Back to Journals » Therapeutics and Clinical Risk Management » Volume 19
Gastric Emptying Velocity After Labor Analgesia Assessed by Sonography: A Prospective Controlled Observational Study
Received 3 March 2023
Accepted for publication 5 June 2023
Published 16 June 2023 Volume 2023:19 Pages 475—484
DOI https://doi.org/10.2147/TCRM.S410984
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Yongfeng Liu,1 Qian Wang,1 Qinghai Zuo2
1Department of Anesthesiology, Medical Center Hospital of Qionglai, Qionglai City, Sichuan Province, People’s Republic of China; 2Department of Anesthesiology, People’s Hospital of Hechuan, Chongqing City, People’s Republic of China
Correspondence: Qinghai Zuo, Department of Anesthesiology, People’s Hospital of Hechuan, 1366 Hill Avenue, Hechuan District, Chongqing City, 401519, People’s Republic of China, Tel +23-42823120, Fax +23-42824243, Email [email protected]
Objective: The effect of labor analgesia on gastric emptying rate will affect the management of fasting during the perinatal period. To evaluate gastric emptying after labor analgesia using the gastric antrum ultrasound examination.
Methods: From September 2022 to January 2023, a prospective controlled observational study was conducted. The Study group (epidural analgesia group) and Observation group (pharmacological and non-pharmacological interventions group) were successively enrolled and grouped using the random envelope method. However, labor analgesia was supplied according to maternal women’s wishes, and intention-to-treat (ITT) and per-protocol (PP) analyses were performed to establish its effect on stomach emptying. The gastric emptying rate during the first stage of labor was considered to be the primary outcome.
Results: From September 2022 to January 2023, 120 persons were studied, 90 in the Study group and 30 in the Observation group. 33 people’s analgesic selection was discordant with the grouped one. ITT analysis showed that the Study group’s cross-sectional area (CSA) fell from baseline (624.19 ± 92.70 mm2) to 334.64 ± 46.32 mm2 after 1 hour and to 217.26 ± 29.90 mm2 after 2 hours. In the Observation group, the CSA similarly dropped from 620.10 ± 100.73 mm2 to 331.30 ± 51.19 mm2 and 214.70 ± 28.73 mm2, p< 0.001. CSA was not significantly different between groups, p> 0.05. The PP analysis also indicated no significant changes in the CSA between the two groups at 3 time-points, p> 0.05. At the first hour, the Study and Observation group had stomach emptying speeds of 300.05 ± 103.74 mm2/h and 259.50 ± 125.25 mm2/h, respectively, which were greater than those at the second hour (115.75 ± 43.51 mm2/h vs 124.36 ± 58.98 mm2/h), p< 0.001.
Conclusion: Epidural analgesia, pharmacological, and non-pharmacological labor analgesia had little effect on gastric emptying, and gastric antrum ultrasonography can be utilized to monitor maternal gastric volume changes.
Keywords: epidural anesthesia, antrum ultrasound, gastric emptying, natural delivery
Introduction
Aspiration of gastric contents is a rare but serious complication of anesthesia,1 which accounts for 9% of all anesthesia-related mortality.2,3 The main risk factors for aspiration are the presence of gastric contents and the delay of gastric emptying.4 Pregnant women are at increased risk for this complication due to the increased intra-gastric pressure associated with the pregnant uterus, which favors gastro-oesophageal regurgitations,5 the increased risk of difficult intubation in the event of general anesthesia,6 and the increased volume of gastric contents, which is primarily caused by delayed gastric emptying during labor.7 In addition, The practice of strict fasting during childbirth has been questioned, and there is a report supporting maternal eating during the perinatal period at their discretion.8 Existing research on the effect of labor analgesia, such as epidural analgesia, pharmacological and non-pharmacological interventions, on gastric emptying is limited. The quantification of the gastric volume and contents may be of particular interest to obstetric anesthetists when emergency anesthesia is required and to improve the fasting management of the perinatal period.
Antrum ultrasound is a new application of bedside ultrasound technology, which can evaluate gastric volume by measuring the cross-sectional area (CSA) of the antrum.9 It allows a standardized and easy-to-perform measurement of the observed antral area, with good intra and inter-rater reliability.10 In the non-pregnant adult, the antral area measured in the supine position correlates positively with the gastric volume.9 Studies have shown that gastric antrum ultrasonography is also reliable in evaluating gastric volume in women in the third trimester.11,12 Therefore, this study focuses on the effect of labor analgesia on gastric emptying, and uses non-invasive bedside ultrasound to evaluate it, exploring fasting management of the perinatal period and the likelihood of satiety parturient assessed by the CSA of the antrum.
