Back to Journals » The Application of Clinical Genetics » Volume 19
Genetic Polymorphisms of Transforming Growth Factor Receptors (TGF-βRI, TGF-βRII) and Risk Factors Associated with Keloid Scars in Burkina Faso: A Cross-Sectional Study
Authors Keto KA ![]() , Belemsigri D, Soubeiga ST
, Belemsigri D, Soubeiga ST ![]() , Bonkoungou M, Gadiaga HNB, Compaore B, Sorgho PA, Yonli AT, Djigma WF
, Bonkoungou M, Gadiaga HNB, Compaore B, Sorgho PA, Yonli AT, Djigma WF ![]() , Simpore J, Niamba P
, Simpore J, Niamba P
Received 11 February 2026
Accepted for publication 7 May 2026
Published 15 May 2026 Volume 2026:19 602982
DOI https://doi.org/10.2147/TACG.S602982
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Martin Maurer
Koffi Agbessi Keto,1 Danielle Belemsigri,2 Serge Theophile Soubeiga,3,4 Marcelin Bonkoungou,5 Hadiaratou Nafore Badiala Gadiaga,2 Bibata Compaore,2 Pegdwinde Abel Sorgho,4 Albert Theophane Yonli,4 Wendkuuni Florencia Djigma,1,6 Jacques Simpore,1,4 Pascal Niamba2,6
1Department of Biochemistry-Microbiology, Laboratory of Molecular Biology and Molecular Genetics, Joseph KI-ZERBO University, Ouagadougou, Burkina Faso; 2Department of Dermatology and Venereology, Yalgado Ouedraogo University Hospital, Ouagadougou, Burkina Faso; 3Department of Biomedical and Public Health, Research Institute for Health Sciences, Ouagadougou, Burkina Faso; 4Department of Molecular Biology, Pietro Annigoni Biomolecular Research Center (CERBA), Ouagadougou, Burkina Faso; 5Department of Dermatology and Venereology, Bogodogo University Hospital, Ouagadougou, Burkina Faso; 6Department of Medicine, Joseph KI-ZERBO University, Ouagadougou, Burkina Faso
Correspondence: Serge Theophile Soubeiga, Department of Biomedical and Public Health, Research Institute for Health Sciences, Ouagadougou, Burkina Faso, Email [email protected]
Background: The keloids scar is a skin scarring pathology with a higher frequency in the black population. Several genetic polymorphisms, including those of transforming growth factor receptors, have been identified as probable susceptibility genes. This study aimed to characterize the polymorphisms of TGF-βRI, TGF-βRII and identify risk factors associated with keloid scars in Burkina Faso.
Methods: This was a cross-sectional study that included 141 subjects with keloids and conducted from April 2021 to April 2022. Genomic DNA was extracted using the “PureLinkTM Genomic DNA Mini kit”. Genotyping of TGF-βRI rs111854391, rs121918710, and TGF-βRII rs104893807, rs28934568 polymorphisms was performed using real-time PCR. Results were considered statistically significant at p< 0.05.
Results: The average age of the study population was 34 ± 15 years and O Rhesus positive blood group (O+) was predominant (36.88%). All subjects (100%) were heterozygous (TG) for rs121918710. Medical or surgical history, family history, blood type, and rs28934568 polymorphism were related to the number of sites of keloids on the body. Patients with a medical history (9.8%) were carriers of the mutant allele C for rs28934568. Mossi ethnic had more than 8 times risk of developing a keloid scar (p=0.030; OR=8.66 (95% CI: 1.230– 60.902).
Conclusion: The presence in all the patients of the mutated allele for the rs 121918710 polymorphism could explain the involvement of this mutation in the occurrence of keloid scars. In addition, ethnicity and blood type were the risk factors associated with keloids.
Keywords: keloids, transforming growth factors, polymorphisms, alleles, Burkina Faso
Background
Following a cutaneous lesion, a process of reaction of cicatrization is set up by the human organism with the aim of leading to the closing of the lesion, on the one hand, and the reconstitution of the damaged tissue, on the other hand.1 When the balance of reparative processes is disturbed, wound healing can be impaired, resulting in pathological scarring, which can be chronic wounds or excessive scar formation ranging from hypertrophic scars to keloids.2,3 The keloid scar represents a pathology of skin healing corresponding to an abnormal proliferation of fibrous tissue in the dermis and which can be responsible for a functional and aesthetic embarrassment.4–6 The pathophysiological process of keloids is not well known, but they can occur in all populations, and there is a high frequency in the black population with a prevalence between 4.5% and 16%.7 In sub-Saharan Africa, where these pathologies predominate, few studies have been conducted, and the frequencies are only hospitalized, including 2.5% in the Congo,8 1.9% in Togo,9 and 0.7% in Benin.10 In Burkina Faso, the frequency is estimated at 10.2% in schools.11 The insufficiency of these data in our regions makes management difficult despite the fact that keloids are one of the most frequent reasons for dermatological consultation.
