Back to Journals » Integrated Pharmacy Research and Practice » Volume 13
Geographical Disparities in the Distribution of Community Pharmacies Providing Aseptic Preparation Services in Japan
Authors Nonomura K, Toyama K, Kondo Y, Tamaki H ![]() , Osanai A, Ino Y, Nakamura M
, Osanai A, Ino Y, Nakamura M ![]() , Iguchi K
, Iguchi K ![]()
Received 27 May 2024
Accepted for publication 26 September 2024
Published 4 October 2024 Volume 2024:13 Pages 181—190
DOI https://doi.org/10.2147/IPRP.S479164
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Walid Al-Qerem
Kazuya Nonomura,1,2 Kazuya Toyama,1 Yufu Kondo,1 Hirofumi Tamaki,1 Arihiro Osanai,1 Yoko Ino,3 Mitsuhiro Nakamura,4 Kazuhiro Iguchi1
1Laboratory of Community Pharmacy, Gifu Pharmaceutical University, Gifu, Japan; 2Mamiya Dispensing Pharmacy, Gifu, Japan; 3Laboratory of Pharmaceutical Health Care and Promotion, Gifu Pharmaceutical University, Gifu, Japan; 4Laboratory of Drug Informatics, Gifu Pharmaceutical University, Gifu, Japan
Correspondence: Kazuhiro Iguchi, Laboratory of Community Pharmacy, Gifu Pharmaceutical University, 1– 25– 4 Daigaku–nishi, Gifu, 501– 1196, Japan, Tel +81-58-230-8100, Fax +81-58-230-8105, Email [email protected]
Purpose: Providing medical, nursing, and welfare services in each community is becoming increasingly important as population ages in Japan, and the demand for aseptic preparation in community pharmacies is expected to increase. In this study, the disparity in the distribution of community pharmacies providing aseptic preparation services were examined to explore how the unequal distribution of the pharmacies can be improved in the future.
Methods: The regional inequality of community pharmacies providing aseptic preparation services was evaluated using Gini coefficients. The regional distribution was evaluated using a geographic information system application.
Results: Only 8.0% of all insurance community pharmacies in Japan provided aseptic preparation services. The Gini coefficient of pharmacies providing aseptic preparation services for the total population of each municipality was 0.410. The population coverage, within 16 km of pharmacies providing aseptic preparation services, was 96.5% of the total population. The residential grid coverage, within 16 km of the pharmacies, was 75.2% of the total network, approximately one quarter not covered. It is estimated that the coverage ratios will improve by some percentage by 2050, although the projected population in 2050 is expected to decrease by approximately 20%.
Conclusion: The current number and distribution of pharmacies providing aseptic preparation services are inadequate, and measures need to be taken to avoid future problems.
Keywords: community pharmacies, aseptic preparation, Gini coefficient, geographic distribution
Introduction
The older adult population is growing worldwide, posing a problem in providing healthcare services. Japan is facing an unprecedented aging society that no other country has yet experienced. It is estimated that the percentage of the population aged 65 and over will increase from 28.9% in 2021 to 37.7% in 2050.1 The continuous aging of the population will cause a further increase in the demand for medical care and long-term care services.
In countries with aging populations, more integrated services are required to provide quality care, and efforts are underway in many countries to link medical, nursing, and home care.2 In Japan, the “Medical Care Plan” was established in 1985 to create a system for providing essential medical care, taking into consideration the regional environment in the communities, and the “Regional Medical Care Vision” was defined in 2017 within this plan.3 This vision aims to optimize the number of healthcare resources and hospital beds in each region, implying an increase in discharged patients from the hospital and home care services. The demand for home healthcare services in Japan is expected to peak after 2040.4 To meet this growing demand, a structure called the “Community-Based Integrated Care System”5–7 has been established. This is a structure in which all people are provided with comprehensive healthcare, nursing, and welfare services so that they can maintain their lives in their communities regardless of the level of care they need in their homes.
The roles of Japanese pharmacists working in community pharmacies have mainly been health counseling, selling medicine, and dispensing prescriptions. Within the “Community-Based Integrated Care System”, patients may receive Total Parenteral Nutrition, chemotherapy with anticancer drugs, and pain relief with opioids in their homes. Thus, the demand for providing aseptic injections in patients’ homes is increasing. Furthermore, the Medical Care Plan, which began in 2024, calls for community pharmacies to provide aseptic preparation services to patients receiving home healthcare.8
Japanese community pharmacists have been providing infusion solutions, prepared aseptically on a clean bench in community pharmacies, to home care patients. However, according to the 8th NDB Open Data9 provided by the Ministry of Health, Labour and Welfare of Japan, the amount of fees related to aseptic preparations are less than 0.01% of all fees for community pharmacists. It is also estimated that less than 1% of all pharmacies provide aseptic preparation services for injectable opioids.10 The low ratio may reflect the small number of patients requiring aseptic preparations in home settings, but it may also be due to the inability of community pharmacists to adequately respond to the demand.
With the recent increase in the number of patients undergoing outpatient cancer chemotherapy and the establishment of laws to support children in medical care, the need for aseptic preparation services in community pharmacies continues to grow in Japan. A survey examining the present state of aseptic preparation in Tokyo’s pharmacies revealed that the labor-intensive task of aseptic adjustment might be concentrated in a select few pharmacies.11 To address the escalating need for aseptic preparation, community pharmacies in each region need to be equipped to meet the future demand, but the current status of the provision for aseptic preparations is unclear.
