Back to Journals » Journal of Pain Research » Volume 18
Gabapentinoids-Induced Rhabdomyolysis/Myopathy: Clinical Characteristics, Management, Outcomes, and Critical Safety Alerts
Received 17 June 2025
Accepted for publication 26 November 2025
Published 4 December 2025 Volume 2025:18 Pages 6491—6503
DOI https://doi.org/10.2147/JPR.S547736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Miao Liu,1 Minghui Long,1 Xingchen Zhou2
1Department of Pharmacy, Hunan Cancer Hospital/The Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, Changsha, Hunan, People’s Republic of China; 2Department of Pharmacy, XiangYa Hospital, Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Xingchen Zhou, Department of Pharmacy, XiangYa Hospital, Central South University, No. 87 XiangYa Road, Changsha, Hunan, 410008, People’s Republic of China, Email [email protected] Minghui Long, Hunan Cancer Hospital/The Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, Changsha, Hunan, 410011, People’s Republic of China, Email [email protected]
Background: Gabapentinoids, increasingly prescribed for neuropathic pain, demonstrate undercharacterized muscular toxicity risks despite perceived safety advantages over opioids, this includes the potential to induce rhabdomyolysis—a critical condition characterized by rapid release of intracellular contents into the systemic circulation due to muscle cell injury, ultimately leading to systemic complications.
Methods: A systematic global review (inception-2024) identified 19 gabapentinoid-induced rhabdomyolysis cases across 15 databases, analyzed via standardized protocols for clinical patterns, management, and outcomes.
Results: Cases (median age 63; 52.6% male) manifested rapid symptom onset (≤ 7 days in 52.9%), severe creatine phosphokinase(CPK) elevation (median 3,095 U/L), and renal impairment (78.9%). All patients discontinued gabapentinoids, with 57.9% receiving hydration/alkalinization and 31.6% requiring dialysis. Biochemical resolution occurred in 78.9% (median 14 days), though one mortality resulted from comorbid complications. Naranjo assessments confirmed probable causality in 84.2% of cases. Of note, a significant majority of patients (89.5%) presented with multiple comorbidities (such as hypertension, diabetes, and hyperlipidemia) and received polypharmacy. Particularly when co-administered with statins (as observed in 7 cases where symptom onset occurred following combination therapy), drug-drug interactions may lead to accumulation of medicinal products, thereby significantly increasing the risk of rhabdomyolysis.
Conclusion: This study provides the first evidence-based framework for gabapentinoid myotoxicity monitoring, emphasizing renal function-guided dosing, early CPK surveillance, and drug interaction vigilance. Clinicians should consider gabapentinoid cessation in unexplained myalgia with CK > 3×ULN, particularly in high-risk populations.
Keywords: gabapentin, rhabdomyolysis/myopathy, characteristics, treatments, abuse
Introduction
Rhabdomyolysis is a clinical syndrome characterized by rapid disintegration of skeletal muscle, resulting in the release of intracellular contents into the systemic circulation. It can be triggered by diverse etiologies including trauma, ischemia, medications, toxins, metabolic disorders, and infections, all of which compromise the integrity and stability of the sarcolemma. The ensuing massive release of muscle-derived components such as myoglobin, creatine kinase, and electrolytes can lead to tissue injury and multi-organ dysfunction. Systemic manifestations range from asymptomatic elevation of muscle enzymes to life-threatening complications, with acute kidney injury and severe electrolyte imbalances representing the most critical outcomes. Central to its pathogenesis are the nephrotoxic and cytotoxic effects of myoglobin and its metabolic derivatives.1,2 Non-traumatic cases predominantly arise from drug toxicity (80% adult prevalence) through mitochondrial ATP disruption (statins via HMG-CoA inhibition);3 calcium dysregulation (anesthetic-induced hyperthermia); or direct sarcolemmal injury (alcohol metabolites).4,5 Although statins/antipsychotics/immunosuppressants are still recognized as high-risk drugs, sporadic cases of rhabdomyolysis have also been reported with the emerging neuromodulator gabapentinoids.4,6 Although the precise mechanisms of gabapentinoid-induced myotoxicity remain to be fully elucidated, proposed pathways include disruption of calcium homeostasis, synergistic interactions with other medications, such as statins, which may collectively precipitate muscle injury.7,8
Despite the widespread use of gabapentinoids (gabapentin/pregabalin) as α2-δ voltage-gated calcium channel ligands for treating neuropathic pain, restless legs syndrome, and epilepsy via presynaptic inhibition of excitatory neurotransmitters (glutamate/substance P),9 their potential for muscular toxicity remains inadequately characterized. Current evidence remains limited to sporadic case reports with knowledge gaps in risk factor stratification and prognostic modeling. This systematic global analysis synthesizes gabapentin-induced myotoxicity profiles, therapeutic approaches, pharmacological interactions, and prognostic patterns, providing actionable insights for rhabdomyolysis recognition, management, and prevention.
