Back to Journals » The Application of Clinical Genetics » Volume 19
Generalized Nevus Lipomatosus Cutaneous Superficialis: A Case Report with Comprehensive Genetic Analysis
Authors Qiu Y ![]() , Su R, Su X, Zhang Y, Tan Y
, Su R, Su X, Zhang Y, Tan Y ![]() , Zhang X, Liu F
, Zhang X, Liu F ![]()
Received 14 January 2026
Accepted for publication 8 June 2026
Published 8 July 2026 Volume 2026:19 592972
DOI https://doi.org/10.2147/TACG.S592972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Ye Qiu, Rina Su, Xiangxi Su, Yankun Zhang, Yaqi Tan, Xiuying Zhang, Fang Liu
Department of Dermatology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Fang Liu, Department of Dermatology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Background: Nevus lipomatosus superficialis (NLS) is a rare cutaneous hamartoma characterized by ectopic adipose tissue in the dermis. Its genetic basis remains largely unknown.
Methods: We conducted a comprehensive clinical, histopathological, and genetic investigation of a 17-year-old female with an exceptionally extensive distribution of lesions (involving trunk, buttocks, lower extremities, and vulva) that was atypical due to the presence of significant pain and recurrent infections. Whole exome sequencing (WES) was performed on the proband and both parents (trio-WES), and whole genome sequencing (WGS) was performed on fresh lesional tissue. Low-level mosaicism or regulatory mechanisms may remain undetected.
Results: Physical examination revealed widespread hyperpigmented plaques. Histopathology confirmed mature adipocytes within the superficial to mid-dermis, consistent with NLS. Under our detection thresholds, we did not identify any pathogenic or likely pathogenic variants from WES or WGS. WES revealed 24 variants of uncertain significance, none of which were compelling for phenotype/pathway relevance. WGS did not identify pathogenic coding or non-coding variants, structural variations, copy number variations, or mitochondrial mutations. No pathogenic mutation was detected, suggesting alternative genetic mechanisms may be involved.
Conclusion: This case represents a rare presentation of extensive NLS with associated pain. Comprehensive genetic analysis did not identify pathogenic variants under our detection thresholds, while suggesting possible somatic mosaicism, recessive inheritance, or non-coding region variations.
Keywords: nevus lipomatosus superficialis, whole exome sequencing, whole genome sequencing, genetic analysis, genetic mechanisms
Introduction
Nevus lipomatosus superficialis (NLS) is an uncommon benign skin condition first described by Hoffman and Zurhelle in 1921.1 It is characterized histologically by the presence of ectopic mature adipocytes within the dermis. Clinically, NLS presents in two forms: the classic type features multiple lesions typically distributed along Blaschko’s lines, while the solitary form presents as an isolated lesion.2
The pathogenesis of NLS remains poorly understood. Current hypotheses suggest that some cases may arise from postzygotic somatic mosaicism, though the underlying genetic drivers remain largely unidentified.3 While the genetic basis is largely unknown, a cytogenetic study reported a 2p24 deletion in one case,4 and a recent molecular study identified PLAG1 overexpression and a specific COL3A1::PLAG1 gene rearrangement,5 implicating dysregulated adipogenesis in its etiology.6 However, most cases still lack a defined genetic abnormality. Extensive/generalized NLS is rarely reported, and symptomatic presentations with pain or recurrent infection are even less common. The extensive, painful, and recurrently infected variant of NLS, as presented here, represents a particularly rare and clinically challenging phenotype.
Because severe/extensive NLS may suggest mosaicism or rare genetic etiologies, we performed trio-WES and lesional WGS to search for germline and somatic mechanisms.7 We present a comprehensive clinical and genetic characterization of a 17-year-old female with extensive, painful NLS, incorporating both WES and WGS to systematically investigate potential genetic mechanisms underlying this rare disorder.
Case Presentation
Study Design and Patient
We conducted a detailed clinical, histopathological, and genetic investigation of a single patient with extensive NLS. The study was approved by the Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University. Written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images. The guardian provided explicit consent for the use of the patient’s anonymized clinical details and photographs.
Clinical Fundings
The patient, a 17-year-old female, presented with extensive, confluent hyperpigmented plaques involving the trunk, buttocks, lower extremities, and vulva (Figure 1). Lesions had developed progressively over 7 years and were associated with significant pain and recurrent infection, particularly on the back. The patient’s grandparents were first cousins (consanguineous); both parents were phenotypically unaffected.
