Back to Journals » Clinical Epidemiology » Volume 13
Global Burden of Ischemic Heart Disease and Attributable Risk Factors, 1990–2017: A Secondary Analysis Based on the Global Burden of Disease Study 2017
Authors Wang F ![]() , Yu Y, Mubarik S
, Yu Y, Mubarik S ![]() , Zhang Y, Liu X
, Zhang Y, Liu X ![]() , Cheng Y
, Cheng Y ![]() , Yu C
, Yu C ![]() , Cao J
, Cao J
Received 28 April 2021
Accepted for publication 4 September 2021
Published 21 September 2021 Volume 2021:13 Pages 859—870
DOI https://doi.org/10.2147/CLEP.S317787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Eyal Cohen
Fang Wang,1,2 Yong Yu,3 Sumaira Mubarik,1 Yu Zhang,4 Xiaoxue Liu,1 Yao Cheng,5 Chuanhua Yu,1,6 Jinhong Cao1
1Department of epidemiology and biostatistics, School of Health Sciences, Wuhan University, Wuhan, Hubei, People’s Republic of China; 2Department of biostatistics, School of Public Health, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 3Computer Teaching and Research Section, School of Public Health, Hubei University of Medicine, Shiyan, Hubei, People’s Republic of China; 4Department of Public Health, Medical College, Hubei Polytechnic University, Huangshi, Hubei, People’s Republic of China; 5Obstetrics Department, Maternal and Child Health Care Hospital of Hubei Province, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 6Global Health Institute, Wuhan University, Wuhan, 430071, People’s Republic of China
Correspondence: Chuanhua Yu; Jinhong Cao
Department of Epidemiology and Biostatistics, School of Health Sciences, Wuhan University, No. 115, Donghu Road, Wuhan, 430071, People’s Republic of China
Tel/Fax +8627-68759299
Email [email protected]; [email protected]
Objective: To estimate the burden of ischemic heart disease (IHD) stratified by gender, age, geographic location, and social-demographic status for 21 regions across the world from 1990 to 2017.
Methods: Using the Global Burden of Disease Study (GBD) Results Tool, we extracted data on the incidence, mortality, disability-adjusted life years (DALYs), and age-standardized rates related to IHD, as IHD burden measures. Trend analyzes were conducted for major regions. Risk factors for DALYs (obtained from the GBD comparative risk assessment framework) were also analyzed.
Results: Globally, 10.6 million (95% uncertainty interval [UI]: 9.6– 11.8) cases of IHD occurred in 2017, with 8.9 million (95%UI:8.8– 9.1) IHD-related deaths. Both the age-standardized incidence rate (ASIR) and death rate (ASDR) declined from 1990 to 2017 (percentage change: 27.4% and 30.0%, respectively), with average annual percent change (AAPC) values of − 1.2% and − 1.3%, respectively. In 2017, the global number of IHD-related DALYs was 170.3 million (95%UI:167.1– 174.0), and the middle socio-demographic index (SDI) quintile contributed the most to these DALYs. In most regions, indicators (incidence, mortality, and DALYs) declined steadily with SDI increased. High systolic blood pressure (SBP) was the most significant contributor to the DALYs in most regions, accounting for 118.18 million DALYs in 2017 globally, followed by high low-density lipoprotein cholesterol and a diet low in nuts and seeds (101.78 and 52.86 million, respectively).
Conclusion: Even though the trend in IHD morbidity and mortality decreased globally, the IHD burden remains high, particularly in regions with lower SDI. It is necessary to learn successful and effective experience in controlling IHD risks and decreasing health disparities to reduce the IHD burden.
Keywords: ischemic heart disease, global burden, risk factors, temporal trends, epidemiology
Introduction
Ischemic heart disease (IHD) is a group of chronic diseases characterized by coronary ischemia of the heart and subsequent myocardial damage. The incidence and mortality rates related-to IHD are falling in most developed and developing countries, but the absolute numbers are still rising,1 and IHD has become a worldwide public health problem.2,3 In Europe, the IHD-related mortality rate has declined overall, especially in the United Kingdom, Netherlands, and Ireland, where the IHD mortality rate has fallen by more than 60%.1 In contrast, epidemiological studies have reported that the prevalent cases and deaths related to IHD increased rapidly in China, the Arab States, India, and Latin America.4–7
Some studies also showed that IHD is a preventable and eradicable disease if the risk factors are effectively controlled.2,4,8 However, the global burden of IHD is increasing rapidly due to the combined effect of social-demographic disadvantage, low health care accessibility, and poor performance of health-care systems.8,9 The IHD incidence and prevalence of IHD differs by age, gender, and region, and specific studies on the IHD burden and risk factors are still lacking globally.2,10,11
It is vital to identify modifiable risk factors in addition to non-modifiable risk factors for IHD for effective health care planning and prevention. The established risk factors for IHD include dietary risks, high blood pressure, high low-density lipoprotein (LDL), and tobacco use, etc.6 Another, the change of risk factors in different regions from 1990 to 2017 were also closely related to social and economic development.12 The primary aim of this study was to describe the influence of age, gender, geographic location, and Socio-demographic Index (SDI) on the global trends in the incidence, mortality, and disability-adjusted life years (DALYs) related to IHD from 1990 to 2017. The secondary aim was to explore IHD DALYs attributable to risk factors, and the relationship between risk exposure and SDI, according to Global Burden of Disease Study (GBD) 2017 data.
Materials and Methods
Data Sources
The GBD data of IHD from 1990 to 2017 derived from the Global Health Data Exchange (GHDx) query tool, which is an ongoing global collaboration that uses all available up-to-date sources of epidemiological data and improved standardized methods to provide a comparative assessment of health loss from 359 diseases and injuries across 195 countries and territories worldwide. The methods used in the GBD have been described elsewhere, and data quality is globally recognized.13–15
In this study, we extracted estimates and their 95% uncertainty interval (UI) from GBD 2017 for the incidence, death, DALYs, and respective age-standardized rate (ASR) as measures of IHD burden (GBD cause code B.2.2, ICD-10 codes: I20-I25.9, ICD-9 codes: 410–414.9). ASRs were age-standardized using the GBD standard and reported per 100,000 population. We also collected the burden caused by level 3 and 4 risk factors.12 The Socio‐demographic Index (SDI),9 which is based on lag distributed income per capita, average educational attainment over the age of 15 years, and total fertility rate under the age of 25, was used to position countries on the development continuum, and to categorize the countries into five SDI quintiles. Ethical approval and consent from an institutional review board or ethics committee was not required for secondary analysis of data in this study.
