Back to Journals » Infection and Drug Resistance » Volume 15
Genetic Diversity and in vitro Activity of Aztreonam/Avibactam and Ceftazidime/Avibactam Against Carbapenem-Resistant Enterobacterales: A Multi-Center Study in Southwest China
Authors Sun S, Chen K, Kong X, Tian W ![]() , Niu S
, Niu S ![]()
Received 19 January 2022
Accepted for publication 7 April 2022
Published 27 April 2022 Volume 2022:15 Pages 2243—2251
DOI https://doi.org/10.2147/IDR.S357396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Shan Sun,1 Kai Chen,2 Xuehua Kong,2 Wenjun Tian,3,* Siqiang Niu1,*
1Department of Laboratory Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2College of Laboratory Medicine, Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Clinical Laboratory Medicine, Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenjun Tian; Siqiang Niu, Email [email protected]; [email protected]
Purpose: This study aimed to understand the distribution characteristics of carbapenemase genes and assess the antimicrobial activities of aztreonam/avibactam (ATM/AVI) and ceftazidime/avibactam (CAZ/AVI) against carbapenem-resistant Enterobacterales (CRE) isolates in Chongqing, Southwest China.
Methods: CRE isolates and their clinical information were collected from 22 hospitals covering all the five regions across Chongqing between January 1, 2016 and December 31, 2017. PCR was used to screen for common carbapenemase genes. And minimum inhibitory concentrations (MICs) were determined by broth microdilution method.
Results: A total of 312 unduplicated CRE isolates (eg, 206 Klebsiella pneumoniae, 43 Escherichia coli, and 42 Enterobacter cloacae) were collected during the two-year study period. Among these CRE isolates, 92.3% carried carbapenemase genes, with a majority of isolates carrying single blaKPC-2 (47.1%) or single blaNDM/IPM (36.2%) and 8.9% of isolates carrying two or three carbapenemase genes. Notably, 95.6% (197/206) K. pneumoniae, 86.0% (37/43) E. coli and 88.1% (37/42) E. cloacae harbored carbapenemase genes. In addition, blaKPC-2 was prevalent in K. pneumoniae (70.4%), while blaNDM was predominant in E. coli (83.7%) and E. cloacae (78.6%). Besides, only metallo-β-lactamase (MBL) genes were detected in the CRE isolates from children. Overall, 0.0%, 48.1%, 59.0%, 61.5% and 63.1% of the CRE isolates were resistant to ATM/AVI, CAZ/AVI, nitrofurantoin, amikacin and trimethoprim/sulfamethoxazole, respectively. 99.7% of the total 312 isolates could be killed by ATM/AVI with the MIC 1 μg/mL, whereas CAZ/AVI showed good antibacterial activity (98.0% susceptible) against the blaKPC-2-carriers with the MIC50/90 values of 1/4 μg/mL.
Conclusion: The distribution features of carbapenemase genes in Chongqing were comprehensively illustrated in terms of species and sources of CRE for the first time in this multi-center study that covered all the geographical locations across Chongqing. ATM/AVI showed superior activity against all CRE isolates regardless of their genotype, whereas CAZ/AVI was active against almost all KPC-producers.