Methods and Materials
Design, Patients, Grouping
A prospective controlled observational study was conducted among pregnant women who gave birth naturally at the Medical Center Hospital of Qionglai from September 2022 to January 2023. The inclusion criteria were as follows: (1) primipara aged 20–40 years; (2) at third trimesters with gestational weeks more than 37 weeks; (3) pregnant women were without obvious abnormalities in the previous prenatal examination and at low risk; (4) voluntarily participated in this study, signed informed consent, and with good compliance. Exclusion criteria were as follows: (1) patients diagnosed with gastroparesis, or combined with esophageal, duodenal, or gastric diseases, or had a history of gastrointestinal surgery; (2) patients who underwent the treatment of serotonin 3 (5-HT3) receptor antagonists and metoclopramide for nausea and vomiting; (3) patients with contraindications for epidural analgesia, such as coagulation dysfunction, usage of anticoagulant drug, scoliosis, or infection at the puncture site; (4) multiple pregnancy; (5) pregnant women with high-risk pathologic pregnancies; (6) be allergic to local anesthetics; (7) be diagnosed with gestational diabetes and gestational hypertension; (8) after 9 weeks of the gestational week, patients still complicated with pregnancy nausea and vomiting; (9) patients with obesity, body mass index (BMI)>35, with or without obstructive sleep apnea; (10) patients who refuse to participate in this study, or were participating in other clinical trials, or who cannot cooperative. Cases in which the study protocol was not strictly followed due to inadequate analgesia and take multi-modal analgesia and cases in which a natural vaginal delivery cannot be achieved and converted to cesarean section were considered as off-cases.
Maternal patients who were admitted to the hospital due to childbirth and met the inclusion and exclusion criteria were successively enrolled and grouped according to the random envelope method and were included in the Study group (epidural analgesia group) and the Observation group (pharmacological and non-pharmacological interventions group) respectively, until the number of patients included satisfied the expected sample size of each group. Labor analgesia was given according to the will of maternal women and finally, the intention-to-treat (ITT) analysis and per-protocol (PP) analysis were carried out to study the effect of labor analgesia on gastric emptying.
The study was designed and implemented in accordance with the Declaration of Helsinki and International Ethical Guidelines for Biomedical Studies Involving Human Subjects. The study protocol has been reviewed and approved by the Ethics Committee of Medical Center Hospital of Qionglai [No. (2022) 42, 2022/08/16] and has been prospectively registered in the Chinese Clinical Trial Registry (ChiCTR2200063277, 2022/09/02).
Study Protocol
When the visual analogue scale (VAS) was greater than 3 and analgesia was needed, the patients were given an experimental diet consisting of 300mL mineral water and 100mL porridge with corn and Lotus (70 kcal, 11.6% protein, 15.7% lipid, 72.7% carbohydrate), and were required to consume it within 15 minutes. Subsequently, the labor analgesic management would be performed according to the patients’ will.
Before the implementation of labor analgesia management (Tbaseline), patients were placed under ASA standard anesthesia,13 given low-flow oxygen therapy, and intravenous infusion channels were established. Subsequently, all patients underwent gastric ultrasonography and obstetric examination to obtain the CSA of the antrum,1 gestational weeks, fetal weight, amniotic fluid index (AFI), abdominal circumference, and uterine height. The antrum sonography would be reexamined twice after taking the experimental diet and underwent the labor analgesia, with an hour interval to assess the changes of CSA of the antrum. In addition, The VAS would be assessed at the end of the first stage of labor (T1) and at 30 minutes after the delivery of the placenta (T2). Generally, 20 international units (IUs) of Oxytocin (Shanghai Hefeng Pharmaceutical Co., LTD, China) were diluted in 500 mL 0.9% saline and were administrated by intravenous (IV) infusion for over one hour if necessary. And the timing of the administration and whether followed by an additional 20 IUs in 1 L of fluid at a rate of 125 mL/hour were determined by the responsible obstetrician.
Analgesic Regimen and Effect Evaluation
The Study group took epidural analgesia plus patient-controlled epidural analgesia (PCEA) for labor analgesia. After a routine epidural puncture, the experimental dose (3mL, 1% lidocaine and 1:200,000 epinephrine) was given into the epidural space. After observation for 5 minutes, the epidural analgesic management was continued if no dramatic changes in heart rate and deep motor block occurred. The initial dose was 20mL of 0.1% ropivacaine combined with 2μg/mL of fentanyl, which was administered equally 4 times and with a duration over 30 seconds, and withdrawal was performed between the two injections. After the completion of the administration, cold stimulus and pinprick were used to evaluate the sensory level, with the target dermatome level around the umbilicus. After the block level was stabilized, the PCEA analgesic pump was connected, and 0.1% ropivacaine 10mL combined with 2μg/mL fentanyl was given every 10–15 minutes. Patients could receive bolus injections according to their own needs, with 3mL 0.1% ropivacaine combined with 2μg/mL fentanyl each injection, locking for 15 minutes.
The Observation group was treated with pharmacological and non-pharmacological interventions for labor analgesia. Non-pharmacological methods, including listening to music, being accompanied by a partner, using the birth ball under the midwife’s guidance, etc. were used in the early stages until the cervix opened to 3–4cm, and a single intravenous injection of 0.02mg/kg midazolam and 1μg/kg fentanyl was used for analgesia. Respiratory depression and VAS were then monitored and the same drug regimen was administered as necessary.
