Back to Journals » Psychology Research and Behavior Management » Volume 13
Gender Differences in Perceived Stigma and Coping Strategies Among People Living with HIV/AIDS at Jugal Hospital, Harar, Ethiopia
Authors Ataro Z ![]() , Mengesha MM
, Mengesha MM ![]() , Abrham A
, Abrham A ![]() , Digaffe T
, Digaffe T ![]()
Received 25 September 2020
Accepted for publication 2 December 2020
Published 14 December 2020 Volume 2020:13 Pages 1191—1200
DOI https://doi.org/10.2147/PRBM.S283969
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Zerihun Ataro,1 Melkamu Merid Mengesha,2 Aklilu Abrham,3 Tesfaye Digaffe4
1Department of Medical Laboratory Sciences, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 3School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 4Department of Human Resource Development, Federal Ministry of Health, Addis Ababa, Ethiopia
Correspondence: Zerihun Ataro
Department of Medical Laboratory Sciences, College of Health and Medical Sciences, Haramaya University, P.O. Box 235, Harar, Ethiopia
Email [email protected]
Background: HIV/AIDS is among the most devastating diseases, having multiple effects on the health and well-being of people living with HIV/AIDS (PLWHA). There is a paucity of studies that examined the gender differences in perceived stigma among PLWHA and the different coping strategies that they use in Ethiopia.
Objective: To assess the gender differences in perceived stigma and coping strategies among PLWHA.
Methods: A comparative cross-sectional study was conducted at Jugal Hospital, Harar, eastern Ethiopia from May 01 to July 30, 2018. A total of 412 (206 females and 206 males) PLWHA were included. Face-to-face interviewer-administered data were collected. Perceived HIV stigma was assessed using the Berger HIV stigma scale. Similarly, the coping strategies were assessed using the Brief Coping Orientation to Problems Experienced (Brief COPE) scale. The data were analyzed using STATA version 13.
Results: The mean Berger stigma scale score was 65.3± 11.3. The overall perceived stigma mean score was not statistically different between males and females (64.8± 10.8 vs 65.8± 11.7, p=0.407). Among the four subscales, women reported a higher level of disclosure stigma than men (21.1± 5.5 vs 20.3± 5.5; p=0.006). Regarding maladaptive coping strategies, men often used substances compared to women (2.8± 1.5 vs 2.1± 0.4; p< 0.001). However, women use behavioral disengagement (4.6± 1.1 vs 4.2± 1.1; p=0.002) and self-distraction (5.9± 1.5 vs 5.5± 1.7; p=0.019) more often than men. Females used a higher level of adaptive coping strategies compared to males (42.5± 4.9 vs 40.9± 6.3, p=0.005). Furthermore, females were found to use more emotional-focused coping than males (27.6± 3.2 vs 26.4± 4.0; p< 0.001).
Conclusion: Women reported a higher level of disclosure stigma than men and the types of coping strategies used vary between male and female. Thus, interventions to support PLWHA must take into account the gender differences in terms of perceived stigma.
Keywords: perceived stigma, coping strategies, PLWHA, Ethiopia
Introduction
Stigma refers to the undesirable traits that adhere to our perception of what a specific type of person should be.1 Its origins are deep within the social structure of society as a whole and in the norms and values that govern everyday life.2 Research on the relationships between health status, stigma, and coping mechanisms found that infection with human immunodeficiency virus (HIV) was inherently stressful and had a significant effect on the quality of life. Research has demonstrated that HIV-related stigma can have a variety of negative effects on health behaviors, such as seeking HIV testing, willingness to disclose HIV status, accessing health care, and on quality of health care provided or received.3
The ability to cope with change is related to the nature of the change, availability of social support, and personal factors. The extent to which people feel in control of their lives varies, and active coping strategies that enhance a feeling of control, such as task-focused coping or positive (adaptive) reframing, is beneficial.2,4 Whereas, a poorer adjustment is associated with persistent denial, venting of emotions, and behavioral disengagement that avoids dealing with change. A poorer (maladaptive) coping strategies and stress are associated with an immunological deterioration and are likely to play a role in the strong connection between HIV and mental problems such as anxiety or depression.2,5
Coping has also been categorized as a problem- or emotion-focused. A problem-focused coping aims at solving the problem or altering the source of the stress, while an emotion-focused coping is directed at reducing or managing the emotional distress associated with or caused by the situation. The degree of sickness and the ability to understand and contain emotions is also important.6
Research evidence has shown that men and women living with HIV have different experiences with both HIV-related perceived stigma and coping strategies used. More women living with HIV reported stigmatizing experiences than do males living with HIV.7–9 Moreover, studies conducted in Bengaluru, India, found that men internalized stigma more frequently than women; yet studies conducted in Burkina Faso, Kenya, Malawi, and Uganda reported the opposite.10−12 Concerning the coping strategies used, men are more likely than women to use problem-based coping strategies or engage in avoidance or denial. The stereotypical male is likely to confront a problem head-on and also they are assumed to be more likely to deny a problem exists. It is believed that women use a more emotional response to problems that seek social support.13
According to the 2016 Ethiopian Demographic and Health survey, the prevalence of HIV in Ethiopia was 1.2%.14 Besides medical problems, PLWHA faced social problems associated with the disease. One of these problems is found to be HIV-related stigma.15 Although large numbers of PLWHA are found in Ethiopia, the situation of perceived stigma and coping strategies related to HIV has not been addressed. Understanding differences in perceived stigma among people living with HIV/AIDS and different coping strategies provide empirical evidence for program planner, decision makers and program implementer at the different level.
