Back to Journals » The Application of Clinical Genetics » Volume 14
Genetic Testing for Aneuploidy in Patients Who Have Had Multiple Miscarriages: A Review of Current Literature
Received 20 May 2021
Accepted for publication 22 June 2021
Published 23 July 2021 Volume 2021:14 Pages 321—329
DOI https://doi.org/10.2147/TACG.S320778
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Ralph S Papas,1 William H Kutteh2,3
1Department of Obstetrics and Gynecology, Saint George Hospital - University Medical Center, Beirut, Lebanon; 2Department of Obstetrics and Gynecology, Baptist Memorial Hospital, Memphis, TN, USA; 3Recurrent Pregnancy Loss Center, Fertility Associates of Memphis, Memphis, TN, USA
Correspondence: William H Kutteh
Recurrent Pregnancy Loss Center, Fertility Associates of Memphis, 80 Humphreys Center, Suite 307, Memphis, TN, 38139, USA
Tel +1 901-747-2229
Fax +1 901-747-4446
Email [email protected]
Abstract: Recurrent pregnancy loss (RPL) is an obstetrical complication that affects about 3% of reproductive age couples. Genetic and non-genetic causes of RPL are multiple; however, aneuploidy is the most common obstetrical complication that can explain single and recurrent pregnancy loss (present in about 60% of recognized clinical pregnancies which result in a miscarriage). Parental karyotyping will only be of potential benefit for 2 to 5 percentage of RPL couples who are translocation carriers. Products of conception (POC) karyotype analysis has been used to direct management in RPL and has been shown to be cost-effective, but the technique has many limitations including high culture failure rate and maternal cell contamination. These limitations can be significantly reduced using POC chromosomal microarray (CMA) technology. We believe that POC genetic testing should be performed after the second and subsequent pregnancy loss using CMA. Although the results will not generally alter the course of treatment, the knowledge of the reason for the loss is of great emotional comfort to many patients. In addition, POC CMA performed in conjunction with a regular complete maternal RPL work-up will identify the group of truly unexplained RPL. Thus, only 10% of patients with RPL will complete an evaluation having a euploid loss and an otherwise normal work-up. This group of “truly unexplained RPL” would be ideal for new research trials and therapies. Pre-implantation genetic testing (PGT) technology has improved recently with day 5 trophectoderm biopsy as compared to biopsy on day 3 as well as with the addition of CMA and next-generation sequencing technologies. The most recent studies on PGT-SR (PGT-Structural rearrangement) show improved clinical and live birth rates per pregnancy, as well as decreased miscarriage rate for translocation carriers. PGT-A (PGT-aneuploidy) may have a limited role in RPL in cases with documented recurrent POC aneuploidy.
Keywords: karyotype, products of conception, chromosomal microarray analysis, aneuploidy, pre-implantation genetic testing, recurrent pregnancy loss
Introduction
Defined by the American Society of Reproductive Medicine (ASRM) and the European Society of Human Reproduction and Embryology (ESHRE), as at least two episodes of miscarriage before 20 to 24 weeks of gestation, Recurrent Pregnancy Loss (RPL) is an obstetrical complication that affects about 3% of reproductive age couples.1–3 A complete 2012 RPL ASRM work-up includes screening for anatomic uterine factors, anti-phospholipid syndrome, endocrine disorders as well as parental karyotyping.1 On the other hand, the latest guidelines published in 2017 by the European Society of Human Reproduction and Embryology (ESHRE), propose omitting parental karyotyping from the routine screening for RPL, except after “individual risk assessment” including a prior child with congenital abnormalities, offspring with unbalanced chromosomes or a translocation identified in Products of Conception (POC).2
Thrombophilia testing for Factor V Leiden, Prothrombin (Factor II), Methylene tetra hydrofolate reductase, and deficiencies of protein S, C, and Antithrombin are not recommended as standard testing for patients with RPL by ASRM and ESHRE.1,2 Only patients with a personal history or strong family history of thrombophilia should be tested.1,2
Genetic testing on products of conception (POC) in RPL cases, has been extensively investigated by many groups over the past twenty years. The ASRM advises against the routine use of POC karyotype analysis, only to be considered in the setting of “ongoing therapy” for RPL, “if the evaluation identifies a remediable cause” to determine whether the event was “random or a treatment failure”.1 The ESHRE published a “strong recommendation” for the use of array-Comparative Genomic Hybridization as a technique for POC genetic analysis, but to be used conditionally for ‘explanatory purposes’ only.2
Unexplained RPL is a diagnosis that represents more than 50% of cases using the recommendations by the ASRM and the ESHRE discussed above, making it frequently elusive to physicians in addition to being psychologically distressing to patients.4,5 Recently, genetic testing using chromosomal microarray (CMA) has raised our awareness about the role of aneuploidy in RPL affecting about 55% of cases. We also identified a role for CMA testing on POC after the second or subsequent miscarriage in directing management. In addition, this strategy will identify a group of patients representing about 10% of cases with “unexplained RPL” based on a negative ASRM work-up and one identified euploid loss by CMA. We believe this group of truly unexplained RPL patients would be ideal candidates for new research trials and therapies.6–8
This review will begin with a brief outline of known genetic causes of RPL and the role of aneuploidy, followed by an overview of the different currently used genetic testing applications in RPL. Techniques discussed will include parental karyotyping, karyotype of POC and CMA of POC. The current role of Pre-implantation genetic testing in RPL will also be outlined. Future directions including maternal cell-free (cf) DNA technology will also be discussed.
