Back to Journals » The Application of Clinical Genetics » Volume 19
Genealogical Identification and Short Tandem Repeat-Based Verification of Suspected Consanguinity in Mongolian Families
Authors Tsend-Ayush A ![]() , Tumurbaatar S
, Tumurbaatar S ![]() , Baatar B, Ganbaatar E, Davaasuren O
, Baatar B, Ganbaatar E, Davaasuren O ![]() , Dagvajantsan B, Dashtseren M
, Dagvajantsan B, Dashtseren M ![]() , Unurjargal T
, Unurjargal T ![]() , Nyamdavaa K, Jav S
, Nyamdavaa K, Jav S ![]() , Chimeddorj B
, Chimeddorj B
Received 17 November 2025
Accepted for publication 18 June 2026
Published 9 July 2026 Volume 2026:19 577541
DOI https://doi.org/10.2147/TACG.S577541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Altansukh Tsend-Ayush,1 Suvd Tumurbaatar,2 Buyandelger Baatar,3 Erdenetuya Ganbaatar,4 Oyunsuren Davaasuren,5 Byambasuren Dagvajantsan,6 Myagmartseren Dashtseren,7 Tsolmon Unurjargal,8 Khurelbaatar Nyamdavaa,9 Sarantuya Jav,1,2 Battogtokh Chimeddorj2
1Department of Molecular Biology and Genetics, School of Biomedicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 2Institute of Biomedical Sciences, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 3Genetic Laboratory, Bonavita Clinical Laboratory, Ulaanbaatar, Mongolia; 4Department of Pediatrics, School of Medicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 5Department of Mental Health, School of Medicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 6Department of Neurology, School of Medicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 7Department of Family Medicine, School of Medicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 8Department of Cardiology, School of Medicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 9Department of Physiology, School of Biomedicine, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia
Correspondence: Battogtokh Chimeddorj, Email [email protected] Sarantuya Jav, Email [email protected]
Purpose: The prevalence of consanguineous marriages remains high in several regions worldwide, particularly the Middle East and South Asia, with a reported rate of 58%. However, the prevalence and genetic characteristics of consanguineous marriages in Mongolia are not well studied. This study aimed to estimate the frequency of consanguineous marriages in selected Mongolian populations, using genealogical and short tandem repeat (STR) analyses.
Patients and Methods: This cross-sectional study was conducted at the Institute of Biomedicine at the Mongolian National University of Medical Sciences. A total of 574 individuals from 185 families across 43 soums in three provinces (X1, X2, and X3) were included. Genealogical analysis was used to construct pedigree-based consanguinity profiles, and STR analysis was performed to validate biological relatedness in selected families.
Results: Seventeen families were consanguineous, with a mean inbreeding coefficient of 0.089 ± 0.136, whereas 42 families were classified as suspected consanguinity. Among the confirmed cases, seven families with complete biological samples were further analyzed using STR markers, of which five showed molecular evidence of consanguinity (probabilities, 76.18– 98.84%). The STR analysis of 29 families classified as suspected or non-consanguineous identified 13 families as non-consanguineous and 10 families showing possible or indeterminate relatedness. Notably, six families initially classified as suspected or non-consanguineous demonstrated molecular evidence of consanguinity (probabilities, 70.75– 99.85%). Genetic diversity analysis revealed reduced heterozygosity in offspring from consanguineous families (expected heterozygosity [HE] = 0.7580, observed heterozygosity[HO] = 0.7045) compared with offspring from non-consanguineous families (HE = 0.7858, HO = 0.8110), with a significant reduction in HO (p = 0.0009).
Conclusion: This study demonstrates the value of integrating genealogical and STR-based molecular approaches for the assessment of consanguinity in Mongolia. Molecular analyses identified consanguineous relationships that were not evident from pedigree information alone and revealed reduced genetic diversity among offspring from consanguineous families. These findings provide important baseline data for understanding the genetic consequences of consanguinity in the Mongolian population and support the need for large scale epidemiological and genetic investigation.
Keywords: family, blood relatives, consanguinity degree, genetic analysis
Introduction
Consanguinity is defined as the union of biologically related individuals who share a certain percentage of genetic information.1,2 Consanguineous marriages remain common in several areas of the world and are influenced by religious, ethnic, cultural, social, and geographical factors. Approximately 20% of the global population prefers consanguineous marriages, depending on religion, race, ethnicity, sociocultural factors, and region.3 Although consanguineous marriages are rare in most developed countries, they are common in some developing countries. Legal restrictions on consanguineous marriage vary considerably between countries.4,5 Ancient traditions of marrying a relative or member of a tribe persist in the Middle East, North Africa, and South Asia.6 As of 2017, the prevalence of consanguineous marriages was 51–58% in Jordan, 54% in Kuwait, 49–33% in Tunisia and Morocco, 58% in Saudi Arabia, 50% in the United Arab Emirates, 52% in Qatar, 40–47% in Yemen, and as high as 68% in Alexandria, Egypt.6
Consanguineous marriages have important medical, social, and economic consequences, as they increase the probability of homozygosity for deleterious recessive alleles and may increase the risk of hereditary disorders, congenital anomalies, and adverse reproductive outcomes. The frequency of congenital disorders is significantly higher among offspring of consanguineous unions.7,8
Despite the well-documented effects of consanguinity in many populations, information on its prevalence and consequences in Mongolia remains limited. In Mongolia, congenital anomalies and inherited disorders continue to be reported across different provinces; however, the contribution of consanguinity to these conditions remains poorly understood.7,8 Consanguineous marriages have not been systematically investigated because of the limited number of studies and various socioeconomic factors. A study suggested that the historically endogamous population structure of Mongolians may have contributed to an increased probability of consanguineous unions within the population.9 However, the prevalence, patterns, and degree of consanguinity among Mongolian families have not been established.