To ensure the continuity and quality of regional healthcare services, addressing disparities and shortages in medical resources is an urgent issue. In Japan, where a super-aging society has been realized, the development of a “Community-based Integrated Care System” has been promoted, making the appropriate allocation of medical resources in each region extremely important. The problem of disparities in medical resources has long been raised in several countries. For example, in Japan, the uneven distribution of doctors across regions and shortages in specific medical specialties have been recognized as major issues.12,13 We analyzed the distribution of pharmacists in Japan and found that the imbalance in the ratio based on geographical distribution has not significantly improved despite an improvement in the pharmacist-to-population ratio due to the recent increase in the number of pharmacists.14,15 The analysis of such regional disparities in medical resources often utilizes the Gini coefficient, a measure commonly used to assess income inequality.12–15 Additionally, Geographic Information Systems (GIS) can process various spatial data comprehensively, providing a visually comprehensible representation; this method has been widely used for multifaceted analyses.16,17
In this study, a survey was conducted to assess the distribution of pharmacies providing aseptic preparation services, aiming to determine whether there were a sufficient number of pharmacies providing aseptic preparation services in each region and whether their distribution was appropriate.
Methods
Dataset
We conducted a cross-sectional study to analyze data from the websites described below. In Japan, universal health insurance has been established. All pharmacy services based on prescriptions from physicians are covered under this insurance system, referred to as “insurance dispensing”. To provide insurance dispensing services, pharmacies must be registered as “insurance pharmacies” with the Bureau of Health and Welfare. In this study, an “insurance pharmacy” is defined as a “community pharmacy”. Additionally, in Japan, community pharmacies can offer aseptic preparation services, which involve preparing medications in an aseptic environment using equipment such as clean benches. To receive fees for these aseptic preparation services, pharmacies must register with the Bureau of Health and Welfare. In this study, a pharmacy that is registered to provide aseptic preparation services is defined as a “community pharmacy providing aseptic preparation services”. Information on each pharmacy was obtained from the information bulletins, that is, ‘List of Contents by Code’ and ‘List of Medical Institutions Receiving Notifications’, published by the Bureau of Health and Welfare (eight regional block offices of Hokkaido, Tohoku, Kanto-Shinetsu, Tokai-Hokuriku, Kinki, Chugoku-Shikoku, Shikoku, and Kyushu). Information bulletins for February 2023 were downloaded from the website of the Bureau of Health and Welfare. A total of 61,122 pharmacies were listed as insurance pharmacies in the bulletins. The address information of the pharmacies and the notification status to claim additional fees for aseptic preparations were extracted from the bulletins. Pharmacies providing aseptic preparation services must be insurance pharmacies; therefore, all 61,122 pharmacies were included in this study. Population data were obtained in February 2023 by downloading the ‘2022 Basic Resident Register’ from the e-Stat website (https://www.e-stat.go.jp/) of the National Statistics Center of Japan, a comprehensive portal on government statistics. Depopulated areas were classified based on the ‘List of Depopulated Areas’ available on the website of the Ministry of Internal Affairs and Communications. ‘Deemed depopulated area’ and ‘partially depopulated area’ are classified as depopulated areas.
Insurance pharmacies are only able to notify the Regional Bureau of Health and Welfare to claim the additional fees for aseptic preparation, home healthcare services, and medical insurance fees if they meet the facility criteria. Therefore, the notification status of additional fees for aseptic preparation and home healthcare services were used as an indicator of pharmacies providing aseptic preparation and home healthcare services in this study.
Gini Coefficient
The Gini coefficient was employed as an indicator of the disparity in medical resources between municipalities. Although it is generally used as an indicator of income inequality, it is also widely used to assess disparities in healthcare resources.15,18 The value of the Gini Coefficient varies from 0 to 1. The closer the Gini coefficient is to 0, the more equal; the closer it is to 1, the more unequal.
The Lorenz curve was obtained by arranging the municipalities in order of ascending number of community pharmacies per population, and then plotting the cumulative relative frequency of the population on the horizontal axis and the cumulative relative frequency of community pharmacies on the vertical axis. The Gini coefficient is calculated based on the ratio of the area bounded by the Lorenz curve and equidistribution line to the area under the equidistribution line. When the Lorenz curve (y; the cumulative relative frequency of community pharmacies, 0≤y≤1) is represented by the function y=L(x), where x is the cumulative relative frequency of the population (0≤x≤1), the Gini coefficient is 1–2∫01L(x)dx.
Geographic Information System
To show the two-dimensional distribution of pharmacies that provide aseptic preparation services, QGIS was used as the Geographic Information System (GIS) application. The pharmacy addresses obtained from the Bureau of Health and Welfare were converted to coordinate information (latitude, longitude) using a CSV address-matching service (Center for Spatial Information Science, University of Tokyo) to show in QGIS. Pharmacy addresses with low geocoding-accuracy in the CSV address-matching service were converted to coordinates using Google Maps. An analysis of the resident population living within a certain distance from the pharmacy was conducted using regional grid statistics. The statistics and grid boundary definitions were downloaded from the e-Stat website, the portal site of official statistics of Japan. The grid size used in this study was 1 km square (reference regional grid), and the population of each grid was based on the 2020 Census. The estimated 1 km grid population in 2050 were obtained from future population estimates published by the National Land Numerical Information.19
In this study, the grid in which residents live was defined as “residential grid”. Moreover, the “covered residential grid” was defined as the residential grids contained within or adjacent to a certain distance (5, 10 or 16 km) from the pharmacy. Here, 16 km is the longest distance from a pharmacy that provides home healthcare services to the destination, according to Japanese medical insurance. The total number of residential grids and the covered residential grids were used to calculate the residential grid coverage ratio by community pharmacies.
