")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 12
Genetic polymorphisms of CYP3A5, CHRM2, and ZNF498 and their association with epilepsy susceptibility: a pharmacogenetic and case–control study
Authors AL-Eitan LN , Al-Dalalah IM, Mustafa MM , Alghamdi MA , Elshammari AK, Khreisat WH , Al-Quasmi MN , Aljamal HA
Received 16 April 2019
Accepted for publication 22 August 2019
Published 4 September 2019 Volume 2019:12 Pages 225—233
DOI https://doi.org/10.2147/PGPM.S212433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Laith N AL-Eitan1,2, Islam M Al-Dalalah1, Mohamed M Mustafa3, Mansour A Alghamdi4, Afrah K Elshammari5, Wael H Khreisat5, Mohammed N Al-Quasmi6, Hanan A Aljamal1
1Department of Applied Biological Sciences, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Biotechnology and Genetic Engineering, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Neuroscience, Jordan University of Science and Technology, Irbid, Jordan; 4Anatomy Department, College of Medicine, King Khalid University, Abha, Saudi Arabia; 5Department of Pediatric Neurology, Queen Rania Hospital for Children, King Hussein Medical Center, Royal Medical Services, Amman, Jordan; 6Department of Medical Laboratory, King Abdullah University Hospital, Irbid, Jordan
Correspondence: Laith N AL-Eitan
Jordan University of Science and Technology, P.O. Box 3030, Irbid 22110, Jordan
Tel +962 2 720 1000 Ext.:23464
Fax +962 2 720 1071
Email [email protected]
Background: A total of 50 million persons were diagnosed worldwide with epilepsy. One-third of them are experiencing debilitating seizures despite optimum anti‐epileptic drugs (AEDs) treatment. Several studies have suggested that CYP3A5, CHRM2, and ZNF498 influence the pharmacokinetics of AEDs. Therefore, the severity of the disease as well as the degree of response to the AEDs could be affected by the genetic polymorphisms within these genes.
Objectives: In this study, we assessed the effect of certain single nucleotide polymorphisms (SNPs) within CYP3A5, CHRM2, and ZNF498 genes on the susceptibility to develop epilepsy and the responsiveness to AEDs treatment.
Methods: A case–control and pharmacogenetic study was conducted on samples of 299 healthy individuals in addition to 296 epileptic patients. Genotypic, allelic, and clinical data association were performed for the selected polymorphisms within the (rs324649, rs420817, rs15524, and rs1859690) in the Jordanian population.
Results: The analysis revealed no significant association of the investigated SNPs with epilepsy in general, partial and generalized epilepsy as well as drug responsiveness. CYP3A5 and ZNF498 were associated with family history (P=0.003 and P=0.002, respectively) and the classification of epilepsy for the ZNF498 variant (P=0.009). On the other hand, CHRM2 was not linked to either disease severity or treatment responsiveness.
Conclusion: Our results failed to confirm the association of CYP3A5, ZNF498, and CHRM2 variants with either disease development or treatment response. Clinical pharmacogenetic studies may contribute to treatment personalization, appropriate drug dose selection, minimizing drug adverse reactions, increasing drug efficacy, and reducing the costive burdens.
Keywords: epilepsy, seizures, cytochrome P-450 CYP3A, pharmacogenetics, humans, anti-epileptic drugs
Introduction
Epilepsy is a chronic neurological disorder with a prevalence of 0.6–1.0% and an incidence of 50–120/100.000 individuals per year.1–4 Epilepsy characterized by uncontrolled electrical activity produced by a group of neurons.5,6 It can be caused by different etiologies such as metabolic disorders and structural brain abnormalities in addition to idiopathic epilepsies which are caused mostly by genetic factors.7 Therefore, International League Against Epilepsy (ILAE) classified epilepsy into two main categories; generalized and partial.4,8,9
Despite the enormous progress that has been made in the field of epilepsy and the introduction of new antiepileptic drugs (AEDs), it still impossible to achieve complete remission in some patients.10–12 Explanations for this condition is uncertain where it seems that the genetic basis may be implicated in epilepsy diagnosis and treatment.12 The outcome of AEDs treatment varies even between patients who have the same syndromes.10 In addition, 20% to 25% of the epileptic patients have a poor response to AEDs.6 This is mostly affected by many factors such as gender, age, weight, smoking, co-medications, heterogeneity in the disease, nutritional status, liver and kidney function, and/or genetic variants.5,9
Pharmacokinetics and pharmacodynamics of AEDs is mostly mediated by the cytochrome P450 (CYP) family that encoding isoforms of different activities. Response to AEDs varies greatly according to the interindividual variability.13 The human CYP3A gene cluster encodes CYP subfamily enzymes that catalyze the metabolism of many exogenous and endogenous chemicals including more than 50% of the commercially available drugs. CYP3A5 is an isoform of CYP3A with a polymorphic expression that implicated in disease risk and drug metabolism.14
Carbamazepine (CBZ) is one of the first-line drugs for partial seizures and can be used also for generalized seizures.8,10,15 CBZ is usually used as monotherapy or combined with other AEDs such as valproic acid (VPA).16–18 Moreover, 95% of the CBZ is metabolized by the liver; CYP3A4 and CYP3A5 are the most common enzymes that convert CBZ to CBZ-10, 11-epoxide (CBZ-E) in the major pathway of CBZ metabolism.19 CYP3A5 along with 888 other enzymes belongs to the CYP enzymes that encoded by 57 human genes, including zinc finger protein 498 (ZNF498) whose products are involved mainly in oxidative drug metabolism.20,21 Zinc finger proteins are of the mostly abundant proteins in the eukaryotic. These proteins provide extraordinarily diverse functions including DNA recognition, RNA packaging, transcriptional activation, apoptosis regulation, binding of lipid, protein folding and assembly, binding interactions in proteins, DNA, and RNA, and gene regulation (inhibition or activation).22,23 For the CHRM2 gene, it belongs to a family of G-protein-coupled receptors (GPCRs), which involved in signaling pathways that are important for regulation of acetylcholine (ACh) release, modulating neuronal excitability, synaptic plasticity, and feedback.24–26
Therefore, this study aimed to investigate the association of CHRM2 (rs324649 and rs420817), CYP3A5 (rs15524), and ZNF498 (rs1859690) variants with the susceptibility of epilepsy development and the responsiveness to AED treatments among the Jordanian population.
