Back to Journals » Clinical Interventions in Aging » Volume 17
Gender-Based Long-Term Outcomes After Revascularization for Three-Vessel Coronary Disease: A Propensity Score-Matched Analysis of a Large Cohort
Authors Liu Y, Zhu Y ![]() , Wang J, Yin D, Lv H, Qu S, Zhou X, Zhu H
, Wang J, Yin D, Lv H, Qu S, Zhou X, Zhu H ![]() , Guo L
, Guo L ![]() , Li Y
, Li Y
Received 11 February 2022
Accepted for publication 11 April 2022
Published 19 April 2022 Volume 2022:17 Pages 545—554
DOI https://doi.org/10.2147/CIA.S362027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Yuguo Liu,1,2,* Yifan Zhu,1,3,* Junjie Wang,1 Da Yin,1 Haichen Lv,1 Shenglin Qu,1 Xuchen Zhou,1 Hao Zhu,1 Lei Guo,1 Yuming Li4
1Department of Cardiology, The First Affiliated Hospital of Dalian Medical University, Dalian City, People’s Republic of China; 2Department of Cardiology, TEDA International Cardiovascular Hospital, Tianjin Medical University Clinical Cardiovascular Institute, Tianjin, People’s Republic of China; 3Jinzhou Medical University Dalian Friendship Hospital Postgraduate Training Base, Dalian City, People’s Republic of China; 4Department of Cardiology, Tianjin Economic-Technological Development Area (TEDA) International Cardiovascular Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Guo, Department of Cardiology, The First Affiliated Hospital of Dalian Medical University, 222 Zhongshan Road, Dalian City, 116011, People’s Republic of China, Tel +86 411-83635963, Email [email protected] Yuming Li, Department of Cardiology, Tianjin Economic-Technological Development Area (TEDA) International Cardiovascular Hospital, Tianjin, People’s Republic of China, Tel +86 22-65208888, Email [email protected]
Objective: To investigate the impact of gender on long-term outcomes after revascularization in patients with three-vessel disease (TVD), a severe and challenging subtype of coronary artery disease.
Methods: This was a single center retrospective cohort study. A total of 3776 patients with TVD who underwent revascularization between 2013 and 2018 were analyzed and were divided into the female group (n = 1039, 27.5%) and the male group (n = 2737, 72.5%). We performed a 1:2 propensity score matching (PSM) to balance the baseline characteristics, and a total of 1506 (504 matched pairs) patients were created after undertaking PSM. The primary outcome was the frequency of major adverse cardiac and cerebrovascular events (MACCE) including all-cause death, myocardial infarction, repeat revascularization, stroke, and readmission for angina pectoris or heart failure. The secondary outcome was the incidence of all-cause death.
Results: Through 2.4-year follow-up, no significant differences in MACCE (25.8% vs 27.5%, p = 0.279) and all-cause death (2.1% vs 2.2%, p = 0.888) were observed between the two cohorts. Similar results as with the early detection were obtained in propensity-matched patients. Multivariable analysis revealed that female gender (hazard ratio 0.99, 95% confidence interval 0.88– 1.17, p = 0.820) was not an independent predictor of MACCE but percutaneous coronary intervention (compared with coronary artery bypass graft surgery), hypertension, diabetes mellitus, atrial fibrillation, left main trunk involvement and left ventricular ejection fraction ≤ 40% were independently associated with a higher MACCE rate in these patients.
Conclusion: For patients with TVD after coronary revascularization, there were no gender-based differences in the long-term outcomes and female gender was not an independent predictor of MACCE.
Keywords: three-vessel disease, coronary revascularization, gender, outcomes, coronary artery disease
Introduction
Coronary artery disease (CAD) is the leading cause of death in women. The literature reports variation in the pathophysiology, clinical manifestations, and long-term prognosis of CAD between both genders. Based on multiple studies, women with CAD have a worse prognosis than men, mainly due to differences in their baseline characteristics, with women having a poor baseline cardiovascular risk profile.1–4
As a special and severe type of CAD, three-vessel disease (TVD) presents in nearly 30% of CAD patients,5 characterized by significant stenosis in all three major coronary arteries,6 and it remains one of the major challenging obstacles in coronary intervention. TVD confers an almost two-fold higher risk of mortality compared with single-vessel disease, which is also a significant risk factor for worse outcomes. Revascularization has shown long-term benefits in patients with TVD.7,8
However, there is a lack of evidence on the prognosis of TVD in female patients and the gender-based long-term outcomes of TVD remain unknown. Therefore, this study aims to investigate the impact of gender on the long-term outcomes after revascularization in TVD patients through a large cohort.
Methods
Study Population and Study Design
Coronary angiography was performed in 13,890 consecutively patients in our institution (the First Affiliated Hospital of Dalian Medical University) between January 2013 and December 2018. Out of 13,890, 4308 (31.0%) were TVD patients. In this study, patients receiving medical therapy alone or suffering from a malignant tumor, immune disease, severe liver, and renal failure were excluded. Thus, a total of 3776 patients with TVD undergoing revascularization were included in this study. The patients were divided into the female group (n = 1039, 27.5%) and the male group (n = 2737, 72.5%) (Figure 1). In this study, patients were considered with TVD through the angiographic confirmation of stenosis ≥ 50% in three epicardial coronary arteries, including the left anterior descending, left circumflex, and right coronary arteries, with or without involvement in the left main artery. Revascularization includes percutaneous coronary intervention (PCI) or coronary artery bypass graft surgery (CABG). In this study, all the stents deployed were drug-eluting stents (DES). A review of our institution’s medical records yielded baseline demographic information. Long-term clinical outcomes data were obtained by telephone, outpatient visits, and hospital readmissions.
