")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 16
Genetic Polymorphism of NQO1 Influences Susceptibility to Coronary Heart Disease in a Chinese Population: A Cross-Sectional Study and Meta-Anaylsis
Authors Zhou YY, Sun JH, Wang L, Cheng YY
Received 26 May 2023
Accepted for publication 11 August 2023
Published 11 September 2023 Volume 2023:16 Pages 825—833
DOI https://doi.org/10.2147/PGPM.S420874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Ying-Yan Zhou,1,* Jing-Hua Sun,2,* Li Wang,1 Yan-Yan Cheng1
1Department of Cardiovascular Medicine, Haikou Third People’s Hospital, Haikou, 571700, People’s Republic of China; 2Department of Laboratory Medicine, First Medical Centre of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan-Yan Cheng, Department of Cardiovascular Medicine, Haikou Third People’s Hospital, Haikou, 571700, People’s Republic of China, Email [email protected]
Objective: The present study is to explore the association between NQO1 gene polymorphism and coronary heart disease (CHD) risk.
Methods: This research were selected 80 CHD patients as the observation group and 130 healthy people who participated in normal physical examination during the same period as the control group. NQO1 gene polymorphism was detected by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method. In addition, we conducted a meta-analysis to summarize the results of three relevant previously published adult population studies on the association between NQO1 gene polymorphism and coronary heart disease (CHD) risk.
Results: There were three genotypes (CC, CT, and TT) for NQO1 C609T polymorphism. The significant associations were found in TT genotype and T allele (all p< 0.05). Specifically, People with the TT genotype have 2.06 times CHD risk as those with the CC genotype. And People with the T allele have 1.62 times CHD risk as those with the C allele. No significant association was found by any genetic models in the meta-analysis (all p > 0.05).
Conclusion: NQO1 gene polymorphism increased the CHD risk in a Chinese population. Combined with individual gene polymorphism, the accuracy of risk assessment for CHD can be improved and individualized health education can be provided for CHD patients by nurses.
Keywords: NQO1, gene polymorphism, coronary heart disease, meta-analysis, nursing
Introduction
Coronary heart disease (CHD) is a common disease that seriously endangers human health and affects the quality of life. Previous studies have found that risk factors for CHD include unhealthy dietary habits, smoking, and hypertension, high cholesterol levels, obesity and overweight, etc. Genetic epidemiological studies show that the incidence of coronary heart disease is associated with genetic factors.1–6 Currently, it has been found that some gene polymorphisms affect the pathophysiological processes such as lipid metabolism, thrombosis, vasoconstriction and diastole, and are closely related to the increased risk of CHD.6–9 Studies have shown that oxidative stress and internal environmental instability play an important role in the occurrence and development of CHD.10–12 (NADPH: quinine oxidoreductase 1) NQO1 is an important opposite enzyme in the body. It is involved in the metabolism of internal and external substances through the deelectron reduction reaction, and is the key enzyme in the metabolism of benzene substances. Benzene metabolite has a strong teratogen effect and can be converted into hydroquinone with low toxicity and removed, which is recognized as a detoxification enzyme and cancer prevention enzyme.
The NQO1 gene was located in 16p22 and the total length was 20kb. There were single nucleotide polymorphisms in cDNA609 loci. The polymorphism of this site leads to the alteration of Proline/serine (Pro/Ser) at the 187 position of the encoded protein, which leads to the decrease of enzyme activity. With NADPH as the receptor, NQO1 can transfer the electrons of NADP or NADPH to quinones, resulting in a double electron reduction reaction to produce low-toxicity hydroquinones and avoids the damage to cells and reduces the carcinogenic risk of quinones. The NQO1 gene has several single nucleotide polymorphisms (SNPs), and NQO1 C609T is the one that has been the subject of the most research. The C-T allele in exon 609 (position 1) of the NQO6 gene has a base pair mutation known as the NQO1C609T (rs1800566, Pro187Ser) polymorphism. Position 187 of the encoded protein is changed by this mutation from proline to serine. Compared to the wild-type protein, this Pro187Ser mutant protein exhibits less quinine reductase activity.
Gene polymorphisms affect the function of NQO1 enzyme. Since genes have genetic polymorphisms, different genotypes have different physiological functions. In recent years, several studies have linked NQO1 gene polymorphisms to the risk of cardiovascular disease. It was shown that the C1T SNP in NQO609 was independently associated with coronary heart disease in a sex-dependent manner in the Iranian population.13 Another report claimed that the NQO1 rs1800566 T carrier genotype was associated with a higher risk of carotid atherosclerotic plaque formation in Korean subjects with type 2 diabetes.14 Thus, studying the relationship between gene polymorphisms and the occurrence of coronary heart disease has become a new and important topic in recent years. At present, findings on the association between NQO1 C609T polymorphism and CHD risk are rare, especially in China and the results of several reports are controversial.15,16 The present study is to further explore the association between NQO1 C609T polymorphism and CHD risk in Chinese population by experimental methods and meta-analysis.
