Back to Journals » Journal of Pain Research » Volume 18
Ginger Moxibustion Activates TRPV1 to Modulate the Locus Coeruleus-Spinal Cord-Uterus Pathway and Alleviates Primary Dysmenorrhea in Rats
Authors Wang X ![]() , Yang L, Bi K
, Yang L, Bi K ![]() , Zhou M
, Zhou M ![]() , Wang D, Zhao Z, Mi S, Li X
, Wang D, Zhao Z, Mi S, Li X
Received 5 August 2025
Accepted for publication 17 December 2025
Published 25 December 2025 Volume 2025:18 Pages 7109—7125
DOI https://doi.org/10.2147/JPR.S554548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Xiaoyan Wang,1,2,* Liyun Yang,1,2,* Kuo Bi,1,2 Min Zhou,1,2 Di Wang,1,2 Zhiguo Zhao,1 Shuqi Mi,1,2 Xinhua Li1,2
1College of Acupuncture-Moxibustion and Tuina, Hebei University of Chinese Medicine, Shijiazhuang, Hebei, People’s Republic of China; 2Hebei International Joint Research Center for Dominant Diseases in Chinese Medicine and Acupuncture, Hebei University of Chinese Medicine, Shijiazhuang, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuqi Mi, College of Acupuncture-Moxibustion and Tuina, Hebei University of Chinese Medicine, No. 3 Xingyuan Road, Shijiazhuang, Hebei, 050200, People’s Republic of China, Email [email protected] Xinhua Li, College of Acupuncture-Moxibustion and Tuina, Hebei University of Chinese Medicine, No. 3 Xingyuan Road, Shijiazhuang, Hebei, 050200, People’s Republic of China, Email [email protected]
Objective: To investigate the effect of ginger moxibustion at “Shenque” (CV8) and “Guanyuan” (CV4) acupoints on primary dysmenorrhea (PD) rats and explore the possible anti-inflammatory and analgesic mechanism.
Methods: Forty female Sprague-Dawley (SD) rats were randomly divided into five groups: blank group (BG), model group (MG), ginger moxibustion group (GMG), antagonist capsazepine group (CPZG), and ibuprofen group (IG). PD models were established via cold stimulation combined with estradiol benzoate and oxytocin administration. GMG received ginger moxibustion, CPZG was pretreated with CPZ before ginger moxibustion, and IG received ibuprofen via gavage. Post-intervention, rat pain thresholds and writhing scores were measured; uterine pathology was observed via HE staining; Enzyme-linked immunosorbent assay (ELISA), immunohistochemistry (IHC), immunofluorescence (IF), and Western blotting (WB) were used to measure relevant biomarkers.
Results: Ginger moxibustion significantly elevated pain thresholds and reduced writhing scores (vs MG, P< 0.01). Capsazepine partially reversed these effects (vs GMG, P< 0.05). Ginger moxibustion up-regulated TRPV1 and SP expression at acupoints (vs MG, P< 0.01), whereas capsazepine suppressed their expression (vs GMG, P< 0.01). Ginger moxibustion decreased uterine NE levels while increasing NE concentrations in both the spinal cord and locus coeruleus (vs MG, P< 0.01); Following CPZ antagonism, uterine NE increased while central NE decreased (vs GMG, P < 0.05). Ginger moxibustion downregulated serum TNF-α, IL-6 and uterine PGF2α (vs MG, P < 0.01), while upregulating β 2-AR expression; It promoted M2-type polarization of macrophages (increased CD206 and M2/M0 ratio, decreased CD86 and M1/M0 ratio, P < 0.01), with CPZ partially reversing this effect.
Conclusion: Ginger moxibustion at “Shenque” (CV8) and “Guanyuan” (CV4) acupoints exerts synergistic analgesic and anti-inflammatory effects by activating the TRPV1 channels in acupoint areas, initiating the bidirectional regulation of the locus coeruleus-spinal cord-uterus norepinephrine (NE) pathway, and inducing M2 polarization of macrophages.
Keywords: primary dysmenorrhea, ginger moxibustion, TRPV1, norepinephrine, macrophage polarization
Introduction
Primary dysmenorrhea (PD) is a common gynecological disorder clinically characterized by lower abdominal pain during or around menstrual periods, which may be accompanied by symptoms such as lower abdominal distension, lumbar soreness, headache, nausea, and diarrhea that may affect daily life and work. According to international epidemiological studies, the incidence of PD ranges from 45% to 95%, making it a significant public health issue.1,2 The pathogenesis of PD remains not fully elucidated, but modern medicine largely attributes it to be the excessive prostaglandin secretion triggering uterine smooth muscle contractions and reduced uterine blood flow.3,4 Current clinical guidelines for PD recommend Nonsteroidal Anti-inflammatory Drugs (NSAIDs) as first-line treatments; however, these medications can produce side effects on cardiovascular, gastrointestinal, hepatic, and renal functions.5,6 Hence, it is of great necessity to explore safe, effective non-pharmacological therapies without toxic side effects. Traditional Chinese Medicine (TCM) posits that cold stimulation constitutes the primary etiological factor for dysmenorrhea, inducing uterine spasms and pain.7 Moxibustion, as an external therapy in TCM, is widely used in the treatment of PD and has few adverse reactions.8–10 A 2025 network meta-analysis of non-pharmacological therapies for PD revealed that moxibustion demonstrate greater efficacy than acupuncture in improving VAS scores of PD.11
It has confirmed that moxibustion, a thermal stimulation, activating Transient Receptor Potential Vanilloid Subfamily Member 1 (TRPV1) channel is one of the certain mechanism.12 TRPV1 is a non-selective cation channel whose activation elevates intracellular cation concentrations, particularly calcium, participating in multiple physiological and pathological processes including pain, inflammation and immunity.13,14 Previous studies have revealed that inflammation serves as a crucial pathological alteration in PD, potentially associated with the induction of central sensitization that contributes to chronic pain development.15–17 Recent studies have shown that the sympathetic nervous system can modulate inflammation by releasing NE to activate immune cell receptors.18,19 Meanwhile, some scholars have found that NE can induce macrophage polarization to the M2-type to achieve anti-inflammatory and tissue repair effects, which may involve the NE-mediated activation of β2-adrenergic receptors (β2-AR) promoting fatty acid uptake, conversion, and storage so as to potentiating M2-type functional capabilities.20 The Locus Coeruleus (LC) is the largest noradrenergic neuron group in the central nervous system, and it may be a new target for anti-inflammation and analgesia.21,22 Besides, previous studies have demonstrated that moxibustion activates TRPV1 to produce analgesic effects in PD rats and alleviates uterine inflammation, while NE-induced macrophage transformation is closely associated with inflammation regulation.16,23 Therefore, it is speculated that the anti-inflammatory and analgesic effects of moxibustion are closely related to the activation of TRPV1 channels at acupoints and the regulation of NE expression in the central nervous system and target organs as well as macrophage polarization.
In this study, ginger moxibustion at “Shenque” (CV8) and “Guanyuan” (CV4) acupoints was used to treat PD rats. Comparing with Ibuprofen and CPZ (Antagonist of TRPV1), and observing the therapeutic effects were through HE staining, immunohistochemistry, immunofluorescence, ELISA assays, and Western blotting, we evaluated therapeutic efficacy on PD. We further investigated the regulatory effects of acupoint TRPV1 channels on central nervous system modulation, target organ NE expression, and macrophage polarization.
Methods
Experimental Animals
Specific pathogen-free (SPF)-grade female nulliparous Sprague-Dawley (SD) rats (weighing 160–180 g; 6–8 weeks) were purchased from Beijing Vital River Laboratory Animal Technology Co., Ltd. (License No. SCXK (Jing) 2021–0006). The rats were allowed free access to food (standard rat chow: 15–20 g/rat/day) and water at a controlled temperature of 18–26°C, relative humidity of 45–60%, and a 12-hour light/dark cycle. This study was conducted in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals (NIH Publication No. 80–23, Revised 1996) and the International Association for the Study of Pain’s Ethical Guidelines for Studies Involving Conscious Animals. The experimental protocol was approved from the Laboratory Animal Ethics Committee of Hebei University of Chinese Medicine (Approval No. DWLL202203115).
Establishment and Treatment of PD Model Rats
Based on the conventional sample size standard in the field of PD animal model research (6–8 animals per group), this study set 8 rats for each experimental group to ensure sufficient statistical power. Ultimately, all 40 rats successfully completed the experiment and were included in the analysis.15–17,24 Forty experimental rats were acclimatized for three days. Rats in the diestrus phase were screened via vaginal smear cytology based on cell morphology, type, and quantity, and were randomly divided into five groups using a random number table: blank group (BG), model group (MG), ginger moxibustion group (GMG), antagonist capsazepine group (CPZG), and ibuprofen group (IG), with 8 rats in each group.
As illustrated in Figure 1, all groups, except the blank group, underwent daily cold stimulation on an ice surface (20 min/day) for 12 consecutive days. Concurrently, the rats received subcutaneous injections of estradiol benzoate (Cat: No. 20240102, Hefei Xinkexin Animal Pharmaceutical Co., Ltd.) at 0.4 mg/rat/day, with additional doses of 0.8 mg/rat on days 4 and 15. One hour after the last estradiol benzoate injection, oxytocin (Cat: No. 20240227, Jiangxi Bolai Pharmacy Co., Ltd.) was administered intraperitoneally at 2 U/rat. Successful model establishment was confirmed by the following behavioral responses: pronounced shivering, huddling, reduced activity with a curled posture, writhing reactions, abdominal retraction, and trunk/hindlimb extension, accompanied by pelvic and unilateral limb rotation.
