-04957-4
11. Gulati M, Dursun E, Vincent K, watt FE. The influence of sex hormones on musculoskeletal pain and osteoarthrit is. Lancet Rheumatol. 2023;5(4):e225–e38. doi:10.1016/S2665-9913(23)00060-7
12. Glyn-Jones S, Palmer AJR, Agricola R, et al. Osteoarthritis. Lancet. 2015;386(9991):376–387. doi:10.1016/S0140-6736(14)60802-3
13. Di Matteo A, Bathon JM, Emery P. Rheumatoid arthritis. Lancet. 2023;402(10416):2019–2033. doi:10.1016/S0140-6736(23)01525-8
14. Alpizar-Rodriguez D, Finckh A. Environmental factors and hormones in the development of rheumatoid arthritis. Semin Immunopathol. 2017;39(4):461–468. doi:10.1007/s00281-017-0624-2
15. Pang H, Chen S, Klyne DM, et al. Low back pain and osteoarthritis pain: a perspective of estrogen. Bone Res. 2023;11(1):42. doi:10.1038/s41413-023-00280-x
16. Parazzini F, Progretto menopausa italia Study G. Menopausal status, hormone replacement therapy use and risk of self-re ported physician-diagnosed osteoarthritis in women attending menopause clinics in Italy. Maturitas. 2003;46(3):207–212. doi:10.1016/S0378-5122(03)00193-2
17. Wang YXJ. Menopause as a potential cause for higher prevalence of low back pain in women than in age-matched men. J Orthop Translat. 2016;8:1–4. doi:10.1016/j.jot.2016.05.012
18. Bengtsson C, Malspeis S, Sparks JA, Costenbader KH, Karlson EW. Post-Menopausal Factors and the Risk of Seropositive and Seronegative Rheumatoid Arthritis Phenotypes: results from the Nurses’ Health Study. Paper presented at: Arthritis & Rheumatology, 2014.
19. Diseases GBD, Injuries C. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Glob al Burden of Disease Study 2021. Lancet. 2024;403(10440):2133–2161.
20. GBDRF C. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2162–2203.
21. Fay MP, Feuer EJ. Confidence intervals for directly standardized rates: a method based o n the gamma distribution. Stat Med. 1997;16(7):791–801.
22. Selvin S. Statistical Analysis of Epidemiologic Data. Vol. 35.
23. Yang X, Chen H, Zhang T, et al. Global, regional, and national burden of blindness and vision loss due to common eye diseases along with its attributable risk factors from 1990 to 2019: a systematic analysis from the global burden of disease study 2019. Aging. 2021;13(15):19614–19642. doi:10.18632/aging.203374
24. Zhai Z, Ruan J, Zheng Y, et al. Assessment of global trends in the diagnosis of mesothelioma from 1990 to 2017. JAMA Network Open. 2021;4(8):e2120360. doi:10.1001/jamanetworkopen.2021.20360
25. Song J, Pan T, Xu Z, et al. A systematic analysis of chronic kidney disease burden attributable to lead exposure based on the global burden of disease study 2019. Sci Total Environ. 2024;908:168189. doi:10.1016/j.scitotenv.2023.168189
26. Chen N, Fong DYT, Wong JYH. Health and economic outcomes associated with musculoskeletal disorders attributable to high body mass index in 192 countries and territories in 2019. JAMA Network Open. 2023;6(1):e2250674. doi:10.1001/jamanetworkopen.2022.50674
27. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease fo r 204 countries and territories in 2020-50: a health-augmented macroec onomic modelling study. Lancet Glob Health. 2023;11(8):e1183–e93. doi:10.1016/S2214-109X(23)00217-6
28. Ding D, Lawson KD, Kolbe-Alexander TL, et al. The economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet. 2016;388(10051):1311–1324. doi:10.1016/S0140-6736(16)30383-X
29. Weng Q, Chen Q, Jiang T, et al. Global burden of early-onset osteoarthritis, 1990-2019: results from the Global Burden of Disease Study 2019. Ann Rheum Dis. 2024;83(7):915–925. doi:10.1136/ard-2023-225324
30. Global Burden of Disease Health Financing Collaborator N. Tracking development assistance for health and for COVID-19: a review of development assistance, government, out-of-pocket, and other private spending on health for 204 countries and territories. Lancet. 1990-2050;398(10308):1317–1343.