Numerous studies have established a significant genetic predisposition to the development of keloids. Many candidate genes are targeted, notably certain Human Leucocyte Antigens (HLA) polymorphisms and transforming growth factors β (TGF-β) and their receptors (TGF-βRI, TGF-βRII),12 intervening in signal transduction through different pathways. TGF-β is widely present in various tissues and cells, with diverse biological functions including regulating cell proliferation, differentiation, migration, apoptosis, and extracellular matrix (ECM) synthesis, and degradation.13 In keloids, TGF-β plays a key role in tissue development, renewal, and repair, and appears to be involved in the pathogenesis compared to other genes.14,15 Existing literature lacks data on whether the TGF-βRI and TGF-βRII polymorphisms observed in other regions have the same functional impact on receptor-ligand binding affinity and downstream signaling within the specific genetic background of African patients.
We aimed to characterize the polymorphisms of transforming growth factor receptors (TGF-βRI, TGF-βRII) and risk factors associated with the occurrence of keloids in patients from Burkina Faso.
Materials and Methods
Study Setting
This was a cross-sectional study that took place from April 2021 to April 2022 in Ouagadougou, Burkina Faso. The patients were recruited in the dermatology departments of three (3) health centers, including the Yalgado Ouedraogo University Hospital (CHU-YO), the Bogodogo University Hospital (CHU-B), and the Medical Center of the General Camp Aboubacar Sangoulé Lamizana (CMCGASL). The Pietro Annigoni Biomolecular Research Center (CERBA) and the Laboratory of Molecular Biology and Genetics (LABIOGENE) were used for biological and genetic analyses.
Recruitment of Patients
A total 141 patients with keloids were recruited. The sample size was calculated using Schwartz formula and a prevalence value of 10.2% reported by Traore et al in 2019. Any adult patient of both sexes, regardless of age, ethnicity, or religion, confirmed with keloids by the dermatologist and who freely agreed to participate in the study was included in this study.
A case is a patient presenting an abnormal proliferation of scar tissue that forms at the site of cutaneous injury (eg, on the site of a surgical incision or trauma); and that does not regress and grows beyond the original margins of the scar Exclusion criteria were as follows: any patient with a skin pathology other than keloids; anyone without keloid scars; or any patient who was eligible but refused to give consent to participate in the study. Dermatologists were in charge of the recruitment of participants.
Biological Samples Collection
Whole blood sample was collected in patients included in a tube impregnated with ethylene diamine tetra-acetic acid (EDTA). The samples were then sent to CERBA for processing. The samples were used for blood/rhesus grouping of the patients, using the Beth Vincent technique, then centrifuged at 3500 rpm for 15 min, aliquoted in cryotubes, and stored at −80°C for molecular analyses.
Detection of Transforming Growth Factor Receptor Polymorphisms TGF-βRI (rs111854391, rs121918710) and TGF-βRII (rs104893807, rs28934568)
Genomic DNA was extracted from whole blood using the “PureLink™ Invitrogen Genomic DNA Minikit” kit (ThermoFisher, USA). Genotyping of polymorphisms was performed using real-time PCR with a 10 µL reaction mixture consisting of 2µL DNA, 5.3 µL sterile water, 2.5 µL TaqMan® Probe Universal qPCR Mix 5x, and 0.2 µL SNP mix (40x). The PCR program consisted of an initial denaturation step and Taq polymerase activation at 95°C for 10 minutes; followed by 35 cycles of denaturation at 92°C for 15 seconds, hybridization and elongation at 60°C for 1 minute.
Ethical Considerations
Our study obtained the approval of the Health Research Ethics Committee (CERS) of the Ministry of Health (Deliberation n°2021-03-058) and the authorization of the health structures of each site for the recruitment of patients. This study complies with the Declaration of Helsinki. All participants received information and gave their signed consent form to participate in the study. For those who were not able to read, they received information in their local language before giving their consent. A parent or legal guardian of participants under 18 years of age provided informed consent. Anonymity and confidentiality were respected for all patients.
Statistical Analysis
Data were entered using Excel 2016 software. Data were analyzed using Statistical Package for the Social Sciences (SPSS) 21.0 software. Allelic discrimination was performed using TaqMan Genotyper® 1.6.0 software to determine the genotype of each polymorphism. Categorical variables were compared using the Pearson’s Chi-square test where cell counts were less than five. To identify independent risk factors for keloid occurrence, variables were entered into a Multivariate Logistic Regression model. Odds ratios and 95% confidence intervals were calculated to assess risk. Results were considered statistically significant for p˂ 0.05.
Results
Socio-Demographic Characteristics
The distribution of the subjects according to sex shows a predominance of the female sex, representing 73.1% of the subjects present at the time of the study with a statistically significant difference (p<0.001). The average age of the study population was 34 ± 15 years with a predominance of the young age group 19 to 29 years (36.2%) (p=0.154). Employees (32.6%), single persons (48.94%), and subjects with higher education (35.5%) were in the majority. The most represented ethnic group was Mossi (59.6%), followed by subjects with parents of different ethnicities (cultural mixing) (16.3%) with a statistically significant difference (p<0.001). Subjects with a medical or surgical history (73.3%) and family history (48.9%) were the most represented with significant differences, respectively, p<0.001 and p=0.018 (Table 1).