When the satisfactory analgesic goals of each group still could not be achieved after the labor analgesia management described above, further analgesic approaches would be integrated and patients would be administered multi-modal analgesia.
Antrum Sonography and Gastric Emptying
The patients who underwent gastric antrum ultrasonography were all in semi-decubitus position, with the head tilted 45 degrees upward. The low-frequency array probe (2–5MHz) of a portable ultrasound machine (M5, Mindray Medical Group Inc, China) was used to scan the antrum. The maximum diameter of the antrum (longitudinal diameter D1 and anteroposterior diameter D2) was measured during the intersystolic phase of the antrum, including the thickness of the entire gastric wall from the serous membrane to the serous membrane. The values of D1 and D2 were measured two times and the average values were used to calculate the CSA of the antrum by the formula as follows: The CSA of the antrum S= (π × D1 × D2)/4.14 A sonographer and an anesthesiologist participated in the antrum ultrasound examination respectively, and both of them had undergone training in antrum sonography and with actual operation cases over 69.
After taking the experimental diet and before administering the labor analgesia, The first scan of the CSA of the antrum (CSAbaseline) was made and the CSAbaseline was taken as the baseline value. The changes of the CSA of antrum at first two hours after taking the experimental diet and finishing the labor analgesia were seen as the gastric emptying velocity, ∆S1=(CSAbaseline-CSApost 1hr) and ∆S2=(CSApost 1hr-CSApost 2hrs).
The Outcomes
The gastric emptying rate during the first stage of labor was considered to be the primary outcome. The secondary outcomes were the VAS at three time periods, the duration of the first, second, and third phases of labor, the total doses of opioids administered, the incidence of nausea and vomiting, and pulmonary problems following delivery. Demographic data of the maternal patients, such as height, weight, BMI, gestational weeks, fundal height, abdominal circumference, fetal weight, AFI, and Apgar score after birth were taken as other outcomes. Aspiration, aspiration pneumonia, and local anesthetic poisoning were considered adverse events.
Sample Size Estimation and Statistic
According to the analysis of the mean and standard deviation of the pre-test results of the gastric emptying velocity at the first stage of labor in two parturients, the non-inferiority test was used, and the defined value of non-inferiority was assumed to be 0.6, and the α value was set to be 0.05 and β=0.2, which could achieve the power of a test to be 80%. Using the PASS software (version 15.0, NCSS, LLC), the number of the Study group is set to be three times that of the Observation group. Considering the 20% off rate, it is finally calculated that 90 patients should be included in the Study group and 30 in the Observation group.
In this study, ITT analysis and PP analysis were combined to analyze the included patients and collected data. SPSS 23.0 software (SPSS, Chicago, Illinois, USA) was used for analysis. Normal distribution measurement data were expressed as mean ± standard deviation, and the Student-t-test was used for comparison. Repeated measurement analysis of variance (ANOVA) within and between the two groups (time effect and time*group effect, respectively), and multiple comparisons were carried out between three-time points by the LSD method. The categorical data were expressed as n(%), and the differences between the two groups were examined by chi-square analysis or Fisher’s exact test. A p value less than 0.05 was seen as a significant difference.
Results
From September 2022 to January 2023, 141 expectant women who intended to give birth naturally at the Medical Centre Hospital of Qionglai met the inclusion and exclusion criteria and were considered research subjects. Four patients who refused to participate in the study were excluded, and the remaining 137 patients were randomly assigned, with 98 patients assigned to the Study group and 39 to the Observation group. In the Study group, eight women who received epidural analgesia for other obstetric reasons were excluded, so the ITT analysis was conducted on 90 patients. 17 of these 90 women received pharmacological and non-pharmacological intervention, leaving 73 women for PP analysis. In the Observation group, 23 of 39 women received pharmacological and non-pharmacological intervention, but of these, 4 required a higher level of analgesic intervention, and 5 converted to cesarean section for other obstetric reasons, so PP analysis was conducted on a total of 14 women. Another 16 individuals in the Observation group underwent epidural analgesia, so a total of 30 people went through the ITT analysis (Figure 1).