Keywords: carbapenem-resistant Enterobacterales, carbapenemase genes, aztreonam/avibactam, ceftazidime/avibactam
Introduction
In recent years, carbapenem-resistant Enterobacterales (CRE), which have become a worldwide threat because of their increasing resistance to carbapenems and worldwide dissemination, are recognized as an urgent threat according to a report by CDC of the US and have been ranked as the critical and highest priority group of pathogens by WHO.1,2 CRE often causes difficult-to-treat or untreatable infection with significant morbidity and mortality.3–6 There are two key mechanisms of carbapenem resistance in Enterobacterales: the production of carbapenemase and the production of ESBL and/or AmpC coupled with outer membrane protein defects and/or active efflux. Three major classes of carbapenemases are implicated in the dissemination of CRE: Ambler class A (eg, KPC), class B metallo-β-lactamase (MBL) (eg, NDM, VIM and IMP), and class D (eg, OXA-48-like) carbapenemases.7 Both of KPC and OXA-48-like enzymes have serine-based hydrolytic activity, while class B enzymes require the presence of metal for their hydrolytic activity.8–10
The carbapenemase-producing CRE (CP-CRE) often co-harbor additional genes conferring resistance to other classes of antimicrobials and make multiple antimicrobials invalid. To tackle this serious resistance crisis, new drugs such as aztreonam/avibactam (ATM/AVI)11 and ceftazidime/avibactam (CAZ/AVI)12 have emerged. CAZ/AVI is effective against KPC-producing CRE and certain class D β-lactamase-producers, but it is not active against MBL-producers.13 Fortunately, ATM maintains stable to MBL hydrolysis, although it can be inactivated by most serine β-lactamases, including ESBL, AmpC, and KPC. Consequently, the combination of ATM and AVI could show potent antimicrobial activity against the CRE including MBL-producers. Hence, with the advent of such novel antimicrobials, the individualized therapeutic regimen should be prescribed based on molecular resistance phenotypes.11,14,15
Recent studies showed that the prevalence of CP-CRE had risen in the last 10 years16,17 and that the dominant carbapenemase genes varied in different regions of the world.4,18,19 In China, several large-scale nationwide surveillances illustrated that the acquisition of blaKPC and blaNDM was responsible for carbapenem resistance, and meanwhile the antimicrobial susceptibility profiles of CRE were described.5,20–22 However, the comprehensive characteristics of carbapenemase genes and the resistance level of commonly used antimicrobials are limited in Chongqing. Moreover, only two previous studies in Chongqing by our research group focused on the activity of CAZ/AVI and ATM/AVI based on the carbapenemase genotypes, but the numbers of recruited hospitals were sparse and the diversity of carbapenemase genes was limited.23,24 To fill this gap and execute effective and personalized antimicrobial therapies targeting CRE infections, this multi-center study covering all the geographical regions in Chongqing, Southwest China was conducted.
Materials and Methods
Collection of CRE Isolates
A total of 22 laboratories participated in this study, which covered all five geographical regions of Chongqing including the West (five hospitals), the South (two hospitals), the Northeast (two hospitals), the Southeast (one hospital) and the Center (12 hospitals). The CRE isolates were identified and determined for antimicrobial sensitivity, according to Clinical and Laboratory Standards Institute (CLSI) in the local laboratories. And between January 1, 2016 and December 31, 2017, all laboratories were required to collect consecutive and nonduplicated CRE isolates, which caused infections, such as pneumonia, bloodstream infection, urinary tract infection, skin and skin structure infections, and so on. Finally, all the CRE isolates, which were part of the routine hospital laboratory procedure and their clinical information including wards, patients’ age and specimen types were collected.
Confirmation of CRE Isolates
Strain identification was confirmed by VITEK MS system (bioMérieux, France) and then reconfirmed by 16S rRNA sequencing. The broth microdilution method was conducted to determine minimum inhibitory concentrations (MICs) of three carbapenems including ertapenem, imipenem and meropenem according to CLSI guidelines. Those isolates of Enterobacterales resistant to at least one of the carbapenems, according to CLSI, 202025 (meropenem and imipenem, ≥4 μg/mL; ertapenem, ≥2 μg/mL) would be enrolled into the following study.