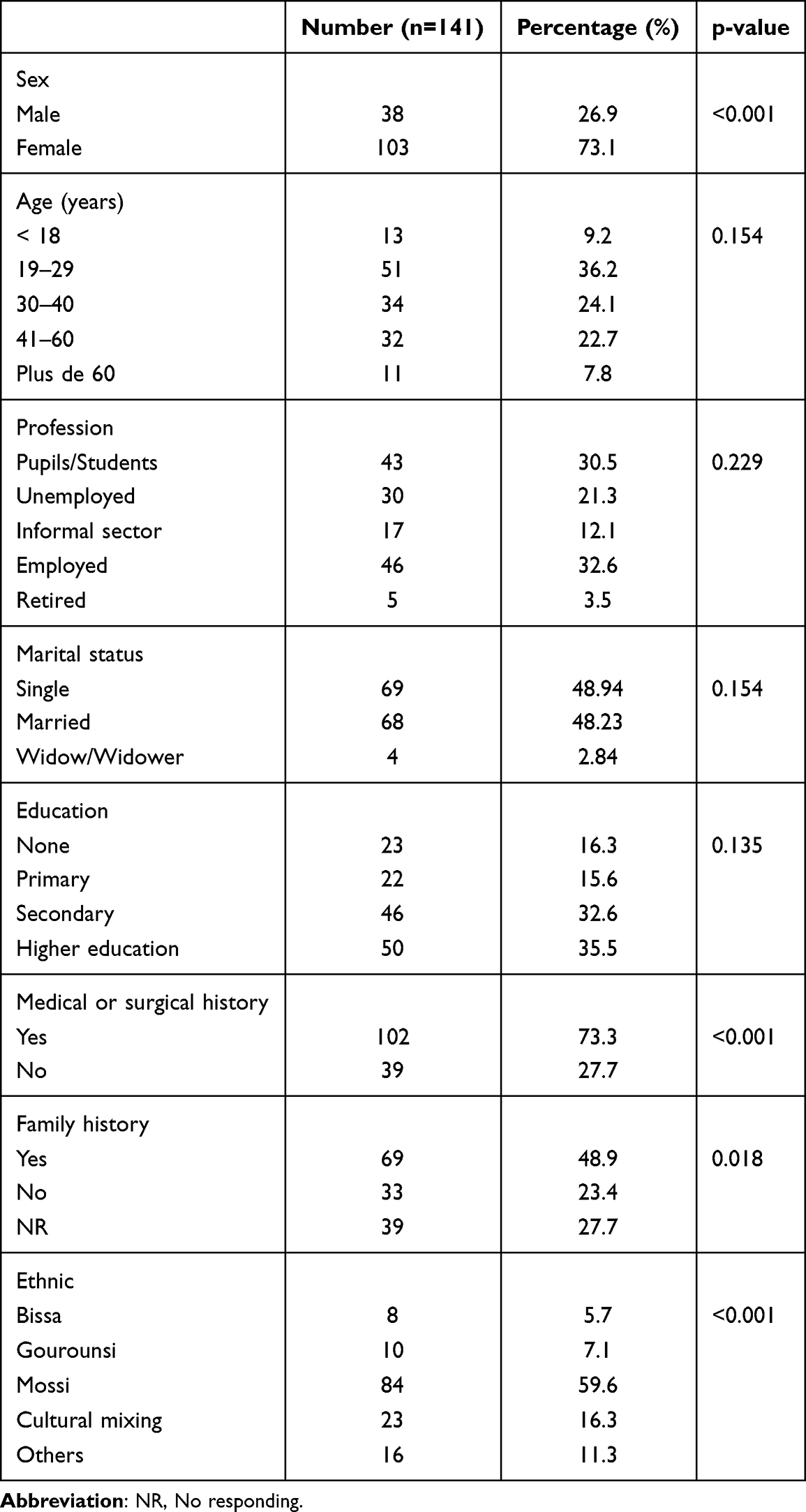 |
Table 1 Sociodemographic Characteristics |
Frequency of Blood Group and Different Polymorphisms of TGFβRI and TGFβRII
The grouping according to the type of blood group and Rhesus factor shows a predominance of blood group O (39.01%). The genetic analyses showed results according to the different polymorphisms as follows: Concerning TGFβRI rs121918710, all patients (100%) were GT heterozygous, indicating that all had the G mutated allele. Concerning TGFβRII rs28934568 68.79% were homozygous wild-type versus 31.21% who were heterozygous and therefore carriers of the C mutated allele (Table 2).
