Back to Journals » Journal of Healthcare Leadership » Volume 14
Giving 200%: Workplace Flexibility and Provider Distress Among Female Physicians
Authors Caperelli Gergel MC ![]() , Terry DL
, Terry DL ![]()
Received 22 January 2022
Accepted for publication 27 May 2022
Published 11 June 2022 Volume 2022:14 Pages 83—89
DOI https://doi.org/10.2147/JHL.S359389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Russell Taichman
Maria C Caperelli Gergel, Danielle L Terry
Guthrie Family Medicine Residency, Sayre, PA, 18840, USA
Correspondence: Danielle L Terry, Guthrie Family Medicine, One Guthrie Square, Sayre, PA, 18840, USA, Tel +1 570.887.3337, Email [email protected]
Introduction: Evidence suggests that female physicians experience higher rates of burnout compared to their male counterparts and are less likely to be satisfied with work-life integration. Understanding factors related to burnout and job turnover among female physicians is particularly relevant given the nationally projected physician shortage and maldistribution of providers. It may be particularly important to explore these factors among resident physicians, as many organizations might aim to pipeline these individuals into their existing workforce. This study aimed to (a) determine prevalence estimates of access to childcare and identify specific difficulties faced by working female physicians who are parents; (b) examine associations between provider distress and workplace flexibility; (c) examine differences in resident and non-resident physicians regarding workplace flexibility and access to parental resources.
Methods: Participants included 839 female medical providers who completed electronic surveys via social media. Descriptive, correlational, and linear regression analyses were used to examine associations.
Results: Few providers indicated that they had access to daycare through their workplace (7.2%, n = 62), but over three quarters of the group indicated that they wished they had access to daycare (76.0%, n = 638). Stress and burnout were negatively associated with how supported female physicians felt at work. This was the case for time off for parental leave, access to a comfortable space and adequate time for breastfeeding, flexibility of the job to handle family conflicts, and amount of time available for family and professional development.
Discussion: Future research might examine whether medical organizations that implement childcare facilities for working female physicians are more likely to retain and/or attract physicians to their employment.
Keywords: physician recruitment, work-family conflict, residents, childcare, medicine
The Association of American Medical Colleges projects a physician shortage by 2034, including deficits in both primary and specialty care.1 These shortages are particularly pronounced in rural and marginalized communities. Although the COVID-19 pandemic has highlighted shortages in a more visible way, population growth and an aging population have been identified as the two primary factors influencing demand.
Between 1990 and 2018, the number of female physicians in the US has grown from 16.9% to 35.8%.2 The number of females enrolled in medical school now exceeds the number of men, further adding to the growth of qualified female physicians.2 Currently, there are higher rates of female physicians who are entering into the primary care workforce.3
Despite a greater proportion of female physicians entering the workforce, it is estimated that nearly 40% of female physicians will leave the profession or reduce their medical practice early in their careers because of work-family conflict.4 Practice gaps exist between men and women, such that nearly a quarter of female physicians do not work fulltime, compared to only 3.6% of male physicians. This gap is even greater for female physicians who have children.4 Traditional expectations surrounding gender roles and mothers do not escape female physicians. Women physicians spend more time than their male colleagues on nonprofessional responsibilities, and on average, spend 8.5 hours more on domestic tasks compared to their male counterparts. For those that are married, male physicians with children spend 12 fewer hours per week on domestic tasks, while working on professional tasks for an average of seven hours longer.5
One framework for understanding differential outcomes in managing distress highlights the difference in resilience within a context of stress.6 Stressors are defined by both the extent of the stress exposure but also the type of the stressor, resulting from membership of a group or social identity. For example, women and other minority groups may exist within psychosocial contexts (eg, history of legalized discrimination, denial of civil rights, physical violence) that promote passive or emotion-focused coping. This can be contrasted with the promotion of problem-focused strategies that are more likely used by the majority or dominant group.