Detection of Carbapenemase Genes
Polymerase chain reaction (PCR) was performed to screen for the presence of the carbapenemase-encoding genes blaKPC, blaIMP, blaNDM, blaVIM and blaOXA-48-like for all confirmed CRE isolates. PCR amplicons were sequenced by Sangon Biotech (Shanghai, China) and then all the sequences were blasted in GenBank (https://blast.ncbi.nlm.nih.gov/Blast.cgi). Those primers designed for identifying the resistance genes mentioned above have been described previously.21,26
Antimicrobial Susceptibility Testing
The broth microdilution method recommended by the CLSI was carried out for antimicrobial susceptibility testing (AST) to determine the MICs of 13 kinds of antimicrobials in addition to the aforementioned carbapenems, including ceftazidime (CAZ), cefepime (FEP), aztreonam (ATM), piperacillin/tazobactam (TZP), aztreonam/avibactam (ATM/AVI), ceftazidime/avibactam (CAZ/AVI), gentamicin (GEN), tobramycin (TOB), amikacin (AMK), ciprofloxacin (CIP), levofloxacin (LEV), trimethoprim/sulfamethoxazole (SXT) and nitrofurantoin (NIT). NIT was tested only for the strains isolated from urine. And then, the results of all AST were interpreted according to the breakpoints of CLSI, 2020.25 As for ATM/AVI and CAZ/AVI, avibactam was fixed at the concentration of 4μg/mL, while aztreonam or ceftazidime was added at different concentrations ranging from 0.125 to 256 μg/mL. The AST was performed in triplicate on three separate days, and the quality control strains were Pseudomonas aeruginosa ATCC 27853 and E. coli ATCC 25922.27 Afterwards, the AST results would be compared between four groups including KPC group (isolates only carrying blaKPC genes), MBL group (isolates only carrying MBL genes), KPC-MBL group (isolates co-harboring blaKPC and MBL genes) and Non-CP group (isolates without any carbapenemases detected). MICs results, patients’ information and carbapenemase genotypes were analysed using WHONET version 5.6 (http://www.whonet.org/contact.html).
Results
Distribution and Clinical Information of CRE Isolates
Ultimately, 312 strains of unduplicated confirmed CRE isolated between January 1, 2016 and December 31, 2017 were enrolled in subsequent experiments. The most common species were K. pneumoniae (n = 206, 66.0%), E. coli (n = 43, 13.8%), and E. cloacae (n = 42, 13.5%), respectively. 127 (40.7%), 104 (33.3%), 40 (12.8%), 23 (7.4%) and 18 (5.8%) isolates were collected from the Center (12 hospitals), Northeast (two hospitals), West (five hospitals), South (two hospitals) and Southeast (one hospital) of Chongqing, respectively.
Approximately half of the CRE isolates were from lower respiratory tract (n = 157, 50.3%), followed by urine (n = 83, 26.6%) and blood (n = 32, 10.3%). Among the total 312 strains, 280 (89.7%) were from adults and 32 (10.3%) were from children. Besides, the numbers of CRE isolates in intensive care unit (ICU) (n = 112, 35.9%) were the largest, followed by those in neurosurgery (n = 44, 14.1%), pediatrics (n = 30, 9.6%) and respiratory department (n = 29, 9.3%).
Carbapenemase Genes Characteristics of CRE Isolates
Of the 312 CRE isolates, 288 (92.3%) were positive for the carbapenemase genes, among which 147 (51.0%) were single blaKPC-2-carriers and 113 (39.2%) owned single MBL genes (blaNDM-1, n = 68, 23.6%; blaNDM-5, n = 41, 14.2%; blaIMP-4, n = 4, 1.4%). In addition, 28 (9.7%) isolates carried two or more genes with at least one MBL gene. However, no blaVIM or blaOXA-48-like was detected. Notably, 197/206 (95.6%) K. pneumoniae, 37/43 (86.0%) E. coli and 37/42 (88.1%) E. cloacae harbored carbapenemase gene. 145/206 (70.4%) carried blaKPC-2 genes in K. pneumoniae, in contrast to 1/43 (2.3%) in E. coli and 1/42 (2.4%) in E. cloacae. However, in the last two, the MBL genes were the most common, accounting for 83.7% (36/43) and 78.6% (33/42), respectively. blaNDM-5 was predominant in E. coli, whilst blaNDM-1 was prevalent in E. cloacae. And only MBLs genes were detectable in the other carbapenem-resistant species, including C. freumdii, K. oxytoca, K. aerogenes, S. marcescens, except that one K. aerogenes isolate carried blaKPC-2 and blaNDM-1 in combination. It is noteworthy that mixed genotypes of blaKPC coupled with MBL gene were more common in K. pneumonia (19/206, 9.2%) and E. clocae (3/42, 7.1%) compared to E. coli (0/43, 0.0%) (Table 1).
