Back to Journals » International Journal of Women's Health » Volume 18
Future Adaptations of Psychosocial Program for Indonesian Pregnant Adolescents: A Research Synthesis
Authors Ermiati E ![]() , Widiasih R
, Widiasih R ![]() , Aini FHQ, Srimurni NA
, Aini FHQ, Srimurni NA
Received 12 November 2025
Accepted for publication 2 April 2026
Published 15 April 2026 Volume 2026:18 580919
DOI https://doi.org/10.2147/IJWH.S580919
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Ermiati Ermiati,1 Restuning Widiasih,1 Farah Huwaida Qurrota Aini,2 Nita Ayu Srimurni2
1Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Ermiati Ermiati, Department of Maternity, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Bandung-Sumedang KM 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +628122109363, Fax +6222-7795596, Email [email protected]
Abstract: Adolescent pregnancy is a persistent global challenge, often accompanied by elevated risks of depression, anxiety, and social isolation. Despite growing international attention, evidence-based psychosocial interventions targeting pregnant adolescents remain limited, particularly in low- and middle-income countries such as Indonesia. This systematic review aimed to synthesize evidence on psychosocial and mental-health interventions for pregnant adolescents aged 10– 19 years and considers implications for Indonesian policy and practice. This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. Searches of PubMed and Scopus covered 2015– 2025. Eight eligible studies were identified. Results indicate that psychosocial interventions, such as mHealth programs, task-sharing models, and human-centered designs, effectively improve adolescent maternal mental health, reducing distress and enhancing bonding. Studies highlight the need for scalable interventions embedded in primary care, especially in resource-limited settings like Indonesia. This review underscores the importance of culturally relevant, integrated care models. It is crucial to engage families and use hybrid delivery models for sustained engagement. Programs combining digital tools with in-person care showed high acceptability but modest behavioral changes. Future research should focus on long-term effectiveness and impact of collaborative care models to enhance outcomes for adolescent mothers.
Keywords: adolescent pregnancy, Indonesia, mental health, psychosocial programs, psychosocial intervention
Introduction
Adolescent pregnancy remains a significant global public health concern, particularly in low- and middle-income countries (LMICs). Adolescence is transitional developmental stage characterized by identity formation, evolving autonomy, and educational engagement.1,2 International estimates indicate that each year approximately 21 million adolescent girls aged 15–19 become pregnant in developing regions, resulting in around 12 million live births, plus at least 0.8 to 2 million births occur among girls younger than 15.3–5 Global projections further suggest that about 13% of adolescent girls will become mothers before turning 18, underscoring the disproportionate burden borne by resource-constraited settings.6 In LMICs including Indonesia, adolescent pregnancy is driven less by individual “choices” and more by poverty, low education, early marriage, restrictive gender norms, and poor access to accurate sexuality education and youth-friendly contraception.7–12 Pregnancy during this period may intensify psychological distress and reduce access to supportive networks. Untreated perinatal mental health problems can adversely affect maternal wellbeing, mother-infant bonding, and child development outcomes. Therefore, adolescent pregnancies greatly affect both physical and psychosocial well-being, which may be the burden is getting heavier in LMICs.
Evidences indicate that adolescent pregnancy is associated with significant physical and psychological consequences. Physically, adolescents are at higher risk of anemia, hypertensive disorders, preterm birth, and delivering low birth weight infants, particularly when access to adequate antenatal care is limited.13–15 Psychologically, pregnant adolescents experience higher rates of depression, anxiety, stigma, and social isolation compared with adult mothers.16–18 When early pregnancy is caused by structural disadvantage, these overlapping health risks make inequality worse and make both the mother and the child more vulnerable in the long term.
Adolescent pregnancy is still prevalent in both urban and rural areas in Indonesia.19 To address this issue, Indonesia established service standards and programs to address the physical and psychological problems that arise from early marriage. The Adolescent Care Health Service Program is aimed to address early marriage, unwanted pregnancy, and HIV to improve adolescents’ knowledge and use of health services and guide program design across Indonesia.20 Other programs exist, such as the early marriage and stunting community programs for nutrition counseling and school-based early-marriage risk education for junior and senior high students, but these programs are not integrated. To manage psychological problems, the Indonesian Ministry of Health suggests a strategic approach of implementing screening at three touchpoints: the first trimester of antenatal care, the fifth antenatal care visit in late pregnancy, and 8–28 days after delivery.21 However, in practice, many districts employ short-term instruments like the Edinburgh Postnatal Depression Scale (EPDS). Through these approaches, programs to help the adolescent pregnancy demography as well as prevent future adolescent pregnancies are implemented in Indonesia.
Several reviews have explored psychosocial programs for adolescent parents and perinatal mental health. A review from a study of psychosocial interventions for pregnant adolescents in high-income countries described programs such as home visits, counseling, group programs, school-linked services, and parenting/skills training produced small-moderate improvements in positive mental health and moderate improvements in school attendance.22 However, most present global findings in aggregates and do not examine how programs fit within specific national systems. As a result, while international evidence identifies promising strategies, clearer guidance is still needed on how these can be realistically adapted to the policies and service contexts of LMICs, including Indonesia. It is expected that international evidence offers several programs models relevant to LMIC contexts. This study aims to synthesize evidence on psychosocial and mental-health programs for pregnant adolescents and young mothers, considers implications for Indonesian policy and practice.