Materials and Methods
Study Design and Literature Search Strategy
This systematic review aimed to investigate the clinical characteristics, management, and outcomes of gabapentinoid-induced rhabdomyolysis by analyzing published case reports. A systematic literature search was conducted across PubMed/Medline, Web of Science, Ovid, Embase, Cochrane Library, Elsevier, SpringerLink, and major Chinese databases (CNKI/Wanfang/VIP) using search terms: gabapentin, gabapentinoids, pregabalin, rhabdomyolysis, myopathy, myositis, spanning inception-December 2024 without language restrictions. Exclusion criteria were: non-clinical studies (mechanistic/animal/reviews), secondary literature (editorials/commentaries), duplicate publications, and unavailable full-text articles.
Data Analyse
A structured data collection instrument was developed and implemented to systematically capture patient demographics (sex, age), clinical characteristics (comorbidities, concomitant medications), therapeutic regimens, and clinical outcomes throughout the study protocol.
Result
Patient
Following systematic screening, nineteen case reports met inclusion criteria in Table 1.7,8,10–24 No other types of studies, such as randomized clinical trials, cohort studies, or case series, related to our research question were identified through the systematic search. Among the 19 myopathy patients (10 males, 9 females) in this study (Table 2), the medication profiles revealed: Gabapentin use in 12 cases and Pregabalin in 7 cases. From a dosage perspective, 75% of gabapentin users and 85.7% of pregabalin users did not exceed the maximum recommended daily dose as stated in the prescribing information for each drug, a figure that includes one case each where the exact dosage was unknown. Analysis of dosing patterns revealed that six patients (31.6%) developed symptoms acutely, nine (47.4%) subacutely, and two (10.5%) chronically, whereas the pattern was not documented in the literature for the remaining two cases (10.5%). The cohort demonstrated a broad age range with a median age of 63 years. Indications for use primarily aligned with approved labeling: restless legs syndrome (3/19, 15.8%), pain management (13/19, 68.4%), and uremia-associated pruritus (1/19, 5.3%), though off-label high-dose use/misuse was also documented (2/19, 10.5%). Seventeen patients presented with comorbidities, including hypertension (9/17, 52.9%), nephrotic syndrome (6/17, 35.3%), psychiatric disorders (anxiety/depression/schizophrenia) (6/17, 35.3%), diabetes mellitus (6/17, 35.3%), and hyperlipidemia (5/17, 29.4%), necessitating concurrent pharmacotherapy. The median latency period for symptom onset was 3 days (range 1–52 days), with temporal distribution as follows: 5 cases (29.4%) occurred within 2 days, 4 cases (23.5%) between 3 and 7 days, 1 case (5.9%) during 8 and 14 days, and 7 cases (41.2%) manifesting after two weeks. Naranjo scale assessment categorized 16 cases (84.2%) as probable adverse drug reactions (with documented scores ranging from 5 to 8 where available) and 3 cases (15.8%) as possible (scores ranging from 1 to 4 where available).
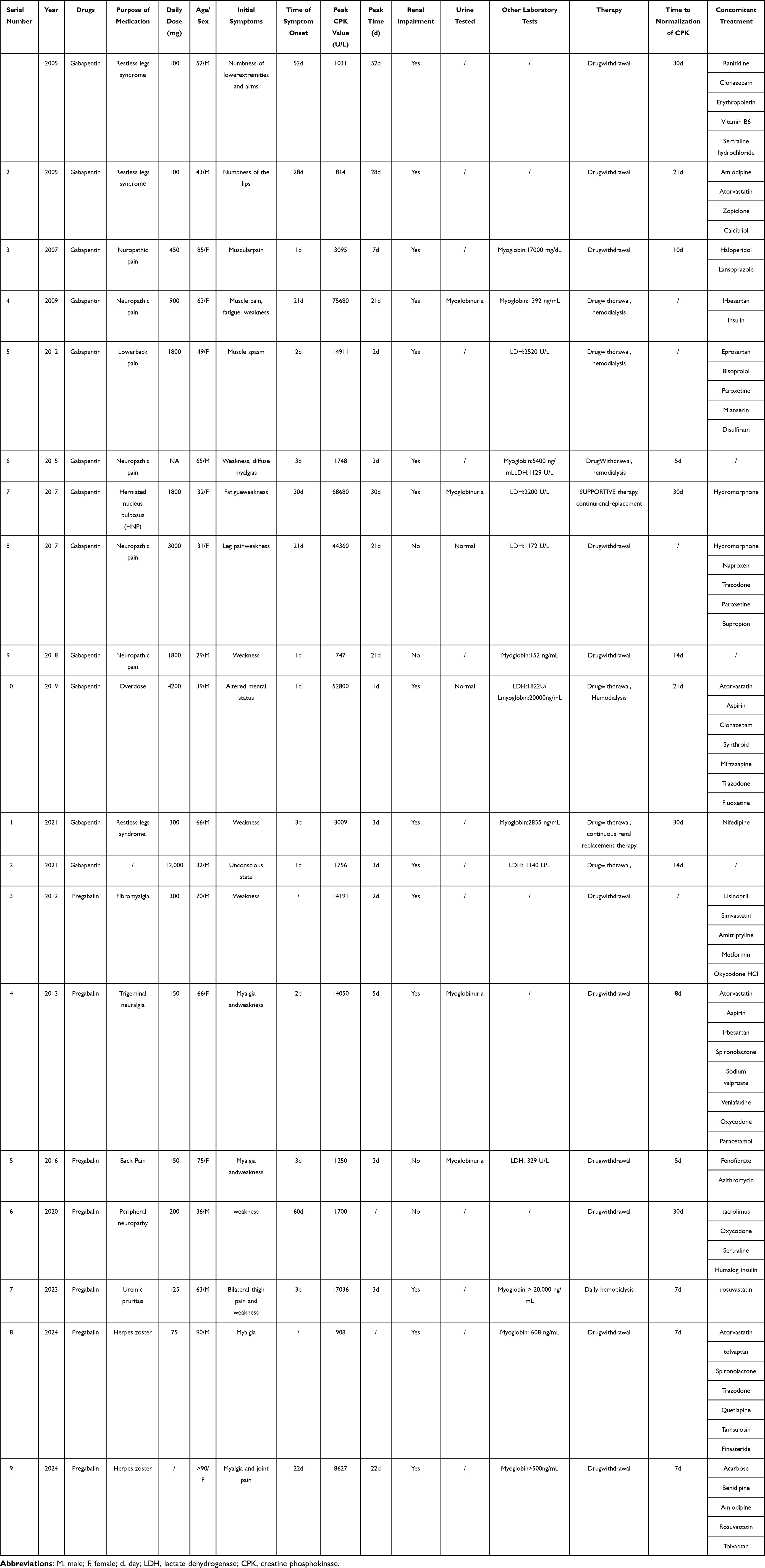 |
Table 1 Gabapentinoids Related Rhabdomyolysis/Myopathy-Summary of Case Reports |
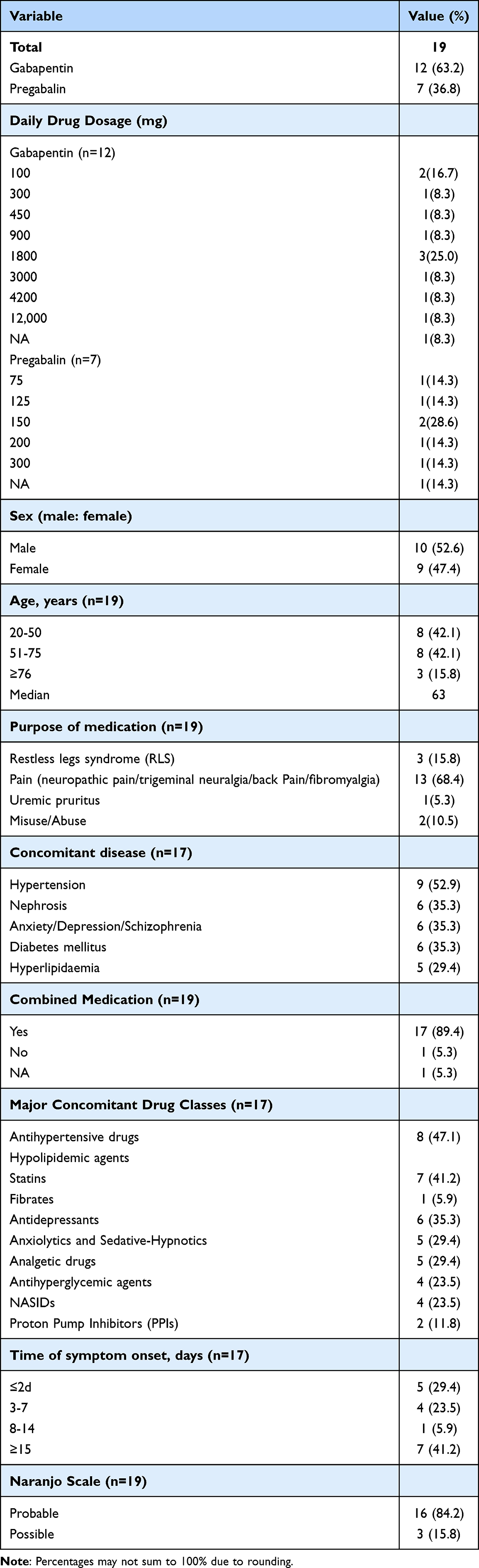 |
Table 2 Characteristics of 19 Patients with Rhabdomyolysis Induced by Gabapentinoids |
Clinical Characteristics and Treatments
Among the 19 included cases, all patients manifested clinical symptoms (Table 3). The most prevalent myopathic manifestations were weakness/numbness (13/19, 68.4%) and myalgia (9/19, 47.4%). Additional presentations included fatigue (2/19, 10.5%), muscle spasms (1/19, 5.3%), unconsciousness (1/19, 5.3%), and altered mental status (1/19, 5.3%). All 19 patients demonstrated elevated creatine CPK levels, with median values of 3,095 U/L (range 747–75,680). Serum myoglobin was quantified in 9 patients (median 2,855 ng/mL). Elevated lactate dehydrogenase (LDH) was observed in 7 cases, reaching a median concentration of 1,172 U/L (329–2,520). Literature-based analysis indicated renal impairment (either new-onset or exacerbation of pre-existing conditions) in 15 patients, with potential confounding factors in RLS-treated cases requiring consideration. Notably, myoglobinuria was documented in 4 patients.