In view of the fact that HIV stigma and its coping strategies are influenced by its sociocultural context, it is important to study the perceived stigma associated with HIV and the coping strategies used in the context of gender. Therefore, this study examined the gender differences in the perceived stigma among PLWHA and the different coping strategies used.
Methods and Materials
Study Area and Period
This study was conducted in Jugal hospital, Harar, eastern Ethiopia from May 01 to July 30, 2018. Harar is one of the ancient cities in Ethiopia located 525 kilometers away from Addis Ababa, the capital city of Ethiopia. Based on the 2007 census conducted by the Central Statistical Agency of Ethiopia (CSA), Harari region had a total population of 183,344, of whom 92,258 were males and 91,086 were females; 99,321 or 54.17% of the population were urban inhabitants.
Study Design
A cross-sectional study was conducted to compare the gender differences in perceived stigma and coping strategies among PLWHA.
Study Population
Adult PLWHA who received HIV/AIDS-related and other health services at Jugal Hospital during the study period.
Inclusion and Exclusion Criteria
All PLWHA receiving care and support aged ≥18 years were included in this study. PLWHA who are seriously sick, could not respond and unable to undergo the assessment were excluded from the study.
Sample Size and Sampling Techniques
Sample size calculation was based on the sample size for comparison of two sample means. From a study carried out in India,16 we get a mean score of 103 for perceived stigma among men and 102.7 among women. Finally, we used STATA version 13 to estimate the sample size with significance level (P<0.05), power (80%), common standard deviation with a proportion of 1:1. Accordingly, we obtained a sample size of 374. By adding a 10% of the calculated sample size for non-response, we obtained a total of 412. Therefore, with a ratio of 1:1, 206 female and 206 male adult PLWHA were recruited by convenient sampling technique.
Data Collection
Data Collection Instruments
Demographic characteristics such as age, sex, occupation, marital status, religion, educational status and residence area were collected from each participant using a structured questionnaire.
The perceived HIV stigma of the study participants was assessed using the Berger HIV stigma scale of 32 items.17 We translated it into local language for use in the present study. All participants were asked to respond to each of the items a four response options (“strong disagree,” “disagree,” “agree,” or “strong agree”). Possible scores ranged from a low of 32 to a maximum of 128, with a larger score showing a higher degree of perceived HIV stigma. The tool had four domains in their original sample of HIV-positive individuals: personalized stigma (12 items), disclosure concerns (8 items), negative self-image (10 items), and concern with public attitudes toward PLWHA (13 items). The scores for each domain vary with the number of items in the domain. There is an overlap of few items across the domains giving a total of 32 items. The personalized stigma items identify the negative consequences of other people’s knowledge that an individual has HIV, such as experiences with or fear of rejection. The items that measured the disclosure concerns are related to controlling information about one’s HIV-positive status. The items in the negative self-image domain measured feelings about being unclean or being inferior to others because of an HIV-positive status. Lastly, public concern about PLWHA focuses on perceptions of what “other people” think of a person with HIV or what people with HIV should expect of others when their HIV-positive status is discovered.17
The coping strategies of the participants were assessed using the 28-items Brief Coping Orientation to Problems Experienced (Brief COPE) scale.18 The Brief COPE is the abbreviated version of the COPE inventory and measures both the dispositional and situational efforts of cope. The Brief COPE has 14 subscales with each subclass having two items (self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioral disengagement, venting, positive reframing, planning, humor, acceptance, religion, self-blame). The Brief COPE was divided into three categories: problem-focused (active coping, planning, and use of instrumental support), emotion-focused (use of emotional support, positive reframing, acceptance, religion, and humor), and dysfunctional coping (venting, denial, substance use, behavioral disengagement, self-distraction, and self-blame). Furthermore, the brief COPE was organized into two categories: the adaptive coping (including all the subscales of the problem-focused and emotion-focused coping categories) and the maladaptive coping strategies (including all the subscales of dysfunctional coping).
Both Berger HIV stigma scale and Brief COPE scale exhibited good reliability in the present sample. The overall scale of the Berger HIV stigma showed a Cronbach’s alpha of 0.876 and all subscales demonstrated acceptable internal consistency (Cronbach’s alpha 0.864–0.883). The overall Brief COPE scale demonstrated acceptable internal consistency with Cronbach’s alpha of 0.761 and the subscales had Cronbach’s alpha of 0.739–0.769.
Data Collectors
All data were collected by the counselors of PLWHA so as to avoid erosion of their privacy. The interviewers were both female and male health workers (Nurse by profession) who received a standard training on counseling services to PLWHA. For the data collection of this study, they were oriented for 2 days by the principal investigator, and a day-to-day onsite support was given during data collection.
Data Analysis
Data were entered into Epi-data software and the analysis was performed using STATA version 13. Internal consistency of the Berger HIV stigma scale and Brief COPE scale was assessed using Cronbach’s alpha. Descriptive summary was presented in terms of mean, range, and proportions depending on the scale of the variable. Data were presented as mean ± SE. The Student’s t-test was used to compare the mean score between the two groups (male and female) compared. Multiple linear regression analyses were applied to determine whether there is a significant difference on perceived stigma and coping strategies between female and male patients by controlling the demographic variable. Variables were included in the multivariate model if the bivariate test resulted in a p-value of less than 0.25. The statistical tests were declared at P-value <0.05.
Data Quality Control
The questionnaire was prepared in English, translated to Amharic and Afan Oromo, the two local languages commonly spoken in the study area, and then back translated to English by a language expert to check its consistency. The questionnaire was pre-tested on 5% of PLWHA who were not part of the actual study. An orientation was given to the data collectors on the objectives of the study, techniques of making a good interview and possible errors, obtaining and maintaining quality data, and the measurement tools used. The completed questionnaires were checked for inconsistencies and missed values during the data collection, and timely communications with data collectors were done and feedback were obtained. Questionnaires with significant problems were excluded from the analysis.