Materials and Methods
Participants
There were 80 CHD patients, including 52 males and 28 females. All patients admitted to the Department of Cardiology from January 2020 to January 2023 met the World Health Organization criteria for naming and diagnosing ischemic heart disease. All patients had ≥50% stenosis of major vessels confirmed by coronary angiography. There were 130 cases in the control group, including 78 males and 52 females. The control group was selected from the hospitalized patients of the same period. All the enrolled patients were excluded from CHD diagnosis after a series of examinations including electrocardiogram, exercise plate, myocardial enzyme spectrum and coronary angiography. All the people in this study are Li nationality in Hainan, and there is no blood relationship between individuals. Diagnosis of coronary heart disease: During coronary angiography, the stenosis degree of right coronary artery, left anterior descending branch, left lateral branch and left main artery were evaluated. The presence of stenosis in each major branch was defined as a meaningful lesion and diagnosed as coronary heart disease.
Investigation of Coronary Heart Disease Risk Factors
The coronary atherosclerosis registration questionnaire was designed to record in detail the clinical manifestations, auxiliary examinations, laboratory results, risk factors and family history of CHD. The classic risk factors for CHD are defined according to the following criteria: hypertension was defined and diagnosed according to the 1999 standards of the World Health Organization and the International Society of Hypertension. Diabetes meets the 1997 diagnostic criteria for diabetes of the American Diabetes Association. Smoking refers to current smokers and former smokers who have quit.
Detection of Gene Polymorphism
Peripheral blood white blood cells were extracted by kit method and leukocyte genome was extracted. PCR restriction fragment length polymorphism (PCR-RFLP) was used to detect gene polymorphism. Primers were synthesized by Shanghai Shenggong Company. PCR reaction system, amplification conditions were all referred to published literatures.17–20
Meta-Analysis Process
The meta-analysis process included literature source, inclusion and exclusion criteria, data extraction and methodological quality assessment. The first author, second author and third author carefully and independently searched and reviewed relevant literatures by searching famous databases including PubMed, Cochrane, Embase, China Biomedicine Network, China National Knowledge Network, Wanfang and VIP database. The keywords were “NQO1”, “single nucleotide polymorphism” and “Coronary heart disease”. The inclusion and exclusion criteria were based on published literatures of meta-analysis. The first author and second author searched, reviewed all potential literatures and extracted all important information. All procedures were based on published meta-analysis literatures.21–34
Statistical Analysis
SPSS18.0 and STATA12.0 were responsible for the statistical analysis of experimental part and meta-analysis. The t-test and χ2 test were enrolled to process Measurement data and counting data. P < 0.05 was considered as significant.
Results
General Information of Study Subjects
Table 1 showed the details of general information of CHD group and control group. The general information included gender, age, smoking status, diabetes and hypertension status. No significant difference was observed between CHD group and control group (P > 0.05).
 |
Table 1 Participates Characteristics of Both CHD Group and Control Group |
Genotyping and Allele Distribution of NQO1 C609T Polymorphism
There were three genotypes (CC, CT, and TT) for NQO1 C609T polymorphism. The significant associations were found in TT genotype and T allele (all P < 0.05). The detailed information is shown in Table 2.