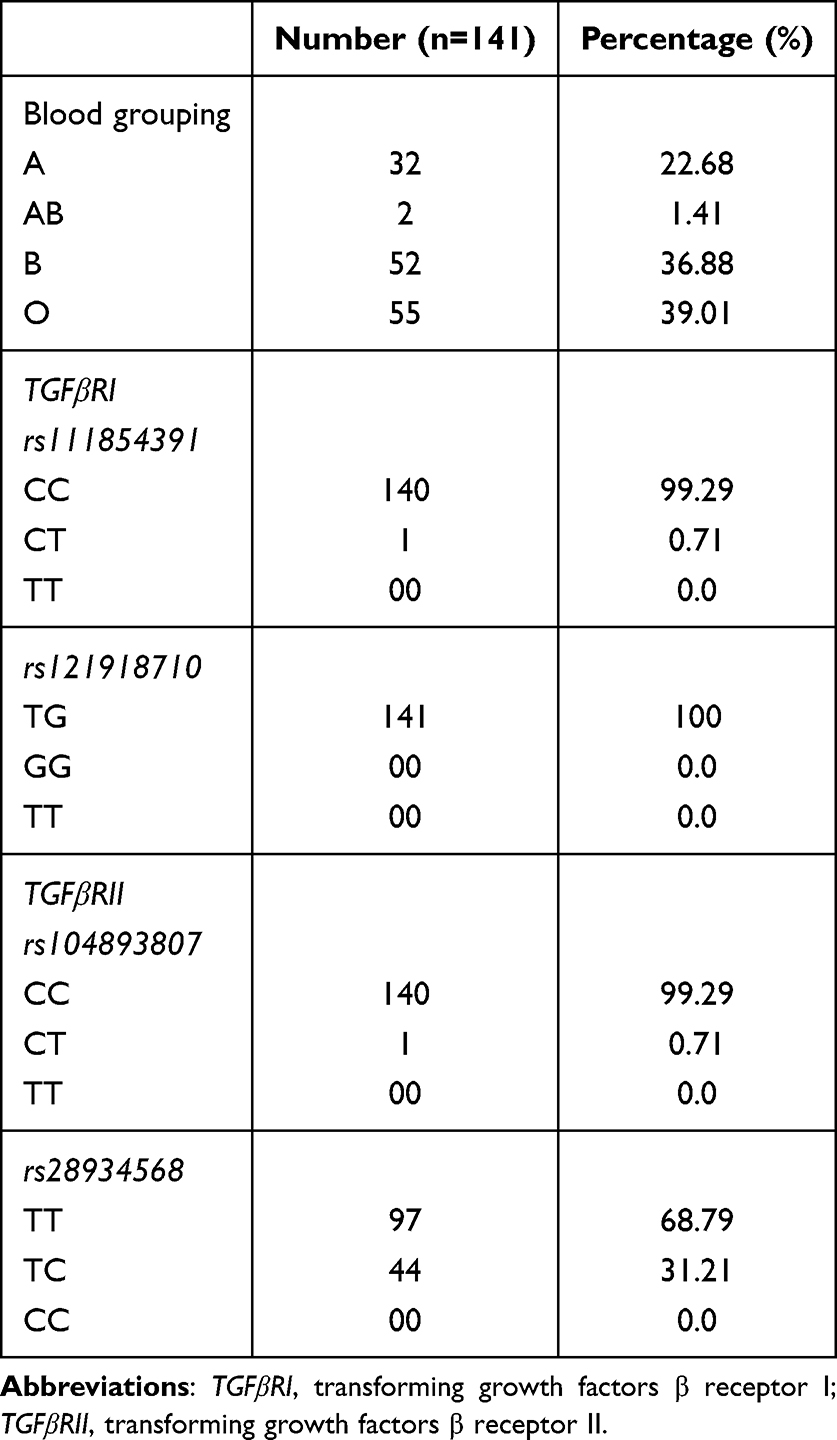 |
Table 2 Frequency of Blood Grouping and Different Genetic Polymorphisms |
Association Between Parameters and the Number of Keloid Location Sites
Bivariate analysis showed that age, occupation, education, ethnicity, medical or surgical history, family history, blood type, and rs28934568 polymorphism were associated with the number of sites of keloids on the body (p<0.001). We note that 31.1% of Mossi patients had at least 3 sites of keloid localization on the body. Then, 41.1% of the patients who presented medical or surgical history had at least 3 keloid sites on the body versus 16.3% (p<0.001) and 33.3% (p<0.001) of the patients who presented familial history had at least 3 keloid sites on the body versus 23.5% (Table 3).
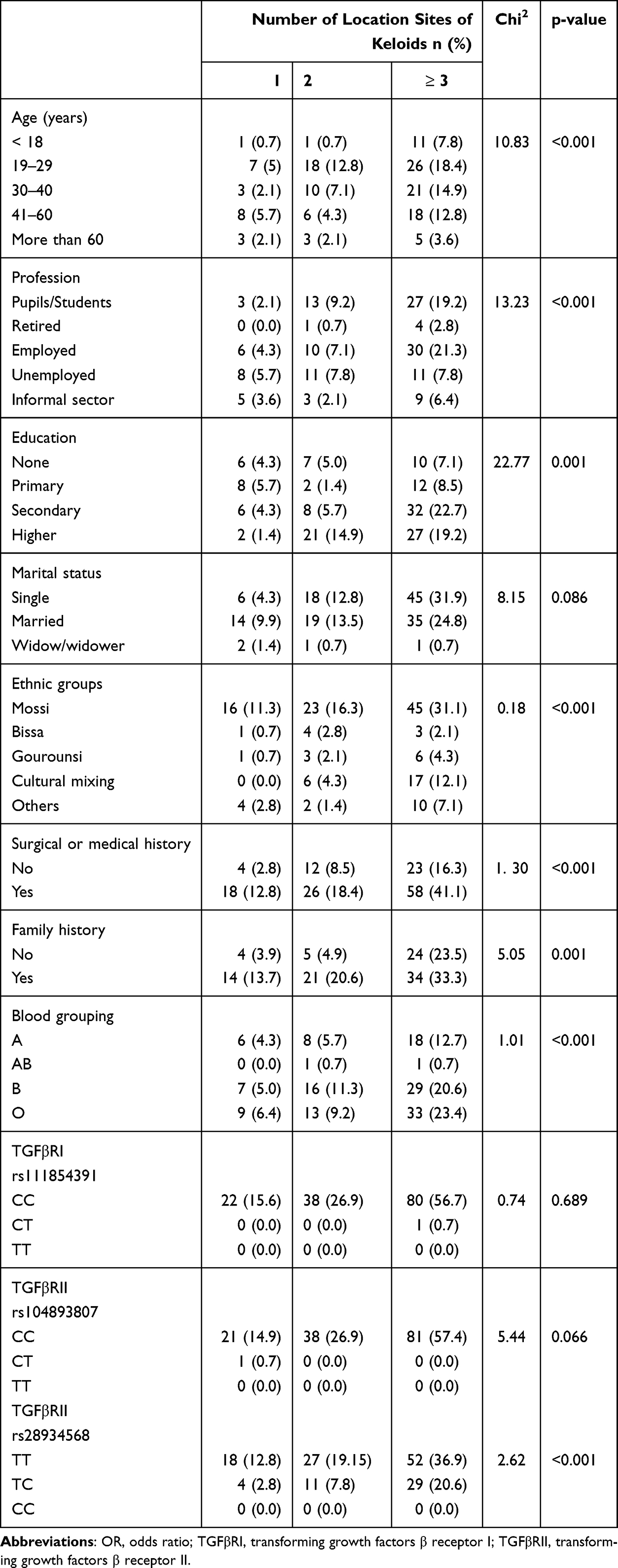 |
Table 3 Association Between Parameters and Number of Keloid Sites |
Risk Factors Associated with Keloids
After univariate and multivariate logistic regression analysis, we found that only Mossi ethnicity was strongly associated with the occurrence of keloids [p=0.030; OR=8.66 (95% CI: 1.230–60.902)]. Mossi had more than 8 times the risk of developing a keloid [p=0.030; OR=8.66 (95% CI: 1.230–60.902)] (Table 4). Sex, education, occupation, marital status, and family history were not associated with keloids.
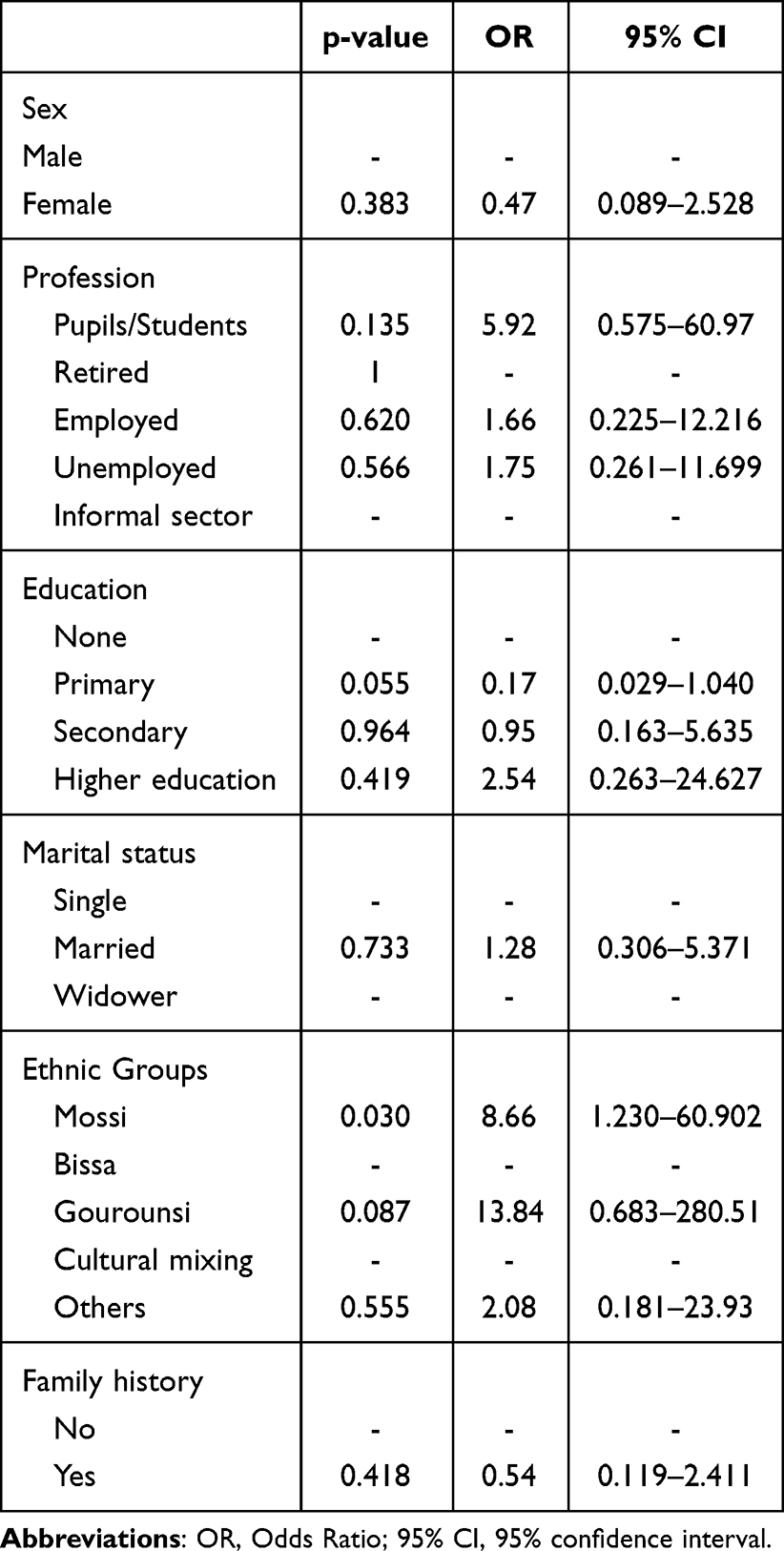 |
Table 4 Multivariate Logistic Regression Analysis of the Risk Factors Associated with Keloids |
Discussion
Our study is the first in Burkina Faso having treated the polymorphism of the receptors of transforming growth factors beta (TGFβRI and TGFβRII) with keloids. It allowed us to characterize four (4) polymorphisms including rs111854391, rs121918710 of TGFβRI gene and rs104893807, rs28934568 of TGFβRII gene. The mean age of the study population was relatively young (34 ± 15 years) with a predominance of the 19 to 29 age group (36.2%) and had more than 3 keloid sites on their bodies. Similar results were found in other studies (31.3 ± 13 years) in Togo16 and Cameroon (≥25 years).17 Young people seem to be more at risk of developing a keloid and this is because they are more exposed to various skin traumas, leading to lesions that can result in keloids, and also due to the fact that skin tension at these ages is at its maximum.18 Indeed, skin tension is directly related to the quantity of elastic and collagen fibers in the dermis; a recurrence of trauma would solicit more elastic fibers and therefore lead