Population migration and demographic changes may influence marriage patterns in Mongolia. Mongolia is divided into 21 provinces, 330 soums, and 1639 administrative subdivisions.7,8 The decline in rural populations due to migration to Ulaanbaatar may contribute to increased geographic and social isolation in some regions, potentially affecting relatedness and marriage patterns.7,8
Genealogical analysis is a practical and informative tool for investigating family history, identifying hereditary disorders, and detecting the patterns and degrees of consanguinity among relatives.10,11 Short tandem repeat (STR) analysis is a widely used molecular approach for assessing biological relatedness and kinship using highly polymorphic DNA markers.7,8 Hence, the combined use of genealogical investigations and STR-based analyses can provide reliable evidence for assessing suspected consanguinity.
To date, no integrated study combining genealogical assessments and STR-based molecular verification of consanguinity has been conducted in Mongolia. Furthermore, important parameters, such as consanguinity patterns, relatedness degree, and inbreeding coefficients, among Mongolian families remain largely unknown. Therefore, this study aimed to identify suspected consanguinity in Mongolian families using genealogical analysis and verify the degree of biological relatedness using STR-based molecular analysis.
Materials and Methods
This was a cross-sectional study conducted at the Institute of Biomedical Sciences, Mongolian National University of Medical Sciences. A total of 574 individuals from 185 families representing 43 soums in 3 provinces (X1, X2, and X3) in Mongolia were included in the study.
Written informed consent was obtained from all adult participants, and consent for minors was obtained from their legal guardians. Written consent was also obtained from the legal guardians of participants who lacked the mental capacity to understand the information or the ability to communicate their consent because of incapacitation. The consent form included patients’ identifiable information, and these features will be used in future analyses and publications. To protect patient confidentiality, all direct identifiers, including names, initials, dates of birth, and specific geographical locations, were removed. Pedigree charts were simplified to display only essential genetic transmission patterns, and non-essential clinical features or timeline details were generalized to ensure that individuals could not be identified. No personally identifiable information was used in any publication or analysis. All data were anonymized and de-identified prior to analysis.
Sample Size
Participant recruitment and data collection were conducted in collaboration with province-level healthcare centers. The study included 574 participants from 185 families, including husbands, wives, and children from families with suspected consanguinity. A purposive, non-probability sampling method was applied to targeted families with suspected consanguinity. Participants were selectively recruited according to predefined inclusion criteria for genealogical and STR-based analyses.
Ethical Approval
Ethical approval was obtained from the Medical Ethical Review Board of the Mongolian National University of Medical Sciences (Approval No. 2022/3-02, Approval date: February 18, 2022) and the Ethics Committee of the Ministry of Health, Mongolia (Approval No. 263, Approval date: June 24, 2022).
Study Settings
The participants were selected from provinces X1, X2, and X3 according to the inclusion criteria and were evaluated and diagnosed by a geneticist, psychiatrist, neurologist, cardiologist, and pediatrician. All medical histories and records of the participants were obtained from X.
Inclusion Criteria
Families were considered eligible for the investigation of suspected consanguinity if they met one or more of the following criteria: 1. reported or documented a history of consanguineous marriage as identified by health professionals; 2. suspicion of biological relatedness between spouses based on genealogical information or community history; 3. recurrent occurrence of congenital anomalies, congenital heart defects, intellectual disability, or hereditary disorders among family members across generations; 4. history of recurrent miscarriage or adverse reproductive outcomes in the family; and 5. availability and willingness of husbands and wives to participate in genealogical assessment and STR analysis.
The participants were required to be of Mongolian ethnicity, capable of understanding and responding to the study questionnaire, and willing to provide informed consent. For participants younger than 18 years, informed consent was obtained from a parent or legal guardian.
Exclusion Criteria
Families were excluded if they did not meet the predefined inclusion criteria. For the STR analysis, families with incomplete pedigree information, an insufficient number of participating family members, or inadequate biological samples were excluded.
Pedigree Analysis
A genealogical pedigree analysis was conducted using structured family history questionnaires administered by a trained genealogist.
Generation of Consanguineous Marriage Types
Consanguineous marriages were classified into three categories: first-, second-, and third-degree consanguinity. These categories were drawn using family pedigree as a model for consanguineous marriages. Marriage between a parent and their child or between siblingswas defined as first-degree consanguinity. Marriages involving an uncle, sister, or grandparent were considered second-degree consanguinity. Second cousin marriages were categorized as third-degree consanguinity.
Inbreeding Coefficient
The inbreeding coefficient (F) was estimated using pedigree-based analysis according to Wright’s method and was calculated using the following formula:

where  is the inbreeding coefficient of the individual being studied; the probability that two alleles at a locus are identical by descent,
is the inbreeding coefficient of the individual being studied; the probability that two alleles at a locus are identical by descent,  is thesummation of all possible common ancestors shared by the parents, and n represents the number of individuals in the pathways connecting the two parents through a common ancestor.
is thesummation of all possible common ancestors shared by the parents, and n represents the number of individuals in the pathways connecting the two parents through a common ancestor.
Blood Sample Collection
Peripheral blood samples were collected in ethylenediaminetetraacetic acid tubes from the study participants in a hospital setting for STR analysis.
DNA Isolation
DNA was isolated from whole blood using a DNA isolation kit (QIAamp DNA Blood Mini Kit) according to the manufacturer’s instructions. The DNA concentration was determined spectrophotometrically.
Specimen Dilution
DNA was diluted using Thermofisher 20X Low TE Buffer (pH 7.5) and nuclease-free deionized water. The DNA concentration was adjusted to 0.25ng/µL.