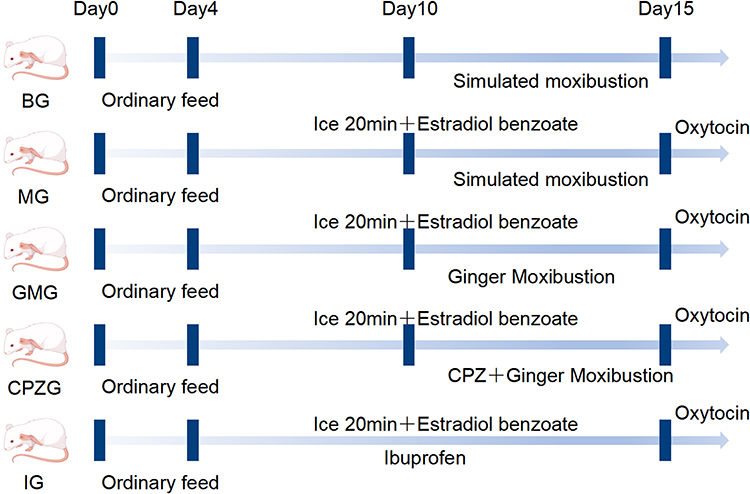 |
Figure 1 Intervention and modeling methods for each group of rats. |
From days 10 to 15, the blank and model groups underwent mock handling without any intervention. In the GPM group, the acupoints “Shenque” (CV8) and “Guanyuan” (CV4) were localized according to the “Experimental Acupuncture Science” rat acupoint standards. Starting from day 10, 75 min post-modeling, a ginger slice (20 mm diameter, 3 mm thickness) was placed over the acupoints, followed by an ignited moxa cone (2 cm diameter, 1.5 cm height) for 10 min, maintaining a local temperature of 43°C. The treatment was performed once daily for six consecutive days. The CPZ group followed the same GPM protocol but received an additional pre-moxibustion intervention: 10 min before each session, 50 μL of capsazepine (CPZ; Cat: No. 138977–28-3, MCE, Wuhan) at 0.5 mg/mL was injected into each acupoint (total 100 μL per rat).25 In the ibuprofen group, from days 4 to 15, ibuprofen tablets (Cat: No. 230202, Guangdong Huanan Pharmaceutical Group Co., Ltd.) were administered via gavage (prepared at 125 mg/100 mL in saline, 6.25 mg/kg/day) 75 min post-modeling, once daily for 12 days.
Behavioral Observation
Within 10–30 minutes after intraperitoneal oxytocin injection on day 12 (administered to all groups except BG), BG received an equivalent volume of normal saline. Writhing responses were observed and scored according to the following criteria: Grade 0, normal behavior; Grade 1, body tilting or unilateral rotation; Grade 2, hind limb extension; Grade 3, abdominal turning with hind limb extension. Writhing score = (Grade 0×0 points) + (Grade 1×1 point) + (Grade 2×2 points) + (Grade 3×3 points). Simultaneously, the abdominal mechanical pain threshold of rats was measured using a Von Frey electronic algesimeter (BIO-EVF4-S, BIOSEB, China). Measurements were taken three times per rat, with the average value recorded.
Histopathological Examination
After perfusion, the uterine tissues were fixed in 4% paraformaldehyde, dehydrated in a graded ethanol series, embedded in paraffin, and sectioned to a thickness of 4 μm. The sections were stained with hematoxylin and eosin (HE) to evaluate histopathological changes. Observations were performed using a light microscope (DFC450C, Leica, China) at 200× magnification.
Enzyme-Linked Immunosorbent Assay (ELISA)
Serum levels of TNF-α, IL-4, IL-6, and IL-10, uterine PGF2α, and NE in the uterus, lumbar spinal cord, and locus coeruleus were measured using ELISA kits.
- Rat IL-4 ELISA Kit (Cat: No. D731009, BBI, Shanghai)
- Rat IL-6 ELISA Kit (Cat: No. D731010, BBI, Shanghai)
- Rat IL-10 ELISA Kit (Cat: No. D731011, BBI, Shanghai)
- Rat TNF-α ELISA Kit (Cat: No. D731168, BBI, Shanghai)
- Rat PGF2α ELISA Kit (Cat: No. D731028, BBI, Shanghai)
- NE ELISA Kit (Cat: No. D751020, BBI, Shanghai)
Protein concentrations were determined using a Lowry assay kit (Cat: PC0030, Solarbio, Beijing). All procedures were performed according to the manufacturer’s protocols.
Immunohistochemistry
Following perfusion, the acupoint skin and uterine tissues were fixed in 4% paraformaldehyde, dehydrated, and paraffin-embedded. For immunohistochemical staining, 4 μm sections were dewaxed in xylene and rehydrated using graded ethanol. After antigen retrieval and blocking, the sections were incubated overnight at 4°C with primary antibodies against TRPV1 (Cat: No.bs-23926R, 1:300, Bioss, Beijing) or β2-AR (Cat: No. bs-0947R, 1:300, Bioss, Beijing). Secondary antibodies were applied at room temperature, followed by DAB staining and hematoxylin counterstaining of the cells. The slides were observed under a light microscope (DFC450C, Leica, China) at 200× magnification. The integrated optical density (IOD) was quantified using the ImageJ software.
Immunofluorescence
Tissue processing was performed following the same protocol described in Section 2.5. For immunofluorescence, the sections were incubated overnight at 4°C with primary antibodies against CD86 (Cat: No. 26903-1-AP, 1:400, Proteintech, Wuhan) or CD206 (Cat: No. 18704-1-AP, 1:400, Proteintech, Wuhan), followed by secondary antibodies conjugated with D-594 fluorophore. After additional antigen retrieval, the sections were incubated with F4/80 primary antibody (Cat: No. 28463-1-AP, 1:400, Proteintech, Wuhan) overnight at 4°C, followed by D-488-conjugated secondary antibodies. The nuclei were counterstained with DAPI-containing antifade mounting medium. Fluorescence images were captured using a microscope (DM750, Leica, China) at 100× magnification, and IOD was quantified with ImageJ software.
Western Blotting Analysis
Protein extracts from the acupoint skin and uterine tissues were analyzed using the following primary antibodies:
- TRPV1 (Cat: No.bs-23926R, 1:1000, Bioss, Beijing)
- β2-AR (Cat: No.bs-0947R, 1:1000, Bioss, Beijing)
- GAPDH (Cat: No.bs-10900R, 1:10000, Bioss, Beijing) as loading control
Immunoreactive bands were visualized by film development, scanned (Epson Perfection V39, Japan), and quantified using the ImageJ software. The band intensities were normalized to GAPDH.
Statistical Analysis
Statistical analyses were performed using Prism 10.1.2 software. Measurement data conforming to normal distribution with homogeneous variance were expressed as mean ± standard deviation (SD) and analyzed by one-way analysis of variance (ANOVA) followed by Tukey’s test. For data not conforming to normal distribution, the rank-sum test was used to compare medians and interquartile ranges (IQR). Categorical data were analyzed using the chi-square test. A significance level of P < 0.05 was adopted.
Results
Comparison of Behavioral Indicator
As shown in Figure 2, Compared with BG, rats in MG exhibited increased writhing scores and decreased pain thresholds (P <0.01). Compared with MG, rats in GMG, CPZG, and IG showed decreased writhing scores and increased pain thresholds (P <0.01). Compared with GMG, rats in the CPZG demonstrated increased writhing scores and decreased pain thresholds (P <0.05, P <0.01).
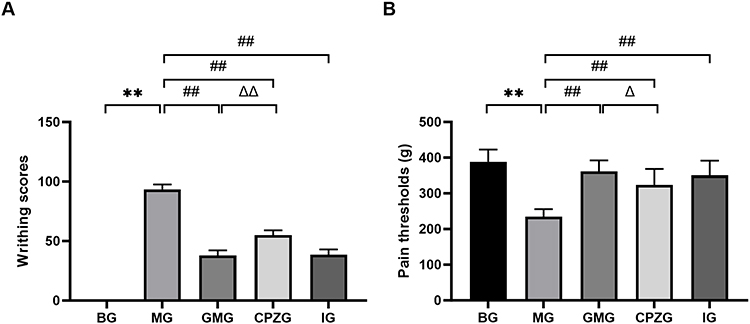 |
Figure 2 Behavioral Indicators in Rats Across Groups, (A) Comparison of writhing scores in rats. (B) Comparison of pain thresholds in rats. (**P<0.01 vs BG; ##P<0.01 vs MG; ΔP<0.05, ΔΔP<0.01 vs GMG.). |
HE Staining of Uterine Tissues of Rats
As shown in Figure 3. In BG, the morphology of the uterine tissue was regular, the endometrial epithelial cells were arranged neatly in columns, and no inflammatory cell infiltration was observed in the tissue. In MG, congestion of the endometrium, a large number of vacuolar degeneration and necrosis, and inflammatory cell infiltration, mainly by neutrophils, were visible in the uterine tissue of rats. In GMG, the uterine tissue structure was similar to that of the blank group, with occasional congestion and necrosis. In CPZG and IG, the morphology of the uterine tissue of rats was relatively regular, vacuolar degeneration and death of endometrial epithelial cells were reduced, and a small amount of inflammatory cell infiltration was visible.
 |
Figure 3 The HE staining results of the uteruses of rats in each group (magnification 200×). The yellow, blue, red, and black arrows represent vacuolar degeneration, neutrophil infiltration, hyperemia, and necrosis, respectively. |
Comparison of PGF2α Content in the Uterus of Rats
PGF2α is a key indicator for evaluating PD. As shown in Figure 4, compared with BG, the PGF2α content in the uterus of rats in MG increased (P < 0.01). Compared with MG, the PGF2α content in the uterus of rats in GMG, CPZG, and IG decreased (P < 0.05 or P < 0.01). Compared with GMG, the PGF2α content in the uterus of rats in the CPZG increased (P < 0.01).
