Back to Journals » Patient Preference and Adherence » Volume 17
Gene Therapy for Hemophilia A: A Mixed Methods Study of Patient Preferences and Shared Decision-Making
Authors Limjoco J, Thornburg CD ![]()
Received 14 February 2023
Accepted for publication 12 April 2023
Published 19 April 2023 Volume 2023:17 Pages 1093—1105
DOI https://doi.org/10.2147/PPA.S406894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Jacqueline Limjoco,1 Courtney D Thornburg1,2
1Hemophilia and Thrombosis Treatment Center, Rady Children’s Hospital San Diego, San Diego, CA, USA; 2Department of Pediatrics, UC San Diego School of Medicine, La Jolla, CA, USA
Correspondence: Courtney D Thornburg, Rady Children’s Hospital San Diego, 3020 Children’s Way, MC 5035, San Diego, CA, 92123, USA, Tel +1 858-966-5811, Fax +1 858-966-8035, Email [email protected]
Purpose: As gene therapies for hemophilia are incorporated into clinical practice, shared decision-making (SDM) is recommended for implementation. SDM tools may facilitate informed decision-making for gene therapy and other novel therapies.
Objective: To inform the development of SDM tools for hemophilia gene therapy.
Patients and Methods: Men with severe hemophilia were recruited from the National Hemophilia Foundation (NHF) Community Voices in Research (CVR). Semi-structured interviews were completed, and the interviews were transcribed verbatim for quantitative and qualitative analysis.
Results: Twenty-five men with severe hemophilia A participated. All participants reported treatment with prophylaxis, nine (36%) on continuous prophylaxis with clotting factor, one (4%) on intermittent prophylaxis with clotting factor, and 15 (60%) on continuous prophylaxis with emicizumab. Ten (40%) indicated that they are excited about gene therapy, 12 (48%) indicated that they are hopeful about gene therapy, one (4%) indicated that they are worried or scared about gene therapy, and one (4%) indicated that they do not have strong feelings about gene therapy. Participants reported engaging Hemophilia Treatment Center, family, and the hemophilia community in their decision-making process. The most reported information needs are efficacy, safety, cost/insurance, mechanism of action, and follow-up. In addition, key information themes that emerged were patient testimonials, hard data and statistics, and comparison to other products. Twenty-two (88%) indicated that a SDM tool would be useful when discussing gene therapy with their hemophilia team. Two indicated that they do their own research, and the tool would not add anything. One needed more information to provide an answer.
Conclusion: These data highlight the utility of a SDM tool for hemophilia gene therapy and key information needs. Data including comparison to other treatments should be provided along with patient testimonials in a transparent format. Patients will engage the Hemophilia Treatment Center, family, and community members in the decision-making process.
Keywords: gene transfer, patient preferences, interviews, factor VIII deficiency
Introduction
Gene transfer is an emerging therapy for individuals with severe hemophilia. The first gene transfer product for hemophilia A (HA) was approved by the European Commission in August 2022 and the first product for hemophilia B (HB) was approved by the US Food and Drug Administration in November 2022; additional approvals are expected over the next few years. Gene transfer adds to the therapeutic options for prevention of spontaneous and traumatic bleeding in adults with hemophilia. Based on clinical trial data, response varies between HA and HB gene therapy (GT) and there is intra-patient variability in regard to factor expression, durability, and side effect profile.1 Shared decision-making (SDM) tools are needed to ensure that both the person with hemophilia (PwH) and health professionals have balanced information about each treatment option and that they can discuss the options in the context of treatment attributes which matter most to the patient as well as the PwH’s treatment goals and any barriers to treatment.2–4 Overall, these should increase access to treatment, reduce decisional conflict, and improve the patient experience.
PwH have a lifetime of experience and are considered subject matter experts. The patient’s voice is key to the development of tools which can be used for SDM about hemophilia treatments. The “Exigency programme” in the United Kingdom was designed to explore knowledge, expectations, and GT among stakeholders including parents of children with hemophilia and men with hemophilia who have not wished to pursue GT or have had GT.5–7 These qualitative studies provide important data regarding information needs for a PwH considering GT. Wang et al developed a clinician-oriented shared decision-making Q&A resource based on roundtable discussions with health care professionals and patients in collaboration with the Bayer Global and European Patient Councils for Hemophilia and the Bayer Hemophilia Employee Council.2 The Q&A resource addresses questions related to treatment regimen/adherence requirements, treatment predictability and variability, treatment durability, and the risk: benefit profile; it is organized from initial information-seeking through short- and long-term follow-up.
To further inform the development and implementation of clinician and patient oriented SDM tools, we conducted a mixed methods study of men in the United States with severe HA to evaluate their current feelings and expectations about GT; information needs related to content, source, and mode of delivery; and preferences related to treatment discussions and SDM.
Materials and Methods
Study Design
The study was approved by the University of California, San Diego Office of IRB Administration, #201024 and was conducted in compliance with the Declaration of Helsinki The IRB approved verbal consenting. Participants informed consent included publication of anonymized responses.
Participant Recruitment and Study Population
The study population includes men with severe HA or HB who have enrolled in the National Hemophilia Foundation (NHF) Community Voices in Research (CVR) and speak English. Eligible men received an IRB approved study invitation email from NHF CVR. Participants contacted the study team at Rady Children’s Hospital San Diego. Participants provided verbal informed consent prior to study commencement.
Study Procedures
Interview Guide Development
A semi-structured interview guide was developed by the principal investigator (PI) based on clinical expertise, review of the literature, and results of a prior survey of men with hemophilia.8 One of the clinical research coordinators (CRC) provided feedback on readability and content. The interview guide included discrete choice questions about sociodemographics and clinical characteristics as well as open-ended questions. Part I of the interview introduced the topic of GT and other novel therapies for hemophilia. Interview questions were open-ended. Part II of the interview included a discussion of experiences related to where patients learn about new therapies and how they make decisions. Part III of the interview was a narrowed, issue-focused discussion encouraging personal reflection about patient preferences and key factors which may influence decision-making about GT including required post-GT short- and long-term monitoring and follow-up. Transcripts were reviewed by the research team in between interviews and interview guides were updated throughout the study. Revisions included modifying the order of the interview questions, how the SDM concept was reviewed, adding questions about when PwH start to have active role in decision-making, adding information to respond to participants questions, and including more prompts.