 |
Table 1 Characteristics of Carbapenemase Genes Among 312 CRE Clinical Isolates |
Besides, it is clear that the proportions of CRE carrying MBL genes in urine and in blood were 60.2% (50/83) and 53.1% (17/32), respectively, while only 35.7% (56/157) strains harbored MBL genes in lower respiratory tract where single blaKPC-2 (91/157, 58.0%) was predominant. Notably, one isolate co-harbouring three carbapenemase genes (blaKPC-2, blaNDM-1 and blaIMP-4) was detected in the blood. Only MBL genes were detected in the CRE isolated from children with the highest prevalence of single blaNDM-5 (19/32, 59.4%), whereas single blaKPC-2 (147/280, 52.5%) was the most common in adults. As for ICU and neurosurgery as well as respiratory department, the percentages of single-blaKPC-2-bearing CRE were 52.7% (59/112), 63.6% (28/44) and 62.1% (18/29), respectively, which were higher than those with MBL genes (41.1%, 31.8% and 31.0%, respectively). On the contrary, in urology, the CRE isolates carrying MBL genes accounted for a large proportion, as high as 73.7% (14/19). In terms of geographical location in Chongqing, carrying single blaKPC-2 was absolutely predominant in Northeast and Southeast with the proportions of 68.0% (70/103) and 100% (16/16), respectively, while MBL genes were prevalent in the other three regions including the Center (75/111, 67.6%), South (12/20, 60%) and West (21/38, 55.3%).
Antimicrobial Susceptibility Testing
For the commonly used antimicrobials, the most effective drugs against the total CRE isolates tested were amikacin (37.5% susceptible), SXT (36.9% susceptible) and nitrofurantoin (28.9% susceptible), respectively. In the three groups categorized according to different carbapenemase genotypes, ceftazidime, cefepime, and three kinds of carbapenems all presented high resistance rates ranging from 94.9% to 100.0%. Nevertheless, the resistance rates of seven antimicrobials including aztreonam (78.8%), three aminoglycosides (28.0–66.9%), two quinolones (61.0–67.8%) and nitrofurantoin (26.3%) in MBL group were evidently lower than those in the other two groups both carrying blaKPC-2. And SXT showed higher resistance rate in KPC-MBL group (82.6%) compared to that in KPC group (58.5%) and in MBL group (65.3%). Additionally, amikacin was the most active drug with the susceptible rate of 70.3%, followed by nitrofurantoin (55.3% susceptible) and SXT (34.7% susceptible) in MBL group, whereas SXT displayed the best antibacterial activity (41.5% susceptible) in KPC group (Table 2).