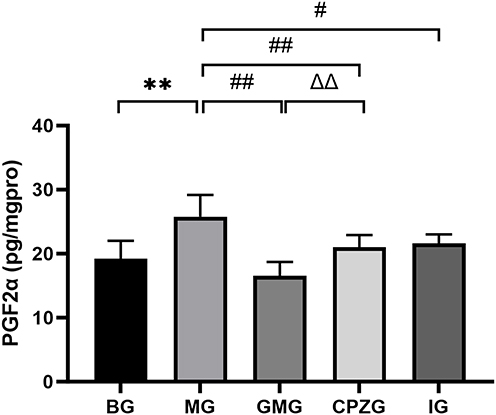 |
Figure 4 The content of PGF2α in the uterus of each group of rats. (**P<0.01 vs BG; #P<0.05, ##P<0.01 vs MG; ΔΔP<0.01 vs GMG.). |
Comparison of TRPV1 and SP Expression in the Acupoint Areas of Rats
As shown in Figures 5 and 6, compared with BG, the expression of TRPV1 and SP in the acupoints of rats in MG was significantly increased (P < 0.01). Compared with MG, the expression of TRPV1 and SP in GMG and CPZG was increased (P < 0.05 or P < 0.01), whereas TRPV1 and SP expression at acupoints was significantly suppressed in CPZG compared with GMG (P <0.05 or P <0.01).
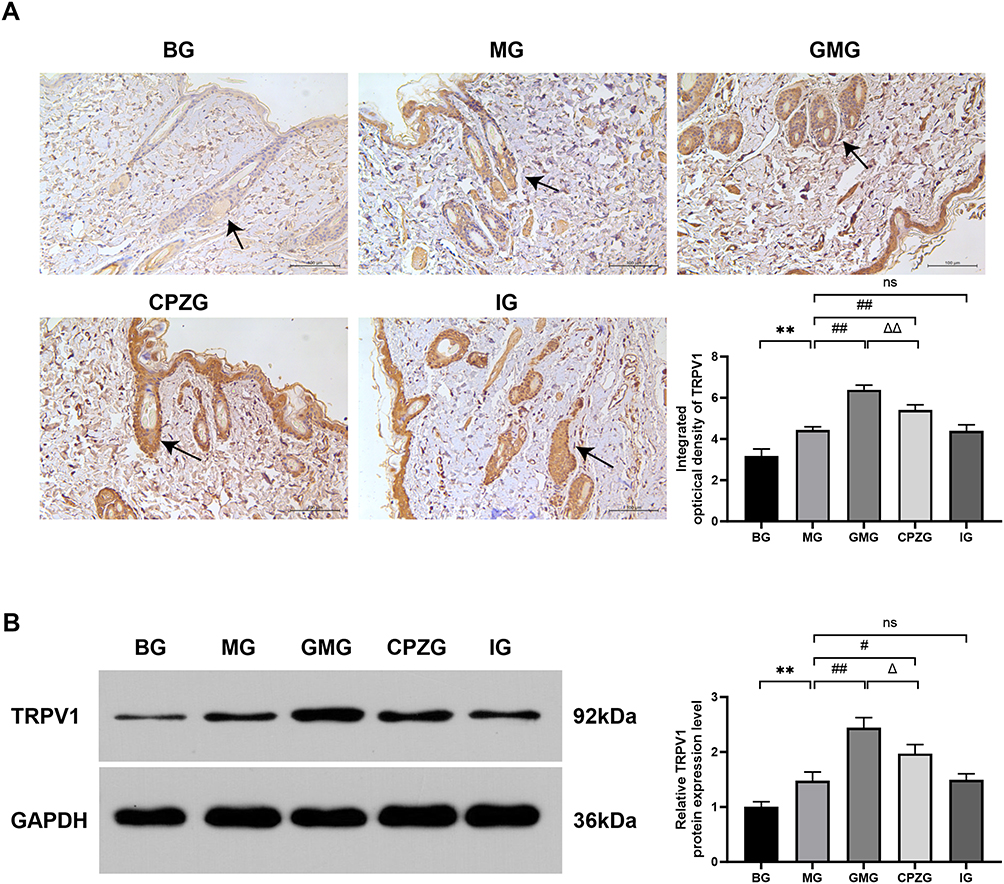 |
Figure 5 Expression of TRPV1 in acupoint areas of rats in each group. (A) Immunohistochemical staining image. The arrow represents the positive expression area (magnification 200×). (B) Western blot band. (**P<0.01 vs BG; #P<0.05, ##P<0.01 vs MG; ΔP<0.05, ΔΔP<0.01 vs GMG; ns: not significant.). |
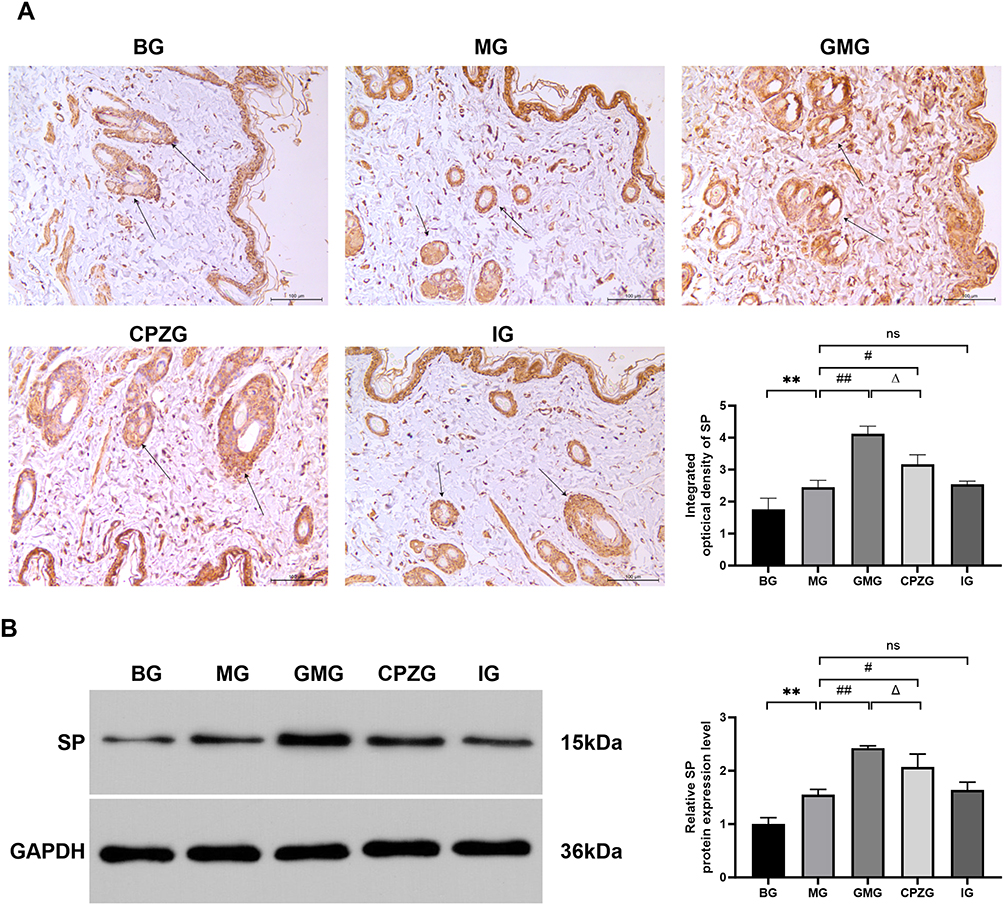 |
Figure 6 Expression of SP in acupoint areas of rats in each group. (A) Immunohistochemical staining image. The arrow represents the positive expression area (magnification 200×). (B) Western blot band. (**P<0.01 vs BG; #P<0.05, ##P<0.01 vs MG; ΔP<0.05 vs GMG; ns: not significant.). |
Comparison of NE content in the uterus, spinal cord, and locus coeruleus nucleus and β2-AR expression in the uterus of rats
As shown in Figure 7, compared with BG, the NE content in the uterus of MG increased (P < 0.01), and the NE content in the spinal cord and locus coeruleus nucleus decreased (P < 0.05 or P < 0.01). Compared with MG, the NE content in the uterus of GMG, CPZG, and IG decreased (P < 0.05 or P < 0.01), and the NE content in the spinal cord and locus coeruleus nucleus increased (P < 0.05 or P < 0.01). Compared with GMG, the NE content in the uterus of rats in CPZG increased (P < 0.05), and the NE content in the spinal cord and locus coeruleus nucleus decreased (P < 0.05).