Materials and Methods
Study Design
This study employed a research synthesis using a scoping review approach. A scoping review was selected to allow a broad and flexible exploration of the available literature, accommodating diverse study designs, methodologies, and types of evidence relevant to the research question.23 This approach is particularly appropriate when the objective is to identify key concepts, gaps in research, and types of evidence across a broad topic area. Consistent with this rationale, the present design acknowledges that psychosocial wellbeing cannot be understood solely through statistical measures, but also requires interpretative consideration of lived experiences, program feasibility, and cultural relevance across diverse contexts.
Search Strategy
This scoping review was guided by the Population–Concept–Context (PCC) framework to ensure alignment with the study objective of synthesizing evidence on psychosocial and mental-health programs for pregnant adolescents and deriving implications for Indonesian policy and practice. The Population (P) comprised pregnant adolescents (10–19 years). Studies including broader age ranges (eg, up to 24 years) were considered if pregnant adolescents formed part of the target population or if interventions were explicitly designed for adolescent and young mothers in transitional age groups; the Concept (C) referred to psychosocial and mental-health programs, including preventive, promotive, and supportive interventions; and the Context (C) encompassed community, primary care, school-based, and digital settings across diverse countries and health systems. Based on this framework, the research question was formulated as: What psychosocial and mental-health programs have been implemented for pregnant adolescents, and what components and delivery approaches may inform future adaptations in the Indonesian context?
We conducted a comprehensive search in PubMed and Scopus to identify relevant peer-reviewed studies, using combined keywords and Boolean operators to capture variations in focus and terminology; the main search string was:
(“adolescent pregnancy” OR “pregnant adolescents” OR “teen mothers” OR “young mothers”) AND (“psychosocial intervention” OR “mental health program” OR “psychological support” OR “mHealth” OR “peer support” OR “community-based program”) AND (“maternal wellbeing” OR “perinatal depression” OR “anxiety” OR “mental health”)
Truncation and phrase searching were applied to increase sensitivity (eg, “interven-*” to retrieve intervention, interventions, and intervention-based). Searches were limited to articles published in English between 2015 and 2025. Additionally, reference lists of included articles were manually screened to identify further relevant studies.
Eligibility Criteria
Eligibility criteria were determined a priori based on the PCC framework. Studies were included if they: (1) involved pregnant adolescents or adolescent mothers as the primary population; (2) evaluated or described psychosocial or mental-health programs aimed at improving maternal wellbeing, preventing or managing perinatal depression or anxiety, or enhancing psychosocial functioning; and (3) were conducted in any country or care setting, including community-based, clinical, school-based, or digital environments. Empirical studies employing quantitative, qualitative, or mixed-methods designs were eligible to ensure comprehensive mapping of program models and implementation approaches. Studies including participants up to 24 years of age were included when pregnant adolescents were represented within the sample or when interventions were commonly delivered to adolescent and young mothers as a combined programmatic group. Findings were interpreted with attention to developmental differences across age ranges.
Studies were excluded if they: (1) focused exclusively on adult pregnant women without separate analysis of adolescents; (2) examined solely pharmacological or biomedical interventions without a psychosocial component; (3) did not report program-related outcomes or descriptions; or (4) were editorials, commentaries, conference abstracts, dissertations, or review articles. This approach ensured that the synthesis captured diverse intervention models while maintaining relevance to future program adaptation within the Indonesian context.
Study Selection Process
All records were exported to Mendeley Reference Manager for organization and de-duplication. Screening was conducted in two sequential phases: title-abstract screening followed by full-text review. Two authors independently assessed each record for eligibility at both stages. Discrepancies were resolved through discussion, and when consensus was not immediately achieved, the remaining authors were consulted to reach a final decision. In line with the collaborative nature of the review, all four authors contributed to the final confirmation of included studies. The study selection process was documented using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram, detailing the numbers of records identified, screened, excluded, and included, thereby providing a transparent audit trail of the process.
Data Extraction
A standardized data extraction sheet was developed to systematically record information from each included study. Extracted data included author and year of publication, country of study, study design, target age group, intervention type, delivery mode, and key findings. The “intervention type” variable captured the overarching classification of the program (eg, home-visiting intervention, psychosocial group-based program, mHealth intervention, clinical mental health treatment), while “delivery mode” referred to the mechanism through which the intervention was implemented (eg, face-to-face sessions, home visits, SMS messaging, group classes, primary care integration). The “key findings” column summarized the primary and secondary outcomes relevant to antenatal care attendance and psychosocial determinants. This structured extraction framework enabled consistent comparison across heterogeneous intervention models and facilitated thematic synthesis of intervention characteristics and outcomes.
Data Synthesis and Analysis
Data were synthesized using a narrative approach due to the variation in study designs, intervention types, and outcome measures. The included programs were compared descriptively to identify their main strengths and weaknesses, particularly in relation to effectiveness, feasibility, and psychosocial impact. The findings were then interpreted in light of the Indonesian context, considering health system structure, sociocultural factors, and resource availability. Based on this comparison, potential contextual adaptations and possible implementation challenges were identified to inform future program development for pregnant adolescents in Indonesia.