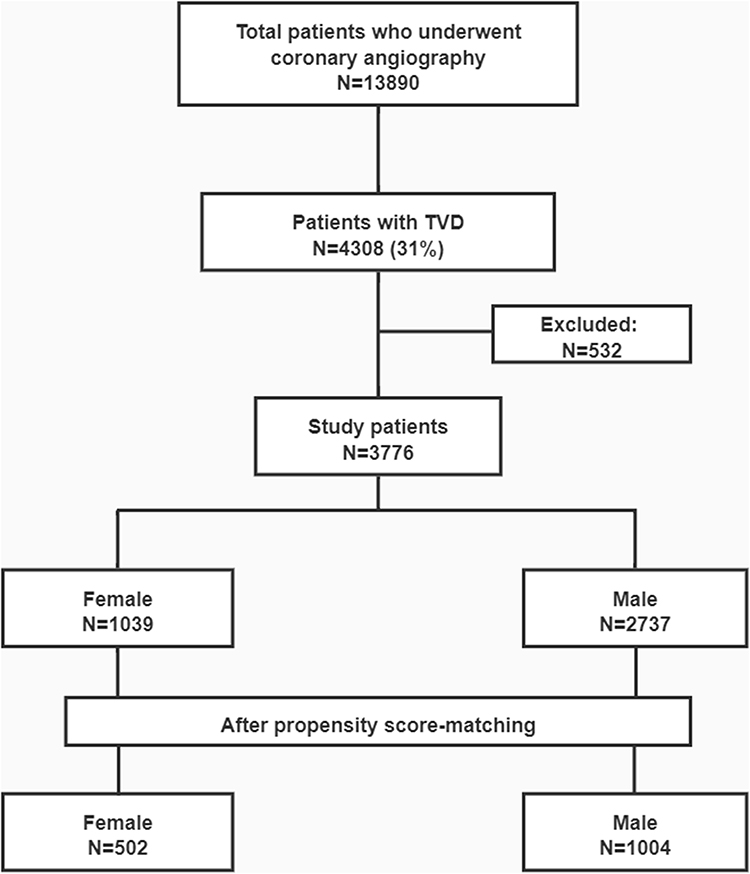 |
Figure 1 Study flow chart. Abbreviation: TVD, three-vessel disease. |
Ethics
This was a single-center, retrospective observational study approved by the Ethics Committee of the First Affiliated Hospital of Dalian Medical University. The protocol followed the ethical principles in the Declaration of Helsinki. All patients gave their written informed consent prior to any study procedures.
Procedures
All patients were treated with aspirin before the PCI and clopidogrel, 300–600 mg, either before PCI (pretreatment) or immediately after the procedure. Unfractionated heparin (70–100 U/kg loading) was administered before PCI and dosage was adjusted to achieve an activated clotting time of 200–250 s during the intervention.9 All patients were prescribed lifelong aspirin and clopidogrel for at least 12 months after the implantation of DES. CABG procedures could be done with or without extracorporeal circulation, and use of arterial conduits was encouraged.
Endpoints
The primary endpoint of this study was major adverse cardiac and cerebrovascular events (MACCE), which was defined a composite of all-cause death, myocardial infarction (MI), repeat revascularization, stroke, and readmission for angina pectoris or heart failure. The secondary outcome was all-cause death.
Statistical Analysis
For nonnormally distributed continuous variables, median and interquartile ranges or mean±standard deviations were estimated, whereas categorical variables were presented as frequencies and proportions. Chi-square tests were applied to evaluate group differences for categorical variables, while rank sum tests were used for continuous variables. Propensity score matching (PSM) was performed to adjust any potential confounders using the logistic regression model. All available variables with potential relevance were tested to estimate the propensity scores in Table 1. PSM was performed using a 1:2 matching protocol using the nearest-neighbor matching algorithm. The covariate balance achieved by matching was assessed by calculating the absolute standardized differences in covariates between the two groups. An absolute standardized difference of <10 for the measured covariate suggests appropriate balance between groups. Event-free survival was estimated by the Kaplan–Meier method, and differences among groups were assessed by means of the Log rank test. Cox proportional hazards methods were used to estimate the independent effect of multiple independent variables on the risk of MACCE. Covariates that were either statistically significant (with P value ≤ 0.1) on univariate analysis or clinically relevant were included in the multivariable Cox regression models. A two tailed probability value of P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 24.0 (SPSS, Inc., Chicago, Illinois) and Stata 15 (StataCorp, College Station, TX).