Conduct of Interviews
Semi-structured interviews of approximately 60 minutes were conducted via telephone or web-conferencing platform by CRCs with expertise in hemophilia. The interviews were recorded when the participants permitted (one requested no recording) and transcribed verbatim using the HIPAA-compliant service TranscribeMe! (https://www.transcribeme.com/).
The target sample was 20 participants based on prior qualitative studies. The sample size was expanded until a diverse sample was enrolled and themes were saturated. Interviews were conducted in August and September 2021. Participants received a gift card for compensation of their time.
Analysis
The interviews resulted in two datasets. The first included self-reported sociodemographic and clinical factors and the second included transcribed text from each interview. Summary statistics were used to characterize the population.
The PI and a CRC conducted independent content analysis of the transcripts.9 The PI listened to each interview and read each interview transcript. Transcripts were coded using a priori codes from the literature and additional codes were added. A CRC reviewed the coding and added additional codes. Differences were resolved through consensus. Codes were organized by themes. Finally, the PI re-coded the transcripts using the final code book in the software program MAXQDA 2020 (Version 20.4.1).
Direct quotes from the participants are labelled with study numbers within the text and Supplementary Tables 1–4.
Results
Twenty-five men with severe HA participated in the study. Twenty-four (96%) speak English as their primary language and 15 (60%) reported White race. Seventeen (68%) had no history of inhibitor, four (16%) had a prior history of inhibitor, and three (12%) reported an active inhibitor. All participants reported treatment with prophylaxis, nine (36%) on continuous prophylaxis with clotting factor, one (4%) on intermittent prophylaxis with clotting factor, and 15 (60%) on continuous prophylaxis with emicizumab. Sociodemographic and clinical characteristics are shown in Table 1 and Table 2.
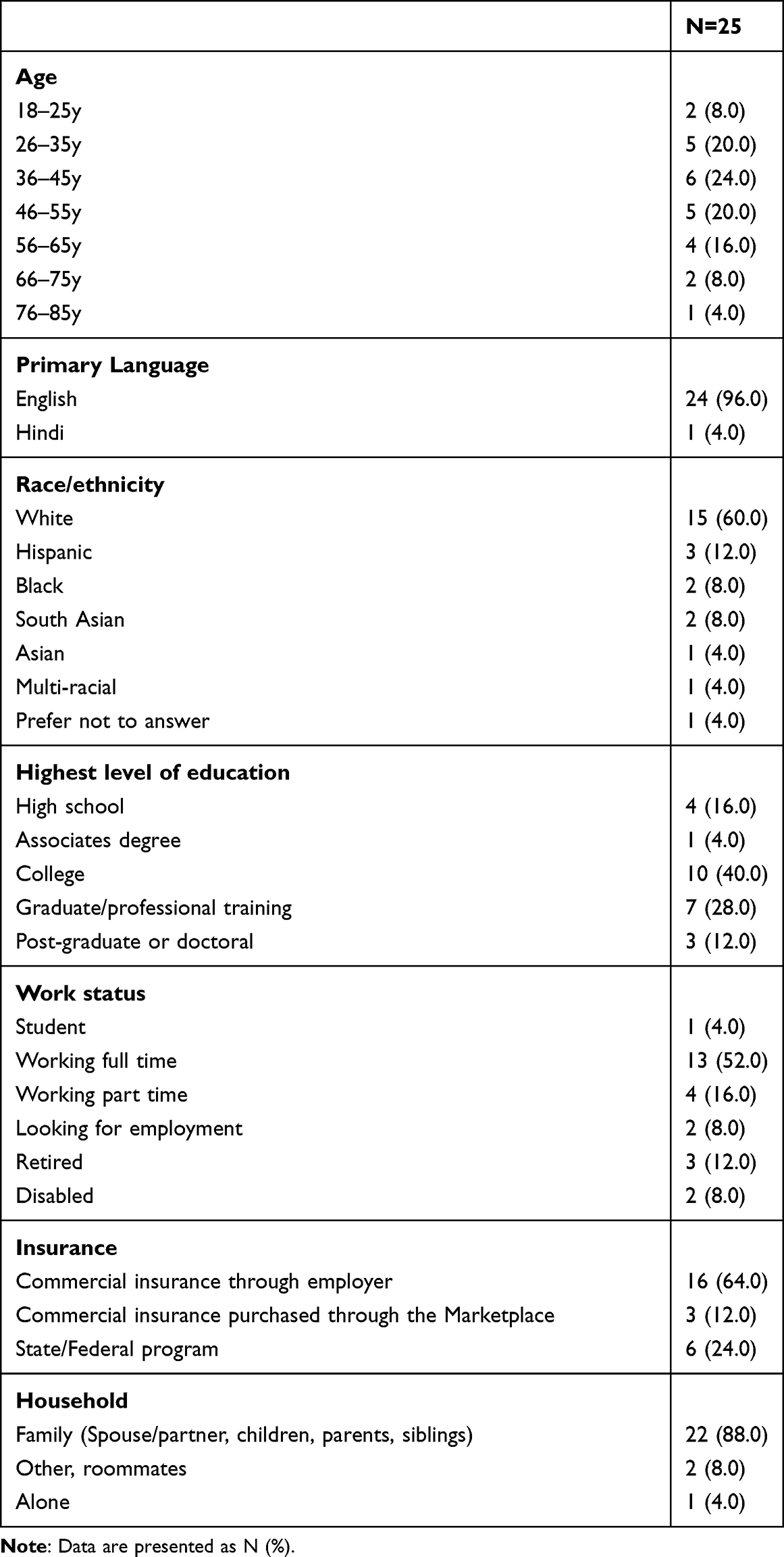 |
Table 1 Sociodemographic Characteristics |
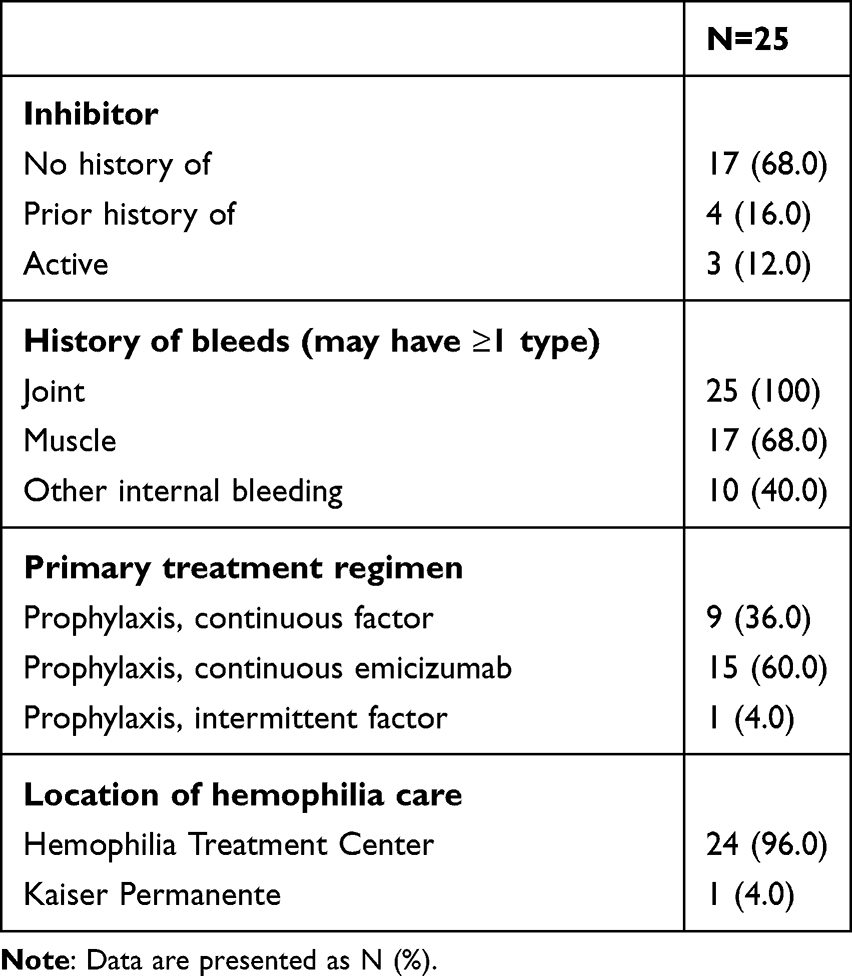 |
Table 2 Clinical Characteristics |
Table 3 shows information needs that participants would like about GT, particularly safety and efficacy data. In addition, participants indicated key stakeholders in decision making include the Hemophilia Treatment Center (HTC), spouse/partner, and friends in the hemophilia community.
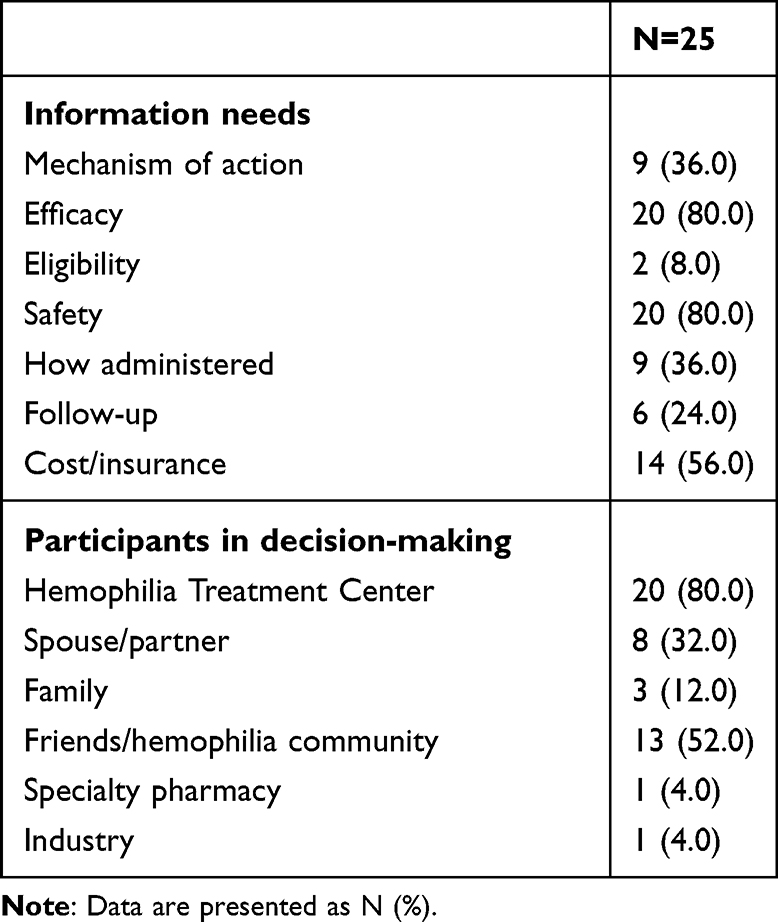 |
Table 3 Decision Making and Preferences |
Feelings and Expectations About Gene Therapy
When asked their opinion about GT, 10 (40%) indicated that they are excited about GT, 12 (48%) indicated that they are hopeful about GT, one (4%) indicated that he is worried or scared about GT, and one (4%) indicated that he does not have strong feelings about GT. One participant explained the excitement based on the expected impact on his life.