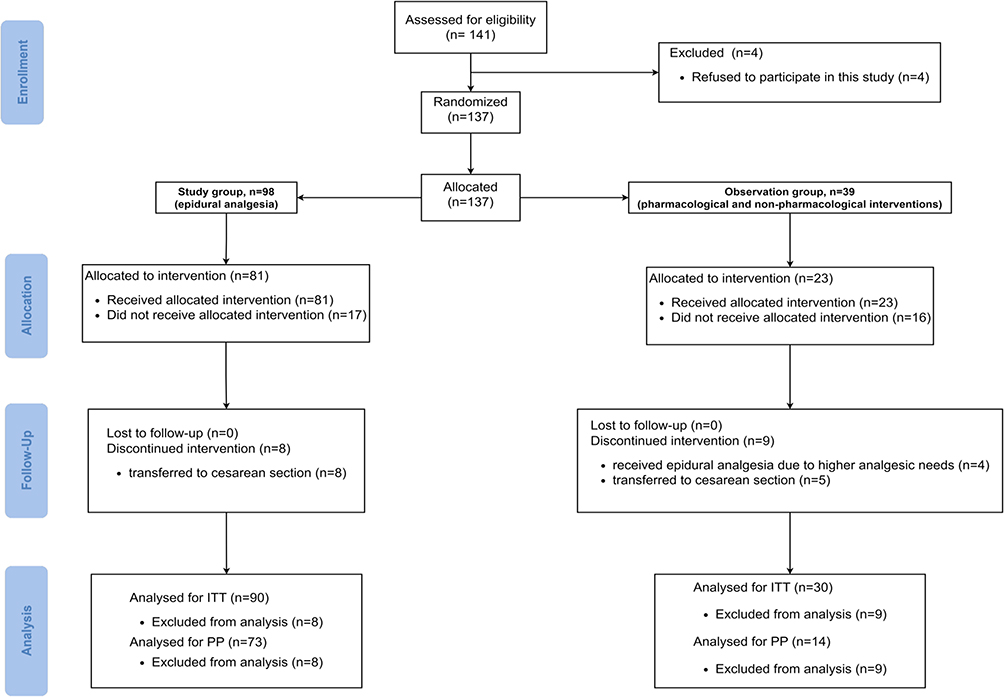 |
Figure 1 The CONSORT flow diagram. Abbreviations: ITT, Intention-to-treat; PP: Per-protocol. |
Results of Intention-to-Treat Analysis
There were no statistically significant differences between the Study group and the Observation group in basic demographic data, fetal weight, labor duration, VAS scores at three time-points, and Apgar score at 1 minute postpartum, p>0.05. The Apgar score at 5 minutes postpartum of the Observation group was 10.00 ± 0.00, which was higher than 9.79 ± 0.51 of the Study group, p=0.025 (Table 1).
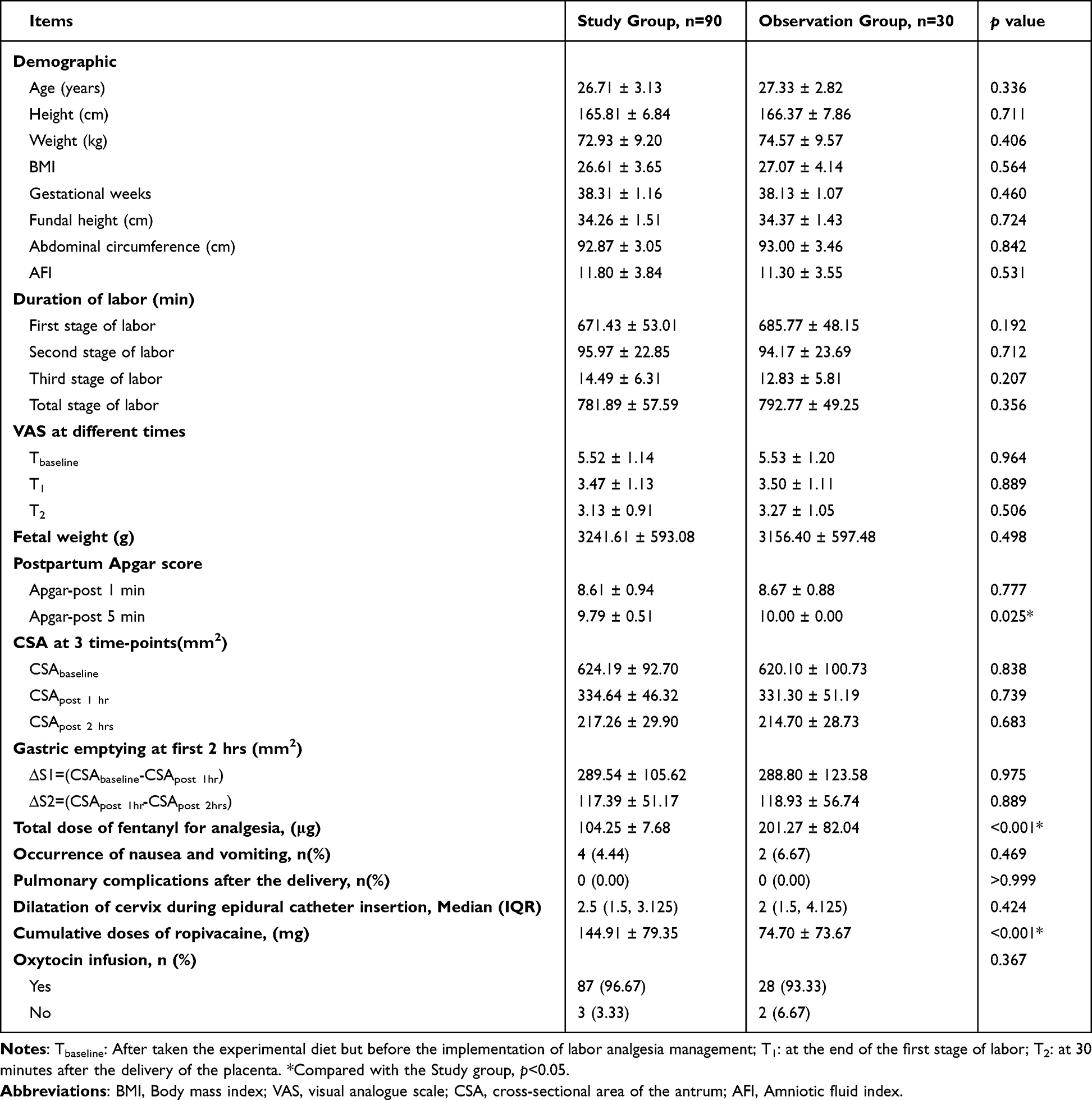 |
Table 1 Results of Intention-to-Treat Analysis |
In the Study group, the CSA decreased from the baseline (624.19 ± 92.70 mm2) to 334.64 ± 46.32 mm2 after 1hr, p<0.001, and to 217.26 ± 29.90 mm2 after 2 hrs, p<0.001. Accordingly, in the Observation group, the CSA also decreased from 620.10 ± 100.73 mm2 to 331.30 ± 51.19 mm2 and 214.70 ± 28.73 mm2, p<0.001. However, there was no significant difference in CSA between the two groups, p>0.05. Similarly, the VAS in the Study group and the Observation group dropped from the baseline (5.52 ± 1.14 vs 5.53 ± 1.20) to (3.47 ± 1.13 vs 3.50 ± 1.11) at T1 and to (3.13 ± 0.91 vs 3.27 ± 1.05) at T2, p<0.001 (Table 1) (Figure 2).
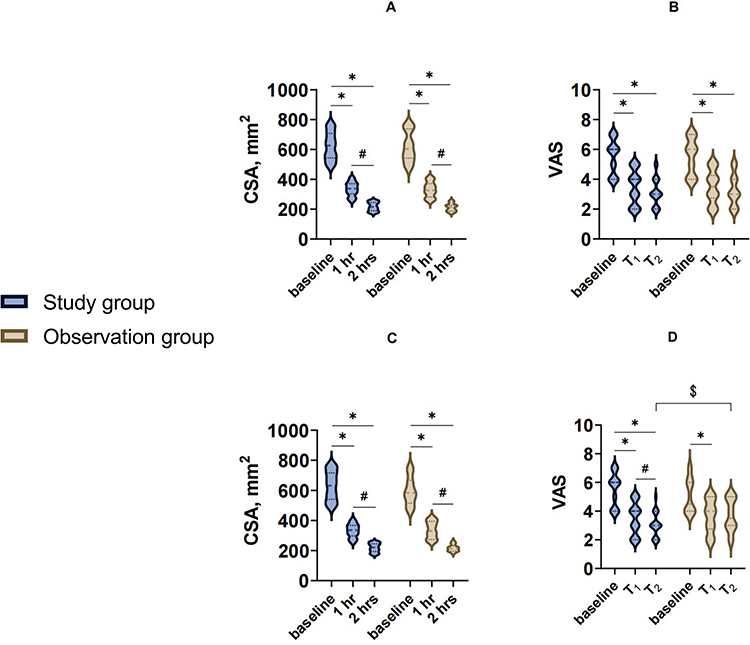 |
Figure 2 The changes of CSA and VAS. (A and B) show the results of ITT analysis, (C and D) show the results of PP analysis. Abbreviations: ITT, Intention-to-treat; PP, Per-protocol; CSA, cross-sectional area of the antrum; VAS, visual analogue scale. Notes: *Compared with the baseline, p<0.001. #Compared with the 1 hr or T1,p<0.001. $Compared with the observation group, p<0.001. |