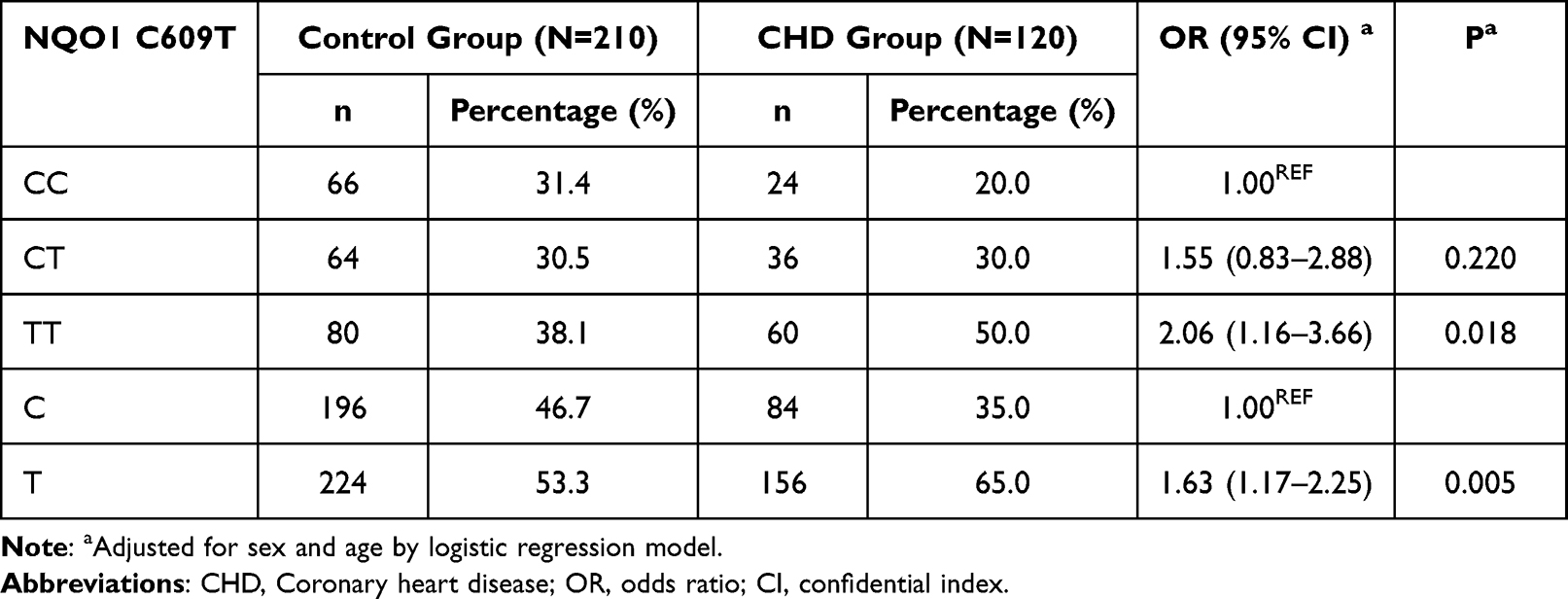 |
Table 2 Comparison of Genotype and Allele Frequency Between CHD Group and Control Group |
Characteristics of All Included Studies
According to our search strategy, three relevant studies were included in this meta analysis. The flow diagram of our meta-analysis is shown in Figure 1. Three literatures were enrolled and all information is listed in Table 3.13,15,16 All the literatures are from Asian population and conforming to HWE. The sample size and source of control were different. And the genotyping methods were PCR-RFLP.