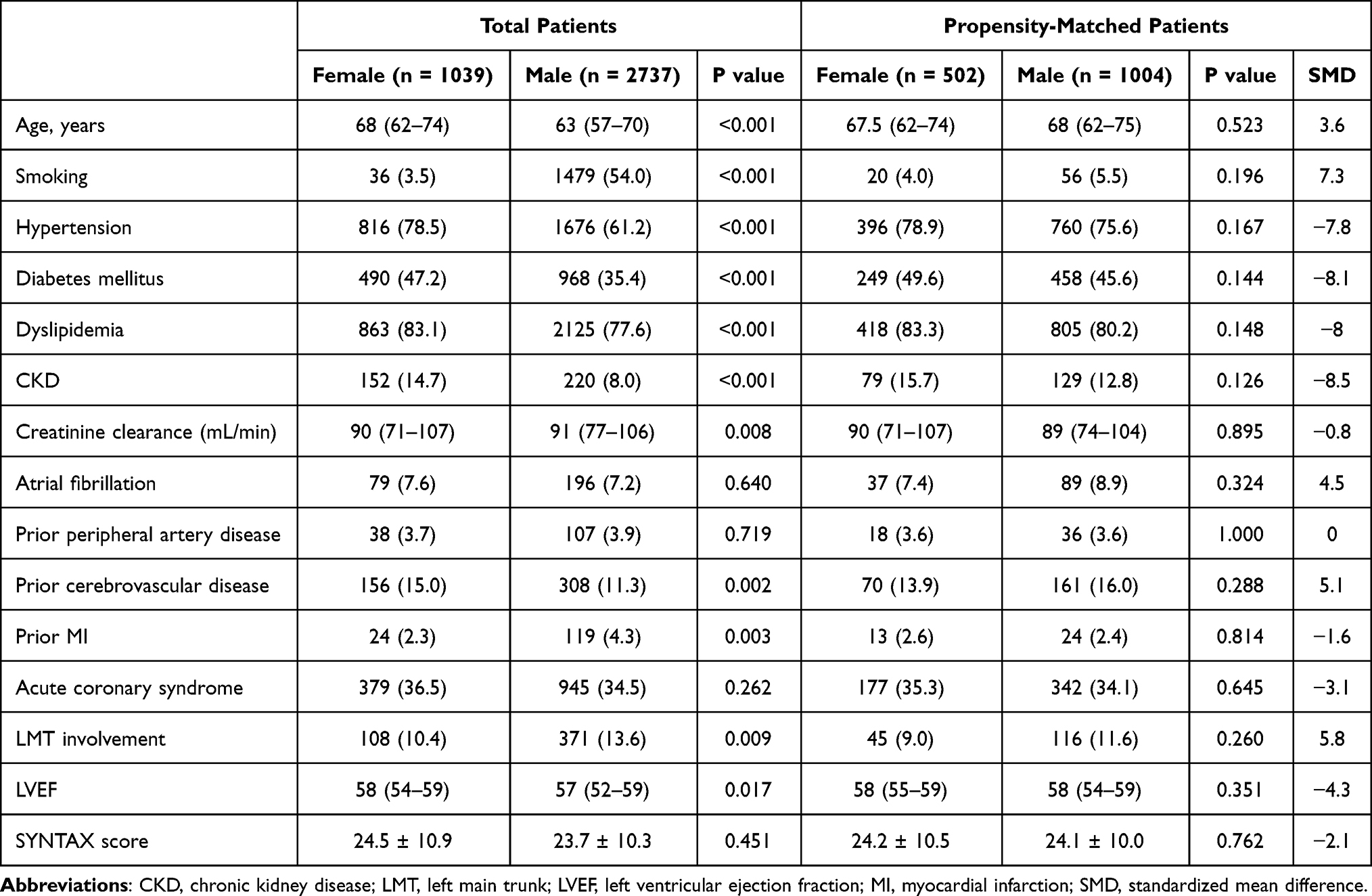 |
Table 1 Baseline Characteristics of Total and Propensity-Matched Patients |
Results
Patient Characteristics
The highest percentage of female patients was 31% in 2015, and the lowest percentage was 24% in 2016. From 2013 to 2015, the MACCE rate in female patients was nearly 30%, however, the MACCE rate had decreased to about 20% since 2016 (Figure 2). 3614 (95.7%) patients underwent PCI and 162 (4.3%) patients were treated with CABG. The baseline characteristics stratified by gender are shown in Table 1. The average age for females was significantly higher than for males. Females were more likely to suffer from chronic diseases such as hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease (CKD), cerebrovascular disease, and left main trunk (LMT) disease. On the other hand, smoking, previous MI, and lower left ventricular ejection fraction (LVEF) were more prevalent among men. However, no significant gender differences were observed in the case of acute coronary syndrome (ACS) and Syntax score. 715 (18.9%) patients were actually treated for three coronary vessels or/and left main and underwent complete revascularization. Among the patients who underwent CABG, internal thoracic artery was used in 154 (95%) patients. 55 patients died in-hospital during hospitalization. A total of 1506 patients were created after undertaking PSM for the entire population. The two matched groups showed no significant differences in baseline characteristics.