Evidence suggests that female physicians experience higher rates of burnout compared to their male counterparts and are less likely to be satisfied with work-life integration.7 Rates of burnout may be even greater among female physicians who are under 40 years of age.8 Understanding factors related to burnout and job turnover among female physicians is particularly relevant given the nationally projected physician shortage and maldistribution of providers.1 It may be important to explore these factors among resident physicians, as many organizations might aim to pipeline these individuals into their existing workforce.
The aims of the following study were to (a) determine prevalence estimates of access to childcare and identify specific difficulties faced by working female physicians who are parents (b) examine associations between provider distress and workplace access and flexibility (c) examine differences in resident and non-resident physicians regarding workplace flexibility and access to parental resources. It was hypothesized that resident physicians would report less workplace flexibility and available accommodations compared to non-resident physician parents. It was also expected that there would be negative associations between burnout and perceived support at work and access to parental/caregiver resources.
Methods
Participants included 839 female medical providers recruited via social media, Facebook © in two different groups that were specifically related to medical providers who were parents (ie, the identified objective of the group was to provide a forum for female physicians who had children). The survey was administered in August 2021. After obtaining permission from the group administrator, recruitment posts to complete an anonymous online survey were posted and an additional prompt was provided two weeks later. These were posted on the “posts” section of the Facebook feed. All procedures were approved by the Guthrie Institutional Review Board. All participants provided informed consent in accordance with the Declaration of Helsinki.
Demographic questions included age, medical specialty, number of children, resident status (ie, whether the provider was currently a medical resident) and race/ethnicity. Several questions assessed respondents estimated time for childcare leave, existence of daycare access at work, and breastfeeding practices.
Eight questions devised by a workgroup of three family medicine physicians assessed provider satisfaction and flexibility with their work environment, including time off for parental leave, feeling supported as a working parent, ability to breastfeed/pump, work around scheduling conflicts, ability to engage in professional development activities and spend time with family. Questions used Likert scale ratings from 1 (none/unsatisfactory) to 7 (completely/satisfactory). See Figure 1. Reliability for this scale was α = 0.80. Two additional questions inquired about providers’ regrets, including “Knowing what I know now, I would still choose to have a child at this stage in my career,” and “Knowing what I know now, I would still choose to have a career in medicine.” Responses ranged from 1 (strongly disagree) to 7 (strongly agree). Additionally, two questions assessed barriers to professional and time spent with family. Response options included an open-ended option.
 |
Figure 1 Additional survey questions. |
The Perceived Stress Scale, four-item version (PSS-4)9 was used to measure perceived stress. Frequency estimates ranged from 0 (never) to 4 (quite often). Items assessed perceived stress in the past month and included questions such as, “In the last month, how often have you felt that you were unable to control the important things in your life?” The PSS-4 has been widely used in a variety of settings, and more recently with medical providers.10 The reliability estimate was adequate for this sample (α = 0.81).
The Mini-Z was used as a proxy for burnout, a single item measure that has been identified as an adequate and more efficient substitute for the Maslach Burnout Inventory.11 The item asks respondents to indicate their level of burnout using their own definition, and they respond from 1 (I enjoy my work. I have no symptoms of burnout.) to 5 (I feel completely burned out and often wonder if I can go on. I am at the point where I may need some changes or may need to seek some sort of help.)
Data Analysis Plan
Data analyses were conducted using statistical software (IBM SPSS, Version 25). For individuals who were missing large portions of data (eg, began the survey, but did not complete the majority of it), those participants were removed from the survey. Otherwise, pairwise deletion was used to allow for greater use of data. Descriptive statistics were used to examine sample characteristics as well as frequencies and overall satisfaction with aspects of family care in their workplace (eg, whether facility offered daycare and if they wished they did). Spearman Rank Correlational analyses were used due to violation of the assumption of normality to examine whether there were associations between stress and other aspects of workplace flexibility. Linear regression analyses using a Bonferroni correction for multiple tests were used to examine whether resident/attending status predicted workplace flexibility and perceptions of workplace support.