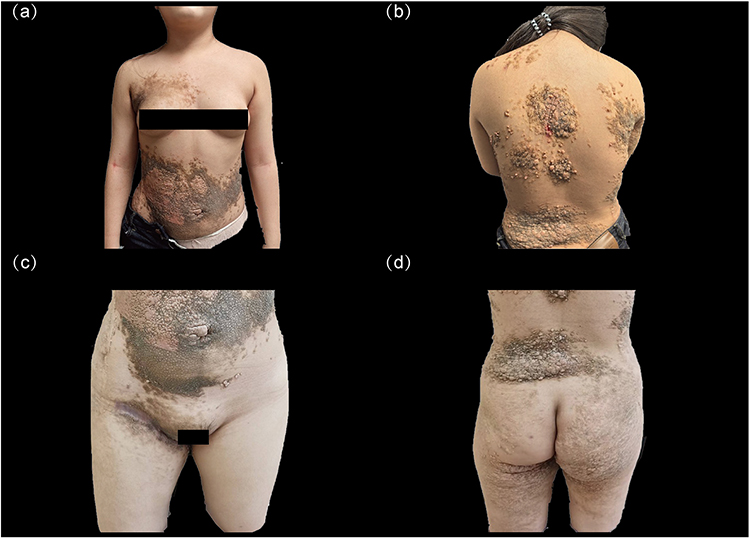 |
Figure 1 Nevus lipomatosus superficialis. Clinical presentation of the extensive and painful variant in a 17-year-old female. (a) Hyperpigmented and hyperplastic plaques on the anterior trunk. (b) Confluent hyperpigmented plaques on the posterior trunk. (c) Close-up view showing lesions involving the trunk and vulva. (d) Extensive involvement of the back, buttocks, and lower extremities. |
Diagnostic Workup
Histopathological Examination
Biopsy specimens revealed epidermal hyperplasia with hyperkeratosis. The superficial to mid-dermis contained mature adipocytes arranged in cord-like and nest-like structures embedded among collagen bundles (Figure 2), diagnostic of NLS. No notable findings beyond dermal adipocytes (such as adnexal involvement or inflammatory changes consistent with infection) were observed.
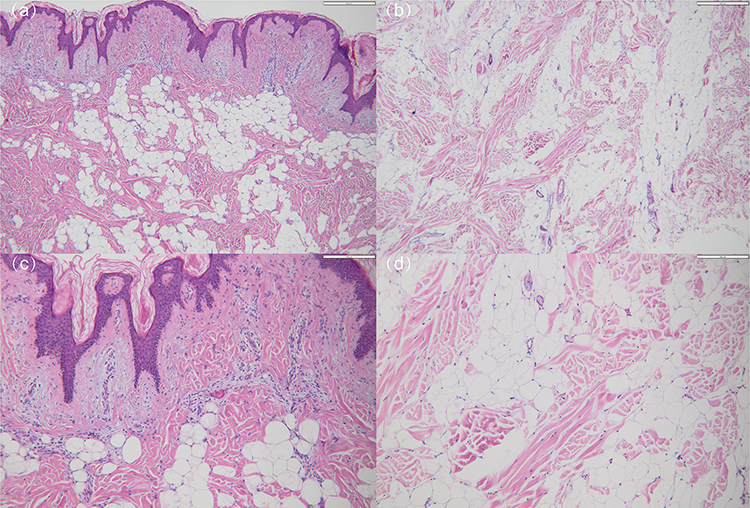 |
Figure 2 Nevus lipomatosus superficialis. Histopathological features (H&E staining). (a) Low-power view (×40, scale bar = 500 μm) of the epidermis and superficial dermis showing epidermal hyperplasia and scattered mature adipocytes. (b) Low-power view (×40, scale bar = 500 μm) of the mid-dermis revealing cord-like and nest-like arrangements of adipocytes embedded among collagen bundles. (c) High-power view (×100, scale bar = 500 μm) of the area in panel “a”, better demonstrating the ectopic adipocytes within the superficial dermis. (d) High-power view (×100, scale bar = 500 μm) of the area in panel “b”, highlighting the mature cytology of the ectopic adipocytes. |
Genetic Analysis
Sample Types and Contributions
Blood trio (proband + both parents) for WES: Peripheral blood samples were collected from the proband and both parents. WES was performed with inheritance-model filtering performed for de novo, recessive, compound heterozygous, and X-linked inheritance patterns. No pathogenic or likely pathogenic variants were identified.