Results
In this study, total of 465 records was initially identified from two databases, namely Scopus (n = 249) and PubMed (n = 216). After the removal of records prior to screening, 88 records flagged as ineligible by automation tools (Tier 2015–2025), 9 excluded for other predefined reasons (Tier Q1–Q4), and 2 without available abstracts, 150 records remained for title and abstract screening. No duplicate records were identified. Of these, 139 records were excluded for not meeting the inclusion criteria. The full texts of 11 articles were then sought for further assessment; however, 3 could not be retrieved. Eight articles underwent full-text eligibility assessment, and 2 were subsequently excluded because they were review articles. In total, 6 studies fulfilled all inclusion criteria and were included in the final review. The selection process is illustrated in Figure 1.
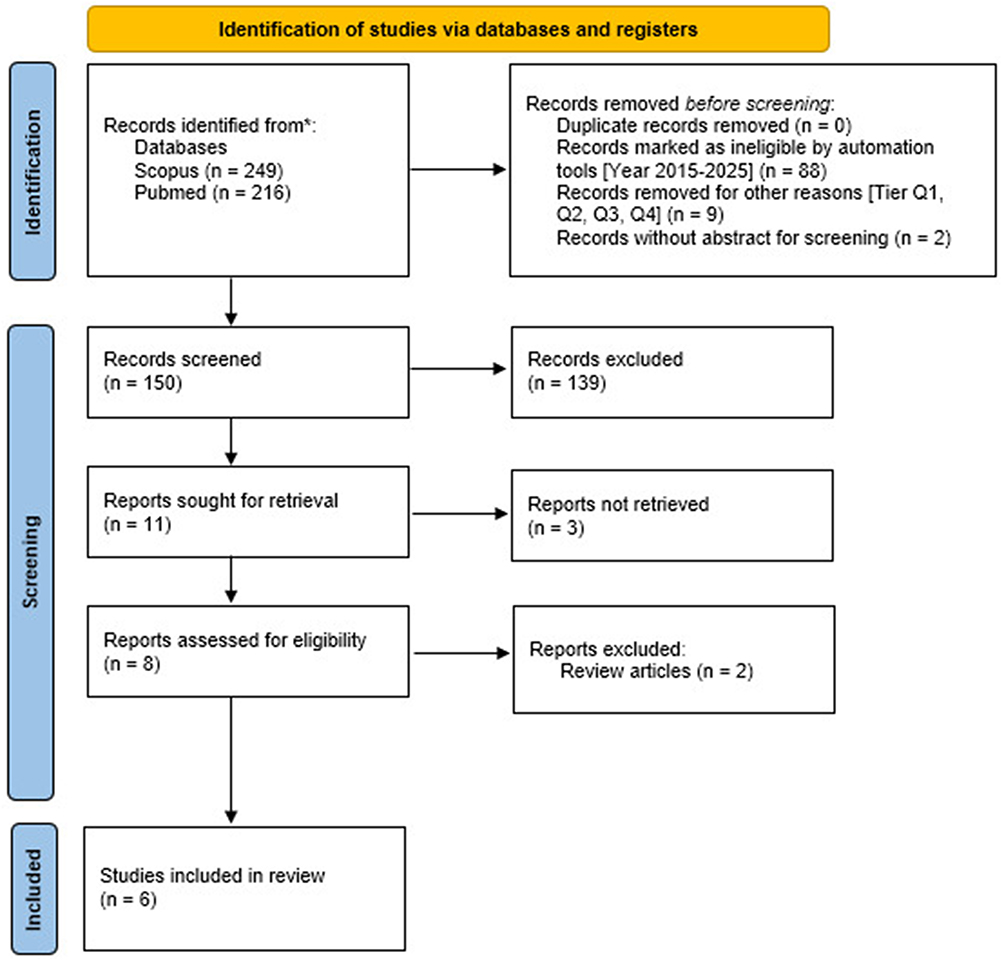 |
Figure 1 PRISMA 2020 flow diagram illustrating the identification, screening, and inclusion process of studies in the scoping review. |
This scoping review included six empirical studies that examined diverse psychosocial and mental health programs targeting pregnant adolescents and young women. Overall, the interventions addressed perinatal depression, psychological distress, social support, parenting preparation, and antenatal care engagement through a range of delivery approaches. The study designs comprised a descriptive program non-empirical (n = 1); intervention protocols, including a mixed-methods protocol integrating qualitative exploration, Nominal Group Technique, and a planned RCT, as well as a cluster randomized controlled trial protocol (n = 2); a qualitative human-centered design study for intervention development (n = 1); a sequential mixed-methods study combining medical file audit, pre–post surveys, and brief interviews (n = 1); and a pilot two-arm randomized controlled trial with a pre–post design (n = 1). Table 1 summarizes the key characteristics and main findings of the included studies.