Residential grid coverage (%) = (number of covered residential grids/total number of residential grids) × 100.
Additionally, the population within the covered grid was used to calculate the population coverage ratio by community pharmacies.
Population coverage (%) = (total population within the covered residential grids/total population within all residential grids) × 100
Ethical Considerations
Ethical approval was not sought for this study because it involves a database-related observational study without directly involving any research participants. All results were obtained from data openly available websites.
Results
The number of insurance community pharmacies in Japan is 61,122, of which only 4,891 provide aseptic preparation services, less than 10% of all community pharmacies (Table 1). Overall, 82.2% of all insurance community pharmacies were located in non-depopulated areas, approximately the same as the proportion of the population in these areas (82.5%). Similar trends were observed in pharmacies providing home healthcare and aseptic preparation services (Table 1).
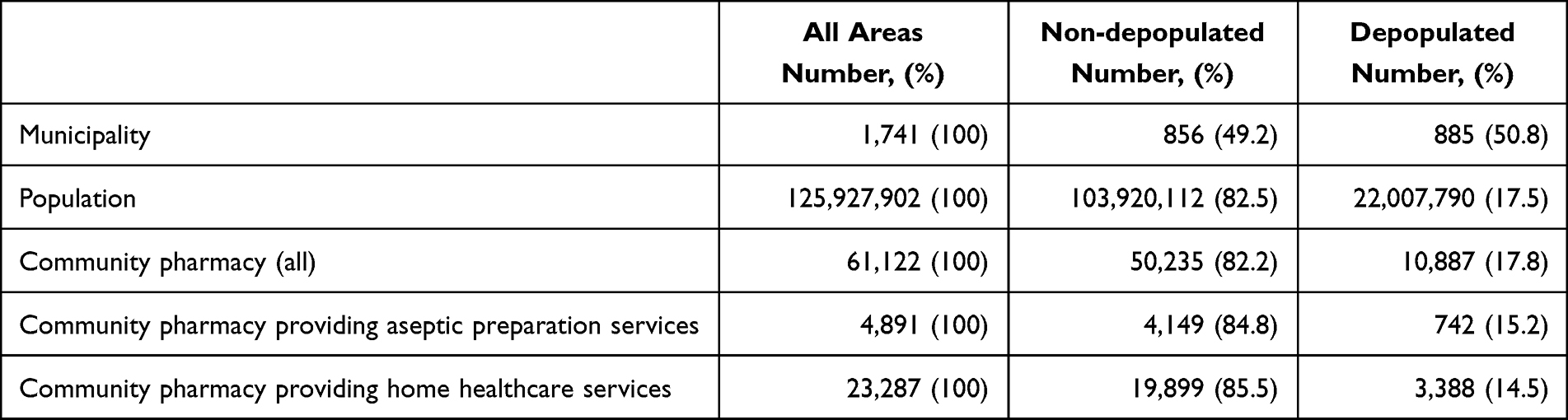 |
Table 1 Summary of Population and Pharmacy Information |
Gini Coefficient
Then, the Gini coefficient, an indicator of unequal distribution, was calculated to evaluate the distribution of pharmacies providing aseptic preparation services. The total number of municipalities was 1,741, of which 856 were non-depopulated and 885 were depopulated (Table 1). The Gini coefficient of the pharmacies providing aseptic preparation services to the total population in each municipality was 0.409. This value was larger than the Gini coefficient of 0.126 for all pharmacies and 0.206 for pharmacies providing home healthcare services (Table 2). The Gini coefficient of pharmacies providing aseptic preparation services to populations in depopulated areas (0.606) was higher than that of populations in non-depopulated areas (0.363).