Materials and methods
Patients and data collection
Jordanian participants including 299 healthy controls and 296 epileptic patients with an age range from neonate up to 15 years of life. This research was conducted in accordance with the Declaration of Helsinki 1975, as revised in 2013 and the study protocol was approved by the Ethics Committee at Jordan University of Science and Technology (16/111/2017). In addition, written informed consent was provided by the parents or legal guardians of the participants. All patients were recruited from the Pediatrics Department, Queen Rania Al-Abdullah Center (QRAC) in the Jordanian Royal Medical Services (JRMS). Selection criteria included all patients that were using antiepileptic medications in the period between October 2017 and January 2018, regardless of whether it was monotherapy or combination therapy. Patients who have progressive and degenerative neurological diseases, systemic diseases (including liver and kidney dysfunction), lack records, unreliable seizure frequency, poor compliance with AEDs, did not visit the clinics regularly, and/or do not agree to be enrolled were excluded. Standardized questionnaires were used to collect clinical and demographic data (Table S1).
According to the international classification of epilepsy, we divided the patients into patients with partial-onset seizures and generalized-onset seizures. Epileptic patients were also classified into patients with good response (ie, patients who have not experienced any type of seizures for a minimum of 3 months after receiving AEDs) and poor responder patients (drug-resistant), who have uncontrolled seizures over the same period. The AEDs were selected according to the seizure type and epilepsy syndrome. Informative details about the selected population, study design, and treatment approach were previously published as this study is a continuation of an extended study by AL-Eitan et al.27
DNA genotyping and analysis
Genomic DNA was extracted from EDTA blood samples (Promega DNA Blood Kit, Madison, WI, USA) according to the manufacture’s procedure. Samples that completed the quantitative requirements and passed DNA integrity test that met with the multiplexing requirements of the SNPs for genotyping were sent to the Australian Genome Research Facility (AGRF, Melbourne Node, Melbourne, Australia). Genotyping of the single nucleotide polymorphisms (SNPs) of CHRM2 (rs324649 and rs420817), CYP3A5 (rs15524), and ZNF498 (rs1859690) were performed with the Sequenom MassARRAY® system (iPLEX GOLD) (Sequenom, San Diego, CA, USA) at the AGRF according to the manufacturer’s recommendations (Sequenom, San Diego, CA, USA) where variants were selected from public databases such as the National Center for Biotechnology Information (NCBI) (http://www.ncbi.nlm.nih.gov/SNP/), Ensembl (http://www.ensembl.org/index.html), and the Applied Biosystems (http://www.appliedbiosystems.com).
The protocol of Sequenom MassARRAY® system was run into five steps including template amplification, dephosphorylation, single base extension (SBE) reactions, sample conditioning, transfer and genotype calling, and bioinformatics. Briefly, these steps started with the amplification of the genomic DNA by polymerase chain reaction (PCR) followed by removing of the unincorporated dNTPs by using shrimp alkaline phosphatase (SAP) enzyme (Sequenom, San Diego, CA, USA). SBE Reactions include a single base extension primer (SBE) enable iPLEX reactions with modified masses related with the termination mixture. Differences in the mass of the extension product used to differentiate the allelic variant. Sample conditioning and transfer were provided to improve the analysis of mass spectrometry by eliminating redundant salts that interfere with it. The information is then presented in type analyzer software (Sequenom Inc., 2003 and 2004).
Genotypic, allelic, and clinical data association were analyzed using the Statistical Package for the Social Sciences (SPSS), version 25.0 (SPSS, Inc., Chicago, IL).
Genotype–phenotype correlation
The distribution of genotypes in patients and the association between the studied variants and several clinical variables (independent variables) were investigated. Clinical and pathological information were included according to the patients’ medical records: gender, age, age at onset of seizure, types of seizures, response to medications, being on either single or combined therapy in addition to history of febrile seizure, psychosis, suicidal thoughts or actions, epilepsy syndromes, response to first drug, as well as family history and classification of epilepsy.
Correction for multiple testing
The target alpha level (0.05/Nem) was calculated by applying the modified Bonferroni procedure where the effective number of SNPs (Nem) was estimated according to the Li and Ji method.28 The overall significance level is set to be 0.0125 or less.
Results
Among the 296 epileptic patients and 299 healthy individuals, the average age was 7.1±4.1 and 5.94±3.7 years (mean±SD), respectively (Table 1). Around half of the controls were males in compare to 54.8% in the patients’ group. No differences revealed in the distributions of the selected SNPs in both the controls and patients (Table 2). In ZNF498 (rs1859690), the AG+GG frequency in patients was 13.2% compared to 20.1% in control group. In addition, epileptic patients were further classified into 172 with generalized epilepsy (GE) and 124 with partial epilepsy (PE). As shown in Table 3, none of the CYP3A5, CHRM2, and ZNF498 variants were linked to the increased risk of developing GE as well as PE. Notably, the frequency of rs15524 and rs1859690 GG genotype in the GE was lower than that in controls [0.6% vs 3.4%, P=0.034 and 0.6% vs 3.3%, P=0.034, respectively]. As in the case of GE, PE has shown no linkage with the included SNPs (Table 4).