Results
Respondents were 839 female medical providers who were mostly white (75.6%, n = 634), followed by Asian or Pacific Islander (11.7%, n = 98) and Latina or Hispanic (6%, n = 50). They were an average of 40.2 (SD = 6.3) years old and reported having an average of 2.2 (SD = 0.9) children. Providers were mostly attending physicians (90.9%, n = 763). Over one-third of respondents (40.2%, n = 337) practiced in Family Medicine (and sub-specialties), 17.6% (n = 148) in Pediatrics (and sub-specialties), and 13.1% (n = 110) in Internal Medicine (and sub-specialties). Of the sample, 16.9% (n = 142) were breastfeeding or pumping at the time they completed the survey. See Table 1.
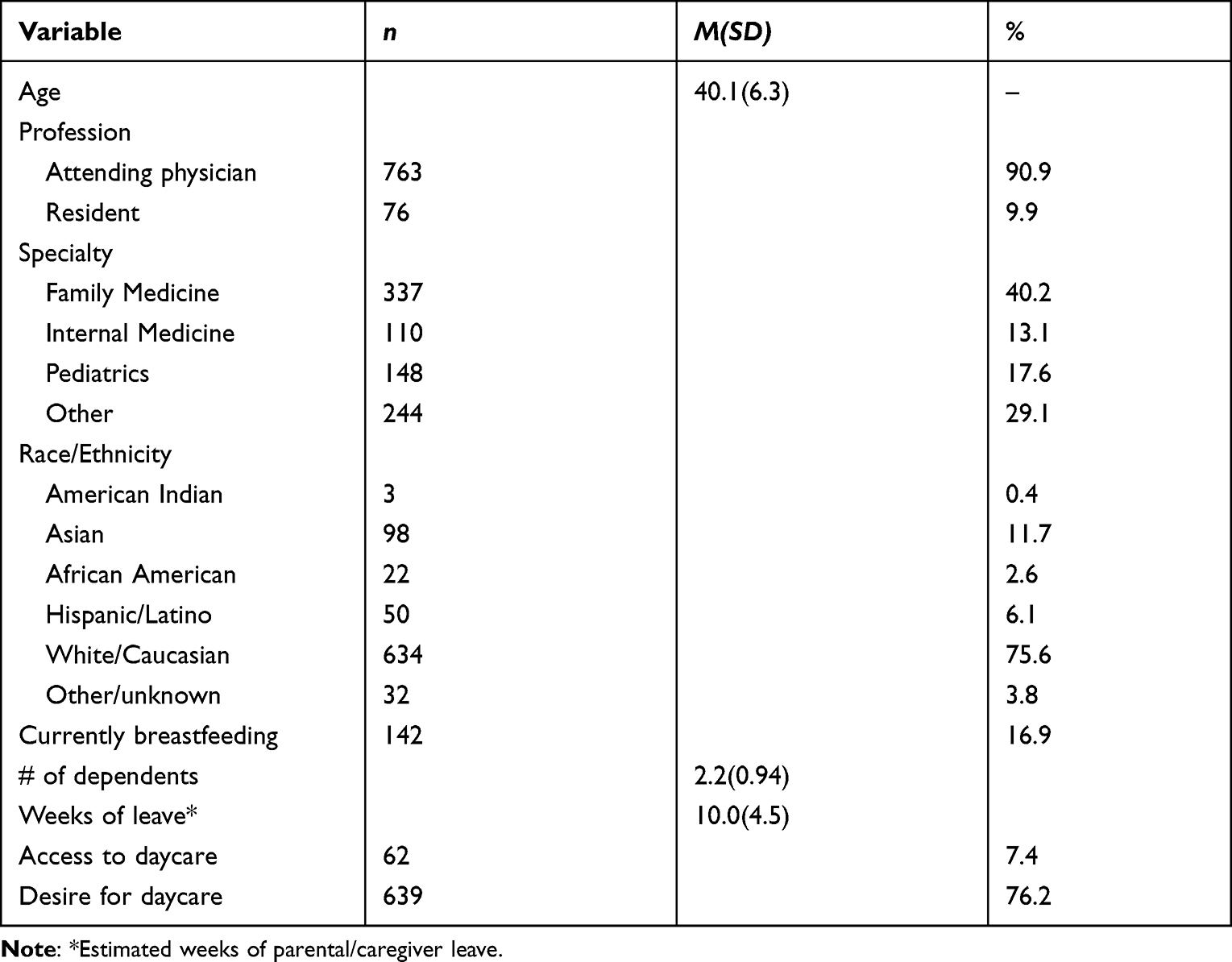 |
Table 1 Study Information (N = 839) |
Child and Work Regrets
Responses from questions asking whether women would still choose to have a child or would still choose a career in medicine were dichotomized to indicate whether women indicated any regrets about their career or family decisions. The majority of women (91.0%, n = 761) indicated that they agreed that they did not have regrets about having children and would make the same decision. However, 69.4% (n = 543) of women indicated that they would still choose a career in medicine, while 29.6% (n = 257) responded that they might choose a different career and/or were unsure.
Childcare
A minority of providers indicated that they had access to daycare through their workplace (7.2%, n = 62), but over three-quarters of the group indicated that they wished they had access to daycare (76.0%, n = 638). Physicians reported that they took an average of 9.9 (SD = 4.5) weeks