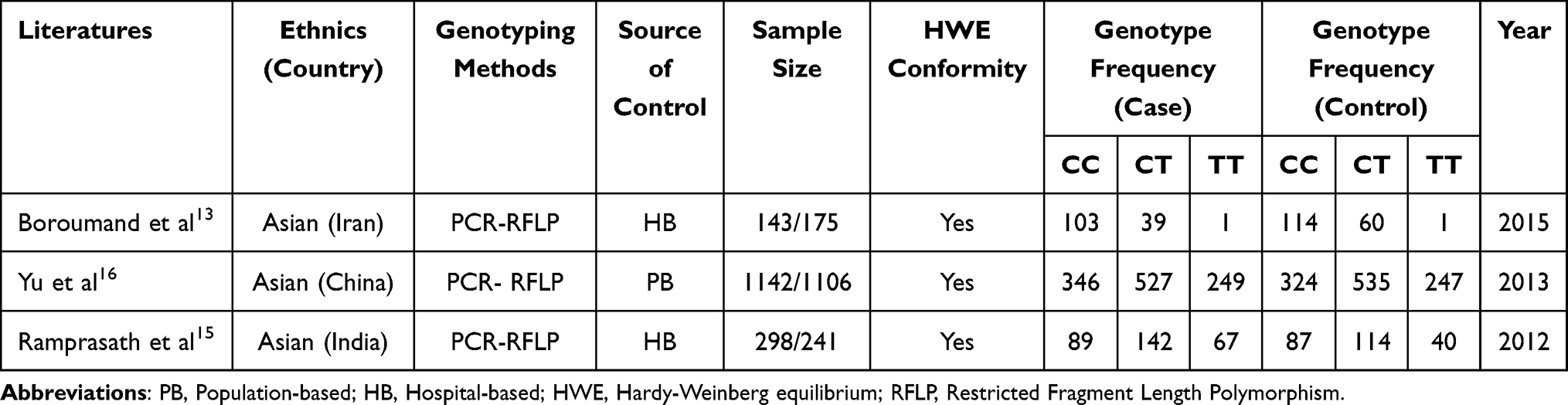 |
Table 3 Main Characteristics of All Case-Control Studies Included in Meta-Analysis |
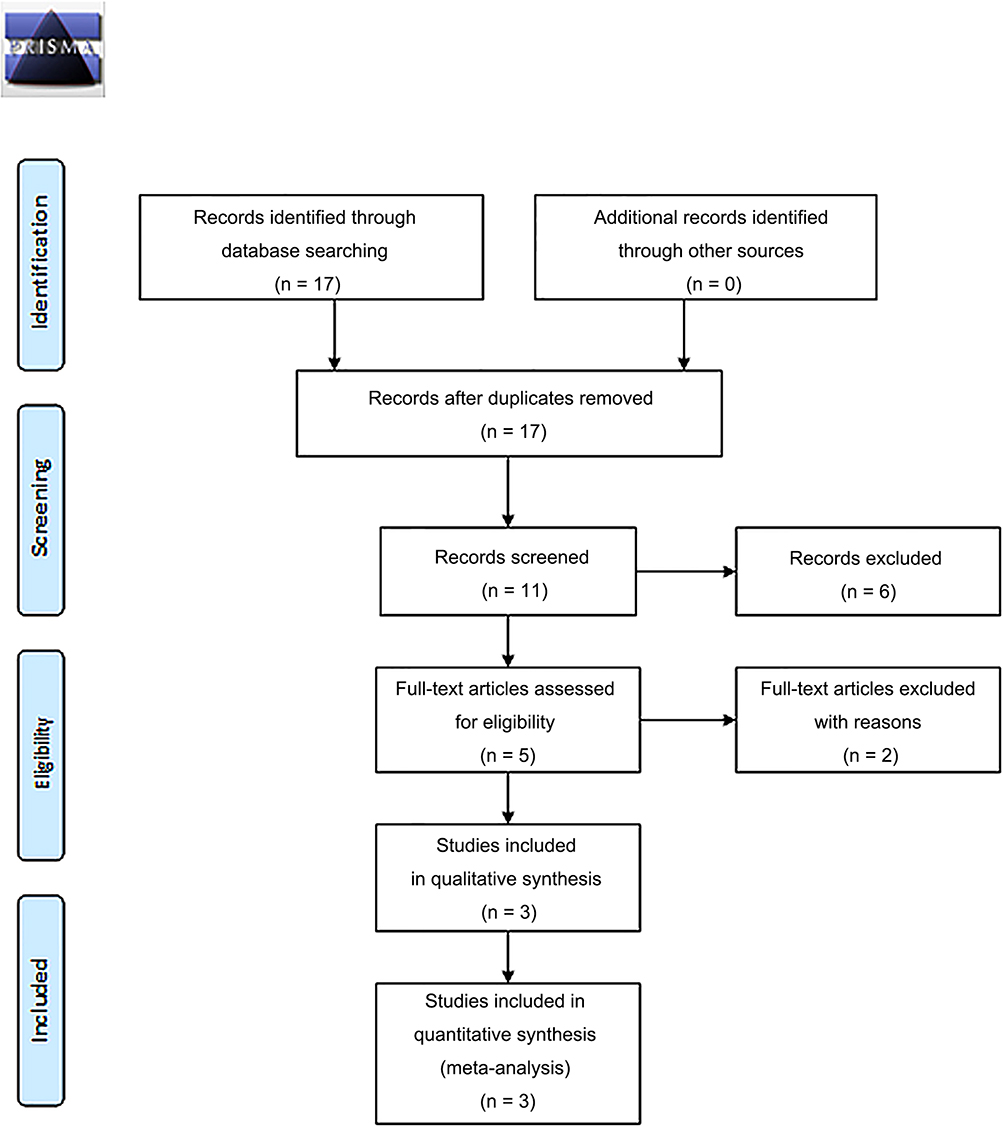 |
Figure 1 PRISMA 2009 Flow Diagram. |
Association of NQO1 C609T Polymorphism with CHD
Overall, no significant association was found by any genetic model. The OR T vs C is 1.02 and the 95% CI is 0.81 to 1.29. The OR TT vs CC is 1.17 and 95% CI is 0.75 to 1.82. The OR TT vs TC/CC is 1.1 and 95% CI is 0.85 to 1.43. All the results were performed by forest plot (Figures 2–5).