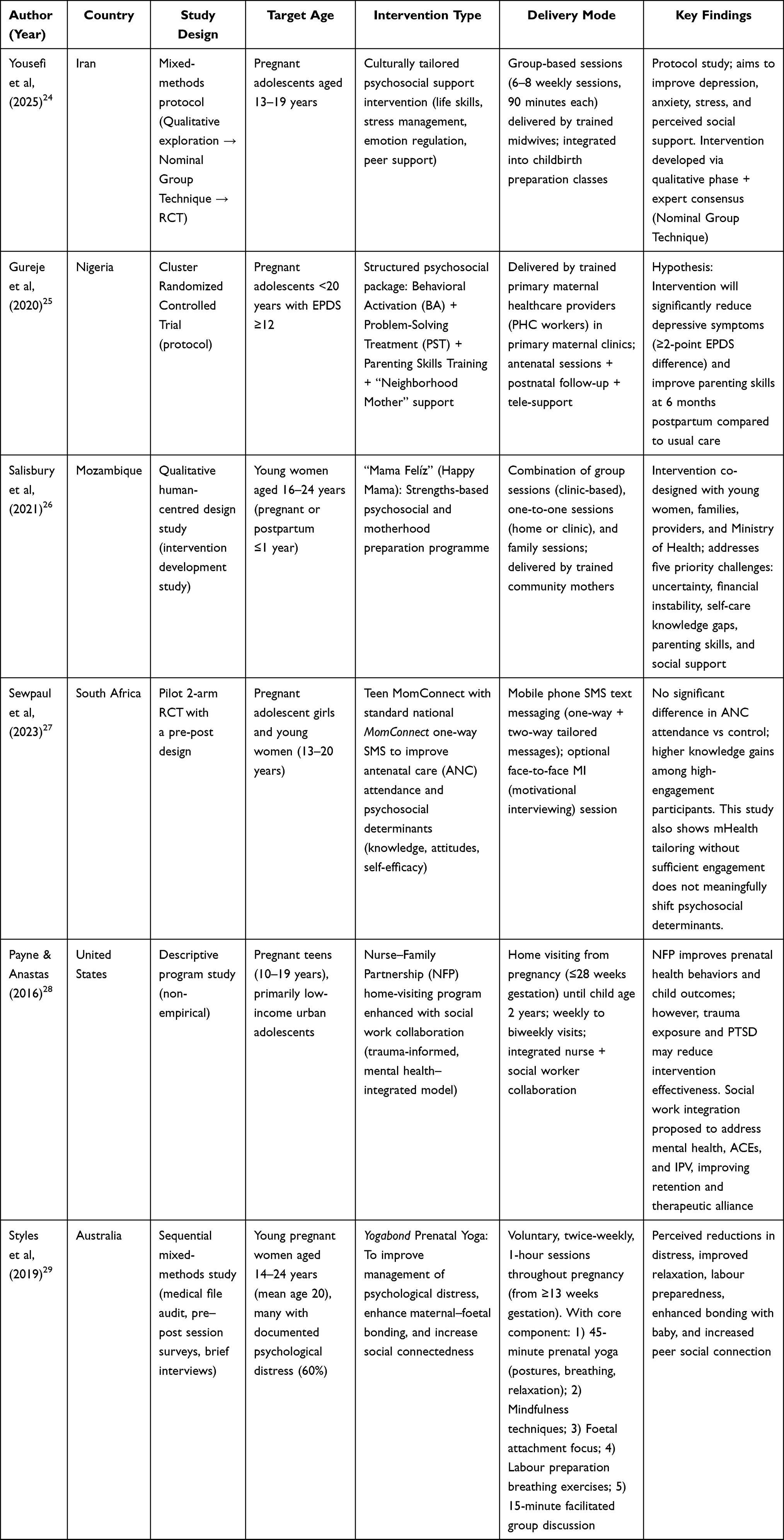 |
Table 1 Summary of Articles |
Description of Included Studies
The studies included a variety of developing countries such as Iran,24 Nigeria,25 Mozambique,26 and South Africa,27 and developed countries such as United States28 and Australia.29 Due to the heterogeneity in program approaches, follow-up durations, and outcome measures, the studies included are categorized based on their program. The categories are comprised of types of approach, intensity levels of intervention, and their psychosocial focus.
Type of Approach
Based on the data synthesis, five primary types of approach emerged: home-based, group-based, digital-based, and Primary Health Center (PHC)-integrated. A study discussing home-based approach centered their programs on the Nurse–Family Partnership (NFP) model, beginning during pregnancy and continuing until the child is 2 years old.28 This approach is primarily one-to-one between a visiting nurse and the mother, and ultimately reduces the burden on vulnerable pregnant adolescents who face poverty, trauma, unstable support, and barriers to health service engagement. Besides the home-based approach with mainly individual components, group-based approaches were discussed in three studies.24,26,29 The group approach is implemented through class sessions, both for educational and counseling purposes24,26 as well as for physical exercise sessions.29 Although group-based interventions may help with normalizing experiences and reduce isolation through shared participations, there may also be discomfort in discussing sensitive issues in mixed or adult-dominated settings, as well as disadvantages in participation due to practical barriers such as scheduling and transport.