The gastric emptying speed at the first hour is 289.54 ± 105.62 mm2/h in the Study group and 288.80 ± 123.58 mm2/h in the Observation group, which were all higher than those at the second hour (117.39 ± 51.17 mm2/h vs 118.93 ± 56.74 mm2/h), p<0.001. However, there was no significant difference between the two groups, p>0.05. The total dose of fentanyl for analgesia used in the Observation group was 201.27 ± 82.04 μg, which was higher than that in the Study group, 104.25 ± 7.68 μg, p<0.001. But the infusion of ropivacaine was 74.70 ± 73.67 mg, which was lower than that in the Study group, 144.91 ± 79.35 mg, p<0.001. There were no differences between the two groups in the occurrence of nausea and vomiting, the pulmonary complications rate after the delivery, the oxytocin infusion rate, and the dilatation of cervix during epidural catheter insertion, p>0.05 (Table 1).
Results of per-Protocol Analysis
Consistent with the results of ITT analysis, there were no statistically significant differences in demographic data, fetal weight, and other data between the two groups, p>0.05. The VAS in the Study group decreased from the baseline to levels at T1 and at T2, p<0.001. Meanwhile, the VAS in the Study group at T2 was 3.05 ± 0.85 which was lower than that of the Observation group, 3.71 ± 1.14, p=0.014. In the Observation group, compared with the VAS score at baseline, VAS decreased at T1, but there was no difference in the VAS between T1 and T2, p>0.05 (Table 2) (Figure 2).