GBD Estimation Framework
Detailed methodological information for IHD from the GBD 2017 estimates and modeling strategy were published elsewhere.9,13,14,16 A standard cause of death ensemble model (CODEm) approach was used to analyze mortality caused by IHD based on available data and added covariates.16 IHD mortality data were gathered from vital registration, verbal autopsy, surveillance systems, surveys, census or police reports.3,14
The non-fatal burden was obtained by estimating and adjusting the incidence and prevalence of acute myocardial infarction (MI), asymptomatic IHD, and angina using DisMod-MR (version 2.1), a meta regression-Bayesian modeling tool with three steps models.13 For MI, the prior remission rate was assumed to be one month, and the maximum excess mortality for all ages was assumed to be 10. Unstable angina was modeled as part of MI. For asymptomatic IHD, it was assumed that there was no remission. For Angina, it included a value prior of 0 for remission, and value before 1 for excess mortality for all ages.13
DALYs were calculated as the sum of Years lived with disability (YLDs) and years of life lost (YLLs).17 YLLs caused by IHD were calculated by subtracting the age at death from the life expectancy for a person of that age.18 YLDs were calculated by multiplying each sequela’s prevalence by its disability weight.19
The GBD study incorporated the comparative risk assessment (CRA) conceptual framework previously12 to quantify the burden of several causes and impairments attributable to 84 behavioral, environmental or occupational, and metabolic risks. We selected DALYs to model the attributable burden of causes and risks in this study.
Analysis Presented in This Paper
The number of incident cases, deaths, DALYs, and respective ASR (per 100,000 population) in different years were adopted to quantitatively estimate the trends of IHD. Trends in ASR reflect the alterations in human disease patterns and risk factors, so the estimated annual percentage change (EAPC) was introduced to describe the trend of ASR over a specified time interval. We also explored IHD burden from all 21 regions across all years from 1990 to 2017, used restricted cubic splines to flexibly model the associations of incidence, mortality, and DALY rates with SDI, dummy variables for outlier regions skewed fit to capture the average relationship for each group. The above statistical description and analyses were performed using the R program (Version 3.6.0, R core team). We assessed the temporal trend-changes on IHD burden from 1990 to 2017, by estimating the average annual percentage change (AAPC) for mortality, incidence, and DALYs with Joinpoint regression analysis. The AAPC is a summary measure of the trend within a pre-specified fixed interval, and it is a weighted average of the annual percentage change calculated by the Joinpoint