Ethical Consideration
The study proposal was approved by the Institutional Health Research and Ethics Review Committee of College of health and Medical Sciences, Haramaya University (IHRERC/249/2018). Letter of permission was written to Harari Regional State Health Bureau. Signed informed consent was obtained from all participants. This study was conducted in accordance with the Declaration of Helsinki, and all ethical and professional considerations were followed throughout the study. During the interview, confidentiality of the collected data and privacy of each participant were kept confidential.
Results
Socio-Demographic Characteristics of the Study Subjects
A total of 412 HIV-positive subjects (206 male and 206 female) were included in this study. The average age was 45.1 years for males and 40.2 years for females. More than half of the participants were married (51.5% for males and 56.8% for females). Majority of the participants reside in urban (96.6% for males and 96.1% for females). In total, 397 patients (96.4%) were living in urban areas, 153 (37.1%) attended primary school, and 285 (69.2%) were orthodox in religion (Table 1).
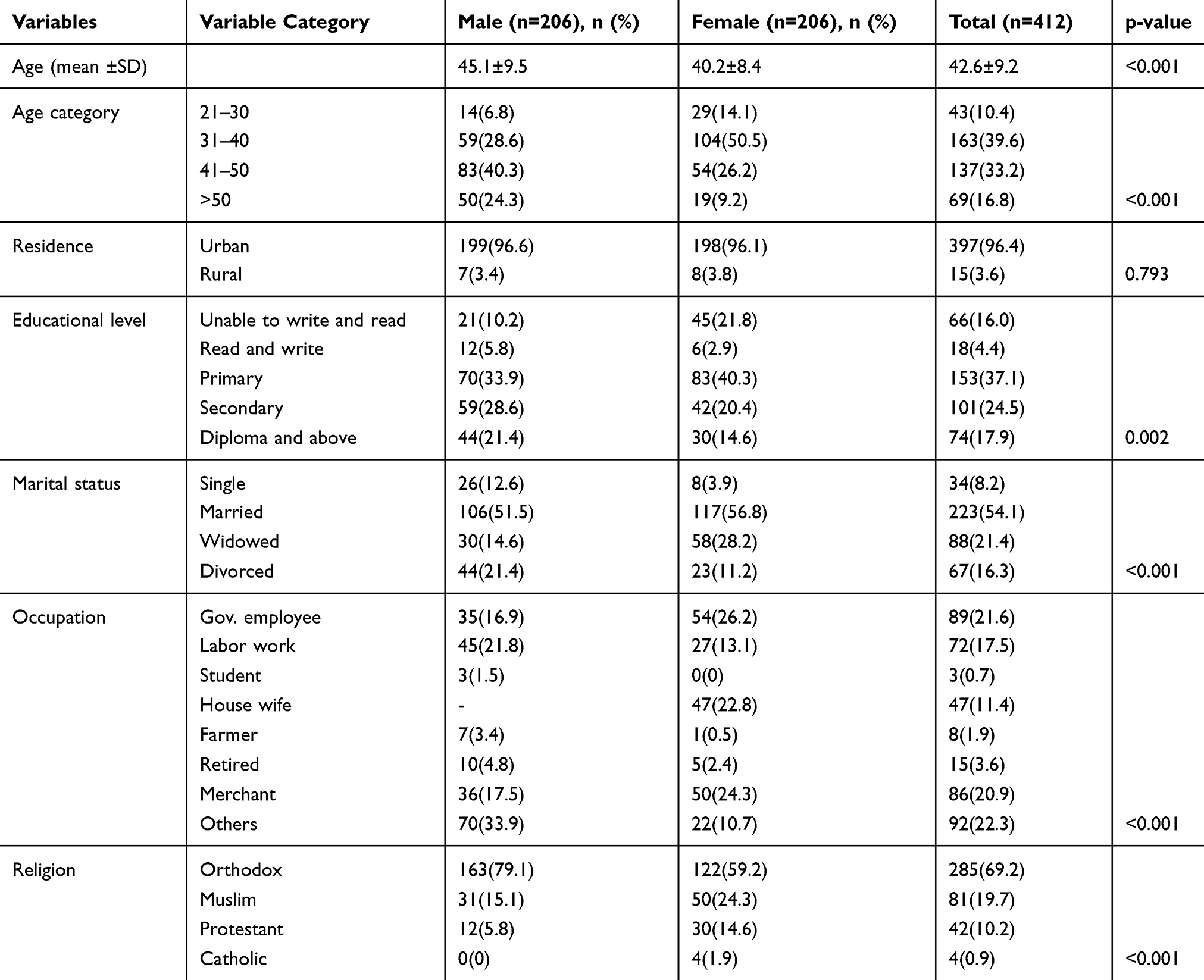 |
Table 1 Socio-Demographic Characteristics of PLWHA in Jugal Hospital, Harar, Eastern Ethiopia |
Descriptive Analysis of Perceived Stigma and Coping Strategies
Analysis of perceived stigma among the study subjects showed a mean score of 65.3±11.3. Total stigma scores are categorized into four stigma levels: minimal (32–56), low (57–80), moderate (81–104) and high (105–128). Overall, positive reframing and turning to religion were the most frequently reported coping strategies, followed by acceptance and planning. Humor was the least frequently reported coping strategy followed by substance use (Figure 1).