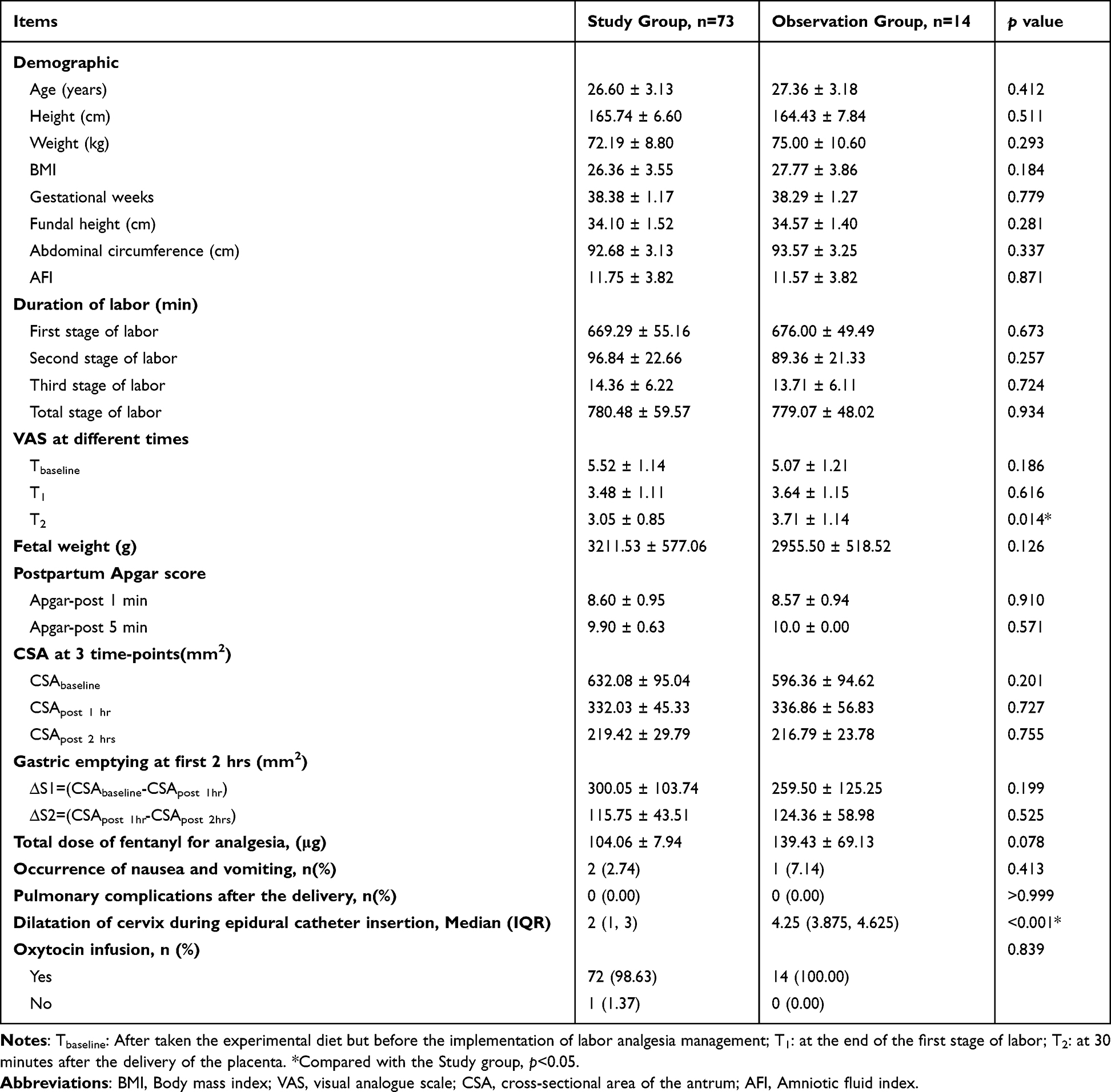 |
Table 2 Results of per-Protocol Analysis |
There was no significant difference in CSA between the two groups at 3 time-points, p>0.05. In both groups, the CSA decreased from the baseline level to levels after 1 hr and 2 hrs, p<0.001. Similarly, the gastric emptying speed at the first hour is 300.05 ± 103.74 mm2/h in the Study group and 259.50 ± 125.25 mm2/h in the Observation group, which were all higher than those at the second hour (115.75 ± 43.51 mm2/h vs 124.36 ± 58.98 mm2/h), p<0.001. The median dilatation of cervix during epidural catheter insertion was 4.25 (3.875, 4.625) cm in the Observation group, which was bigger than that in the Study group 2 (1, 3) cm, p<0.001. However, there was no significant difference between the two groups, p>0.05. The total dose of fentanyl used for analgesia, the incidence of nausea and vomiting, the oxytocin infusion rate, and the rate of pulmonary problems after delivery did not differ between the two groups, p>0.05 (Table 2) (Figure 2).