model, whose weights equal to the length of the annual percentage change interval. We obtained AAPCs and their 95% confidence interval (CI) for each trend segment identified by the model from 1990 to 2017, with a maximum number of four points allowed. AAPC is considered the significance when it is different from 0 at the alpha of 0.05. Joinpoint analysis was performed using Joinpoint regression program version 4.6.0.0 (April, 2018) from the Statistical Research and Applications Branch, Surveillance Research Program of the US National Cancer Institute (NCI).
Result
Overall Status of Ischemic Heart Disease Burden in 2017
Globally, the incident cases of IHD have increased to 10.6 million (95% UI: 9.6–11.8) with an age-standardized incidence rate (ASIR) of 135.6 (122.2–150.4) per 100,000 persons in 2017 (Table 1). The number of IHD incident cases increased between 1990 and 2017, with a noticeable increase in middle and low SDI countries (1.11 and 1.04 times), and less obviously in high SDI countries. The global ASIR in 2017 was 27.4% lower than those of 1990s (135.6 cases per 100,000 population [122.2–150.4] vs 186.7 [171.4–203.2]).
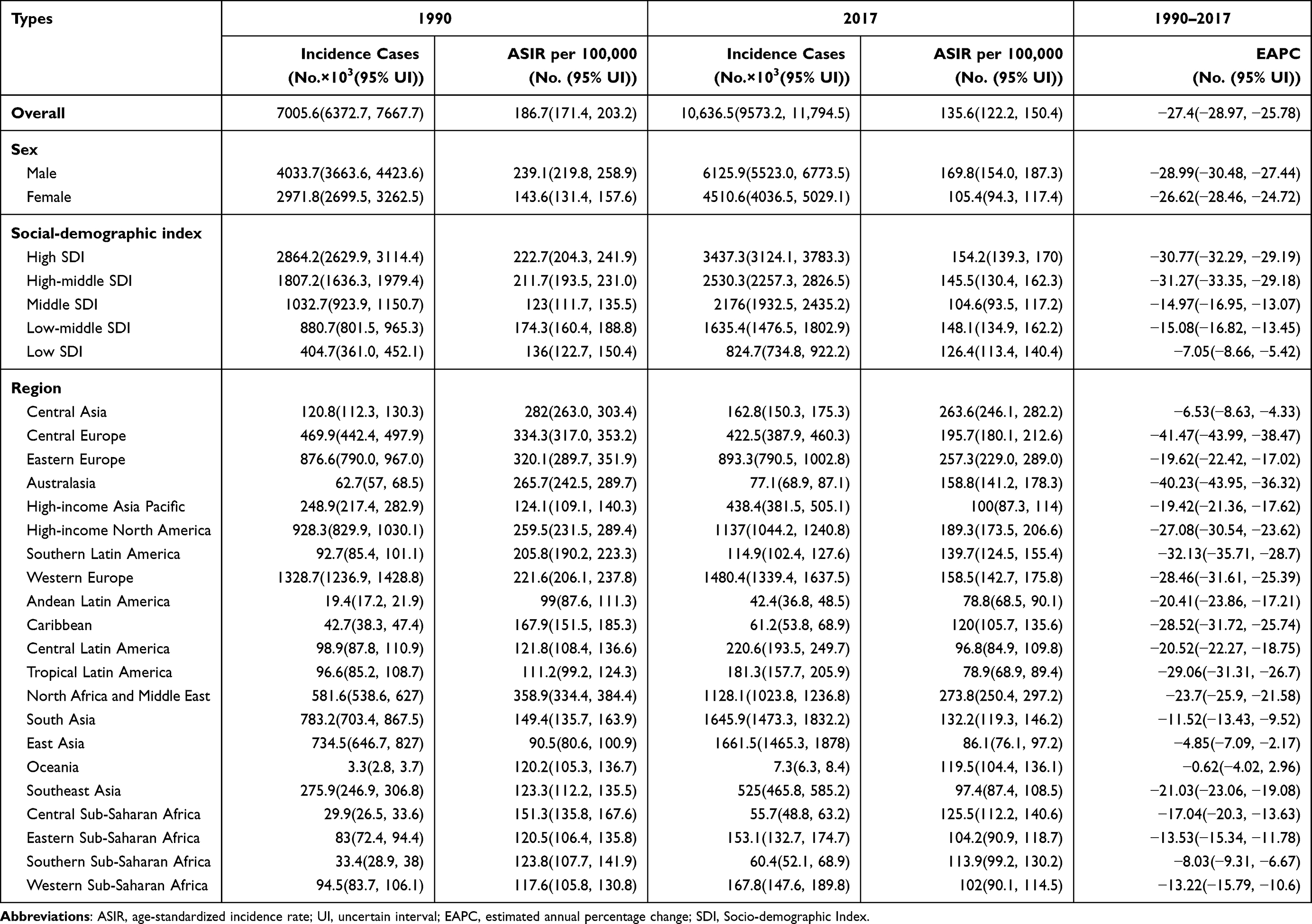 |
Table 1 The Incidence Cases and Age-Standardized Incidence of Ischemic Heart Disease in 1990 and 2017, and Its Temporal Trends from 1990 to 2017 |
The death number of IHD is 8.9 million (8.8–9.1) globally, with an age-standardized death rate (ASDR) of 117.0 (115.1–119.7) per 100,000 persons in 2017 (Table S1). IHD-related DALYs were 170.3 million (167.1–174.0) to which the middle SDI quintile contributed the most. Correspondingly, the age-standardized DALY rate was 2132.1 (2093.7–2179.8), with the greatest decline in high SDI quintile (59.3%) and least in the low SDI quintile (7.8%). The age-standardized DALY rates of low-middle and middle quintiles both fell by 10%, with the same downward trend (Table S1 and Figure 1).
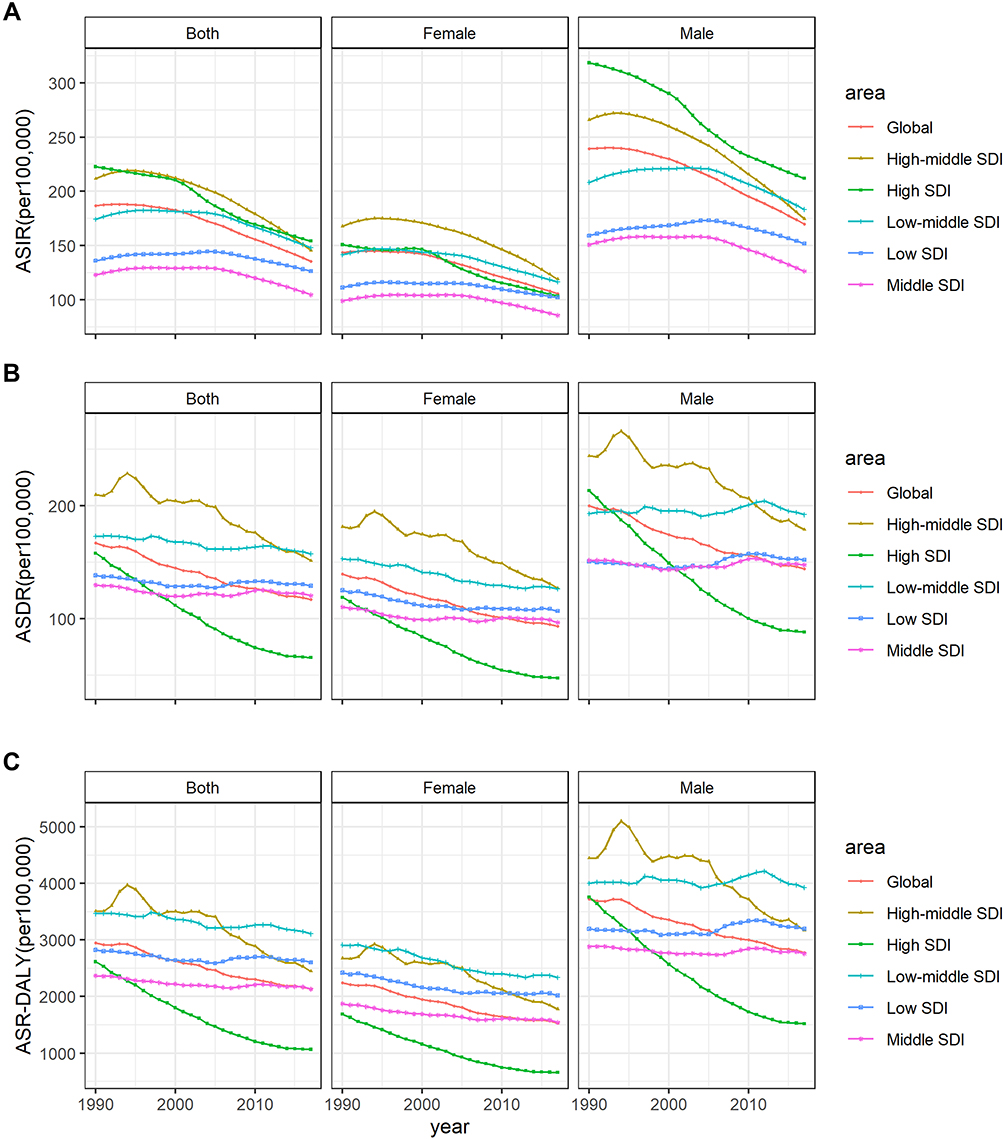 |
Figure 1 The age-standardized incidence(a), death(b), and DALY(c) rates of global ischemic heart disease for both sexes, 1990–2017. |
IHD Burden Affected by Age and Gender
In 2017, the numbers of IHD incident cases in males and females were 6.13 million (5.52–6.77) and 4.51 million (4.04–5.03), respectively (Table 1). The ASIR of males was 1.61 times that of females. The death and DALY rates of IHD in males were 1.55 and 1.81 times higher than those in females (Table S1).
The differences between age groups from 1990 to 2017 were demonstrated in Figure S1. The IHD incidence in the 70+ age group was the highest among the three age groups globally. The number of incident cases increased fastest in the middle SDI quintile compared to other SDI quintiles. The proportion of elderly incident cases was the largest among the three age groups, respectively, in high, high-middle, and middle SDI quintiles.