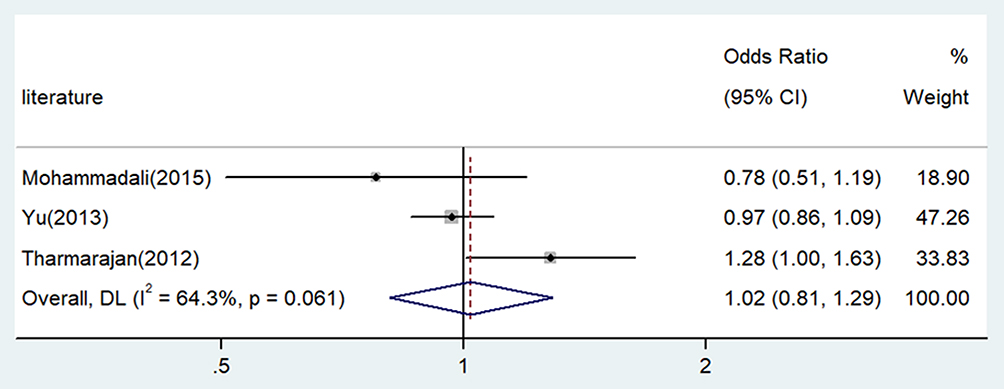 |
Figure 2 Forest plot for the associations between NQO1 C609T polymorphism and CHD risk through allele contrast (T vs C). Data from these studies.13,15,16 Abbreviations: OR, odds ratio; CI, confidence interval; CHD, coronary heart disease. |
 |
Figure 3 Forest plot for the associations between NQO1 C609T polymorphism and CHD risk through homozygote comparison (TT vs CC). Data from these studies.13,15,16 Abbreviations: OR, odds ratio; CI, confidence interval; CHD, coronary heart disease. |
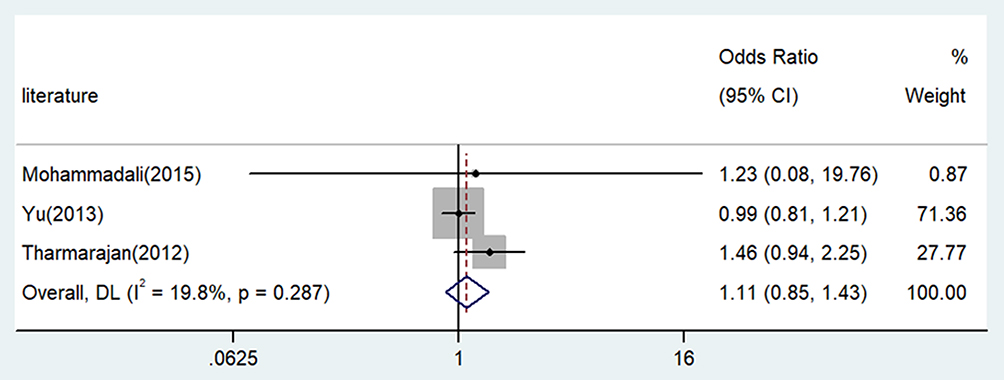 |
Figure 4 Forest plot for the associations between NQO1 C609T polymorphism and CHD risk through recessive genetic model (TT vs TC/CC). Data from these studies.13,15,16 Abbreviations: OR, odds ratio; CI, confidence interval; CHD, coronary heart disease. |
 |
Figure 5 Forest plot for the associations between NQO1 C609T polymorphism and CHD risk through dominate genetic model (TT/TC vs CC). Data from these studies.13,15,16 Abbreviations: OR, odds ratio; CI, confidence interval; CHD, coronary heart disease. |
Sensitivity Analysis of Meta-Analysis
We also performed a sensitivity analysis, omitting one study at a time and calculating the combined ORs of the remaining studies, and found that no single study was detected to alter the combined ORs of the two novel functional polymorphisms in the allele comparison model. This analysis indicates that the results of the current meta-analysis are relatively stable and credible. The results are shown in Table 4.