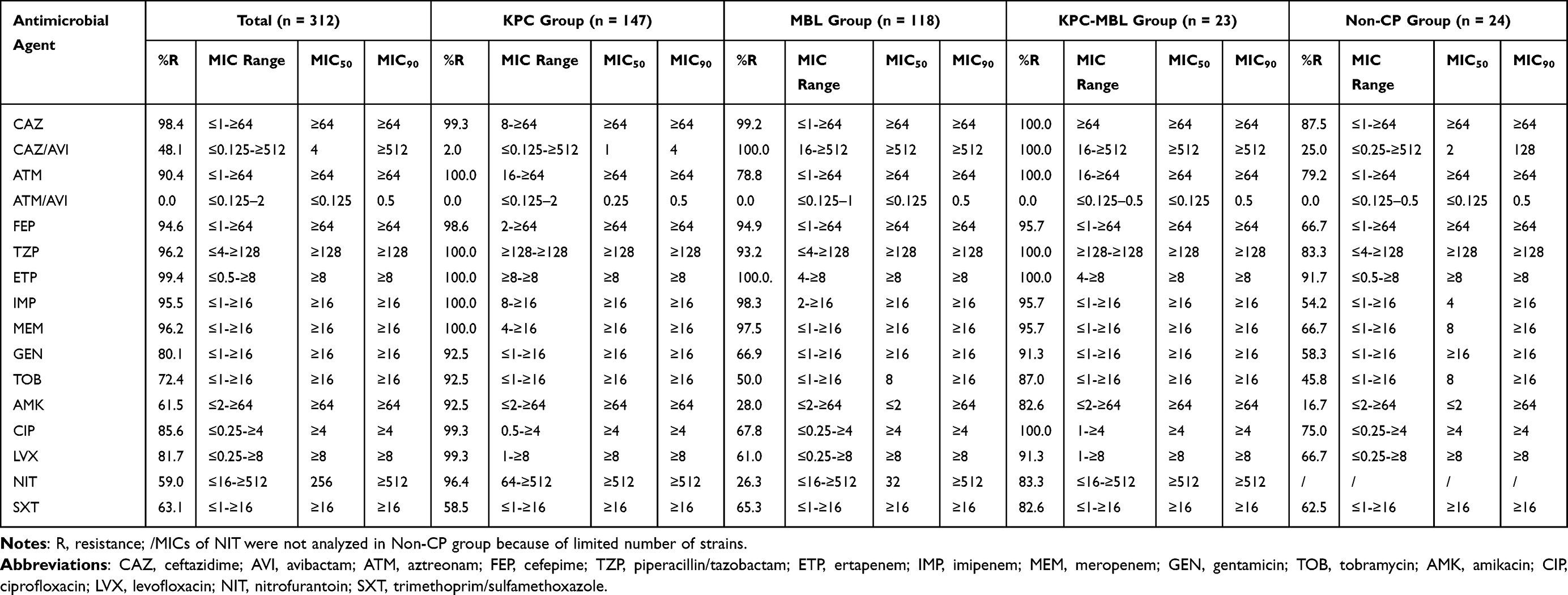 |
Table 2 Antimicrobial Susceptibility of 312 CRE Isolates and Different Isolates by Genotypes (MICs, μg/mL) |
Among the total CRE isolates, 48.1% (150/312) were resistant to CAZ/AVI with MIC90 of ≥512 μg/mL, among which 94.0% (141/150) carried MBL genes, 2.0% (3/150) only harbored blaKPC-2 and 4.0% (6/150) did not have any carbapenemase genes. For the 147 single KPC-2-producers, 144 (98.0%) were sensitive to CAZ/AVI and 100 (68.0%) could be killed by CAZ/AVI of 1 μg/mL (Figure 1). In addition, all 312 CRE were extremely sensitive to ATM/AVI with MIC50/MIC90 of ≤0.125/0.5 μg/mL, among which 99.7% isolates could be killed by ATM/AVI of 1 μg/mL (Figure 2).