to the accumulation of extracellular matrix (ECM) constituents and consequently contribute to the occurrence of keloids. The Mossi ethnic group was in the majority. This predominance reflects the ethnic distribution of the population of Burkina Faso, of which 40% are Mossi. We also observed that 16.3% of the study population had parents of different ethnicities. This indicates the existence of cohesion and inclusion of all ethnic groups in Burkina Faso, which represents a cultural wealth for the country. The predominance of patients with a family history of keloids (48.9%) corroborates the existence of a genetic predisposition to the occurrence of keloids.19,20 In contrast, family history was found in only 22.4% of a study population of students.11 Results from other countries show much lower rates of family history including 2.3% in the Democratic Republic of Congo21 and 21.9% in Togo.22 This predominance has also been observed in studies conducted in Nigeria and Benin with frequencies of 26.5% and 34.53%, respectively.17,23 Indeed, the pre-sternal location is still today the most associated with spontaneous keloid.24 The patients in our study were predominantly of blood group O. This predominance was also reported by Mouhari-Touré and al. in 2012 and Nangole et al in 2021 in Kenya.22,25 On the other hand, blood group A predominance has been reported in South India26 and Syria.27 The study conducted in Syria also showed a significant association between blood type A and keloid occurrence. This could be justified by the fact that blood group antigens would facilitate intracellular uptake signal transduction or adhesion through the organization of membrane microdomains.28 Mossi ethnicity, medical or surgical history, and familial history were associated with the number of keloids location. Most of them presented at least 3 keloids location in their body. A study also reported large areas of the body affected by keloids in patients29 suggesting the keloid formation in most part of the body. Keloid formation mainly occurs in parts of the body with high concentrations of melanocytes and is rare on the soles of the feet and palms of the hands where melanocyte concentration is minimal.30