P15 Yeah. So I guess I’m excited because it more or less—it [gene therapy] provides security if it’s in your body, and it’s extended over time, and you don’t have to consider other treatment options or worry about treatment anymore. You’re kind of, more or less, secured. And that’s super advantageous. You have freedom to travel without the logistics of bringing along a month’s supply of factor or whatever you have to do, which is kind of-- and then further with preserved joint health. So, I’m very excited in that option. And I’m also, I guess, I would say, hopeful because I know within my lifetime, it’s going to come to fruition. It’s already there, but I think I will make that switch in my life. And that is just going to unlock-- I’m not going to say unlock doors, but it will unlock just something in your head that you can do and achieve more, I guess.
Excitement was tempered by some of the current unknowns and limitations.
P17 Yeah. Because, in my opinion, there hasn’t been established real-time usage of gene therapy to actually say, Yes, it works for a really long time. That’s one of the reasons why I’m not excited about gene therapy.
P25 There’s still the joint damage that I don’t think the gene therapy is going to undo that. I think that gene therapy would just eliminate the bleeds. But if someone is in a wheelchair because of hemophilia, because of a joint that is completely useless, then I don’t think gene therapy would fix that. But it would prevent any further deterioration in one’s quality of life.
Participants have high expectations regarding efficacy and durability.
P16 My expectation is if I have a factor VIII level over 50%, maybe I’ll get some bruises, but that’s-- going from 0 to 50, would be awesome. I don’t want to be a mild hemophiliac. I want to be either me severe, or I want to be clotting over 50%. Be like a carrier, a symptomatic carrier. Sure, I can do that. I don’t want to be a mild, though. Two of my daughters have 41. So they have Stimate. But I have another daughter over 100%.But you see my point is I don’t want to be 41%. I don’t want a dog tag that says, Affected carrier. Mild hemophilia, like my oldest daughter carries. I want to be a clotter.
P15 So again, my primary consideration is just having the high levels of efficacy and coverage. So I just want to know that when I take a product, I essentially can complete that infusion and don’t really necessarily have to consider hemophilia in my day-to-day activities, and I can go about doing activities as I would knowing that I have that coverage, so having the confidence in that efficacy.
Motivation to pursue GT included not needing prophylaxis, avoiding injury and pain, and health care insurance issues.
P15 I know it may have an upfront cost. But over the course of your lifetime, that’s going to allow you to not have super selective insurance options.
P18 But yeah, I mean, just not having to worry about doing it prophylactically or anything like that. I mean, it would be life-changing.
P24 I would be able to be a normal person who goes and works out and doesn’t get injured every time I work out. That would be my expectation in that I could do that pain free.
The psychological impact was identified, both positive and negative outcomes.
P27 I feel like it would simplify my life still further and give me additional psychological security….Yeah. I feel like it would still significantly improve my life, and as I say, it would be better to go into my senior-most years without having to worry about hemophilia.
P11 So I feel like the gain of maybe not having to infuse but then maybe being worried about some other deleterious unknown side effects with regards to the genetic cure, we’ll call it, that would add a layer of stress, but I don’t know, maybe not stress, but doubt or worry at least until it’s more established.
Additional illustrative quotes are listed in Supplementary Tables 1–4.
Learning About GT and Novel Therapies
Overall, participants had heard about GT, and they all wanted to learn more. Participants indicated that they seek out information and learn about GT from various sources and different learning modes. Participants identified several types of professionals from whom they receive information including clinicians at the HTC, industry and pharmacy representatives, and scientists. The HTC team was identified as an important source of information including physicians, nurse practitioners, and nurses. One participant (P20) said,
If I hear through my friends in hemophilia community, it does not carry as much weight as I carry as I hear from MD or researcher. My friends have all levels of knowledge, they still have not as much research or data. I like hearing it from trusted sites.
Although most identified some discussion about GT, none reported in depth discussion. One participant (P15) noted that the annual visit is
kind of this whirlwind event where you’re just seeing all the staff members, and you’re getting your checkups and crossing all the boxes off, so there’s a lot going on already. And it’s just, again, reminding myself to prioritize to ask certain questions.
Participants highlighted doing their own research either before or after discussion with doctor.
P3 Yeah. So I’ll gather as much information as I possibly can, particularly data so that I can analyze that data to see what-- I use that as my primary or initial source of decision-making.
P4 But I also like to-- I’m a research guy. I like going in and looking up stuff and seeing what I could find on my own. And then I can go back to them and have a very healthy discussion about stuff, because we’re on at least something of a similar level where we can speak intelligently of things that are central to whatever the treatment is.
Most participants discussed the importance of the hemophilia community as a source of information, especially those who already have experience with GT.
P3 I also will talk to people in the community about what they know about it. I’m friends with a lot of people in the community. I’m part of the Blood Brotherhood, and we get to chat about what new treatments and what problems we’re facing and all kinds of things.
Participants identified the following social media use: Instagram, Facebook chat groups, Reddit, YouTube. There were a variety of levels of use from passive to active participation. In addition to learning about new technologies, participants reported looking for information about connection and shared experiences. In addition to social media, participants reported using news alerts and press releases to learn about new treatments. Hemophilia organizations were identified as a source of information including the NHF, Hemophilia Federation of America, World Federation of Hemophilia (WFH), and local chapters. Information was obtained through attending meetings, viewing websites, and reading newsletters and other educational materials from the organizations. Participants also learn through industry sponsored events, industry meeting booths, industry supported presentations, participation in advisory boards, and industry publications (newsletters, advertisements). However, some noted, that they prefer not to receive information directly from industry.
P23 I’m a little bit hesitant to fully trust pharmaceutical literature because they’re obviously selling a product and would not always give the full negative information that they could.
Information Needs
Participants identified several key information needs to be included in education and decision-making tools. The themes were like those identified in other qualitative studies and are summarized in Supplementary Tables 2–4.
Data Access and Transparency
In addition to the types of data that are needed, the type of data and data presentation are critical. For example, real world evidence may inform decision making.
P27 I often like to have a few months of a product being out there and being used to get a sense of how is it in the real world in terms of safety and efficacy, but safety, in particular.
In considering potential risks and benefits, participants require information on the risk: benefit comparison to other products and indicated that the individual risk: benefit assessment may change with age.