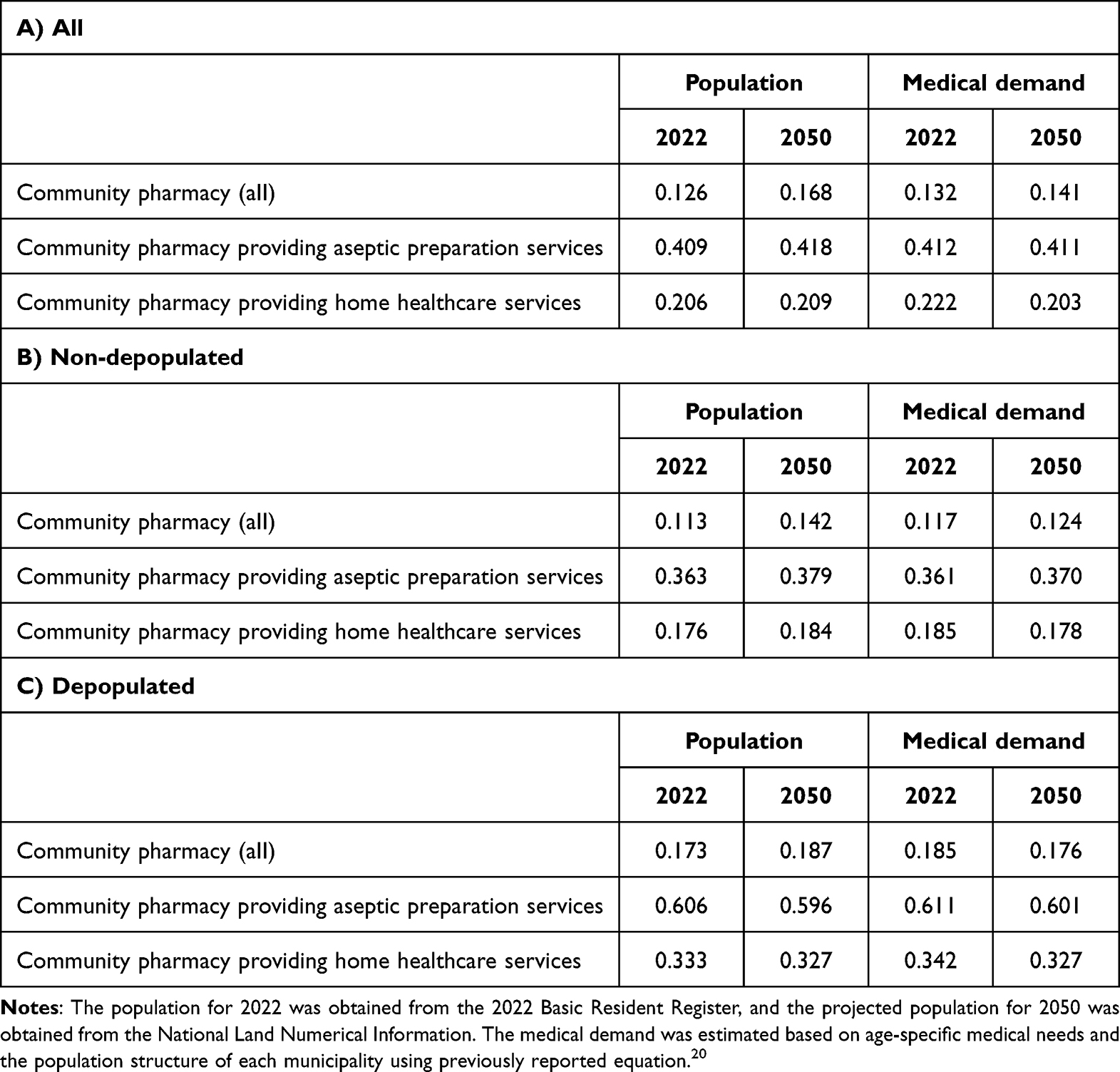 |
Table 2 Gini Coefficient of the Number of Pharmacies and Medical Demand |
The Gini coefficient of pharmacies providing aseptic preparation services relative to the projected population of each municipality in 2050 was 0.418, showing no improvement compared to the Gini coefficient based on the 2022 population (Table 2). Here, the Gini coefficients of pharmacies providing aseptic preparation services relative to the medical demand in each municipality were calculated for both 2022 and 2050. The medical demand was estimated based on age-specific medical needs and the population structure of each municipality, using previously reported equation.20 The resulting Gini coefficients of pharmacies providing aseptic preparation services were 0.418 for the 2050 population, 0.412 for the 2022 medical demand, and 0.411 for the 2050 medical demand (Table 2). This indicates that assuming existing pharmacies remain in operation by 2050, the distribution of these services will not show improvement in its inequality despite shifts in population and medical demand.
Population Coverage and Residential Coverage
To further investigate the distribution of pharmacies providing aseptic preparation services, the proportion of residents was measured based on the distance (5 km, 10 km, and 16 km) from pharmacies providing aseptic preparation services (population coverage). The population coverage within 5 km of pharmacies providing aseptic preparation services was 86.8%, coverage within 10 km was 93.3%, and coverage within 16 km was 96.5% (Table 3A). In addition, the proportion of residential grids within the distance from pharmacies providing aseptic preparation services was measured (residential grid coverage). Consequently, residential grid coverage within 5 km of pharmacies providing aseptic preparation services was 35.9% of the total grid, the coverage within 10 km was 58.0%, and that within 16 km was 75.2% (Table 3B).