of medical leave during the birth or adoption of their child/children. There was a significant difference between amount of parental leave that residents (n = 76) used compared to attending physicians (n = 763, t (820) = 4.89, p < 0.001). Resident physicians reported using significantly fewer weeks of leave (M = 7.5, SD = 3.1) compared to attending physicians (M = 10.2, SD = 4.5).
Barriers to Family Time and Professional Development
Female providers reported that the most common barriers to spending time with their family were needing to do other chores in their homes (75.9%, n = 626) followed by excessive fatigue after a workday (69.0%, n = 569) and not having enough time due to their work schedules (53.7%, n = 443). Providers reported that the most common barrier to their professional development was choosing to spend time with their family instead (86.2%, n = 716), followed by the need to do chores or other tasks around the home (74.2%, n = 619), and feeling too fatigued from work (68.7%, n = 573).
Distress and Work Flexibility
Results of the Pearson correlational analyses indicated that perceived stress and burnout were negatively associated with how supported physicians felt at work (r = −0.43, p < 0.001; r =−.42, p < 0.001). In addition, analyses indicated that time off for parental leave, access to a comfortable space and adequate time for breastfeeding, flexibility of the job to handle family conflicts, and amount of time available for family and professional development were all significantly negatively associated with stress and burnout (range of r = -. 11 to −0.47, p < 0.001). See Table 2 for correlation matrix.