IHD Burden in Different Regions and Groups
From 1990 to 2017, the largest declines of ASIR were in high and high-middle SDI countries. Among the 21 GBD regions, North Africa and Middle East had the highest ASIR of IHD in 2017 (273.8 cases per 100,000, 95% UI: 250.4–297.2), followed by Central Asia and then Eastern Europe (Table 1, Figure 1). Young people in Oceania, Central sub-Saharan Africa (SSA), and Eastern SSA had relatively high IHD incidence rates. The lower the SDI level, the higher the proportion of young people. Moreover, elderly IHD incidence was higher in Western and Central Europe (Figure S2).
Regionally, IHD deaths were the highest in South Asia during the study period, reaching 1.9 (1.8–2.0) million cases in 2017. Since 1990, the ASDR of IHD has declined globally, especially in the high SDI quintile, with a decline of 58.4%. The largest increases in the ASDR have occurred in East Asia and Central Asia (Table S2). In 2017, Oceania, Central Asia, and Eastern Europe were the areas with the highest IHD related age-standardized DALYs among the regions. The age-standardized DALY rates increased in three regions including Central Asia, Oceania, and East Asia. Six regions including Central Europe, Australasia, and Western Europe showed the decreasing trend of DALY cases from 1990 to 2017 (Table S2).
IHD Burden and Sociodemographic Transition
The study showed significant trend changes and the estimated annual percentage change in incidence, mortality and DALY for periods covered by each trend (Table 2 and Figure S3). Joinpoint results showed that the incidences of all SDI quantile regions were downward trends. In the high SDI quintile, the ASIR decreased from 1990 to 2017, with an overall AAPC of −1.3%. However, other SDI quantile areas showed upward trends first and decreased thereafter. Similarly, the ASDR also showed the same decline in the high SDI quintile as the global trend, while other SDI quintiles showed fluctuation. DALYs also showed a similar trend with ASDR. The lower the regional SDI level, the higher the trend volatility.
 |
Table 2 Joinpoint Analysis for IHD-Related Age-Standardized Incidence, Mortality, and DALY Rate in Different SDI Quintiles, 1990–2017 |
When each region’s ASIR, ASDR and DALYs for each year from 1990 to 2017 were plotted against an index of that region’s sociodemographic status in the same year, the distinct patterns of epidemiological change were observed in Figure 2. Both an increase in SDI and a decline in IHD on mortality and DALYs occurred in many regions. Despite significant SDI improvement, IHD mortality did not decrease in East Asia and South Asia. The estimated relationship between SDI and ASRs shown as the black line, there was a gradual decline for ASDR and DALY rates as SDI increases, with a more rapid decline at the highest SDI levels.
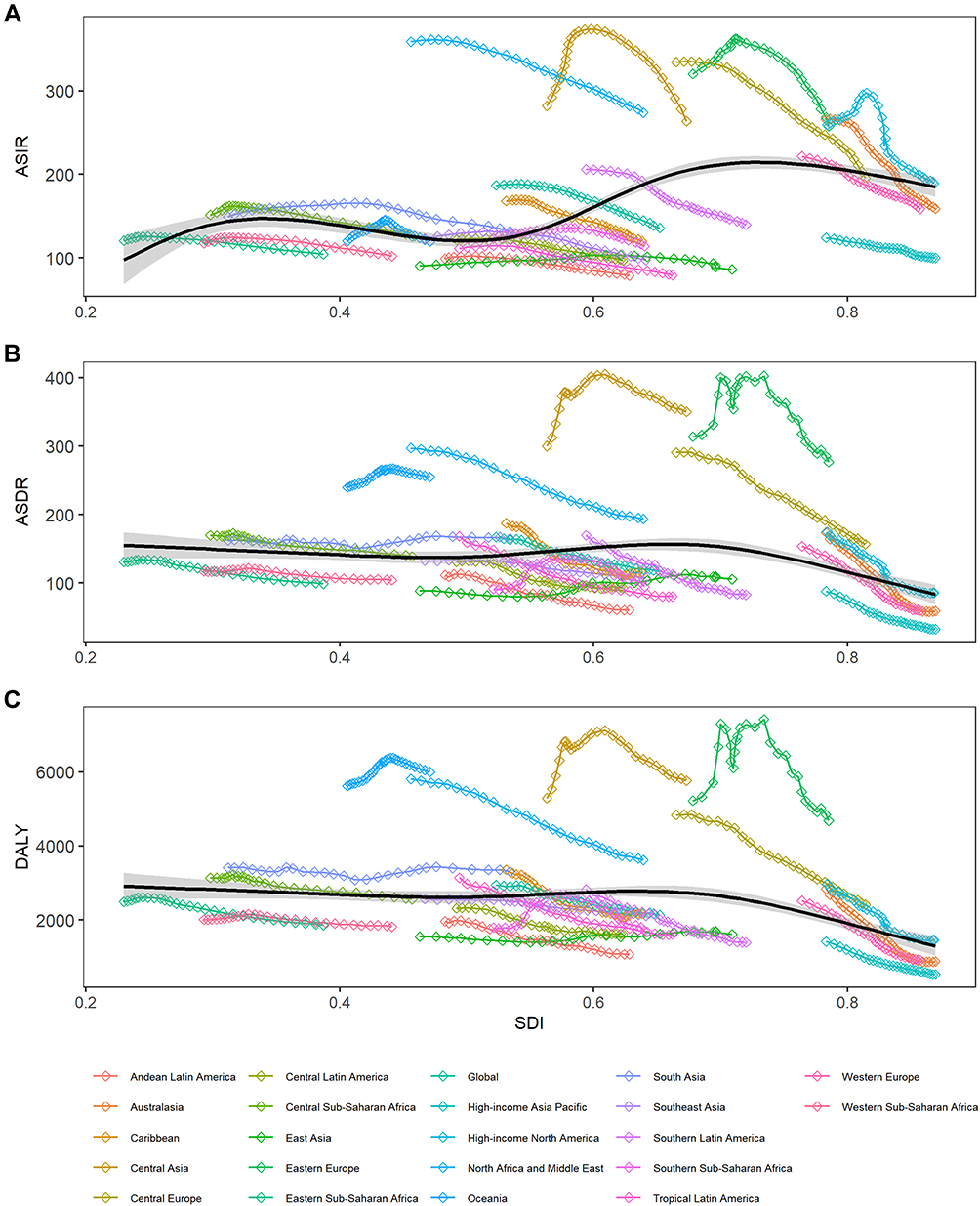 |
Figure 2 Relationship between the age-standardized incidence (A), death (B), and DALY (C) rates for IHD and social-demographic index over time. Each colored line represents a time trend of the relationship for the specified region. Each point represents a specific year for that region. The black line represents the overall global trend for the age-standardized rate of IHD concerning to SDI. |
Framlingham Risk Factors Attributable to IHD Burden
Figure 3 shows the ranking of risk factors that cause DALYs in different regions. Globally, high systolic blood pressure (SBP) was the most significant factor of DALYs in the most GBD regions in 2017, accounting for 94.8 million (81.1–107.5) DALYs, followed by high low-density lipoprotein (LDL) cholesterol, diet low in nuts and seeds (82.2 and 42.6 million, respectively) (Table S3). High LDL cholesterol was the leading risk of DALYs in five regions, most of which are high-income countries. It was noteworthy that South Asia was the only region where diet in low nuts and seeds contribute DALYs ranked the third, which also made it a third place in the ranking of global DALY. The three regions with the highest cumulative DALY rates caused by the top six risk factors were Oceania, Central Asia and Eastern Europe (Figure S4).