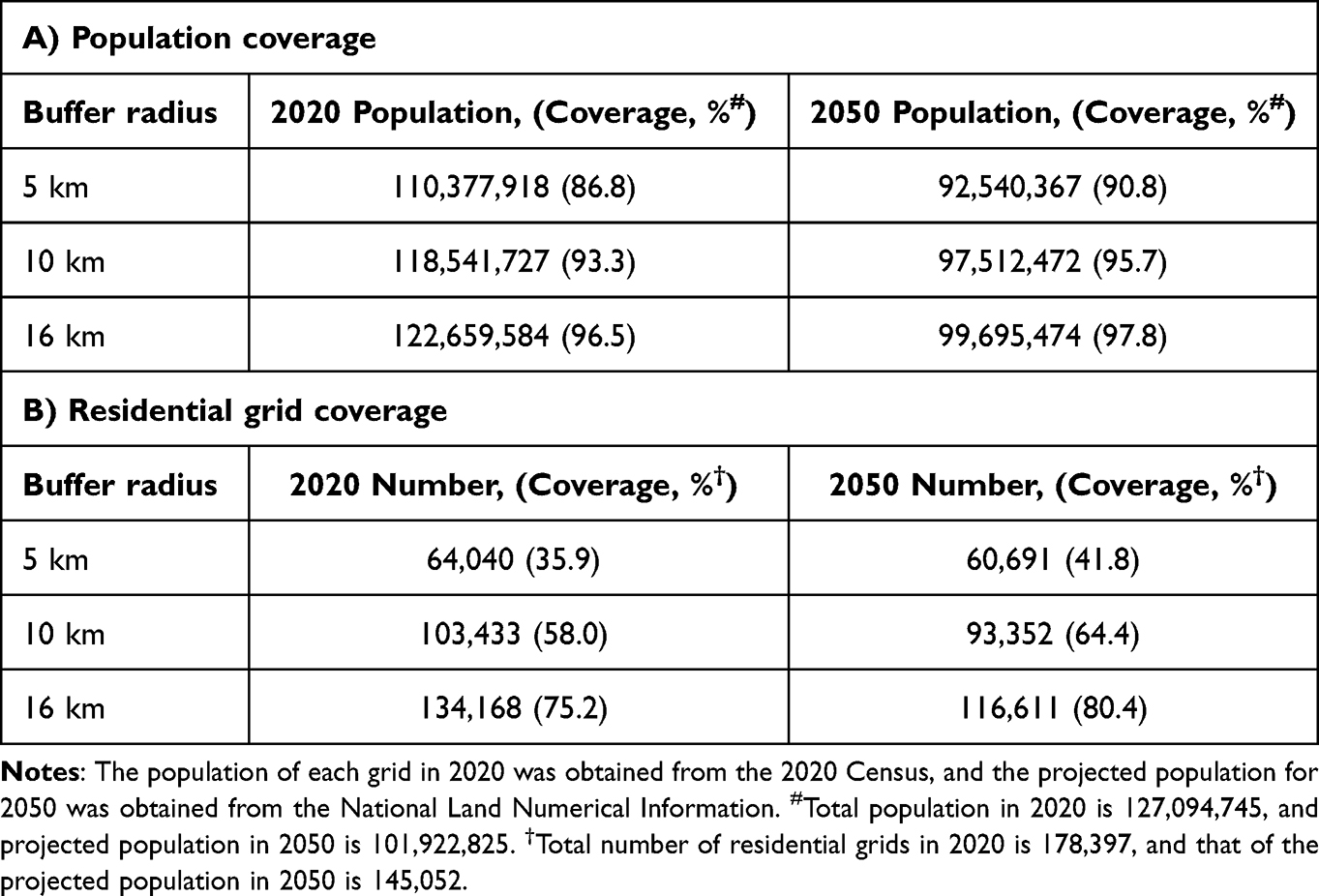 |
Table 3 Population Coverage and Residential Grid Coverage of Community Pharmacies Providing Aseptic Preparation Services Based on the 2020 Census Population and 2050 Projected Future Population |
Estimation of Population Coverage and Residential Coverage in 2050
To predict the unequal distribution in 2050, the coverage ratios were estimated by adapting the projected population of 2050 to the current pharmacy location data. The projected population in 2025 was approximately 20% smaller than the population in 2020 (101,922,825 vs 127,094,745) (Table 3). Assuming that existing pharmacies providing aseptic preparation will remain in the same location in 2050, the population coverage for the projected population in 2050 is estimated to be 90.8% within 5 km of pharmacies providing aseptic preparation services, 95.7% within 10 km, and 97.8% within 16 km (Table 3A). Additionally, the residential grid coverage is estimated at 41.8% within 5 km of pharmacies providing aseptic preparation services, 64.4% within 10 km, and 80.4% within 16 km (Table 3B). Compared with the population decline (approximately 20%), the improvement in the population coverage is estimated at only between 1.3% and 4.0%, and the improvement in the residential grid coverage at approximately 6%.
To better understand the results, the pharmacies providing aseptic preparations, the areas within 16 km of the pharmacies, and residential grids on a map (Figure 1) were plotted. In the residential grid, a low population is shown in blue, a high population is shown in orange, and areas within 16 km are shown in light red. Even when based on projected population in 2050, the blue low-population grids outside the 16 km delineation were distributed in the same way as for the 2020 population (Figure 1).