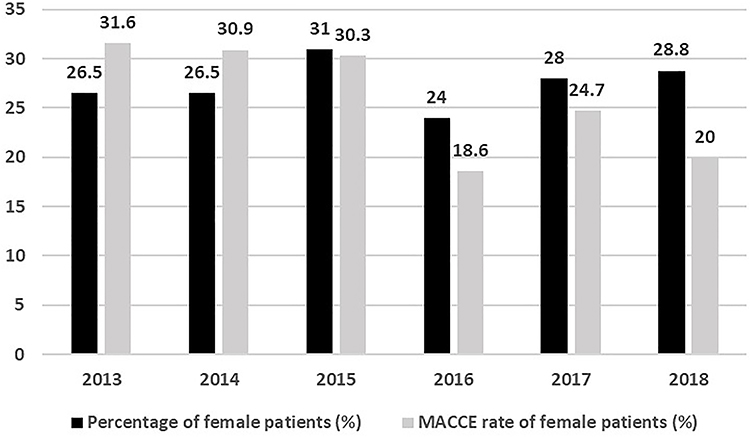 |
Figure 2 Trend in female percentage and annual MACCE percentage among females over years. Abbreviation: MACCE, major adverse cardiac and cerebrovascular events. |
Clinical Follow-Up
The median follow-up was 2.4 (1.1 to 4.1) years. When the two cohorts in MACCE (25.8% vs 27.5%, p = 0.279) and all-cause death (2.1% vs 2.2%, p = 0.888) were compared, no significant differences were observed. Female patients had a significantly low incidence of repeat revascularization (14.9% vs 19.1%, p = 0.003) and pectoris readmission (11.0% vs 14.6%, p = 0.004) compared to males. In contrast with male patients, female patients had a higher rate of readmission due to heart failure (9.3% vs 6.4%, p = 0.001). In the case of MI (8.9% vs 10.0%, p = 0.297) and stroke (1.4% vs 1.0%, p = 0.232), no significant differences were found between both genders (Table 2) (Figure 3).
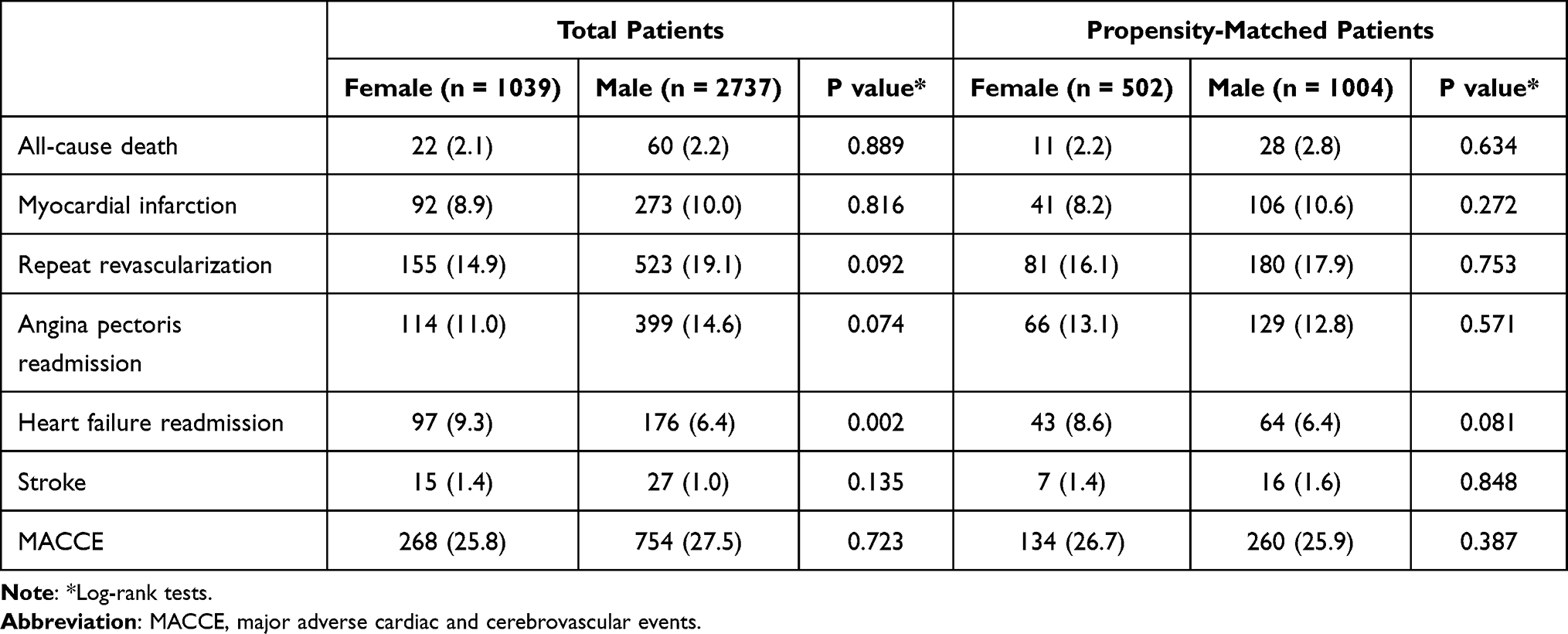 |
Table 2 Clinical Outcomes of Total and Propensity-Matched Patients |
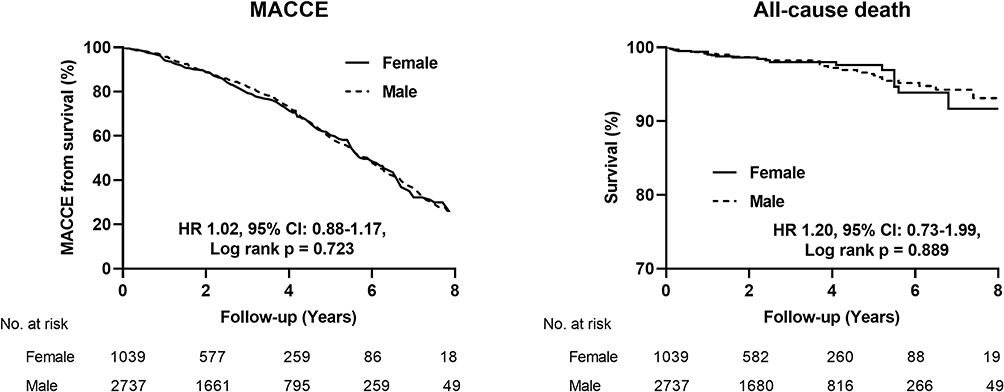 |
Figure 3 Kaplan–Meier analysis for major adverse cardiac and cerebrovascular events (MACCE) and all-cause death in total patients with TVD after revascularization. Abbreviation: TVD, three-vessel disease. |