Genetic Causes of Recurrent Miscarriage
Human reproduction is an extremely inefficient process. Approximately 70% of human conceptions never achieve viability, and 50% spontaneously fade before being noticed.9,10 Spontaneous miscarriage is the most common complication of pregnancy and aneuploidy is the most common cause of miscarriage.
Sixty percent of recognized clinical pregnancies which result in a miscarriage have a chromosomal anomaly that can explain the loss.11,12 In spite of this high rate of aneuploidy, it is important to realize that genetic factors alone cannot be the only causative factor for miscarriages in many RPL cases.
Figure 1 describes our published experience using 24-chromosome microarray on 26,107 miscarriage tissues and illustrates the importance of aneuploidy in miscarriage.12
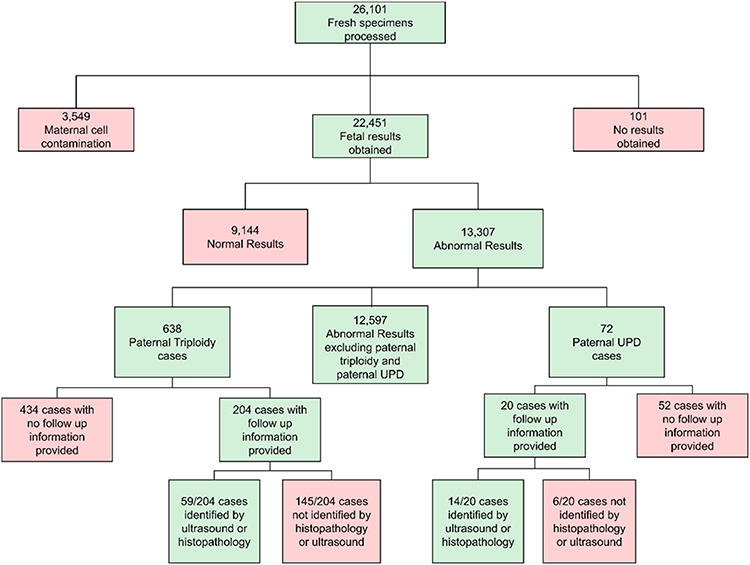 |
Figure 1 Results of 24- chromosome microarray on 26,107 miscarriage tissues.Note: Reproduced from: Maisenbacher MK, Merrion K, Kutteh WH. Single-nucleotide polymorphism microarray detects molar pregnancies in 3% of miscarriages. Fertil Steril. 2019;112(4):700–706.12 Copyright ©2019 The Authors. Published by Elsevier Inc. on behalf of the American Society for Reproductive Medicine. CC BY-NC-ND license (https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode). |
Table 1 describes ten years of laboratory experience using chromosomal microarray; It illustrates the rates of abnormal results including aneuploidy, obtained from a total of 63,277 miscarriage tissues. Uniparental diploidy is a rare finding. Autosomal trisomies due to meiotic nondisjunction during gametogenesis, are the most common aneuploidies occurring in 60% of abnormal cases. Trisomy 16 is the most common early miscarriage trisomy (20% to 30% of cases). Trisomy 21, 18, and 13, account for most trisomies in late miscarriage. Monosomy X is the most common single abnormality, accounting for 20% of cases, and polyploidies occur in another 20%.13
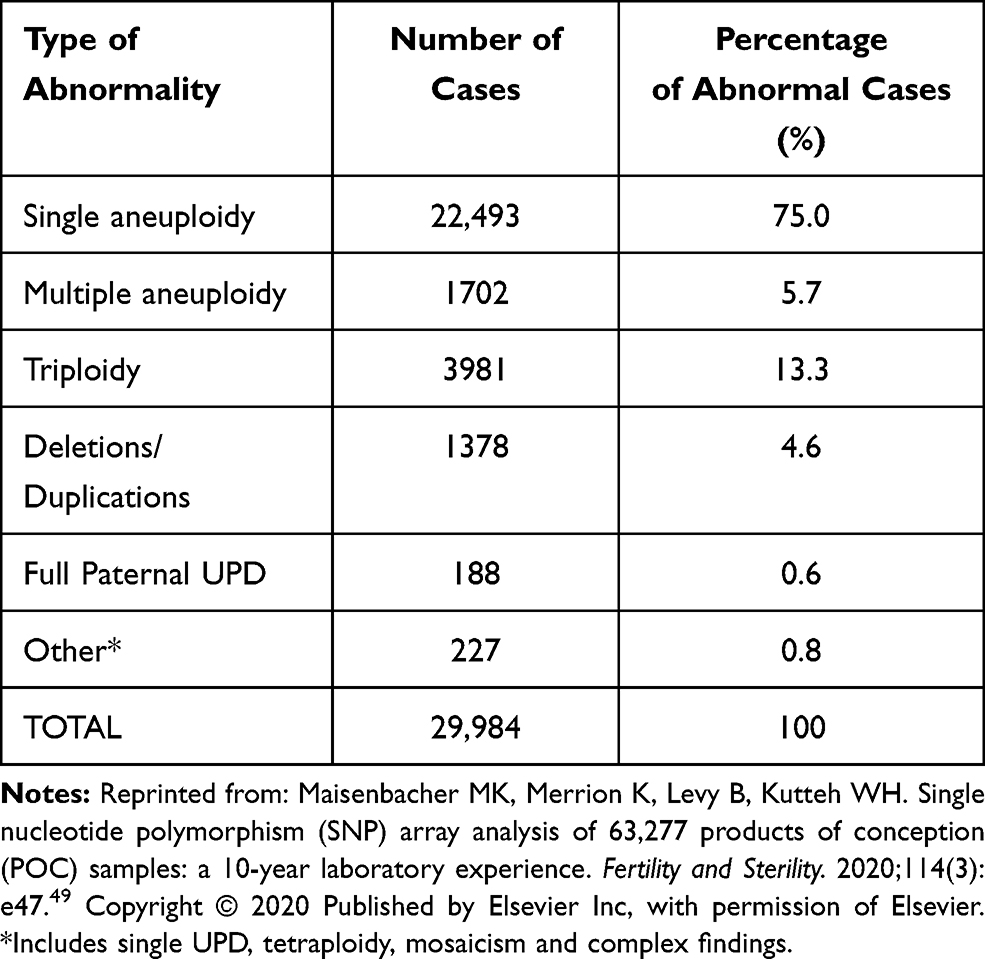 |
Table 1 Rates of Abnormal Results |
A balanced reciprocal or a Robertsonian translocation occurs in about 2–5% of RPL couples (chromosomal inversion, sex chromosome aneuploidy, and supernumerary chromosome accounting for smaller percentages). When identified, these chromosomal abnormalities could represent major contributing factors for RPL as well as significant prognostic information for subsequent pregnancies.1,13,14 In couples with RPL who have a parental genetic abnormality, a balanced translocation is the genetic abnormality in 85% of cases. Less commonly known genetic causes associated with RPL, requiring further clinical research, include copy number changes, confined placental mosaicism, skewed X chromosome inactivation, as well as single-gene disorders.13
Types of Genetic Testing
The different types of genetic testing used in the setting of RPL will be discussed in this section. The advantages and disadvantages of each testing modality are summarized in Table 2.