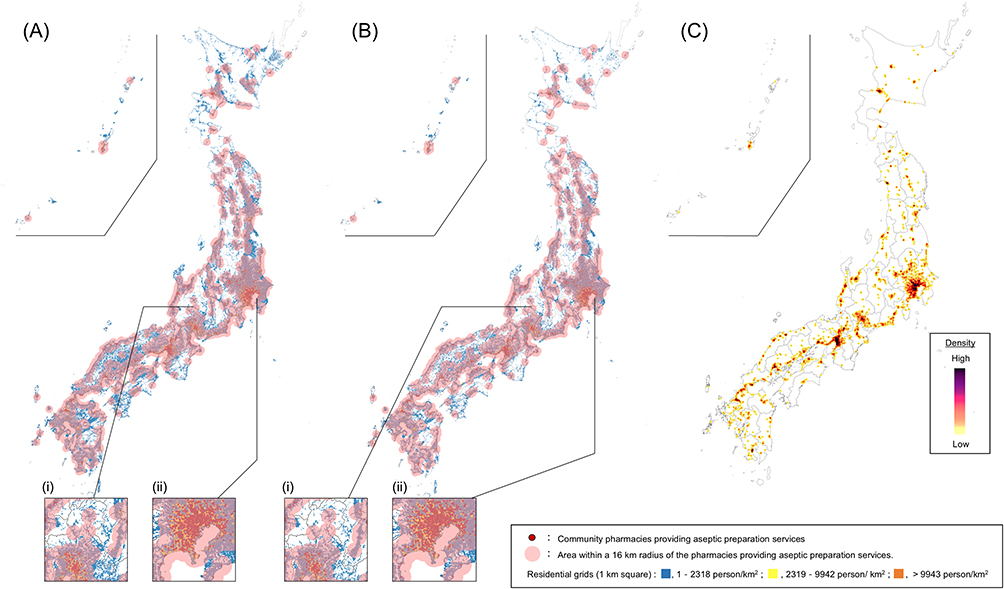 |
Figure 1 Location of community pharmacies providing aseptic preparation services (A, B) Community pharmacies providing aseptic preparation services with population grids of 2020 (A) and projected population of 2050 (B). QGIS was used to plot pharmacies providing aseptic preparation services on a map of Japan based on the address information of pharmacies providing aseptic preparation services and regional grid statistics (1 km grid data), and areas within 16 km of the pharmacies providing aseptic preparation services were indicated in light red. The number of grids within 16 km relative to the total number of grids is defined as “residential grid coverage”, and the population living within 16 km relative to the total population is defined as “population coverage”. The enlarged views show the depopulated area (i) and the non-depopulated area (ii). (C) Heatmap of community pharmacies providing aseptic preparation services. |
Discussion
This study examined whether community pharmacies providing aseptic preparation services in Japan were appropriately located in each region. The following five findings were identified regarding the current status of the distribution of these pharmacies. First, the number of pharmacies providing aseptic preparation services was 4,891, approximately 8% of the total of 61,122 insurance community pharmacies. Second, considering that 15.2% of the number of pharmacies providing aseptic preparation services are located in depopulated areas and 17.5% of the total population is located in such areas, the distribution of pharmacies providing aseptic preparation services between depopulated and non-depopulated areas is almost equal to the population. Third, with regard to the distribution between municipalities, the Gini coefficient of all pharmacies for the municipal population was low (0.126), but that of pharmacies providing aseptic preparation services was high (0.409), suggesting that the distribution of pharmacies providing aseptic preparation services was unbalanced in relation to the municipal population. In particular, the unequal distribution among municipalities classified as depopulated areas was significant, with a Gini coefficient of 0.606. The Gini coefficients calculated based on the estimated population structure and medical demand for 2050 did not show improvement compared to the results from 2022. Fourth, 3.5% of the total population did not live within 16 km of pharmacies providing aseptic preparation services, and this small population was distributed in 24.8% of the residential grids. Fifth, despite a population decrease of approximately 20% by 2050, the maximum increase in residential grid coverage of pharmacies providing aseptic preparation services based on a 10 km radius was only 6.4%. This study revealed that regional and long-term care provision systems for aseptic preparation services are inadequate.
What is required to improve the provision of aseptic preparation services by pharmacies? First, technical training opportunities are thought to be effective in increasing the number of pharmacies capable of aseptic preparation. A lack of knowledge and skills in aseptic preparation has been cited as a reason for the inability to develop a framework for aseptic preparation. In fact, regional pharmacy associations in Japan have organized training for the acquisition of aseptic preparation techniques. It is necessary to continue organizing training sessions in the region. Second, from the perspective of pharmacy managers, it is also necessary to solve the shortage of human resources for aseptic preparation and to improve the profitability of aseptic preparation costs, including the cost of installing clean benches and other equipment.21 With regard to the shortage of human resources, the fact that only pharmacists can perform aseptic preparation in Japan and the slow spread of aseptic preparation techniques may be obstacles to improvement. In countries such as the USA and the UK, aseptic preparation is performed by pharmacy technicians.22,23 Pharmacy technicians need to complete technical training to perform aseptic preparation, and a training system for this has already been established.23–25 If laws and/or regulations on dispensing practices, together with the establishment of education and training systems for aseptic dispensing, allow aseptic dispensing by non-pharmacists, it is expected that human resource barriers will be improved. In terms of costs, profitability is expected to improve owing to the expected increase in demand for aseptic preparation based on the government’s proposed Medical Care Plan and the fact that an increase in fees for aseptic preparation is being considered.8 From the patient’s perspective, the expected cost increases may lead to avoidance of aseptic preparation. Nevertheless, many countries, including Japan, have developed healthcare subsidy systems26,27 and social systems to reduce or exempt patients from costs. In other words, if the system for the provision of aseptic preparation services by pharmacies is improved, a situation in which the patient’s cost burden becomes a barrier to the provision of aseptic preparation services could be avoided.26,27
Does an increase in the number of pharmacies providing aseptic preparation services improve the aseptic preparation provision in a region? We believe that an increase in the number may lead to an improvement in the number of pharmacies per population for the following reasons. Matsumoto et al reported that an increase in the number of advanced medical imaging devices (PET, CT, and MRI) in Japan made their regional distribution more equal.28 We showed that the increase in the number of pharmacies between 2008 and 2018 improved the distribution of pharmacists per population.14 Therefore, an increase in the number of pharmacies providing aseptic preparation services can improve the distribution per population. However, as in a previous study, the distribution per area does not necessarily lead to improvement, even when the distribution per population improved.14 Furthermore, dispensing, which requires special equipment and techniques, such as aseptic preparations, may not need to be implemented in all pharmacies, although a certain level of distribution in the region is required.