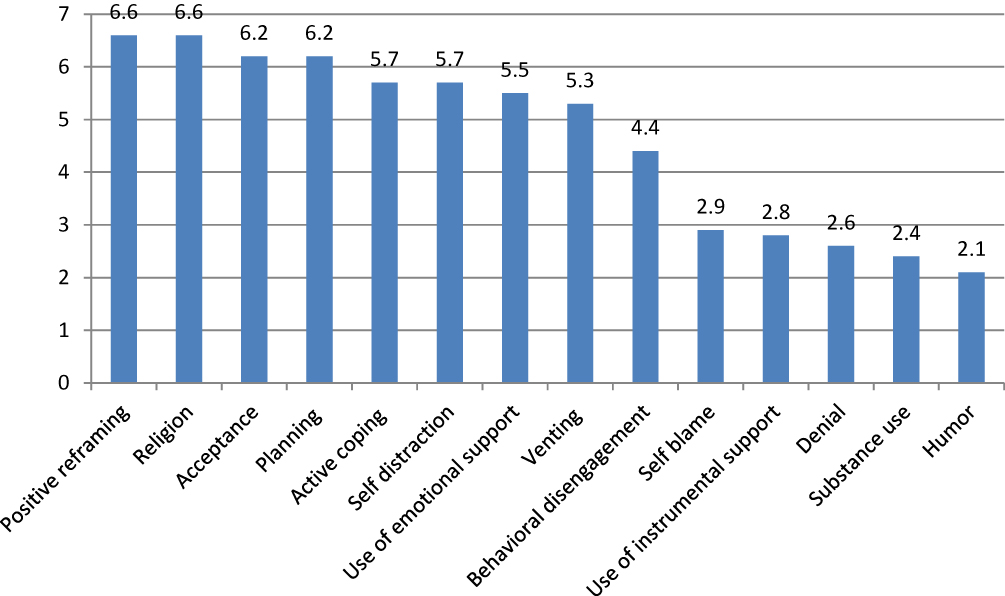 |
Figure 1 Coping strategies used by HIV-positive patients in Jugal Hospital, Harar, eastern Ethiopia. |
Gender Difference in Perceived Stigma
The total perceived stigma mean score was not statistically different between men and women (64.8±10.8 vs 65.8±11.3, p=0.407). Women reported a higher level of disclosure stigma than men (21.8±5.6 vs 20.3±5.5, p=0.006), whereas no significant gender difference was found in the other perceived stigma subclasses (personalized stigma scale, negative image scale, public attitude scale) (Table 2). In the multivariable model, after controlling for demographic variables, there was no significant difference on the mean level of total perceived stigma score between male and female PLWHA. However, female PLWHA had a higher level of disclosure stigma score compared to male (Table 3).
 |
Table 2 Gender Difference on Perceived Stigma Among PLWHA in Jugal Hospital, Harar, Eastern Ethiopia |
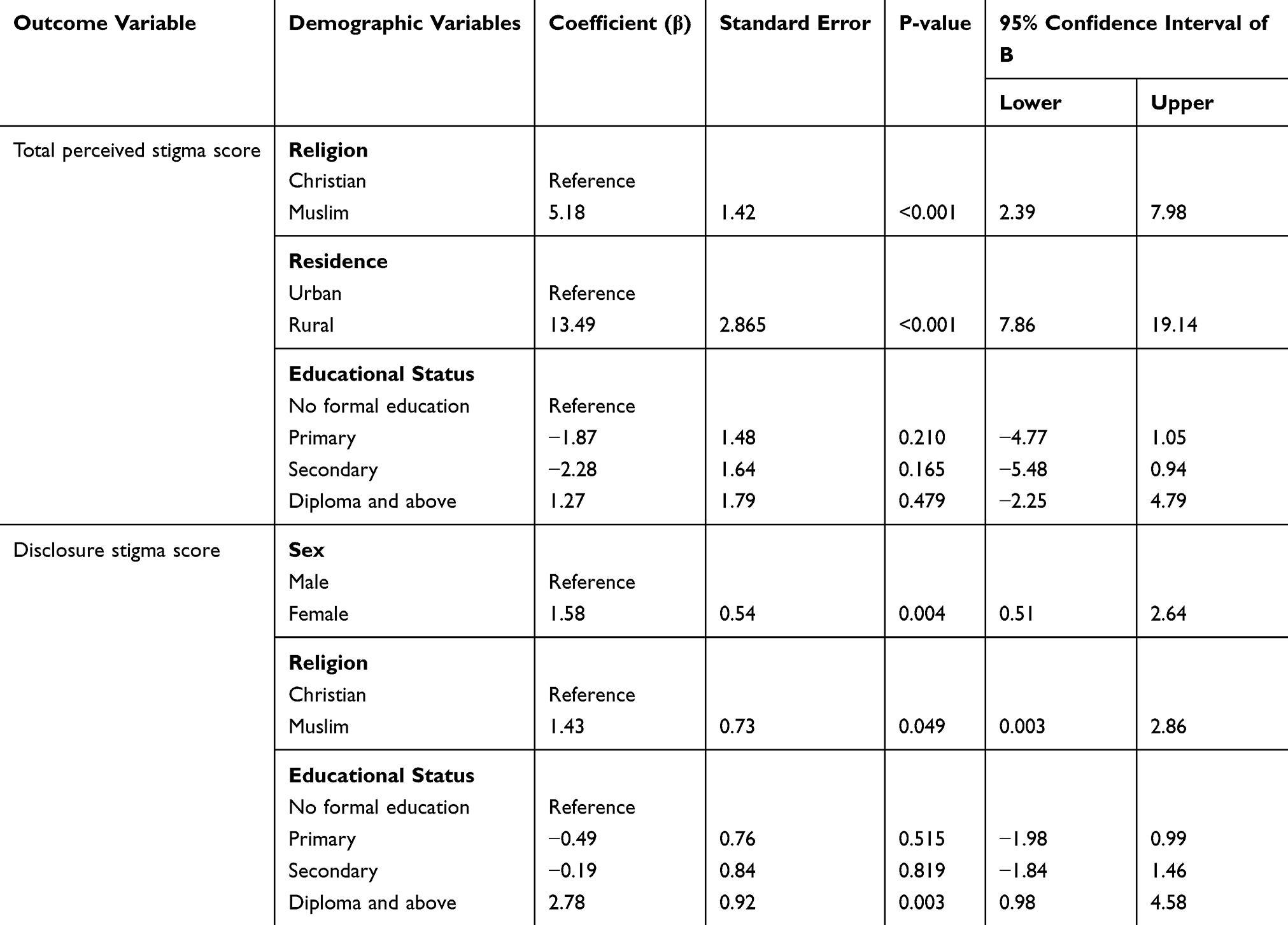 |
Table 3 Multivariable Linear Regression Models with Outcomes of Total Stigma Scores and Disclosure Stigma Score for PLWHA in Jugal Hospital, Harar, Eastern Ethiopia |
Gender Difference in Coping Strategies