STR Amplification
The diluted DNA was amplified using the Thermofisher GlobalFiler Express PCR Amplification kit according to the manufacturer’s instructions, targeting 21 autosomal STRs and 3 Y chromosome STRs.
DNA Sequencing
Amplified DNA products were subjected to DNA sequencing on an Applied Biosystems (ABI) 3500 genetic analyzerusing the manufacturer’s reagents and protocols (Thermo Fisher Scientific, City, State, USA). Raw data generated by the 3500 Series Data Collection Software v4.0.2 wereimported into GeneMapper™ ID-X Software v1.6 for allelic designation. Peaks were detected in 21 autosomal loci, two loci on the Y chromosome, and the amelogenin locus, indicating that the alleles were fully identifiable.
Kinship analysis was performed using the GeneProof program based on the allelic frequency values of the family members involved in the study.
STR-based relatedness probabilities were operationally categorized as follows: The values between 0–30% were considered “non-consanguineous” for suspected consanguinity; 30–70% was considered “possible/indeterminate consanguinity” for suspected consanguinity; and 70–99% was considered “consanguineous” marriages for suspected consanguinity.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows version 25and Microsoft Excel software. Descriptive statistics, means, and standard deviations were calculated. Agreements and associations between pedigree-based classification and STR-based relatedness classification were evaluated using Fisher’s exact test. Statistical significance was set at p<0.05.
Results
This study included 574 individuals from 185 families, representing 43 soums across three provinces. Seventeen families within the regions covered by this study were confirmed by genealogical analysis to have consanguineous marriages. In addition, 42 families were suspected of having a high probability of consanguinity. Hence, a total of 59 families (31.9%) were identified as consanguineous marriages and suspected consanguinity (Table 1).
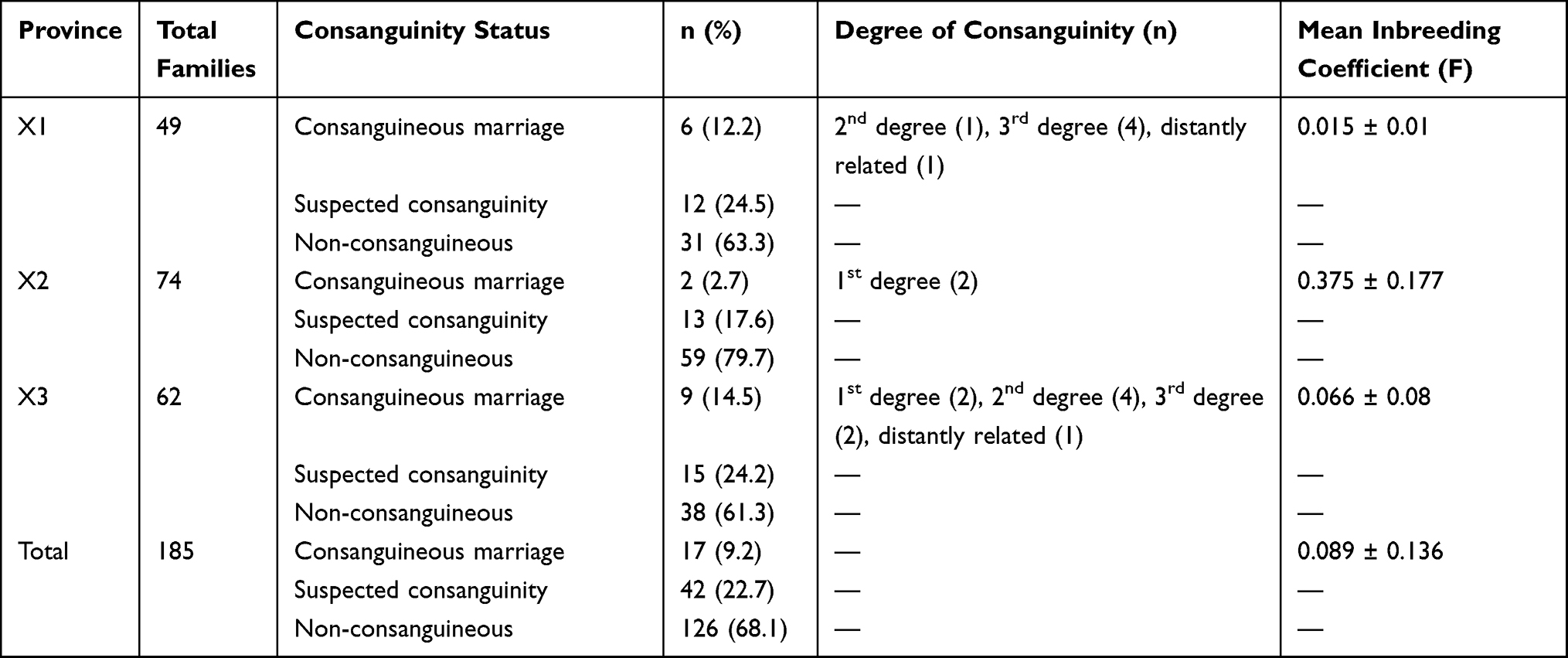 |
Table 1 Distribution and Degree of Consanguinity Among Participating Families |
Among the 49 families that participated in X1 province, six families were identified as consanguineous marriages by genealogical analysis, 12 families were likely to be suspected of consanguineous marriage, and 31 families were either unrelated or could not be determined in the study. Of the 74 families from X2 province, two families were identified as consanguineous marriages, 14 families were likely to be related, and 58 families were not related. Among the 62 families from X3 province, nine families were identified as having a consanguineous marriage, 15 families were suspected to have a consanguineous marriage, and 38 families were either unrelated or could not be determined in the study.