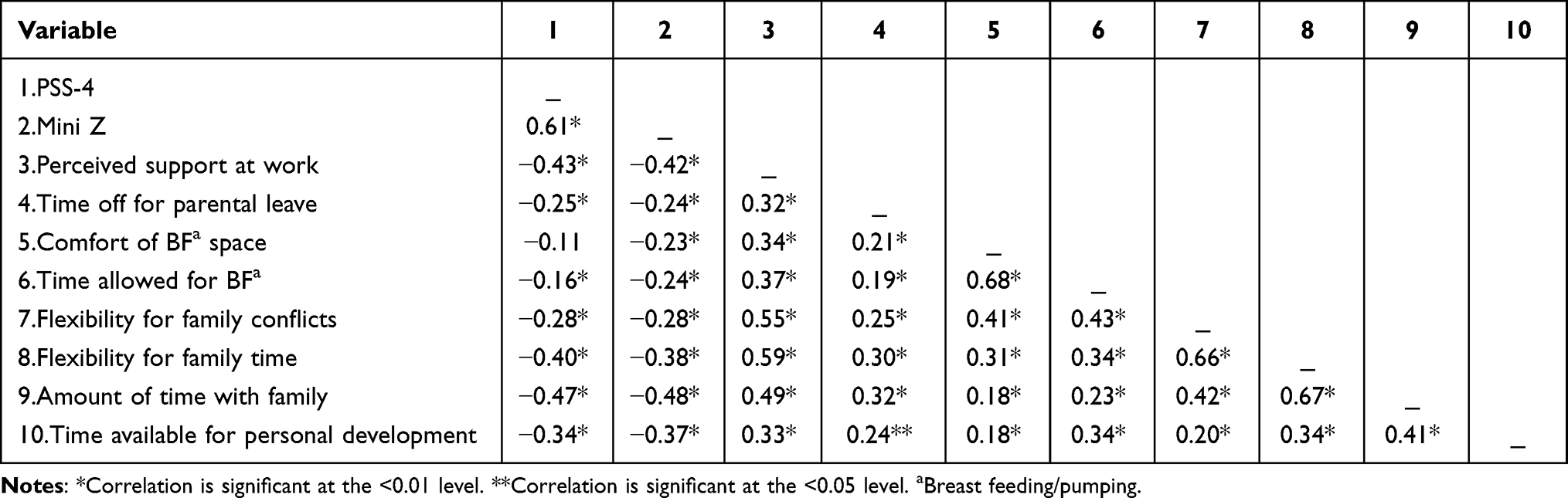 |
Table 2 Correlations of Study Variables (N = 840) |
Resident and Attending Comparisons
Four independent linear regression analyses controlling for race/ethnicity using Bonferroni correction for multiple tests indicated that residents did not significantly differ from attendings on responses to the Mini Z (burnout) or PSS-4 (stress). Resident respondents were from 20 different specialties, with the highest proportion from family medicine (n = 15, 21.1%) and pediatrics (n = 16, 22.5%). Residents and attendings did not significantly differ in the time and space allotted for breastfeeding/pumping, and/or personal development. However, residents reported significantly less flexibility in the workplace related to family conflicts (eg, sick children; F (2, 812) = 7.30, p = <0.001) and amount of flexibility to allow for additional time with family (F (2, 814) = 10.85, p = <0.001). That is, results indicated that residents had less ability to spend additional time with their families and tend to their family’s needs.
Discussion
This study aimed to better understand factors related to burnout and stress among female physicians. Other research has suggested that work-family conflict is one driver of burnout, and these conflicts pose a threat to those resources that preserve well-being. Understanding utilization and whether there is a desire for onsite childcare and workplace flexibility may be useful for healthcare management entities. In addition, identifying discrepancies between resident and attending physician experiences may be useful as organizations attempt to pipeline trainees into their organization.
There are several implications of this study. First, findings highlight a discrepancy between what female physicians have access to, and what they would desire in their workplace. Consistent with previous research,2 our findings suggested that access to childcare was a challenge faced among female physicians. Less than 10% of respondents reported that they had access to childcare at their work location, yet over 75% reported they wished their facility offered it. Future research might examine whether medical organizations that implement childcare facilities for working female physicians are more likely to retain and/or attract physicians to their employment. Other reviews have suggested that investment in strategies that improve retention of employees and may also improve the overall success of a company.12 Access to these resources may help ease the burden physician mothers face when searching for reliable childcare.