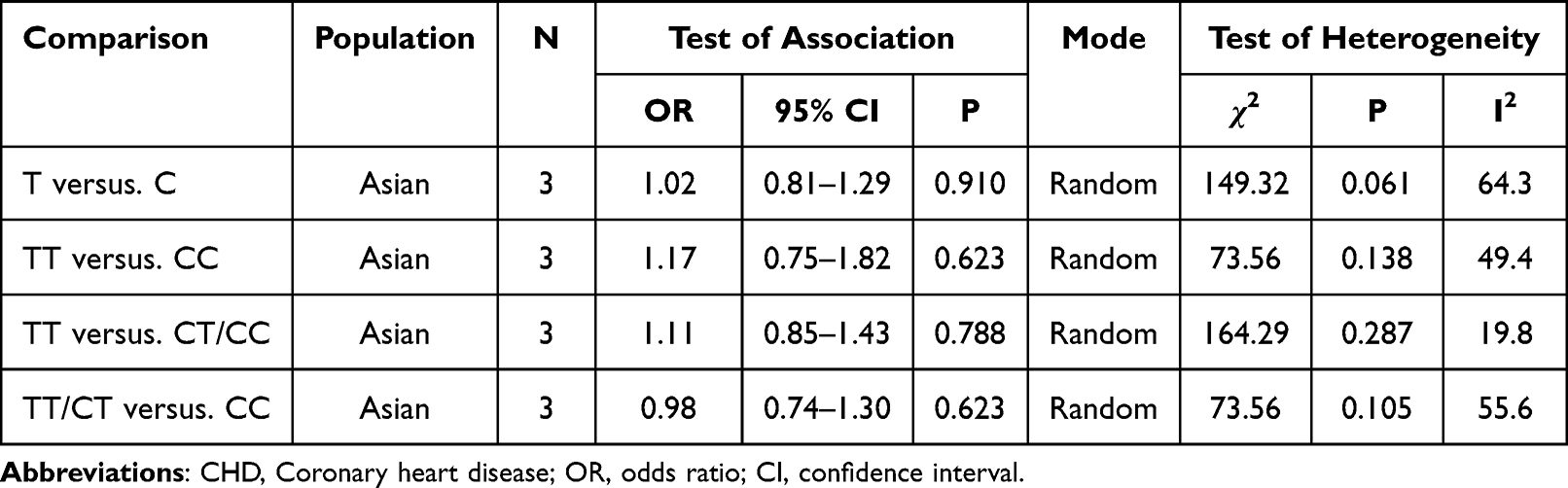 |
Table 4 Meta-Analysis of the NQO1 C609T Polymorphism and CHD Risk |
Discussion
CHD is the myocardial damage caused by the imbalance between myocardial blood supply and myocardial demand. It is affected by multiple factors and presents the pathogenesis mode combined with genetic susceptibility and environmental factors. Currently, it is believed that coronary heart disease is a complex polygenic disease caused by the interaction of various environmental factors and genetic factors. The genetic factors, namely susceptibility genes, may play a very important role in the occurrence and development of coronary heart disease by affecting the pathophysiological processes such as lipid metabolism, oxidative stress and inflammatory response, thrombosis and internal environmental stability.
With the development of molecular biology, the screening of susceptibility genes related to CHD has become one of the research hotspots. Numerous studies have shown that genotype is closely related to the occurrence and development of CHD, especially in the high-risk population with diabetes. Gene polymorphism may be involved in the process of atherosclerosis by affecting the metabolism of internal and external substances in the body, and there may be some differences among different races and regions.
In the present study, the Han ethnic group in Hainan area of China was selected as the research object, and we investigated the distribution frequency of genotype and allele in CHD patients and control population in Hainan area. Our results indicated that gene polymorphism existed in the Han ethnic group in Hainan. Specifically, People with the TT genotype have 2.06 times CHD risk as those with the CC genotype. And People with the T allele have 1.62 times CHD risk as those with the C allele. Interestingly, our results differ from those previously published. The above mentioned literatures suggested that NQO1 C609T polymorphism were not associated with CHD risk. We think that it is not an unfamiliar event when performing genetic association studies. The results of genetic polymorphisms vary greatly by race, population and geographic factors, which has been reported by various literatures. Although one study of a Chinese population has been reported, it focused on a population from northern China. China is a vast country with 56 ethnic groups. There are regional and ethnic differences among different ethnic groups.
We hypothesize that genetic polymorphisms may appear differently in different populations and ethnicities, and may be associated with different diseases. That is to say, the occurrence and development of CHD may be different in different races and nationalities carrying CHD-related genes. Therefore, it is necessary to further expand the sample size and investigate the population of different races and regions, which will help to clarify the pathogenesis of CHD and provide new possible measures for its prevention and treatment.
In the nursing process for CHD patients, nurses can take targeted care if they know the genetic polymorphisms of patients. For one thing, nurses can learn which patients are at higher risk. On the other hand, nurses can disseminate the knowledge of genetic polymorphism to the general public, especially the elderly, so that more patients can be served.
Conclusion
NQO1 gene polymorphism increased the CHD risk in a Chinese population. Combined with individual gene polymorphism, the accuracy of risk assessment for CHD can be improved and individualized health education can be provided for CHD patients by nurses.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Third People’s Hospital of Haikou. Written informed consent was obtained from all participants.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Disclosure
The authors declare that they have no competing interests.