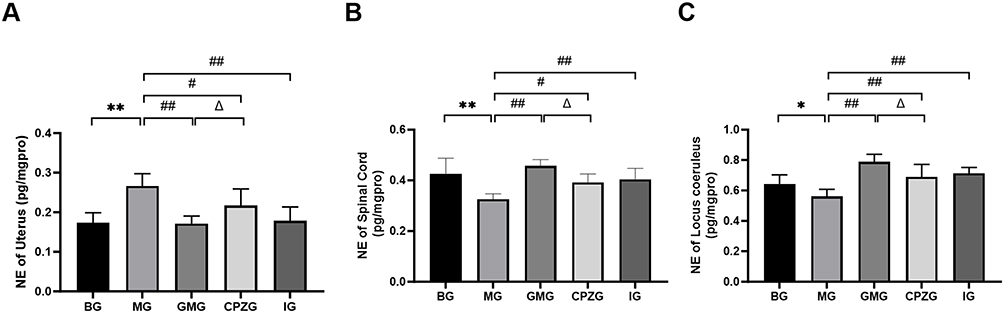 |
Figure 7 The NE content in the uterus, spinal cord, and locus coeruleus of rats in each group. (A) NE levels in the uterus. (B) NE levels in the spinal cord. (C) NE levels in the locus coeruleus. (*P<0.05, **P<0.01 vs BG; #P<0.05, ##P<0.01 vs MG; ΔP<0.05 vs GMG.). |
As shown in Figure 8, compared with BG, the expression of uterine β2 - AR in MG was decreased (P < 0.01). Compared with MG, the expression of uterine β2 - AR in GMG, CPZG, and IG was increased (P < 0.05 or P < 0.01). Compared with GMG, the expression of uterine β2 - AR in CPZG was decreased (P < 0.05 or P < 0.01).
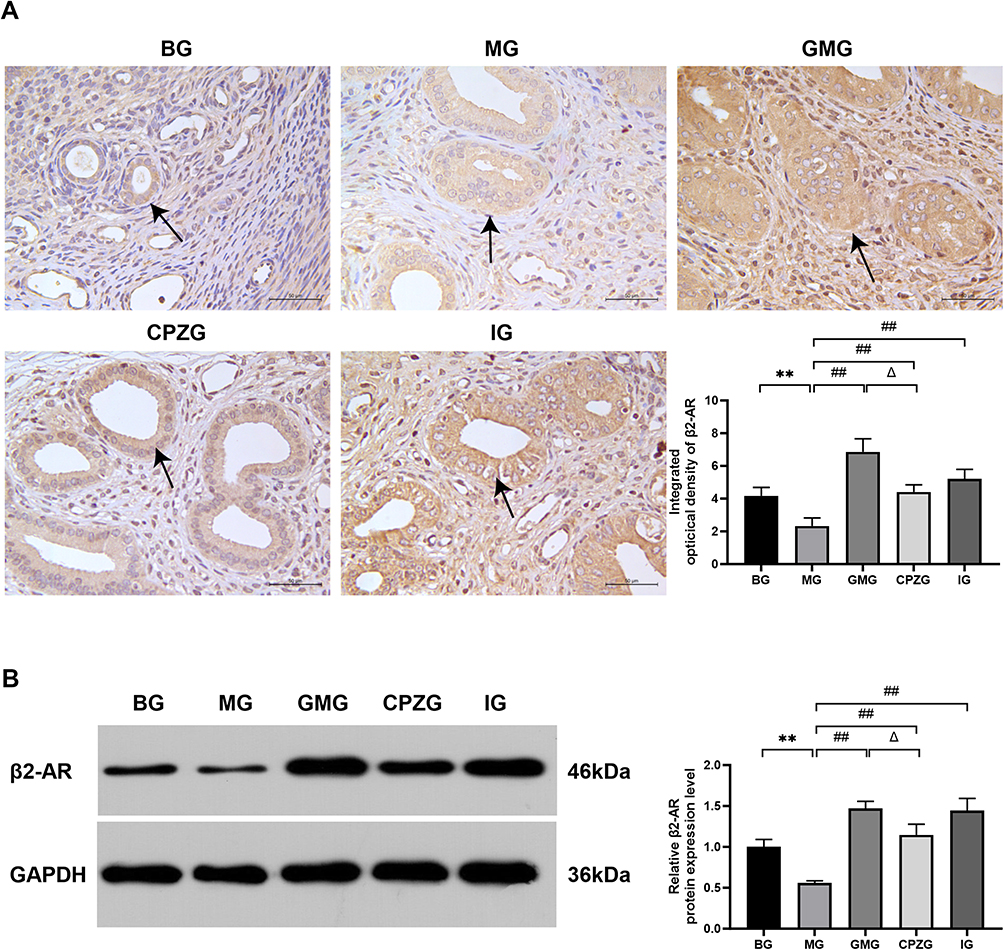 |
Figure 8 Expression of β2 - AR in the uterus of each group of rats. (A) Immunohistochemical staining image. The arrow represents the positive expression area (magnification 200×). (B) Western blot band. (**P<0.01 vs BG; ##P<0.01 vs MG; ΔP<0.05 vs GMG.). |
Comparison of Macrophage Distribution in Each Group of Rats
CD86 is a marker of M1 polarization of macrophages. The ratio of M1/M0 macrophages was compared by co-staining with CD86 and F4/80. As shown in Figure 9, compared with BG, the expression of CD86 in the uterus and the M1/M0 ratio in MG increased (P < 0.01). Compared with MG, the expression of CD86 in the uterus and the M1/M0 ratio in GMG, CPZG, and IG decreased (P < 0.05 or P < 0.01). Compared with GMG, the expression of CD86 in the uterus and the M1/M0 ratio in CPZG of rats increased (P < 0.05).
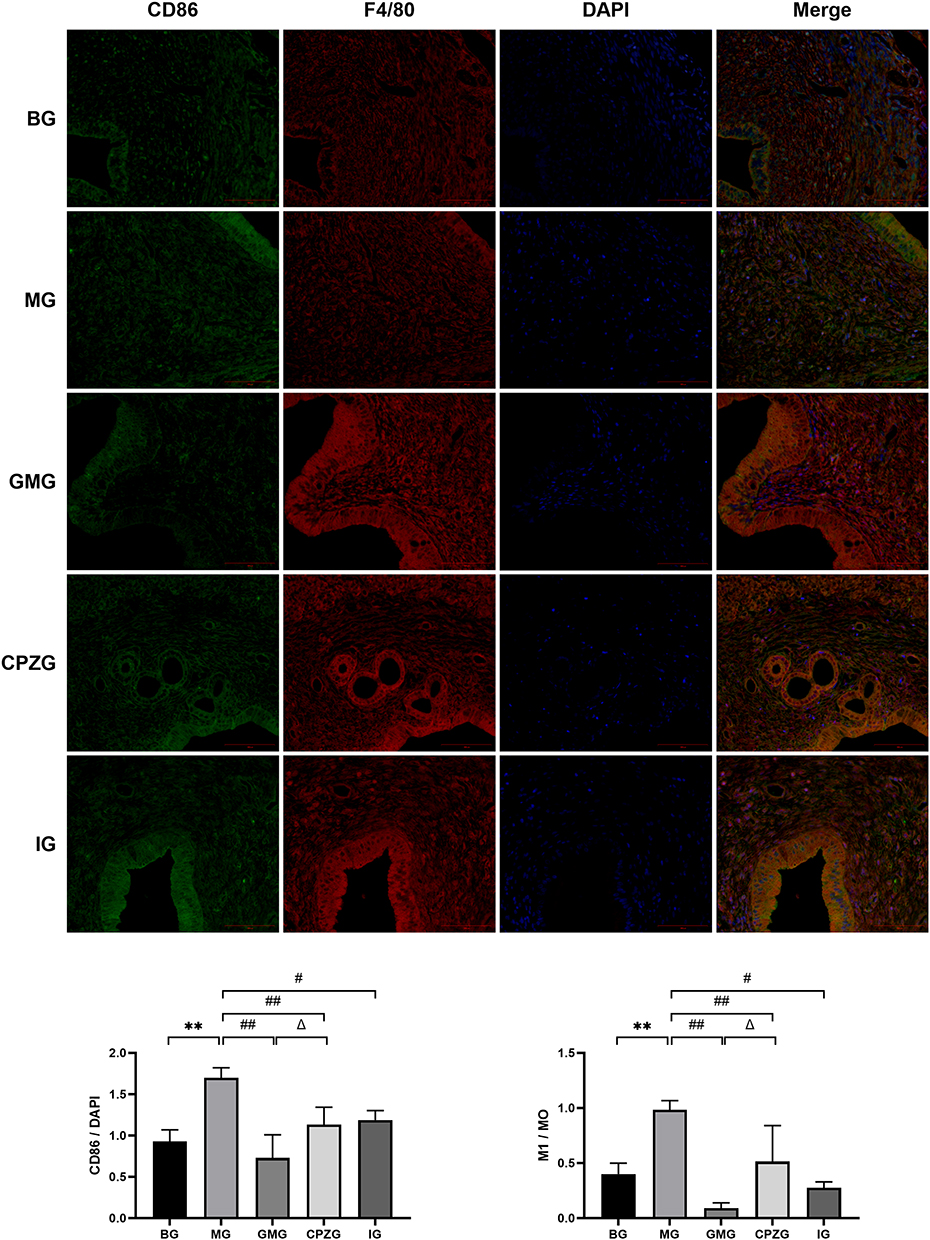 |
Figure 9 Expression of CD86 in rat uterus and M1/M0 ratio across groups (magnification 100×). (**P<0.01 vs BG; #P<0.05, ##P<0.01 vs MG; ΔP<0.05 vs GMG.). |
CD206 is a marker of M2 macrophage polarization. Co-staining of CD206 and F4/80 was used to compare the M2/M0 ratio of macrophages. As shown in Figure 10, compared with BG, the expression of CD206 in the uterus and the M2/M0 ratio in MG decreased (P < 0.01). Compared with MG, the expression of CD206 in the uterus and the M2/M0 ratio in GMG, CPZG, and IG increased (P < 0.05 or P < 0.01). Compared with GMG, the expression of CD206 in the uterus and the M2/M0 ratio in CPZG of rats decreased (P < 0.01).