We categorized families with consanguineous marriages into four degrees of consanguinity. Among the participants from X1 province, four families had third degree of consanguinity, one family had second degree of consanguinity, and one family had distant consanguinity. For participants from X2 Province, first-degree consanguinity was observed in two families. In X3 province, two families had first-degree consanguinity, four families had second-degree consanguinity, two families had third-degree consanguinity, and one family had distant consanguinity. Accordingly, of the degree consanguinity range across provinces was estimated as follows: first-degree consanguinity, 23.5%; second-degree consanguinity, 29.4%; third-degree consanguinity, 35.3%; and distant consanguinity, 11.8%.
The inbreeding coefficient (F) for families with confirmed consanguineous marriages was calculated and averaged across the study regions. The average inbreeding coefficient was 0.089±0.136 (n = 17). The average inbreeding coefficient for X1, X2, and X3 provinces were 0.015±0.01, 0.375±0.177, and 0.066±0.08, respectively.
Furthermore, of the 17 genealogically confirmed families with consanguineous marriage, we selected seven families based on the following criteria and evaluated them to confirm consanguineous marriage. The requirements were that both spouses and their children in each family have to complete questionnaires with the blood samples provided. Based on these criteria, STR analysis was performed to investigate two STR markers on the Y chromosome (DYS391, Y indel): amelogenin for sex determination and 21 autosomal STR loci in the X1-28, X1-38, X1-44, X3-02, X3-08, X3-57, and X2-07.
We illustrated the consanguinity patterns in these families and observed different patterns depending on the degree of consanguinity. In family X1-28, the grandfathers of the husband and wife were biological brothers (sibs), whereas in family X1-44, the husband and wife had different fathers but the same mother. As for–X1-38, the grandparents of the husband and wife were biological brother and sisters (sibs). In family X3-02, the husband and wife had the same father but different mothers, whereas in family X3-08, the husband and wife were the biological brothers and sisters of one grandfather’s father and the other grandfather’s mother. In families with the X3-57 code, the husband and wife’s mothers were biological sisters. X2-07 was not a marriage, but the child of the third-generation wife was her father’s; therefore, further genetic studies were needed for confirmation (Figure 1).
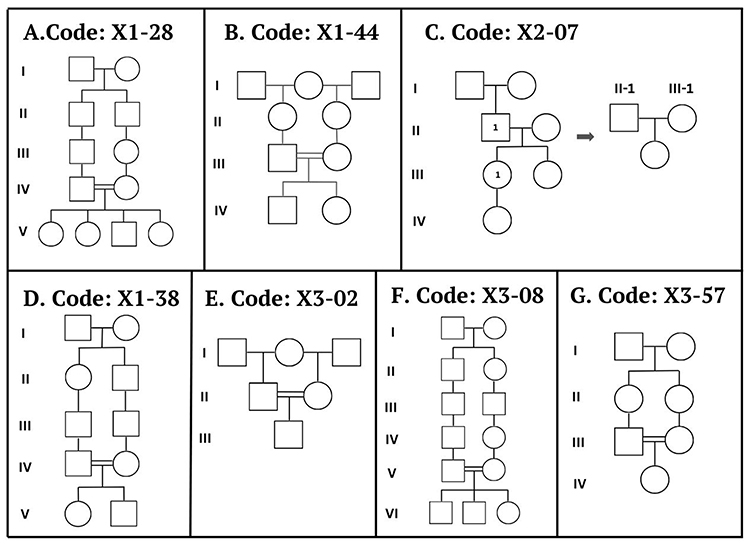 |
Figure 1 Consanguinity patterns for families with consanguineous marriages. (A–G) Pedigree diagrams of families X1-28, X1-44, X2-07, X1-38, X3-02, X3-08, and X3-57, respectively, showing familial relationships and consanguineous marriages identified through pedigree analysis. Roman numerals (I–VI) denote generations, starting from the oldest generation (I) to the most recent generation. Pedigree symbols follow standard conventions: squares represent males, circles represent females, horizontal lines represent unions, vertical lines represent descent, and double lines indicate consanguineous relationships. |
In determining the degree of consanguinity of these seven families, there were two families with first-degree of consanguinity, two families with second-degree of consanguinity, two families with third-degree of consanguinity, and one family with distant consanguinity.
Regarding the STR analysis results, a kinship analysis was used to evaluate families with consanguineous marriages. The percentages of shared alleles of autosomal STR markers between spouses in consanguineous families were 76.18% for X1-28 family, 86.91% for X1-38 family, 11% for X1-44 family, 98.78% for X3-02 family, 61.6% for X3-08 family, 94.26% for X3-57 family, and 99.84% for X2-07 family. These results confirm that spouses in families X1-28, X-38, X3-02, and X3-57, as well as among family members in X2-07, were biologically related. However, consanguineous marriages were not confirmed in families X1-44 and X3-08. Among the suspected and non-consanguine families, STR analysis was conducted on 29 families with complete questionnaires and blood samples.
Notably, six families, including one genealogically suspected consanguineous family and five non-consanguineous families, had consanguineous marriages. Table 2 shows a comparison of pedigree- and STR-based analyses for detecting consanguinity in the 13 families. Among the 13 families described, 11 were consistently identified as consanguineous using both pedigree- and STR-based analyses. A statistically significant association was observed between the pedigree-based classification and STR-based relatedness analysis (Fisher’s exact test, p = 0.028). These findings suggest a general consistency between genealogical assessment and molecular evidence for identifying consanguineous relationships.