Lesional tissue types: Formalin-fixed paraffin-embedded (FFPE) tissue from the patient’s lesion underwent WES (QC successful). Fresh lesional tissue underwent WGS (QC successful). Both tissue types were used to maximize detection of somatic variants and to compare variant calling across different sample preparations.
Somatic Variant Calling Parameters
For somatic variant calling, blood-derived DNA was used as the matched normal comparator. The minimum variant allele frequency (VAF) threshold for somatic calling was set at 5%. Mean sequencing depth was >50× for WGS and >100× for WES. A complete summary of sequencing quality metrics and coverage is provided in Supplementary Table 1. Lesional tissue cellularity was estimated at approximately 70%; therefore, low-level mosaicism below the 5% VAF threshold cannot be excluded. We do not claim “no mosaicism”; rather, we state that no pathogenic variants were identified under our detection thresholds.
Variant Interpretation
For both WES and WGS datasets, the pathogenicity of identified variants was interpreted according to the American College of Medical Genetics and Genomics (ACMG) guidelines, involving filtering against population frequency databases (eg, gnomAD) and utilizing in silico prediction tools (eg, REVEL).
Management and Follow-Up
Based on medical records from our institution, the patient received treatment for recurrent infections. Antibiotic therapy included oral minocycline capsules (50 mg twice daily) and topical mupirocin ointment. After treatment, clinical improvement was noted. The patient was followed up, during which a reduction in infection frequency and alleviation of pain were observed.
Genetic Fundings
WES Analysis
WES analysis did not identify any pathogenic or likely pathogenic variants. A total of 24 variants of uncertain significance (VUS) were identified; however, none were considered compelling for phenotype or pathway relevance based on current skin/adipose biology evidence. The complete list of VUS is provided in Supplementary Table 2.
WGS Analysis
Comprehensive genome-wide analysis identified no pathogenic structural variants, copy number variations, uniparental disomy, or mitochondrial mutations. No additional coding or non-coding variants of clear clinical significance were detected. Our SV/CNV pipeline is expected to detect structural variants larger than 1 kb; smaller rearrangements or complex structural variants below this resolution may remain undetected. A summary of all genetic findings and their clinical interpretations is presented in Supplementary Table 3.
Discussion
This case is remarkable for the extensive distribution of NLS and the presence of pain and recurrent infection, which are uncommon features that significantly impact quality of life.8 This case provides insight into the genetic heterogeneity of NLS and the challenges of identifying pathogenic mutations.
The absence of pathogenic findings despite extensive analysis contrasts with emerging genetic evidence in NLS, such as the 2p24 deletion and the recently reported COL3A1::PLAG1 rearrangement which drives adipocyte proliferation.9 Under our analytic pipeline and coverage thresholds, we did not identify any pathogenic or likely pathogenic variants. Our WGS robustly excluded large structural variations (detection threshold: >1 kb for SVs/CNVs). However, what remains possible includes: low-level mosaicism (below our 5% VAF threshold), variants in low-mappability regions of the genome, complex structural variants below our 1 kb detection resolution, and epigenetic mechanisms not assessable by WGS alone.
Although the consanguineous background raises the theoretical possibility of autosomal recessive inheritance, this alone is insufficient to support such a conclusion without identification of pathogenic variants or evidence of carrier status.10 No biallelic pathogenic variants were identified, and this hypothesis remains unsubstantiated without genetic evidence. This point should be interpreted more cautiously.
The proposed alternative mechanisms (such as variants of uncertain significance, somatic mosaicism, and recessive inheritance) would benefit from deeper contextualization within existing literature to clarify whether these hypotheses are supported by prior evidence or represent novel insights. A key limitation is the investigation of a single case. Future studies should employ transcriptomic analysis or deep sequencing of multiple tissue samples to probe for somatic mutations and regulatory defects.11
Further mechanistic studies may clarify somatic or regulatory contributions and guide targeted management. Defining these mechanisms will be crucial for understanding this rare condition.