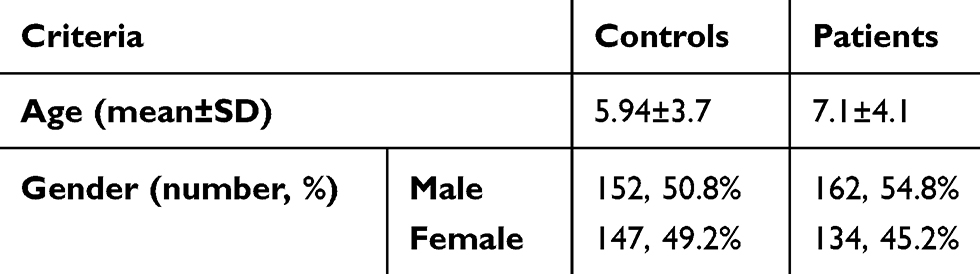 |
Table 1 Gender and age-matched distribution in the epileptic patients (n=296) and the control individuals (n=299) |
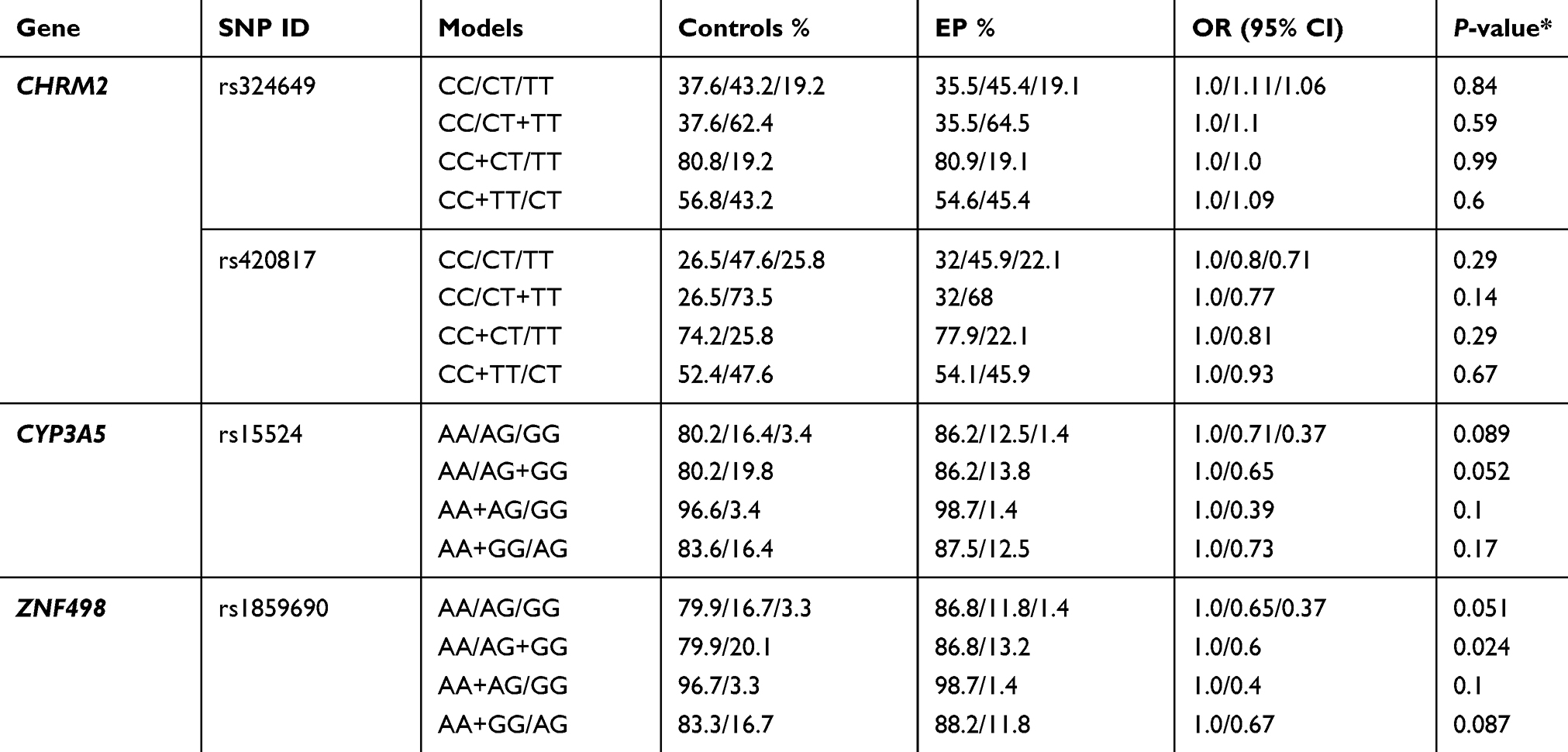 |
Table 2 The association of CHRM2, CYP3A5, and ZNF498 polymorphisms in epileptic patients (EP) (n=296) and control individuals (n=299) |
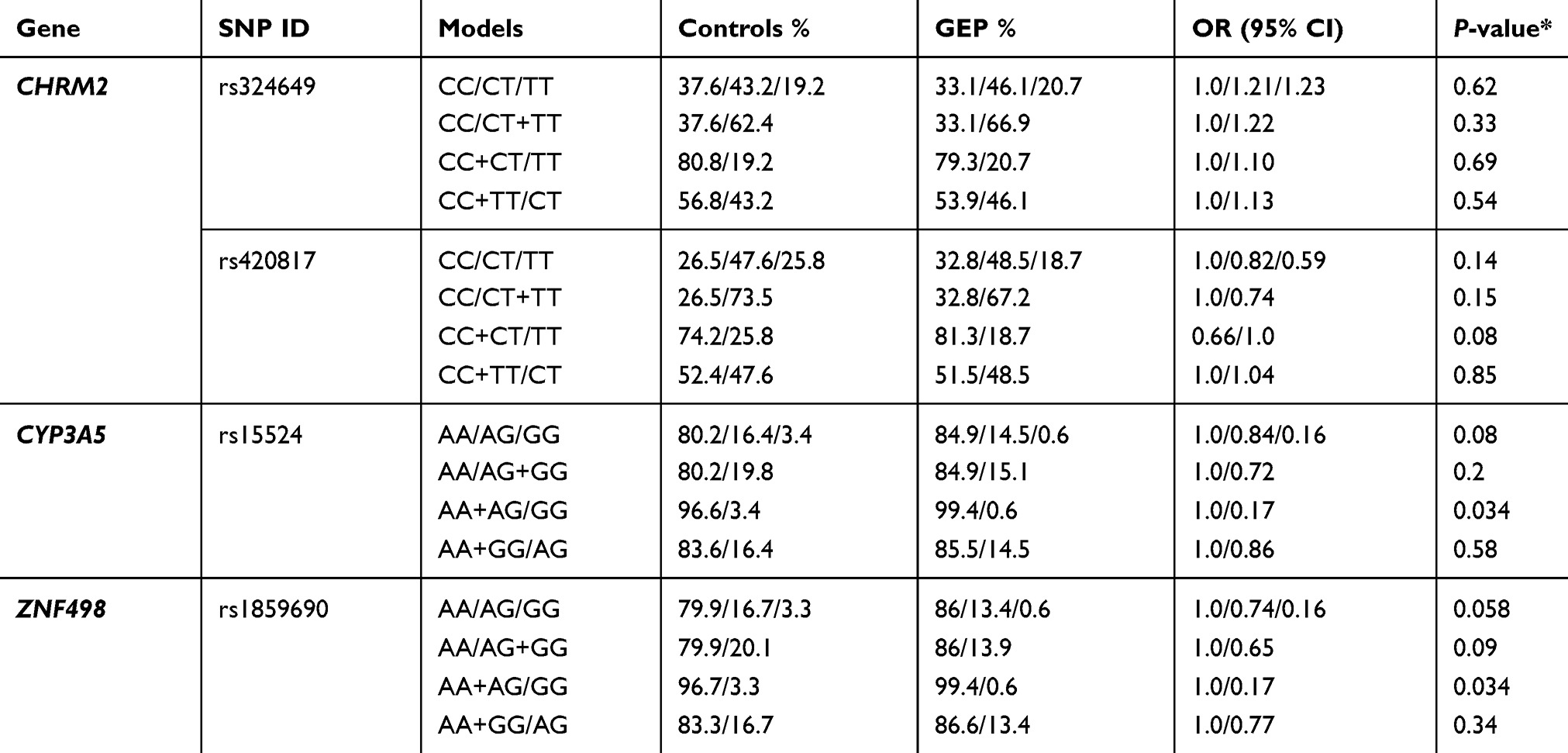 |
Table 3 The association of CHRM2, CYP3A5, and ZNF498 polymorphisms in generalized epilepsy patients (GEP) (n=172) and control individuals (n=299) |
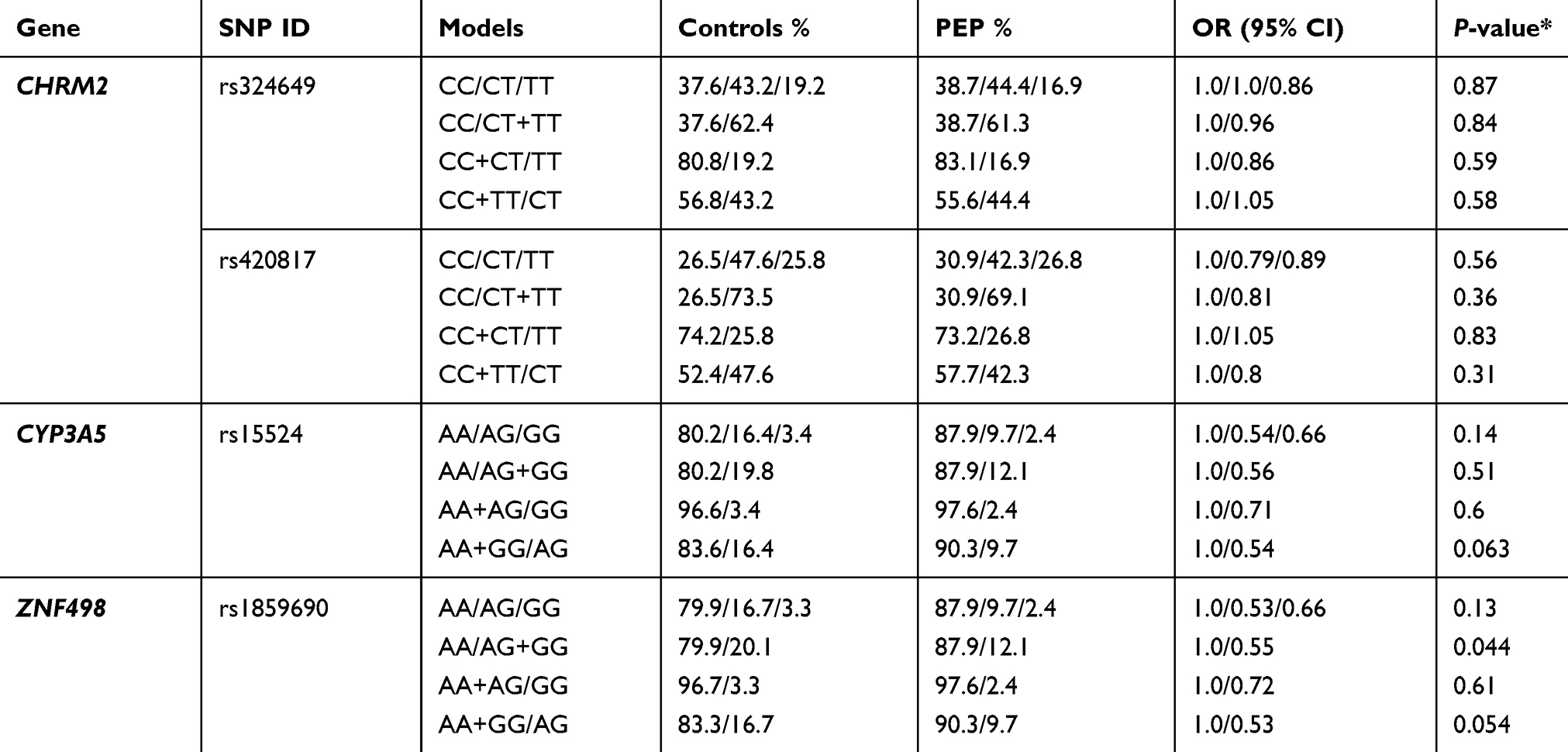 |
Table 4 The association of CHRM2, CYP3A5, and ZNF498 polymorphisms in partial epilepsy patients (PEP) (n=124) and control individuals (n=299) |
The distributions of the four SNPs (rs324649, rs420817, rs15524, and rs1859690) were analyzed in 171 poor responder and 124 good responder patients that were classified according to their response to the AEDs as previously mentioned in AL-Eitan et al study.29 CHRM2 (rs324649) variant was of a nominal significance (not statistically significant, but it is in the borderline) in poor responder patients (P=0.012) (Table 5). Nevertheless, there was no association between AEDs responsiveness and the investigated genotypes (Table 5).