Patients matched to propensity did not show significant differences compared in terms of MACCE rate (26.7% vs 25.9%, p = 0.387), all-cause death (2.2% vs 2.8%, p = 0.634), MI (8.2% vs 10.6%, p = 0.272), repeat revascularization (16.1% vs 17.9%, p = 0.753), pectoris readmission (13.1% vs 12.8%, p = 0.571), heart failure readmission (8.6% vs 6.4%, p = 0.081) and stroke (1.4% vs 1.6%, p = 0.848) (Table 2) (Figure 4).
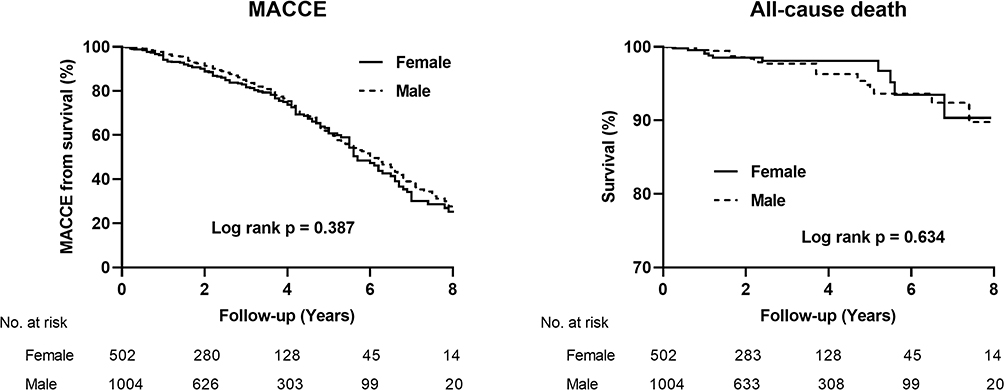 |
Figure 4 Kaplan–Meier analysis for major adverse cardiac and cerebrovascular events (MACCE) and all-cause death in propensity-matched patients with TVD after revascularization. Abbreviation: TVD, three-vessel disease. |
Adjusted Cox proportional-hazard analysis reveals significant association between a higher MACCE rate of patients underwent revascularization and PCI (hazard ratio [HR] 1.99, 95% confidence interval [CI] 1.43–2.77, p < 0.001), hypertension (HR 1.15, 95% CI: 1.00–1.32, p = 0.042), diabetes mellitus (HR 1.23, 95% CI: 1.08–1.39, p = 0.001), atrial fibrillation (HR 1.33, 95% CI: 1.08–1.63, p = 0.005), LMT involvement (HR 1.18, 95% CI: 1.07–1.30, p = 0.001) and LVEF ≤ 40% (HR 1.95, 95% CI: 1.65–2.32, p < 0.001) (Table 3). Furthermore, the analysis reveals that female gender was not an independent predictor of MACCE in patients who underwent revascularization (HR 1.02, 95% CI: 0.88–1.17, p = 0.780).