P1 So with something like going to gene therapy, I would just want to see if that could be more effective than what I’m currently doing and easier to take.
P20 A Venn diagram would be good on the left side with current medicines, in the middle with similarities, and the right side with the treatment considering. How often do you treat, side effects, access, any return on investment.
Participants may consider comparison to both current and future options based on possibility of further improvements in treatment options over time.
P16 So the real question is, do I jump on the first one, or do I jump on the first one that gives me longer-lasting clotting? Gee, now we’re going from, I mean, you can do once a month with Hemlibra if you’re doing a big bolus dose with two shots, right? So now I’m talking about once every 5 years, once every 10 years, once every longer. Will my insurance pay for the second one if I had to do it again? That’s my biggest concern, is if I jump on one that doesn’t work as long as I want it to, am I screwed? You’re one and done?
Transparency of data and trust in data was also a theme.
P1 I don’t want that to be hidden from me. I want that always to be available so I can really find out everything, whether it’s good or bad.
P11 Sometimes people can embellish things if they just tell you one-on-one. So being able to see it represented in, yeah, just a way that can’t be manipulated or massaged, I think is good.
Seeing statistics matters to some participants.
P3 I do very much value data. So the information that I want is down to a level where it’s like, This is the efficacy. This is the percentage of people who respond well to it. I like facts and numbers, not, Oh, we think it’s going to work like this.
Stakeholders
Participants were asked about who should lead the conversation about GT. The responses ranged from physician led to patient led, but overall, the participants indicated that it would be a two-way conversation. Those that felt like the conversation should be led by the physician indicated an expectation for the physician to start the conversation.
P1 I mean I’m comfortable leading and bringing it up, but if it’s approved and available like that I would kind of expect them to at least bring it up as well.
On the other hand, participants pointed out the expertise of the patient community.
P8 I think it will be me. I am the patient. I am the one who knows. And even my doctor tells me this, and this is not the first hematologist I know who tells me this, that, You, the hemophiliac, sometimes know even more than I, the hematologist. And in the hemophilia space, that’s very common. And probably the interesting thing, the funny thing, about hemophiliacs is that most of us get really involved with the condition and learn a lot about it. And the good hematologists out there - there are many - they understand that, and they know that their patients are somehow a little more educated about the condition than the regular population. So in most cases, doctors are inclined to leave us lead the conversation, because they understand that we understand the condition.
One participant highlighted that the discussion should not lead to a recommendation from the physician but enough information for the patient to make the decision after considering the options.
P10 I don’t generally get a recommendation. That’s not really the process. It’s not like they’re asking the question with-- it’s not like if they said, Do you want to hear about new treatments? And then I say, “Yes”, it’s not like they say, Well, I think that you would really do well on this or that. I think that they really try to stay impartial, and they just try to give me the best information that they have.
Key participants for treatment discussions include: the doctor [experienced in GT], nurse, nurse practitioner, social worker, family, industry or pharmacy representative, patients who have had GT.
P27 I would want to talk about it with several members of the team, the physician foremost……. I’d be interested in what the nurse practitioner could add from her interactions with other patients. I’d be similarly interested, perhaps, in speaking with the social worker just to make sure that I’ve got my head on right with it and that my-- there’s a lot to adjust to in the idea of-- let’s say it really is effectively curative. I feel like there’s a lot to adjust to in the idea of no longer being a hemophiliac.
P10 And beyond that, I mean, I’m willing to hear from other people. I mean, I think hearing directly from other community members that may be on a certain treatment, I mean, that’s interesting to me, and it has some value to me.
When asked about the time for decision making about GT, most participants indicated that it would take time and multiple conversations for them to decide. One participant indicated that he does not want to be pressured into a decision.
P1 I guess just, hopefully, they wouldn’t be pressuring to do something. They’d give you enough time to decide or if it takes multiple sessions to really think about it, I think that’s good. Because I have experienced kind of being nudged and stuff to, when I was younger, doing prophylactic. But I just knew with half-life, the way they worked with the inhibitor medication, it would have just been a nightmare. So I have been kind of pressured before to do something that just wouldn’t fit with my lifestyle. But that’s really the only thing; just that it’s totally your decision.
Some participants noted hesitation about making quick decisions about new therapies given history of blood product contamination.
P13 I’m a type of person-- I’m not the type of person just to jump on something because someone says so. I like to see other people use it before-- I know I’m kind of old. I’m 53 years old. And I seen when they came out-- in the ‘80s, they came out with the [treatment?] stuff, and it was infected with HIV. So I learned a long time ago, don’t be the first one to jump on something like that.
Shared Decision-Making Tool
Twenty-two (88%) indicated that a SDM tool, either in paper or electronic form, would be useful when discussing GT with their hemophilia team. Two men indicated that they do their own research, and the tool would not add anything. One needed more information to provide an answer.
P12 I think it’s a good idea in general. I just think that, like I say, me, personally, this is something I’m going to do my own version of. But I don’t think I would benefit from a generic tool that someone else had designed. Like I say, I sort of have my own questions, my own things that I want to hear the results of. So I think, again, the methodology is right, absolutely, no problem, but I don’t think I would benefit from a tool.
Identified benefits of the tool include laying out the pros and cons, having a checklist of information so nothing is missed in the conversation, and having something tangible to take home for further review and discussion.
P18 Oh yes. Definitely. I mean, it kind of-- yeah. I mean, I think this would also generate questions, I mean, conversations with the medical provider because being able to see it laid out with the pros and cons or benefits and risk as they put it here, I think it’s really beneficial because, I mean, sometimes it doesn’t cross your mind, either yours or the medical provider. So, I mean, it’s good to have something here in black and white.
P27 I mean, really, this ought to be handed to the patient with a pen and additional note-taking paper, to be encouraged to mark it up, and yeah, you could-- because once you get home, you’re in a different place, yeah, and recalling it all and really evaluating-- yeah, being able to walk out with this for the real soul-searching decision-making at home, I think it’d be very helpful.