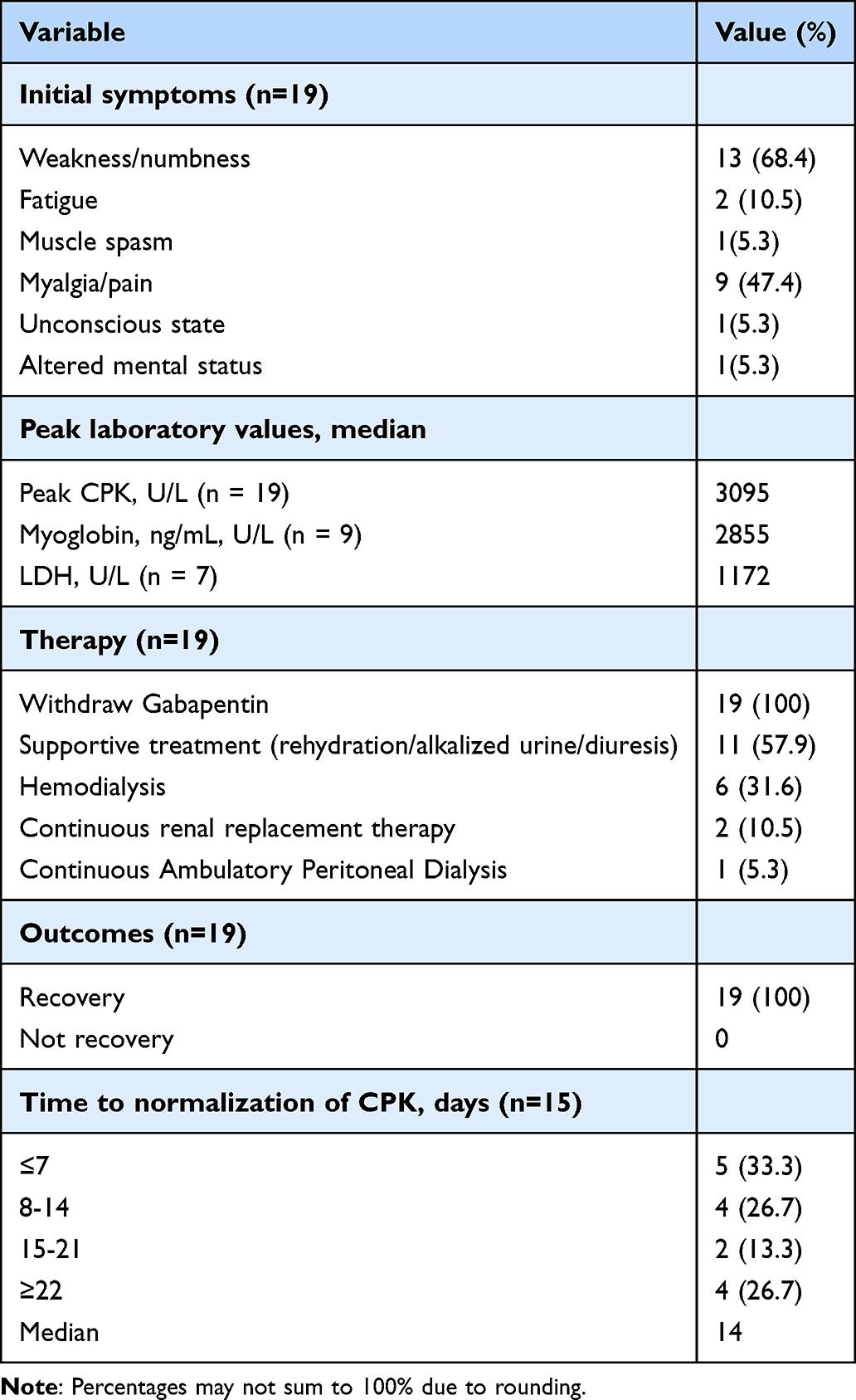 |
Table 3 Clinical Characteristics of Rhabdomyolysis/Myopathy Caused by Gabapentinoids |
Literature-documented therapeutic interventions demonstrated immediate discontinuation of suspected causative agents in all 19 myopathy cases, with 11 patients (11/19, 57.9%) receiving explicitly documented supportive care including hydration, urine alkalinization, and diuresis, while renal replacement modalities comprised intermittent hemodialysis in 6 patients (6/19, 31.6%), notably, including two preexisting dialysis-requiring cases developing complications post low-dose gabapentin therapy. Supplemented by continuous renal replacement therapy (CRRT) in two patients (2/19, 10.5%) and peritoneal dialysis in one patient (1/19, 5.3%).