The shortage of pharmacies providing aseptic preparation services in rural areas can lead to distortions in regional healthcare. While in some countries, aseptic preparation is performed in specialized facilities, in Japan, it is conducted at community pharmacies equipped with aseptic preparation facilities. When community pharmacies are unable to provide this service, patients may be forced to choose hospitalization over home healthcare; this can negatively impact their quality of life and result in inefficient use of limited medical resources.
In Japan’s healthcare insurance system, an additional fee has been set to evaluate the facility setup of pharmacies providing home healthcare services that have clean benches.29 This economic incentive could potentially lead to an increase in community pharmacies providing aseptic preparation services. Additionally, to promote the development of aseptic preparation services in rural areas, policies providing economic incentives such as increased fees for aseptic preparation services at such pharmacies may be effective. To stabilize operations of community pharmacy in rural areas, the Japanese healthcare insurance system offers preferential treatment in dispensing basic fees in these regions.29 Such economic incentives could accelerate the development of regional aseptic preparation supply system.
Factors contributing to changes in pharmacy distribution include not only the aforementioned economic and policy-related factors but also social factors. Since the outbreak of COVID-19, remote work has become increasingly prevalent in Japanese society, leading to a situation where work location is less constrained. This trend means that individuals who previously had to reside in urban areas due to their jobs can now choose to live in rural areas. The trend towards remote work may continue in the future, potentially accelerating the migration of populations to rural areas. Changes in population distribution driven by societal shifts could, in turn, impact the distribution of pharmacies.30,31
This study has following limitations. First, the linear distance from pharmacies providing aseptic preparation services was used as the distance indicator. If road distances were used instead of linear distances, the coverage might be smaller because road distances are within linear distances and therefore have a smaller coverage area. There are limitations to both distance analyses, as there are many mountainous areas in Japan and the time distance from a pharmacy to a patient’s home differs significantly between depopulated and non-depopulated areas. Second, pharmacies that submitted a notification of additional fees for aseptic preparation were assumed as those providing aseptic preparation services; however, the analysis of this assumption could not be assessed in terms of the actual number of aseptic preparations. Third, it is not possible to determine the demand for aseptic preparations in relation to the population size. Fourth, when calculating coverage ratio, each grid was at a linear distance from the pharmacy, and grids that were partially tangential to a circle centered on the pharmacy were included in the coverage calculation, even if they were not fully included in the area. The population of grids touching the area was included in the coverage calculation even if the actual residence was not located within the area. Therefore, the coverage assessment was based on a grid unit of 1 km square. Finally, the Gini coefficient and coverage ratios for 2050 are based on the assumption that the pharmacies existing in 2022 will continue to operate in 2050. As the population is expected to decrease, the number of pharmacies is also expected to decrease. Therefore, the Gini coefficient calculated for 2050 should be interpreted with caution. In addition, a decrease in the number of pharmacies will result in a smaller coverage area; hence, the coverage rate in 2050 may be overestimated.
Conclusion
In Japan, there are significant disparities in the availability of aseptic preparation services across different regions, with some depopulated areas being particularly underserved due to their distance from pharmacies offering these services. The current distribution of pharmacies providing aseptic preparation services seemed to be insufficient to meet the needs of all residents, especially in rural areas. From the perspective of community-based integrated care systems, it is crucial that pharmacies providing aseptic preparation services are evenly distributed across all regions. Targeted strategic planning and policy interventions are necessary to ensure equitable access to these services in every area. By proactively addressing these disparities, future healthcare inequalities can be prevented and better preparation can be made for the growing demand for aseptic preparation services.
Funding
This research was partially supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI, Grant Numbers 24K13369, 21K06646, and 22K10446.
Disclosure
The authors declare no conflicts of interest regarding this research.
References
1. Ministry of Health, Labour and Welfare. Handbook of health and welfare statistics 2022, Part 1–Population and households, Chapter 1–Population. Available from: https://www.mhlw.go.jp/english/database/db-hh/1-1.html.
2. Allaire JF, Morin P, Doré C, Hyppolite SR, Suzanne Badji M, Zomahou HTV. Integrated community care delivered by public health-care and social-care systems: results from a realist synthesis. Int J Integr Care. 2024;24(1):11. doi:10.5334/ijic.7042
3. Health and Global Policy Institute. Japan health policy NOW, regional medical care delivery system maintenance. Available from: https://japanhpn.org/en/section-4-4/.
4. Iwata H, Matsushima M, Watanabe T, et al. The need for home care physicians in Japan – 2020 to 2060. BMC Health Serv Res. 2020;20(1):752. doi:10.1186/s12913-020-05635-2
5. Health and Global Policy Institute. Japan health policy NOW, Japan’s long-term care insurance system. Available from: https://japanhpn.org/en/section-3-2/.
6. Ministry of Health, Labour and Welfare. Establishing “the community-based integrated care system”. Available from: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/dl/establish_e.pdf.
7. Song P, Tang W. The community-based integrated care system in Japan: health care and nursing care challenges posed by super-aged society. BioSci Trends. 2019;13(3):279–281. doi:10.5582/bst.2019.01173
8. Ministry of Health, Labour and Welfare. Summary of opinions on the review of guidelines for the establishment of a system for in-home medical care (article in Japanese). Available from: https://www.mhlw.go.jp/content/10800000/001015858.pdf.