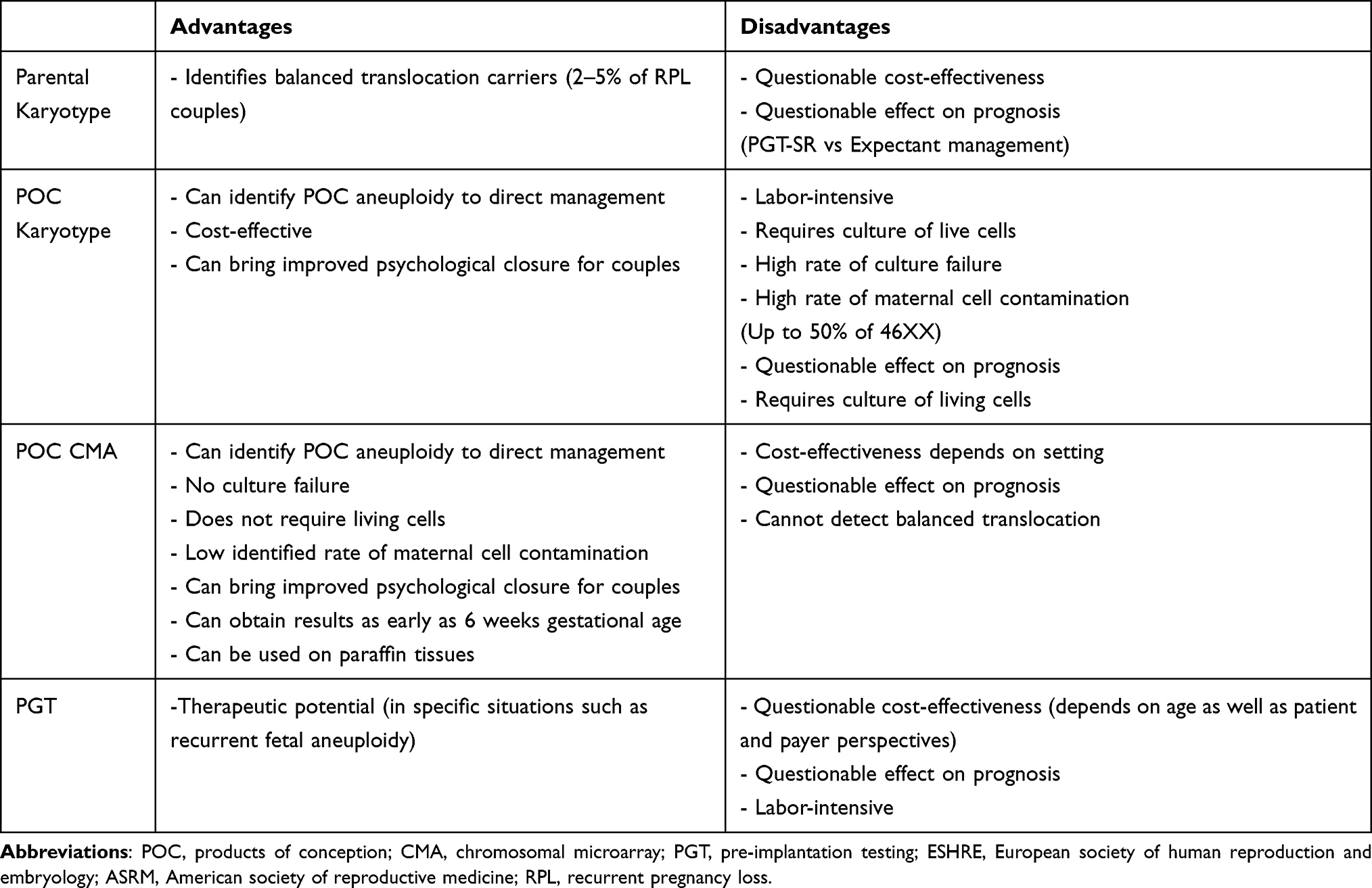 |
Table 2 Summary Pros and Cons of the Different Genetic Tests for Aneuploidy Currently Recommended in RPL |
Parental Karyotyping
The rate of balanced parental chromosomal rearrangement in RPL is 5 to 10 folds more common in RPL compared to the general population, and parental karyotype analysis remains currently widely used. The ESHRE guidelines state that RPL couples should be informed that when a parental karyotype abnormality is found, the “cumulative live birth rates are good, as are the chances of a healthy child, despite a higher risk of subsequent pregnancy loss.”2 Recent studies have shown that routine parental karyotyping for all RPL couples is not cost-effective.15–17 Ultimately, parental karyotyping will be of only potential benefit for a very low percentage of RPL couples given the fact that even when a parental chromosomal abnormality is identified the chances of the couple having a healthy child by natural conception will remain potentially unchanged. This was validated by two prospective studies and the two most recent systematic reviews on the topic that found no overall difference in live birth rate when Preimplantation Genetic Testing (PGT) was used compared to natural conception in those cases.17,18 The latest studies on PGT for carriers of translocations might show differently and will be discussed further below.