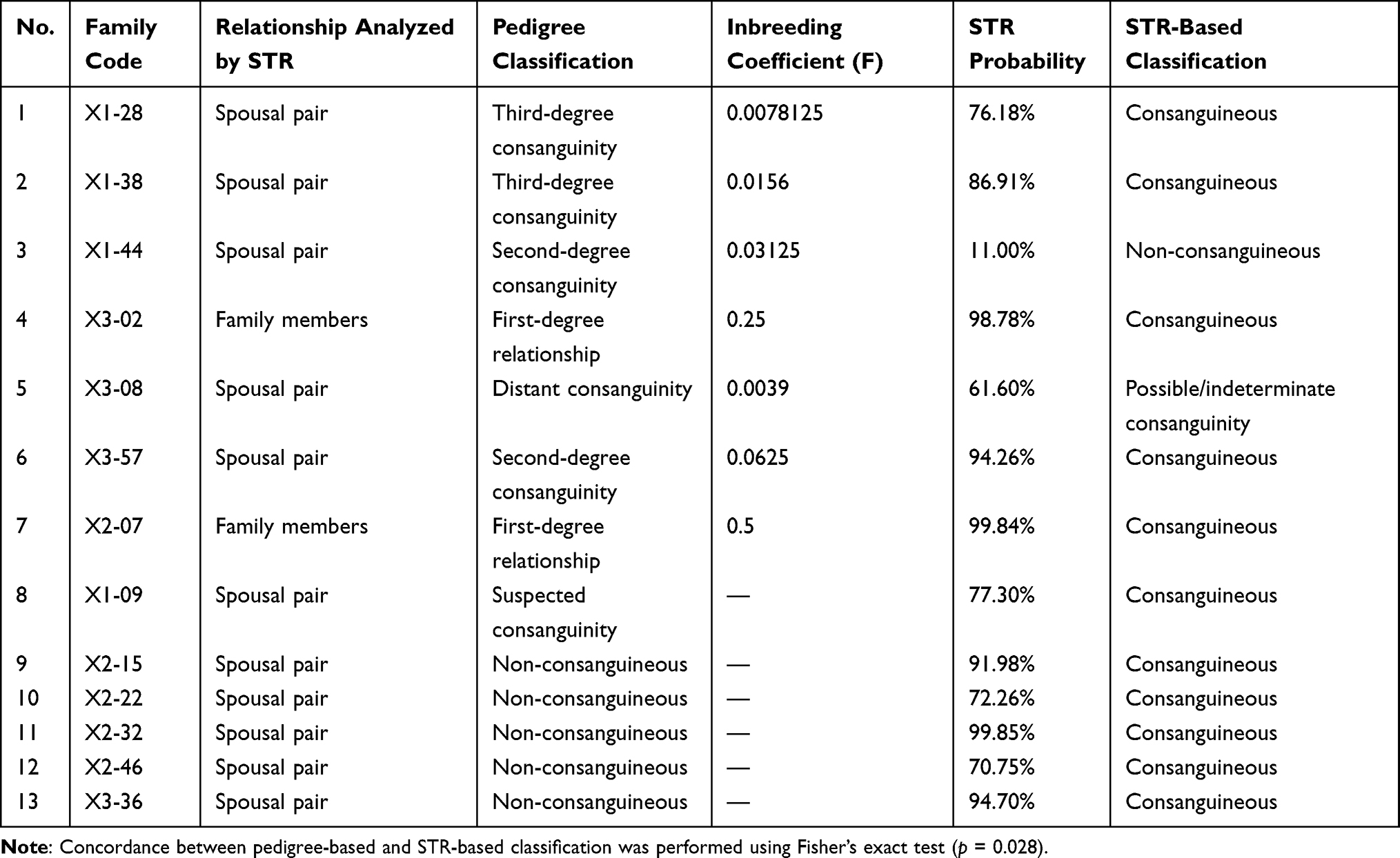 |
Table 2 Comparison of Pedigree Analysis and Short Tandem Repeat (STR)-Based Relatedness Among Investigated Families |
According to the results presented in Table 3, among the 23 families classified as non-consanguineous by pedigree analysis, 13 were confirmed as non-consanguineous based on STR analysis, whereas 10 families showed possible or indeterminate levels of consanguinity. Notably, some of these cases were initially classified as suspected consanguinity based on the pedigree information. Overall, these findings indicate that some families initially considered unrelated may present genetic evidence of distant or uncertain biological relationships.
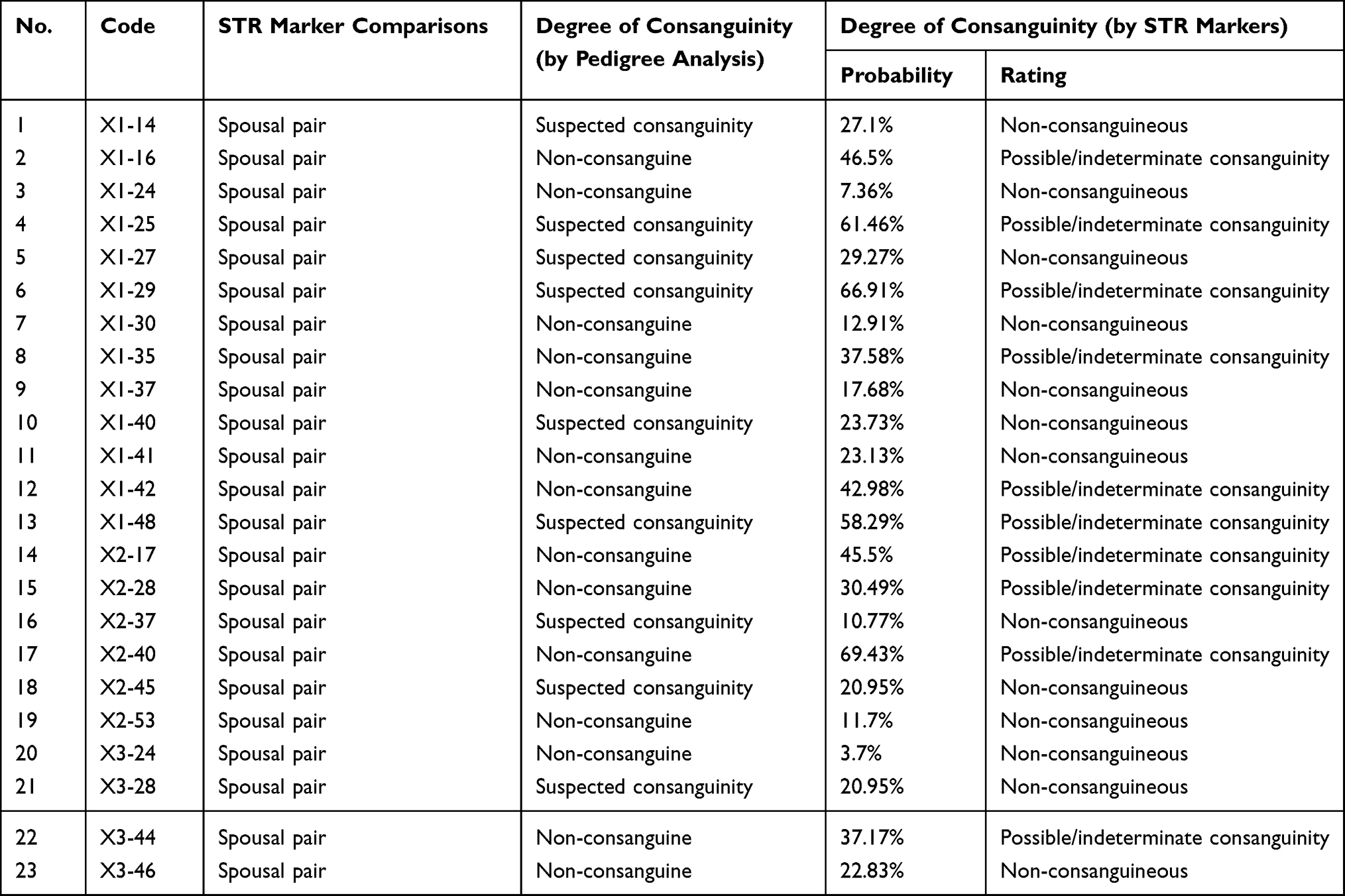 |
Table 3 Non-Consanguine Families Analyzed by Pedigree Analysis and Short Tandem Repeat (STR) Markers |
Significant differences in the mean gene diversity (expected heterozygosity, HE) were observed between consanguineous and non-consanguineous families (p = 0.006). Among the offspring, children from consanguineous families demonstrated significantly lower observed heterozygosity (HO) and a higher fixation index (f) than those from non-consanguineous families (p<0.05), indicating that reduced genetic variability and increased homozygosity are associated with consanguinity (Table 4).
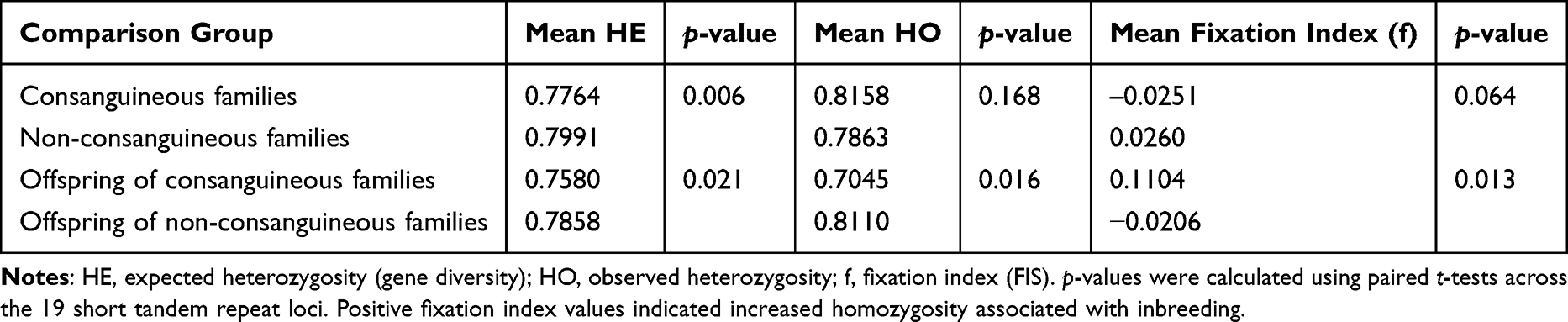 |
Table 4 Summary Comparison of Genetic Diversity and Heterozygosity Between Consanguineous and Non-Consanguineous Families and Their Offspring |
Among the children, variability in heterozygosity was locus dependent, with the SE33 marker showing the highest observed heterozygosity in both groups, whereas the D3S1358 marker exhibited comparatively lower values.
Discussion
Consanguineous marriage remains a decisive issue that should be considered not only internationally12–14 but also in Mongolia. By reducing the incidence of high-risk or consanguineous marriages, decreasing the prevalence and burden of genetic disorders is possible.15 Consanguineous marriage has multiple effects, such as impacting reproductive health; increasing the risk of having a child with birth defects, genetic disorders, and developmental disabilities; and increasing the frequency of chronic non-communicable diseases.16,17 Therefore, to prevent consanguineous marriages in Mongolia, detecting autosomal recessive genetic disorders17 and neurological and mental disorders (including intellectual disability)18–20 is necessary.
In this study, we investigated the incidence of consanguinity in a target population selected by non-probability sampling and assessed several relevant parameters. According to our findings, the incidence of genealogically confirmed consanguineous marriage and suspected consanguineous marriage was 9.19% and 22.7%, respectively. The findings of this study should be interpreted in light of several limitations. In particular, the number of confirmed consanguineous families was relatively small in some provinces, which may have influenced the observed regional estimates. Consequently, the higher mean values observed in certain areas may reflect sample size limitations rather than true population-level differences. Further studies with larger and more geographically representative samples are warranted to confirm these findings.