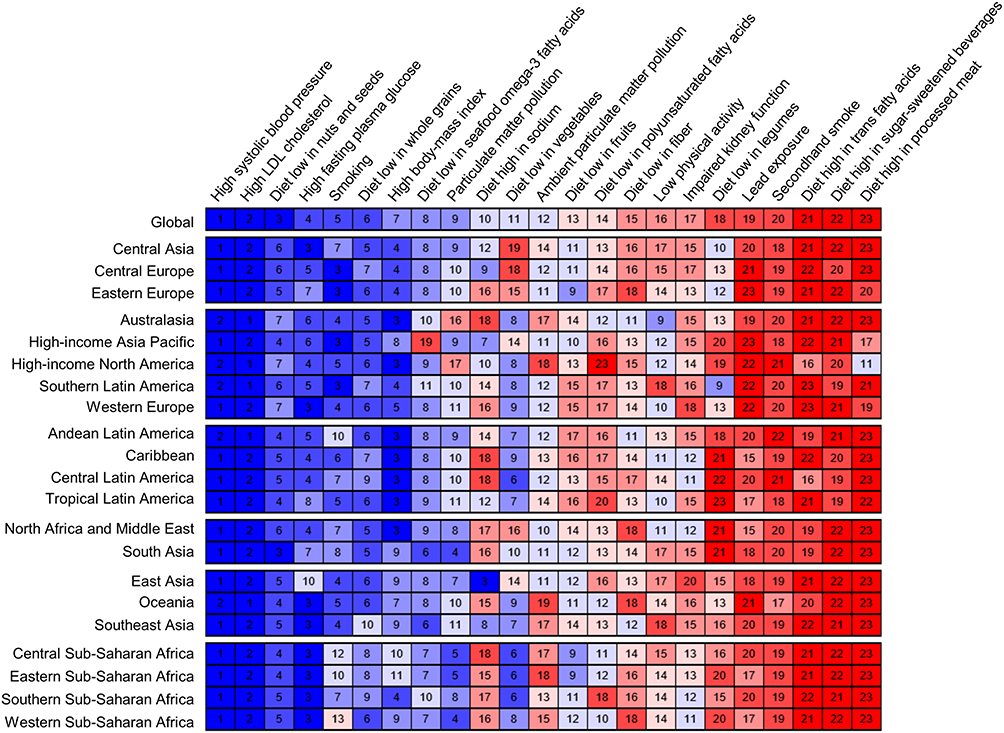 |
Figure 3 Ranking the risk factors for DALYs, by global and region, 2017. |
From 1990 to 2017, the DALY rate of IHD attribute to high SBP and high LDL cholesterol had fallen substantially (Figure S5). Notable declines occurred in the high SDI (−65.0% and −63.4%, respectively) regions. On the contrary, high SBP attributed to DALYs modest decline in the low (−4.3%), low-middle (−3.8%), and the middle (−4.5%) SDI quintiles, with very slight fluctuations. DALY rates from five other risk factors showed similar trend changes and fluctuations, except for high FPG.
For behavioral risk factors, dietary factors including diet low in nuts and seeds, and diet low in whole grains, showed highly similar decrease trends in all regions, with the smallest reductions in low SDI quantile subregion. For smoking, the significant reductions for DALYs in each region occurred between 1990 and 2017, with the most considerable reduction observed in the high SDI quantile (−72.9% [−74.3, −71.5]). DALY caused by smoking in high-middle SDI quantile had been the highest among all GBD regions.
Discussion
The study of the GBD 2017 data showed the change trends and patterns of the incidence, mortality, and DALYs of IHD worldwide, as well as their most relevant risk factors. This study revealed that the burden of IHD was high and vary widely between countries and territories, with the absolute number of cases showing an increasing trend in all 21 regions except Central Europe. The ASIR have the downward pattern in all countries, with the most quickly declining trends in high SDI countries. The number of deaths increased globally, with only the high SDI areas declined. IHD remained the leading cause of death worldwide in 2017, accounting for 15.96% of all deaths.14
IHD Burden in Different Regions and Groups
GBD 2017 (includes 195 countries and territories) was divided into 21 regions based on epidemiological similarities and geographical proximity by IHME.15 The data was collected and analyzed for top-down hierarchical estimation and real-time updated from more than 156 countries and territories by nearly 10,000 researchers.13 Our regional analysis showed that DALYs and death rate in all regions declined steadily with SDI increased during the same period.