References
1. Wang N, Sun Y, Zhang H, et al. Long-term night shift work is associated with the risk of atrial fibrillation and coronary heart disease. Eur Heart J. 2021;42(40):4180–4188. doi:10.1093/eurheartj/ehab505
2. Biddinger KJ, Emdin CA, Haas ME, et al. Association of habitual alcohol intake with risk of cardiovascular disease. JAMA Netw Open. 2022;5(3):e223849. doi:10.1001/jamanetworkopen.2022.3849
3. Fan M, Sun D, Zhou T, et al. Sleep patterns, genetic susceptibility, and incident cardiovascular disease: a prospective study of 385 292 UK biobank participants. Eur Heart J. 2020;41(11):1182–1189. doi:10.1093/eurheartj/ehz849
4. Sofianopoulou E, Kaptoge SK, Afzal S; Emerging Risk Factors Collaboration E-CVDVDSC. Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses. Lancet Diabetes Endocrinol. 2021;9(12):837–846. doi:10.1016/S2213-8587(21)00263-1
5. Holmes MV, Ala-Korpela M, Smith GD. Mendelian randomization in cardiometabolic disease: challenges in evaluating causality. Nat Rev Cardiol. 2017;14(10):577–590. doi:10.1038/nrcardio.2017.78
6. Khera AV, Emdin CA, Drake I, et al. Genetic risk, adherence to a healthy lifestyle, and coronary disease. N Engl J Med. 2016;375(24):2349–2358. doi:10.1056/NEJMoa1605086
7. Libby P, Pasterkamp G, Crea F, Jang IK. Reassessing the mechanisms of acute coronary syndromes. Circ Res. 2019;124(1):150–160. doi:10.1161/CIRCRESAHA.118.311098
8. Fioranelli M, Bottaccioli AG, Bottaccioli F, Bianchi M, Rovesti M, Roccia MG. Stress and inflammation in coronary artery disease: a review psychoneuroendocrineimmunology-based. Front Immunol. 2018;9:2031. doi:10.3389/fimmu.2018.02031
9. Katsiki N, Dimitriadis GD, Mikhailidis DP. Serum uric acid and diabetes: from pathophysiology to cardiovascular disease. Curr Pharm Des. 2021;27(16):1941–1951. doi:10.2174/1381612827666210104124320
10. Kao TW, Huang CC. Inflammatory burden and immunomodulative therapeutics of cardiovascular diseases. Int J Mol Sci. 2022;23(2):804. doi:10.3390/ijms23020804
11. Daiber A, Kroller-Schon S, Frenis K, et al. Environmental noise induces the release of stress hormones and inflammatory signaling molecules leading to oxidative stress and vascular dysfunction-Signatures of the internal exposome. Biofactors. 2019;45(4):495–506. doi:10.1002/biof.1506
12. Tzoulaki I, Castagne R, Boulange CL, et al. Serum metabolic signatures of coronary and carotid atherosclerosis and subsequent cardiovascular disease. Eur Heart J. 2019;40(34):2883–2896. doi:10.1093/eurheartj/ehz235
13. Boroumand M, Pourgholi L, Goodarzynejad H, et al. NQO1 C609T polymorphism is associated with coronary artery disease in a gender-dependent manner. Cardiovasc Toxicol. 2017;17(1):35–41. doi:10.1007/s12012-015-9353-8
14. Han SJ, Kang ES, Kim HJ, et al. The C609T variant of NQO1 is associated with carotid artery plaques in patients with type 2 diabetes. Mol Genet Metab. 2009;97(1):85–90. doi:10.1016/j.ymgme.2009.01.012
15. Ramprasath T, Murugan PS, Kalaiarasan E, Gomathi P, Rathinavel A, Selvam GS. Genetic association of Glutathione peroxidase-1 (GPx-1) and NAD(P)H:Quinone Oxidoreductase 1(NQO1) variants and their association of CAD in patients with type-2 diabetes. Mol Cell Biochem. 2012;361(1–2):143–150. doi:10.1007/s11010-011-1098-5
16. Yu X, Liu J, Zhu H, et al. Synergistic association of DNA repair relevant gene polymorphisms with the risk of coronary artery disease in northeastern Han Chinese. Thromb Res. 2014;133(2):229–234. doi:10.1016/j.thromres.2013.11.017
17. Chen X, Qin L, Li P, Mo W. Cyfip1 is downregulated in acute lymphoblastic leukemia and may be a potential biomarker in acute lymphoblastic leukemia. Tumour Biol. 2016;37(7):9285–9288. doi:10.1007/s13277-016-4786-7
18. Chen X, Zhang H, Li P, Yang Z, Qin L, Mo W. Gene expression of WWOX, FHIT and p73 in acute lymphoblastic leukemia. Oncol Lett. 2013;6(4):963–969. doi:10.3892/ol.2013.1514
19. Chen X, Li P, Yang Z, Mo WN. Expression of fragile histidine triad (FHIT) and WW-domain oxidoreductase gene (WWOX) in nasopharyngeal carcinoma. Asian Pac J Cancer Prev. 2013;14(1):165–171. doi:10.7314/APJCP.2013.14.1.165
20. Chen X, Su X, Lin M, et al. Expression of miR-192-5p in colon cancer serum and its relationship with clinicopathologic features. Am J Transl Res. 2021;13(8):9371–9376.