Clinical outcomes demonstrated universal symptomatic improvement across the cohort, with creatine phosphokinase (CPK) normalization achieved in 15/19 patients (median 14 days; range 7–21+ days) whereas post-discharge CPK monitoring was unavailable for 4 resolved cases—specifically, biochemical recovery occurred within 7 days in 5 patients (33.3%), 8–14 days in 4 (26.7%), 15–21 days in 2 (13.3%), and exceeded three weeks in the remaining 4 (26.7%). Mortality was exclusively observed in an 83-year-old multimorbid patient who developed acute respiratory failure culminating in death on day 19 despite complete myopathy resolution, with autopsy findings dissociating the terminal event from muscular pathology. Our findings highlight a common challenge in outpatient settings: the documentation of laboratory parameters often begins after symptom appearance. Moving forward, a heightened clinical suspicion that triggers earlier and more frequent CPK testing could yield valuable insights into the early phases of this condition.
Discussion
Our analysis of 19 globally reported cases provides critical insights into the clinical profile of gabapentinoid-induced rhabdomyolysis. The key findings include a rapid median onset of symptoms (3 days), a high prevalence of polypharmacy (89.5%) and comorbidities, and a strong association with concomitant statin use (noted in 7 cases). Despite these risks, prompt drug discontinuation and supportive care led to biochemical resolution in most patients.
These findings both align with and refine the existing understanding of drug-induced rhabdomyolysis. The rapid symptom onset observed in our cohort (≤7 days in 52.9% of cases) suggests a direct toxic effect on muscle cells rather than a slow metabolic accumulation. The exceedingly high rate of polypharmacy underscores that gabapentinoid-induced myotoxicity is rarely an isolated event but frequently occurs in a complex pharmacological context, where drug interactions and additive toxicities play a significant role. This is strongly supported by the Naranjo scale assessment, which confirmed a probable causal relationship in 84.2% of cases. The association with statins, a well-known risk factor for myopathy, highlights a potentially synergistic mechanism of muscle injury that clinicians must be vigilant about.
Our analysis robustly identifies three critical risk dimensions that converge to heighten vulnerability to gabapentinoid-induced rhabdomyolysis: pre-existing comorbidities, polypharmacy-driven drug interactions, and advanced age. First, the near-universal presence of comorbidities (89.5%) in our cohort is by no means coincidental. Conditions such as hypertension, diabetes, and chronic kidney disease inherently contribute to microangiopathy, chronic inflammatory states, and elevated baseline oxidative stress, thereby compromising skeletal muscle homeostatic reserve and tolerance. This renders patients’ muscle tissue more vulnerable to potentially myotoxic agents, significantly lowering the threshold for toxicity.25–27 Our findings suggest that gabapentinoids likely act as the “last straw,” triggering muscle injury on a substrate already weakened by underlying comorbidities. Notably, the widespread use of polypharmacy further exacerbates the risk of drug-drug interactions. The observation that as many as seven patients were concurrently using statins is of particular clinical concern. Statins are well-established myotoxic agents due to their inhibition of HMG-CoA reductase and impact on mitochondrial function.28 When co-administered with gabapentinoids, these drugs may exhibit marked synergistic toxicity—potentially through concerted mitochondrial inhibition or additive disruption of myocyte calcium homeostasis—thereby substantially accelerating the onset of rhabdomyolysis. This interaction reflects a broader clinical challenge. Beyond statins, other medications commonly used in this population, such as psychotropic agents (which may affect muscle tone via neurotransmitter systems) and diuretics (which can precipitate dehydration and electrolyte disturbances), may increase the risk of muscle toxicity through distinct mechanisms.5,29–31 Therefore, a comprehensive medication review is essential before prescribing gabapentinoids. For patients already taking other potentially myotoxic drugs, it is advisable to initiate gabapentinoids at a lower dose, apply a more gradual titration scheme, educate patients on monitoring muscular symptoms, and consider baseline and periodic creatine kinase monitoring. Age is another critical risk factor, with a median age of 63 years in this cohort. Advanced age is closely associated with physiological decline in renal function, reduction in muscle mass (sarcopenia), multimorbidity, and polypharmacy.32,33 Elderly patients exhibit altered pharmacokinetics and reduced physiological reserve, rendering them not only more susceptible to drug toxicity but also more likely to present with atypical clinical manifestations that are easily overlooked. Of particular importance, gabapentin is primarily excreted unchanged by the kidneys,34 in the setting of impaired renal function, gabapentinoids are prone to accumulation. Hence, dose adjustment and enhanced therapeutic drug monitoring are recommended for elderly patients and those with chronic kidney disease.