A study by Gureje et al implemented another approach by integrating their intervention package with primary maternal care clinics25 This primary health center (PHC)-integrated approach is delivered along with maternal services that are already part of routine service delivery. Through this approach, the study was able to combine psychological treatment, parenting support, and community support in one package, as well as ensuring real-world scalability. However, it relies greatly on provider training, fidelity, workload, and the quality of implementation within PHC systems. Lastly, the digital-based approach in the study by Sewpaul et al differs from the others Rather than relying on repeated face-to-face contact, it delivers support, information, and encourage healthy behavior remotely and asynchronously through two-way mobile messaging.27 However, this approach does not guarantee high engagement from participants, and digital support may not be enough when barriers are structural, emotional, or interpersonal.
Intensity Levels
The intensity levels of the interventions vary from high to low, based on how much time and effort are needed. Two studies are considered to have high intensity level of interventions, with weekly to fortnightly sessions that start during pregnancy until six weeks up to six months postpartum if needed.25,28 Moderate intensity of intervention was found in two studies, with one article suggesting flexibility with psychosocial contact distributed across multiple formats rather than a single repeated modality,26 and the other included eight sessions spanning for gestational weeks 20 to 37.24 The remaining two articles implemented a lower level of intensity, with interventions completed twice a week for one hour for at least eight sessions29 and only receiving text messages with a subset of in-person motivational interviewing sessions.27
Psychosocial Focus
Across the six studies included, five of psychosocial focus were discussed, including knowledge and psychoeducation; coping and self-regulation; mental health symptom reduction; stigma and social marginalization; and bonding and attachment. Knowledge-building is the most universal component across the interventions, with five studies discussing knowledge and psychoeducational focus through different antenatal topics.24–28 Mental health symptom reduction was also another major focus in the studies included, such as reducing adolescent perinatal depression;25 anxiety and stress;24 psychological distress;29 as well as trauma and PTSD.28 Addressing stigma and social marginalization was discussed in four studies, with the majority discussing the negative attitudes and social exclusion associated with adolescent pregnancy.24–26,28 Finally, bonding and attachment was discussed in three studies, which discussed the importance of strengthening mother-child connection through mindfulness exercises and counseling.25,28,29
Discussion
This review synthesized evidence from six diverse psychosocial and mental health interventions targeting pregnant adolescents and young women across varied global contexts. Despite differences in study design, delivery mode, and intervention intensity, the findings collectively highlight the importance of structured psychosocial support in shaping antenatal engagement and mental well-being. At the same time, variations in effectiveness, feasibility, and implementation demands suggest that not all models are equally transferable across settings. The following sections discuss the effectiveness of these intervention approaches and consider their relevance and potential adaptation within the Indonesian context.
Characteristics and Approaches of Psychosocial Programs
Pregnant adolescents face high risks of depression, anxiety, stigma, and poor obstetric outcomes.22 A variety of positive psychosocial outcomes was identified, reflecting the diverse range of studies contributing to the data synthesis. This variation may be attributable to differences in types of approach or the content of the interventions implemented; it may also be explained by differences in the types of positive psychosocial outcomes measured across the six studies that reported this outcome.
Our findings have shown that various types of effective psychosocial programs, such as continuous home-based relational care, classroom-style antenatal sessions, or digital-based support through text messages, can improve the psychosocial and mental health needs of pregnant adolescents.24–29 Home-based approach entails an intervention program built around nurse home visiting, with a sustained relationship between the mother and the nurse.28 This approach reaches mothers in their own environments, making it especially suitable for adolescents with complex psychosocial needs. This is relevant with a previous study that found personalized home visiting programs for adolescent mothers can enhance parenting skills, maternal well-being, and certain child health outcomes.30 In comparison, we found that group-based approach was less likely to be personalized. However, it was also highlighted that interventions carried out in group sessions can normalize experiences and reduce isolation through shared participation.24,26,29 This is in line with previous studies which revealed that group prenatal care provides benefits such as alleviating stigma, enhance self-efficacy, and promote healthier pregnancy behaviors.31 Studies that explore the differences in group-based and home-based intervention approaches to determine their relative effectiveness and feasibility for adolescent pregnant mothers, while also examining how each approach addresses implementation challenges such as logistical barriers, cultural differences, and the need for trained facilitators are needed to cover this literature gap.
A notable finding from this review is that the interventions provided varied in terms of the intensity, reflecting differences in intervention design, delivery setting, and targeted psychosocial outcomes. Interventions range from brief psychosocial sessions lasting a few weeks to more extended programs including multiple components, such as educational, counseling, and physical activity programs over several months. High-intensity approaches provided frequent and continual contact with a healthcare provider from pregnancy until two years postpartum, suggesting that adaptive intervention designs may balance feasibility with clinical responsiveness.25,28 Programs with a moderate intensity relied on scheduled sessions delivered through different modalities, indicating a structured but time-limited approach to psychosocial support,24,26 and programs with a lower intensity prioritized scalability.27,29 Recent studies suggest that higher-intensity interventions often produce stronger psychosocial engagement but require greater cost, trained personnel, and sustained system capacity, which may limit accessibility in resource-limited settings.22,32 Conversely, lower-intensity interventions can expand reach and reduce delivery costs, but may require complementary support mechanisms to achieve meaningful behavioral change.32,33 These findings highlight the importance of identifying context-appropriate intensity levels that balance effectiveness, feasibility, and scalability when designing psychosocial support programs for pregnant adolescents.