POC Karyotyping
The use of karyotype analysis of RPL POC using G-banding technique has been studied by many groups. Around the time of publication of the ASRM guidelines, we and others have proposed a new clinical algorithm for the evaluation and management of RPL based on the results of POC karyotype19 or POC CMA.20 Following this original algorithm, if the cytogenetic analysis reveals aneuploid POC, no further evaluation or treatment is recommended as a genetic cause for the pregnancy loss has been identified. If an unbalanced chromosomal translocation or inversion is identified, then parental karyotyping to identify a balanced parental translocation should be performed in addition to genetic counseling. Finally, if the miscarriage tissue is found to be euploid and maternal cell contamination has been ruled out, a full 2012 ASRM RPL work-up was recommended.
Such decision-making was found to be cost-effective by two groups,19,21 however POC karyotyping has important limitations especially regarding the facts, it can be labor-intensive, needs live cells and culture failure is significantly high (about 30%) and it carries a high rate of maternal cell contamination. This led many groups to the use of more advanced technology discussed below.
POC CMA
ESHRE recognized that the “genetic analysis of pregnancy tissue has the benefit of providing the patient with a reason for the pregnancy loss and may help to determine whether further investigations or treatments are required”.2
As stated earlier, “analysis by traditional G-banding karyotyping is limited by the failure of tissue culture and the fact that it does not distinguish between maternal contamination and a normal (euploid) female fetus”.2
Sahoo et al performed 8118 consecutive CMA POC analysis on cases of spontaneous abortions and RPL. SNP-based CMA was found to be a “robust platform”, with successful results obtained in >90% of cases. The authors state that “SNP-based CMA can identify aneuploidy, polyploidy, whole-genome homozygosity, segmental genomic imbalances, and maternal cell contamination, thus maximizing sensitivity and decreasing false-negative results. Understanding the etiology of fetal loss enables clarification of recurrence risk and assists in determining appropriate management for future family planning”.22
ESHRE recommends microarray as the preferred modality for POC genetic testing.2 Up to 50% of “46, XX normal” reports by traditional karyotyping of POC result from maternal cell contamination.12,23–25 The recent report by Maisenbacher et al, on CMA results of 26,101 miscarriages, found a successful read in over 86% of cases, identified a chromosomal anomaly that could explain a pregnancy loss in 59% of cases, and reported 13% of all results were secondary to maternal cell contamination.12 By comparison, in another study, conventional cytogenetic was performed on 5457 consecutive POC miscarriage samples and showed only 75% culture successes.24
In addition to allowing far better resolution (10–100 kb) than the 10 Mb that is achievable using conventional G-banding karyotype analysis, CMA offers another advantage. Indeed, CMA does not require successful cell culture and cells to be in metaphase for analysis. Therefore, it can be performed on non-viable tissue such as on Paraffin-fixed samples.
Limitations of CMA include its inability to detect balanced translocations.24–26 However, a balanced translocation in the embryo typically does not lead to miscarriage. Another limitation of CMA lies in its inability to detect low-level mosaicism.24–26
A complete assessment comprising the evaluation for parental chromosomal abnormalities, uterine anomalies, endocrine imbalances, autoimmune factors as well as CMA analysis of miscarriage tissue was performed by Popescu et al, on a cohort of 100 prospectively recruited RPL cases. Results confirmed that in 95% of RPL cases, at least one potential cause for the miscarriage could be identified when CMA analysis of POC was added to the standard ASRM RPL work-up at the time of the second or subsequent loss. Moreover, this algorithm was found to be significantly more cost-effective, producing savings of over 50% for the health system based on US numbers.6
The results of this prospective cohort study suggest that an RPL evaluation after the second miscarriage should include systematic CMA analysis of POC. The addition of CMA testing of POC should be considered as a more effective and cost-efficient for the great majority of RPL couples compared to traditional POC karyotyping (at least in the US).6,7
More recently, in 2020, our group has published a new clinical algorithm omitting parental karyotype analysis and replacing it with POC CMA.7 This new algorithm permits the isolation of a specific group of cases with a normal modified ASRM work-up in addition to having one euploid loss diagnosed. Representing 10% of RPL cases, this new group of patients, we believe, would be ideal for further research and investigation on new etiologies and therapies for unexplained RPL.7,8 Also, by providing an explanation for the loss in more than 90% of couples, this approach has the potential to bring improved and important closure and psychological relief for couples dealing with RPL, compared to regular ASRM work-up where more than 50% of cases remain “unexplained”.6,7 This proposed evaluation was considered as cost-efficient at least in a US setting but has been criticized as possibly not cost saving in other settings like in Canada.6–8
Based on the concern that countries outside the USA might have limited financial resources, another RPL algorithm was published by our group based on the Canadian health care system.8 This clinical algorithm starts with a regular ASRM work-up including parental karyotype and reserves the use of POC genetic analysis for cases that remain unexplained. This would potentially eliminate the POC CMA on about half of the RPL patients who presumably had a potential cause identified and treated after the ASRM workup.8 The strength of this proposed evaluation relies in the fact that it can identify the group of unexplained RPL with a euploid loss that would be ideal for further research and investigation.7,8 Moreover, it might be more cost-effective in a setting where genetic testing of POC is not routinely performed for expense or availability reasons. Therefore, it could be considered as more appealing for clinical application in some settings.