The mechanistic pathway underlying these clinical observations, while not fully elucidated, appears to center on intracellular calcium disruption.4,35 As observed in our cases with rapid symptom progression, calcium homeostasis disruption from channel inhibition causes overload, triggering protease activation (eg, calpains) and phospholipases that degrade contractile proteins and membrane components, ultimately leading to sarcolemmal rupture.36–38 This process may be compounded by mitochondrial dysfunction through respiratory chain interference or oxidative phosphorylation disruption, while calcium imbalance exacerbates mitochondrial damage.39 Additionally, renal-excreted gabapentinoids may accumulate in impaired renal function, potentiating toxicity risks.40,41 The oxidative muscle damage via free radical overproduction or compromised antioxidant defenses represents another plausible pathway that may contribute to the observed clinical manifestations.42 Though mechanistic certainty awaits clarification,16,43 the evidence points to multifactorial pathways.
From a clinical management perspective, our cases demonstrate that rhabdomyolysis can occur regardless of whether renal function is normal or not, requiring rigorous dose titration with serial creatinine kinase and renal function monitoring. The renal-dependent pharmacokinetics of these drugs, characterized by prolonged half-life (132 hours) in renal impairment,15 elevate intoxication risks. However, their low molecular weight (171 Da and 159 Da) and limited protein binding permit effective dialysis,44 which was required in 31.6% of our cases. Management should focus on trigger removal and metabolic correction, utilizing diuretics to enhance toxin clearance. In severe cases, continuous renal replacement therapy (CRRT) or plasma exchange demonstrate efficacy against gabapentinoids-related neurotoxicity.45
Several limitations inherent to this study should be considered when interpreting its findings. Firstly, as a case series constructed from retrospectively reported data, the availability of specific clinical parameters was heterogeneous. Most notably, the exact length of hospital stay and detailed data regarding intensive care unit (ICU) admission were not consistently documented across all cases. This reflects a common challenge in aggregating real-world clinical data where documentation priorities may differ. Nevertheless, the universal outcome of “hospitalization leading to improvement and discharge” was confirmed for all surviving patients, providing clear qualitative evidence of the clinical course.
In conclusion, our analysis establishes that gabapentinoids represent emerging myotoxic agents capable of inducing rhabdomyolysis, particularly in patients with renal impairment, polypharmacy, or genetic susceptibility. While mechanistic certainty awaits clarification,16,43 clinicians should maintain vigilance for gabapentinoids-associated myopathy, particularly in high-risk populations. Future pharmacogenomic studies are imperative to identify genetic susceptibility factors, which could pave the way for personalized prescribing and risk stratification. Future prospective studies should also aim to standardize the collection of healthcare utilization metrics, such as hospital stay duration, to better quantify the burden of this adverse event. Ultimately, as gabapentinoid prescriptions continue to rise, a balanced approach weighing therapeutic benefits against these underappreciated myotoxic risks is crucial for ensuring patient safety.
Conclusion
This systematic analysis establishes gabapentinoids as emerging myotoxic agents capable of inducing rhabdomyolysis, particularly in patients with renal impairment, polypharmacy, or genetic susceptibility. Our synthesis of 19 global cases reveals consistently rapid symptom onset, universal CPK elevation, and frequent renal involvement, with most cases demonstrating probable causality according to the Naranjo assessment. Although immediate drug discontinuation and supportive care often led to biochemical resolution within a few weeks, the high prevalence of comorbidities and complex drug interactions underscores the necessity for rigorous risk stratification. Looking forward, our findings necessitate a paradigm shift in clinical practice. The proposed evidence based monitoring framework emphasizes renal function guided dosing, vigilant CPK surveillance, and heightened awareness of drug interactions, especially with statins. This framework should be integrated into routine care for patients prescribed these medications. However, critical knowledge gaps persist. The precise mechanistic pathways, whether through calcium dysregulation, mitochondrial toxicity, or inflammatory modulation, remain elusive and warrant dedicated in vitro and translational research. Future pharmacogenomic studies are imperative to identify genetic susceptibility factors, which could pave the way for personalized prescribing and risk stratification. Ultimately, as gabapentinoid prescriptions continue to rise, a balanced approach is crucial. Clinicians must weigh their therapeutic benefits against these underappreciated myotoxic risks. Vigilance, prompt intervention upon unexplained biochemical abnormalities, and further mechanistic investigations are essential to mitigate the burden of this serious adverse event and ensure patient safety.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Baeza-Trinidad R. Rhabdomyolysis: a syndrome to be considered. Medicina Clínica. 2022;158:277–283. doi:10.1016/j.medcli.2021.09.025
2. Kodadek L, Ii SPC, Seshadri A, et al. Rhabdomyolysis: an American Association for the Surgery of Trauma critical care committee clinical consensus document. Trauma Surg Acute Care Open. 2022;7:e000836. doi:10.1136/tsaco-2021-000836
3. Singh D, Chander V, Chopra K. Rhabdomyolysis. Methods Find Exp Clin Pharmacol. 2005;27:39–48. doi:10.1358/mf.2005.27.1.875435
4. Cabral BMI, Edding SN, Portocarrero JP, Lerma EV. Rhabdomyolysis. Dis Mon. 2020;66:101015. doi:10.1016/j.disamonth.2020.101015
5. Huerta-Alardin AL, Varon J, Marik PE. Bench-to-bedside review: rhabdomyolysis -- an overview for clinicians. Crit Care. 2005;9:158–169. doi:10.1186/cc2978
6. Xavier Bosch MD, Poch E, Josep MG. Rhabdomyolysis and acute kidney. New Engl J Med. 2009;361:62–72. doi:10.1056/NEJMra0801327
7. Choi MS, Jeon H, Kim HS, et al. A case of gabapentin-induced rhabdomyolysis requiring renal replacement therapy. Hemodial Int. 2017;21:E4–E8. doi:10.1111/hdi.12458
8. Kaufman MB, Choy M. Pregabalin and Simvastatin: first report of a case of rhabdomyolysis. Pharmacy and Therapeutics. 2012;37:579–595.