The ASRs differences among regions may attribute to the differences in health care interventions, modifiable risk factors, and demography.20 Lower SDI levels, such as Africa and other LMICs, should have higher ASDR and ASIR due to low health literacy, low medical treatment level and unhealthy living habits.6,21 The burden of IHD is rising in SSA, which was previously considered a rare disease, and now it ranks 8th among the main causes of death for men and women in this region.22 Some studies showed that low SDI areas, such as SSA, are at the beginning of epidemiological transition, facing a contemporary double burden caused by infectious and non-communicable diseases.23,24 Other studies indicated, in low SDI regions, that IHD was relatively low due to few cardiovascular risk factors such as diabetes, obesity, metabolic disorders, and ethnic risk,6,25 and due to artificially low case-diagnosis rates and misclassification of potential causes of death with insufficient health care systems and scarcity of cardiac professionals.26
Eastern Europe, Central Europe and Central Asia of the 21 regions had the highest IHD death rates. In Eastern Europe, the ASDR has been declined steadily since 2005 after experiencing two upward and downward trends. Possible assumptions include socio-economic inequality, dietary habit difference, access to health care, and the proportion of health budget expenditures.27 It experienced two great events in the 20th century: the Revolutions of 1989 and the Dissolution of the Soviet Union. The series of revolutions in 1989 in Eastern Europe caused violent social unrest, and governments were also unstable or frequently changed in various countries.28 Since 1991, many communist parties in Europe have disbanded, and Central and Eastern European countries have generally experienced a transitional recession. The education and health systems had been severely damaged, and a higher risk of disease incidence and death was also shown.28,29 Belarus, for example, had the highest IHD incidence in Eastern Europe, which had been increasing since 1990, declining after 2010.30 High-middle SDI areas have higher mortality rates than those with high or low SDI areas, the causes of regional differences need to be considered from multiple perspectives. On the one hand, the decline rate in high-middle SDI quantile is slower than that in high SDI regions. The improvement of medical quality is related to the economic growth of a country.31 In high SDI areas, the early mortality level is relatively high. However, in the United States, Germany, Australia, and New Zealand, the overall mortality level of IHD has shown a rapid downward trend with the adoption of effective prevention measures of cardiovascular disease (CVD), and the use of innovative drugs, etc.32
On the other hand, due to low use of secondary prevention drugs and insufficient early diagnosis capabilities, and so on, the IHD mortality in some countries with low SDI was higher.21 While prevention and treatment levels have improved in high-middle SDI region since the economy developed, there have been changed in unhealthy lifestyles such as poor diet, lack of exercise, and sedentary lifestyle.33 The changes have become the main risk factors for CVD, such as high blood pressure, high fasting glucose, which will lead to higher ASDR. In Ukraine with high-middle SDI. An analysis in 2019 showed that high rate of smoking, obesity, and hypertension also contributed to its high IHD mortality.32 The high IHD death rate in Bulgaria related to the widespread alcohol abuse.34,35 A report showed that alcohol consumption of Bulgarians accounted for 1.7% of total consumer spending in 2017, which is higher than the EU average.36 In addition, other risk factors such as alcohol and psychological stress, also played a role in CVD mortality in Eastern Europe.28,37
Framingham Risk Factors
Risk factors for IHD include modifiable and non-modifiable factors. The Framingham Heart Study clarified to cardiovascular “risk factors” for the first time, including high blood pressure, hyperlipidemia and diabetes.38 The studies have shown that much of the burden on IHD can attributed to modifiable atherosclerotic risk factors.6,39 Non-modifiable risk factors include age (above 50 years), gender, genetics and family history of IHD. This study analyzed age patterns in different SDI regions in the past 27 years and found that the incident cases continued to increase globally since 1990, especially the most massive increase in age >75 years old, unlike the study by Dai et al.39 In the middle and below SDI regions, the incidence of the population over 50 years old increased rapidly. The risk was also significantly higher for men across the gender, similar in all regions.
This study analyzed 23 level-3 risk factors that caused the DALYs in order to the prevention and control of IHD. IHD causes many premature deaths, and patients who survive after treatment often have chronic disabilities. DALY is a standard global health metric routinely applied in health policy decision-making,40 it can provide a comprehensive measure of early mortality and treatment-related morbidity, and can also reflect the differences in different regions.17
High systolic blood pressure (SBP) remains the most critical risk factor for DALYs from IHD, although the attributable value has decreased since 1990. The fluctuations of high SBP in high-SDI quantiles were indeed close to that of all-cause deaths, but showed a different decreasing trend since 2005. Previous studies demonstrated that increased SBP is associated with increased CVD risk.41 In addition to a high prevalence of CVD itself, high blood pressure can also cause severe body multiple organ dysfunction.42 The prevalence of hypertension was very high in countries worldwide, especially in European and American countries.43,44 High fasting plasma glucose (FPG) was also considered a potential risk factor for IHD.32 Unlike the other five risk factors, in middle and below SDI quantiles, the contribution of high FPG showed a slight upward trend. This was also in line with the conventional understanding that obesity or hyperglycemia is more likely to occur in high-income countries or regions.45 In Oceania, Central Asia, North Africa and the Middle East, the phenomenon that high FPG leads to higher DALY, was considered to be due to local changes in food types, because incorrectly promoting high-calorie and low-nutrition foods will cause high FPG and obesity.45
As for dietary factors, globally, low seeds and nuts diet and low-whole-grain diet accounted for more than 25% of DALY among the top six risk factors, and ranked the third most significant risk. Because the South Asia (one of the most densely populated regions in the world, eg, India, and Bangladesh) was the only region where diet in low nuts and seeds contribute to DALYs ranked third, which also affects the ranking globally, made this diet ranked a third place of risk factors in the global DALY. Furthermore, the age-standardized DALY rate associated with the low nuts and seeds diet remains the highest in Eastern Europe. In most Western European countries (eg, Greece and Italy), high DALY caused by improper diet is relatively less than in other regions.46 Because Western Europe, adopts the Mediterranean dietary pattern, which is rich fruits, vegetables and whole grains, and low saturated fat, high monounsaturated fatty acids and dietary fiber.47 Smoking is another major behavioral risk factor.48 In Oceania, Central Asia, Central and Eastern Europe, smoking-related DALYs exceeded 1000 per 100,000 population. The WHO Eastern Mediterranean Region (EMR), which comprises 22 high, middle and low-income countries/territories, has a high prevalence of smoking, particularly among men.49 Smoking rates in EMR are currently estimated to be on the rise, although global smoking rates are falling under various measures.50 High SDI countries such as Iceland, Canada, and Norway have successfully reduced smokers’ prevalence by more than half through policy guidelines.51,52 However, many countries worldwide have taken measures to control tobacco and made some progress, tobacco still threatens people’s health all over the world, and further efforts are needed.53,54
The data in this study came from the estimates of GBD, and all GBD limitations were also applicable to this article. Although GBD provides a continuously improved high-quality estimate of the global burden of disease,55 there were some unavoidable limitations. For example, methods developed to estimate missing data and adjust for measurement differences among source studies were no real substitute for high-quality IHD surveillance data from every GBD region, using standardized case definitions and measurement methods. Furthermore, the estimates based on data from some countries, many of which lacked raw data and the estimates were influenced by parameters and models. However, GBD provided us with a reasonable basis for international comparison.