Participants had recommendations for the tool including tailoring to patient baseline education and health literacy.
P3 I guess you’ve got to meet people where they’re at. If they don’t want to get bogged down in that information, you’ve got to just find out what level of information they actually do want and give it to them that way.
There were also suggestions regarding content both in the amount of information and information to address misconceptions.
P3 Enough for people to realize that this is their lives they’re dealing with, and they need to be informed about what’s going on so that they can have a hand in that decision-making. I think too many people leave that research and information gathering and decision part to their doctors. And that’s not good.
P3 Just make it very strong. Don’t water it down. Make them realize that this is going to affect their lives, and they need to be an informed participant in that discussion and in that decision.
P12 I would be prepared to face reluctance of other people to enter into something like this. And never underestimate how wild some opinions might be on stuff like this, which hopefully, the scientific community is now learning how wild opinions can be. And they need to be prepared to address those, rather than brush them off as they have in the past.
Utility and implementation of the tool was considered for both patients and providers.
P4 Okay. So you sit down, and the doctor can give you the pamphlet, Here, take a look at this. I want you to look at this. Yeah, I mean, anything that helps facilitate understanding and communication is important, whether it’s a pamphlet, a little video clip, a slideshow, whatever. I was a teacher, so I’m not beholden to one thing or another. It’s whatever it takes to reach the student; in this case, the patient, so.
Discussion
This qualitative study of men with severe HA informs the utility, content, and implementation for SDM tools for hemophilia GT. Implementation of SDM is applicable for all medical decision-making, but it is even more relevant for GT given that it is not reversible, there is a different side effect profile and follow-up compared to other hemophilia treatment, and there is variability in treatment response.
Athale published SDM tools, including clinician and patient facing documents, related to key treatment decisions related to prophylaxis and immune tolerance induction.10 To our knowledge there are no other published SDM tools for hemophilia, but there is a call to action for education and SDM tools and assurance of informed consent and pre-GT education2,4–7,11,12 in anticipation of commercial approval of GT for hemophilia. In a qualitative study of men who underwent GT, the men reported that they were unprepared for the side effects of immunosuppression as well as the follow-up requirements,6 and in another study participants noted that patients need to be better prepared.13 Khair et al recommended starting GT discussions with parents of young children.
Most of the participants in this study identified the utility of SDM tools and identified key benefits including provision of standardized information and a checklist such that all pertinent information is covered, and having something tangible to take notes and to take home for further consideration and discussion with family.
Overall, participants have high expectations of GT regarding factor expression and impact on health and daily life. In a qualitative study of men who received GT, most participants described GT as life-changing with improvements in physical activity and decreased burden of travel. One participant had limited impact due to chronic joint disease. This limitation was also identified in our study. As part of SDM, providers should assess patient expectations and see how those expectations align with the available data on GT outcomes. It is critical that patients make informed decisions with a clear understanding of expected outcomes as well the variability between patients. It will be important to consider individual patient characteristics regarding expected outcomes which may vary based on age, prior treatment, etc.
Content
We identified that most participants are excited or hopeful about GT, and participants communicated a strong interest in learning more about GT plus some gaps in knowledge that need to be addressed for informed decision-making. Participants identified key information needs. The key attributes identified are concordant with previously published quantitative and qualitative research.14–18 In addition to this information, participants in this and other studies have identified the potential positive and negative psychosocial impact; anxiety of loss of expression, loss of control, impact on identity.6,7,19 Participants acknowledged that they may have new worries after their GT infusion about such as worries about potential side effects. This highlights the key role of mental health screening and social work and psychology support for all individuals with hemophilia and particularly along the gene therapy journey. SDM tools should discuss potential psychologic impact and the importance of utilizing mental health resources throughout the GT journey. The NHF Medical and Scientific Advisory Council is publishing a psychosocial assessment template for social workers to assess patients considering GT (personal communication).
In addition to safety and efficacy data of GT, SDM must include comparative data, in an unbiased way, to other treatment options, both those currently available and future therapies. Information should be transparent and unbiased and additional resources should be available. Some participants shared concern about getting information directly from industry and overall preferred information from clinicians, patient advocacy groups, and the hemophilia community. Participants identified the importance of transparency. SDM tools will need to present data clearly without oversimplifying the information and provide access to additional educational resources and primary data as well as opportunity for continued review.
Tools will need to be dynamic and updated with new data which is critical especially for those who are not yet considering GT based on too many unanswered questions and unknowns.
Development and Design of SDM Tools
Optimally, SDM tools will be developed by multi-disciplinary groups including patients, clinicians and patient advocacy groups that do not have financial or other vested interested in gene therapy. Participants were very engaged in the research and have been engaged as key stakeholders in other hemophilia research and should be included as part of the SDM development and testing team such as with the coreHEM multistakeholder project.20
GT has introduced a new lexicon to hemophilia therapy. Several authors have published on the importance of a standard approach to talking about GT such that patients and clinicians are speaking the same language, that jargon and unnecessary details are avoided and that meet all levels of health literacy.2,21,22
Participants noted that they appreciate visuals and videos for learning about GT. Therefore, SDM may be multi-modal to meet patients learning preferences. Van Balen et al evaluated the impact of visuals on decision making about prophylaxis and demonstrated positive outcomes.16 Engaging experts in Medical Education and visual arts may improve readability. In general, readability of patient education materials is low, and interventions to improve readability include testing with readability tools and patient testing.23,24
Implementation
Participants demonstrated different levels of knowledge about GT and readiness to consider GT as a treatment. Implementation of tools may include an assessment to first evaluate where patient is in readiness to engage in a discuss of new treatment options. Are patients satisfied with current therapy; do they want to optimize current treatment; what is the patient’s risk tolerance?
Participants highlighted the importance of meeting PwH where they are and highlighted that some PwH will have little baseline knowledge and difficulty understanding complex statistical information, whereas others will have advanced understanding based on self-study, discussion within the hemophilia community or attendance at medical conferences prior to discussion at the HTC.