As shown in Table 4 there was significant difference by gender in terms of the three factors of emotional-focused coping strategies: use of emotional support, religion and humor. The mean score showed that women more often used emotional support (5.8±1.6 vs 5.1±1.8; p<0.001) and religion (6.9±1.3 vs 6.4±1.6; p<0.001) compared to men. However, men use humor more often than women (2.2±0.6 vs 2.1±0.3; p=0.010). Moreover, there was significant difference by gender with the use of instrumental support (2.7±0.9 vs 3.0±0.9; p=0.001) as a coping mechanism (Table 4).
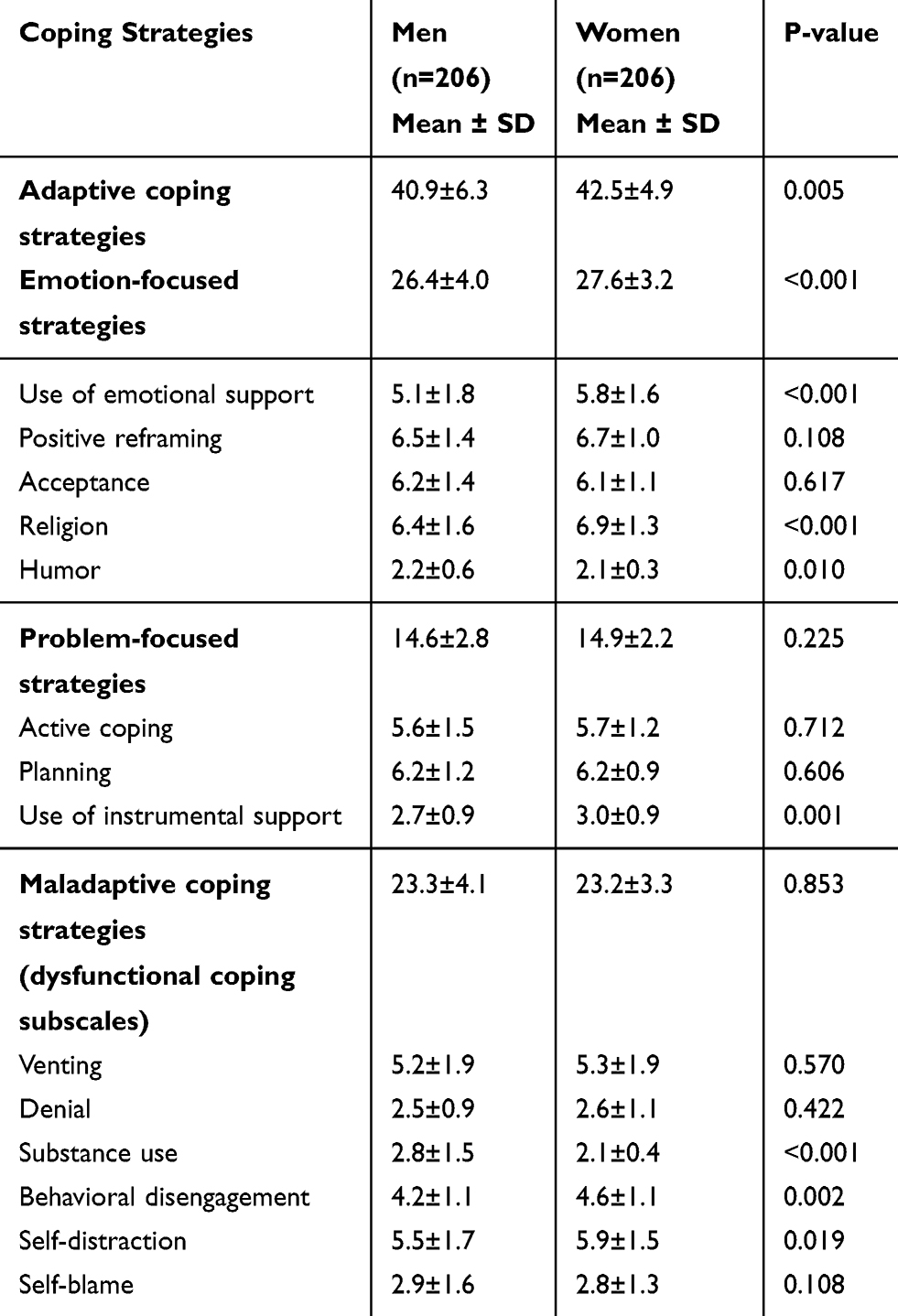 |
Table 4 Gender Difference in Coping Strategies Among PLWHA in Jugal Hospital, Harar, Eastern Ethiopia |
Regarding maladaptive/dysfunctional coping strategies, there was statistically significant gender difference in the use of substance, behavioral disengagement and self-distraction. Men use substance more in comparison to women (2.8±1.5 vs 2.1±0.4; p<0.001). However, women use behavioral disengagement (4.6±1.1 vs 4.2±1.1; p=0.002) and self-distraction (5.9±1.5 vs 5.5±1.7; p=0.019) more often than the men. Results further showed that there was no significant gender difference between respondents in the use of other coping strategies such as positive reframing, acceptance, active coping, planning, venting, denial, and self-blaming (Table 4).