9. Mathieson S, Lin CC, Underwood M, Eldabe S. Pregabalin and gabapentin for pain. BMJ. 2020;369:m1315. doi:10.1136/bmj.m1315
10. Lipson J, Lavoie S, Zimmerman D. Gabapentin-induced myopathy in 2 patients on short daily hemodialysis. Am J Kidney Dis. 2005;45:e100–4. doi:10.1053/j.ajkd.2005.02.024
11. Tuccori M, Lombardo G, Lapi F, Vannacci A, Blandizzi C, Tacca MD. Gabapentin-induced severe myopathy. Ann Pharmacother. 2007;41:1301–1305. doi:10.1345/aph.1K077
12. Bilgir O, Calan M, Bilgir F, et al. Gabapentin-induced rhabdomyolysis in a patient with diabetic neuropathy. Intern Med. 2009;48:1085–1087. doi:10.2169/internalmedicine.48.1766
13. Juan ET-D, Olague-Diaz P, Royo-Maicas P, Fernandez-Najera E, Garcia-Maset R. Acute renal failure due to gabapentin. A case report and literature. Nefrologia. 2012;32:130–131. doi:10.3265/Nefrologia.pre2011.Nov.11087
14. Falcon FTD, Brunetti C, De Prisco O, et al. Rabdomiolisi da gabapentin: a case report. G Ital Nefrol. 2015;32:1–4.
15. Qiu X, Tackett E, Khitan Z. A case of gabapentin overdose induced rhabdomyolysis requiring renal replacement therapy. Clin Case Rep. 2019;7:1596–1599. doi:10.1002/ccr3.2302
16. Coupal TM, Chang DR, Pennycooke K, Ouellette HA, Munk PL. Radiologic findings in gabapentin-induced myositis. J Radiol Case Rep. 2017;11:30–37. doi:10.3941/jrcr.v11i4.3092
17. Ghosh S, Villan S, Yazeedi WA. Gabapentin-induced myositis in a patient with spinal cord injury - a case report. Qatar Med J. 2020;2020:30. doi:10.5339/qmj.2020.30
18. Latief M, Bhat MI, Wani ML, et al. Gabapentin toxicity and role of dialysis. J Ren Hepat Disord. 2021;6:7–9. doi:10.15586/jrenhep.v6i1.104