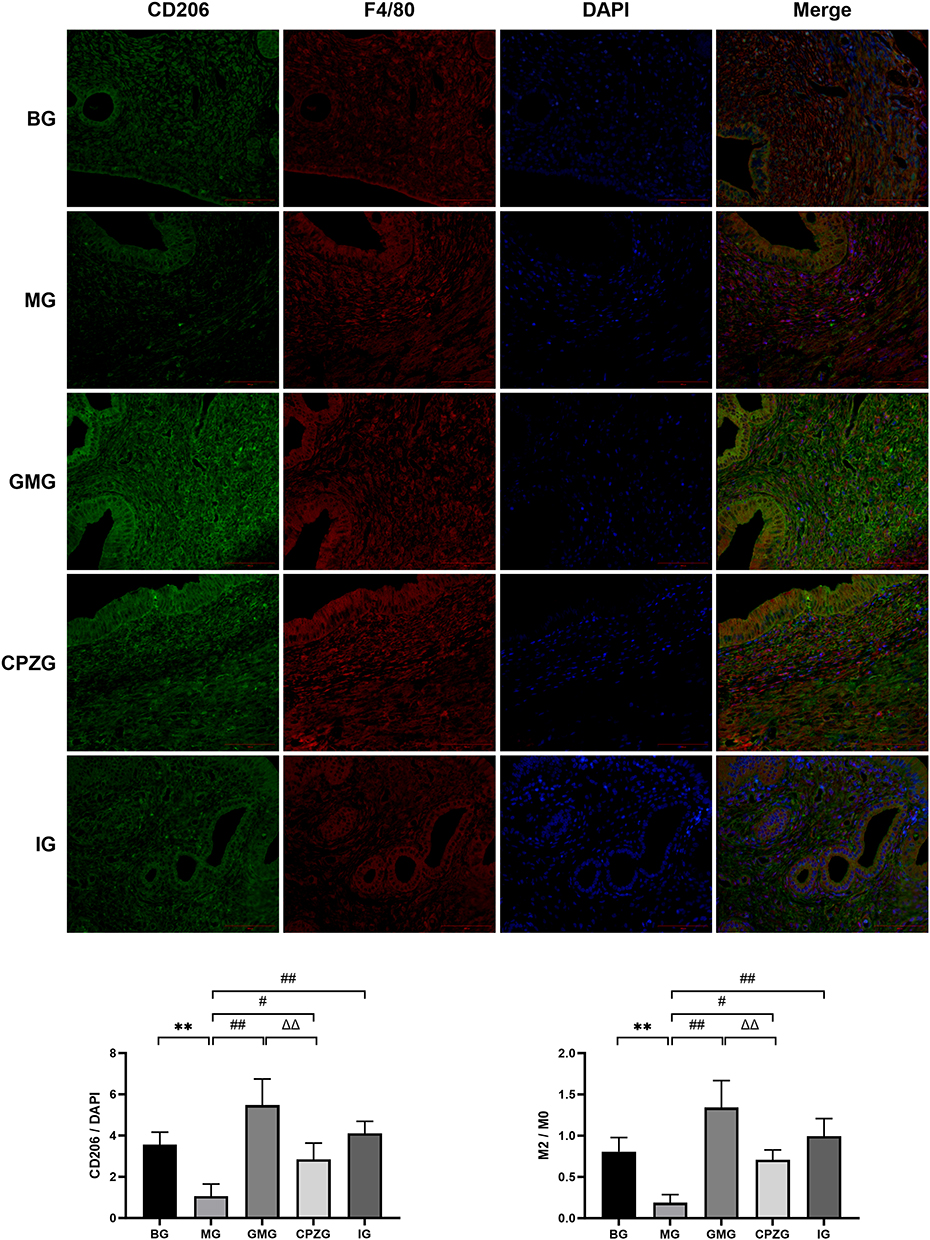 |
Figure 10 Expression of CD206 in rat uterus and M2/M0 ratio across groups (magnification 100×). (**P<0.01 vs BG; #P<0.05, ##P<0.01 vs MG; ΔΔP<0.01 vs GMG.). |
Comparison of Serum Inflammatory Factor Levels in Each Group of Rats
As shown in Figure 11, compared with BG, the levels of TNF-α and IL-6 in the serum of rats in MG increased (P < 0.01), while the levels of IL-4 and IL-10 in the serum decreased (P < 0.01). Compared with MG, the levels of TNF-α and IL-6 in the serum of GMG, CPZG and IG decreased (P < 0.05 or P < 0.01), and the levels of IL-4 and IL-10 in the serum increased (P < 0.05 or P < 0.01). Compared with GMG, the levels of TNF-α and IL-6 in the serum of rats in CPZG (P < 0.05), while the levels of IL-4 and IL-10 in the serum decreased (P < 0.05).
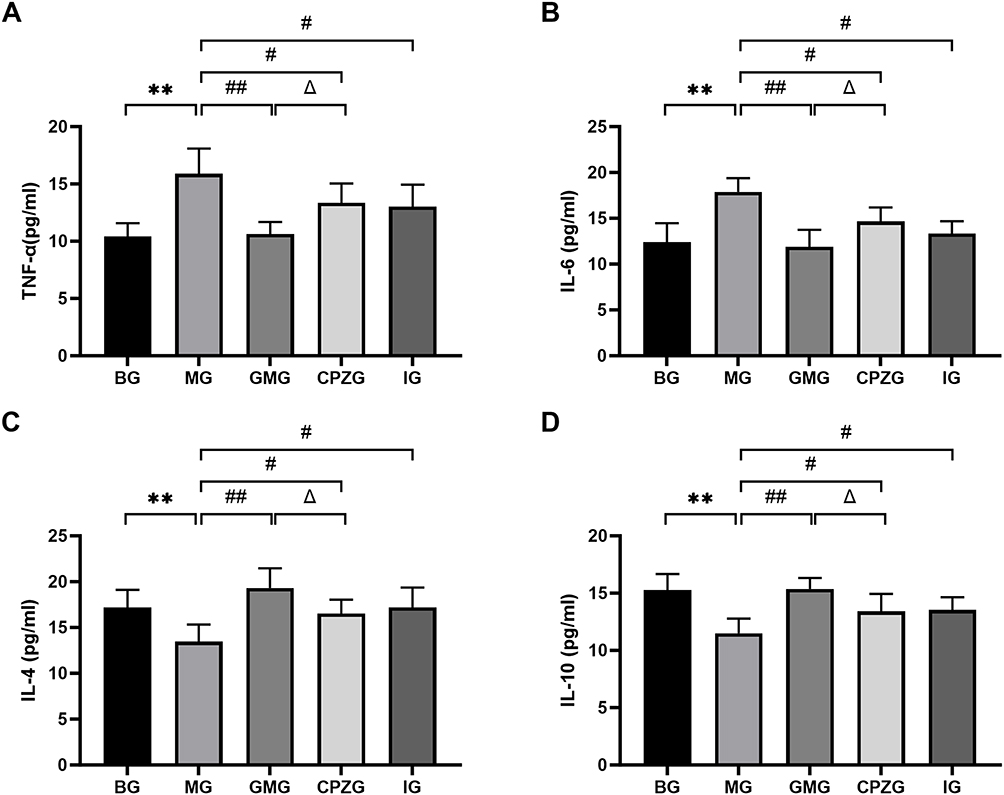 |
Figure 11 The content of serum inflammatory factors in each group of rats. (A) The serum levels of TNF-α. (B) The serum levels of IL-6. (C) The serum levels of IL-4. (D) The serum levels of IL-10. (**P<0.01 vs BG; #P<0.05, ##P<0.01 vs MG; ΔP<0.05 vs GMG.). |
Discussion
Pathological Mechanism of PD and Basis for Ginger Moxibustion Intervention
The pathogenesis of PD is complicated with neurological, endocrine, genetic, immunological, psychological, and lifestyle factors.26–28 Modern research widely recognizes prostaglandins (PGs) as the primary cause of PD, among which PGF2α can trigger abnormal uterine contractions, leading to uterine hypoxia and pain.29 As a first-line treatment for PD, Ibuprofen alleviates uterine pain by inhibiting cyclooxygenase (COX) activity, blocking prostaglandin synthesis, and thereby reducing uterine contractions and ischemic conditions.1
In TCM theory, PD is classified under the category of “menstrual abdominal pain”, with the core pathogenesis being “obstruction leads to pain”, primarily caused by external factors such as cold-dampness evil obstructing qi and blood.30,31 A famous classic of TCM called “Jingyue Quanshu” states: “When cold congeals in the uterus, menstrual flow contains blood clots accompanied by severe abdominal pain”, highlighting the critical role of cold pathogens in PD pathogenesis.32 Modern research has also demonstrated that cold stimulation causes abnormal hemorheology and increased uterine arterial blood flow resistance in PD patients, providing objective support for the “obstruction leads to pain” mechanism induced by cold pathogens.33 As an external therapy of TCM, ginger moxibustion combines the warming effect of moxibustion with the acrid-warm medicinal properties of ginger, thereby enhancing its efficacy in warming meridians, dispelling cold, dredging collaterals, and alleviating pain.34,35 According to the basic theory of meridians and collaterals, both the Conception Vessel (passing through Shenque CV8) and Thoroughfare Vessel (passing through Guanyuan CV4) originate from the uterus. Ginger moxibustion stimulates acupoints along the Conception Vessel, regulating qi and blood flow in both the Conception and Thoroughfare Vessels and achieving the therapeutic principle that “free flow prevents pain”.36
This study replicated a PD model using cold stress combined with estradiol benzoate and oxytocin administration. Results demonstrated a lowered pain threshold and elevated writhing scores in rats. Pathological examination revealed significant inflammatory cell infiltration in uterine tissues alongside increased uterine PGF2α levels. Interventions using ginger moxibustion at the “Shenque” (CV8) and “Guanyuan” (CV4) acupoints, as well as ibuprofen administration, both reversed the aforementioned indicators. This demonstrates that ginger moxibustion yields favorable therapeutic outcomes in treating PD.