Occurrence of Adverse Events
Throughout the prenatal period, aspiration, aspiration pneumonia, and local anesthetic toxicity did not occur in either group.
Discussion
In this study, ultrasound was used to assess the changes in the cross-sectional area of the antrum to represent the changes in stomach volume after the administration of an experimental diet and to observe the rate of gastric emptying during delivery after the labor analgesia. As a prospective observational study, the patients included in the study were grouped by the random envelope method, but the subjective will of the patients was the main factor in the choice of labor analgesia. Therefore, ITT analysis and PP analysis were conducted for the included women. We found that there was no statistically significant difference between the effects of epidural analgesia and labor analgesia with pharmacological and non-pharmacological interventions on maternal gastric emptying. ITT analysis suggested that epidural analgesia could reduce the use of opioids, and PP analysis suggested that epidural analgesia had a better analgesia effect 30 minutes after the end of the third stage of labor. In the ITT analysis, the Apgar score at 5 minutes postpartum had a significant difference, but with no clinical significance. In addition, PP analysis showed no significant differences in Apgar scores at 5 minutes postpartum between the two groups.
Antrum ultrasonography can measure gastric volume changes by measuring the CSA of the antrum, and previous studies have shown a favourable association.15 Gastric volume and antral CSA correlated best in the right lateral decubitus position (RLDP) compared to the semi-decubitus position.16 In this investigation, semi-decubitus antrum ultrasonography was utilized to improve coordination, however we were unable to determine gastric volume in 3 grades.17 This study assessed the stomach antrum CSA after the experimental diet and its fluctuations in the subsequent two hours. For these followed reasons, this study did not measure the CSA of the gastric antrum when the patients were admitted to the hospital for delivery, nor did it collect the time and contents of the last feeding. First, this study included only primiparas without emergent or difficult labor. Second, the first labor was protracted, and the puerpera fasted after admission and were only given the experimental diet when the condition was satisfied. Third, concomitant disorders that could impede stomach emptying were excluded from this investigation. To exclude preoperative stomach motility abnormalities, future research should still evaluate the baseline gastric antrum CSA. The CSA of the antrum and its alterations following the experimental diet were similar to those in the previous study,14 and there was no statistical difference between the two groups. The antrum CSA was not clearly depicted in most women in the third hour, therefore this study only observed changes in the first 2 hours after administering the experimental food. In this study, the gastric emptying speed was not linear but showed that the emptying speed in the first hour was faster than that in the second hour, which might be related to the size of the stomach capacity.18
This study gives a 70-kcal diet, which is far lower than the needed energy of pregnant women during labor. This experiment diet was given for these reasons: First, previous investigations about stomach emptying have used this experimental diet. Second, there are no guidelines or research on energy supplementation during labor. In addition, the indirect calorimetry (IDC), the “gold standard” for energy usage, and the Harris-Benedict formula, the standard for basal metabolic rate (BMR) evaluation, cannot be used on pregnant women, let alone during childbirth.19 Third, this study focuses on how labor analgesia affects stomach emptying speed, and food type affects stomach emptying more than energy intake. According to earlier studies, this study supplied a carbohydrate-rich diet, because fat and protein may decrease stomach emptying more than carbohydrates. In future studies, to avoid ketosis and augment the mother’s energy intake, labor analgesia’s effect on stomach emptying should be investigated in the experiment diet with increased protein and energy.
It is noteworthy that the results of this study cannot be applied generally. Due to tight inclusion and exclusion criteria, patients with large BMIs and obesity were excluded from the study, along with those who had gestational diabetes and diabetic pregnancy. Actually, those patients were all at high risk of delayed gastric emptying and the emptying speed might be more affected by labor analgesia.20 Gastric emptying in these high-risk populations should be studied in further research.
There were also the following limitations in this study. First, the quality of ultrasound images was not quantitatively analyzed, despite the fact that the antrum ultrasonography was evaluated by two individuals to limit the likelihood of accidental errors. Second, the changes of antrum CSA were evaluated using ultrasound alone to reflect the variation of the gastric volume instead of the virtual changes of stomach volume, and no other methods were used to confirm the estimated gastric volume changes. Meanwhile, for the accurate gastric volumes cannot be obtained directly, it makes the significance of studying correlations between gastric volumes and the antral CSA limited. Third, there is no assessment of the labor experience and of the subjective attitude of the maternal patients about the given diet during childbirth.
Conclusions
There was no difference between epidural analgesia and pharmacological and non-pharmacological interventions of labor analgesia on gastric emptying, and the antrum ultrasonography can be used to monitor the changes in the gastric volume of maternal patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The study protocol has been reviewed and approved by the Ethics Committee of Medical Center Hospital of Qionglai [No. (2022) 42, 2022/08/16] and conducted in compliance with the Declaration of Helsinki.
Informed Consent Statement
All patients provided informed consent for participation.