There was a significant difference in the levels of adaptive coping strategies between males and females. Females showed a higher level of adaptive coping compared to males (42.5±4.9 vs 40.9±6.3, p=0.005). Females were found to use more emotional-focused coping than males (27.6 ±3.2 vs 26.4±4.0; p=0.001) (Table 4). In a multiple regression analysis, after controlling for demographic variables, the score of adaptive coping strategies and emotion-focused coping strategies were higher among female compared to male (Table 5).
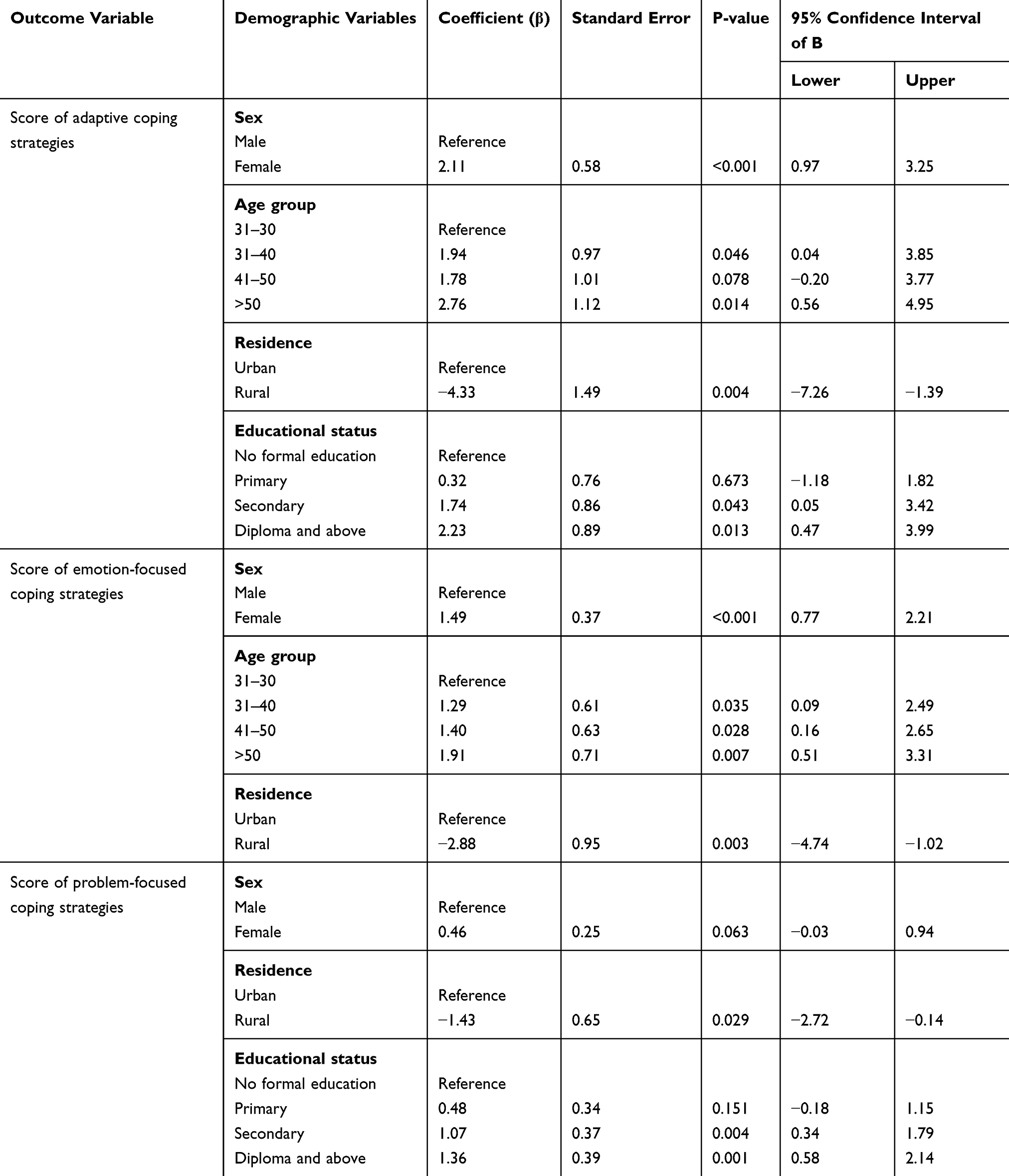 |
Table 5 Multivariable Linear Regression Models with Outcomes of Score of Adaptive Coping Strategies, Emotion-Focused Coping Strategies and Problem-Focused Coping Strategies for PLWHA in Jugal Hospital, Harar, Eastern Ethiopia |
Discussion
Analysis of perceived stigma among the study subjects revealed an average score of 65.3 (SD, 11.3). Although recent advances in medical technologies have made HIV a chronic and manageable condition, PLWHA continue to suffer from stigma.19 Total stigma scores are categorized into four stigma levels: minimal (32–56), low (57–80), moderate (81–104) and high (105–128). Based on this classification, the level of stigma reported in our study was low. This was quite similar to the findings of Li et al, in Henan province of China and Lingaraj et al, in Coimbatore, India.20,21 This may be explained by the fact that with the wide-scale ART rollout and better management of HIV, the fear of developing AIDS has now decreased in common people and resulted in a decrease in stigma.22
When both the groups were compared for perceived stigma, women scored slightly a higher mean score of perceived stigma. However, this difference was not statistically significant. Different studies from the Western and African settings found higher rates of perceived stigma in women than men.2,9,23,24 Women are traditionally expected to uphold the moral fabric of society.25 Social rejection (personalized stigma), negative self-image (internalized stigma) and total stigma were reported to be higher in women.24
Our findings indicated that women had a higher level of disclosure stigma than men. This result was consistent with the study conducted in Kenya, which showed that many women living with HIV reported high levels of stigma, leading to conceal their status from family and friends for fear of HIV/AIDS discrimination.26 The explanation for the high HIV stigma score may be that HIV-based stigma builds on other established biases related to gender. Women may suffer more stigma because the community may view them as being promiscuous at least once in their lifetime when they are infected with HIV.