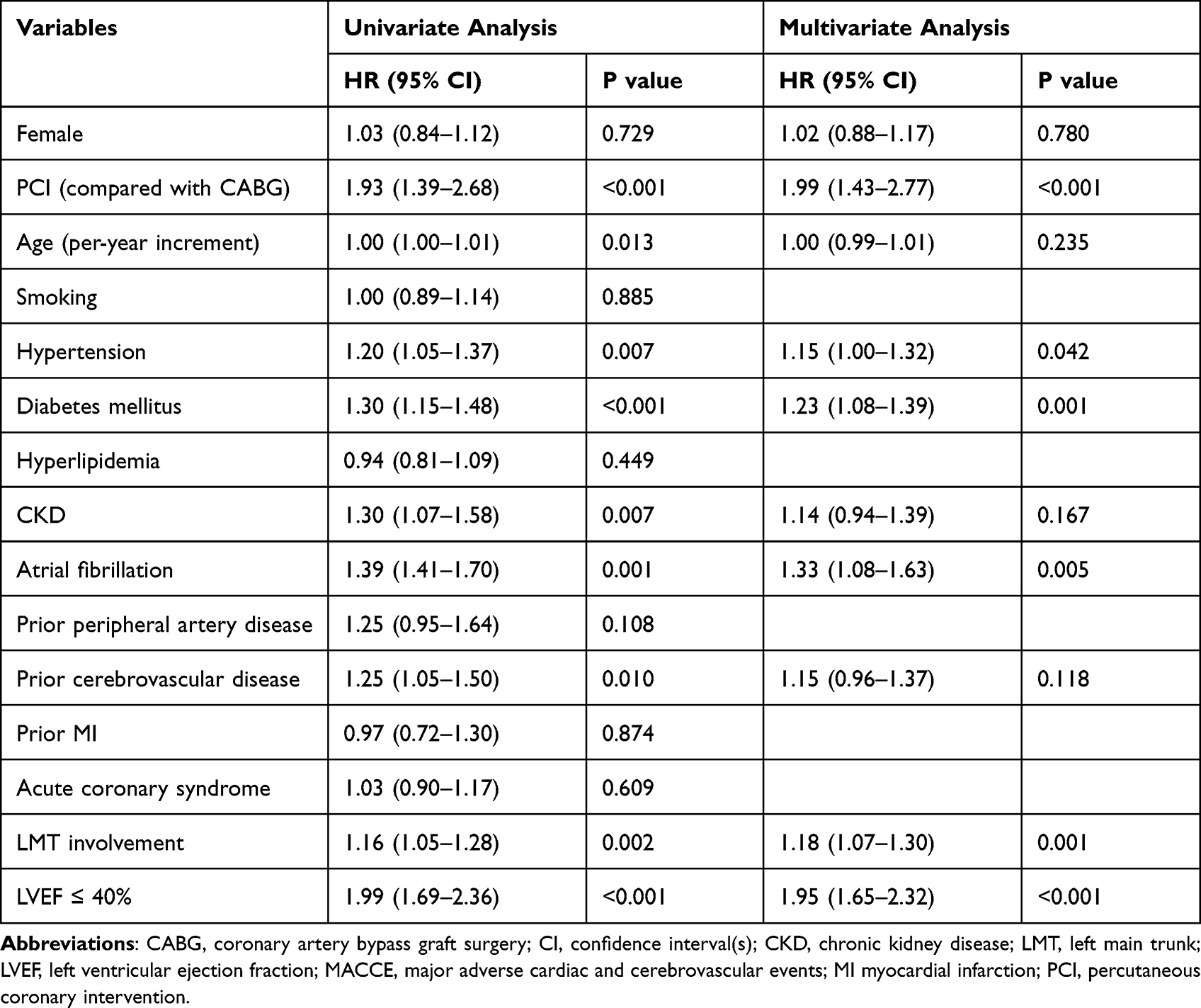 |
Table 3 Univariate and Multivariate Analysis of MACCE for the Entire Cohort |
Discussion
The principal clinical findings from this large cohort study can be summarized as follows: (1) female patients with TVD who underwent revascularization had more unfavorable baseline risk profiles, including hypertension, diabetes mellitus, dyslipidemia, CKD, prior cerebrovascular disease and LMT disease. (2) there were no sex-related differences in the long-term outcome after coronary revascularization among patient with TVD. (3) PCI (compared with CABG), hypertension, diabetes mellitus, atrial fibrillation, LMT involvement and LVEF ≤ 40% were independently associated with a higher MACCE rate in these patients. Female gender was not an independent predictor of MACCE.
Three-vessel disease is a special and severe form of CAD associated with a high risk of adverse outcomes, and it remains one of the major challenging obstacles in coronary intervention. We use an angiographic stenosis ≥50% as the criterion to define a coronary stenosis to put more emphasis on this severe type of CAD, which is consistent with previous study,7 though it is not a candidate to revascularization for non-left main arteries. Evidence shows that in women with TVD, revascularization was superior to medical therapy for the primary composite endpoint of overall mortality, unstable angina that required revascularization, or Q-wave MI.10 So far, there is a lack of sufficient evidence regarding the prognosis of TVD in female patients and the impact of gender on long-term outcomes after revascularization of TVD patients remains unclear. To the best of our knowledge, this is the first study to explore sex differences in long-term clinical outcomes following revascularization among patients with TVD.
Indeed, despite the well-established similarity in incidence of CAD among women and men, women are medically managed for their coronary disease more frequently. The study by Hollenbeak et al reveals that women with acute MI had 24% lower odds of receiving PCI after controlling for factors such as age, race/ethnicity, severity at admission, location of the infarct, or source of admission.11 Furthermore, studies show that women tend to have a smaller body size, smaller arterial diameter, hormonal differences, atypical and delayed presentation.12
Research shows that female patients were on average older than male patients at the time of their first invasive cardiovascular procedure. This may presumably be due to estrogen’s potentiating protective effects against coronary atherosclerosis until menopause, causing a delayed CAD process.3,13 Despite the high risk, females tend to have less severe obstructive epicardial CAD at elective angiography and have an increased incidence of microvascular disease, coronary spasm, and spontaneous coronary artery dissection than males.14,15 In our study, the number of male patients who underwent revascularization was nearly three times higher than that of female patients. Furthermore, at the time of coronary revascularization, women are older and have a worse cardiovascular risk profile and other comorbidities than men.16 In this regard, our data are consistent with previous studies.