21. Chen X, Wang Z, Yan Y, et al. XRCC3 C18067T polymorphism contributes a decreased risk to both basal cell carcinoma and squamous cell carcinoma: evidence from a meta-analysis. PLoS One. 2014;9(1):e84195. doi:10.1371/journal.pone.0084195
22. Wang Z, Chen X, Liu B, Li S, Liu M, Xue H. Quantitative assessment of the associations between DNA repair gene XRCC3 Thr241Met polymorphism and gastric cancer. Tumour Biol. 2014;35(2):1589–1598. doi:10.1007/s13277-013-1219-8
23. Yan Y, Chen X, Li T, Li M, Liang H. Association of OGG1 Ser326Cys polymorphism and pancreatic cancer susceptibility: evidence from a meta-analysis. Tumour Biol. 2014;35(3):2397–2402. doi:10.1007/s13277-013-1317-7
24. Chen X, Yan Y, Li P, Yang Z, Qin L, Mo W. Association of GSTP1 -313A/G polymorphisms and endometriosis risk: a meta-analysis of case-control studies. Eur J Obstet Gynecol Reprod Biol. 2013;171(2):362–367. doi:10.1016/j.ejogrb.2013.10.005
25. Chen X, Mo W, Peng Q, Su X. Lack of association between Fas rs180082 polymorphism and risk of cervical cancer: an update by meta-analysis. BMC Med Genet. 2013;14(1):71. doi:10.1186/1471-2350-14-71
26. Si D, Yao Y, Chen X, Qiu J. Ethnicity-stratified analysis of the association between P53 rs1042522 polymorphism and women HPV infection: a meta-analysis. Microb Pathog. 2021;161(Pt A):105099. doi:10.1016/j.micpath.2021.105099
27. Niu K, Chen X, Lu Y, Xu M. COL3A1 rs1800255 polymorphism is associated with pelvic organ prolapse susceptibility in Caucasian individuals: evidence from a meta-analysis. PLoS One. 2021;16(4):e0250943. doi:10.1371/journal.pone.0250943
28. Jin X, Wu Y, Yin S, Chen X, Zhang Y. Association between the IL-10 and IL-6 polymorphisms and brucellosis susceptibility: a meta-analysis. BMC Med Genet. 2020;21(1):63. doi:10.1186/s12881-020-01006-0
29. Jin X, Yin S, Zhang Y, Chen X. Association between TLR2 Arg677Trp polymorphism and tuberculosis susceptibility: a meta-analysis. Microb Pathog. 2020;144:104173. doi:10.1016/j.micpath.2020.104173
30. Yuanyuan G, Xue Y, Yachao L, Xiao F, Xu C. Association between IL-18 -607 C/A polymorphism and the risk of prostate cancer: a meta-analysis of case-control studies. Asian Pac J Cancer Prev. 2019;20(6):1595–1602. doi:10.31557/APJCP.2019.20.6.1595
31. Jin X, Yin S, Zhang Y, Chen X. Quantitative assessment of the association between IL-10 −592 A/C polymorphism and Kawasaki disease risk in Chinese population: evidence from a meta-analysis. Cardiol Young. 2018;28(6):811–815. doi:10.1017/S1047951118000380
32. Jin X, Yin S, Zhang Y, Chen X. Association between TLR2 + 2477G/A polymorphism and bacterial meningitis: a meta-analysis. Epidemiol Infect. 2018;146(5):642–647. doi:10.1017/S0950268818000298
33. Chen X, Jiang M, Zhao RK, Gu GH. Quantitative assessment of the association between ABC polymorphisms and osteosarcoma response: a meta-analysis. Asian Pac J Cancer Prev. 2015;16(11):4659–4664. doi:10.7314/APJCP.2015.16.11.4659
34. Qin LY, Chen X, Li P, Yang Z, Mo WN. Association between the XRCC3 Thr241Met polymorphism and cervical cancer risk: a meta-analysis. Asian Pac J Cancer Prev. 2014;14(11):6703–6707. doi:10.7314/APJCP.2013.14.11.6703
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.