Effective and appropriate coping strategies may minimize the impact of encountering stressful situations on one's well-being. In this study, we found that the major coping strategies employed by the study participants were positive reframing, turning to religion, acceptance and planning. These strategies are positive strategies that have been documented as very adaptive in studies and accelerate recovery from distress.27,28 We also found that a low level of substance use, which is a maladaptive strategy. Coping strategies adopted by PLWHA have very important practical applications as such strategies determine health outcomes and even the chances of spreading HIV to others.29 Among PLWHA, coping strategies such as behavioral disengagement and denial are found to be associated with disease progression and a poor psychological status, whereas the coping strategy of acceptance is associated with a lower level of distress.30
In this study, females used significantly more emotional-based coping than males. The findings are mixed with regard to gender differences in coping with HIV infection, ranging from studies that highlighted the lack of gender differences,31,32 to studies that pointed to a higher degree of avoidance coping, spiritual coping, and seeking social support as coping strategies for HIV-infected women.33,34
This study found that male patients were more likely than female patients to use substances. This is consistent with the finding that male patients were more likely to engage in risky behavior than female.35 In this study, females showed a higher level of adaptive coping compared to males. Our finding is consistent with the study from South Africa in which female patients were more likely to use adaptive strategies such as planning and religious practices.36 However, our findings do not support those of other authors, who found that more maladaptive than adaptive ways of coping were being used among women.37,38
There are some limitations to consider in interpreting the findings of the study. First, the participants in this study were actively involved in the hospital’s medical care and other services and may vary substantially from those individuals who have not visited medical cares. Thus, the patients in the present study may not be representative of all the PLWHA and limits the generalizability of our findings. Second, this study was cross-sectional; thus, cause and effect cannot be determined and it may not be sensitive to changes in levels of the measurements over time.
Conclusion and Recommendation
In this study, PLWHA in the study setting experienced a low level of perceived HIV stigma. This study suggests perceived HIV stigma may vary with gender due to unique traits of males and females. Women reported a higher level of disclosure stigma than their men counterpart. Thus, interventions to support PLWHA must take gender and the unique traits of males and females into account in terms of perceived stigma. In addition, it is critical to apply tailored approaches to address the different challenges faced by women and men living with HIV. Greater involvement of family, community and nongovernmental organizations is warranted to reduce the discrimination and increase support for women with HIV.
The major coping strategies employed by the respondents were positive reframing, turning to religion, acceptance and planning; these strategies are positive coping strategies. Females used significantly more emotional-based coping than males. Male patients were more likely than female patients to use substances. The use of maladaptive coping strategy should be discouraged by improving patients coping strategies to use adaptive and positive coping mechanisms. This can be achieved both by one-on-one health education in health facilities and through the mass media.
Acknowledgments
The authors greatly acknowledge Haramaya University for funding this research. Our special thanks go to our study participants for willing to participate in this study and to the data collectors for their management and collection of data.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brimlow DL, Cook JS, Seaton R. Stigma and HIV/AIDS: A Review of the Literature. Rockville, MD: US Department of Health and Human Services; 2003.
2. Nyblade L, Pande R, Mathur S, et al. Disentangling HIV and AIDS stigma in Ethiopia, Tanzania and Zambia. 2003.
3. Brown L, Macintyre K, Trujillo L. Interventions to reduce HIV/AIDS stigma: what have we learned? AIDS Educ Prev. 2003;15(1):49–69.
4. Silva R, Rocha V, Davim RMB, Torres G. Ways of coping with AIDS: opinion of mothers with HIV children. Rev Lat Am Enfermagem. 2008;16(2):260–265.
5. Deichert NT, Fekete EM, Boarts JM, Druley JA, Delahanty DL. Emotional support and affect: associations with health behaviors and active coping efforts in men living with HIV. AIDS Behav. 2008;12(1):139–145.
6. Myint T, Mash B. Coping strategies and social support after receiving HIV-positive results at a South African district hospital. SAMJ. 2008;98(4):276–277.
7. Asiedu G, Myers-Bowman K. Gender differences in the experiences of HIV/AIDS-related stigma: a qualitative study in Ghana. Health Care Women Int. 2014;35(7–9):703–727.
8. Gupta G, Selvaggio K. Addressing Gender in the AIDS Epidemic through PEPFAR Programs. Washington, DC: International Center for Research on Women. 2007.
9. Loutfy MR, Logie CH, Zhang Y, et al. Gender and ethnicity differences in HIV-related stigma experienced by people living with HIV in Ontario, Canada. PLoS One. 2012;7(12):e48168.