TRPV1 Serves as the Key Molecule Mediating the Effects of Ginger Moxibustion
TRPV1 is primarily expressed in subsets of small-diameter unmyelinated (C) and medium-diameter myelinated (Aδ) nociceptors, which can be activated by multiple stimuli such as acidic conditions (pH < 6.0), noxious heat (≥43°C), peptide toxins, and various endogenous or exogenous ligands.13 The expression of TRPV1 in the skin and subcutaneous tissue of acupoints is higher than that in non-acupoint regions, and its expression is further upregulated after acupuncture and moxibustion stimulation.37 It has been verified that moxibustion induces stimulation conduction by activating TRPV1 and HSP expression in acupoint tissues, thereby initiating or activating multiple central endogenous analgesic systems to produce analgesic effects.38 Furthermore, upon TRPV1 activation at acupoints by acupuncture and moxibustion stimulation, it triggers local calcium influx and ATP release, activating sensory afferent fibers (C/Aδ fibers) to exert analgesic and neuroinflammatory regulation effects.39 Besides, there exists dense nerve fibers nearby acupoints which play a role in the transmission of acupuncture signal. For instance, acupuncture and moxibustion can activate TRPV1 channels at acupoints to release neuropeptides such as CGRP and SP, which is involved in the regulation of neural signals aiming at the function of analgesic and anti-inflammatory.40 Not only that, activation of TRPV1 channels can also induce mast cell degranulation, which may be pivotal to the anti-inflammatory and analgesic effects triggered by moxibustion.41
This study further revealed that ginger moxibustion significantly increased the expression of TRPV1 and SP proteins at the “Shenque” (CV8) and “Guanyuan” (CV4) acupoints. However, the TRPV1 antagonist CPZ partially reversed its analgesic and anti-inflammatory effects, manifested by phenomena such as rebound in uterine PGF2α levels and elevation of serum pro-inflammatory factors. These results confirm that the TRPV1 channel serves as a critical mediator in ginger moxibustion for treating PD, with its mediated neural signals regulating downstream effects.
Locus Coeruleus-Spinal Cord NE Pathway Mediates Central Analgesia and Peripheral Anti-Inflammatory Synergy
C/Aδ nerve fibers, as primary signal conduits for TRPV1, play a vital role in nociceptive transmission.42 Their afferent signals ascend through the spinal cord to the periaqueductal gray (PAG), subsequently projecting to the LC.43,44 Activated TRPV1 receptors can induce neuronal excitation in the LC and upregulate c-Fos expression.45 In our previous study, we demonstrated that mild moxibustion at Shenque (CV8) and Guanyuan (CV4) alleviated PD by modulating central sensitization, evidenced by reduced TRPV1, CD11B, and c-Fos expression in the spinal dorsal horn and hypothalamus.17 The LC is a key noradrenergic nucleus within the brainstem.46 Activation of the locus coeruleus-spinal cord noradrenergic pathway may exert analgesic effects by increasing spinal NE levels, and it might be related to the NE-mediated suppression of microglial and astrocyte activation in the spinal cord, consequently reducing pro-inflammatory factor expression while enhancing anti-inflammatory factor expression.47,48 A study oriented in postoperative pain has confirmed that electroacupuncture activates the LC-NE pathway projecting to the spinal cord, releasing NE to enhance inhibitory neurotransmitters within the spinal cord, ultimately producing analgesic effects. However, inhibiting locus coeruleus activity blocked electroacupuncture-induced analgesic effects by optogenetics experiments further demonstrated that.49 Furthermore, NE released by postganglionic sympathetic nerve fibers acts on target organs through a dual-receptor mechanism (β-AR for anti-inflammatory effects, α-AR for pro-inflammatory effects), dynamically regulating immune function.50 Studies have found that NE promotes fatty acid uptake and storage via macrophage β2-AR, inducing M2 polarization (characterized by elevated CD206 and IL-10 levels) and suppressing inflammation.20 Acupuncture and moxibustion exert organ-specific immunomodulation through neural transmission via the synergistic action of the cholinergic anti-inflammatory pathway and the NE pathway.44
This study demonstrated that ginger moxibustion exerted a site-specific modulation of NE levels, which underlay its synergistic analgesic and anti-inflammatory actions. Specifically, ginger moxibustion displayed its effects through a coordinated mechanism that regulated the expression of NE at distinct locations—elevating central NE to promote analgesia while optimizing the peripheral NE environment to foster anti-inflammation—thus illustrating the holistic regulatory advantage of acupuncture and moxibustion therapy.
M2-Type Macrophage Polarization Serves as the Core Mechanism Underlying Ginger Moxibustion’s Improvement of Uterine Inflammation
The severity of uterine inflammation is closely correlated with the occurrence and progression of PD. Inflammation can directly trigger uterine smooth muscle and vascular contraction by releasing prostaglandins, leukotrienes, and cytokines, leading to uterine hypoxia and pain; or by influencing neurotransmitters to further regulate pain perception, thereby forming a feedback loop between inflammation and pain.29,51,52 Moxibustion exerts its anti-inflammatory effects through multidimensional regulation of complex inflammatory networks by modulating molecular components (inflammatory factors, free radicals), cellular activities (immune cell activation), and systemic integration (neuro-endocrine-immune axis), representing a feasible therapeutic approach with significant potential.53–55 Although existing studies have extensively explored the analgesia mechanisms of moxibustion, it remains insufficient in the perspective of anti-inflammatory for PD treatment.56–58
Macrophage polarization plays a critical role in inflammatory responses. M1-type macrophages are typically associated with pro-inflammatory reactions, while M2-type macrophages are involved in anti-inflammatory processes and tissue repair. Therefore, promoting M2-type polarization of macrophages is of significant importance for alleviating inflammatory responses in lesion sites.59 M2-type macrophages primarily secrete anti-inflammatory factors and neuroprotective mediators, which inhibit pain signal transmission by binding to receptors on nociceptive neurons.60 Studies have indicated that anti-inflammatory cytokines (e.g., IL-10) released by M2-type macrophages can counteract the effects of TNF-α on sodium channels in dorsal root ganglia, playing a crucial role in suppressing neuropathic pain.61 Within the peritoneal immune microenvironment, macrophages can also participate in the pathogenesis of uterine pain by secreting Netrin-1, which influences nerve fiber growth and distribution. Furthermore, polarization toward M2 macrophages reduces neuroinflammation and pain by modulating neuro-immune interactions.62,63 β2-AR activation elevates intracellular cAMP/PKA levels, subsequently phosphorylating and activating the nuclear transcription factor PPARγ.20 Activated PPARγ directly binds to the M2-type gene promoter, driving macrophage polarization toward the M2 phenotype. This manifests as increased release of the anti-inflammatory factor IL-10 and enhanced tissue repair capabilities.64
In this study, the endometrium of PD model rats exhibited inflammatory cell infiltration and a surge in serum pro-inflammatory factors (TNF-α, IL-6). While Ibuprofen demonstrated some regulatory effects on inflammatory factors, it showed no significant impact on uterine β2-AR expression or macrophage polarization. Ginger moxibustion reduced local NE levels in the uterus, releasing inhibition of β2-AR internalization while upregulating its expression; Furthermore, the GMG exhibited decreased CD86+ (M1-type) macrophages and increased CD206+ (M2-type) macrophages in the uterus, with a reduced M1/M0 ratio and elevated M2/M0 ratio, confirming it promotes M2-type polarization of macrophages through β2-AR mediation. TRPV1 antagonist CPZ partially reversed these effects, indicating that TRPV1 activation by ginger moxibustion plays a pivotal role in regulating uterine inflammation and mediating analgesia.