After adjusting baseline risk profiles, there is insufficient data about gender-based differences in the long-term outcomes following coronary revascularization.17–19 Though some studies showed opposite results (sex-related differences were observed), in more recent trials, these differences were reduced.20 The reason may lie in the utilization of more advanced therapeutic methods, and in particular, the implantation of DES. According to previous studies, PCI may reduce or eliminate gender differences in mortality.11,18 In a recent study examining the impact of gender on prognosis in ACS patients receiving DES, although women had worse baseline characteristics, no difference in long-term outcomes among sexes was observed.21 In the present study, all patients who underwent PCI were implanted with DES were enrolled to prevent the confounding effect in the association between gender and outcome caused by using bare-metal stents.22
In the current study, we used propensity matching for available characteristics to create groups of women and men with balanced baseline characteristics, and showed that the long-term outcomes following coronary revascularization did not differ between the two cohorts. Furthermore, in line with former studies, we found that after adjustment for advanced age and comorbidities, sex was no longer an independent predictor of MACCE. Additionally, when combined endpoints including repeat revascularizations and re-hospitalizations are adopted, previous study showed different outcomes for PCI vs CABG for patients with complex coronary disease.23 Thus, we considered the strategy of revascularization as a relevant variable to be included within the multivariable adjustment to reduce the impact of confounding factors,24 and we found PCI (compared with CABG) was independently associated with a higher MACCE rate in these patients, possibly due to the incomplete revascularization of PCI, which was consistent with prior study.23 Therefore, with the latest refinement equipment and techniques, in treating patients with TVD, revascularization should be highly preferred as the treatment option and should not be limited by gender.
Limitations
This study is retrospective and is inherently limited by its design. Despite our efforts to adjust for all preoperative variables, there were still unadjusted confounders. Moreover, as all patients in our cohort have undergone revascularization (we excluded those treated only medically), so we have no data on the outcomes of conservative treatment patients. Therefore, these findings may not reflect the outcomes of all treatment modalities for TVD patients. In addition, angiographic evaluation of coronary stenosis is somewhat limiting both for percutaneous revascularization and for CABG where physiology assessment can be associated with a reduction of anastomoses and therefore procedural time and need for on pump surgery,25 and the use of physiology assessment in our study was relatively low. However, we believe that this real-world registry contributes to the present understanding of TVD prognosis in females undergoing revascularization and the imp act of invasive therapy in different subgroups of both genders.
Conclusion
The present study suggests no gender-based differences in long-term outcomes after coronary revascularization among TVD patients through a large cohort, and the female gender was not an independent predictor of MACCE. These findings may provide clinical insight into treatment options for unselected patients with TVD. Validating our findings requires further randomized controlled trials with long-term follow-up.
Abbreviations
TVD, three-vessel disease; MACCE, major adverse and cerebrovascular events; CAD, coronary artery disease; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft surgery.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors acknowledge all participants of the study and the interventional cardiologists and surgeons from the First Affiliated Hospital of Dalian Medical University. Especially, we acknowledge and thank Dr. Shaoke Meng for his invaluable assistance.
Funding
This study was supported by the Dalian Medical Science Research Project (2112002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Regitz-Zagrosek V, Oertelt-Prigione S, Prescott E, et al; Group EUCCS. Gender in cardiovascular diseases: impact on clinical manifestations, management, and outcomes. Eur Heart J. 2016;37(1):24–34.
2. Khamis RY, Ammari T, Mikhail GW. Gender differences in coronary heart disease. Heart. 2016;102(14):1142–1149. doi:10.1136/heartjnl-2014-306463
3. Guo L, Lv H, Zhong L, et al. Gender differences in long-term outcomes of medical therapy and successful percutaneous coronary intervention for coronary chronic total occlusions. J Interv Cardiol. 2019;24:484–488.