10. Malavé S, Ramakrishna J, Heylen E, Bharat S, ML E. Differences in testing, stigma, and perceived consequences of stigmatization among heterosexual men and women living with HIV in Bengaluru, India. AIDS Care. 2014;26(3):396–403.
11. Neuman M, Obermeyer CM; MATCH Study Group. Experiences of stigma, discrimination, care and support among people living with HIV: a four country study.. AIDS Behav. 2013;17(5):1796–1808.
12. Yebei VN, Fortenberry JD, Ayuku DO. Felt stigma among people living with HIV/AIDS in rural and urban Kenya. Afr Health Sci. 2008;8(2):97–102.
13. Carpenter A Gender differences in coping styles or just individual differences in the stress appraisal process. 2013.
14. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
15. Lifson AR, Demissie W, Tadesse A, et al. Barriers to retention in care as perceived by persons living with HIV in rural Ethiopia: focus group results and recommended strategies. J Int Assoc Provid AIDS Care. 2013;12(1):32–38.
16. Chivate P, Umate M, Nimkar S, Sousa AD. Gender differences in perceived stigma and hope in people living with HIV/AIDS: an exploratory study. Int J Commun Med Public Health. 2017;4(2):487–493.
17. Berger BE, Ferrans CE, FR L. Measuring stigma in people with HIV: psychometric assessment of the HIV stigma scale. Res Nurs Health. 2001;24(6):518–529.
18. Carver CS. You want to measure coping but your protocol’s too long: consider the brief COPE. Int J Behav Med. 1997;4(1):92–100.
19. Grossman CI, Stangl AL. Global action to reduce HIV stigma and discrimination. J Int AIDS Soc. 2013;16:18881.
20. Li Z, Sheng Y. Investigation of perceived stigma among people living with human immunodeficiency virus/acquired immune deficiency syndrome in Henan province, china. Int j Nurs Sci. 2014;1(4):385–388.
21. Chitra L, Jayalakshmi L, Vinod R. Stigma in women living with HIV in Coimbatore District of Tamil Nadu. IOSR J Dental Med Sci. 2015;13:29–32.
22. Kaai S, Bullock S, Sarna A, et al. Perceived stigma among patients receiving antiretroviral treatment: a prospective randomised trial comparing an m-DOT strategy with standard of-care in Kenya. SAHARA J. 2010;7:2.
23. Bond V, Levy C, Clay S, Kafuma T, Nyblade L, Bettega N. Kanayaka:” The light is on”: understanding HIV and AIDS related stigma in urban and rural Zambia. 2003.
24. Swendeman D, Rotheram-Borus MJ, Comulada S, Weiss R, Ramos ME. Predictors of HIV-related stigma among young people living with HIV. Health Psychol. 2006;25(4):501.
25. Ogden J, Nyblade L Common at its core: HIV-related stigma across contexts. 2005.
26. Colombini M, Mutemwa R, Kivunaga J, Moore LS, Mayhew SH. Experiences of stigma among women living with HIV attending sexual and reproductive health services in Kenya: a qualitative study. BMC Health Serv Res. 2014;14(1):412.
27. Kraaij V, van der Veek SM, Garnefski N, Schroevers M, Witlox R, Maes S. Coping, goal adjustment, and psychological well-being in HIV-infected men who have sex with men. AIDS Patient Care STDS. 2008;22(5):395–402.
28. Lewis CL, Brown SC. Coping strategies of female adolescents with HIV/AIDS. ABNF J. 2002;13(4):72.
29. Friedland J, Renwick R, McColl M. Coping and social support as determinants of quality of life in HIV/AIDS. AIDS Care. 1996;8(1):15–32.
30. Antoni MH. Phenomenology of HIV-1: A stress moderator model. Couns Psychol. 1991;19(4):543–550.
31. Ashton E, Vosvick M, Chesney M. Social support and maladaptive coping as predictors of the change in physical health symptoms among persons living with HIV/AIDS. AIDS Patient Care STDS. 2005;19(9):587–598.
32. Gore-Felton C, Koopman C, Turner-Cobb J, Duran R, Israelski D, Spiegel D. The influence of social support, coping and mood on sexual risk behavior among HIV-positive men and women. J Health Psychol. 2002;7(6):713–722.
33. Tarakeshwar N, Pearce M. Development and implementation of a spiritual coping group intervention for adults living with HIV/AIDS: a pilot study. Ment Health Relig Cult. 2005;8(3):179–190.
34. Vosvick M, Gore-Felton C, Koopman C, Thoresen C, Krumboltz J, Spiegel D. Maladaptive coping strategies in relation to quality of life among HIV adults. AIDS Behavior. 2002;6(1):97–106.
35. Mahalik JR, Levine Coley R, McPherran Lombardi C, Doyle Lynch A, Markowitz AJ, Jaffee SR. Changes in health risk behaviors for males and females from early adolescence through early adulthood. Health Psychol. 2013;32(6):685.
36. Olley BO, Gxamza F, Seedat S, et al. Psychopathology and coping in recently diagnosed HIV/AIDS patients-the role of gender. South Afr Med J. 2003;93(12):928–931.
37. Kaplan MS, Marks G, Mertens SB. Distress and coping among women with HIV infection: preliminary findings from a multiethnic sample. Am J Orthopsychiatry. 1997;67(1):80–91.
38. Sherbourne C, Forge NG, Kung F-Y, Orlando M, Tucker J. Personal and psychosocial characteristics associated with psychiatric conditions among women with human immunodeficiency virus. Women’s Health Issues. 2003;13(3):104–110.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.