Relevance and Adaptation for Indonesia
Indonesia has a strong primary health care system through community health center services (Puskesmas) and independent midwifery practices. Compared with the Nigerian study’s model, which is integrated into primary maternal care services, and the Australian study’s facility-based approach, a model embedded in routine antenatal care (ANC) services appears most realistic for the Indonesian context. Interventions that can be integrated into ANC visits without establishing a new system are more structurally and administratively feasible. Adapting an intervention model that utilizes primary care services such as Puskesmas and midwives allows for the inclusion of support and education components without the need for new service infrastructure. This is a more realistic approach within the Indonesian health system than a stand-alone, resource-intensive model.
Adaptation is not only structural but also cultural. In the Indonesian context, adolescent pregnancy is strongly influenced by cultural and religious norms surrounding premarital sex, where premarital pregnancy is widely perceived as socially unacceptable and may lead to stigma and social pressure from both families and the broader community.34 This requires a culturally sensitive, non-judgmental approach, and the inclusion of family support as a protective factor. Studies in Iran24 demonstrate the importance of interventions developed through exploring the contextual needs of pregnant adolescents, which is relevant in Indonesia, where social norms and family values are highly dominant. Therefore, intervention models cannot be adopted directly without a process of cultural adaptation. Cultural adaptation can be achieved through reframing language to make it more non-stigmatizing and avoid netively labeling mental health, involving the family as the primary support system in the intervention process, integrating religious values as a coping mechanism aligned with community beliefs, and modifying delivery methods to suit local literacy levels and communication norms to make them more easily understood and accepted by pregnant adolescents.
In terms of technology, although many health intervention studies use SMS or phone systems, the Indonesian digital context demonstrates the dominance of instant messaging apps and social media. Recent digital reports indicate that WhatsApp is the most widely used app in Indonesia, with approximately 112 million active users, making it one of the primary communication platforms.35 Therefore, if a digital component is to be integrated, a more realistic platform would be WhatsApp support groups or app-based reminder messages. This adaptation is crucial to ensure the intervention remains practical and relevant to the everyday communication patterns of Indonesian adolescents.
Limited human resources are also a crucial consideration in adapting psychosocial interventions in Indonesia. Various studies have shown that the distribution of health workers in Puskesmas remains uneven, with some regions experiencing shortages of doctors and midwives, particularly in remote areas and Eastern Indonesia.36 This situation can increase the workload of health workers, particularly midwives, who are the primary providers of antenatal care at the primary level. Therefore, intervention models with high intensity, numerous face-to-face sessions, or complex multidisciplinary engagement may be difficult to implement widely. In this context, simpler, more structured intervention approaches that can be integrated into routine services by primary health workers after brief training are more realistic, while still providing necessary support to pregnant adolescents through a combination of face-to-face and digital approaches.
Overall, adaptive model for Indonesia is an intervention integrated within Puskesmas, low-cost, does not significantly burden the system, and uses a hybrid approach of face-to-face and simple digital support. This model allows for greater sustainability, scalability, and cultural acceptance, without relying on additional resources that are difficult to meet within Indonesia’s current health system.
Limitations
This scoping review has several limitations that should be acknowledged. Only six studies met the inclusion criteria, indicating that the current evidence base on psychosocial programs for pregnant adolescents remains limited. The identified interventions were developed within specific sociocultural and health system contexts which may not fully reflect the diversity of Southeast Asian settings. As a result, direct transferability to Indonesia should be interpreted with caution. In addition, the present study proposes a conceptual adaptation rather than an empirically validated intervention model. The recommended adaptation strategies are derived from interpretive synthesis and contextual analysis and have not yet undergone stakeholder validation, feasibility assessment, or field testing within the Indonesian healthcare.
Recommendations
Future research should focus on developing and empirically testing culturally adapted psychosocial programs for pregnant adolescents within the Indonesian health system. Pilot implementation studies integrated into routine antenatal care services at Puskesmas and midwifery practices are recommended to assess feasibility and acceptability in real-world settings. Further research should also explore the involvement of family members as part of the support system, given the strong influence of family structures in Indonesia. In addition, digital support components using commonly used platforms such as WhatsApp may be explored to enhance accessibility and continuity of psychosocial support for adolescents. Finally, stakeholder engagement, including healthcare providers, adolescents, and policymakers, is essential to ensure that future interventions are contextually relevant, culturally sensitive, and scalable within existing maternal health services.
Conclusion
This review highlights that psychosocial support programs demonstrate considerable potential to improve the well-being of pregnant adolescents by addressing emotional, social, and behavioral challenges during pregnancy and early motherhood. However, the review of existing programs also highlights several implementation challenges, including the need for sustained participant engagement, availability of trained facilitators, and the substantial time and resource commitments required for higher-intensity interventions. These challenges may limit the feasibility of implementing certain models, particularly in resource-constrained health systems. Therefore, future adaptations of psychosocial programs should focus on optimizing delivery strategies to enhance feasibility, cultural relevance, and scalability within the Indonesian context. Developing context-sensitive models that balance intervention intensity with available resources may improve program effectiveness while maintaining accessibility for pregnant adolescents. Overall, these findings underscore the importance of adapting evidence-based psychosocial interventions to strengthen supportive care for pregnant adolescents and promote healthier maternal-child outcomes in Indonesia.