Genotyping of the different variants of the study genes revealed some peculiarities. The entire study population was heterozygotes (TG) so presented the mutated allele (G) for the TGFβI rs121918710 polymorphism. This result corroborates that of Loeys et al in 2005 who reported that patients with Marfan syndrome, a disorder of the extracellular matrix (ECM), were heterozygous and that the mutated allele was absent in family members without the disease. This missense mutation could be responsible for the disruption of extracellular matrix homeostasis due to abnormal signaling through these receptors.31 This is evidenced by other results obtained by Loeys et al, who found in heterozygous patients diagnosed with Marfan syndrome an accumulation of connective tissue collagen, which is also characteristic of keloid tissue.32 Furthermore, the identification of 100% heterozygosity for TGFβRI rs121918710 may be a population-specific variant and have implications for autosomal dominant inheritance. Indeed, a study reported that the pattern of inheritance in families was consistent with an autosomal dominant mode with incomplete clinical penetrance and variable expression.29 This could explain why, in our findings, family history was not associated with keloid occurrence. In contrast, for the TGFβRI rs111854391 and TGFβRII rs104893807 polymorphisms, only 0.71% of the study subjects (ie 1/141) carried mutated alleles. These polymorphisms might not be related to the occurrence of keloids. For the TGFβRII rs28934568 polymorphism, 31.21% of the study population was heterozygous (TC). Interestingly, our findings show the absence of mutated homozygotes genotypes across all four studied SNPs. This finding is consistent with previous literature reporting a low frequency of the mutated allele in similar cohorts.14 The paucity of mutated homozygotes suggests that the investigated TGF-β polymorphisms may exert their influence primarily through a heterozygous effect or that the mutated allele is subject to strong evolutionary constraints in this population, precluding the high-frequency emergence of homozygous genotypes. This is consistent with previous studies on the presence of this polymorphism in populations with extracellular matrix disorders such as Marfan syndrome.33,34 Note that the polymorphisms in our study are all located in the kinase zone of the beta growth factor receptors, which are proteins with kinase activity. Therefore, any qualitative modification could have an impact on the functions of these growth factors. The association of the rs28934568 polymorphism, age, profession, ethnicity, medical or surgical history, and family history with the number of keloids explains the plurality of factors favoring the occurrence of keloids.