We believe however, that a strategy including universal POC advanced genetic analysis has a role in research as it classifies all RPL cases into sub-groups with or without POC aneuploidy and could therefore help determine over time whether the addition of routine genetic POC testing could have a prognostic value in RPL independently of ASRM or ESHRE work-up result. Indeed, whether genetic testing of POC has any prognostic significance remains a matter of debate.27–29 Also, the typical clinical scenario includes cases presenting after two to three episodes of miscarriage and without a complete work-up being performed. In many cases, such as after spontaneous or medically induced miscarriage, POC of the last miscarriage has not been preserved for future genetic testing. In our opinion, therefore, either POC of second or subsequent loss should be routinely collected and preserved for possible future genetic testing, or a policy of direct routine POC genetic testing at the second or subsequent miscarriage should be adopted.
Rational on which is the best approach for management of RPL varies and should depend on the type and costs of genetic testing available and remains a matter of debate in the literature.6–8 However, these new approaches have led to improved awareness and understanding among us about the role that aneuploidy plays in RPL, as well as the role of genetic testing of POC in RPL.
Role of PGT
Pre-implantation genetic testing (PGT) is a form of genetic testing that requires in-vitro fertilization (IVF) and embryo biopsy, and therefore involves qualified and experienced laboratory staff as well as large added costs. It can be considered potentially therapeutic though in specific situations only. Many groups have published on two technologies mainly, PGT-SR (PGT- Structural chromosomal Rearrangement) and PGT-A (PGT-Aneuploidy). We will discuss each of these technologies and their roles in the setting of RPL, separately below.
PGT-SR involves a targeted approach typically used when known chromosomal abnormalities are present in parental genomes. The role of PGT-SR in RPL has been well defined to situations with the presence of balanced parental translocation diagnosed by karyotyping and in the presence of unbalanced translocation or inversion detected on POC genetic testing.30,31
PGT-SR has evolved over the years since its introduction in the early 1990s, from FISH, quantitative real-time PCR (qPCR) to comprehensive testing methods such as array-based comparative genomic hybridization, single nucleotide polymorphism (SNP) array and more recently next-generation sequencing (NGS). In addition, the performance of the biopsy has evolved from day 3 IVF multi-cell embryo biopsy to day 5 blastocyst trophectoderm biopsy.
The addition of CMA technology and day 5 trophectoderm biopsy have improved PGT-SR ability to screen for 24 chromosome aneuploidy and unbalanced translocation in preimplantation IVF embryos, and to select the most competent balanced and euploid embryo(s) for transfer. Unlike past reports, discussed earlier, the most recent publications reveal improved clinical and live birth rates per pregnancy, as well as decreased miscarriage rate for translocation carriers.32–35
PGT-A on the other hand is a technology that was developed to screen for chromosomal aneuploidies that arise spontaneously. Its role, for cases where aneuploidy is thought to play a significant effect, remains heavily debated in clinical practice. Few studies have investigated the role of PGT-A role in RPL specifically. The ESHRE recommends against its use for RPL couples without a genetic cause.2,29,30
PGT-A has many limitations including a high cost, a risk of having no euploid embryo to transfer especially with advanced maternal age as well as possible embryo wastage and the presence of embryos with mosaicism of unknown clinical significance.36 Therefore, proper counseling is essential before use. The largest prospective, randomized controlled trial of the use of PGT-A by Munne et al was conducted using NGS on a total of 661 patients with at least 2 blastocysts to biopsy. The investigators reported no advantage for the use of PGT-A versus morphology alone for embryo selection for IVF in women under 37 years old.37 In a recent study, NGS PGT-A with trophectoderm biopsy, in poor responders with four or fewer oocytes available was found not to improve LBR per oocyte retrieval. Despite a lower miscarriage rate in this study, 31 patients would need to be treated to prevent one miscarriage.38
In 2020, using PGT Liu et al found a significantly higher rate of chromosomal abnormalities in blastocysts of young women with idiopathic RPL compared with women with no or sporadic miscarriage.39 But the role of PGT-A in in RPL, remains to be clarified. In an intent to treat analysis, Murugappan et al found similar clinical outcomes in terms of pregnancy rate, live birth and clinical miscarriage in RPL patients whether expectant management or PGT-A were used.40
Interpretation of this study was limited by the predominant use of Day 3 biopsy on multi-celled embryos which has been shown to lower pregnancy rates.34
Currently PGT-A use is not recommended by any society guidelines in either IVF patients with infertility or in RPL patients. At least two studies are currently being conducted and might help better elucidate the role of PGT-A, if any, in both RPL and ASRM unexplained RPL.41,42