This study assessed macrophage polarization using classical surface markers, including CD86 and CD206, as well as the M1/M0 and M2/M0 ratios. Although macrophage activation states are highly plastic and complex, making it difficult for a single marker to fully capture their functional profile, however, the combination of markers used here—together with the reversal effect seen with CPZ treatment—has provided strong support for the hypothesis that ginger moxibustion promoting M2 polarization of uterine macrophages through TRPV1 receptor activation.
Study Limitations and Future Perspectives
This study has several limitations: (1) The model validation metrics lacked indicators such as cold coagulation and blood stasis syndrome scores and hemorheological parameters; (2) The use of CPZ may nonspecifically affect other ion channels like Transient Receptor Potential Ankyrin 1 (TRPA1). Future research should refine experimental designs by employing TRPV1 knockout rat models for further validation; (3) Given the high plasticity of macrophage activation states, future studies could incorporate additional markers (such as M1-associated iNOS, TNF-α and M2-associated Arg1, YM1/2) combined with functional assays to verify dissect phenotypes more precisely. (4) Additionally, the current study has not utilized optogenetics to inhibit or specifically activate the Locus Coeruleus to observe effects on PD. Future studies will employ neural tracing techniques to clarify direct Locus Coeruleus-uterus projections and apply optogenetics to verify their necessity in ginger moxibustion effects.
Conclusion
Ginger moxibustion at “Shenque” (CV8) and “Guanyuan” (CV4) acupoints exerts synergistic analgesic and anti-inflammatory effects via a multi-target mechanism: activating acupoint TRPV1, regulating the locus coeruleus-spinal cord-uterus NE pathway bidirectionally, and inducing uterine macrophage M2 polarization through β2-AR upregulation, providing new insights into how this traditional therapy alleviates PD by integrating neural signaling, neurotransmitter regulation, and immune modulation.
Acknowledgments
This study was supported by the Natural Science Foundation of Hebei Province (Grant No. H2023423004) and the Yan Zhao Medical Research Project of Hebei University of Chinese Medicine (Grant Nos. YZZY2023018 and YZZZ2024005).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kirsch E, Rahman S, Kerolus K, et al. Dysmenorrhea, a narrative review of therapeutic options. J Pain Res. 2024;17:2657–2666. doi:10.2147/jpr.S459584
2. Martire FG, Piccione E, Exacoustos C, Zupi E. Endometriosis and adolescence: the impact of dysmenorrhea. J Clin Med. 2023;12(17). doi:10.3390/jcm12175624
3. Guimarães I, Póvoa AM. Dismenorreia primária: avaliação e tratamento. [Primary Dysmenorrhea: assessment and Treatment]. Rev Bras Ginecol Obstet. 2020;42(8):501–507. doi:10.1055/s-0040-1712131
4. Sen E, Ozdemir O, Ozdemir S, Atalay CR. The relationship between serum ischemia-modified albumin levels and uterine artery doppler parameters in patients with primary dysmenorrhea. Rev Bras Ginecol Obstet. 2020;42(10):630–633. doi:10.1055/s-0040-1715141
5. No BMG. 345: primary dysmenorrhea. J Obstet Gynaecol Can. 2025;47(5):102840. doi:10.1016/j.jogc.2025.102840
6. Gobba S, Kibone W, Kiguba R. Self-reported gastrointestinal adverse effects of non-steroidal anti-inflammatory drugs in female students with dysmenorrhoea at Makerere University: prevalence, discontinuation and associated factors. a cross sectional study. BMJ Open. 2024;14(6):e079660. doi:10.1136/bmjopen-2023-079660
7. Xiao L, Li Z, Junlu C, et al. International standard of traditional Chinese medicine techniques: clinical guidelines for dysmenorrhea (2022). J Tradit Chin Med. 2024;44(6):1277–1287. doi:10.19852/j.cnki.jtcm.2024.06.012
8. Song S, Chen H. Systematic review and meta-analysis of the effectiveness of moxibustion therapy for primary dysmenorrhea. Front Med Lausanne. 2025;12:1545146. doi:10.3389/fmed.2025.1545146
9. Chen SC, Ruan JY, Zhang B, et al. Traditional Chinese medicine interventions based on Meridian theory for pain relief in patients with primary dysmenorrhea: a systematic review and network meta-analysis. Front Med Lausanne. 2024;11:1453609. doi:10.3389/fmed.2024.1453609
10. Duan W, Chen D, Li D, et al. Traditional Chinese medicine treatment strategies for primary dysmenorrhea. Front Endocrinol. 2025;16:1580051. doi:10.3389/fendo.2025.1580051
11. Liu J, Wang Y, Zhang J, et al. Efficacy and safety of non-pharmacological therapies for primary dysmenorrhea: a network meta-analysis. J Pain Res. 2025;18:975–991. doi:10.2147/jpr.S498184
12. Zeng J, Lu Y, Chu H, et al. Research trends and frontier hotspots of TRPV1 based on bibliometric and visualization analyses. Heliyon. 2024;10(2):e24153. doi:10.1016/j.heliyon.2024.e24153
13. Rahman MM, Jo YY, Kim YH, Park CK. Current insights and therapeutic strategies for targeting TRPV1 in neuropathic pain management. Life Sci. 2024;355:122954. doi:10.1016/j.lfs.2024.122954
14. Chen HC, Chen MY, Hsieh CL, Wu SY, Hsu HC, Lin YW. TRPV1 is a responding channel for acupuncture manipulation in mice peripheral and central nerve system. Cell Physiol Biochem. 2018;49(5):1813–1824. doi:10.1159/000493627
15. Meng XY, Gao F, Wang D, et al. Effects of mild moxibustion on proteins expression of BDNF/TrkB signaling pathway in hypothalamus of primary dysmenorrhea rats with cold and dampness stagnation syndrome. Chin J Inf Traditional Chin Med. 2024;31(03):127–131. doi:10.19879/j.cnki.1005-5304.202304679
16. Sun YQ, Liang YL, Wang D, et al. Study on the mechanism of mild moxibustion in treating primary dysmenorrhea rats based on the regulation of TRPV1 expression based on cAMP-PKA signaling pathway. Chin J Inf Traditional Chin Med. 2024;31(10):96–101. doi:10.19879/j.cnki.1005-5304.202403253
17. Sun YQ, Liang YL, Wang D, et al. Effect of moxibustion at Shenque(CV8)and Guanyuan(CV4)on TRPV1 channel in spinal dorsal horn and hypothalamus of dysmenorrhea rats. J Acupuncture Tuina Sci. 2025;23(2):117–125. doi:10.1007/s11726-025-1491-3
18. Freire BM, de Melo FM, Basso AS. Adrenergic signaling regulation of macrophage function: do we understand it yet? Immunother Adv. 2022;2(1):ltac010. doi:10.1093/immadv/ltac010
19. Elenkov IJ, Wilder RL, Chrousos GP, Vizi ES. The sympathetic nerve--an integrative interface between two supersystems: the brain and the immune system. Pharmacol Rev. 2000;52(4):595–638. doi:10.1016/s0031-6997(24)01470-4
20. Petkevicius K, Bidault G, Virtue S, et al. Norepinephrine promotes triglyceride storage in macrophages via beta2-adrenergic receptor activation. FASEB j. 2021;35(2):e21266. doi:10.1096/fj.202001101R
21. Lee G, Kim W. The modulatory effect of acupuncture on the activity of locus coeruleus neuronal cells: a review. Evid Based Complement Alternat Med. 2017;2017:9785345. doi:10.1155/2017/9785345
22. Zou H, Pu W, Zhou J, et al. Noradrenergic locus coeruleus-CA3 activation alleviates neuropathic pain and anxiety- and depression-like behaviors by suppressing microglial neuroinflammation in SNI mice. CNS Neurosci Ther. 2025;31(3):e70360. doi:10.1111/cns.70360
23. Zou HL, Li J, Zhou JL, Yi X, Cao S. Effects of norepinephrine on microglial neuroinflammation and neuropathic pain. Ibrain. 2021;7(4):309–317. doi:10.1002/ibra.12001
24. Tuo L, Tang S, Li S, Gu S, Xie Z. Murine models and research progress on dysmenorrhea. Reprod Sci. 2023;30(8):2362–2372. doi:10.1007/s43032-023-01220-0
25. Shinoda M, Ogino A, Ozaki N, et al. Involvement of TRPV1 in nociceptive behavior in a rat model of cancer pain. J Pain. 2008;9(8):687–699. doi:10.1016/j.jpain.2008.02.007
26. Pakpour AH, Kazemi F, Alimoradi Z, Griffiths MD. Depression, anxiety, stress, and dysmenorrhea: a protocol for a systematic review. Syst Rev. 2020;9(1):65. doi:10.1186/s13643-020-01319-4
27. Drejza M, Rylewicz K, Majcherek E, et al. Dysmenorrhea in Polish adolescent girls: impact on physical, mental, and social well-being-results from POLKA 18 Study. J Clin Med. 2024;13(20). doi:10.3390/jcm13206286
28. Jaleel G, Shaphe MA, Khan AR, et al. Effect of exercises on central and endocrine system for pain modulation in primary dysmenorrhea. J Lifestyle Med. 2022;12(1):15–25. doi:10.15280/jlm.2022.12.1.15
29. Iacovides S, Avidon I, Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. 2015;21(6):762–778. doi:10.1093/humupd/dmv039
30. Tseng TG, Kuan CY, Lo YP, et al. Clinical association of body symptoms and primary dysmenorrhea among young and middle-aged women: an observational study. Front Med Lausanne. 2025;12:1529470. doi:10.3389/fmed.2025.1529470
31. Yu-jie D, Yuan-qi J, Yi L, et al. Research progress on traditional Chinese medicine in treatment of dysmenorrhea. Chin Trad Herbal Drugs. 2022;53(12):3842–3851. doi:10.7501/j.issn.0253-2670.2022.12.031