31. Jin Z, Wang D, Zhang H, et al. Incidence trend of five common musculoskeletal disorders from 1990 to 2017 at the global, regional and national level: results from the glob al burden of disease study 2017. Ann Rheum Dis. 2020;79(8):1014–1022. doi:10.1136/annrheumdis-2020-217050
32. Hurwitz EL, Randhawa K, Yu H, Côté P, Haldeman S. The Global Spine Care Initiative: a summary of the global burden of lo w back and neck pain studies. Eur Spine J. 2018;27(Suppl 6):796–801. doi:10.1007/s00586-017-5432-9
33. Diseases GBD, Injuries C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222.
34. Lim J-K, Wong H-K. Variation of the cervical spinal Torg ratio with gender and ethnicity. Spine J. 2004;4(4):396–401. doi:10.1016/j.spinee.2003.11.011
35. Manchikanti L, Singh V, Datta S, Cohen SP, Hirsch JA; American Society of Interventional Pain P. Comprehensive review of epidemiology, scope, and impact of spinal pain. Pain Physician. 2009;12(4):E35–70. doi:10.36076/ppj.2009/12/E35
36. Zou Y, Yue M, Ye X, et al. Epidemiology of acute hepatitis C and hepatitis C virus-related cirrho sis in reproductive-age women, 1990-2019: an analysis of the Global Burden of Disease study. J Glob Health. 2024;14:04077. doi:10.7189/jogh.14.04077
37. Hartvigsen J, Nielsen J, Kyvik KO, et al. Heritability of spinal pain and consequences of spinal pain: a comprehensive genetic epidemiologic analysis using a population-based sample of 15,328 twins ages 20-71 years. Arthritis Rheum. 2009;61(10):1343–1351. doi:10.1002/art.24607
38. Szoeke CE, Cicuttini FM, Guthrie JR, Dennerstein L. The relationship of reports of aches and joint pains to the menopausal transition: a longitudinal study. Climacteric. 2008;11(1):55–62. doi:10.1080/13697130701746006
39. Collaborators GBDD. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 195 0-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1160–1203.
40. Mikkonen P, Viikari-Juntura E, Remes J, et al. Physical workload and risk of low back pain in adolescence. Occup Environ Med. 2012;69(4):284–290. doi:10.1136/oemed-2011-100200
41. Vuori IM. Dose-response of physical activity and low back pain, osteoarthritis, and osteoporosis. Med Sci Sports Exerc. 2001;33(6 Suppl):S551–86;discussion609–10. doi:10.1097/00005768-200106001-00026
42. Rees CS, Smith AJ, O’Sullivan PB, Kendall GE, Straker LM. Back and neck pain are related to mental health problems in adolescence. BMC Public Health. 2011;11:382. doi:10.1186/1471-2458-11-382
43. Demyttenaere K, Bruffaerts R, Lee S, et al. Mental disorders among persons with chronic back or neck pain: results from the World Mental Health Surveys. Pain. 2007;129(3):332–342. doi:10.1016/j.pain.2007.01.022
44. Leboeuf-Yde C. Body weight and low back pain. A systematic literature review of 56 journal articles reporting on 65 epidemiologic studies. Spine. 2000;25(2):226–237. doi:10.1097/00007632-200001150-00015
45. Matringe CH. Nutrition and eating behaviour in older adulthood. 2007.
46. Annear M. Sedentary behavior and physical inactivity in the Asia-Pacific region: current challenges and emerging concerns. Int J Environ Res Public Health. 2022;19(15):9351. doi:10.3390/ijerph19159351
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.