Sato et al showed that PGT-A could improve live birth rate per IVF transfer in RPL cases with history of POC aneuploidy.43 Zhou et al found no improvement with the use of PGT-A in terms of live birth rate or the rate of miscarriage for women younger than 38 years without recurrent pregnancy loss but with a history of POC with embryonic chromosomal abnormalities.44
Very recently, proposed criteria considered necessary to perform successful PGT-A on RPL patients were updated and published by our group.8,20 These include couples with a negative ASRM or ESHRE workup, a history of aneuploid pregnancy loss, female partner with a normal ovarian reserve producing a high number of oocytes and blastocysts available for biopsy. In addition, IVF is to be undertaken in centers with extensive experience with embryo biopsy and overall PGT-A practice.8
Lee et al conducted an economic evaluation study on PGT-A in first fresh IVF stimulations cycles and their related frozen transfers, on the whole USA population between 2014 and 2016. A total of 158,665 IVF cycles were analyzed, of which 16.2% intended to use PGT-A. PGT-A cost-effectiveness was found to be dependent on patient age and payer perspective; and the authors recommended against routine PGT-A as it was found to be associated with higher costs and worse clinical outcomes in patients younger than 35. At age 35 and older, PGT-A led to more cumulative birth but was associated with higher costs from both patient and payer perspectives. Of note, only starting at the age 39, was the incremental cost per live birth favoring PGT-A from a patient perspective.45
We agree with recommendations in favor of expectant management in most cases of RPL explained by ASRM or ESHRE guidelines. But we believe there might be a role for PGT-A in RPL, especially in cases with recurrent POC aneuploidy as identified by one of our proposed algorithms,7 as well as in cases unexplained by ASRM or ESHRE workups having one episode of aneuploidy diagnosed as identified by the latest proposed criteria by our group.8 The challenge with PGT-A remains in older patients, given the drawbacks of this technology discussed above, and particularly with the high prevalence of diminished ovarian reserve in this population.46 In fact, in older patients and those with diminished ovarian reserve, there are often very few oocytes retrieved and the selection technique can become counterproductive. Therefore, judicious use of PGT-A should always be advised in the presence of diminished ovarian reserve.
Future Directions
Maternal cell-free (cf) DNA is a technology currently used for non-invasive prenatal testing, that involves detecting embryonal chromosomal abnormalities in cf DNA from shed and ruptured placental cells present in maternal blood. It has been recently proposed as a replacement for POC genetic analysis in RPL.47,48 cf DNA technology offers the advantage of not having to collect a POC sample. Some patients miscarry before a sample can be obtained, and many miscarriages are currently managed medically, therefore this technology might have a role. However, larger data sets are needed to validate the use of cf DNA for RPL patients. While neither POC genetic testing nor maternal cf DNA are anticipated to improve outcome in RPL, both are likely to provide a reason for the loss especially in cases unexplained by ESHRE or ASRM workups.
Conclusion
Human reproduction is an extremely complicated but inefficient process. It has been estimated that approximately 70% of human conceptions never achieve viability, and that 50% fail spontaneously before being detected.9,10 Spontaneous miscarriage is the most common complication of pregnancy, and represents one of the last points in the reproductive process to prevent the birth of an abnormal baby. Large studies have indicated that fetal aneuploidy is the most common cause of miscarriage in over 55% of cases. We believe that genetic testing on the products of conception should be performed after the second and subsequent pregnancy loss. Although the results will not generally alter the course of treatment, the knowledge of the reason for the loss is of great emotional comfort to many patients. We have outlined the different methods of genetic testing that are available for the detection of fetal aneuploidy while discussing the advantages and disadvantages of each.
Disclosure
RS Papas reported no conflicts of interest for this work. WH Kutteh is a research investigator and speaker for Natera and reported no other potential conflicts of interest for this work.
References
1. Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98(5):1103–1111. doi:10.1016/j.fertnstert.2012.06.048
2. Bender Atik R, Christiansen OB, Elson J; ESHRE Guideline Group on RPL. ESHRE guideline: recurrent pregnancy loss. Human Reproduction Open. 2018;2018(2):hoy004. doi:10.1093/hropen/hoy004
3. van Dijk MM, Kolte AM, Limpens J, et al. Recurrent pregnancy loss: diagnostic workup after two or three pregnancy losses? A systematic review of the literature and meta-analysis. Hum Reprod Update. 2020;26(3):356–367. doi:10.1093/humupd/dmz048
4. Shahine L, Lathi R. Recurrent pregnancy loss: evaluation and treatment. Obstetrics Gynecol Clin. 2015;42(1):117–134. doi:10.1016/j.ogc.2014.10.002
5. Dimitriadis E, Menkhorst E, Saito S, Kutteh WH, Brosens JJ. Recurrent pregnancy loss. Nat Rev Dis Primers. 2020;6(1):1–9.