Abbreviations
ANC, Antenatal Care; EPDS, Edinburgh Postnatal Depression Scale; LMICs, Low- and Middle-Income Countries; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, Randomized Controlled Trial.
Acknowledgments
The authors appreciated the Universitas Padjadjaran for facilitating the database search and financial support for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang J. Autonomously connected: adolescent autonomy in the contexts of family, peer, and school.Utrecht: Utrecht University, 2025. 274 p. doi:10.33540/3112
2. Crocetti E. Identity formation in adolescence: the dynamic of forming and consolidating identity commitments. Child Dev Perspect. 2017;11(2):145–12. doi:10.1111/cdep.12226
3. Naghizadeh S, Mirghafourvand M. Knowledge and attitudes of adolescent girls and their mothers about early pregnancy: a cross-sectional study. BMC Pregnancy Childbirth. 2022;22(1). doi:10.1186/s12884-022-04551-z
4. Neal S, Matthews Z, Frost M, Fogstad H, Camacho A, Laski L. Childbearing in adolescents aged 12–15 years in low resource countries: a neglected issue. New estimates from demographic and household surveys in 42 countries. Acta Obstet Gynecol Scand. 2012;91(9):1114–1118. doi:10.1111/j.1600-0412.2012.01467.x
5. Gurung R, Målqvist M, Hong Z, et al. The burden of adolescent motherhood and health consequences in Nepal. BMC Pregnancy Childbirth. 2020;20(1). doi:10.1186/s12884-020-03013-8
6. UNICEF. Early childbearing. UNICEF for every child. 2024.
7. Malunga G, Sangong S, Saah FI, Bain L. Prevalence and factors associated with adolescent pregnancies in Zambia: a systematic review from 2000–2022. Arch Public Health. 2023;81:27. doi:10.1186/s13690-023-01045-y
8. Yakubu I, Salisu W. Determinants of adolescent pregnancy in sub-Saharan Africa: a systematic review. Reprod Health. 2018;15(1). doi:10.1186/s12978-018-0460-4
9. Kumari R, Pal SK, Kumar J. Exploring the patterns and socio-economic determinants of teenage pregnancy in India. Int J Community Med Public Heal. 2025;12(5):2124–2134. doi:10.18203/2394-6040.ijcmph20251365
10. Mohr R, Carbajal J, Sharma B. The influence of educational attainment on teenage pregnancy in low-income countries: a systematic literature review. J Soc Work Glob Commun. 2019;4:2. doi:10.5590/JSWGC.2019.04.1.02
11. Pradhan R, Wynter K, Fisher J. Factors associated with pregnancy among adolescents in low-income and lower middle-income countries: a systematic review. J Epidemiol Community Heal. 2015;69:918–924. doi:10.1136/jech-2014-205128
12. Kassa G, Arowojolu A, Odukogbe A, Yalew A. Prevalence and determinants of adolescent pregnancy in Africa: a systematic review and Meta-analysis. Reprod Health. 2018;15:195. doi:10.1186/s12978-018-0640-2
13. Wang R, Xu S, Hao X, et al. Anemia during pregnancy and adverse pregnancy outcomes: a systematic review and meta-analysis of cohort studies. Front Glob Women’s Heal. 2025;6:1502585. doi:10.3389/fgwh.2025.1502585
14. Maheshwari M, Khalid N, Patel P, Alghareeb R, Hussain A. Maternal and neonatal outcomes of adolescent pregnancy: a narrative review. Cureus. 2022;14. doi:10.7759/cureus.25921
15. Staniczek J, Manasar-Dyrbuś M, Stojko R, et al. Adolescent pregnancy: a comparative insight into the prevalence and risks of obstetric complications in a Polish cohort. J Clin Med. 2024;13(19):5785. doi:10.3390/jcm13195785
16. De Carvalho AF, Guaranha DDFK, Marmett B, et al. Mental health issues in adolescent mothers and young adult mothers: the Brazilian context. J Pediatr. 2025;101(4):608–615. doi:10.1016/j.jped.2025.03.011
17. Mwita M, Konje E, Patten S, Dewey D. Depressive and generalized anxiety symptoms among adolescent pregnant women attending antenatal clinics in Mwanza Tanzania. Discov Ment Heal. 2025;5:1–7. doi:10.1007/s44192-025-00291-6
18. Wainaina C, Sidze E, Maina B, et al. Psychosocial challenges and individual strategies for coping with mental stress among pregnant and postpartum adolescents in Nairobi informal settlements: a qualitative investigation. BMC Pregnancy Childbirth. 2021;21(1). doi:10.1186/s12884-021-04128-2