19. Dongxue XFW, Jiqiu H. Rhabdomyolysis caused by gabapentin. Adverse Drug React J. 2021;23:328–329.
20. Gunathilake R, Boyce LE, Knight AT. Pregabalin‐associated rhabdomyolysis. Med j Aust. 2013;199:624–625. doi:10.5694/mja13.10769
21. Kato K, Iwasaki Y, Onodera K, et al. Pregabalin- and azithromycin-induced rhabdomyolysis with purpura: an unrecognized interaction: a case report. Int. J. Surg. Case Rep. 2016;26:221–223. doi:10.1016/j.ijscr.2016.07.007
22. Zhai W, Liu H, Li J, Xin H. Pregabalin-induced rhabdomyolysis: a case series and literature analysis. J Int Med Res. 2024;52. doi:10.1177/03000605241257776
23. Hegde V, Shekar N, Garrett F, Baz M, Anstead M. Pregabalin-induced myopathy in a double lung transplant recipient. Cureus. 2020. doi:10.7759/cureus.11935
24. Kim DE, Song SH. Pregabalin-induced rhabdomyolysis in hemodialysis patient. Korean J Intern Med. 2024;39:366–367. doi:10.3904/kjim.2023.379
25. Nandy A, Gaïni S. Severe rhabdomyolysis as complication of interaction between atorvastatin and fusidic acid in a patient in lifelong antibiotic prophylaxis: a dangerous combination. Case Rep Med. 2016;1–4. doi:10.1155/2016/4705492
26. Brinton EA, Maki KC, Jacobson TA, Sponseller CA, Cohen JD. Metabolic syndrome is associated with muscle symptoms among statin users. J Clin Lipidol. 2016;10:1022–1029. doi:10.1016/j.jacl.2016.05.003
27. Jeon YK, Shin MJ, Saini SK, et al. Vascular dysfunction as a potential culprit of sarcopenia. Exp Gerontol. 2021;145:111220. doi:10.1016/j.exger.2020.111220
28. Safitri N, Alaina MF, Pitaloka DAE, Abdulah R. A narrative review of statin-induced rhabdomyolysis: molecular mechanism, risk factors, and management. Drug, Healthcare and Patient Safety. 2021;13:211–219. doi:10.2147/DHPS.S333738
29. Deng Z, Wang S, Wu C. Rhabdomyolysis associated with newer-generation anti-seizure medications (ASMs): a real-world retrospective and pharmacovigilance study. Front Pharmacol. 2023;14. doi:10.3389/fphar.2023.1197470
30. Heng G, Soh TH, Kwok C. Rhabdomyolysis associated with mirtazapine and quetiapine therapy: a case report and review of the literature. Cureus. 2024.
31. Hohenegger M. Drug induced rhabdomyolysis. Curr. Opin. Pharmacol. 2012;12:335–339. doi:10.1016/j.coph.2012.04.002
32. Turnheim K. When drug therapy gets old: pharmacokinetics and pharmacodynamics in the elderly. Exp Gerontol. 2003;38:843–853. doi:10.1016/S0531-5565(03)00133-5
33. Zazzara MB, Palmer K, Vetrano DL, Carfì A, Onder G. Adverse drug reactions in older adults: a narrative review of the literature. Eur Geriatric Med. 2021;12:463–473. doi:10.1007/s41999-021-00481-9
34. Miller A, Price G. Gabapentin toxicity in renal failure: the importance of dose adjustment. Pain Med. 2009;10:190–192. doi:10.1111/j.1526-4637.2008.00492.x
35. Catterall WA, Perez-Reyes E, Snutch TP, Striessnig J. International union of pharmacology. XLVIII. nomenclature and structure-function relationships of voltage-gated calcium channels. Pharmacol Rev. 2005;57:411–425. doi:10.1124/pr.57.4.5
36. Guis S, Mattei JP, Cozzone PJ, Bendahan D. Pathophysiology and clinical presentations of rhabdomyolysis. Joint Bone Spine. 2005;72:382–391. doi:10.1016/j.jbspin.2004.04.010
37. Goll DE, Thompson VF, LI H, et al. Calpain system: physiology and pathophysiology. Physiol Rev. 2003;83(3):731–801. doi:10.1152/physrev.00029.2002
38. Mouchlis VD, Dennis EA. Membrane and inhibitor interactions of intracellular phospholipases A2. Adv. Bio. Regul. 2016;61:17–24. doi:10.1016/j.jbior.2015.11.011
39. Wallace DC. Mitochondrial diseases in man and mouse. Science. 1999;283:1482–1488. doi:10.1126/science.283.5407.1482
40. Karaoulanis SE, Syngelakis M, Fokas K. Rhabdomyolysis after lamotrigine overdose: a case report and review of the literature. Ann. Gen. Psychiatry. 2016;15. doi:10.1186/s12991-016-0093-3
41. Calandre EP, Rico-Villademoros F, Slim M. Alpha2delta ligands, gabapentin, pregabalin and mirogabalin: a review of their clinical pharmacology and therapeutic use. Expert Rev Neurother. 2016;16:1263–1277. doi:10.1080/14737175.2016.1202764
42. Kośmider K, Kamieniak M, Czuczwar SJ, Miziak B. Second generation of antiepileptic drugs and oxidative stress. Int J Mol Sci. 2023;24:3873. doi:10.3390/ijms24043873
43. Kukkar A, Bali A, Singh N, Jaggi AS. Implications and mechanism of action of gabapentin in neuropathic pain. Arch Pharm Res. 2013;36:237–251. doi:10.1007/s12272-013-0057-y
44. H AEJ, Farber HW, Farber HW. Gabapentin toxicity requiring intubation in a patient receiving long-term hemodialysis. Ann Intern Med. 2002;137:74. doi:10.7326/0003-4819-137-1-200207020-00029
45. Desai A, Kherallah Y, Szabo C, Marawar R. Gabapentin or pregabalin induced myoclonus: a case series and literature review. J Clin Neurosci. 2019;61:225–234. doi:10.1016/j.jocn.2018.09.019
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.