Analysis of the risks of keloid occurrence showed that only Mossi ethnicity had more than 8 times the risk of developing keloids (p=0.030; OR=8.66 (95% CI: 1.230–60.902). This result differs from that of Kouotou et al in Cameroon in 2019, who reported that patients with familial history had more than 4 times the risk of developing keloids.17 This difference could be due to the fact that the parameter “ethnicity” was not considered in the study population in Cameroon. Thus, the lack of association between family history and the occurrence of keloids in our study would justify the “incomplete clinical penetrance and variable expression” character attributed to the mode of inheritance proposed for keloids.35,36 Further large-scale studies would therefore be required to test this hypothesis. Also, conducting a study with a control population would allow for better comparisons and explanation of our results. Our study is limited to the hospital level and might not perfectly represent the entire population of Burkina Faso. In addition, the data collected only from people with keloids do not allow us to truly associate the polymorphisms and risk factors taken into account in this study with the occurrence of keloids.
Conclusion
Our study characterized for the first time in Burkina Faso the polymorphisms of the TGFβRI gene and the TGFβRII gene that appear to be involved in the occurrence of keloid scars. All patients in our study carried the T mutated allele of the rs12191870 polymorphism of the TGFβRI gene and the Mossi ethnic group was at the highest risk of developing keloid scarring in Burkina Faso. Further studies with a larger population and including control group would be important to better understand the implications of these polymorphisms.
Acknowledgments
The authors thank all clinical and administrative staff of the hospitals for their authorization and support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by L’OREAL Research and Innovation. France. The funding contributed to the purchase of reagents and consumables.
Disclosure
The authors declare no competing interest in this work.
References
1. Zhang T, Wang X-F, Wang Z-C, et al. Current potential therapeutic strategies targeting the TGF-β/Smad signaling pathway to attenuate keloid and hypertrophic scar formation. Biomed Pharmacother. 2020;129:110287. doi:10.1016/j.biopha.2020.110287
2. Bran GM, Goessler UR, Hormann K, Riedel F, Sadick H. Keloids: current concepts of pathogenesis (Review). Int J Mol Med. 2009;24(3):283–10.
3. Tsai C-H, Ogawa R. Keloid research: current status and future directions. Scars Burns Healing. 2019;5:2059513119868659. doi:10.1177/2059513119868659
4. Carmassi M, Eraud J, Gonelli D, et al. Cicatrices chéloïdes: étude d’une série de cas. Ann Pathol. 2015;35(2):148–153. doi:10.1016/j.annpat.2014.10.007
5. Limandjaja GC, Niessen FB, Scheper RJ, et al. The keloid disorder: heterogeneity. histopathology. mechanisms and models. Front Cell Dev Biol. 2020;8:360. doi:10.3389/fcell.2020.00360
6. Walsh LA, Wu E, Pontes D, et al. Keloid treatments: an evidence-based systematic review of recent advances. Syst Rev. 2023;12(1):42. doi:10.1186/s13643-023-02192-7
7. Shih B, Bayat A. Genetics of keloid scarring. Arch Dermatol Res. 2010;302(5):319–339. doi:10.1007/s00403-009-1014-y
8. Boui M, Lemnaouer A. Dermatological experience at the Moroccan mobile field hospital in Brazzaville. Congo. Med Trop. 2009;69(1):13–17.
9. Pitché P, Kombaté K, Barruet K, et al. Giant cheloid scars. Ann Dermatol Venereol. 2000;127(3):333.
10. Adegbidi H, Atadokpede F, Do Ango-Padonou F, et al. Keloid acne of the neck: epidemiological studies over 10 years. Int J Dermatol. 2005;44(s1):49–50. doi:10.1111/j.1365-4632.2005.02815.x
11. Traoré A, Korsaga/Somé N, Zoungrana/Ouédraogo A. Keloids and hypertrophic scars in secondary school in the city of Ouagadougou (Burkina Faso). Our Dermatol Online. 2019;10(e):e321–e328. doi:10.7241/ourd.2019e.32
12. Jagadeesan J, Bayat A. Transforming growth factor beta (TGFbeta) and keloid disease. Int J Surg. 2007;5(4):278–285. doi:10.1016/j.ijsu.2006.04.007
13. Dong X, Gao M, Guo H, et al. The regulatory role of immune microenvironment-related cells and pathways in the pathogenesis of keloids. Front Immunol. 2025;16:1529564. doi:10.3389/fimmu.2025.1529564
14. Bayat A, Bock O, Mrowietz U, et al. Genetic susceptibility to keloid disease: transforming growth factor beta receptor gene polymorphisms are not associated with keloid disease. Exp Dermatol. 2004;13(2):120–124. doi:10.1111/j.0906-6705.2004.00165.x
15. Ghazawi FM, Zargham R, Gilardino MS, et al. Insights into the pathophysiology of hypertrophic scars and keloids: how do they differ? Adv Skin Wound Care. 2018;31(1):582–595. doi:10.1097/01.ASW.0000527576.27489.0f
16. Mouhari-Toure A, Saka B, Kombaté K, et al. Is there an association between keloids and blood groups? Int Sch Res Notices. 2012;2012(1):750908.