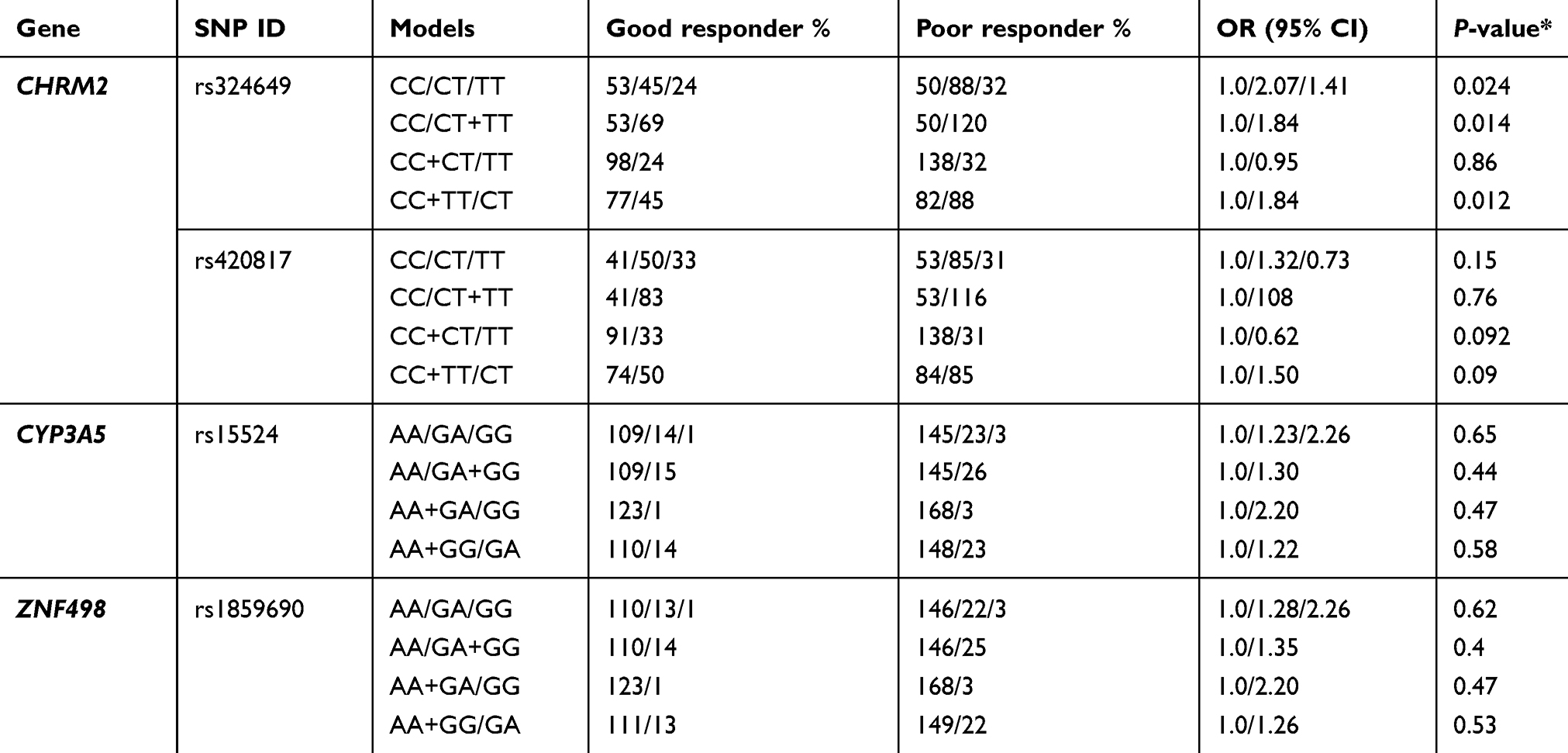 |
Table 5 The association of ZNF498, CYPA5, and CHRM2 SNPs in good responder (n=124) and poor responder (n=171) patients |
Finally, certain pathological and clinical manifestation were assisted for further correlation, revealed no relationship between response to the first drug (ie, 10 mg/kg of VPA for patients diagnosed with GE or 5 mg/kg daily of CBZ for patients diagnosed with PE) and the included SNPs (Table 6). In CYP3A5, it was correlated with family history of epilepsy and the classification of epilepsy (ie, which is being either idiopathic, symptomatic, or cryptogenic) (P=0.003 and 0.009, respectively) (Table 6). Moreover, ZNF498 was also of a linkage with family history (P=0.002) (Table 6). Haplotypes association of the CHRM2 gene was conducted and failed to provide any linkage with epilepsy, its subtypes, and response to the treatment (Table S2, S3, S4, and S5). Sequenom MassARRAY scatter plot for the investigated SNPs is shown in Figure 1, that was stained for different genotype calls where GG (green), GA (yellow) and AA (blue) and no call (red) in A and B figures, and CC (green), CT (yellow) and TT (blue) and no call (red) in C and D figures.