6. Popescu F, Jaslow CR, Kutteh WH. Recurrent pregnancy loss evaluation combined with 24-chromosome microarray of miscarriage tissue provides a probable or definite cause of pregnancy loss in over 90% of patients. Human Reproduction. 2018;33(4):579–587. doi:10.1093/humrep/dey021
7. Papas RS, Kutteh WH. A new algorithm for the evaluation of recurrent pregnancy loss redefining unexplained miscarriage: review of current guidelines. Curr Opin Obstet Gynecol. 2020;32(5):371–379. doi:10.1097/GCO.0000000000000647
8. Dahdouh EM, Kutteh WH. Genetic Testing of Products of Conception in Recurrent Pregnancy Loss Evaluation. Reprod Biomed Online. 2021. doi:10.1016/j.rbmo.2021.03.015
9. Edmonds DK, Lindsay KS, Miller JF, Williamson E, Wood PJ. Early embryonic mortality in women. Fertil Steril. 1982;38(4):447–453. doi:10.1016/S0015-0282(16)46579-9
10. Wilcox AJ, Weinberg CR, Baird DD. Risk factors for early pregnancy loss. Epidemiology. 1990;1(5):382–385. doi:10.1097/00001648-199009000-00008
11. van den Berg MM, van Maarle MC, van Wely M, Goddijn M. Genetics of early miscarriage. Biochimica et Biophysica Acta. 2012;1822(12):1951–1959. doi:10.1016/j.bbadis.2012.07.001
12. Maisenbacher MK, Merrion K, Kutteh WH. Single-nucleotide polymorphism microarray detects molar pregnancies in 3% of miscarriages. Fertil Steril. 2019;112(4):700–706. doi:10.1016/j.fertnstert.2019.06.015
13. Blue NR, Page JM, Silver RM. Genetic abnormalities and pregnancy loss. Semin Perinatol. 2019;43(2):66–73. doi:10.1053/j.semperi.2018.12.002
14. Dahdouh EM, Balayla J, García-Velasco JA. Comprehensive chromosome screening improves embryo selection: a meta-analysis. Fertil Steril. 2015;104(6):1503–1512. doi:10.1016/j.fertnstert.2015.08.038
15. Flynn H, Yan J, Saravelos SH, Li TC. Comparison of reproductive outcome, including the pattern of loss, between couples with chromosomal abnormalities and those with unexplained repeated miscarriages. J Obstetrics Gynaecol Res. 2014;40(1):109–116. doi:10.1111/jog.12133
16. Bedaiwy MA, Maithripala SI, Durland US, et al. Reproductive outcomes of couples with recurrent pregnancy loss due to parental chromosome rearrangement. Fertil Steril. 2016;106(3):e343. doi:10.1016/j.fertnstert.2016.07.970
17. Ikuma S, Sato T, Sugiura-Ogasawara M, Nagayoshi M, Tanaka A, Takeda S. Preimplantation genetic diagnosis and natural conception: a comparison of live birth rates in patients with recurrent pregnancy loss associated with translocation. PLoS One. 2015;10(6):e0129958. doi:10.1371/journal.pone.0129958
18. Iews M, Tan J, Taskin O, et al. Does preimplantation genetic diagnosis improve reproductive outcome in couples with recurrent pregnancy loss owing to structural chromosomal rearrangement? A systematic review. Reprod Biomed Online. 2018;36(6):677–685. doi:10.1016/j.rbmo.2018.03.005
19. Bernardi LA, Plunkett BA, Stephenson MD. Is chromosome testing of the second miscarriage cost saving? A decision analysis of selective versus universal recurrent pregnancy loss evaluation. Fertil Steril. 2012;98(1):156–161. doi:10.1016/j.fertnstert.2012.03.038
20. Brezina PR, Kutteh WH. Classic and cutting-edge strategies for the management of early pregnancy loss. Obstetrics Gynecol Clin. 2014;41(1):1–8. doi:10.1016/j.ogc.2013.10.011
21. Foyouzi N, Cedars MI, Huddleston HG. Cost-effectiveness of cytogenetic evaluation of products of conception in the patient with a second pregnancy loss. Fertil Steril. 2012;98(1):151–155. doi:10.1016/j.fertnstert.2012.04.007
22. Sahoo T, Dzidic N, Strecker MN, et al. Comprehensive genetic analysis of pregnancy loss by chromosomal microarrays: outcomes, benefits, and challenges. Genetics in Medicine. 2017;19(1):83–89. doi:10.1038/gim.2016.69
23. Mathur N, Triplett L, Stephenson MD. Miscarriage chromosome testing: utility of comparative genomic hybridization with reflex microsatellite analysis in preserved miscarriage tissue. Fertil Steril. 2014;101(5):1349–1352. doi:10.1016/j.fertnstert.2014.02.004
24. Wang BT, Chong TP, Boyar FZ, et al. Abnormalities in spontaneous abortions detected by G-banding and chromosomal microarray analysis (CMA) at a national reference laboratory. Mol Cytogenet. 2014;7(1):1–6. doi:10.1186/1755-8166-7-33
25. Levy B, Sigurjonsson S, Pettersen B, et al. Genomic imbalance in products of conception: single-nucleotide polymorphism chromosomal microarray analysis. Obstet Gynecol. 2014;124(2 PART 1):202–209. doi:10.1097/AOG.0000000000000325
26. Robberecht C, Schuddinck V, Fryns JP, Vermeesch JR. Diagnosis of miscarriages by molecular karyotyping: benefits and pitfalls. Genetics in Medicine. 2009;11(9):646–654. doi:10.1097/GIM.0b013e3181abc92a
27. Ogasawara M, Aoki K, Okada S, Suzumori K. Embryonic karyotype of abortuses in relation to the number of previous miscarriages. Fertil Steril. 2000;73(2):300–304. doi:10.1016/S0015-0282(99)00495-1
28. Goldstein M, Svirsky R, Reches A, Yaron Y. Does the number of previous miscarriages influence the incidence of chromosomal aberrations in spontaneous pregnancy loss? J Mater Fetal Neonatal Med. 2017;30(24):2956–2960. doi:10.1080/14767058.2016.1269317