A nationwide study reported a consanguineous marriage prevalence of one in five families (20%) in the Turkish population.12 The prevalence of consanguineous marriages can vary across regions due to differences in religion, race, ethnicity, sociocultural factors, and regions.21,22
As the prevalence of consanguineous marriages in Mongolia has not yet been investigated at the nationwide level, future studies should comprehensively assess the prevalence of consanguineous marriagesnationwide among the total population and focus on measures to reduce consanguinity. Various strategiesare available to prevent genetic disorders, congenital anomalies, and autosomal recessive disorders associated with consanguineous marriages.17,23,24
Genetic counseling and confirmation tests for consanguineous and suspected consanguineous families have become increasingly important.13,25 Therefore, proposing genetic screening activities for both premarital and post-marriage couplesis necessary26,27 to identify blood relatives or consanguinity and offer appropriate genetic counseling services.
International premarital screening and genetic counseling were introduced in 2004 to detect hemoglobin disorders,26–28 particularly sickle cell anemia and thalassemia.29,30 Considering that it is an important public health indicator in many foreign countries, the significance of premarital genetic counseling and screening for couples of marriageable ages has been well established.26,31,32
The findings of this study highlight the potential value of genetic counseling and screening programs for the early identification and management of hereditary disorders in Mongolia. As genomic medicine becomes increasingly integrated into healthcare systems worldwide, understanding the genetic characteristics of the Mongolian population may contribute to the development of more effective prevention and intervention strategies. Given the country’s unique demographic and population structure, genetic services should be evaluated within the context of local healthcare needs and resources. However, the implementation of such programs requires careful consideration of ethical, social, and cultural factors. Ensuring informed consent, protecting privacy, and minimizing the risk of stigma or discrimination will be essential for the responsible use of genetic information. In addition, improving genetic literacy among healthcare professionals and the public may facilitate the appropriate interpretation and application of genetic data. Further population-based studies are warranted to better characterize genetic variation and hereditary disease burden in Mongolia and to inform evidence-based approaches to genetic counseling and screening.
Conclusions
This study demonstrates the value of integrating genealogical and STR-based molecular approaches for the assessment of consanguinity in Mongolia. Molecular analyses identified consanguineous relationships that were not evident from pedigree information alone and revealed reduced genetic diversity among offspring from consanguineous families. These findings provide important baseline data for understanding the genetic consequences of consanguinity in the Mongolian population and support the need for large scale epidemiological and genetic investigation.
Abbreviations
STR, short tandem repeat; HE, expected heterozygosity; HO, observed heterozygosity; F, inbreeding coefficient; FIS, fixation index.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Inform Consent
The study was conducted in accordance with the principles of the Declaration of Helsinki. The Institutional Review Board Committee of Mongolian National University of Medical Sciences approved the study protocol (Approval No. 2022/3-02, Approval date: February 18, 2022) and the Ethics Committee of the Ministry of Health, Mongolia (Approval No. 263, Approval date: June 24, 2022).
Acknowledgments
The authors express their sincere gratitude to Professor Damdindorj Boldbaatar for his administrative and institutional support. We also extend our deep appreciation to Professor Khishigsuren Zuunnast (Department of Mental Health, School of Medicine, Mongolian National University of Medical Sciences [MNUMS]) and Professor Purevdorj Ichinchorloo for their expert supervision. Special thanks are due to PhD. Khongorzul Batchuluun (Institute of Biomedical Sciences, MNUMS) MSc. Elberelt Unurbat (Institute of Biomedical Sciences, MNUMS), Dr. Anujin Tseveenjav (Institute of Biomedical Sciences, MNUMS), PhD. Tsevelmaa Nanjidsuren (Institute of Biomedical Sciences, MNUMS), MSc. Purevdorj Munkhuu (Department of Molecular Biology and Genetics), PhD Otgontsetseg Erdenebayar (Department of Molecular Biology and Genetics), Assoc.Prof. Munkhtsetseg Bazarragchaa (Department of Molecular Biology and Genetics), MSc Khaliun Battumur (Department of Molecular Biology and Genetics), and MSc. Otgonbyamba Dashdorj (Bonavita Clinical Laboratory) for their invaluable contributions to the methodology, data collection, and clinical analysis phases of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the project (Project No. ШУТБИХХЗГ-2022/94) of the Foundation of Science and Technology of Mongolia and an internal grant (Project No. 2022/23) from the Science and Technology Foundation, Mongolian National University of Medical Sciences, Mongolia.
Disclosure
The authors have no competing interests to declare.
References
1. Fareed M, Afzal M. Genetics of consanguinity and inbreeding in health and disease. Ann Hum Biol. 2017;44(2):99–11. doi:10.1080/03014460.2016.1265148
2. Alvarez G, Quinteiro C, Ceballos FC. Inbreeding and genetic disorder. Adv Study Genet Disord. 2011;21–44.
3. Bener A, Mohammad RR. Global distribution of consanguinity and their impact on complex diseases: genetic disorders from an endogamous population. Egypt J Med Hum Genet. 2017;18(4):315–320. doi:10.1016/j.ejmhg.2017.01.002
4. Bittles A. A community genetics perspective on consanguineous marriage. Public Health Genomics. 2008;11(6):324–330. doi:10.1159/000133304
5. Saputra RA, Sanjaya UH. Legal construction of consanguineous marriages (analysis of article 8 of law number 1 of 1974 concerning marriage). Perspektif Hukum. 2023;239–261.