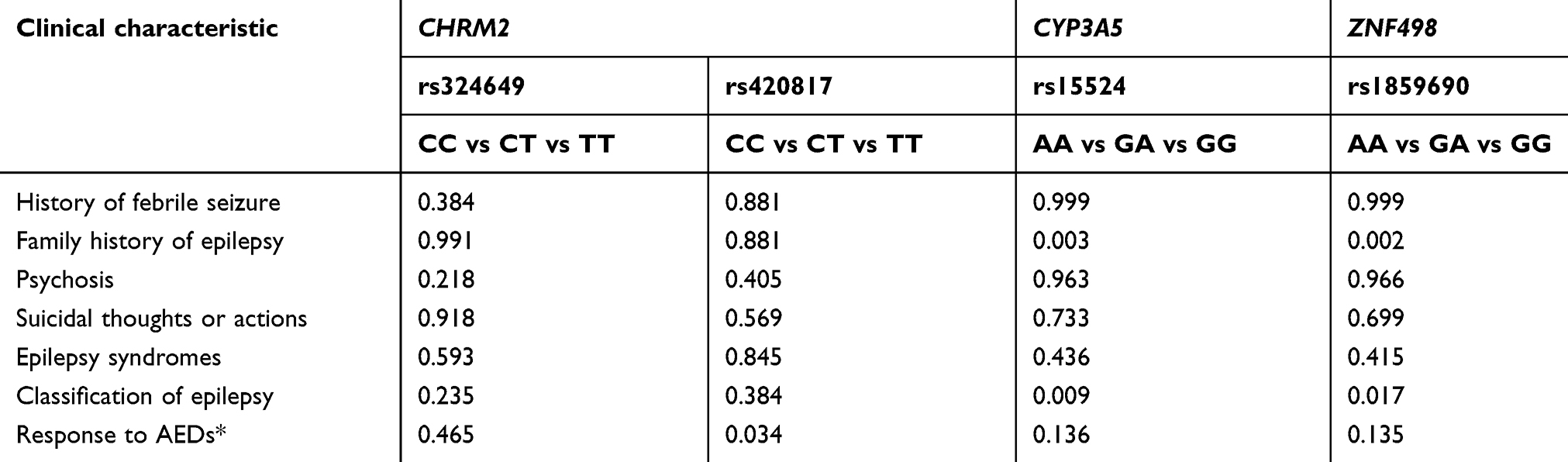 |
Table 6 The association between CHRM2 (rs324649 and rs420817), CYP3A5 (rs15524), and ZNF498 (rs1859690) and the clinical characteristics |
 |
Figure 1 Scatter plot from the sequenom data of the studied variants. The scatter plot illustrates rs159690 SNP within ZNF498 gene (A) rs15524 SNP within CYP3A5 (B) and rs420817 and rs324649 SNPs within CHRM2 (C and D, respectively). The X and Y axes denote mass measurements for the two alleles (G, A, low mass allele versus high mass allele) at the rs159690 and rs15524 (A and B, respectively). At (C) and (D) the X and Y axes denote mass measurements for the C, T (low mass allele versus high mass allele) at rs420817 and rs324649 SNPs. Every single sample is represented by one point. The points in the scatter plot are colored depending on the genotype calls. |
Discussion
Epilepsy is one of the most occurring diseases of the Central Nervous System (CNS) affecting children, with approximately 5% to 10% having a seizure during their first two decades of life and around 1% of them developing epilepsy. Childhood epilepsy is one of the major psychiatrists’ concern due to the associated behavioral problems that found to be of a prevalence of four times in compare to healthy children and two times in compare to children with non-CNS chronic diseases.30 Taking into account, that around 80% of people diagnosed with epilepsy were live in low to middle income countries where limited resources of diagnosis and treatment.31
There are five major categories of the genes that involve in the pharmacogenomic response to psychotropic drugs in CNS disorders. These genes could be associated with (1) CNS pathogenesis, (2) drug transporters, (3) drug metabolism, (4) drug mechanism of action, and (5) multifaceted cascades and metabolism reactions.32 According to Wang et al, the search in several databases resulted in 977 genes associated with epilepsy, its core symptoms, and syndromes.7
In this report, the frequency of particular polymorphisms in CYP3A5, ZNF498, and CHRM2 genes was investigated in epileptic patients as well as in the healthy individuals to evaluate the association of these variants with epilepsy susceptibility and treatment in Jordanians. This study showed that CYP3A5 (rs15524) lack of association with the susceptibility of epilepsy in general, generalized and partial subtypes. Based on the genotypic and allelic analysis, the frequency of GG genotype was six-fold lower in GE patients than in the healthy individuals where the AA genotype could be associated with epilepsy as the frequency was higher in epileptic patients. This hypothesize the possibility that the presence of G in the epileptic patients decreases the risk of GE in compare to A which increases the risk of PE but not confirmed. CYP3A5 polymorphism is unlikely seem to represent a risk factor for epilepsy development as well as on carbamazepine metabolism in Serbian pediatric epileptic patients. In consistence with this study, the variant allele frequencies of CYP3A5 did not differ significantly in other Caucasian populations such as Bosnian, Macedonian, Greek, Italian, Polish, British, Dutch, Finnish, Russian, and Australian.33
Regarding the association of rs1859690 within ZNF498o, there is a lack of data to the best of our knowledge. The AA genotype frequency was higher in patients suggesting that this genotype may act as a risk factor in epilepsy. On the other hand, AG+GG frequency was higher in controls compared with both partial and generalized epilepsy patients could indicate that the homozygous G or the heterozygous AG has low risk of epilepsy and may be considered as protective factor. This SNP needs further assessment in the future studies within Jordanian as well as other populations to confirm its exact role.