 |
Figure 1 The MICs distribution of CAZ/AVI against 147 CRE isolates carrying single blaKPC gene. |
 |
Figure 2 The MICs distribution of ATM/AVI against 312 CRE isolates. |
Discussion
In China, CRE infection poses a serious public-health threat and the production of carbapenemases is the major mechanism of carbapenem resistance in CRE.5,20–22 In Chongqing, Southwest China, the diversity of carbapenemase genes was comprehensively illustrated for the first time in our multi-center study, which covered all the five geographical regions across Chongqing. We discovered that the carbapenem resistance was mainly caused by blaKPC-2 and blaNDM1/5 in Chongqing as was shown in the previous nationwide studies,5,20–22 otherwise, three studies all reported the higher proportions of blaKPC-2 clustering between 51.6% and 57.0% than that of 47.1% in our study and the lower percentages of MBL genes ranging from 31.4% to 38.6% compared to that of 45.2% in our study.5,20,21 Besides, in accordance with the aforementioned two studies,20,21 blaKPC-2 was the most frequently detected carbapenemase gene in K. pneumoniae, whilst blaNDM-5 and blaNDM-1 were the most dominant genes in E. coli and E. clocae, respectively. Notably, the proportion of co-carrying blaKPC-2 and blaNDM was 6.7% (21/312) in our study, with K. pneumoniae being the most common species in this category, while the prior reports showed the obviously lower percentages ranging from 0.1% to 1.9%.5,20,21
Additionally, variations in the prevalence rate of different carbapenemase genes were also observed based on different geographical regions, patients’ age, wards and infection sites in this study. For example, the three districts of South, West and Center of Chongqing showed the similar distribution features of carbapenemase genes with more than 55% isolates carrying at least one MBL gene among the CP-CRE in each region. Probably, those locations are geographically close and the frequent flow of patients between them contributes to their resemblance to gene distribution. It is noteworthy that in children, only MBL genes were detected and blaNDM-5 was the most prevalent gene, completely different from the adults in which the majority of isolates harbored blaKPC-2. In contrast to this conclusion, certain studies focusing on pediatric patients reported more kinds of genes, such as blaOXA-232 and blaKPC-2.20,28
Notably, 100% CRE isolates were extremely sensitive to ATM/AVI, and they could all be inhibited by ATM/AVI of ≤2 μg/mL (MIC50/90, ≤0.125/0.5 μg/mL), independent of their carbapenem resistance mechanism, as other publications have already shown. Zou et al24 showed a similar MIC50/90 (≤0.125/1 μg/mL) of ATM/AVI among 120 CRE from three secondary hospitals in Chongqing. They also found that 90.0% isolates could be inhibited by ATM/AVI of ≤1μg/mL, while 99.7% CRE isolates could be killed at the same drug concentration in our study. Besides, a study on the activity of ATM/AVI against MBL-producing Enterobacterales collected from six tertiary care hospitals in China also observed the equal MIC50/90 (≤0.125/1 μg/mL).29
Currently, the continual emergence of CRE poses a particularly critical threat to healthcare worldwide. Infections due to these so-called superbugs are related to high mortality because of limited therapeutic options. Recently, a multicenter research study in China has reported a high incidence and mortality of infections caused by CRE.22 Therefore, treatment of CRE infections is challenged and the personalized therapy to target them should be recommended and adopted based on the antimicrobial susceptibility pattern and molecular type of the bacteria and the source and severity of infection.30 However, the culture of pathogens is time-consuming. Besides, tests of rapid carbapenemase screening and/or genotyping are not been performed in most of the laboratories in China. It is unrealistic to refuse to prescribe antimicrobials until the results of AST and genotypes were available, especially for the critically ill patients, such as bloodstream infection with high mortality rates,31,32 and thus local antimicrobial susceptibility profiles together with molecular epidemiological characteristics are of most importance for clinicians to initiate the prompt and appropriate empirical therapy.
In conclusion, our multi-center study covered all the geographical locations in Chongqing for the first time in which the distribution features of carbapenemase genes in terms of species and sources of CRE were illustrated comprehensively. And it revealed high resistance levels against commonly used antimicrobials among the CRE isolates and resistance differences between CRE isolates with or without blaKPC in Chongqing. ATM/AVI exhibited potent activity against all CRE isolates including MBL producers, whereas CAZ/AVI was active against almost all KPC producers. The clinical application of these new agents should be gradually personalized based on genotypes to limit misuse and avoid the emergence of resistance.
Ethical Approval
The isolates and data which were part of the routine hospital laboratory procedure analyzed in the study were obtained in accordance with the standards and approved by the Chongqing Medical University Institutional Review Board and Biomedical Ethics Committee (Ethical review batch number: 2020-644). For this study, with no contact with the patients, so, the ethics committee determined that informed consent was not required.
Acknowledgments
The authors would like to thank all laboratories enrolled in this study.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82072349).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. Available from: https://www.who.int/medicines/publications/global-priority-list-antibiotic-resistant-bacteria/en/.