4. Hara H, Takahashi K, van Klaveren D, et al. Sex differences in all-cause mortality in the decade following complex coronary revascularization. J Am Coll Cardiol. 2020;76(8):889–899. doi:10.1016/j.jacc.2020.06.066
5. Bradley SM, Spertus JA, Kennedy KF, et al. Patient selection for diagnostic coronary angiography and hospital-level percutaneous coronary intervention appropriateness: insights from the National Cardiovascular Data Registry. JAMA Intern Med. 2014;174(10):1630–1639. doi:10.1001/jamainternmed.2014.3904
6. Min JK, Dunning A, Lin FY, et al. Age- and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings results from the International Multicenter CONFIRM (Coronary CT angiography evaluation for clinical outcomes: an International Multicenter Registry) of 23,854 patients without known coronary artery disease. J Am Coll Cardiol. 2011;58(8):849–860. doi:10.1016/j.jacc.2011.02.074
7. Xu JJ, Zhang Y, Jiang L, et al. Comparison of long-term outcomes in patients with premature triple-vessel coronary disease undergoing three different treatment strategies: a Prospective Cohort Study. Chin Med J. 2018;131(1):1–9. doi:10.4103/0366-6999.221273
8. Thuijs DJFM, Kappetein AP, Serruys PW, et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet. 2019;394(10206):1325–1334. doi:10.1016/S0140-6736(19)31997-X
9. Guo L, Wang J, Ding H, et al. Long-term outcomes of medical therapy versus successful recanalisation for coronary chronic total occlusions in patients with and without type 2 diabetes mellitus. Cardiovasc Diabetol. 2020;19(1):100. doi:10.1186/s12933-020-01087-4
10. Hueb W, Lopes N, Gersh BJ, et al. Ten-year follow-up survival of the Medicine, Angioplasty, or Surgery Study (MASS II): a randomized controlled clinical trial of 3 therapeutic strategies for multivessel coronary artery disease. Circulation. 2010;122(10):949–957. doi:10.1161/CIRCULATIONAHA.109.911669
11. Hollenbeak CS, Weisman CS, Rossi M, Ettinger SM. Gender disparities in percutaneous coronary interventions for acute myocardial infarction in Pennsylvania. Med Care. 2006;44(1):24–30. doi:10.1097/01.mlr.0000188915.66942.69
12. Douglas PS, Ginsburg GS. The evaluation of chest pain in women. N Engl J Med. 1996;334(20):1311–1315. doi:10.1056/NEJM199605163342007
13. Guo L, Lv HC, Huang RC. Percutaneous coronary intervention in elderly patients with coronary chronic total occlusions: current evidence and future perspectives. Clin Interv Aging. 2020;15:771–781. doi:10.2147/CIA.S252318
14. Shaw LJ, Bugiardini R, Merz CN. Women and ischemic heart disease: evolving knowledge. J Am Coll Cardiol. 2009;54(17):1561–1575. doi:10.1016/j.jacc.2009.04.098
15. Mehta LS, Beckie TM, DeVon HA, et al. Acute myocardial infarction in women: a scientific statement from the American Heart Association. Circulation. 2016;133(9):916–947. doi:10.1161/CIR.0000000000000351
16. Heer T, Hochadel M, Schmidt K, et al. Sex differences in percutaneous coronary intervention-insights from the coronary angiography and PCI registry of the German Society of Cardiology. J Am Heart Assoc. 2017;6(3):e004972. doi:10.1161/JAHA.116.004972
17. Kovacic JC, Mehran R, Karajgikar R, et al. Female gender and mortality after percutaneous coronary intervention: results from a large registry. Catheter Cardiovasc Interv. 2012;80(4):514–521. doi:10.1002/ccd.23338
18. Duvernoy CS, Smith DE, Manohar P, et al. Gender differences in adverse outcomes after contemporary percutaneous coronary intervention: an analysis from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium (BMC2) percutaneous coronary intervention registry. Am Heart J. 2010;159(4):677–683.e671. doi:10.1016/j.ahj.2009.12.040
19. Lansky AJ, Hochman JS, Ward PA, et al. Percutaneous coronary intervention and adjunctive pharmacotherapy in women: a statement for healthcare professionals from the American Heart Association. Circulation. 2005;111(7):940–953. doi:10.1161/01.CIR.0000155337.50423.C9
20. Thompson CA, Kaplan AV, Friedman BJ, et al. Gender-based differences of percutaneous coronary intervention in the drug-eluting stent era. Catheter Cardiovasc Interv. 2006;67(1):25–31. doi:10.1002/ccd.20564
21. Fath-Ordoubadi F, Barac Y, Abergel E, et al. Gender impact on prognosis of acute coronary syndrome patients treated with drug-eluting stents. Am J Cardiol. 2012;110(5):636–642. doi:10.1016/j.amjcard.2012.04.039
22. Guo L, Zhong L, Chen K, Wu J, Huang RC. Long-term clinical outcomes of optimal medical therapy vs. successful percutaneous coronary intervention for patients with coronary chronic total occlusions. Hellenic J Cardiol. 2018;59:281–287. doi:10.1016/j.hjc.2018.03.005
23. Bertaina M, De Filippo O, Iannaccone M, et al. Percutaneous coronary intervention or coronary artery bypass graft in left main coronary artery disease: a comprehensive meta-analysis of adjusted observational studies and randomized controlled trials. J Cardiovasc Med. 2018;19(10):554–563. doi:10.2459/JCM.0000000000000703
24. Yang L, Guo L, Lv H, et al. Predictors of adverse events among chronic total occlusion patients undergoing successful percutaneous coronary intervention and medical therapy. Clin Interv Aging. 2021;16:1847–1855. doi:10.2147/CIA.S337069
25. Bruno F, D’Ascenzo F, Marengo G, et al. Fractional flow reserve guided versus angiographic guided surgical revascularization: a meta-analysis. Catheter Cardiovasc Interv. 2021;98(1):E18–E23. doi:10.1002/ccd.29427
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.