Carbamazepine is an anticonvulsant that frequently used as the first-line therapy for different forms of epilepsy in both adult and childhood.34,35 Pharmacogenetic analysis showed no significant differences between the selected variants and drug responsiveness. Moreover, there was no association between these SNP genetic haplotypes and drug resistance, contrasted with previous studies that showed an association of these genotypes with response to AEDs.18,19 CYP3A5 rs15524 was found to be related to the metabolism of the AEDs such as tacrolimus and carbamazepine;20,36,37 however, there is a lack of data regarding its association with epilepsy. Emich-Widera et al failed to confirm the association of CYP3A5 polymorphism with drug resistance in Caucasian children with epilepsy.15 This could be explained by the diversity in ethnicity and genetic background of the individuals since for most of the CYP enzymes, the same drug can be differentially metabolized as they exhibited an age, sex, and ethnic differences.32
Muscarinic cholinergic receptors system has been involved in the pathophysiology of some of psychiatric and neurological disorders such as schizophrenia, bipolar, major depressive, substance abuse, Alzheimer’s and Parkinson’s disease.38 CHRM2 variants did not show any statistically significant relationship with any of the epilepsies, AEDs response, and the studied clinical variables. The rs15524 of CYP3A5 was the only associated SNP with the classification of epilepsy. In addition, both CYP3A5 rs15524 and ZNF498 rs1859690 showed an association with the family history which can elicit the inheritance nature of this disease.
There are some limitations related to our investigation. First, SNPs and the selected genes were restricted to what already mentioned in the literatures, as there is limited information about these genes and their functionality. Second, the sample size was relatively small, and finally, the lack of ancestry informative marker data on our population. All these limitations require additional improvements in future investigations.
In conclusion, the genetic background of epilepsies is heterogeneous and there is a very limited genetic association. The benefits of clinical studies dose not only help in drugs development strategies, but also will help in developing preventive plans focusing on disease screening, seizure control, and treatment optimization.
Ethics approval and informed consent
All procedures contributing to this work complied with the ethical standards of the relevant national and institutional committees on human experimentation and the Declaration of Helsinki with an IRB no. 16/111/2017.
Data availability
The datasets generated and analyzed during the current study are not publicly available. The consent from participants did not cover data sharing but are available from the corresponding author on reasonable request.
Acknowledgment
This work was supported by the Deanship of Research at Jordan University of Science and Technology under grant number RN: 104/2017.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lopez-Garcia MA, Feria-Romero IA, Serrano H, et al. Influence of genetic variants of CYP2D6, CYP2C9, CYP2C19 and CYP3A4 on antiepileptic drug metabolism in pediatric patients with refractory epilepsy. Pharmacol Rep. 2017;69(3):504–511. doi:10.1016/j.pharep.2017.01.007
2. Bhalla D, Lotfalinezhad E, Timalsina U, et al. A comprehensive review of epilepsy in the Arab world. Seizure. 2016;34:54–59.
3. Bicalho MA, Sukys-Claudino L, Guarnieri R, Lin K, Walz R. Socio-demographic and clinical characteristics of Brazilian patients with epilepsy who drive and their association with traffic accidents. Epilepsy Behav. 2012;24(2):216–220.
4. Stafstrom CE, Carmant L. Seizures and epilepsy: an overview for neuroscientists. Cold Spring Harb Perspect Med. 2015;5(6).
5. Winkler AS, Kerschbaumsteiner K, Stelzhammer B, Meindl M, Kaaya J, Schmutzhard E. Prevalence, incidence, and clinical characteristics of epilepsy–a community-based door-to-door study in northern Tanzania. Epilepsia. 2009;50(10):2310–2313.
6. Cohen N. Pharmacogenomics and Personalized Medicine. Totowa, NJ: Humana Press; 2008:299.
7. Wang J, Lin ZJ, Liu L, et al. Epilepsy-associated genes. Seizure. 2017;44:11–20.
8. Allen NM, Conroy J, Shahwan A, et al. Unexplained early onset epileptic encephalopathy: exome screening and phenotype expansion. Epilepsia. 2016;57(1):e12–e17.
9. Henning O, Nakken KO. [New epilepsy classification]. Tidsskr Nor Laegeforen. 2017;137:23–24.
10. Genç F, Kutlu G, Gomceli YB, Inan LE. Demographic and clinical findings of patients with refractory epilepsy followed by the epilepsy department of the Ankara education and research hospital. Epilepsi. 2013;19(2):79–85. doi:10.5505/epilepsi.2013.68552
11. Piperidou C, Karlovasitou A, Triantafyllou N, et al. Association of demographic, clinical and treatment variables with quality of life of patients with epilepsy in Greece. Qual Life Res. 2008;17(7):987–996. doi:10.1007/s11136-008-9375-9
12. Dasgupta A. Handbook of Drug Monitoring Methods. Totowa, N.J.: Humana Press; 2008:211–223.
13. Balestrini S, Sisodiya SM. Pharmacogenomics in epilepsy. Neurosci Lett. 2018;667:27–39. doi:10.1016/j.neulet.2017.01.014
14. Cacabelos R, Martinez-Bouza R, Carril JC, et al. Genomics and pharmacogenomics of brain disorders. Curr Pharm Biotechnol. 2012;13(5):674–725.