2. CDC. Antibiotic resistance threats in the United States; 2019. Available from: https://www.cdc.gov/drugresistance/biggest-threats.html.
3. Suay-García B, Pérez-Gracia MT. Present and future of carbapenem-resistant Enterobacterales (CRE) infections. Antibiotics. 2019;8(3):122. doi:10.3390/antibiotics8030122
4. Nordmann P, Poirel L. Epidemiology and diagnostics of carbapenem resistance in Gram-negative bacteria. Clin Infect Dis. 2019;69(Suppl 7):S521–S528. doi:10.1093/cid/ciz824
5. Zhang R, Liu L, Zhou H, et al. Nationwide surveillance of clinical carbapenem-resistant Enterobacterales (CRE) strains in China. EBioMedicine. 2017;19:98–106. doi:10.1016/j.ebiom.2017.04.032
6. Falagas ME, Tansarli GS, Karageorgopoulos DE, Vardakas KZ. Deaths attributable to carbapenem-resistant Enterobacterales infections. Emerg Infect Dis. 2014;20(7):1170–1175. doi:10.3201/eid2007.121004
7. Karampatakis T, Antachopoulos C, Iosifidis E, et al. Molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae in Greece. Future Microbiol. 2016;6(11):809–823. doi:10.2217/fmb-2016-0042
8. Goodman KE, Simner PJ, Tamma PD, et al. Infection control implications of heterogeneous resistance mechanisms in carbapenem-resistant Enterobacterales (CRE). Expert Rev Anti Infect Ther. 2016;14(1):95–108. doi:10.1586/14787210.2016.1106940
9. Li XZ, Plésiat P, Nikaido H. The challenge of efflux-mediated antibiotic resistance in Gram-negative bacteria. Clin Microbiol Rev. 2015;28(2):337–418. doi:10.1128/CMR.00117-14
10. Tzouvelekis LS, Markogiannakis A, Psichogiou M, et al. Carbapenemases in Klebsiella pneumoniae and other Enterobacterales: an evolving crisis of global dimensions. Clin Microbiol Rev. 2012;25(4):682–707. doi:10.1128/CMR.05035-11
11. Sader HS, Mendes RE, Pfaller MA, et al. Antimicrobial activities of aztreonam–avibactam and comparator agents against contemporary (2016) clinical Enterobacterales isolates. Antimicrob Agents Chemother. 2018;62(1):e01856–17. doi:10.1128/AAC.01856-17
12. Sader HS, Castanheira M, Shortridge D, et al. Antimicrobial activity of ceftazidime–avibactam tested against multidrug-resistant Enterobacteriaceae and Pseudomonas aeruginosa isolates from U.S. Medical centers, 2013 to 2016. Antimicrob Agents Chemother. 2017;61(11):e01045–17. doi:10.1128/AAC.01045-17
13. Falcone M, Paterson D. Spotlight on ceftazidime/avibactam: a new option for MDR gram-negative infections. J Antimicrob Chemother. 2016;71(10):2713–2722. doi:10.1093/jac/dkw239
14. Abboud MI, Damblon C, Brem J, et al. Interaction of avibactam with class B metallo-β-lactamases. Antimicrob Agents Chemother. 2016;60(10):5655–5662. doi:10.1128/AAC.00897-1610
15. Bush K. Game changers: new β-lactamase inhibitor combinations targeting antibiotic resistance in Gram-negative bacteria. ACS Infect Dis. 2018;4(2):84–87. doi:10.1021/acsinfecdis.7b00243
16. Li H, Zhang J, Liu Y, et al. Molecular characteristics of carbapenemase-producing Enterobacterales in China from 2008 to 2011: predominance of KPC-2 enzyme. Diagn Microbiol Infect Dis. 2014;78(1):63–65. doi:10.1016/j.diagmicrobio.2013.10.002
17. Zhang R, Chan EW, Zhou H, et al. Prevalence and genetic characteristics of carbapenem- resistant Enterobacterales strains in China. Lancet Infect Dis. 2017;17(3):256–257. doi:10.1016/S1473-3099(17)30072-5