Conclusion
Implications: In this case of extensive and painful NLS, comprehensive trio-WES (blood) and lesional WGS did not identify pathogenic germline or somatic variants under our detection thresholds. These negative results exclude known pathogenic mechanisms within the limits of our analysis but do not rule out low-level mosaicism, variants in non-coding regions, or epigenetic mechanisms.12 This case highlights the genetic heterogeneity of NLS and underscores the need for further mechanistic studies, including transcriptomic analysis and deep sequencing, to clarify the etiology of this rare condition. The findings also emphasize the importance of cautious interpretation of negative genetic results in clinical practice.13
Patient Consent Statement
Written informed consent was obtained from the patient’s legal guardian(s) for the publication of this case report and any accompanying images. The guardian provided explicit consent for the use of the patient’s anonymized clinical details and photographs. This consent for publication is separate from the general informed consent for participation. A copy of the signed consent form is available for review by the Editor-in-Chief.
Funding
Our work was supported by the National Natural Science Foundation of China (NSFC) (82273551).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hoffman E, Zurhelle E. Uberneinen Naevus lipomatodes cutaneus superficialis der linken Glutaagegend. Arch Dermatol Syphilol. 1921;130:327–5. doi:10.1007/BF01826150
2. Ioannidou DJ, Stefanidou MP, Panayiotides JG, Tosca AD. Nevus lipomatosus cutaneous superficialis (Hoffmann-Zurhelle) with localized scleroderma like appearance. Int J Dermatol. 2001;40(1):54–57. doi:10.1046/j.1365-4362.2001.01067-3.x
3. Alsalman HH, Alhallaf RA, Alhuzaimi A, Alhumidi AA, Alakeel A, Alsaif FM. Hairy nevus lipomatosus cutaneous superficialis: a rare presentation. JAAD Case Rep. 2020;6(10):1116–1118. doi:10.1016/j.jdcr.2020.07.030
4. Cardot-Leccia N, Italiano A, Monteil MC, Basc E, Perrin C, Pedeutour F. Naevus lipomatosus superficialis: a case report with a 2p24 deletion. Br J Dermatol. 2007;156(2):380–381. doi:10.1111/j.1365-2133.2006.07622.x
5. Yu W, Zhu X, Nohr E. Novel finding of PLAG1 overexpression and COL3A1::PLAG1 rearrangement in nevus lipomatosus superficialis. Pediatr Dev Pathol. 2025;28. doi:10.1177/1093526625137608
6. Baraldi C, Barisani A, Fanti PA, Patrizi A. Clinical, dermoscopic and histopathological features of solitary nevus lipomatosus cutaneous superficialis. Indian J Dermatol Venereol Leprol. 2021;87(3):399–401. doi:10.25259/IJDVL_399_19
7. Arasheben A, Prasad V, Frugoli A, Barr S. Nevus lipomatosus superficialis in a serous inflammatory capsule: a case report. Am J Case Rep. 2022;23:e937969.
8. Yang JW, Park MO. The nevus lipomatosus superficialis of face: a case report and literature review. Arch Plast Surg. 2024;51(2):196–201. doi:10.1055/a-2222-1226
9. Bergonse FN, Cymbalista NC, Nico MM, et al. Giant nevus lipomatosus cutaneus superficialis: case report and review of the literature. J Dermatol. 2000;27(1):16–19. doi:10.1111/j.1346-8138.2000.tb02110.x
10. Sawada Y. Solitary nevus lipomatosus superficialis on the forehead. Ann Plast Surg. 1986;16(4):356–358. doi:10.1097/00000637-198604000-00011
11. Cali JJ, Russell DW. Characterization of human sterol 27-hydroxylase. A mitochondrial cytochrome P-450 that catalyzes multiple oxidation reaction in bile acid biosynthesis. J Biol Chem. 1991;266(12):7774–7778. doi:10.1016/S0021-9258(20)89517-9
12. Baggen J, Jacquemyn M, Persoons L, et al. TMEM106B is a receptor mediating ACE2-independent SARS-CoV-2 cell entry. Cell. 2023;186(16):3427–3442. doi:10.1016/j.cell.2023.06.005
13. Medell-Gago M, Guerra-Guerra T, González-Pérez O, Concepción-Quiñones L. Nevo lipomatoso cutáneo superficial. Comunicación de 4 casos incluyendo una presentación inusual asociada a lipoma gigante y lipomatosis difusa [Nevus lipomatosus cutaneous superficialis. Report of four cases including an unusual presentation associated with massive lipomas and diffuse lipomatosis]. Rev Esp Patol. 2018;51(1):37–43. doi:10.1016/j.patol.2017.03.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.