SDM may be initiated and/or led by the clinician or patient and this preference may be solicited prior to the discussion. Decision-making will likely require multiple visits for education, comparison to alternatives, and goal setting. Participants indicated that they do not want to feel pressured. They also emphasized that it takes time for discussion and may need to be done outside of the typical comprehensive clinic which one participant described as a “whirlwind”. Participants identified nurses are key participants in decision making as demonstrated in other studies.5,13
Providers will need general training on SDM tools as well as how to implement within different resource settings and languages.25–27 The framework for incorporating SDM tools into discussion of new treatments will include assessing baseline knowledge, health literacy, language preference, patient activation; identifying who is included in the process; assessing patient goals; providing baseline education; utilizing the SDM tools; assessing next steps after a decision is made; and evaluating the decision. A key information checklist to include in a SDM tool is shown in Box 1.
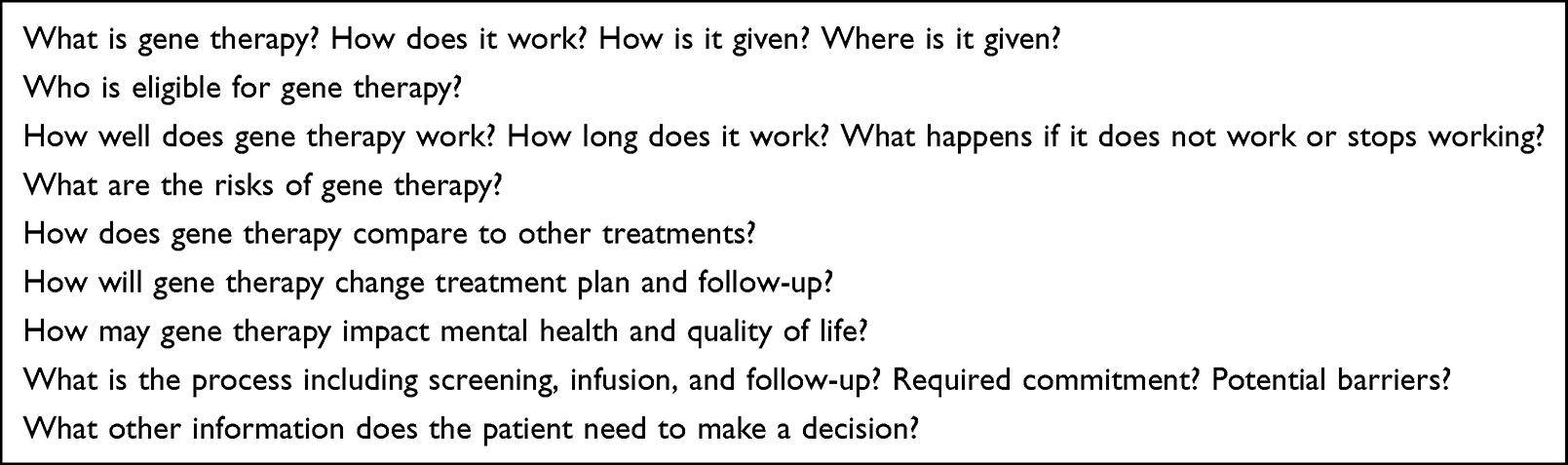 |
Box 1 Checklist for Hemophilia Shared Decision-Making Tools |
Strengths and Limitations
Although the study was open to men with severe HA or HB, only men with HA responded to the study invitation, which limits generalizability. Additional research should be conducted in the HB population given different treatment options and differences in safety and efficacy between HA and HB gene therapy, and recruitment through the Coalition for Hemophilia B may considered. Also, this study did not include PwH who had undergone GT, such that we only have the perspective of PwH who are considering GT. Future qualitative work, such as that done in the Exigency Programme,6 should be conducted in the US to describe the experience of men who have had GT and how their experience may inform the development of SDM tools.
Next Steps
Data from this study as well as a survey of men with HA and HB8 will be used to inform the development of SDM tools for clinicians. The tools will prepare clinicians to discuss GT and alternative treatment options with PwH in the context of their values and preferences. A patient centric SDM is being developed by the WFH.
Conclusions
Data from this mixed methods study of men in the United States with severe HA identify key treatment attributes, expectations, and decision-making preferences to inform the development and implementation of a patient oriented SDM tool. In addition, we identified a variety of expectations related to factor expression, durability, and freedom from medical care as well as potential limitations that should be addressed during informed consent discussions.
Abbreviations
SDM, shared decision-making; NHF, National Hemophilia Foundation; HA, hemophilia A; HB, hemophilia B; GT, gene therapy; CVR, Community Voices in Research; HTC, Hemophilia Treatment Center; WFH, World Federation of Hemophilia.
Data Sharing Statement
Data are available to investigators at academic institutions by contacting the corresponding author.
Acknowledgments
We thank the study participants for their participation. Jennifer Han and Hannah Reyes reviewed initial recordings. Hannah Reyes conducted some of the interviews and initial coding.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, the study design, execution, acquisition of data, analysis and interpretation, or in all of these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
A grant was provided by the National Hemophilia Foundation for the conduct of the study. The National Hemophilia Foundation had no input on the content of the manuscript. A grant was provided by BioMarin for the conduct of the study. BioMarin had no input on the content of the manuscript.
Disclosure
JL and CDT receive research funding from BioMarin and the National Hemophilia Foundation. CT receives honorarium from BioMarin, CSL Behring, Genentech, Pfizer, and Sanofi Genzyme and reports personal fees from Takeda, Octapharma, Bluebird Bio, Cyclerion, and HEMA Biologics, outside the submitted work.