18. Bush K, Bradford PA. Epidemiology of β-lactamase-producing pathogens. Clin Microbiol Rev. 2020;33(2):e00047–19. doi:10.1128/CMR.00047-19
19. Hsu LY, Apisarnthanarak A, Khan E, et al. Carbapenem-resistant Acinetobacter baumannii and Enterobacterales in South and Southeast Asia. Clin Microbiol Rev. 2017;30(1):1–22. doi:10.1128/CMR.masthead.30-11
20. Han R, Shi Q, Wu S, et al. Dissemination of carbapenemases (KPC, NDM, OXA-48, IMP, and VIM) among carbapenem-resistant Enterobacterales isolated from adult and children patients in China. Front Cell Infect Microbiol. 2020;10:314. doi:10.3389/fcimb.2020.00314
21. Wang Q, Wang X, Wang J, et al. Phenotypic and genotypic characterization of carbapenem-resistant Enterobacterales: data from a longitudinal large-scale CRE study in China (2012–2016). Clin Infect Dis. 2018;67(S2):S196–205. doi:10.1093/cid/ciy660
22. Zhang Y, Wang Q, Yin Y, et al. Epidemiology of carbapenem-resistant Enterobacterales infections: report from the China CRE network. Antimicrob Agents Chemother. 2018;62(2):e01882–17. doi:10.1128/AAC.01882-17
23. Wei J, Zou C, Wang D, et al. Genetic diversity and in vitro activity of ceftazidime/avibactam and aztreonam/avibactam against imipenem-resistant Enterobacterales isolates in Southwest China: a single-centre study. J Glob Antimicrob Resist. 2020;22:448–451. doi:10.1016/j.jgar.2020.04.023
24. Zou C, Wei J, Shan B, et al. In vitro activity of ceftazidime-avibactam and aztreonam-avibactam against carbapenem-resistant Enterobacterales isolates collected from three secondary hospitals in Southwest China between 2018 and 2019. Infect Drug Resist. 2020;13:3563–3568. doi:10.2147/IDR.S273989
25. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing.
26. Tian X, Sun S, Jia X, et al. Epidemiology of and risk factors for infection with extended-spectrum β-lactamase-producing carbapenem-resistant Enterobacterales: results of a double case–control study. Infect Drug Resist. 2018;11:1339–1346. doi:10.2147/IDR.S173456
27. Niu S, Wei J, Zou C, et al. In vitro selection of aztreonam/avibactam resistance in dual-carbapenemase-producing Klebsiella pneumonia. J Antimicrob Chemother. 2020;75(3):559–565. doi:10.1093/jac/dkz468
28. Tian D, Pan F, Wang C, et al. Resistance phenotype and clinical molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae among pediatric patients in Shanghai. Infect Drug Resist. 2018;11:1935–1943. doi:10.2147/IDR.S175584
29. Zhang B, Zhu Z, Jia W, et al. In vitro activity of aztreonam–avibactam against metallo-β- lactamase-producing Enterobacterales-A multicenter study in China. Int J Infect Dis. 2020;97:11–18. doi:10.1016/j.ijid.2020.05.075
30. Rodríguez-Bano J, Gutiérrez-Gutiérrez B, Machuca I, Pascual A. Treatment of infections caused by extended-spectrum-beta-lactamase-, AmpC-, and carbapenemase-producing Enterobacterales. Clin Microbiol Rev. 2018;31(2):e00079–17. doi:10.1128/CMR.00079-17
31. Gutiérrez-Gutiérrez B, Salamanca E, de Cueto M, et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to carbapenemase-producing Enterobacterales (INCREMENT): a retrospective cohort study. Lancet Infect Dis. 2017;17(7):726–734. doi:10.1016/S1473-3099(17)30228-1
32. Tumbarello M, Viale P, Viscoli C, et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: importance of combination therapy. Clin Infect Dis. 2012;55(7):943–950. doi:10.1093/cid/cis588
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.