6. Parkin R. Arranged marriages: whose choice and why? Reflections on the principles underlying spouse selection worldwide. History Anthropol. 2021;32(2):271–287. doi:10.1080/02757206.2021.1905255
7. Islam MM. The practice of consanguineous marriage in Oman: prevalence, trends and determinants. J Biosoc Sci. 2012;44(5):571–594. doi:10.1017/S0021932012000016
8. Hamamy H, Alwan S. The sociodemographic and economic correlates of consanguineous marriages in highly consanguineous populations. In: Genomics and Society. Academic Press; 2016;335–361.
9. Yang X, Sarengaowa, He G, et al. Genomic insights into the genetic structure and natural selection of Mongolians. Front Genetics. 2021;12:735786. doi:10.3389/fgene.2021.735786
10. Bennett RL. The Practical Guide to the Genetic Family History. John Wiley & Sons; 2011.
11. Hunter-Zinck H, Musharoff S, Salit J, et al. Population genetic structure of the people of Qatar. Am J Hum Genet. 2010;87(1):17–25. doi:10.1016/j.ajhg.2010.05.018
12. Kaplan S, Pinar G, Kaplan B, et al. The prevalence of consanguineous marriages and affecting factors in Turkey: a national survey. J Biosoc Sci. 2016;48(5):616–630. doi:10.1017/S0021932016000055
13. Nouri N, Nouri N, Tirgar S, et al. Consanguineous marriages in the genetic counseling centers of Isfahan and the ethical issues of clinical consultations. J Med Ethics History Med. 2017;10:12.
14. Do Q-T, Iyer S, Joshi S. The economics of consanguineous marriage. Rev Econom Stat. 2007;95.
15. Hamamy H. Consanguineous marriages: preconception consultation in primary health care settings. J Commun Genet. 2012;3(3):185–192. doi:10.1007/s12687-011-0072-y
16. Anwar S, Taslem Mourosi J, Arafat Y, Hosen MJ. Genetic and reproductive consequences of consanguineous marriage in Bangladesh. PLoS One. 2020;15(11):e0241610. doi:10.1371/journal.pone.0241610
17. Khayat AM, Alshareef BG, Alharbi SF, AlZahrani MM, Alshangity BA, Tashkandi NF. Consanguineous marriage and its association with genetic disorders in Saudi Arabia: a review. Cureus. 2024;16(2):e53888. doi:10.7759/cureus.53888
18. Shawky RM, Elsayed SM, Zaki ME, Nour El-Din SM, Kamal FM. Consanguinity and its relevance to clinical genetics. Egypt J Med Hum Genet. 2013;14(2):157–164. doi:10.1016/j.ejmhg.2013.01.002
19. Ben-Omran T, Al Ghanim K, Yavarna T, et al. Effects of consanguinity in a cohort of subjects with certain genetic disorders in Qatar. Mol Genet Genomic Med. 2020;8(1):e1051. doi:10.1002/mgg3.1051
20. Merten M. Keeping it in the family: consanguineous marriage and genetic disorders, from Islamabad to Bradford. BMJ. 2019;365:l1851. doi:10.1136/bmj.l1851
21. Hussain R. 945Social and cultural aspects of customary consanguineous marriages in South Asia. In: Kumar D, editor. Genomics and Health in the Developing World. Oxford University Press; 2012.
22. Bittles A. A community genetics perspective on consanguineous marriage. Commun Genet. 2008;11(6):324–330.
23. Naibkhil N, Chitkara E. Consanguineous marriages increase risk of congenital anomalies-studies in four generation of an Afghan family. Biomed Res. 2016;27:34–39.
24. Bittles AH, Black ML. Consanguinity, human evolution, and complex diseases. Proc Natl Acad Sci. 2010;107(suppl_1):1779–1786. doi:10.1073/pnas.0906079106
25. Bennett R, Motulsky A, Bittles A, et al. Genetic counseling and screening of consanguineous couples and their offspring: recommendations of the national society of genetic counselors. J Genet Counseling. 2002;11(2):97–119. doi:10.1023/A:1014593404915
26. Bener A, Al-Mulla M, Clarke A. Premarital screening and genetic counseling program: studies from an endogamous population. Int J App Basic Med Res. 2019;9(1):20–26. doi:10.4103/ijabmr.IJABMR_42_18
27. Ibrahim NK, Bashawri J, Al bar H, et al. Premarital screening and genetic counseling program: knowledge, attitude, and satisfaction of attendees of governmental outpatient clinics in Jeddah. J Infect Public Health. 2013;6(1):41–54. doi:10.1016/j.jiph.2012.05.001
28. AlOtaiby S, Alqahtani A, Saleh R, Mazyad A, Albohigan A, Kutbi E. Comprehension of premarital screening and genetic disorders among the population of Riyadh. J Taibah Univ Sci. 2023;18(4):822–830. doi:10.1016/j.jtumed.2023.01.006
29. Alhamdan NA, Almazrou YY, Alswaidi FM, Choudhry AJ. Premarital screening for thalassemia and sickle cell disease in Saudi Arabia. Genet Med. 2007;9(6):372–377. doi:10.1097/GIM.0b013e318065a9e8
30. Memish ZA, Saeedi MY. Six-year outcome of the national premarital screening and genetic counseling program for sickle cell disease and β-thalassemia in Saudi Arabia. Ann Saudi Med. 2011;31(3):229–235. doi:10.4103/0256-4947.81527
31. Shiloh S, Reznik H, Bat-Miriam-Katznelson M, Goldman B. Pre-marital genetic counselling to consanguineous couples: attitudes, beliefs and decisions among counselled, noncounselled and unrelated couples in Israel. Soc Sci Med. 1995;41(9):1301–1310. doi:10.1016/0277-9536(94)00433-T
32. Elhadi YAM, Alrawa SS, Alfadul ESA, et al. Consanguinity and willingness to perform premarital genetic screening in Sudan. Eur J Hum Genet. 2023.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.