19. Badan Pusat Statistik. Age specific fertility Rate/ASFR (15-19) by Area, 2017. BPS-Statistics Indonesia. 2020.
20. Wijaya AA, Agustina D, Utami TN. Effectiveness of PKPR program on adolescent reproductive health at sigambal health center. J Biomedika Dan Kesehat. 2025;8(2):181–191. doi:10.18051/JBiomedKes.2025.v8.181-191
21. Ministry of Health of the Republic of Indonesia. Peraturan Menteri Kesehatan Nomor 21 Tahun 2021 tentang Penyelenggaraan Pelayanan Kesehatan Masa Sebelum Hamil, Masa Hamil, Persalinan, dan Masa Sesudah Melahirkan, Pelayanan Kontrasepsi, dan Pelayanan Kesehatan Seksual [Regulation of the Minister of Health Number 21 of 2021 on the Implementation of Health Services Before Pregnancy, During Pregnancy, Childbirth, Postpartum, Contraceptive Services, and Sexual Health Services]. Jakarta; 2023.
22. Laurenzi CA, Gordon S, Abrahams N, et al. Psychosocial interventions targeting mental health in pregnant adolescents and adolescent parents: a systematic review. Reprod Health. 2020;17(65):1–15. doi:10.1186/s12978-020-00913-y
23. Trapé CA, Sivalli Campos CM, de Freitas Oliveira C, et al. Scoping review of evidence synthesis: concepts, types and methods. PLoS One. 2025;20(5):e0323555. doi:10.1371/journal.pone.0323555
24. Yousefi S, Montazeri S, Javadifar N. Design, implementation, and evaluation of a psychosocial intervention to improve mental health in pregnant adolescents: a mixed-methods protocol. Reprod Health. 2025;22(119):1–13. doi:10.1186/s12978-024-01916-9
25. Gureje O, Kola L, Oladeji BD, et al. Responding to the challenge of adolescent perinatal depression (RAPID): protocol for a cluster randomized hybrid trial of psychosocial intervention in primary maternal care. Trials. 2020;21(1):1–11. doi:10.1186/s13063-020-4086-9
26. Salisbury TT, Atmore KH, Nhambongo I, et al. Integrating human-centred design into the development of an intervention to improve the mental wellbeing of young women in the perinatal period: the Catalyst project. BMC Pregnancy Childbirth. 2021;21(183):1–11. doi:10.1186/s12884-020-03485-8
27. Sewpaul R, Resnicow K, Crutzen R, Dukhi N, Ellahebokus A, Reddy P. A tailored mhealth intervention for improving antenatal care seeking and health behavioral determinants during pregnancy among adolescent girls and young women in south africa: development and protocol for a pilot randomized controlled trial. JMIR Res Protoc. 2023;12:1–14. doi:10.2196/43654
28. Payne NA, Anastas JW. The mental health needs of low-income pregnant teens: a nursing – social work partnership in care. Res Soc Work Pract. 2016;25(5):595–606. doi:10.1177/1049731514545656
29. Styles A, Loftus V, Nicolson S, Harms L. Prenatal yoga for young women a mixed methods study of acceptability and benefits. BMC Pregnancy Childbirth. 2019;19(499):1–12. doi:10.1186/s12884-019-2564-4
30. Fatori D, Argeu A, Brentani H, et al. Maternal parenting electronic diary in the context of a home visit intervention for adolescent mothers in an Urban deprived area of São Paulo, Brazil: randomized controlled trial. JMIR mHealth uHealth. 2020;8(7):1–15. doi:10.2196/13686
31. Walton S, Roberson K, Onsomu E, Hall S, Dearman C. Evaluating Centering group prenatal care in rural women with low socioeconomic status to promote access to care and improve pregnancy outcomes. J Public Health. 2021;29(2):285–291. doi:10.1007/s10389-019-01121-0
32. Montazeri S, Yousefi S, Javadifar N. Psychosocial prenatal interventions for teenage pregnant: a systematic review. J Fam Reprod Heal. 2025;19(2):69–84. doi:10.18502/jfrh.v19i2.19295
33. Sangsawang B, Deoisres W, Hengudomsub P, Sangsawang N. Effectiveness of psychosocial support provided by midwives and family on preventing postpartum depression among first-time adolescent mothers at 3-month follow-up: a randomised controlled trial. J Clin Nurs. 2022;31(5–6):689–702. doi:10.1111/jocn.15928
34. Astuti AW, Hirst J, Bharj KK. Indonesian adolescents’ experiences during pregnancy and early parenthood: a qualitative study. J Psychosom Obstet Gynecol. 2020;41(4):317–326. doi:10.1080/0167482X.2019.1693538
35. Prasastisiwi AH. Indonesia Masuk 3 Besar Negara Pengguna WhatsApp Terbanyak di Dunia [Indonesia ranks among the top three countries with the largest WhatsApp users in the world]. GoodStats. 2024.
36. Nurul H, Rahman H, Ayu P. Membandingkan Ketimpangan Ketersediaan Tenaga Kesehatan Puskesmas di Wilayah Indonesia Timur [Comparing inequalities in the availability of primary health center workforce in eastern Indonesia]. Wind Public Heal J. 2020;1(1):31–37. doi:10.33096/woph.v1i1.8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.