Second, consistent with our hypothesis, this study suggested that the workplace flexibility and access to resources was worse among medical residents. Notably, medical residents in this study reported that, on average, they took nearly three fewer weeks for parental leave compared to attending female physicians. Residents also reported significantly less flexibility to allow for time with family and less flexibility related to managing family conflict (ie, sick children). These findings are not surprising considering the additional training demands expected of many medical residency programs. Other studies have suggested that the demands of residency are associated with complications in pregnancy, such as increased risk of gestational hypertension, placental abruption, preterm labor, and intrauterine growth restriction (IUGR).13 On average, female physicians tend to have their first child 7.4 years later than other females.13 Stentz and colleagues found that 25% of female physicians would have attempted to start a family sooner and 65.3% of respondents reported that their career influenced childbearing decisions “quite a bit” to “very much.” Providing mechanisms to support these providers may allow for greater quality of life, reduced pregnancy complications, and increase retention and allegiance to an organization. Considering the overlap in the childbearing years, the desire to retain and pipeline qualified residents into organizations from residency training programs, administrative decisions that consider organizational strategies to support residents who are working parents may support these organizational goals.
Finally, consistent with our hypotheses, stress and burnout were negatively associated with how supported female physicians felt at work. This was the case for time off for parental leave, access to a comfortable space and adequate time for breastfeeding, flexibility of the job to handle family conflicts, and amount of time available for family and professional development. The finding that greater stress and burnout are associated with poorer work flexibility and access to parental resources is not particularly surprising. Evidence suggests that female physicians report greater burnout compared to males,14,15 and work–family conflict has been associated with greater burnout and stress.16 In the general population, compared to men, women have greater social consequences for working while managing a family, including remaining single, having fewer children, or experiencing divorce.17 Female physicians spend more time on household tasks and caring for children than their male counterparts.2 More male physicians report having a spouse that stays home to take care of household responsibilities, while female physicians are more likely to have a spouse that is employed full-time. Our findings suggest that female physicians identified these types of tasks (household tasks) as a barrier to spending time with family and focusing on personal development. Notably, our findings suggested that most women did not regret having children; however, a sizeable portion of them (29.6%) expressed doubt about whether they would make the same decision about choosing a career in medicine.
Formal work policies that aim to address some of the disproportional work burden of family management may enhance gender diversity and retention in the workplace.18,19 Although there are numerous ways to create family-friendly policies and practices (eg, access to paid sick days, family leave, alternative work schedules, flexible scheduling, telework), access to onsite childcare and flexible scheduling is one of several aspects to consider in addition to others that could be explored among working physicians. It is also the case that having increased flexibility in scheduling, working from home, parental leave policies and pre-tax childcare payment benefits all genders.20 Future research might examine both the existence and utilization of other resources available to working parents, and how that might impact their professional choices within an organization. Furthermore, examining gender differences related to the impact of policy change among physicians may provide additional information that aids in the retention, recruitment, and measures of wellbeing of physicians.
There were several limitations in this study. First, findings are limited by use of convenience sampling, which may also limit the generalizability. Although the sample size was large, the group required self-selection and identification of parental status. This may have resulted in a sample that was more heavily invested and interested in parenting and parenting resources.
Second, the sample is also comprised of female providers. Physician burnout disproportionately impacts female providers.2 However, it also impacts providers of other genders, and physician turnover and burnout are a nationwide concern. Future studies might consider multi-site sampling with use of parents with other gender-identities. This would also allow for comparisons to address specific needs of medical providers and any gender differences. This study was cross-sectional, and limits conclusions that can be made about the directionality of correlational findings. Finally, these data were collected during the COVID-19 pandemic, and parents and medical providers have been identified as vulnerable populations.10,21 Scores on burnout and stress measures may have been exacerbated by this unique time in history.
Consent Statement
All participants provided informed consent, in accordance with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest and/or funding sources in this work.
References
1. Association of American Medical Colleges. The complexities of physician supply and demand: projections from 2017–2032; 2020. Available from: https://aamc-black.global.ssl.fastly.net/production/media/filer_public/31/13/3113ee5c-a038-4c16-89af-294a69826650/2019_update_-_the_complexities_of_physician_supply_and_demand_-_projections_from_2017-2032.pdf.