29. Zhu X, Li J, Zhu Y, et al. Application of chromosomal microarray analysis in products of miscarriage. Mol Cytogenet. 2018;11(1):1–6. doi:10.1186/s13039-018-0396-y
30. Viotti M. Preimplantation genetic testing for chromosomal abnormalities: aneuploidy, mosaicism, and structural rearrangements. Genes. 2020;11(6):602. doi:10.3390/genes11060602
31. Carvalho F, Coonen E, Goossens V, et al.; ESHRE PGT Consortium Steering Committee. ESHRE PGT Consortium good practice recommendations for the organisation of PGT. Human Reproduction Open. 2020;2020(3):hoaa021. doi:10.1093/hropen/hoaa021
32. Huang C, Jiang W, Zhu Y, et al. Pregnancy outcomes of reciprocal translocation carriers with two or more unfavorable pregnancy histories: before and after preimplantation genetic testing. J Assist Reprod Genet. 2019;36(11):2325–2331. doi:10.1007/s10815-019-01585-9
33. Tan YQ, Tan K, Zhang SP, et al. Single-nucleotide polymorphism microarray-based preimplantation genetic diagnosis is likely to improve the clinical outcome for translocation carriers. Human Reproduction. 2013;28(9):2581–2592. doi:10.1093/humrep/det271
34. Treff NR, Northrop LE, Kasabwala K, Su J, Levy B, Scott JRT. Single nucleotide polymorphism microarray–based concurrent screening of 24-chromosome aneuploidy and unbalanced translocations in preimplantation human embryos. Fertil Steril. 2011;95(5):1606–1612. doi:10.1016/j.fertnstert.2010.11.004
35. Dahdouh EM, Balayla J, Audibert F, et al. Technical update: preimplantation genetic diagnosis and screening. J Obstetrics Gynaecol Canada. 2015;37(5):451–463. doi:10.1016/S1701-2163(15)30261-9
36. Paulson RJ. Hidden in plain sight: the overstated benefits and underestimated losses of potential implantations associated with advertised PGT-A success rates. Human Reproduction. 2020;35(3):490–493. doi:10.1093/humrep/dez280
37. Munné S, Kaplan B, Frattarelli JL, et al. Preimplantation genetic testing for aneuploidy versus morphology as selection criteria for single frozen-thawed embryo transfer in good-prognosis patients: a multicenter randomized clinical trial. Fertil Steril. 2019;112(6):1071–1079. doi:10.1016/j.fertnstert.2019.07.1346
38. Deng J, Hong HY, Zhao Q, et al. Preimplantation genetic testing for aneuploidy in poor ovarian responders with four or fewer oocytes retrieved. J Assist Reprod Genet. 2020;37(5):1147–1154. doi:10.1007/s10815-020-01765-y
39. Liu XY, Fan Q, Wang J. Higher chromosomal abnormality rate in blastocysts from young patients with idiopathic recurrent pregnancy loss. Fertil Steril. 2020;113(4):853–864. doi:10.1016/j.fertnstert.2019.11.016
40. Murugappan G, Shahine LK, Perfetto CO, Hickok LR, Lathi RB. Intent to treat analysis of in vitro fertilization and preimplantation genetic screening versus expectant management in patients with recurrent pregnancy loss. Human Reproduction. 2016;31(8):1668–1674. doi:10.1093/humrep/dew135
41. Lei C, Sui Y, Ye J, et al. Comparison of PGS 2.0 versus conventional embryo morphology evaluation for patients with recurrent pregnancy loss: a study protocol for a multicentre randomized trial. BMJ Open. 2020;10(10):e036252.
42. Lei C, Sui Y, Ye J, et al. Comparison of PGT-A versus conventional embryo morphology evaluation for patients with recurrent pregnancy loss: a study protocol for a multicentre randomised trial. BMJ Open. 2020;10(10):e036252. doi:10.1136/bmjopen-2019-036252
43. Sato T, Sugiura-Ogasawara M, Ozawa F, et al. Preimplantation genetic testing for aneuploidy: a comparison of live birth rates in patients with recurrent pregnancy loss due to embryonic aneuploidy or recurrent implantation failure. Human Reproduction. 2019;34(12):2340–2348. doi:10.1093/humrep/dez229
44. Zhou T, Zhu Y, Zhang J, et al. Effects of PGT-A on Pregnancy Outcomes for Young Women Having One Previous Miscarriage with Genetically Abnormal Products of Conception. Reproductive Sci. 2021;1–7. doi:10.1007/s43032-020-00271-x
45. Lee M, Lofgren KT, Thomas A, et al. The cost-effectiveness of preimplantation genetic testing for aneuploidy in the United States: an analysis of cost and birth outcomes from 158,665 in vitro fertilization cycles. Am J Obstet Gynecol. 2021. doi:10.1016/j.ajog.2021.01.021
46. Bunnewell SJ, Honess ER, Karia AM, Keay SD, Al Wattar BH, Quenby S. Diminished ovarian reserve in recurrent pregnancy loss: a systematic review and meta-analysis. Fertil Steril. 2020;113(4):818–827. doi:10.1016/j.fertnstert.2019.11.014
47. Yaron Y, Pauta M, Badenas C, et al. Maternal plasma genome-wide cell-free DNA can detect fetal aneuploidy in early and recurrent pregnancy loss and can be used to direct further workup. Human Reproduction. 2020;35(5):1222–1229. doi:10.1093/humrep/deaa073
48. Colley E, Devall AJ, Williams H, et al. DNA in the Investigation of Miscarriage. J Clin Med. 2020;9(11):3428. doi:10.3390/jcm9113428
49. Mainsenbacher MK, Merrion K, Levy B, Kutteh WH Single nucleotide polymorphism (SNP) array analysis of 63,277 products of conception (POC) samples: a 10-year laboratory experience. Fertility and Sterility. 2020;114(3):e47.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.