17. Kouotou EA, Nansseu JR, Omona Guissana E, et al. Epidemiology and clinical features of keloids in Black Africans: a nested case–control study from Yaoundé. Cameroon. Int J Dermatol. 2019;58(10):1135–1140. doi:10.1111/ijd.14610
18. Bayat A, Walter JM, Bock O, et al. Genetic susceptibility to keloid disease: mutation screening of the TGFbeta3 gene. Br J Plast Surg. 2005;58(7):914–921. doi:10.1016/j.bjps.2005.04.009
19. Brown JJ, Ollier W, Arscott G, et al. Genetic susceptibility to Keloid scarring: SMAD gene SNP frequencies in Afro-Caribbeans. Exp Dermatol. 2008;17(7):610–613. doi:10.1111/j.1600-0625.2007.00654.x
20. Trace AP, Enos CW, Mantel A, et al. Keloids and Hypertrophic Scars: a Spectrum of Clinical Challenges. Am J Clin Dermatol. 2016;17(3):201–223. doi:10.1007/s40257-016-0175-7
21. Kibadi K. Deuxième piercing auriculaire à but esthétique et apparition de cicatrices pathologiques chez les négroïdes: à propos de 172 observations dans une zone endémique de chéloïdes. Ann Chir Plast Esthet. 2021;66(1):42–51. doi:10.1016/j.anplas.2020.07.004
22. Mouhari-Toure A, Saka B, Kombaté K, et al. Is there an association between keloids and blood groups? ISRN Dermatol. 2012;2012:1–4. doi:10.5402/2012/750908
23. Yedomon GH, Adegbidi H, Atadokpede F, et al. Keloids on dark skin: a consecutive series of 456 cases. Med Sante Trop. 2012;22(3):287–291. doi:10.1684/mst.2012.0052
24. Petit A. Histoire de la chéloïde. Ann Dermatol Venereol. 2016;143(1):81–95. doi:10.1016/j.annder.2015.11.008
25. Nangole FW, Ogeng’o J, Agak G, et al. Blood group and human leucocyte antigen sub-type as determinants to keloid formation and recurrence in keloid patients. J Dermatol Res. 2021;2(3):1–10.
26. Ramakrishnan KM, Thomas KP, Sundararajan CR. Study of 1.000 patients with keloids in south India. Plast Reconstr Surg. 1974;53(3):276–280. doi:10.1097/00006534-197403000-00004
27. Shaheen A, Khaddam J, Kesh F. Risk factors of keloids in Syrians. BMC Dermatol. 2016;16(1):13. doi:10.1186/s12895-016-0050-5
28. Cooling L. Blood groups in infection and host susceptibility. Clin Microbiol Rev. 2015;28(3):801–870. doi:10.1128/CMR.00109-14
29. Marneros AG, Norris JE, Olsen BR, Reichenberger E. Clinical genetics of familial keloids. Arch Dermatol. 2001;137(11):1429–1434. doi:10.1001/archderm.137.11.1429
30. Eryilmaz T, Uygur S. Keloids: a rare location and review of the literature. European J Plast Surg. 2010;33(4):221–223. doi:10.1007/s00238-010-0404-x
31. Adès LC, Sullivan K, Biggin A, et al. FBN1. TGFBR1. and the Marfan-craniosynostosis/mental retardation disorders revisited. Am J Med Genet A. 2006;140(10):1047–1058. doi:10.1002/ajmg.a.31202
32. Loeys BL, Chen J, Neptune ER, et al. A syndrome of altered cardiovascular. craniofacial. neurocognitive and skeletal development caused by mutations in TGFBR1 or TGFBR2. Nat Genet. 2005;37(3):275–281. doi:10.1038/ng1511
33. Mizuguchi T, Collod-Beroud G, Akiyama T, et al. Heterozygous TGFBR2 mutations in Marfan syndrome. Nat Genet. 2004;36(8):855–860. doi:10.1038/ng1392
34. Kirmani S, Tebben PJ, Lteif AN, et al. Germline TGF-β receptor mutations and skeletal fragility: a report on two patients with Loeys-Dietz syndrome. Am J Med Genet. 2010;152(4):1016–1019. doi:10.1002/ajmg.a.33356
35. Marneros AG, Norris JEC, Watanabe S, et al. Genome scans provide evidence for keloid susceptibility loci on chromosomes 2q23 and 7p11. J Invest Dermatol. 2004;122(5):1126–1132. doi:10.1111/j.0022-202X.2004.22327.x
36. Chen Y, Gao J-H, Liu X-J, et al. Characteristics of occurrence for Han Chinese familial keloids. Burns. 2006;32(8):1052–1059. doi:10.1016/j.burns.2006.04.014
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.