2. Chesak SS, Cutshall S, Anderson A, Pulos B, Moeschler S, Bhagra A. Burnout among women physicians: a call to action. Curr Cardiol Rep. 2020;22(7):45. doi:10.1007/s11886-020-01300-6
3. Accreditation Council for Graduate Medical Education. Data resource book: academic year 2020–2021; 2021. Available from: https://www.acgme.org/globalassets/pfassets/publicationsbooks/2020-2021_acgme_databook_document.pdf.
4. Frank E, Zhao Z, Sen S, Guille C. Gender disparities in work and parental status among early career physicians. JAMA Netw Open. 2019;2(8):e198340–e198340. doi:10.1001/jamanetworkopen.2019.8340
5. Jolly S, Griffith KA, DeCastro R, Stewart A, Ubel P, Jagsi R. Gender differences in time spent on parenting and domestic responsibilities by high-achieving young physician-researchers. Ann Intern Med. 2014;160(5):344–353. doi:10.7326/M13-0974
6. Turner RJ, Avison WR. Status variations in stress exposure: implications for the interpretation of research on race, socioeconomic status, and gender. J Health Soc Behav. 2003;44(4):488–505. doi:10.2307/1519795
7. Marshall AL, Dyrbye LN, Shanafelt TD, et al. Disparities in burnout and satisfaction with work–life integration in U.S. Physicians by gender and practice setting. Acad Med. 2020;95(9):1435–1443. doi:10.1097/ACM.0000000000003521
8. Eden AR, Jabbarpour Y, Morgan ZJ, Wilkinson E, Peterson LE. Burnout among family physicians by gender and age. J Am Board Fam Med. 2020;33(3):355. doi:10.3122/jabfm.2020.03.190319
9. Cohen ST, Kamarch R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–396. doi:10.2307/2136404
10. Terry DL, Hui P, Buntoro S. The initial positive and negative impacts of the COVID-19 pandemic on rural healthcare providers: associations with team culture and leadership. J Healthc Manag. 2021;66(5):396–406.
11. Rohland BM, Kruse GR, Rohrer JE. Validation of a single-item measure of burnout against the Maslach Burnout inventory among physicians. Stress Health. 2004;20(2):75–79. doi:10.1002/smi.1002
12. Amaram DI. Attracting and retaining women talent in the global labor market: a review. J Hum Resour. 2019;7(1):1–10.
13. Stentz NC, Griffith KA, Perkins E, Jones RD, Jagsi R. Fertility and childbearing among American female physicians. J Womens Health. 2016;25(10):1059–1065. doi:10.1089/jwh.2015.5638
14. Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clin Proc. 2015;90(12):1600–1613. doi:10.1016/j.mayocp.2015.08.023
15. Shanafelt TD, Dyrbye LN, Sinsky C, et al. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016;91(7):836–848. doi:10.1016/j.mayocp.2016.05.007
16. Weinhold I, Gurtner S. Understanding shortages of sufficient health care in rural areas. Health Policy. 2014;118(2):201–214. doi:10.1016/j.healthpol.2014.07.018
17. Tower LE, Alkadry MG. The social costs of career success for women. Rev Public Pers Adm. 2008;28(2):144–165. doi:10.1177/0734371X08315343
18. Johnson M. Child care assistance: Georgia’s opportunity to bolster working families, economy. Ga Budg Policy Inst Rep. 2015;2015. doi:10.1377/forefront.20110907.013460
19. Matos K. Modern families: same and different sex couples negotiating at home. NY Fam Work Inst. 2015;76:1–12.
20. Feeney MK, Stritch JM. Family-friendly policies, gender, and work–life balance in the public sector. Rev Public Pers Adm. 2019;39(3):422–448. doi:10.1177/0734371X17733789
21. Russell BS, Hutchison M, Tambling R, Tomkunas AJ, Horton AL. Initial challenges of caregiving during COVID-19: Caregiver burden, mental health, and the parent–child relationship. Child Psychiatry Hum Dev. 2020;51(5):671–682. doi:10.1007/s10578-020-01037-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.