9. Ministry of Health, Labour and Welfare. 8th NDB open data Japan. Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000177221_00012.html.
10. Doi M, Hisahara K, Otomo S, Igarashi M, Ariumi H, Yoshiyama Y. Establishment of an opioid injection supply system to address demands during non-standard working hours. Part I: operational challenges. (article in Japanese). J Jpn Assoc Home Care Med. 2019;1:15–21. doi:10.34458/jahcm.1.1_15
11. Kushida K, Hirohara M. Advanced pharmaceutical management functions in home pharmaceutical care. (article in Japanese). Yakugaku Zasshi. 2020;140:877–884. doi:10.1248/yakushi.19-00237-5
12. Matsumoto K, Seto K, Hayata E, et al. The geographical maldistribution of obstetricians and gynecologists in Japan. PLoS One. 2021;16(1):e0245385. doi:10.1371/journal.pone.0245385
13. Matsumoto M, Kimura K, Inoue K, Kashima S, Koike S, Tazuma S. Aging of hospital physicians in rural Japan: a longitudinal study based on national census data. PLoS One. 2018;13(6):e0198317. doi:10.1371/journal.pone.0198317
14. Iguchi K, Ueyama M, Nishio H, et al. Impact of the increase in the number of community pharmacists on their geographical distribution in Japan: a retrospective survey. J Pharm Policy Pract. 2022;15(1):96. doi:10.1186/s40545-022-00499-9
15. Yajima S, Shimauchi A, Sakai C, et al. Survey of the distribution of community pharmacists using government statistics. (article in Japanese). Yakugaku Zasshi. 2018;138(7):991–1000. doi:10.1248/yakushi.17-00230
16. Berenbrok LA, Tang S, Gabriel N, et al. Access to community pharmacies: a nationwide geographic information systems cross-sectional analysis. J Am Pharm Assoc. 2022;62(6):1816–1822. doi:10.1016/j.japh.2022.07.003
17. Tew MM, Hatah E, Arif F, Abdul Wahid MA, Makmor-Bakry M, Abdul Maulad KN. Geospatial analysis of distribution of community pharmacies and other health care facilities providing minor ailments services in Malaysia. J Pharm Policy Pract. 2021;14(1):24. doi:10.1186/s40545-021-00308-9
18. Castillo-Salgado C, Schneider C, Loyola E, Mujica O, Roca A, Yerg T. Measuring health inequalities: Gini coefficient and concentration index. Epidemiol Bull. 2001;22(1):3–4.
19. National Land Information Division. Ministry of land, infrastructure, transport and tourism. 1km mesh future estimated population data. Available from: https://nlftp.mlit.go.jp/ksj/gml/datalist/KsjTmplt-mesh1000h30.html.
20. Japan Medical Association Research Institute. Working paper No. 323, current and future health care delivery systems in the region. (article in Japanese). Available from: https://www.jmari.med.or.jp/download/wp323_data/intro.pdf.
21. Kimura M. Consideration of advanced pharmaceutical control functions through pharmacy-provided home pharmaceutical care. (article in Japanese). Yakugaku Zasshi. 2020;140(7):841–850. doi:10.1248/yakushi.19-00237-1
22. Appendix A: ASHP guidelines on compounding sterile preparations. Buchanan EC, Schneider PJ, Forrey RAeditors. In: Compounding Sterile Preparations.
23. General Pharmaceutical Council. Pharmacy technician education and training. Available from: https://www.pharmacyregulation.org/education/pharmacy-technician.
24. Pharmacy Technician Certification Board. Certified compounded sterile preparation technician. Available from: https://www.ptcb.org/credentials/certified-compounded-sterile-preparation-technician.
25. Zellmer WA, McAllister EB, Silvester JA, Vlasses PH. Toward uniform standards for pharmacy technicians: summary of the 2017 pharmacy technician stakeholder consensus conference. Am J Health Syst Pharm. 2017;74(17):1321–1332. doi:10.2146/ajhp170283
26. Okubo S. Comparison of out-of-pocket payment systems in Japan, Germany, France, and the United Kingdom. (article in Japanese). J Health Care Soc. 2021;31(1):45–59. doi:10.4091/iken.31-45
27. Ministry of Health, Labour and Welfare. Overview of medical service regime in Japan. Available from: https://www.mhlw.go.jp/bunya/iryouhoken/iryouhoken01/dl/01_eng.pdf.
28. Matsumoto M, Koike S, Kashima S, Awai K. Geographic distribution of CT, MRI and PET devices in Japan: a longitudinal analysis based on national census data. PLoS One. 2015;10(5):e0126036. doi:10.1371/journal.pone.0126036
29. Ministry of Health, Labour and Welfare. Overview of the revision of dispensing fees 2024. (article in Japanese). Available from: https://www.mhlw.go.jp/content/12400000/001238903.pdf.
30. Cabinet Office. A new influx of individuals into rural areas is occurring as a result of the growth in telework and other related phenomena. (article in Japanese). Available from: https://www5.cao.go.jp/j-j/cr/cr20-21/chr20-21_01-03.html.
31. Biagetti M, Croce G, Mariotti I, Rossi F, Scicchitano S. The call of nature. Three post-pandemic scenarios about remote working in Milan. Futures. 2024;157:103337. doi:10.1016/j.futures.2024.103337
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.