Conclusion
In summary, this analysis of the global burden of IHD showed that the trends of morbidity and mortality were decreasing globally, but the incidence, death and DALY of IHD were still at a high level and caused a considerable burden of disease. Most of the risk factors of IHD are modifiable, corresponding measures should be taken to cope with attributable risk factors and reduce the burden of IHD. IHD burden was difference in different SDI regions. It is necessary to learn successful and effective experience in controlling IHD risks and decreasing health disparities between countries with different development levels.
Abbreviations
ASIR, age-standardized incidence rate; ASDR, age-standardized death rate; AAPC, average annual percent change; CVD, cardiovascular disease; DALY, disability-adjusted life years; FPG, fasting plasma glucose; GBD, Global Burden of Disease Study; IHD, ischemic heart disease; LDL, low-density lipoprotein; UI, uncertainty interval; SDI, Socio‐demographic Index; SBP, systolic blood pressure.
Data Sharing Statement
The list of data sources used is publicly available at the Global Health Data Exchange website (http://ghdx.healthdata.org/gbd-results-tool), no additional data available.
Acknowledgments
We would like to thank the Institute for Health Metrics and Evaluation for the data.
Funding
This work was supported by the National Key Research and Development Program of China (No. 2018YFC1315302, 2017YFC1200502); the National Natural Science Foundation of China (Grant No. 81773552).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hartley A, Marshall DC, Salciccioli JD, Sikkel MB, Maruthappu M, Shalhoub J. Trends in mortality from ischemic heart disease and cerebrovascular disease in Europe:1980 to 2009. Circulation. 2016;133(20):1916–1926. doi:10.1161/CIRCULATIONAHA.115.018931
2. Khan MA, Hashim MJ, Mustafa H, et al. Global epidemiology of ischemic heart disease: results from the global burden of disease study. Cureus. 2020;12(7):e9349. doi:10.7759/cureus.9349
3. Mensah GA, Roth GA, Fuster V. The global burden of cardiovascular diseases and risk factors: 2020 and beyond. J Am Coll Cardiol. 2019;74(20):2529–2532. doi:10.1016/j.jacc.2019.10.009
4. Liu S, Li Y, Zeng X, et al. Burden of cardiovascular diseases in China, 1990–2016: findings from the 2016 Global Burden of Disease Study. JAMA Cardiol. 2019;4(4):342–352. doi:10.1001/jamacardio.2019.0295
5. India State-Level Disease Burden Initiative CVD Collaborators. The changing patterns of cardiovascular diseases and their risk factors in the states of India: the Global Burden of Disease Study 1990–2016. Lancet Glob Health. 2018;6(12):e1339–e1351. doi:10.1016/S2214-109X(18)30407-8
6. Yusuf S, Rangarajan S, Teo K, et al. Cardiovascular risk and events in 17 low-, middle-, and high-income countries. N Engl J Med. 2014;371(9):818–827. doi:10.1056/NEJMoa1311890
7. Lanas F, Serón P, Lanas A. Coronary heart disease and risk factors in latin america. Glob Heart. 2013;8(4):341–348. doi:10.1016/j.gheart.2013.11.005
8. Mendoza W, Miranda JJ. Global shifts in cardiovascular disease, the epidemiologic transition, and other contributing factors: toward a new practice of global health cardiology. Cardiol Clin. 2017;35(1):1–12. doi:10.1016/j.ccl.2016.08.004
9. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
10. Moran AE, Oliver JT, Mirzaie M, et al. Assessing the global burden of ischemic heart disease: part 1: methods for a systematic review of the global epidemiology of ischemic heart disease in 1990 and 2010. Glob.Heart. 2012;7(4):315–329. doi:10.1016/j.gheart.2012.10.004
11. Moran AE, Tzong KY, Forouzanfar MH, et al. Variations in ischemic heart disease burden by age, country, and income: the global burden of diseases, injuries, and risk factors 2010 study. Glob.Heart. 2014;9(1):91–99. doi:10.1016/j.gheart.2013.12.007
12. GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural,environmental and occupational, and metabolic risks or clusters of risks,1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1345–1422. doi:10.1016/S0140-6736(17)32366-8
13. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence,and years lived with disability for 354 diseases and injuries for 195 countries and territories,1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
14. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories,1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
15. Murray CJ, Ezzati M, Flaxman AD, et al. GBD 2010: design, definitions, and metrics. Lancet. 2013;380(9859):2063–2066. doi:10.1016/S0140-6736(12)61899-6
16. Foreman KJ, Lozano R, Lopez AD, Murray CJ. Modeling causes of death: an integrated approach using CODEm. Popul.Health.Metr. 2012;10(1):1–23. doi:10.1186/1478-7954-10-1
17. GBD 2017 DALYs and HALE Collaborators. Global, regional,and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories,1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859–1922. doi:10.1016/S0140-6736(18)32335-3
18. GBD 2017 Population and Fertility Collaborators. Population and fertility by age and sex for 195 countries and territories,1950–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1995–2051. doi:10.1016/S0140-6736(18)32278-5
19. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
20. Gwon JG, Choi J, Han YJ. Community-level socioeconomic inequality in the incidence of ischemic heart disease: a nationwide cohort study. BMC Cardiovasc Disord. 2020;20(1):87. doi:10.1186/s12872-020-01389-1
21. Mokdad AH, Forouzanfar MH, Daoud F, et al. Health in times of uncertainty in the eastern Mediterranean region,1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Glob Health. 2016;4(10):e704–e713. doi:10.1016/S2214-109X(16)30168-1
22. Mensah GA. Ischaemic heart disease in Africa. Heart. 2008;94:836–843. doi:10.1136/hrt.2008.142778
23. Brink AJ, Aalbers J. Strategies for heart disease in sub-Saharan Africa. Heart. 2009;95:1559–1560. doi:10.1136/hrt.2009.175745
24. Yuyun MF, Sliwa K, Kengne AP, Mocumbi AO, Bukhman G. Cardiovascular diseases in sub-saharan Africa compared to high-income countries: an epidemiological perspective. Glob Heart. 2020;15(1):15. doi:10.5334/gh.403
25. Walker AR, Sareli P. Coronary heart disease: outlook for Africa. J R Soc Med. 1997;90(1):23–27. doi:10.1177/014107689709000108
26. Mensah GA, Roth GA, Sampson UK, et al. Mortality from cardiovascular diseases in sub-Saharan Africa,1990–2013: a systematic analysis of data from the Global Burden of Disease Study 2013. Cardiovasc.J.Afr. 2015;26(2 Suppl1):S6–S10. doi:10.5830/CVJA-2015-036
27. Frost MJ, Tran JB, Khatun F, Friberg IK, Rodríguez DC. What does it take to be an effective national steward of digital health integration for health systems strengthening in low-and middle-income countries? Glob Health Sci Pract. 2018;6(Suppl1):S18–S28. doi:10.9745/GHSP-D-18-00270
28. Murphy A, Johnson CO, Roth GA, et al. Ischaemic heart disease in the former Soviet Union 1990–2015 according to the Global Burden of Disease 2015 Study. Heart. 2018;104(1):58–66. doi:10.1136/heartjnl-2016-311142
29. Roberts B, Stickley A, Balabanova D, Haerpfer C, McKee M. The persistence of irregular treatment of hypertension in the former Soviet Union. J Epidemiol Community Health. 2012;66(11):1079–1082. doi:10.1136/jech-2011-200645
30. GBD Compare(Viz Hub) [homepage on the Internet]. Institute for Health Metrics and Evaluation (IHME). Available from: http://ihmeuw.org/5j7h.