References
1. Leebeek FWG, Miesbach W. Gene therapy for hemophilia: a review on clinical benefit, limitations, and remaining issues. Blood. 2021;138(11):923–931. doi:10.1182/blood.2019003777
2. Wang M, Negrier C, Driessler F, Goodman C, Skinner MW. The hemophilia gene therapy patient journey: questions and answers for shared decision-making. Patient Prefer Adherence. 2022;16:1439–1447. doi:10.2147/PPA.S355627
3. Katz SJ, Belkora J, Elwyn G. Shared decision making for treatment of cancer: challenges and opportunities. J Oncol Pract. 2014;10(3):206–208. doi:10.1200/JOP.2014.001434
4. Woollard L, Gorman R, Rosenfelt DJ. Addressing patient education priorities in the era of gene therapy for haemophilia: towards evidence-informed shared decision-making. Haemophilia. 2021;27(2):e302–e304. doi:10.1111/hae.14214
5. Khair K, Steadman L, Chaplin S, Holland M, Jenner K, Fletcher S. Parental perspectives on gene therapy for children with haemophilia: the Exigency study. Haemophilia. 2021;27(1):120–128. doi:10.1111/hae.14188
6. Fletcher S, Jenner K, Pembroke L, Holland M, Khair K. The experiences of people with haemophilia and their families of gene therapy in a clinical trial setting: regaining control, the Exigency study. Orphanet J Rare Dis. 2022;17(1):155. doi:10.1186/s13023-022-02256-2
7. Fletcher S, Jenner K, Holland M, Chaplin S, Khair K. An exploration of why men with severe haemophilia might not want gene therapy: the exigency study. Haemophilia. 2021;27(5):760–768. doi:10.1111/hae.14378
8. Limjoco J, Calatroni A, Aristizabal P, Thornburg CD. Gene therapy preferences and informed decision-making: results from a National Hemophilia Foundation Community Voices in research survey. Haemophilia. 2023;29(1):51–60. doi:10.1111/hae.14706
9. Green J, Thorogood N. Analysing Qualitative Data. London: Sage Publications; 2004.
10. Athale A, Giguere A, Barbara A, Krassova S, Iorio A. Developing a two-sided intervention to facilitate shared decision-making in haemophilia: decision boxes for clinicians and patient decision aids for patients. Haemophilia. 2014;20(6):800–806. doi:10.1111/hae.12495
11. Valentino LA, Blanchette V, Negrier C, et al. Personalising haemophilia management with shared decision making. J Haem Pract. 2021;8(1):69–79. doi:10.17225/jhp00178
12. Hermans C, Noone D, Benson G, et al. Hemophilia treatment in 2021: choosing the “optimal” treatment using an integrative, patient-oriented approach to shared decision-making between patients and clinicians. Blood Rev. 2022;52:100890. doi:10.1016/j.blre.2021.100890
13. Aradom E, Gomez E. The patient gene therapy journey: findings from qualitative interview with trial participants at one UK haemophilia centre. J Haem Pract. 2021;8(1):32–44. doi:10.17225/jhp00174
14. Woollacott I, Morgan G, Chowdary P, et al. Examining patient and professional perspectives in the UK for gene therapy in haemophilia. Haemophilia. 2022;28(4):588–609. doi:10.1111/hae.14572
15. Witkop M, Morgan G, O’Hara J, et al. Patient preferences and priorities for haemophilia gene therapy in the US: a discrete choice experiment. Haemophilia. 2021;27(5):769–782. doi:10.1111/hae.14383
16. van Balen EC, Krawczyk M, Gue D, et al. Patient-centred care in haemophilia: patient perspectives on visualization and participation in decision-making. Haemophilia. 2019;25(6):938–945. doi:10.1111/hae.13830
17. van Overbeeke E, Hauber B, Michelsen S, Goldman M, Simoens S, Huys I. Patient preferences to assess value IN gene therapies: protocol development for the PAVING study in hemophilia. Front Med. 2021;8:595797. doi:10.3389/fmed.2021.595797
18. van Overbeeke E, Michelsen S, Hauber B, et al. Patient perspectives regarding gene therapy in haemophilia: interviews from the PAVING study. Haemophilia. 2021;27(1):129–136. doi:10.1111/hae.14190
19. Miesbach W, Klamroth R. The patient experience of gene therapy for hemophilia: qualitative interviews with trial patients. Patient Prefer Adherence. 2020;14:767–770. doi:10.2147/PPA.S239810
20. Iorio A, Skinner MW, Clearfield E, et al. Core outcome set for gene therapy in haemophilia: results of the coreHEM multistakeholder project. Haemophilia. 2018;24(4):e167–e172. doi:10.1111/hae.13504
21. Sidonio RF, Pipe SW, Callaghan MU, Valentino LA, Monahan PE, Croteau SE. Discussing investigational AAV gene therapy with hemophilia patients: a guide. Blood Rev. 2021;47:100759. doi:10.1016/j.blre.2020.100759
22. Hart DP, Branchford BR, Hendry S, et al. Optimizing language for effective communication of gene therapy concepts with hemophilia patients: a qualitative study. Orphanet J Rare Dis. 2021;16(1):189. doi:10.1186/s13023-020-01555-w
23. Downey T, Millar BC, Moore JE. Improving health literacy with mumps, measles and rubella (MMR) vaccination: comparison of the readability of MMR patient-facing literature and MMR scientific abstracts. Ther Adv Vaccines Immunother. 2022;10:25151355221118812. doi:10.1177/25151355221118812
24. Rooney MK, Santiago G, Perni S, et al. Readability of patient education materials from high-impact medical journals: a 20-year analysis. J Patient Exp. 2021;8:2374373521998847. doi:10.1177/2374373521998847
25. Hoffmann TC, Del Mar C, Santhirapala R, Freeman A. Teaching clinicians shared decision making and risk communication online: an evaluation study. BMJ Evid Based Med. 2021;26(5):253. doi:10.1136/bmjebm-2020-111521
26. Theriault G, Bell NR, Grad R, Singh H, Szafran O. Teaching shared decision making: an essential competency. Can Fam Physician. 2019;65(7):514–516. doi:10.15766/mep_2374-8265.9413
27. NHS Health Education England, Elearning for Healthcare. Shared decision making: an online learning resource to assist healthcare professionals in embedding shared decision-making in everyday practice. elfh: elearning for healthcare. 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.