32. Zhang JB. Jingyue Quanshu. China Press of Chinese Medicine; 1994:961.
33. Wang D, Cheng X, Fang H, et al. Effect of cold stress on ovarian & uterine microcirculation in rats and the role of endothelin system. Reprod Biol Endocrinol. 2020;18(1):29. doi:10.1186/s12958-020-00584-1
34. Wei JZ, Shen XY, Ding GH, Zhao L. Investigation of pathway and mechanism of heat stimulating action of sandwiched moxibustion. Chin Acupuncture Moxibust. 2007;(05):391–393.
35. Tian L, Luo Y, Zou X,F, Wan Q. Research progress of ginger in patients with primary dysmenorrhea. Chin J Ethnomedicine Ethnopharm. 2022;31(11):59–62+66. doi:10.3969/j.issn.1007-8517.2022.11.zgmzmjyyzz202211016
36. Liu W, Jiang HL, Liu CY, et al. Acupoint selection and medication rules of application therapy in treatment of dysmenorrhea: a study based on data mining. World Chin Med. 2023;18(22):3259–3264+3270. doi:10.3969/j.issn.1673-7202.2023.22.018
37. Abraham TS, Chen ML, Ma SX. TRPV1 expression in acupuncture points: response to electroacupuncture stimulation. J Chem Neuroanat. 2011;41(3):129–136. doi:10.1016/j.jchemneu.2011.01.001
38. Li YW, Zhao JM, Chen L, et al. Effect of electroacupuncture and moxibustion on visceral pain and expression of VR 1 and HSP 70 of “Tianshu” (ST 25) region in colorectal distension-induced visceral hypersensitivity rats. Acupuncture Res. 2016;41(4):291–297. doi:10.13702/j.1000-0607.2016.04.002
39. Wu SY, Chen WH, Hsieh CL, Lin YW. Abundant expression and functional participation of TRPV1 at Zusanli acupoint (ST36) in mice: mechanosensitive TRPV1 as an “acupuncture-responding channel”. BMC Complement Altern Med. 2014;14:96. doi:10.1186/1472-6882-14-96
40. Fan Y, Kim DH, Ryu Y, et al. Neuropeptides SP and CGRP underlie the electrical properties of acupoints. Front Neurosci. 2018;12:907. doi:10.3389/fnins.2018.00907
41. Wang LN, Wang XZ, Li YJ, et al. Activation of subcutaneous mast cells in acupuncture points triggers analgesia. Cells. 2022;11(5). doi:10.3390/cells11050809
42. Zhang ZY, Wan HY, Su YS, He W, Jing XH. Characteristics of acupoint effects on inflammation and neuro-immune interaction. Acupuncture Res. 2024;49(09):972–978. doi:10.13702/j.1000-0607.20230506
43. Dubin AE, Patapoutian A. Nociceptors: the sensors of the pain pathway. J Clin Invest. 2010;120(11):3760–3772. doi:10.1172/jci42843
44. Yu WL, Zhang Z, Zamponi GW. Spared nerve injury leads to reduced activity of neurons projecting from the ventrolateral periaqueductal gray to the locus coeruleus. Mol Brain. 2024;17(1):46. doi:10.1186/s13041-024-01121-6
45. Xue BJ, Zhang XX, Shi GM, He RR. Increased expression of c-fos in the brainstem nuclei involved in cardiova scular regulation by capsaicin. Acta Physiologica Sinic. 2000;(02):159–162+182. doi:10.3321/j.issn:0371-0874.2000.02.015
46. España JC, Yasoda-Mohan A, Vanneste S. The locus coeruleus in chronic pain. Int J Mol Sci. 2024;25(16). doi:10.3390/ijms25168636
47. Li J, Wei Y, Zhou J, et al. Activation of locus coeruleus-spinal cord noradrenergic neurons alleviates neuropathic pain in mice via reducing neuroinflammation from astrocytes and microglia in spinal dorsal horn. J Neuroinflammation. 2022;19(1):123. doi:10.1186/s12974-022-02489-9
48. Chen W, Ma X, Fu YM, Liu CZ, Li HP, Shi GX. Electroacupuncture regulates sympathetic nerve through the NTS(Glu)-RVLM circuit to relieve spontaneous pain in SNI rats. CNS Neurosci Ther. 2025;31(3):e70327. doi:10.1111/cns.70327
49. Chu WG, Zhang R, Li HT, et al. Locus coeruleus noradrenergic-spinal projections contribute to electroacupuncture-mediated antinociception in postoperative pain in mice. Adv Sci. 2025:e01182. doi:10.1002/advs.202501182
50. Sohn R, Jenei-Lanzl Z. Role of the sympathetic nervous system in mild chronic inflammatory diseases: focus on osteoarthritis. Neuroimmunomodulation. 2023;30(1):143–166. doi:10.1159/000531798
51. Barcikowska Z, Rajkowska-Labon E, Grzybowska ME, Hansdorfer-Korzon R, Zorena K. Inflammatory markers in dysmenorrhea and therapeutic options. Int J Environ Res Public Health. 2020;17(4). doi:10.3390/ijerph17041191
52. Aksoy AN, Laloglu E, Ozkaya AL, Yilmaz EP. Serum heme oxygenase-1 levels in patients with primary dysmenorrhea. Arch Gynecol Obstet. 2017;295(4):929–934. doi:10.1007/s00404-017-4312-1
53. Li N, Guo Y, Gong Y, et al. The anti-inflammatory actions and mechanisms of acupuncture from acupoint to target organs via neuro-immune regulation. J Inflamm Res. 2021;14:7191–7224. doi:10.2147/jir.S341581
54. Zijlstra FJ, van den Berg-de Lange I, Huygen FJ, Klein J. Anti-inflammatory actions of acupuncture. Mediators Inflamm. 2003;12(2):59–69. doi:10.1080/0962935031000114943
55. Sun R, Wu L, Sun Y. Immunological studies on acupuncture and moxibustion treatment of rheumatoid arthritis: a review. Medicine. 2024;103(2):e36875. doi:10.1097/md.0000000000036875
56. Yu WY, Ma LX, Zhang Z, et al. Acupuncture for primary dysmenorrhea: a potential mechanism from an anti-inflammatory perspective. Evid Based Complement Alternat Med. 2021;2021:1907009. doi:10.1155/2021/1907009
57. Chen B, Guo Q, Zhang Q, Di Z, Zhang Q. Revealing the central mechanism of acupuncture for primary dysmenorrhea based on neuroimaging: a narrative review. Pain Res Manag. 2023;2023:8307249. doi:10.1155/2023/8307249
58. Jin P, Wang F, Zeng F, et al. Revealing the mechanism of central pain hypersensitivity in primary dysmenorrhea: evidence from neuroimaging. Quant Imaging Med Surg. 2024;14(4):3075–3085. doi:10.21037/qims-23-1687
59. Pinho-Ribeiro FA, Verri WA Jr, Chiu IM. Nociceptor sensory neuron-immune interactions in pain and inflammation. Trends Immunol. 2017;38(1):5–19. doi:10.1016/j.it.2016.10.001
60. Zhao W, Ma L, Deng D, et al. M2 macrophage polarization: a potential target in pain relief. Front Immunol. 2023;14:1243149. doi:10.3389/fimmu.2023.1243149
61. Zhu X, Chen S, Xie Y, Cheng Z, Zhu X, Guo Q. Role of M1/M2 macrophages in pain modulation Alectinib treatment for 2 non-small cell lung carcinoma patients carrying different novel ALK fusions. J Central South Univ. 2024;49(7):1155–1163. doi:10.11817/j.issn.1672-7347.2024.240017
62. Ding S, Guo X, Zhu L, et al. Macrophage-derived netrin-1 contributes to endometriosis-associated pain. Ann Transl Med. 2021;9(1):29. doi:10.21037/atm-20-2161
63. Chen S, Liu Y, Zhong Z, Wei C, Liu Y, Zhu X. Peritoneal immune microenvironment of endometriosis: role and therapeutic perspectives. Front Immunol. 2023;14:1134663. doi:10.3389/fimmu.2023.1134663
64. Bouhlel MA, Derudas B, Rigamonti E, et al. PPARgamma activation primes human monocytes into alternative M2 macrophages with anti-inflammatory properties. Cell Metab. 2007;6(2):137–143. doi:10.1016/j.cmet.2007.06.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.