31. Lange S, Vollmer S. The effect of economic development on population health: a review of the empirical evidence. Br Med Bull. 2017;121(1):47–60. doi:10.1093/bmb/ldw052
32. Nowbar AN, Gitto M, Howard JP, Francis DP, Al-Lamee R. Mortality from ischemic heart disease. Circ Cardiovasc Qual Outcomes. 2019;12(6):e005375. doi:10.1161/CIRCOUTCOMES.118.005375
33. Kotseva K, De Backer G, De Bacquer D, et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur J Prev Cardiol. 2019;26(8):824–835. doi:10.1177/2047487318825350
34. Popova S, Rehm J, Patra J, Zatonski W. Comparing alcohol consumption in central and eastern Europe to other European countries. Alcohol Alcohol. 2007;42(5):465–473. doi:10.1093/alcalc/agl124
35. Ceci FM, Ceccanti M, Petrella C, et al. Alcohol drinking, apolipoprotein polymorphisms and the risk of cardiovascular diseases. Curr Neurovasc Res. 2021;18(1):150–161. doi:10.2174/1567202618666210406123503
36. Household spending on alcohol close to €130 billion [homepage on the Internet]. European Commission, Eurostatl. Available from: https://ec.europa.eu/eurostat/en/web/products-eurostat-news/-/ddn-20190101-1.
37. Ginter E. Cardiovascular disease prevention in eastern Europe. Nutrition. 1998;14(5):452–457. doi:10.1016/s0899-9007(98)00017-3
38. Mahmood SS, Levy D, Vasan RS, Wang TJ. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. Lancet. 2014;383(9921):999–1008. doi:10.1016/S0140-6736(13)61752-3
39. Dai H, Much AA, Maor E, et al. Global, regional, and national burden of ischemic heart disease and its attributable risk factors, 1990–2017: results from the global Burden of Disease Study 2017. Eur Heart J Qual Care Clin Outcomes. 2020:qcaa076. doi:10.1093/ehjqcco/qcaa076
40. Polinder S, Haagsma JA, Stein C, Havelaar AH. Systematic review of general burden of disease studies using disability-adjusted life years. Popul Health Metr. 2012;10(1):21. doi:10.1186/1478-7954-10-21
41. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi:10.1016/s0140-6736(02)11911-8
42. Lawes CM, Bennett DA, Lewington S, Rodgers A. Blood pressure and coronary heart disease: a review of the evidence. Semin Vasc Med. 2002;2(4):355–368. doi:10.1055/s-2002-36765
43. NCD Risk Factor Collaboration. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet. 2017;389(10064):37–55. doi:10.1016/S0140-6736(16)31919-5
44. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
45. Bhupathiraju SN, Hu FB. Epidemiology of obesity and diabetes and their cardiovascular complications. Circ Res. 2016;118(11):1723–1735. doi:10.1161/CIRCRESAHA.115.306825
46. Yu ITS, Li W, Wong TW. Effects of age, period and cohort on acute myocardial infarction mortality in Hong Kong. Int J Cardiol. 2004;97(1):63–68. doi:10.1016/j.ijcard.2003.07.032
47. Caprara G. Mediterranean-type dietary pattern and physical activity: the winning combination to counteract the rising burden of non-communicable diseases (NCDs). Nutrients. 2021;13(2):429. doi:10.3390/nu13020429
48. Prescott E, Scharling H, Osler M, Schnohr P. Importance of light smoking and inhalation habits on risk of myocardial infarction and all cause mortality. A 22 year follow up of 12149 men and women in the Copenhagen City Heart Study. J Epidemiol Community Health. 2002;56(9):702–706. doi:10.1136/jech.56.9.702
49. Heydari G, Zaatari G, Al-Lawati JA, et al. MPOWER, needs and challenges: trends in the implementation of the WHO FCTC in the Eastern Mediterranean Region. East Mediterr Health J. 2018;24(1):63–71. doi:10.26719/2018.24.1.63
50. World Health Organization. WHO Global Report on Trends in the Prevalence of tobacco use 2000–2025, third edition. Geneva; 2019.
51. Lund KE, Lund M, Bryhni A. Tobacco consumption among men and women 1927–2007. Tidsskr nor Laegeforen. 2009;129(18):1871–1874. doi:10.4045/tidsskr.08.0248
52. Slama K. Global perspective on tobacco control. Part I. The global state of the tobacco epidemic. Int J Tuberc Lung Dis. 2008;12(1):3–7.
53. Johnson NB, Hayes LD, Brown K, et al. CDC National Health Report: leading causes of morbidity and mortality and associated behavioral risk and protective factors–United States, 2005–2013. MMWR Suppl. 2014;63(4):3–27.
54. Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA. 2004;291(10):1238–1245. doi:10.1001/jama.291.10.1238
55. Phillips DE, Lozano R, Naghavi M, et al. A composite metric for assessing data on mortality and causes of death: the vital statistics performance index. Popul Health Metr. 2014;12:14. doi:10.1186/1478-7954-12-14
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.