Disclosure
The authors confirm that the PI for this paper is Qinghai Zuo, who had direct clinical responsibility for patients. The authors declare no competing interests.
References
1. Jay L, Zieleskiewicz L, Desgranges FP, et al. Determination of a cut-off value of antral area measured in the supine position for the fast diagnosis of an empty stomach in the parturient: a prospective cohort study. Eur J Anaesthesiol. 2017;34(3):150–157. doi:10.1097/EJA.0000000000000488
2. Mendelson CL. The aspiration of stomach contents into the lungs during obstetric anesthesia. Am J Obstet Gynecol. 1946;52:191–205. doi:10.1016/S0002-9378(16)39829-5
3. Lienhart A, Auroy Y, Péquignot F, et al. Survey of anesthesia-related mortality in France. Anesthesiology. 2006;105(6):1087–1097. doi:10.1097/00000542-200612000-00008
4. Practice Guidelines for Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration: application to Healthy Patients Undergoing Elective Procedures. An updated report by the American Society of Anesthesiologists Task Force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology. 2017;126(3):376–393. doi:10.1097/ALN.0000000000001452
5. Vanner RG, Goodman NW. Gastro-oesophageal reflux in pregnancy at term and after delivery. Anaesthesia. 1989;44(10):808–811. doi:10.1111/j.1365-2044.1989.tb09096.x
6. Kinsella SM, Winton AL, Mushambi MC, et al. Failed tracheal intubation during obstetric general anaesthesia: a literature review. Int J Obstet Anesth. 2015;24(4):356–374. doi:10.1016/j.ijoa.2015.06.008
7. Wright PM, Allen RW, Moore J, Donnelly JP. Gastric emptying during lumbar extradural analgesia in labour: effect of fentanyl supplementation. Br J Anaesth. 1992;68(3):248–251. doi:10.1093/bja/68.3.248
8. Singata M, Tranmer J, Gyte GM. Restricting oral fluid and food intake during labour. Cochrane Database Syst Rev. 2013;2013(8):CD003930. doi:10.1002/14651858.CD003930.pub3
9. Bouvet L, Mazoit JX, Chassard D, Allaouchiche B, Boselli E, Benhamou D. Clinical assessment of the ultrasonographic measurement of antral area for estimating preoperative gastric content and volume. Anesthesiology. 2011;114(5):1086–1092. doi:10.1097/ALN.0b013e31820dee48
10. Kruisselbrink R, Arzola C, Endersby R, Tse C, Chan V, Perlas A. Intra- and interrater reliability of ultrasound assessment of gastric volume. Anesthesiology. 2014;121(1):46–51. doi:10.1097/ALN.0000000000000193
11. Arzola C, Cubillos J, Perlas A, Downey K, Carvalho JCA. Interrater reliability of qualitative ultrasound assessment of gastric content in the third trimester of pregnancy. Br J Anaesth. 2014;113(6):1018–1023. doi:10.1093/bja/aeu257
12. Cho EA, Huh J, Lee SH, et al. Gastric ultrasound assessing gastric emptying of preoperative carbohydrate drinks: a randomized controlled noninferiority study. Anesth Analg. 2021;133(3):690–697. doi:10.1213/ANE.0000000000005411
13. Checketts MR, Alladi R, Ferguson K, et al. Recommendations for standards of monitoring during anaesthesia and recovery 2015: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia. 2016;71(1):85–93. doi:10.1111/anae.13316
14. Bouvet L, Schulz T, Piana F, Desgranges FP, Chassard D. Pregnancy and labor epidural effects on gastric emptying: a prospective comparative study. Anesthesiology. 2022;136(4):542–550. doi:10.1097/ALN.0000000000004133
15. Van de Putte P, Perlas A. Ultrasound assessment of gastric content and volume. Br J Anaesth. 2014;113(1):12–22. doi:10.1093/bja/aeu151
16. Darwiche G, Almér LO, Björgell O, Cederholm C, Nilsson P. Measurement of gastric emptying by standardized real-time ultrasonography in healthy subjects and diabetic patients. J Ultrasound Med. 1999;18(10):673–682. doi:10.7863/jum.1999.18.10.673
17. Perlas A, Davis L, Khan M, Mitsakakis N, Chan VW. Gastric sonography in the fasted surgical patient: a prospective descriptive study. Anesth Analg. 2011;113(1):93–97. doi:10.1213/ANE.0b013e31821b98c0
18. Szarka LA, Camilleri M. Gastric emptying. Clin Gastroenterol Hepatol. 2009;7(8):823–827. doi:10.1016/j.cgh.2009.04.011
19. Yatabe T. Strategies for optimal calorie administration in critically ill patients. J Intensive Care. 2019;7:15. doi:10.1186/s40560-019-0371-7
20. Sabry R, Hasanin A, Refaat S, Abdel Raouf S, Abdallah AS, Helmy N. Evaluation of gastric residual volume in fasting diabetic patients using gastric ultrasound. Acta Anaesthesiol Scand. 2019;63(5):615–619. doi:10.1111/aas.13315
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.