15. Emich-Widera E, Likus W, Kazek B, et al. CYP3A5*3 and C3435T MDR1 polymorphisms in prognostication of drug-resistant epilepsy in children and adolescents. Biomed Res Int. 2013;2013:526837. doi:10.1155/2013/526837
16. Kartal A. Knowledge of, perceptions of, attitudes and practices regarding epilepsy among medical students in Turkey. Epilepsy Behav. 2016;58:115–118. doi:10.1016/j.yebeh.2016.02.042
17. Chen HF, Tsai YF, Hsi MS, Chen JC. Factors affecting quality of life in adults with epilepsy in Taiwan: a cross-sectional, correlational study. Epilepsy Behav. 2016;58:26–32. doi:10.1016/j.yebeh.2016.02.019
18. Meng H, Guo G, Ren J, Zhou H, Ge Y, Guo Y. Effects of ABCB1 polymorphisms on plasma carbamazepine concentrations and pharmacoresistance in Chinese patients with epilepsy. Epilepsy Behav. 2011;21(1):27–30. doi:10.1016/j.yebeh.2011.02.015
19. Yun W, Zhang F, Hu C, et al. Effects of EPHX1, SCN1A and CYP3A4 genetic polymorphisms on plasma carbamazepine concentrations and pharmacoresistance in Chinese patients with epilepsy. Epilepsy Res. 2013;107(3):231–237.
20. Wang P, Yin T, Ma HY, et al. Effects of CYP3A4/5 and ABCB1 genetic polymorphisms on carbamazepine metabolism and transport in Chinese patients with epilepsy treated with carbamazepine in monotherapy and bitherapy. Epilepsy Res. 2015;117:52–57.
21. Zhu X, Yun W, Sun X, Qiu F, Zhao L, Guo Y. Effects of major transporter and metabolizing enzyme gene polymorphisms on carbamazepine metabolism in Chinese patients with epilepsy. Pharmacogenomics. 2014;15(15):1867–1879.
22. Laity JH, Lee BM, Wright PE. Zinc finger proteins: new insights into structural and functional diversity. Curr Opin Struc Biol. 2001;11(1):39–46.
23. Isalan M; Zinc Fingers. Encyclopedia of Biological Chemistry. Elsevier Inc; 2013:575–579.
24. Szczepankiewicz A, Breborowicz A, Sobkowiak P, Kramer L, Popiel A. [Association of A/T polymorphism of the CHRM2 gene with bronchodilator response to ipratropium bromide in asthmatic children]. Pneumonol Alergol Pol. 2009;77(1):5–10.
25. Gosso FM, de Geus EJ, Polderman TJ, Boomsma DI, Posthuma D, Heutink P. Exploring the functional role of the CHRM2 gene in human cognition: results from a dense genotyping and brain expression study. BMC Med Genet. 2007;8:66.
26. Gosso MF, van Belzen M, de Geus EJ, et al. Association between the CHRM2 gene and intelligence in a sample of 304 Dutch families. Genes Brain Behav. 2006;5(8):577–584.
27. AL-Eitan LN, Al-Dalalah IM, Elshammari AK, Khreisat WH, Almasri AY. The impact of potassium channel gene polymorphisms on antiepileptic drug responsiveness in arab patients with epilepsy. J Pers Med. 2018;8(4).
28. Li J, Ji L. Adjusting multiple testing in multilocus analyses using the eigenvalues of a correlation matrix. Heredity. 2005;95(3):221–227.
29. AL-Eitan LN, Al-Dalalah IM, Mustafa MM, et al. Effects of MTHFR and ABCC2 gene polymorphisms on antiepileptic drug responsiveness in Jordanian epileptic patients. Pharmgenomics Pers Med. 2019;12:87–95.
30. Dunn DW, Austin JK. Behavioral issues in pediatric epilepsy. Neurology. 1999;53(5 Suppl 2):S96–S100.
31. Tamashiro EY, Felipe CR, Genvigir FDV, et al. Influence of CYP3A4 and CYP3A5 polymorphisms on tacrolimus and sirolimus exposure in stable kidney transplant recipients. Drug Metab Pers Ther. 2017;32(2):89–95.
32. Cacabelos R. Pharmacogenomics of Central Nervous System (CNS) drugs. Drug Dev Res. 2012;73(8):461–476.
33. Milovanovic DD, Radosavljevic I, Radovanovic M, et al. CYP3A5 polymorphism in serbian paediatric epileptic patients on carbamazepine treatment. Serbian J Exp Clin Res. 2015;16(2):93–99.
34. Magiorkinis E, Diamantis A, Sidiropoulou K, Panteliadis C. Highights in the history of epilepsy: the last 200 years. Epilepsy Res Treat. 2014;2014:582039.
35. Thorn CF, Leckband SG, Kelsoe J, et al. PharmGKB summary: carbamazepine pathway. Pharmacogenet Genomics. 2011;21(12):906–910.
36. Esterhuizen AI, Carvill GL, Ramesar RS, et al. Clinical application of epilepsy genetics in Africa: is now the time? Front Neurol. 2018;9:276.
37. Zhang X, Men T, Liu H, Li X, Wang J, Lv J. Genetic risk factors for post-transplantation diabetes mellitus in Chinese Han renal allograft recipients treated with tacrolimus. Transpl Immunol. 2018;49:39–42.
38. Scarr E. Muscarinic receptors: their roles in disorders of the central nervous system and potential as therapeutic targets. CNS Neurosci Ther. 2012;18(5):369–379.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.